Embed Size (px)
Citation preview

7/7/20
1
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 1
NC Department of Health and Human Services
Substance Exposed Infants-What to Know for Best Infant Outcomes- July 9, 2020
Current Photo Release with Children and Youth Branch
Megan Canady, MSW, MSPH UNC Center for Maternal & Infant Health UNC School of Medicine
Melissa L. Godwin, LCSWClinical Assistant ProfessorSchool of Social WorkUniversity of North Carolina, Chapel Hill
Gerri Mattson, MD, MSPH, FAAPPediatric Medical ConsultantChildren and Youth BranchNCDHHS
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 2
Webinar Logistics
• The sound for this webinar is provided in VoIP--you will use your computer speakers; be sure to turn up the volume.
• You will use the CHAT function box to communicate with the presenters.
• The webinar will be archived and posted on the Child Health Provider resource page.
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 3
Disclosures
• 2.0 NCPD Contact Hours and 2.0 CPH Recertification Credits may be earned upon successful completion.
• For successful completion, participants must attend 100% of educational activity and complete the online course evaluation. There will be no partial credit awarded.
• No conflict of interest exists for anyone in the position to control content for this activity.
1
2
3

7/7/20
2
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 4
• This educational activity is being jointly provided by the Public Health Nursing Institute for Continuing Excellence.
• The Public Health Nursing Institute for Continuing Excellence is approved as a provider of nursing continuing professional development by the North Carolina Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation.
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 5
Agenda9:05-9:40
Melisa Goodwin , LCSW – Infants who are Substance Exposed
9:45-9:53
Break
9:53-10:20
Megan Canady, MSW, MSPH - Addressing Safe Infant Sleep and Tobacco Exposure forHigher Risk Infants
10:20-10:50
Dr. Gerri Mattson, MD, MSPH, FAAP -Supporting the Care of Premature Infants and their Families
10:50 Q & A
NC Department of Health and Human Services
Infants who are Substance Exposed
Melissa L. Godwin, LCSWClinical Assistant ProfessorSchool of Social WorkUniversity of North Carolina, Chapel [email protected]
4
5
6

7/7/20
3
Terms
• Substance Use Disorder
• Addicted‐psychological aspects of substance use
• Dependency‐physiological aspects of drug use
• Recovery‐ Reducing symptoms of the disease of addiction with the goal of disease remission
Also: Consider ‘person first’ language ex. ‘Infant with NAS’ or ‘mother insured with Medicaid’
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Jasmine1. Multiple children, always
seemingly pregnant.
2. Never enough food in the house, unkempt house, utilities often off.
3. Kids always behind on pediatric visits.
4. Multiple calls to CW from neighbors and Headstartconcerning neglect.
5. Never home when home‐visit is scheduled.
6. Doesn’t seem to want help, always very angry and avoidant.
Jasmine1. Multiple children, always
seemingly pregnant.
2. Never enough food in the house, unkempt house, utilities often off.
3. Kids always behind on pediatric visits.
4. Multiple calls to CW from neighbors and Headstartconcerning neglect.
5. Never home when home‐visit is scheduled.
6. Doesn’t seem to want help, always very angry and avoidant.
1. Partner won’t let her use contraception, believes if she does that means she’s cheating.
2. Any income is used on addiction, she is too depressed/pregnant/desperate to clean the house
3. She doesn’t have transportation and everyone she knows is using and unreliable for providing rides
4. She wishes the people who call CW on her offered to help her with rides, food, support
5. She wants to be a good mother and is afraid that if she is home the kids will be taken.
6. She is afraid. Afraid she will lose her children, afraid she will loose any chance to show what a good mother she can be, afraid to go to jail. Afraid they will take away the one thing that sometimes help‐ her drug. She feels deep shame of the situation she is in.
7
8
9

7/7/20
4
• Genetic vulnerability 50‐60%• Adverse Childhood Experiences• Brain disorder• Primary chronic disease
• Relapse risk factors for hypertension, asthma & diabetes: − lack of adherence to diet, medications, or behavior change− low socioeconomic status,− low family supports− psychiatric co‐morbidity
Facts on Substance Use Disorders
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Adverse Childhood Experiences (ACE) Study
• Center for Disease Control & Kaiser Permanente HMO Collaboration
• 17,000 participants
• Collection of data over 10 years
• Self report and healthcare data
https://www.cdc.gov/violenceprevention/acestudy/
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
What are ACEs?1. Emotional abuse
2. Physical abuse
3. Sexual abuse
4. Emotional neglect
5. Physical neglect
6. Witnessing domestic violence
7. Alcohol or other substance abuse in the home
8. Mentally ill or suicidal household members
9. Parental separation or divorce
10. Having a household member imprisoned
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
10
11
12

