Embed Size (px)
Citation preview
REVIEW
Current status of corneal collagen cross-linking for keratoconus: a review
Clin Exp Optom 2013; 96: 155–164 DOI:10.1111/cxo.12020
Elsie Chan FRANZCOGrant R Snibson FRCS FRANZCOFRCOphth(UK)Royal Victorian Eye and Ear Hospital, Melbourne,Australia and Centre for Eye Research Australia,Melbourne, AustraliaE-mail: [email protected]
Over the past decade, corneal collagen cross-linking has become commonplace as atreatment option for individuals with progressive keratoconus. This is based on laboratorydata suggesting that cross-linking using riboflavin and ultraviolet-A irradiation increasescollagen diameter and the biomechanical strength of the treated cornea. Case series andlimited randomised controlled trials support these findings with data demonstrating thatcross-linking slows and possibly halts the progression of keratoconus. In some patientscross-linking results in an improvement in maximum corneal curvature, visual acuity,spherical equivalent and higher-order aberrations. The number of reported complicationsis small. More recently, variations in the treatment protocol have been described, althoughthey have not yet been subject to comparative studies. While the published data indicatecross-linking is effective in modifying the natural history of keratoconus, the long-termimpact of this treatment is still unknown. This paper reviews the theoretical basis, pre-clinicalresearch and clinical results of corneal collagen cross-linking in keratoconus.
Submitted: 1 August 2012Revised: 24 September 2012Accepted for publication: 3 October 2012
Key words: collagen, cornea, cross-linking, keratoconus
Until recently, individuals diagnosed withkeratoconus had the choice of spectacles,rigid contact lenses and in some cases intra-corneal ring segments to improve theirvisual acuity; however, none of these optionsalter the natural history of the disease andeventually patients with advanced diseasemay require corneal transplantation forvisual rehabilitation. Keratoconus remainsthe leading indication for corneal grafting inAustralasia.1
Over the past decade, corneal collagencross-linking has been introduced as a treat-ment that has been reported to slow or haltthe progression of disease. It is based ona theory that the decreased biomechanicalstrength of the cornea in eyes with kerato-conus may be related to a decrease in intra-and inter-fibrillar cross-links within collagenfibres.2 The induction of molecular cross-links appears to increase corneal stabilityand thus slows the progression of thedisease. This review outlines the develop-ment of corneal collagen cross-linking andreviews the studies published on this topic inthe peer-reviewed literature.
BACKGROUND
The concept of cross-linking has beenaround for some time in industry. The
formation of covalent bonds between longpolymer molecules to increase the strengthof materials is used in other fields, includ-ing the manufacturing of plastics and theproduction of bioprosthetic heart valves.Spoerl and Seiler3 and Spoerl, Huhle andSeiler4 in 1998 were the first to introducethe concept of using cross-linking tostrengthen corneal tissue, exploring differ-ent techniques using both photosensi-tisation and chemical cross-linking. Thecurrent technique involves the use of ribo-flavin (vitamin B2), which is exposed to ameasured dose of longer wavelength ultra-violet A light (UVA) radiation (370 nm)at 3 mW/cm2 (5.4 J/cm2). Riboflavin is ahydrophilic compound with a molecularweight of 376.37 g/mol. It has three lightabsorption peaks at 270 nm, 366 nm and445 nm, with the middle wavelength pro-viding the greatest margin of safety for theocular structures. Riboflavin plays two rolesin corneal collagen cross-linking, actingboth as a photosensitiser and absorbingultraviolet radiation to limit the depth ofthe treatment effect. In the photosensitis-ing process, free radicals are produced,which catalyse a reaction resulting in theformation of covalent bonds between thecollagen molecules and microfibrils.5,6 Thisis a process that may involve singlet oxygen
production, although the exact mechanismis not fully understood.7
EFFECTS OF CROSS-LINKING ONTHE CORNEA
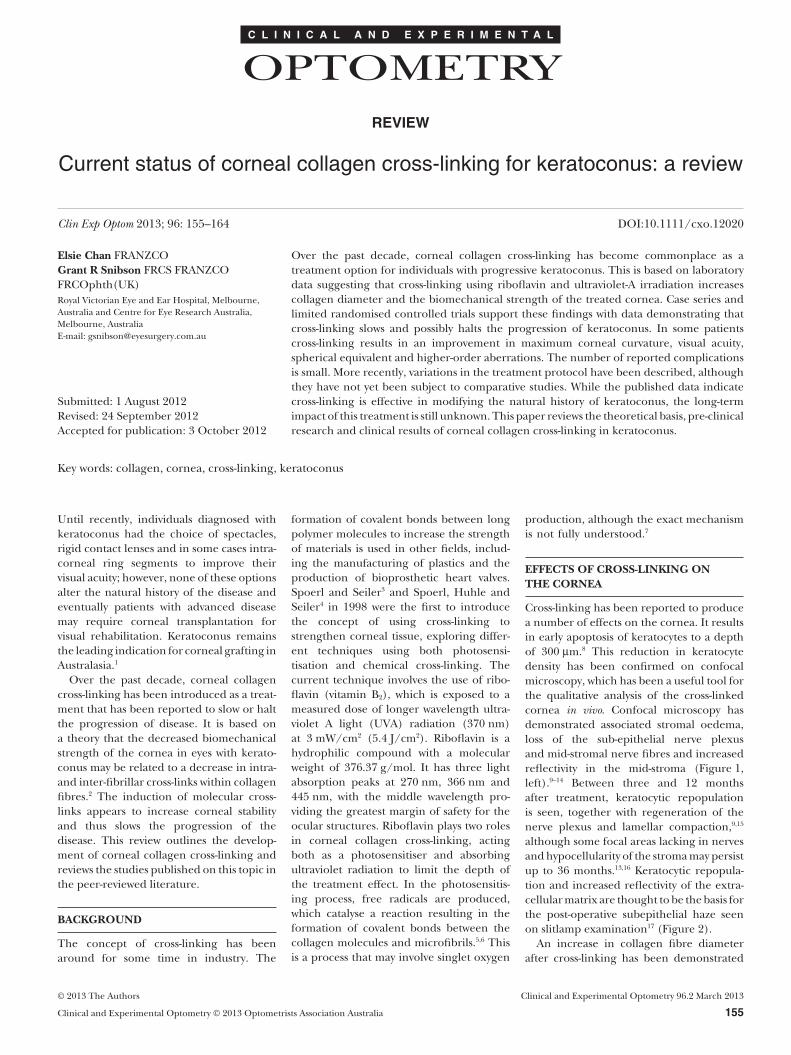
Cross-linking has been reported to producea number of effects on the cornea. It resultsin early apoptosis of keratocytes to a depthof 300 mm.8 This reduction in keratocytedensity has been confirmed on confocalmicroscopy, which has been a useful tool forthe qualitative analysis of the cross-linkedcornea in vivo. Confocal microscopy hasdemonstrated associated stromal oedema,loss of the sub-epithelial nerve plexusand mid-stromal nerve fibres and increasedreflectivity in the mid-stroma (Figure 1,left).9–14 Between three and 12 monthsafter treatment, keratocytic repopulationis seen, together with regeneration of thenerve plexus and lamellar compaction,9,15
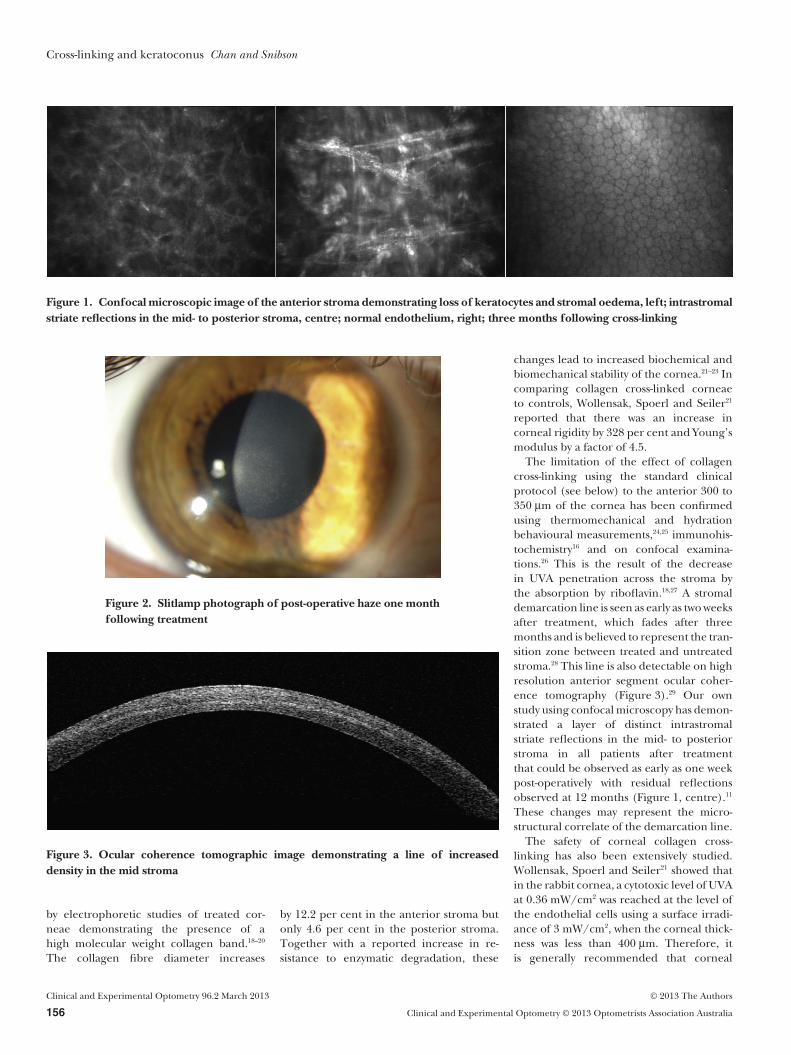
although some focal areas lacking in nervesand hypocellularity of the stroma may persistup to 36 months.13,16 Keratocytic repopula-tion and increased reflectivity of the extra-cellular matrix are thought to be the basis forthe post-operative subepithelial haze seenon slitlamp examination17 (Figure 2).
