Embed Size (px)
Citation preview
Cultural Competence Education for Healthcare Providers to Increase Knowledge of Breast Cancer Screening Recommendation in
Filipino-American Women
Dr. Michelle Modina, DNP, ANP-C, GNP, RN
January 17, 2015

Researcher’s Background
Proud to be a nurse for over 20 years Adult/Geriatric NP since 2001 specializing in breast
cancer screening and education Assistant Professor of Nursing at West Coast University Adjunct Professor at Chamberlain University Independent Contractor for White Memorial Medical
Center’s Breast Cancer Screening and Education Program
Learning Objectives/Outcomes
Increase cultural awareness about FA culture, healthcare beliefs and practices
Recognize and describe cultural issues and barriers to obtaining a screening mammogram and offer suggestions for practice
Value the importance of HCP screening mammogram recommendation as one of the strongest indicators of mammogram utilization in FA women
Increased knowledge will change practice to incorporate culturally appropriate breast CA screening recommendation
Statement of the problem
With breast cancer as the #1 killer of Filipino-American women, studies have shown that mammograms are underutilized by Filipino-American women and that a healthcare provider recommendation is an important reason why they obtain screening mammography.

Research question
Does cultural competence education change a healthcare provider’s knowledge of breast cancer screening recommendations appropriate for Filipino-American women?
Methodology
Design: One-group pretest-posttest quasi-experimental Instrument: Paired-sample t test using SPSS software Intervention: 30-min Cultural Competence Education IV: comparison of pre-intervention and post-intervention
trials DV: percent of correct score on the T/F objective test Setting: St. Vincent Medical Center Cancer Tumor Board
Meeting in Downtown Los Angeles Participants: 25 HCPs measured immediately before and
after cultural competence education
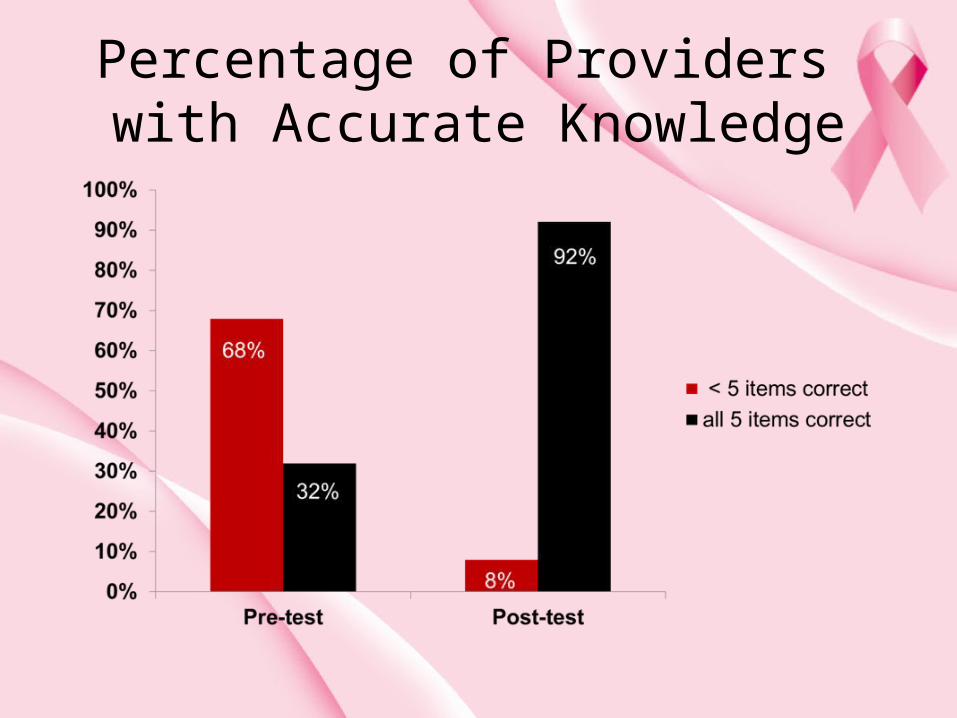
Percentage of Providers with Accurate Knowledge
Why it matters?
Breast CA leading cause of cancer deaths in Fil-Am women
Highest mortality rate but do not have highest incidence of breast cancer