7/7/20
5
“It’s hard to get enough of something that almost works.” Dr. Vincent Felitti
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Characteristics and Signs of Addiction
CHARACTERISTICS OF ADDICTION 11 SIGNS OF SUBSTANCE USE DISORDERS1. Inability to consistently abstain 1. Taking the substance in larger amounts or for longer
than intended
2. Impairment in behavioral control 2. Wanting to cut down or stop, but unable to do so
3. Craving 3. Cravings or urges to use the substance
4. Diminished recognition of significant problems with one’s behaviors and interpersonal relationships
4. Spending a lot of time obtaining, using, or recovering from using the substance
5. Dysfunctional emotional responses 5. Regularly unable to do what should be done at work, home, or school due to substance use
6. Continuing to use, even when it causes relationship problems
7. Giving up important social, work, or recreational activities due to substance use
8. Using substances again and again, even in dangerous situations
9. Recurrent use of the substance, even when knowing it could worsen a physical or psychological problem
10. Needing more of the substance to get the desired effect (tolerance)
11. Development of withdrawal symptoms, which can be relieved by taking more of the substance
Source: American Society of Addiction Medicine (ASAM). Definition of Addiction. Adoption Date: April 12, 2011. https://www.asam.org/resources/definition‐of‐addiction; American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Fifth Edition. 2013
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
ASAM Levels of Care
Source: http://maryland.beaconhealthoptions.com/provider/manual/Appendix-C-ASAM-Criteria.pdf
Level of Care
Adult Title Description
0.5 Early Intervention Assessment and education
OTP (Level 1)
Opioid Treatment ProgramDaily or several times weekly opioid and medication and counseling available
1 Outpatient Services Less than 9 hours of service per week
2.1 Intensive Outpatient Services More than 9 hours of service per week
2.5 Partial Hospitalization Services 20 or more hours of service per week
3.1Clinically Managed Low-intensity Residential Services
20-hour structure with available personnel; at least 5 hours clinical service per week
3.3Clinically Managed Population-specific High-Intensity Residential Services
24-hour care with trained counselors; less intense environment for those with cognitive and other impairments
3.5Clinically Managed High-intensity Residential Services
24-hour care with trained counselors
3.7Medically Monitored Intensive Inpatient Services
24-hour nursing care with physician available; 16-hour per day counselor available
4Medically Managed Intensive Inpatient Services
24-hour nursing care and daily physician care; counseling available
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
13
14
15

7/7/20
6
• Reduction or elimination of substance dependence
• Improvement in personal and social functioning
• Improvement in mental and physical health
• Reduction in risky behavior that could affect health, and ability to work.
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020 16
Recovery from a substance use disorder is characterized by:
Opioid Use Disorder TreatmentMAT: Medication‐Assisted Treatment
• Reduces illicit opioid use
• Protects against opioid‐related overdoses
• Prevents injection behaviors
• Reduces criminal behavior
Types: Methadone, Buprenorphine, Naltrexone
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Why Use Opioids as a Treatment Medication?With opioid medications we are not replacing one addiction for another. Opioid medications are long‐acting medication that help with:
• CRAVING
– An individual’s cravings are controlled
• COMPULSION
– Individual is no longer compulsively using opioids
• CONTROL
– Medication‐assisted treatment gives back control to the individual
• CONSEQUENCES
– Medication assisted treatment helps the individual focus on rebuilding her life
An individual receiving opioid pharmacotherapy must be monitored by a medical team that evaluates adequacy of medication dosage and general health and well‐being of the individual.
Slide Source: Dr.Hendree Jones
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
16
17
18

7/7/20
7
Pregnancy and Opioid Use Disorders & Treatment
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Shared Goals
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Slide source: Hendree Jones
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020 21
Context of Substance Use during Pregnancy
0%
10%
20%
30%
40%
50%
60%
non-Pregnant Pregnant
Se
lf-r
ep
ort
ed
Pa
st
Mo
nth
Us
e (
%)
Tobacco Products
Alcohol
Any Illicit Drug
Marijuana
Cocaine
Heroin
Pain Relievers
National Survey on Drug Use and Health, 2015
Past Month Use • The two most common drugs used by non-pregnant women have been alcohol and tobacco
• This same statement is true for pregnant women
• Among pregnant women, approximately .2% used heroin, and 1.1% used pain relievers non-medically in the past month
SAMHSA Office of Applied Statistics
19
20
21

7/7/20
8
• Best outcomes for birth (meaning full term and birth weight) and parenting (preventing maltreatment) with a substance exposed pregnancy, is connection to substance use disorder treatment as soon as possible.
• Contacting the Perinatal Substance Use Specialist at 1800‐688‐4232 is an important first step.
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Key Information
Active Opioid Use Disorder During Pregnancy
• Active opioid use disorder (OUD) during pregnancy can include a variety of opioids, prescription and otherwise.
• Level and type of opioids can vary greatly from hour to hour and day to day, depending on access.
• The variability can put mother and fetus in frequent withdrawal and distress.
• Common risks associated with an active (OUD) include exposure to HIV, Hepatitis C and other infections transmitted through needle use or trading sex for drugs. Ongoing trauma, and overdose are also risks. Behaviors that can result in legal consequences are also common.
• Without treatment, women with opioid use disorders who become pregnant face increased risks of preterm delivery and low birth weight.
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
• For opioid use disorders, medication assisted treatment (MAT) with methadone or buprenorphine as a part of comprehensive treatment has the best outcomes for long term recovery.
• Abstinence based recovery with opioid use disorders (OUD) results in high relapse rates. It is possible to achieve recovery from an OUD with abstinence, however it requires a high level of supports which many people don’t have.
Key Information
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
22
23
24