An increase in collagen fibre diameterafter cross-linking has been demonstrated
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 155
by electrophoretic studies of treated cor-neae demonstrating the presence of ahigh molecular weight collagen band.18–20
The collagen fibre diameter increases
by 12.2 per cent in the anterior stroma butonly 4.6 per cent in the posterior stroma.Together with a reported increase in re-sistance to enzymatic degradation, these
changes lead to increased biochemical andbiomechanical stability of the cornea.21–23 Incomparing collagen cross-linked corneaeto controls, Wollensak, Spoerl and Seiler21
reported that there was an increase incorneal rigidity by 328 per cent and Young’smodulus by a factor of 4.5.
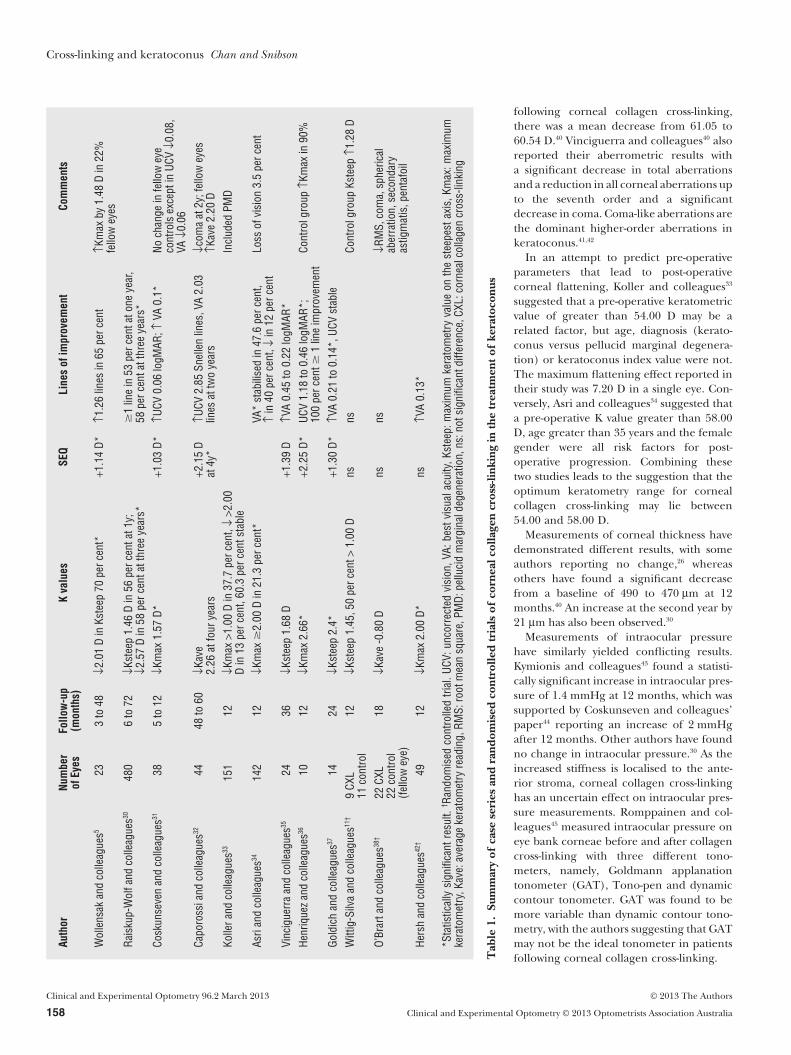
The limitation of the effect of collagencross-linking using the standard clinicalprotocol (see below) to the anterior 300 to350 mm of the cornea has been confirmedusing thermomechanical and hydrationbehavioural measurements,24,25 immunohis-tochemistry16 and on confocal examina-tions.26 This is the result of the decreasein UVA penetration across the stroma bythe absorption by riboflavin.18,27 A stromaldemarcation line is seen as early as two weeksafter treatment, which fades after threemonths and is believed to represent the tran-sition zone between treated and untreatedstroma.28 This line is also detectable on highresolution anterior segment ocular coher-ence tomography (Figure 3).29 Our ownstudy using confocal microscopy has demon-strated a layer of distinct intrastromalstriate reflections in the mid- to posteriorstroma in all patients after treatmentthat could be observed as early as one weekpost-operatively with residual reflectionsobserved at 12 months (Figure 1, centre).11
These changes may represent the micro-structural correlate of the demarcation line.
The safety of corneal collagen cross-linking has also been extensively studied.Wollensak, Spoerl and Seiler21 showed thatin the rabbit cornea, a cytotoxic level of UVAat 0.36 mW/cm2 was reached at the level ofthe endothelial cells using a surface irradi-ance of 3 mW/cm2, when the corneal thick-ness was less than 400 mm. Therefore, itis generally recommended that corneal
Figure 1. Confocal microscopic image of the anterior stroma demonstrating loss of keratocytes and stromal oedema, left; intrastromalstriate reflections in the mid- to posterior stroma, centre; normal endothelium, right; three months following cross-linking
Figure 2. Slitlamp photograph of post-operative haze one monthfollowing treatment
Figure 3. Ocular coherence tomographic image demonstrating a line of increaseddensity in the mid stroma
Cross-linking and keratoconus Chan and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
156 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

collagen cross-linking is performed only ineyes where the minimum stromal thicknessis 400 mm, the depth at which the UV irradi-ance is half the threshold for damage tothe endothelial cell layer. Spoerl and col-leagues27 further calculated the radiantexposures to the anterior lens surface, pos-terior lens surface and retina, all of whichwere well below the damage threshold.Based on these findings, four criteria wereproposed for ‘safe’ treatment:1. the epithelium should be removed to
encourage riboflavin absorption2. riboflavin (0.1 per cent) should be
applied for 30 minutes prior to UVA3. homogenous UV irradiance should be
delivered at 3 mW/cm2 and4. the minimum stromal thickness should
be maintained at 400 um or greater.27
TREATMENT PROTOCOLS
The most widely used treatment protocol isbased on the protocol from Dresden. Whilein their earlier studies the cornea was soakedwith riboflavin drops for five minutes priorto 30 minutes of UVA irradiation,22 this waslater extended to soaking for 30 minute with
riboflavin.27 At the beginning of the proce-dure, topical anaesthetic is applied beforea 9.0 mm epithelial debridement is per-formed. Riboflavin 0.1 per cent solution in20 per cent dextran is then instilled everythree to five minutes for 30 minutes. Slit-lamp examination is performed to confirmthe presence of riboflavin in the aqueousprior to commencement of UV irradiationat 370 nm, with an irradiance of 3 mW/cm2
at a diameter of 8.0 mm for 30 minutes.During irradiation, riboflavin and topicalanaesthetic are continued every four to fiveminutes (Figure 4). At the conclusion oftreatment, ofloxacin ointment is appliedand a bandage contact lens soaked with 0.3per cent ofloxacin is inserted and retaineduntil epithelium healing is complete. Alter-native protocols differ mainly in the dura-tion of the riboflavin soaking period, whichthey perform for 10 minutes.14 Other minorvariations include the use of other pre-operative drops, such as pilocarpine oneper cent to reduce UV light penetration tothe lens and posterior segment. Topicalsteroid and non-steroidal anti-inflammatorydrops are commonly used during the post-operative period.11,14
CLINICAL STUDIES
Corneal collagen cross-linking has beenrapidly incorporated into clinical practicearound the world over the past 10 years, withan ever-increasing number of publicationsreporting its safety and efficacy in reducingthe progression of keratoconus; however,only a few randomised controlled trials havebeen conducted.