7/7/20
9
Pregnancy and Medication Assisted Treatment
• Women who are pregnant experience the same benefits as non‐pregnant population with Opioid Use Disorders
– Stability– Focus on building life in recovery– Less vulnerable to violence, infections and legal consequences
• Women on MAT are more likely to engage in prenatal care and SUD treatment
• Developing baby doesn’t go through frequent periods of withdrawal, reducing prenatal complications
• Infant more likely to be born full term and average weight for gestational age.
SAMHSA, 2009
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
• An increase in methadone dose over the course of pregnancy is typically needed to maintain a therapeutic dose due to increase in blood volume of pregnant woman.
• A therapeutic dose is one that addresses the physical aspects of opioid withdrawal and the psychological aspects of craving.
• Dose increase does not increase likelihood of withdrawal symptoms in infants.
Key Information
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Why Not Taper Medication During Pregnancy?
• Tapering or withdrawing women from medication is an acute‐care approach to a long‐term chronic medical condition
• While research shows that medication tapering during pregnancy does not frequently result in spontaneous abortions or miscarriages, tapering does not avoid NAS
• The high relapse rate to opioid use also poses a risk for adverse maternal, fetal and child outcomes
• If tapering is considered by the medical provider and patient as the most optimal treatment, high levels of support, relapse prevention and child safety planning are needed
Slide Source: Dr. Hendree JonesNCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
25
26
27

7/7/20
10
• Breastfeeding is recommended with MAT, if there are no contraindications, and can be particularly helpful to a newborn with withdrawal symptoms.
• MAT dose adjustment is typically needed postpartum, however is not automatic, and requires good communication with provider.
• Postpartum is complicated, and MAT is only one part of it, support is necessary in this delicate period.
Key Information
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
• Postpartum is not the time to stop MAT as part of treatment and recovery due to:
• Time of increased stress with caretaking role
• Time of decreased sleep
• Increased risks of post partum mood disorders
• Increased risks of relapse
Extra support and stability should be goal
Key Information
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Substance Exposed Pregnancies, Impact
Exposure to Tobacco, Alcohol, Illicit Opioids, Marijuana, Amphetamines or Cocaine may result in:
o Low birth weight for gestational age
o Prematurity
o Increased risk of SIDS
ACOG, AAP 2016
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
28
29
30

7/7/20
11
Risks of Tobacco/Smoking
• Smoking during pregnancy can disrupt fetal development. (The American College of Obstetricians and Gynecologists [ACOG], 2013)
• Cognitive, emotional, and behavioral problems in children are associated with a woman’s smoking during pregnancy. (SAMHSA, 2011d)
• Children of mothers who smoked during pregnancy are more likely to have asthma, colic, and childhood obesity. (ACOG, 2013)
• The effectiveness of nicotine replacement therapy (NRT) in pregnant women is inconclusive. (ACOG, 2013)
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Fetal Alcohol Spectrum Disorders
• Prenatal exposure to alcohol is one of the leading causes of developmental disabilities and birth defects in children.
• Up to 1 in 20 U.S. school children may have a FASD. (CDC, 2016a)
• Data estimates are that 2–5% of children in the United States have a FASD. (CDC, 201ba; May et al., 2014)
• It is estimated that almost 70% of the children in foster care are affected by prenatal alcohol exposure in varying degrees (NOFAS, 2016). Among those, 1–1.5% have FAS. (Williams et al., 2015)
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Long‐term Effects of FASD
• Of all commonly used substances, alcohol produces the most serious lasting neurobehavioral effects in the fetus.
• Children exposed to alcohol in the womb can have a range of serious life‐long issues, including delayed developmental outcomes.
• Lifetime costs for one individual with FASD are estimated to be up to $244 million. (CDC, 2015b; Williams & Smith, 2015)
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
31
32
33

7/7/20
12
Opioid Exposed Pregnancy
Neonatal Abstinence Syndrome (NAS) or Neonatal Opioid Withdrawal Syndrome (NOWS)
o Confounding factors‐ tobacco, anti‐depressants, and other substances
o Medication Assisted Treatment
o Anticipated and treatable
(ACOG 2015, AAP 2012;Kocherlakota 2015)
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Opioid Exposed Pregnancy
Language matters
• Infants born who have been consistently exposed to opioids in utero, have a developed a physical dependence and may experience withdrawal, including symptoms of NAS.
• Physical dependence is not addiction. NAS is not an indicator of addiction in an infant.
• Addiction is characterized by “ …an inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one’s behaviors and interpersonal relationships, and a dysfunctional emotional response.”
American Society of Addiction Medicine
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Neonatal Abstinence Syndrome
• Withdrawal symptoms due to exposure during pregnancy
• 60‐90% of infants exposed to methadone in utero may experience withdrawal symptoms
• Infants with opioid should be observed for a minimum of 5‐7 days
o This may not be the practice at all hospitals
• Not associated with maternal dose
• Finnegan Scoring Tool
• Eat, Sleep, Console Method
Committee Opinion No.711. American College of Obstetricians and Gynecologists. American Journal Obstetrics and Gynecology 2017
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
34
35
36

7/7/20
13
NAS Intervention and Treatment
Non‐pharmacologic management:
• Includes environmental controls emphasizing quiet zones, low lighting, swaddling, gentle handling and feeding on demand. Breastfeeding and ‘rooming in’ are also beneficial. ‘Eat, Sleep, Console Approach’.
Pharmacologic management:
• Includes the use of a variety of medications to ease the withdrawal symptoms of the infant. Common medications include opioids (dilute tincture of opium, morphine, or methadone) and phenobarbital.
Committee Opinion No.711. American College of Obstetricians and Gynecologists. American Journal Obstetrics and Gynecology 2017
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
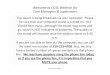
Smoking Impacts NAS
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
H.E. Jones et al. / Drug and Alcohol Dependence 131 (2013) 271–277
1.82.5
3.9
6.1
0
1
2
3
4
5
6
7
Non-Smoking
Below-AverageSmoking
AverageSmoking
Above-AverageSmoking
Me
an
Am
ou
nt
of
Mo
rph
ine
(m
g)
Total Amount of Morphine Needed to Treat NAS
8[V9.4
11.7
14.6
0
2
4
6
8
10
12
14
16
Non-Smoking Below-AverageSmoking
AverageSmoking
Above-AverageSmoking
Me
an
Nu
mb
er
of
Da
ys
Total Length of Hospital Stay1
Length of Stay Decreases with Eat, Sleep, Console @ UNC
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020 39
Blount, T. et al. Reduction in Length of Stay and Morphine Use forNAS With the “Eat, Sleep, Console” Method.Pediatrics. 2019.
37
38
39