Case seriesA summary of some of the published caseseries5,11,30–38 is shown in Table 1. The firstreport of the clinical outcomes of cornealcollagen cross-linking was published by Wol-lensak, Spoerl and Seiler,5 where 23 eyes of22 patients were treated with corneal colla-gen cross-linking. Progression of kerato-conus was halted in all eyes, with a decreasein corneal curvature of 2.00 D seen in 16eyes. Subsequent studies have shown areduction in the mean spherical equivalentwith a hyperopic shift, an improvement inthe uncorrected vision and visual acuity, areduction in topographic power and increas-ing corneal symmetry. The average improve-ment in the maximum keratometric reading(Kmax or Ksteep, the maximum keratomet-ric reading on the steep axis) ranges from1.46 to 2.26 D. This is in contrast to fellow eyecontrol groups, where there was a progres-sion of disease.5,32 While there remains alimited number of longer-term studies, thetwo published studies suggest stabilisationof K values after one to two years.30,32 Unpub-lished results from the randomised control-led trial conducted in Melbourne suggestthat there are a few treated patients whocontinue to improve even beyond three orfour years of treatment.
Caporossi and colleagues39 report that theinitial worsening of keratometric readingsobserved in the first month may be due totransient haze and corneal oedema. Simi-larly, Doors and colleagues29 postulated thatit may be due to corneal remodelling in thefirst month. In contrast, Vinciguerra andcolleagues40 suggested that it may be theresult of epithelial debridement. Immedi-ately after the removal of epithelium, theyfound that the steepest point on the anteriorcurvature changed from a mean of 58.82 Dto 61.05 D. This may be in part due tothe epithelial layer being thickest aroundthe cone and thinnest at its apex, mask-ing the underlying steepness. Comparingtopographic values at the steepest pointafter de-epithelialisation and one month
Figure 4. Intra-operative photograph demonstrating the ultravio-let light source irradiating the cornea, which has been soakedwith riboflavin
Cross-linking and keratoconus Chan and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 157
following corneal collagen cross-linking,there was a mean decrease from 61.05 to60.54 D.40 Vinciguerra and colleagues40 alsoreported their aberrometric results witha significant decrease in total aberrationsand a reduction in all corneal aberrations upto the seventh order and a significantdecrease in coma. Coma-like aberrations arethe dominant higher-order aberrations inkeratoconus.41,42
In an attempt to predict pre-operativeparameters that lead to post-operativecorneal flattening, Koller and colleagues33
suggested that a pre-operative keratometricvalue of greater than 54.00 D may be arelated factor, but age, diagnosis (kerato-conus versus pellucid marginal degenera-tion) or keratoconus index value were not.The maximum flattening effect reported intheir study was 7.20 D in a single eye. Con-versely, Asri and colleagues34 suggested thata pre-operative K value greater than 58.00D, age greater than 35 years and the femalegender were all risk factors for post-operative progression. Combining thesetwo studies leads to the suggestion that theoptimum keratometry range for cornealcollagen cross-linking may lie between54.00 and 58.00 D.
Measurements of corneal thickness havedemonstrated different results, with someauthors reporting no change,26 whereasothers have found a significant decreasefrom a baseline of 490 to 470 mm at 12months.40 An increase at the second year by21 mm has also been observed.30
Measurements of intraocular pressurehave similarly yielded conflicting results.Kymionis and colleagues43 found a statisti-cally significant increase in intraocular pres-sure of 1.4 mmHg at 12 months, which wassupported by Coskunseven and colleagues’paper44 reporting an increase of 2 mmHgafter 12 months. Other authors have foundno change in intraocular pressure.30 As theincreased stiffness is localised to the ante-rior stroma, corneal collagen cross-linkinghas an uncertain effect on intraocular pres-sure measurements. Romppainen and col-leagues45 measured intraocular pressure oneye bank corneae before and after collagencross-linking with three different tono-meters, namely, Goldmann applanationtonometer (GAT), Tono-pen and dynamiccontour tonometer. GAT was found to bemore variable than dynamic contour tono-metry, with the authors suggesting that GATmay not be the ideal tonometer in patientsfollowing corneal collagen cross-linking.
Auth
orNu
mbe
rof
Eyes
Follo
w-u
p(m
onth
s)K
valu
esSE
QLi
nes
ofim
prov
emen
tCo
mm
ents
Wol
lens
akan
dco
lleag
ues5
233
to48
↓2.0
1D
inKs
teep
70pe
rcen
t*+1
.14
D*↑1
.26
lines
in65
perc
ent
↑Km
axby
1.48
Din
22%
fello
wey
esRa
isku
p-W
olfa
ndco
lleag
ues30
480
6to
72↓K
stee
p1.
46D
in56
perc
enta
t1y;
↓2.5
7D
in58
perc
enta
tthr
eeye
ars*
�1
line
in53
perc
enta
tone
year
,58
perc
enta
tthr
eeye
ars*
Cosk
unse
ven
and
colle
ague
s3138
5to
12↓K
max
1.57
D*+1
.03
D*↑U
CV0.
06lo
gMAR
;↑VA
0.1*
Noch
ange
infe
llow
eye
cont
rols
exce
ptin
UCV
↓0.0
8,VA
↓0.0
6Ca
poro
ssia
ndco
lleag
ues32
4448
to60
↓Kav
e2.
26at
four
year
s+2
.15
Dat
4y*
↑UCV
2.85
Snel
len
lines
,VA
2.03
lines
attw
oye
ars
↓com
aat
2y;f
ello
wey
es↑K
ave
2.20
DKo
llera
ndco
lleag
ues33
151
12↓K
max
>1.0
0D
in37
.7pe
rcen
t,↓
>2.0
0D
in13
perc
ent,
60.3
perc
ents
tabl
eIn
clud
edPM
D
Asri
and
colle
ague
s3414
212
↓Km
ax�
2.00
Din
21.3
perc
ent*
VA*
stab
ilise
din
47.6
perc
ent,
↑in
40pe
rcen
t,↓
in12
perc
ent
Loss
ofvi
sion
3.5
perc
ent
Vinc
igue
rra
and
colle
ague
s3524
36↓K
stee
p1.
68D
+1.3
9D
↑VA
0.45
to0.
22lo
gMAR
*He
nriq
uez
and
colle
ague
s3610
12↓K
max
2.66
*+2
.25
D*UC
V1.
18to
0.46
logM
AR*;
100
perc
ent�
1lin
eim
prov
emen
tCo
ntro
lgro
up↑K
max
in90
%
Gold
ich
and
colle
ague
s3714
24↓K
stee
p2.
4*+1
.30
D*↑V
A0.
21to
0.14
*,UC
Vst
able
Witt
ig-S
ilva
and
colle
ague
s11†
9CX
L11
cont
rol
12↓K
stee
p1.
45,5
0pe
rcen
t>1.
00D
nsns
Cont
rolg
roup
Kste
ep↑1
.28
D
O’Br
arta
ndco
lleag
ues38
†22
CXL
22co
ntro
l(fe
llow
eye)
18↓K
ave
-0.8
0D
nsns
↓RM
S,co
ma,
sphe
rical
aber
ratio
n,se
cond
ary
astig
mat
is,p
enta
foil
Hers
han
dco
lleag
ues42
†49
12↓K
max
2.00
D*ns
↑VA
0.13
*
*Sta
tistic
ally
sign
ifica
ntre
sult.