7/7/20
14
MAT Exposure /Early Childhood
• Majority of studies demonstrating harm, confounded by environmental factors and poly substance exposure (alcohol & tobacco)
• MOTHER Study, longitudinal with methadone and buprenorphine across 6 sites‐@ 36 months:
• Well within the range of normal development in physical growth
measures, cognitive development and language development
• No difference between infants treated for NAS and those not
• No difference between infants exposed to methadone vs
buprenorphine
Source: Behnke and Smith 2013; Jones et al 2015; Kaltenbach et al 2018
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Treatment Works: Examples from the FieldNC Perinatal/ Maternal and CASAWORKS Initiatives
• High engagement in prenatal care
• Healthy newborn birth weights for pregnant women who enter treatment prior to delivery
• Lower recidivism with child welfare among families engaging with treatment services
• Fewer number of days in out‐of‐home foster care placement for children of parents involved with child welfare as compared to parents with substance use problems not engaged in the services
• Successful engagement with pediatric care for families involved with services
• Increased affectional bonds and reduced conflict among families engaged in parenting programs, and
• Successful engagement in the work force
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
− Provides screening, information & referral for pregnant and
parenting women with dependent children
− Provides consultation, training & technical assistance for the
public and for professionals regarding perinatal substance use,
treatment and resources
−Weekly Bed Availability List ([email protected])
− Available Monday through Friday from 8 am to 6 pm
− 1‐800‐688‐4232
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Perinatal Substance Use Project
40
41
42

7/7/20
15
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
Perinatal Substance Use Project/Judith Johnson-Hostler1800-688-4232
• Key Messages
• Pregnancy and Opioid Exposure: Guidance for North Carolina
• Service Locator Map
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
North Carolina Fetal Alcohol Prevention Program (FASDinNC)
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
• Training, education, and resources on FASD
• Located within The Arc of North Carolina
• Contact Amy Hendricks at
• 1‐800‐662‐8706
43
44
45

7/7/20
16
Lending Hope
• Believe substance use disorder recovery is possible.
• Learn from someone in long term recovery, view first person recovery videos, attend open 12 step meetings. https://facesandvoicesofrecovery.org/resources/recovery‐stories.html
• Share the belief that recovery is possible with individuals, families and colleagues.
NCDHHS DIVISION OF MHDDSAS | INFANTS WHO ARE SUBSTANCE EXPOSED |JULY 2020
www.MomBaby.org
Addressing Safe Infant Sleep and Tobacco Exposure for
Higher Risk Infants
July 9, 2020
Megan Canady, MSW, MSPH UNC Center for Maternal & Infant Health
www.MomBaby.org
Safe Infant Sleep
46
47
48

7/7/20
17
www.MomBaby.org
After a full investigation, SUIDs that occur during an unobserved sleep period may be diagnosed as one of the three manners:
• Sudden Infant Death Syndrome (SIDS)- is the sudden death of an infant younger than 1 year of age that cannot be explained even after a full investigation that includes a complete autopsy, examination of the death scene, and review of the clinical history.
• Accidental suffocation and strangulation in bed (ASSB) -when it has been determined that a baby died in their sleep by suffocation, overlay, wedging or entrapment, or strangulation.
• Undetermined/Unknown- not certain on why the baby died—other manners or causes of death cannot be ruled out, so definite cause can not be determined.
Sudden Unexpected Infant Death (SUID) is the death of an infant younger than 1 year of age that occurs suddenly and unexpectedly.
www.MomBaby.org
Unsafe Sleep Environment Related to Infant Deaths, 2017
Source: Office of the Chief Medical Examiner-Division of Public Health North Carolina Department of Health and Human Services
www.MomBaby.org
Link to full report: http://pediatrics.aappublications.org/content/early/2016/10/20/peds.2016-2938
American Academy of Pediatrics (AAP)
Recommendations for a Safe Infant Sleeping
Environment
49
50
51

7/7/20
18
www.MomBaby.org
SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping EnvironmentTASK FORCE ON SUDDEN INFANT DEATH SYNDROME Pediatrics Nov 2016, 138 (5) e20162938; DOI: 10.1542/peds.2016-2938
www.MomBaby.org
SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping EnvironmentTASK FORCE ON SUDDEN INFANT DEATH SYNDROME Pediatrics Nov 2016, 138 (5) e20162938; DOI: 10.1542/peds.2016-2938
www.MomBaby.org
SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping EnvironmentTASK FORCE ON SUDDEN INFANT DEATH SYNDROME Pediatrics Nov 2016, 138 (5) e20162938; DOI: 10.1542/peds.2016-2938
52
53
54

7/7/20
19
www.MomBaby.org
Shifting from:Telling parents what to do
Safer Sleep Conversations
To:Working with parents as a resource & partner in problem-solving
www.MomBaby.org
• What have you heard about ways to keep your baby safe while they sleep?
• Can you tell me about where your baby will sleep?(or Where does your baby sleep?)
• Can you tell me more about why your baby sleeps with you?
Conversation Starters
www.MomBaby.org
Bed SharingBed sharing is when an infant sleeps on the same surface (bed, couch, chair, etc.) as another person (parent, sibling, caregiver, etc.)
• On the rise, despite known risks
• There is no 100% safe way to bed share
• Associated with the majority of sleep-related infant deaths in NC
• Certain factors put infants at higher risk of death if bed sharing
55
56
57

7/7/20
20
www.MomBaby.org
Helping Parents Understand the Risks of Bed SharingThese factors put your baby at higher risk of sleep-related deaths.
It is strongly recommended that you stop sleeping with your baby, especially if…
www.MomBaby.org
www.MomBaby.org
Safe Infant Sleep Resources
• Posters and patient education materials available
for free through Women’s Health Branch
http://whb.ncpublichealth.com/provpart/pubmanbro.htm
• Social media toolkit to promote safe sleep
• SafeSleepNC.org for tailored information for
healthcare professionals & parents/caregivers
(English and Spanish)
Visit SafeSleepNC.org for more information
58
59
60

7/7/20
21
www.MomBaby.org
Tobacco Exposure and Infant Health
www.MomBaby.org
Tobacco Use During Pregnancy in NC
1 in 12 babies in NC are born to women
reporting tobacco use during pregnancy
In some counties almost 30% of babies
are born to women who smoked
www.MomBaby.org
Tobacco Use Causes Poor Birth & Infant Outcomes
Maternal/Fetal Harm From Tobacco
o Infertilityo Miscarriageo Ectopic Pregnancyo Premature Birtho Low Birth Weighto Stillbirtho SIDS
Infant/Child Harm From Tobacco
o SIDSo Ear infectionso Respiratory Infectionso Asthmao Links with childhood
obesity, cancer, & attention disorders, and cardiovascular disease & diabetes in adulthood
61
62
63

7/7/20
22
www.MomBaby.org
Secondhand Tobacco Exposure• Secondhand tobacco is the smoke/vape a
tobacco user breathes out.
• Secondhand smoke contains about 4,000 chemicals and more than 50 are known to cause cancer.
• Anytime children breathe in secondhand tobacco they are exposed to these chemicals.
• Secondhand aerosol from e-cigarettes is not “harmless water vapor” and exposure should be avoided, especially by pregnant women, infants, children, and adolescents.
www.MomBaby.org
Thirdhand Tobacco Exposure• Thirdhand tobacco is the left-over pollution after a
cigarette or e-cigarette.
• Can be found in the walls, upholsteryon the seats of a car, or even a child's hair.
• There is no safe level of exposure to thirdhand tobacco.
• Thirdhand smoke contains more than 250 chemicals.
• Smoking/vaping in different rooms using fans, or smoking in front of an open window does not prevent thirdhand tobacco exposure.
https://www.healthychildren.org/English/health-issues/conditions/tobacco/Pages/How-Parents-Can-Prevent-Exposure-Thirdhand-Smoke.aspx
www.MomBaby.org
Information to Share with Families
• Do not smoke or vape or allow people to smoke or vape in your house or car. Ask people who do smoke or vape to step outside.
• Ask caregivers and relatives to stop smoking or vaping around you and your children.
• Choose a babysitter/childcare center that is smoke/vape free.
• If you smoke or vape, consider quitting.
64
65
66

7/7/20
23
www.MomBaby.org
Quitline NC
Perinatal-Specific Services
• Protocol for women who are pregnant, plan to get pregnant, and those that are postpartum
• Up to 10 calls
Behavioral Health-Specific Services
• 2 additional calls
• 12 weeks of combination NRT
• Enhanced Assessment
www.MomBaby.org
NC Perinatal Tobacco Cessation Resources-You Quit Two Quit
• Free on-site or virtual training on evidence-based
tobacco use screening and cessation counseling for
practices
• Patient education materials available to order for FREE
through Women’s Health Branch
http://whb.ncpublichealth.com/provpart/pubmanbro.htm
Visit YouQuitTwoQuit.org for more information
www.MomBaby.org
• Sleep-related deaths are a leading cause of infant mortality in our state
• It is critical to work with families to make sleep safer, especially for higher risk infants
• Eliminating tobacco exposure reduces poor birth & infant outcomes
• Visit SafeSleepNC.org and YouQuitTwoQuit.org for more information
Summary
67
68
69

7/7/20
24
www.MomBaby.org
Megan Canady, MSW, MSPH [email protected]
MomBaby.orgSafeSleepNC.org
YouQuitTwoQuit.org
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 71
NC Department of Health and Human
Services
Division of Public HealthSupporting the Care of Premature
Infants and Their Families
Gerri Mattson, MD, MSPH, FAAPPediatric Medical ConsultantChildren and Youth Branch
Current Photo Release with Children and Youth Branch
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 72
Premature Birth = Preterm Birth
• 1 in 10 babies was born too early in the US in 2018−Rates have been increasing yearly since 2014
• Preterm birth and low birth weight accounted for about 17% of infant deaths in the US
• Racial and ethnic disparities remain−Rate of preterm birth among non-Hispanic black
women (14%) was 50% higher than non-Hispanic white women (5%)
https://www.cdc.gov/reproductivehealth/features/premature-birth/index.html
70
71
72