† Rand
omis
edco
ntro
lled
trial
.UCV
:unc
orre
cted
visi
on,V
A:be
stvi
sual
acui
ty,K
stee
p:m
axim
umke
rato
met
ryva
lue
onth
est
eepe
stax
is,K
max
:max
imum
kera
tom
etry
,Kav
e:av
erag
eke
rato
met
ryre
adin
g,RM
S:ro
otm
ean
squa
re,P
MD:
pellu
cid
mar
gina
ldeg
ener
atio
n,ns
:not
sign
ifica
ntdi
ffere
nce,
CXL:
corn
ealc
olla
gen
cros
s-lin
king
Tab
le1.
Sum
mar
yof
case
seri
esan
dra
ndom
ised
cont
rolle
dtr
ials
ofco
rnea
lcol
lage
ncr
oss-
linki
ngin
the
trea
tmen
tof
kera
toco
nus
Cross-linking and keratoconus Chan and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
158 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

Randomised controlled trialsWittig-Silva and colleagues11 in 2008 pub-lished the early results from a randomisedcontrolled prospective study performed inMelbourne. In this paper, nine eyes under-went corneal collagen cross-linking and11 eyes were in the control group with12-month data reported. There was a signifi-cant improvement in visual acuity andflattening in maximum and average K inthe treatment group, whereas deteriorationof these parameters was recorded in thecontrol group. A second randomised, fellow-eye controlled trial was published by O’Brartand colleagues38 in 2011. After 18 months,there was an improvement in simulatedkeratometry, 3.0 mm and 5.0 mm keratom-etry, simulated astigmatism and coneapex power and wavefront measurements(root mean square, coma and pentafoil)compared with untreated eyes. No treatedeyes progressed, whereas three out of 22untreated eyes showed progression. Interest-ingly, the reduction in keratometricmeasurements was less in these two ran-domised controlled trials than in severalearlier studies and no significant differencewas seen in visual acuity and sphericalequivalent.
The most recently reported randomisedcontrolled trial46 was part of the multicentretrial performed under the guidelines of theUS Food and Drug Administration andincluded patients with both keratoconusand post-laser in situ keratomileusis (LASIK)ectasia. Eyes randomised to the controlgroup crossed over to the treatment groupafter only three months. A second controlgroup included the fellow eye of partici-pants, although there was no requirementfor this eye to have any signs of ectasia or tomeet the other inclusion criteria of thestudy. One-year data were published byHersch, Greenstein and Fry46 and the kera-toconus subgroup results are shown inTable 1. Treatment failures occurred in 4.2per cent (one patient with keratoconus andtwo with post-LASIK ectasia).
Paediatric case seriesWhile the onset of keratoconus usuallyoccurs during the second decade of life,those diagnosed at a much younger agehave a greater rate of progression leading tocorneal transplantation.47,48 Corneal trans-plantation in the young can be successful49
with a 90 per cent graft survival rate at 10years in adolescent (13 to 19 years) recipi-ents reported in the Australian Corneal
Graft Registry.49 Overall, the 20-year graftsurvival for a penetrating graft for kerato-conus in recipients of all ages is 49 per cent.50
As each subsequent transplant has a higherrisk of early failure,51 delaying surgery, par-ticularly in this young group of patients,would be advantageous.
There have been two studies reporting theresults of corneal collagen cross-linking forprogressive keratoconus in a paediatric agegroup (up to 18 years) over two years.39,52
Both found a statistically significant gainin uncorrected vision and visual acuitywith Vinciguerra and colleagues’ study52
also reporting significant improvementsin spherical equivalent (1.57 D), simulatedkeratometry in the flat meridian (46.32 to45.30 D) and mean average corneal power(49.69 to 48.90 D). Interestingly, neitherstudy found any change in Kmax or simu-lated keratometry in the steep meridian,which had been observed in adult studies.Some of the previously mentioned studieshave also included patients from the age of10 years,32 13 years5 and 14 years,46 althoughthere has been no sub-analysis for theyounger age group.
VARIATIONS INTREATMENT PROTOCOLS
Thin corneaeBased on the work of Wollensak and col-leagues, Hafezi and colleagues53 introducedthe use of hypo-osmolar riboflavin to swellthe cornea where the stromal bed was lessthan 400 mm. Hypo-osmolar riboflavin isformulated with dextran and has a low col-loidal osmotic pressure. Corneal thicknesswas measured prior to treatment and hypo-osmolar riboflavin was instilled until thestromal thickness was at least 400 mm. A vari-able degree of stromal swelling was noted,ranging from 36 to 105 mm over periodsranging from three to 20 minutes.
There have been limited studies on theefficacy of corneal collagen cross-linkingin thin corneae less than 400 mm. Usingimmunohistochemistry to examine kerato-cyte counts, there was no difference in eyebank corneal buttons where hypo-osmolarriboflavin was used compared to isotonicriboflavin.16 A clinical study of 32 eyes over12 months using hypo-osmolar riboflavin toswell the cornea to greater than 400 mmfound no change in mean K at the apex orthe visual acuity.54 Of more concern is therecent paper by Kymionis and colleagues,55
who reported using the Dresden protocolfor 14 eyes with a mean stromal thickness lessthan 400 mm. After 12 months, they found astatistically significant decrease in endothe-lial cell density from 2,733 to 2,441 cellsper mm2, despite an improvement in uncor-rected vision, visual acuity and mean Kvalues.
Kaya, Utine and Yilmaz56 took a diff-erent approach to thin corneae. Theyperformed custom pachymetry-guidedepithelial debridement to ensure that theepithelium remained intact in thinnerareas of less than 400 mm. They reportedtheir confocal examination findings,describing areas under intact epitheliumhaving no changes consistent with cornealcollagen cross-linking with minimal effecton keratocytes. This has implications forthe transepithelial technique describedbelow. No other subjective or objectiveresults were reported.
Transepithelial cornealcollagen cross-linkingDue to the post-operative pain and risk ofcomplications that result from epithelialdebridement, the concept of cross-linkingwith the epithelium remaining largely intactis appealing. As riboflavin does not readilypenetrate the intact epithelium,57 varyingtechniques have been used to promote ribo-flavin absorption into the stroma. Theseinclude the use of drops containing pre-servatives, such as benzalkonium chloridepre-operatively to break the epithelial tightjunctions or the creation of superficialepithelial trauma without complete epithe-lial debridement; however, animal studieshave not supported the use of incompletemanual epithelial removal.57 In such cases,the collagen cross-linking effect is reducedor non-homogenous.58 Similarly, topical pre-servatives may produce only one-fifth of thecross-linking effect achieved with completeepithelial removal.59
While transepithelial cross-linking isgaining popularity, there is limited support-ive clinical evidence in the peer-reviewedliterature. The first study describing cross-linking without epithelial debridement waspublished by Chan, Sharma and Wachler,60
who reported the use of intracorneal ringsegments with or without collagen cross-linking for the treatment of keratoconus.After placement of an inferior segment,the cornea was soaked with riboflavin withdiluted carboxymethylcellulose rather thandextran for five minutes followed by UVA for
Cross-linking and keratoconus Chan and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 159

30 minutes. An improvement was found inmanifest cylinder, average K and steepest Kin the cross-linked group.60
Two other studies have reported theirresults of transpithelial cross-linking. Lecci-sotti and Islam61 used a riboflavin prepara-tion containing gentamicin 0.3 per cent,ethylenediaminetetraacetic acid (EDTA)0.01 per cent and benzalkonium chloride0.01 per cent, which was instilled every 15minutes for three hours. Oxybuprocaine0.4 per cent containing the preservativep-hydroxybenzoate was then used everyfive minutes for 30 minutes. There was areported improvement in visual acuity by0.036 logMAR, spherical equivalent by0.35 D and mean average simulated K by only0.10 D.61 These results, while encouraging,suggest a lesser effect compared to cornealcollagen cross-linking with epithelial debri-dement. It remains to be seen what degree ofcross-linking is necessary to stop the progres-sion of keratoconus. Baiocchi, Mazzotta andCaporossi62 also posit that the dose of ultra-violet energy may need to be increased,where epithelium remains intact to achievethe same effect.
Fillipello, Stagni and O’Brart63 similarlyused an ‘enhanced’ riboflavin solution with0.1 per cent aqueous riboflavin contain-ing trometamol and sodium EDTA tobreak down epithelial intercellular junc-tions. Examination using anterior segmentoptical coherence tomography demon-strated a dense line at 100 mm, which com-pares with the demarcation line seen at adepth of 320 to 340 mm in conventionalcollagen cross-linking. This suggests thatthe effect of transepithelial collagen cross-linking may be more superficial.