7/7/20
25
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 73
Preterm Birth
• The earlier a baby is born, the higher the risk of death or serious disability
• Long term problems may include developmental delay and lower performance in school
• Important to monitor development closely for years as may be while before see delays or problems
• However, late preterm infants are also at high risk for developmental concerns
https://www.cdc.gov/reproductivehealth/features/premature-birth/index.html
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 74
Definitions of Gestational Age Periods from Late Preterm to Post Term
Dan L. Stewart et al. Pediatrics 2019;144:e20192760 https://pediatrics.aappublications.org/content/pediatrics/144/5/e20192760.full.pdf
©2019 by American Academy of Pediatrics
70% of preterm births
and 7% of live births
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 75
Subdivisions of Preterm Birth Based on Birth Gestational Age
• “Late preterm” are born 34 weeks to less than 37 weeks
• “Moderate preterm” is designated as 32 to less than 34 weeks
• “Very preterm” is designated 28 weeks to less than 32 weeks
• “Extremely preterm” is less than 28 weeks gestation
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4438860/pdf/nihms662605.pdf
73
74
75

7/7/20
26
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 76
Human Viability
• Human viability: the gestational age at which there is a 50% chance of survival with or without medical care
• Viability in developed, high income countries, like the US is somewhere between 22-24 weeks
• These are considered “extremely preterm” infants
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4438860/pdf/nihms662605.pdf
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 77
How Preterm Births Occur
• Not completely understood
• Two-thirds of preterm deliveries as a result of preterm labor and/or premature rupture of membranes
• There are several types risk factors that have been associated with preterm births
• Public health and clinical strategies are used to try to prevent and reduce many of these risk factors in order to reduce preterm birth
https://pediatrics.aappublications.org/content/pediatrics/144/5/e20192760.full.pdf
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 78
Risk Factors for Prematurity
• Prior history of delivering a premature baby
• Infection or inflammation
• Maternal stress (acute or chronic)
• Uterine, placental and/or fetal anomalies
• Pregnancy with multiples
https://www.cdc.gov/reproductivehealth/features/premature-birth/index.html and Stewart et al Pediatrics 2019 https://pediatrics.aappublications.org/content/pediatrics/144/5/e20192760.full.pdf
76
77
78

7/7/20
27
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 79
Risk Factors (cont.)
• Short time (less than 18 months) between pregnancies (i.e, unintended)
• Maternal health conditions such as diabetes or hypertension
• Tobacco use and substance abuse
https://www.cdc.gov/reproductivehealth/features/premature-birth/index.html and Stewart et al Pediatrics 2019 https://pediatrics.aappublications.org/content/pediatrics/144/5/e20192760.full.pdf
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 80
Possible Conditions Seen With Premature Infants
www.marchofdimes.org
• Hyperbilirubinemia
• Infections or Sepsis
• Apnea of prematurity
• Necrotizing enterocolitis (NEC)
• Feeding problems
• Bronchopulmonary dysplasia (BPD)
• Chronic lung disease
• Anemia
• Patent ductus arteriosus (PDA)
• Intracranial or intraventricular hemorrhage (IVH)
• Retinopathy of prematurity (ROP)
• Hearing problems
• Developmental delays
• Intellectual or developmental disabilities
• Neonatal abstinence syndrome (with exposure)
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 81
Current Photo Release with Children and Youth Branch
79
80
81

7/7/20
28
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 82
NICU Courses Can Vary: Monitor Since Risk With All Preterm Infants
• Short stays for late preterm infants that are stable and “feed and grow”
• Lengthy with intubation and even ECMO
• Life and death for some with “coding” episodes that parents may see
• Lots of things going on even with attempts to minimize noise and light and try to allow for privacy
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 83
Potential Red Flags in Infants
• Breathing problems (too slow or too fast)
• Color changes (pale overall or blue around lips)
• Overly fussy or irritable
• Increased sweating
• Tremors and jitteriness (even seizures): low body temperature, low blood sugar or chemistries not normal, exposure to substance, infection, etc…
• Increased muscle tone
• Exaggerated startle response
• Difficulty consoling
83
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 84
Additional Potential Red Flags
• Not gaining weight
• Poor feeding
• Poor sleeping or increased wakefulness
• Warm to touch
• Overly quiet or sleepy
• Not voiding at least 4 times a day
• Mottling
• Stools with blood
• Vomiting (more than just spit ups) especially projective or forceful
82
83
84

7/7/20
29
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 85
Possible Concerns with Mothers
• Postpartum depression or anxiety
• Experience of trauma
• Stress from NICU
• Grieving process
• Lack of support from family and work
• Inability or desire to visit frequently
• Poor bonding to infant
• Financial burden on the family
• Substance abuse
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 86
Added Stress of COVID-19 and Birth of Premature Infant
• Limited to who can attend the birth
• Wear full PPE for birth
• Separation if mother suspect or positive for COVID-19
• Concerns for infection of infant while in the hospital
• Not as many visits to the hospital
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 87
Importance of CMARC Care Management: Psychosocial
• The hospital may be far away from the family’s home and many parents have been or not been in the hospital and have varying levels of emotional support
• Parents need to reintegrate into the community, their families and build or reestablish supports
• Parents may need help to find additional resources to address some any social determinants, trauma, substance use, and other psychosocial stressors
85
86
87

7/7/20
30
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 88
Using A Trauma Informed Approach
• Mothers and other family members of premature infants may experience PTSD-like symptoms from having an infant in a NICU
• Mothers of premature infants may have experienced their own trauma in one or more forms−Physical, sexual or emotional abuse −Alcohol or substance use −Mental health condition
• Re-traumatization of mothers can occur and should be avoided during care management
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 89
Using A Trauma Informed Approach
• Mothers need support to recover, heal from any trauma and build their resiliency and increase protective factors − Listen−Ask about exposure, symptoms and strengths−Provide some support based on some training
from the National Center for Child Traumatic Stress Network
−Communicate with the medical home about concerns
−Refer as appropriate
89
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 90
Examples of Follow Up for Premature Infants
• Medical home
• Special Infant Care Clinic (SICC)
• Different therapies: OT, PT or speech for feeding
• Special premature formulas
• Mixing breast milk with human milk fortifier
• Equipment: feeding tubes, ventilators, monitors, pumps, braces, etc
• Other specialists − Ophthalmology or Audiology
− Neurology, Pulmonary, GI, Infectious disease
− Developmental behavioral pediatrician
− Others
88
89
90