Combined cornealcollagen cross-linking andrefractive surgeryCombining cross-linking with photorefrac-tive keratectomy (PRK) in eyes with kerato-conus is being performed by an increasingnumber of centres around the world and hasbeen reported by Kymionis and colleagues.64
After a mean follow-up of 19 months, therewas a significant improvement of 0.46 and0.084 logMAR units in uncorrected visionand visual acuity, respectively. The meanspherical equivalent improved from -2.30 to-1.08 D and mean steep and flat keratometricvalues improved 2.35 and 1.18 D, respec-tively; however, 10 per cent of eyes lostone line of visual acuity, which is greater
than the rate of loss of vision at 3.5 per centfor conventional corneal collagen cross-linking alone.34
Coskunseven and colleagues44 performeda randomised trial over six months compar-ing cross-linking followed by intracornealring segment implantation and cross-linkingperformed after ring segment implantationwith a mean duration between treatments ofseven months. While uncorrected vision,visual acuity, mean spherical equivalent,cylinder and mean K values improved inboth groups, the overall effect was greaterwhere cross-linking was performed after ringsegment implantation.44
It should be kept in mind that the flatten-ing effect over at least 24 months observedin cross-linking studies would make simul-taneous or sequential surface ablation orintracorneal ring segment implantationless predictable in its refractive outcome.To compensate for this, some clinicianstarget an undercorrection with the refractivetreatment.65
Duration of irradiationRocha and colleagues66 introduced theconcept of ‘flash-linking’, whereby a newcross-linking agent is used instead of ribofla-vin and the UVA irradiation stage only takes30 seconds at 4.2 mW/cm2, rather than theconventional 30 minutes at 3 mW/cm2. Thecross-linking agent used in their paper onporcine eyes was a polyvinyl pyrrolidone.Measurements of corneal stiffness usingsurface wave elastometry in ex vivo porcineeyes suggested that ‘flash-linking’ and con-ventional collagen cross-linking may have acomparable effect.66
It remains uncertain what the optimalparameters are to achieve an effective cross-linking effect using riboflavin and UVA.Modifications could be made to the ribofla-vin concentration or to the UVA dose. Someclinicians have advocated that using a higherirradiance of UVA with a shorter exposuretime may produce a similar effect to thatachieved using the Dresden protocol. WhileUVA devices delivering up to 18 mW/cm2
are available commercially, there are nopublished reports to support their safetyand efficacy. For the treatment of thinnercorneae, use of a higher concentration ofriboflavin may be safer due to the linearcorrelation that appears to exist between theabsorption coefficient and riboflavin con-centration up to 0.1 per cent.67 Alternatively,Wollensak, Spoerl and Seiler21 postulatedthat the UVA dose could be reduced to
2 mW/cm2 in thin corneae based on thework of Spoerl, Huhle and Seiler4 on theminimum dose to produce a stiffeningeffect.
IontophoresisThere are two recent reports that ionto-phoresis may increase the efficiency of ribo-flavin penetration into the corneal stroma.Iontophoresis involves the use of a smallelectrical current to enhance the penetra-tion of a drug across a tissue. Riboflavin issuitable for iontophoresis due to its lowmolecular weight, water solubility and itsnegative charge.68 The use of iontophoresishas two major advantages compared to thecurrent protocol using topical application ofriboflavin drops, as it can be performedacross the intact corneal epithelium andreduces the duration of the riboflavinsaturation phase. Pre-clinical testing hasdemonstrated the efficacy of this methodin increasing the mechanical rigidity of thecornea.69 Research into this promising newtechnique is continuing.
ADVERSE EFFECTS AND SAFETY
With a rapidly increasing number ofcross-linking procedures being performedaround the world, there is an increasingnumber of reports29,32,34,36,45,70–83 of adverseevents, which are outlined in Table 2. Whilea minor degree of stromal oedema seen onslitlamp examination may be seen in up to70 per cent of patients in the first monthand a temporary haze in 9.8 per cent32
(Figure 4), more significant stromal hazehas been reported in up to 8.6 per centof treated eyes and may persist for up tosix months.71 Other reported complica-tions have included recurrent erosion syn-drome,38 corneal oedema,34,36,70 Desçemetsmembrane folds,29 corneal melting andperforation.81,82
One of the most common complicationsappears to be the development of sterilecorneal infiltrates72–75 (Figure 5). These havebeen seen in up to 7.6 per cent of cases andresolve with an increase in topical steroidtherapy but sometimes leaving a residualscar.76 The pathogenesis of these sterile infil-trates is not known but may be the result ofan altered immune response to antigen ora phototoxic effect from the cross-linkingprocess.84
Microbial keratitis has also been reportedby various authors with a range of organisms,including pseudomonas,78 acanthamoeba79
Cross-linking and keratoconus Chan and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
160 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

and fusarium.80 Some of these cases requiredsubsequent penetrating keratoplasty.78,79
There are several potential risk factorsfor the development of microbial keratitis,which include the presence of an epithelialdefect, a contact lens and the use of topical
steroids or non-steroidal inflammatorydrops post-operatively. Cross-linking mayalso change the response of the corneato injury and infection.85 There has beenone report of herpes simplex virus-relatedkeratouveitis.83
The most worrying complications arereported cases of endothelial damage. Inone case, the corneal thickness had been 400mm prior to epithelial removal and isotonicriboflavin had been used.70 In anotherreport, the endothelial cell count followingcollagen cross-linking was 1,776 cells permm2 compared to 2,978 cells per mm2 in thefellow eye despite the pre-operative cornealthickness having been 448 mm.77 As mostpatients with progressive keratoconus areless than 35 years old, any deleterious effectof collagen cross-linking on the endothe-lium would have devastating consequencesin the long term. It would also eliminate theoption of anterior lamellar grafting in theevent of continued disease progressionfollowing collagen cross-linking. Anteriorlamellar keratoplasty is usually a suitableoption in cases of keratoconus as only thecorneal stroma is replaced and the hostDesçemets membrane and endothelium(with or without some posterior stroma)are preserved. This eliminates the riskof endothelial rejection and endothelialfailure. Damage to the endothelium wouldnecessitate full thickness transplantation(penetrating keratoplasty).
References Complication Possible mechanism Comments
29, 32, 34, 36, 70 Stromal oedema, Desçemetsmembrane folds
Endothelial cell injury Minor degree of stromal oedema seen in up to 70 percent of treated eyes in first month. More significantoedema in published case reports all resolved.
17, 32, 71 Haze CXL effect with stromal scarring Temporary haze reported in 9.8 per cent of cases withadverse effect on acuity. More significant haze in8.6 per cent that persists at 12 months.
72–76 Sterile infiltrates Phototoxic effect from CXL;altered immune response toantigen
One of the most common adverse effects reported in upto 7.6 per cent of cases. Improves with topical steroidtreatment with variable degree of residual scarring.Differential diagnosis is microbial keratitis.
29, 70, 77 Endothelial irregularity ordamage
Direct CXL effect Corneal thickness should be > 400 mm at time ofirradiation. Recommend regular monitoring of thicknessduring treatment. Resolves if minor.
78–80 Microbial keratitis BCL related; epithelial defect,use of steroid drops; change incorneal response to infection
81, 82 Corneal melting and perforation Acute inflammatory response?45 Recurrent corneal erosion
syndromeSecondary to epithelialdebridement
Single case report
83 HSV keratouveitis Use of steroid drops A history of HSV infection is a contra-indication to CXL76 Progression of keratoconus Up to 7.6 per cent. Refer to text for possible risk factors
BCL: bandage contact lens, CXL: corneal collagen cross-linking, HSV: herpes simplex virus
Table 2. Summary of reported complications of corneal collagen cross-linking
Figure 5. Subepithelial infiltrates as a complication followingcross-linking treatment
Cross-linking and keratoconus Chan and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 161

There have been no reports of anydamage to the crystalline lens. An examina-tion of the lens using Scheimpflug imagingdid not find any evidence of lens opacifica-tion.35 There also appears to be no effect onthe foveal thickness measured on retinalocular coherence tomography.86
There are several publications reportingtreatment failure. A loss of two Snellenlines34,76 has been reported in 2.9 to 3.5 percent and 7.6 per cent of eyes progress by over1.00 D on maximum K measurements afterone year.76 Risk factors for treatment failureincluded a high pre-operative maximum Kvalue (greater than 58.00 D; odds ratio 5.32)and age greater than 35 years (odds ratio13.14).76 It may be related to the treatmentoccurring at a more advanced stage of thedisease or where pre-operative parametershave included risk factors for progression.34
Hafezi87 also reported a treatment failure ina patient with a pre-operative corneal thick-ness of 268 mm following epithelial removaldespite swelling the stroma to 406 mm withhypo-osmolar riboflavin, suggesting thatthere may be a minimum stromal thicknessrequired to stabilise the disease. Raiskup-Wolf and colleagues30 have treated twopatients with repeat collagen cross-linkingfollowing progressive disease.
PATIENT SELECTION
In all the previously mentioned clinicalstudies, corneal collagen cross-linking hasbeen performed in eyes with progressivekeratoconus. While the definition of pro-gression has varied between studies, it needsto be stressed that there is no study com-paring collagen cross-linking at the time ofinitial diagnosis of keratoconus to deter-mine if the collagen cross-linking alters thesubsequent rate of progression. There is cur-rently little evidence to suggest that cross-linking is useful in stable disease. Therefore,we feel that a diagnosis of stable keratoconusis in itself an insufficient indication forcollagen cross-linking given the risk ofcomplications.
Progression can be recorded by varyingmeans. The most reproducible method is bykeratometric measurements, either using atopographer or a manual keratometer. Dueto the inherent variability in imaging with acorneal topographer, more than one scanmay be needed to obtain a representativeimage. Typically, we follow the criteria forprogression used by Wittig-Silva and col-leagues,11 which is an increase in maximum
keratometric value of at least 1.00 D over 12months or less. Other authors have definedprogression as an increase in keratometry of3.00 D in six months,88 or as little as 1.00 Dover 24 months.89
When keratometric measurements arenot available, a record of the change in sub-jective refraction is useful, although mostclinicians would agree that a consistentsubjective refraction in a patient with kera-toconus may be difficult to achieve. Progres-sion is suggested by an increase in manifestcylinder of more than 1.00 D or an increasein spherical equivalent of at least 0.50 D over12 months. A 0.1 mm decrease in back opticzone radius of the best fitting contact lensprovides further evidence.11 On occasion, aclear history of subjective worsening ofvision may be the only evidence of progres-sion available at the time of presentation.In such cases, there should always be scopefor clinical judgement as delaying collagencross-linking in eyes with clearly progressivedisease may be detrimental, particularly inyounger patients.
Generally accepted contraindications totreatment include a history of herpetic eyedisease, pregnant or breastfeeding womenand central corneal opacities. It is alsoimportant not to proceed with the irradia-tion phase of treatment if the stromal thick-ness is less than 400 mm in order to reducethe risk of endothelial cell damage.
OTHER APPLICATIONS
While collagen cross-linking was developedto halt the progression of keratoconus,it is being used for an increasing rangeof indications, including microbial kerati-tis,90 pellucid marginal degeneration,33
bullous keratopathy and non-healing cor-neal ulcers.91
Corneal collagen cross-linking has alsobeen used in cases of post-LASIK ectasia,with variable results. Hafezi and colleagues77
found that half their cases with iatro-genic keratectasia improved by 2.00 Dor more following collagen cross-linking80
and Hersh, Greenstein and Fry46 reporteda reduced effect compared with collagencross-linking in cases of keratoconus. It waspostulated that the reduced effect could bedue to the influence of the flap, which mayimpede the diffusion of riboflavin or changethe behaviour of the anterior stroma to thecross-linking process. Cross-linking has alsobeen used in an attempt to stop the progres-sion of recurrent ectasia in three patients
with keratoconus following penetratingkeratoplasty.92
CONCLUSION
We are now able to offer patients a treatmentwith the potential to alter the natural historyof keratoconus and possibly even haltdisease progression. Therefore, it is incum-bent on eye-care professionals to identifypatients with early keratoconus and docu-ment progression, so that these patients aregiven the opportunity to benefit from cross-linking treatment. Further research directedat decreasing both the duration of the satu-ration and irradiation phases could bringmajor benefits in reducing the cost andimproving the access to corneal collagencross-linking throughout the world. In theyears to come, we will know if collagen cross-linking has lived up to its expectations inreducing the need for rigid contact lens wearor surgical intervention for individuals withkeratoconus.
REFERENCES1. Williams KA, Lowe MT, Jones VJ, Loh RS, Coster
DJ. The Australian Corneal Graft Registry 2012Report. Adelaide, Australia, 2012.
2. Andreassen TT, Simonsen AH, Oxlund H. Biome-chanical properties of keratoconus and normalcorneas. Exp Eye Res 1980; 31: 435–441.
3. Spoerl E, Seiler T. Techniques for stiffening thecornea. J Refract Surg 1999; 15: 711–713.
4. Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res 1998; 66: 97–103.
5. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for thetreatment of keratoconus. Am J Ophthalmol 2003;135: 620–627.
6. Sung HW, Chang WH, Ma CY, Lee MH. Crosslink-ing of biological tissues using genipin and/or car-bodiimide. J Biomed Mater Res A 2003; 64: 427–438.
7. McCall AS, Kraft S, Edelhauser HF, Kidder GW,Lundquist RR, Bradshaw HE, Dedeic Z et al.Mechanisms of corneal tissue cross-linking inresponse to treatment with topical riboflavin andlong-wavelength ultraviolet radiation (UVA). InvestOphthalmol Vis Sci 2010; 51: 129–138.
8. Wollensak G, Spoerl E, Reber F, Seiler T. Kerato-cyte cytotoxicity of riboflavin/UVA-treatment invitro. Eye (Lond) 2004; 18: 718–722.
9. Mazzotta C, Balestrazzi A, Traversi C, Baiocchi S,Caporossi T, Tommasi C, Caporossi A. Treatmentof progressive keratoconus by riboflavin-UVA-induced cross-linking of corneal collagen:ultrastructural analysis by Heidelberg RetinalTomograph II in vivo confocal microscopy inhumans. Cornea 2007; 26: 390–397.
10. Kymionis GD, Diakonis VF, Kalyvianaki M, Portal-iou D, Siganos C, Kozobolis VP, Pallikaris AI. One-year follow-up of corneal confocal microscopy aftercorneal cross-linking in patients with post-laser insitu keratosmileusis ectasia and keratoconus. AmJ Ophthalmol 2009; 147: 774–778.
Cross-linking and keratoconus Chan and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
162 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

11. Wittig-Silva C, Whiting M, Lamoureux E, LindsayRG, Sullivan LJ, Snibson GR. A randomizedcontrolled trial of corneal collagen cross-linkingin progressive keratoconus: preliminary results.J Refract Surg 2008; 24: S720–S725.
12. Knappe S, Stachs O, Zhivov A, Hovakimyan M,Guthoff R. Results of confocal microscopy exami-nations after collagen cross-linking with riboflavinand UVA light in patients with progressive kerato-conus. Ophthalmologica 2011; 225: 95–104.
13. Croxatto JO, Tytiun AE, Argento CJ. Sequential invivo confocal microscopy study of corneal woundhealing after cross-linking in patients with kerato-conus. J Refract Surg 2010; 26: 638–645.
14. Mazzotta C, Traversi C, Baiocchi S, Caporossi O,Bovone C, Sparano MC, Balestrazzi A et al. Cornealhealing after riboflavin ultraviolet-A collagen cross-linking determined by confocal laser scanningmicroscopy in vivo: early and late modifications. AmJ Ophthalmol 2008; 146: 527–533.
15. Mazzotta C, Caporossi T, Denaro R, Bovone C,Sparano C, Paradiso A, Baiocchi S et al. Morpho-logical and functional correlations in riboflavin UVA corneal collagen cross-linking for keratoconus.Acta Ophthalmol 2012; 90: 259–265.
16. Messmer EM, Meyer P, Herwig MC, Loeffler KU,Schirra F, Seitz B, Thiel M et al. Morphological andImmunohistochemical Changes After CornealCross-Linking. Cornea 2012. May 10 (Epub ahead ofprint)
17. Mazzotta C, Balestrazzi A, Baiocchi S, Traversi C,Caporossi A. Stromal haze after combinedriboflavin-UVA corneal collagen cross-linkingin keratoconus: in vivo confocal microscopicevaluation. Clin Experiment Ophthalmol 2007; 35:580–582.
18. Wollensak G, Wilsch M, Spoerl E, Seiler T. Colla-gen fiber diameter in the rabbit cornea after colla-gen crosslinking by riboflavin/UVA. Cornea 2004;23: 503–507.
19. Wollensak G, Redl B. Gel electrophoretic analysisof corneal collagen after photodynamic cross-linking treatment. Cornea 2008; 27: 353–356.