7/7/20
31
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 91
Providing Education to Support a Safe, Stable and Nurturing Environment
• Review signs and symptoms of illness and when to call the doctor, appropriate ER use and urgent care list
• Review need for well child visits and immunization schedule if needed to be adjusted for prematurity
• Discuss developmental milestones and provide anticipatory guidance to support mother-infant dyad interactions and bonding (including breastfeeding)
• Reinforce adjusted age based on presence of prematurity and explain how it relates to developmental and growth expectations and delays
• Safe sleep environment and avoid tobacco exposure
91
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 92
Early Intervention: Part C
• Premature infants may be eligible based on meeting criteria for developmental delay and/or one or more established conditions
• Examples of stablished conditions include:−Gestational age less than 27 weeks or less than
1000 grams−BPD requiring supplemental oxygen at discharge
from the NICU−NEC requiring surgery− Intraventricular hemorrhage III or IV
https://beearly.nc.gov/data/files/pdf/policies/Eligibility_Categories_Policy.pdf
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 93
Additional Important Linkages to Support Development
• Home visiting−Parents as Teachers−Healthy Families America −Child First
• Positive Parenting Program (Triple P)
• Newborn home visiting
• Family Support Groups
• Maternal Mental Health, Substance Use Disorder Treatment, including Medication Assisted Therapy (MAT) Providers
91
92
93

7/7/20
32
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 94
Adjusted Age/Corrected Age
• What is corrected age?How old the baby would be if born on their due dateUse up until 24 months corrected age
• Why is it important to know?Developmental milestonesNutrition
• CalculationAsk MOC “How old would your baby be if born on
their due date?” Not always accurate
Age in weeks – weeks premature = corrected ageBorrowed and adapted from Community Care of Lower Cape Fear
(CCLCF)
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 95
Current Photo Release with Children and Youth Branch
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 96
Safety• Car seat vs car bed
• Sleep environment−Back to sleep in crib−Appropriate mattress and crib, temperature
• Eliminate exposure to tobacco/smoke and not around caregiver misusing drugs or alcohol
• Assure caregivers not around with short fuses especially if fussy or difficult to care for baby−Prevention of abuse and neglect
94
95
96

7/7/20
33
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 97
Nutrition and Growth• Important to monitor weight −Also inputs and outputs
• Determine if increased work of breathing with feeds or color changes
• Follow recommendations from providers could include type/mixing of formula, fortifier for breast milk, additional supplements, additives or thickeners, equipment−Prevention of anemia and other deficiencies
• Difficult to do this via telemedicine but hybrid home visit may be an option
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 98
Fenton 2013 Growth Calculators for Preterm Infants
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 99
Medicaid, WIC and SNAP
• Medicaid or WIC should cover medically necessary formulas
• Videos from NC Child about SNAP (EBT) and WIC: https://www.facebook.com/ncchildorg/videos/1347909468751418/ (English) https://www.facebook.com/ncchildorg/videos/247718229943542/ (Spanish)
• WIC services: physical presence is waived and use of online referral form is most direct way to refer families: https://www.nutritionnc.com/wic/covid19.htm
97
98
99

7/7/20
34
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 100
ePASSPublic Portal of NC FAST
Improved to support social distancing!
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 101
Child Care
• Five-star quality childcare is ideal
• Medical care plan required for medical needs during care
• Encourage having childcare provider work with Child Care Health Consultant (CCHC)
• Find a CCHC to work with and support child careproviders to meet needs of premature infants in partnership with families: https://healthychildcare.unc.edu/cchcs-during-covid-19/
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 102
Summary
• The causes of preterm births are often not fully understood and may be a combination of factors
• Preterm births do occur in some situations where there is substance exposure
• Preterm infants may experience a variety of medical and non-medical issues and risks
• Care managers have a role to help support safe, stable and nurturing environments for premature infants
• Care managers can help ensure non-judgmental team-based care with the family in the center
100
101
102

7/7/20
35
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 103
Helpful Websites
• March of Dimes: https://www.marchofdimes.org/index.aspx#
• CDC Preterm Birth: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm
• Postpartum Support International: https://www.postpartum.net/
• UNC Center for Maternal and Infant Healthhttps://www.mombaby.org/
• NC Perinatal Health Strategic Planhttps://whb.ncpublichealth.com/phsp/
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 104
Questions?
Current Photo Release with Children and Youth Branch
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 105
Contact Information
Melissa L. Godwin, LCSWClinical Assistant ProfessorSchool of Social WorkUniversity of North Carolina, Chapel [email protected]
Megan Canady, MSW, MSPH UNC Center for Maternal & Infant Health UNC School of Medicine [email protected]
Gerri Mattson, MD, MSPH, FAAPPediatric Medical ConsultantChildren and Youth [email protected]
103
104
105