20. Mencucci R, Marini M, Paladini I, Sarchielli E,Sgambati E, Menchini U, Vannelli GB. Effects ofriboflavin/UVA corneal cross-linking on kerato-cytes and collagen fibres in human cornea. ClinExperiment Ophthalmol 2010; 38: 49–56.
21. Wollensak G, Spoerl E, Seiler T. Stress-strainmeasurements of human and porcine corneasafter riboflavin-ultraviolet-A-induced cross-linking.J Cataract Refract Surg 2003; 29: 1780–1785.
22. Spoerl E, Wollensak G, Seiler T. Increased resist-ance of crosslinked cornea against enzymatic diges-tion. Curr Eye Res 2004; 29: 35–40.
23. Kohlhaas M, Spoerl E, Schilde T, Unger G, WittigC, Pillunat LE. Biomechanical evidence of the dis-tribution of cross-links in corneas treated with ribo-flavin and ultraviolet A light. J Cataract Refract Surg2006; 32: 279–283.
24. Spoerl E, Wollensak G, Dittert DD, Seiler T. Ther-momechanical behavior of collagen-cross-linkedporcine cornea. Ophthalmologica 2004; 218: 136–140.
25. Wollensak G, Aurich H, Pham DT, Wirbelauer C.Hydration behavior of porcine cornea crosslinkedwith riboflavin and ultraviolet A. J Cataract RefractSurg 2007; 33: 516–521.
26. Caporossi A, Baiocchi S, Mazzotta C, Traversi C,Caporossi T. Parasurgical therapy for keratoconusby riboflavin-ultraviolet type A rays induced cross-linking of corneal collagen: preliminary refractive
results in an Italian study. J Cataract Refract Surg2006; 32: 837–845.
27. Spoerl E, Mrochen M, Sliney D, Trokel S, Seiler T.Safety of UVA-riboflavin cross-linking of thecornea. Cornea 2007; 26: 385–389.
28. Seiler T, Hafezi F. Corneal cross-linking-inducedstromal demarcation line. Cornea 2006; 25: 1057–1059.
29. Doors M, Tahzib NG, Eggink FA, Berendschot TT,Webers CA, Nuijts RM. Use of anterior segmentoptical coherence tomography to study cornealchanges after collagen cross-linking. Am J Ophthal-mol 2009; 148: 844–851.
30. Raiskup-Wolf F, Hoyer A, Spoerl E, PillunatLE. Collagen crosslinking with riboflavin andultraviolet-A light in keratoconus: long-termresults. J Cataract Refract Surg 2008; 34: 796–801.
31. Coskunseven E, Jankov MR 2nd, Hafezi F. Contral-ateral eye study of corneal collagen cross-linkingwith riboflavin and UVA irradiation in patients withkeratoconus. J Refract Surg 2009; 25: 371–376.
32. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T.Long-term results of riboflavin ultraviolet a cornealcollagen cross-linking for keratoconus in Italy: theSiena eye cross study. Am J Ophthalmol 2010; 149:585–593.
33. Koller T, Pajic B, Vinciguerra P, Seiler T. Flatteningof the cornea after collagen crosslinking forkeratoconus. J Cataract Refract Surg 2011; 37: 1488–1492.
34. Asri D, Touboul D, Fournie P, Malet F, Garra C,Gallois A, Malecaze F et al. Corneal collagencrosslinking in progressive keratoconus: multi-center results from the French National ReferenceCenter for Keratoconus. J Cataract Refract Surg 2011;37: 2137–2143.
35. Vinciguerra P, Camesasca FI, Romano MR.Corneal crosslinking and lens opacity. Ophthalmol-ogy 2011; 118: 2519.
36. Henriquez MA, Izquierdo L Jr, Bernilla C, Zakrze-wski PA, Mannis M. Riboflavin/Ultraviolet Acorneal collagen cross-linking for the treatment ofkeratoconus: visual outcomes and Scheimpfluganalysis. Cornea 2011; 30: 281–286.
37. Goldich Y, Marcovich AL, Barkana Y, Mandel Y,Hirsh A, Morad Y, Avni I et al. Clinical and cornealbiomechanical changes after collagen cross-linkingwith riboflavin and UV irradiation in patients withprogressive keratoconus: results after 2 years offollow-up. Cornea 2012; 31: 609–614.
38. O’Brart DP, Chan E, Samaras K, Patel P, Shah SP.A randomised, prospective study to investigatethe efficacy of riboflavin/ultraviolet A (370 nm)corneal collagen cross-linkage to halt the progres-sion of keratoconus. Br J Ophthalmol 2011; 95: 1519–1524.
39. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T,Denaro R. Age-related long-term functional resultsafter riboflavin UV A corneal cross-linking. J Oph-thalmol 2011; 2011: 608041.
40. Vinciguerra P, Albe E, Trazza S, Seiler T, Epstein D.Intraoperative and postoperative effects of cornealcollagen cross-linking on progressive keratoconus.Arch Ophthalmol 2009; 127: 1258–1265.
41. Maeda N, Fujikado T, Kuroda T, Mihashi T,Hirohara Y, Nishida K, Watanabe H et al. Wave-front aberrations measured with Hartmann-Shacksensor in patients with keratoconus. Ophthalmology2002; 109: 1996–2003.
42. Alio JL, Shabayek MH. Corneal higher order aber-rations: a method to grade keratoconus. J RefractSurg 2006; 22: 539–545.
43. Kymionis GD, Grentzelos MA, Kounis GA, Portal-iou DM, Detorakis ET, Magarakis M, KarampatakisVE et al. Intraocular pressure measurements aftercorneal collagen crosslinking with riboflavin andultraviolet A in eyes with keratoconus. J CataractRefract Surg 2010; 36: 1724–1727.
44. Coskunseven E, Jankov MR 2nd, Hafezi F, Atun S,Arslan E, Kymionis GD. Effect of treatmentsequence in combined intrastromal corneal ringsand corneal collagen crosslinking for keratoconus.J Cataract Refract Surg 2009; 35: 2084–2091.
45. Romppainen T, Bachmann LM, Kaufmann C,Kniestedt C, Mrochen M, Thiel MA. Effect ofriboflavin-UVA-induced collagen cross-linking onintraocular pressure measurement. Invest Ophthal-mol Vis Sci 2007; 48: 5494–5498.
46. Hersh PS, Greenstein SA, Fry KL. Corneal collagencrosslinking for keratoconus and corneal ectasia:One-year results. J Cataract Refract Surg 2011; 37:149–160.
47. Tuft SJ, Moodaley LC, Gregory WM, Davison CR,Buckley RJ. Prognostic factors for the progressionof keratoconus. Ophthalmology 1994; 101: 439–447.
48. Leoni-Mesplie S, Mortemousque B, Touboul D,Malet F, Praud D, Mesplie N, Colin J. Scalability andseverity of keratoconus in children. Am J Ophthalmol2012; 154: 56–62 e51.
49. Lowe MT, Keane MC, Coster DJ, Williams KA. Theoutcome of corneal transplantation in infants,children and adolescents. Ophthalmology 2011; 118:492–497.
50. Kelly TL, Williams KA, Coster DJ. Corneal trans-plantation for keratoconus: a registry study. ArchOphthalmol 2011; 129: 691–697.
51. Kelly TL, Coster DJ, Williams KA. Repeatpenetrating corneal transplantation in patientswith keratoconus. Ophthalmology 2011; 118: 1538–1542.
52. Vinciguerra P, Albe E, Frueh BE, Trazza S, EpsteinD. Two-year corneal cross-linking results in patientsyounger than 18 years with documented progres-sive keratoconus. Am J Ophthalmol 2012.
53. Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagencrosslinking with ultraviolet-A and hypo-osmolarriboflavin solution in thin corneas. J Cataract RefractSurg 2009; 35: 621–624.
54. Raiskup F, Spoerl E. Corneal cross-linking withhypo-osmolar riboflavin solution in thin kerato-conic corneas. Am J Ophthalmol 2011; 152: 28–32.
55. Kymionis GD, Portaliou DM, Diakonis VF, KounisGA, Panagopoulou SI, Grentzelos MA. Corneal col-lagen cross-linking with riboflavin and ultraviolet-Airradiation in patients with thin corneas. Am J Oph-thalmol 2012; 153: 24–28.
56. Kaya V, Utine CA, Yilmaz OF. Efficacy ofcorneal collagen cross-linking using a custom epi-thelial debridement technique in thin corneas: aconfocal microscopy study. J Refract Surg 2011; 27:444–450.
57. Hayes S, O’Brart DP, Lamdin LS, Doutch J,Samaras K, Marshall J, Meek KM. Effect of com-plete epithelial debridement before riboflavin-ultraviolet-A corneal collagen crosslinking therapy.J Cataract Refract Surg 2008; 34: 657–661.
58. Samaras K, O’Brart DP, Doutch J, Hayes S, MarshallJ, Meek KM. Effect of epithelial retention andremoval on riboflavin absorption in porcinecorneas. J Refract Surg 2009; 25: 771–775.
59. Wollensak G, Iomdina E. Biomechanical and histo-logical changes after corneal crosslinking with andwithout epithelial debridement. J Cataract RefractSurg 2009; 35: 540–546.
Cross-linking and keratoconus Chan and Snibson
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 163

60. Chan CC, Sharma M, Wachler BS. Effect of inferior-segment Intacs with and without C3-R on kerato-conus. J Cataract Refract Surg 2007; 33: 75–80.
61. Leccisotti A, Islam T. Transepithelial corneal colla-gen cross-linking in keratoconus. J Refract Surg2010; 26: 942–948.
62. Baiocchi S, Mazzotta C, Caporossi A. Reply:Safety and efficacy of transepithelial crosslinking(C3-R/CXL). J Cataract Refract Surg 2010; 36: 188–189.
63. Filippello M, Stagni E, O’Brart D. Transepithelialcorneal collagen crosslinking: bilateral study.J Cataract Refract Surg 2012; 38: 283–291.
64. Kymionis GD, Portaliou DM, Kounis GA, Limnop-oulou AN, Kontadakis GA, Grentzelos MA.Simultaneous topography-guided photorefractivekeratectomy followed by corneal collagen cross-linking for keratoconus. Am J Ophthalmol 2011; 152:748–755.
65. Kanellopoulos AJ. Comparison of sequential vssame-day simultaneous collagen cross-linking andtopography-guided PRK for treatment of kerato-conus. J Refract Surg 2009; 25: S812–S818.
66. Rocha KM, Ramos-Esteban JC, Qian Y, Herekar S,Krueger RR. Comparative study of riboflavin-UVAcross-linking and ‘flash-linking’ using surface waveelastometry. J Refract Surg 2008; 24: S748–S751.
67. Iseli HP, Popp M, Seiler T, Spoerl E, Mrochen M.Laboratory measurement of the absorption coeffi-cient of riboflavin for ultraviolet light (365 nm).J Refract Surg 2011; 27: 195–201.
68. Waring GO IV. Iontophoretic delivery of riboflavinand future applications with corneal CXL withUV-A for keratoconus treatment. Paper presentedat The American Society of Refractive Surgery Sym-posium And Congress, 24th April, 2012, Chicago
69. Vinciguerra R, Spoerl E, Romano MR, Rosetta P,Vinciguerra P. Comparative stress strain measure-ments of human corneas after transepithelial UV-Ainduced cross-linking: impregnation with ionto-phoresis, different riboflavin solutions and irradi-ance power. Paper presented a The Association forResearch in Vision and Ophthalmology AnnualMeeting, 7th May, 2012; Fort Lauderdale, Florida.
70. Gokhale NS. Corneal endothelial damage after col-lagen cross-linking treatment. Cornea 2011; 30:1495–1498.
71. Raiskup F, Hoyer A, Spoerl E. Permanent cornealhaze after riboflavin-UVA-induced cross-linking inkeratoconus. J Refract Surg 2009; 25: S824–828.
72. Angunawela RI, Arnalich-Montiel F, Allan BD.Peripheral sterile corneal infiltrates and meltingafter collagen crosslinking for keratoconus. J Cata-ract Refract Surg 2009; 35: 606–607.
73. Rodriguez-Ausin P, Gutierrez-Ortega R, Arance-GilA, Romero-Jimenez M, Fuentes-Paez G. Keratopa-thy after cross-linking for keratoconus. Cornea2011; 30: 1051–1053.
74. Koppen C, Vryghem JC, Gobin L, Tassignon MJ.Keratitis and corneal scarring after UVA/riboflavincross-linking for keratoconus. J Refract Surg 2009;25: S819–S823.
75. Mangioris GF, Papadopoulou DN, Balidis MO,Poulas JL, Papadopoulos NT, Seiler T. Cornealinfiltrates after corneal collagen cross-linking.J Refract Surg 2010; 26: 609–611.
76. Koller T, Mrochen M, Seiler T. Complication andfailure rates after corneal crosslinking. J CataractRefract Surg 2009; 35: 1358–1362.
77. Hafezi F, Kanellopoulos J, Wiltfang R, Seiler T.Corneal collagen crosslinking with riboflavin andultraviolet A to treat induced keratectasia after
laser in situ keratomileusis. J Cataract Refract Surg2007; 33: 2035–2040.
78. Sharma N, Maharana P, Singh G, Titiyal JS. Pseu-domonas keratitis after collagen crosslinking forkeratoconus: case report and review of literature.J Cataract Refract Surg 2010; 36: 517–520.
79. Rama P, Di Matteo F, Matuska S, Paganoni G,Spinelli A. Acanthamoeba keratitis with perfora-tion after corneal crosslinking and bandagecontact lens use. J Cataract Refract Surg 2009; 35:788–791.
80. Garcia-Delpech S, Diaz-Llopis M, Udaondo P,Salom D. Fusarium keratitis 3 weeks after healedcorneal cross-linking. J Refract Surg 2010; 26: 994–995.
81. Labiris G, Kaloghianni E, Koukoula S, Zissimopou-los A, Kozobolis VP. Corneal melting after collagencross-linking for keratoconus: a case report. J MedCase Rep 2011; 5: 152.
82. Gokhale NS, Vemuganti GK. Diclofenac-inducedacute corneal melt after collagen crosslinking forkeratoconus. Cornea 2010; 29: 117–119.
83. Kymionis GD, Portaliou DM, Bouzoukis DI, SuhLH, Pallikaris AI, Markomanolakis M, Yoo SH. Her-petic keratitis with iritis after corneal crosslinkingwith riboflavin and ultraviolet A for keratoconus.J Cataract Refract Surg 2007; 33: 1982–1984.
84. Ghanem RC, Netto MV, Ghanem VC, SanthiagoMR, Wilson SE. Peripheral sterile corneal ring infil-trate after riboflavin-UVA collagen cross-linking inkeratoconus. Cornea 2012; 31: 702–705.
85. Kymionis G, Portaliou D. Corneal crosslinking withriboflavin and UVA for the treatment of kerato-conus. J Cataract Refract Surg 2007; 33: 1143–1144;author reply 1144.
86. Goldich Y, Marcovich AL, Barkana Y, Avni I, ZadokD. Safety of corneal collagen cross-linking withUV-A and riboflavin in progressive keratoconus.Cornea 2010; 29: 409–411.
87. Hafezi F. Limitation of collagen cross-linking withhypoosmolar riboflavin solution: failure in anextremely thin cornea. Cornea 2011; 30: 917–919.
88. Vinciguerra P, Albe E, Trazza S, Rosetta P, Vin-ciguerra R, Seiler T, Epstein D. Refractive, topo-graphic, tomographic, and aberrometric analysisof keratoconic eyes undergoing corneal cross-linking. Ophthalmology 2009; 116: 369–378.
89. Greenstein SA, Fry KL, Hersh PS. In vivo biome-chanical changes after corneal collagen cross-linking for keratoconus and corneal ectasia: 1-yearanalysis of a randomized, controlled, clinical trial.Cornea 2012; 31: 21–25.
90. Makdoumi K, Mortensen J, Crafoord S. Infectiouskeratitis treated with corneal crosslinking. Cornea2010; 29: 1353–1358.
91. Ehlers N, Hjortdal J, Nielsen K, Sondergaard A.Riboflavin-UVA treatment in the management ofedema and nonhealing ulcers of the cornea.J Refract Surg 2009; 25: S803–S806.
92. Richoz O, Schutz JS, Pajic B, Coskunseven E, HafeziF. Crosslinking for recurrent keratoconus. Ophthal-mology 2012; 119: 878–878.
Cross-linking and keratoconus Chan and Snibson
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
164 Clinical and Experimental Optometry © 2013 Optometrists Association Australia





