7/7/20
36
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 106
References• American Academy of Pediatrics. Hudak, M L. , Tan, R C. The Committee on Drugs and The Committee on Fetus and
Newborn. Neonatal Drug Withdrawal. Pediatrics,129 (2) e540-e560, 2012. https://doi.org/10.1542/peds.2011-3212. Retrieved July 6, 2020.
• American College of Obstetrics and Gynecology, Committee on Ethics. ACOG Committee Opnion No. 422: At risk drinking and Illicit Drug Use: Ethical Issues in Obstetric and Gynecologic Practice. American Journal of Obstetrics & Gynecology. 112:1449-1460, 2008.
• American College of Obstetrics and Gynecology, Committee on Obstetric Practice. American Society of Addiction Medicine. ACOG Committee Opinion No. 711: Opioid Use and Opioid Use Disorder in Pregnancy. American Journal of Obstetrics & Gynecology. August 2017 https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/08/opioid-use-and-opioid-use-disorder-in-pregnancy. Retrieved July 6, 2020.
• American College of Obstetrics and Gynecology, Committee on Obstetric Practice. ACOG Committee Opinion No. 807: Smoking Cessation During Pregnancy. American Journal of Obstetrics & Gynecology. May 2020. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/05/tobacco-and-nicotine-cessation-during-pregnancy.Retrieved July 6, 2020.
• American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th Edition. Washington, D.C.: American Psychiatric Association, 2013.
• American Society of Addiction Medicine (ASAM). Definition of Addiction. Adoption Date: April 12, 2011. https://www.asam.org/resources/definition-of-addiction;
• Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN). Breastfeeding Recommendations for Women Who Receive Medication-Assisted Treatment for Opioid Use Disorders: AWHONN Practice Brief Number 4. Journal of Obstetric, Gynecologic and Neonatal Nursing, 45 (4), 2016.
• Anderson T. et al. (2019). Maternal Smoking Before and During Pregnancy and the Risk of Sudden Unexpected Infant Death.
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 107
References• Pediatrics, 143 (4) e20183325; DOI: https://doi.org/10.1542/peds.2018-3325
Blount, T. et al. Reduction in Length of Stay and Morphine Use for NAS With the “Eat, Sleep, Console” Method. Pediatrics. 2019.
• Centers for Disease Control and Prevention, (2016). Sudden unexpected infant death and sudden infant death syndrome.
• Fiore M.C., et al. (2008). Treating tobacco use and dependence: 2008 update - clinical practice guidelines. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Agency for Healthcare Research and Quality.
• Jones H.E., Heil S.H., Tuten M., Chisolm M.S., Foster J.M., O'Grady K.E., Kaltenbach K. (2013). Cigarette smoking in opioid-dependent pregnant women: neonatal and maternal outcomes. Drug Alcohol Depend. 131(3):271-7.
• Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. New England Journal of Medicine 363 (24): 2320-31, 2010.
• Jones HE, O’Grady KE, Malfi D, et al. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. American Journal of Addiction 17 (5):372-86, 2008.
• Kennedy C, Finkelstein N, Hutchins E. Improving screening for alcohol use during pregnancy: the Massachusetts ASAP program. Maternal Child Health Journal. 8(3):137-47, 2004.
• Kocherlakota, P. Neonatal Abstinence Syndrome. Pediatrics. 134:e547–e561, 2014.
• Melvin C.L., Dolan-Mullen P., Windsor R.A., Whiteside H.P. Jr, Goldenberg R.L.. (2009). Recommended cessation counselling for pregnant women who smoke: A review of the evidence. Tob Contr, 9 Suppl 3:III80-4.
• Moon R. et al. (2016). SIDS and Other Sleep-Related Infant Deaths: Updated 2016 Recommendations for a Safe Infant Sleeping Environment TASK FORCE ON SUDDEN INFANT DEATH SYNDROME Pediatrics. 138 (5) e20162938; DOI: 10.1542/peds.2016-2938
NCDHHS, Division of Public Health | Substance Exposed Infants – What to Know for Best Infant Outcomes| July 9, 2020 108
References
• Moon R. et al. (2016). Safe infant sleep interventions: What is the evidence for successful behavior change? Current Pediatric Reviews, 12 (1), pp. 67-75, 10.2174/5733 96311666151026110148
• NIH/National Institute on Alcohol Abuse and Alcoholism. (2020, January 20). Combined prenatal smoking and drinking greatly increases SIDS risk. Science Daily. Retrieved July 2, 2020 from www.sciencedaily.com/releases/2020/01/200120113415.htm
• North Carolina State Center for Health Statistics 2018. (2019). Causes of Infant Mortality.
• North Carolina Vital Statistics Vol 1-2017 (2019). NC State Center for Health Statistics
• Office of the Chief Medical Examiner-Division of Public Health North Carolina Department of Health and Human Services, 201. (2018). Sleep-Related Death Infant Investigations.
• Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (2013). The N-SSATS Report: Tobacco Cessation Servicesexternal icon. Rockville, MD
• Tong, V. T., Dietz, P. M., Morrow, B., D'Angelo, D. V., Farr, S. L., Rockhill, K. M. (2013). Trends in smoking before, during, and after pregnancy--Pregnancy Risk Assessment Monitoring System, United States, 40 sites, 2000-2010. MMWR SurveillSumm, 62(6), 1-19.
• U.S. Department of Health and Human Services, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health (Ed.). (2014). The health consequences of smoking - 50 years of progress: a report of the Surgeon General.
• U.S. Preventive Service s Task Force. (2015). Tobacco Smoking Cessation in Adults, Including Pregnant Women: Behavioral and Pharmacotherapy Interventions. Available from: https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/tobacco-use-in-adults-and-pregnant-women-counseling-and-interventions1
106
107
108