Evidence shows that FA women likely to obtain mammogram if HCPs recommended it
30-60% Asian Americans report no prior mammogram compared to 10-21% of White women
In 2012, CDC and NCI report Asian Americans have lowest cancer screening rates
Why it matters?
US-born Filipino women younger than 55 had higher rates than White women of same age
When Asian women migrate to the US, risk of developing BC increases up to six-fold
Asian women living in the US for as little as a decade had an 80% higher risk of breast CA than new immigrants
LA County with highest incidence of breast cancer cases in California, 23.8% never received a mammogram
Study shows beliefs and perceptions of HCPs matter
Current Guidelines
USPSTF- biennial, 50-74 years oldACS- 40 years old, no specific age for stoppingACOG- every one to two years from 40-50
years old, annually after 50, no specific age for stopping
ACR, SBI (Society of Breast Imaging)- support ACOG recommendations
NCI- 40 years old, every 1-2 yearsCDP: EWC- 40 years old, every year
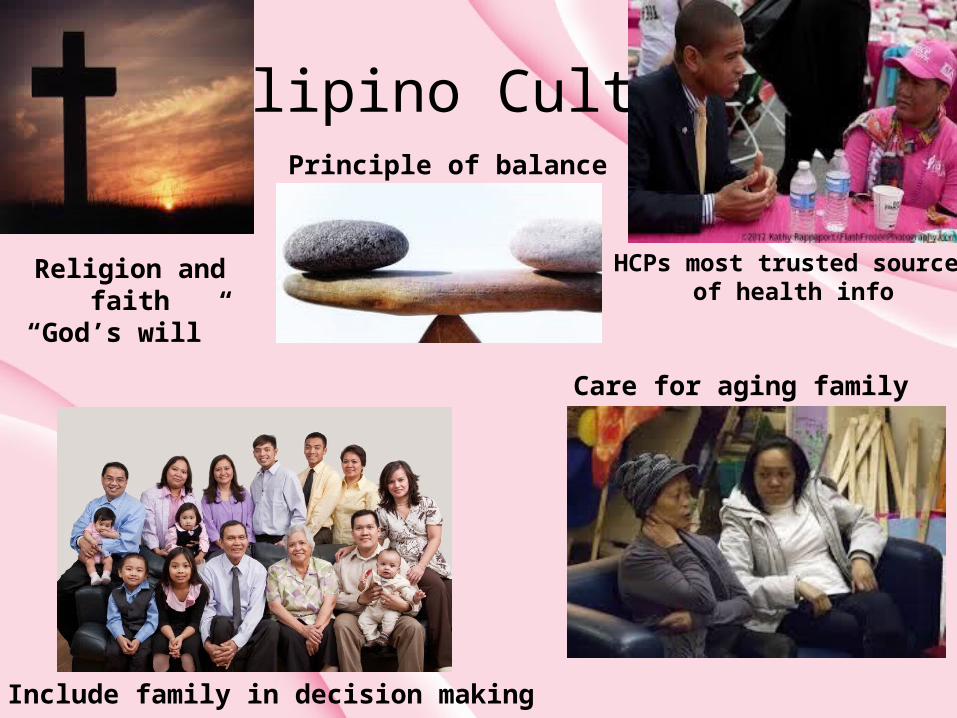
Filipino Culture
Religion and faith“God’s will”
Include family in decision making process
Care for aging family
Principle of balance
HCPs most trusted source of health info

Reasons to hesitate
Concern over cost and immigration status Only needed in the presence of symptoms, wait until
severely ill Low perceived need Inconvenience and difficulty getting to mammo facility Language barrier esp. 1st gen immigrants
Reasons to hesitate
Acculturation Embarrassment Belief that breast cancer caused by factors beyond
human control such as spiritual forces, fate, and predestination
Don’t know where to go
HCP Barriers
Differ in breast cancer screening guideline adherence
Mid-level practitioners more likely than MDs or DOs to adhere to guidelines
Physician age, gender, & specialty area associated with breast cancer screening practices
OB-GYNs favor aggressive breast cancer screening
Variations not fully understood Not enough evidence available
EBP Suggestions for Practice
HCP recommendation works- most trusted Provision of culturally sensitive care Discussion of BC and mammography in
churches, senior, and community centers- weekends preferred
Female HCP if possible Follow-up phone calls
EBP Suggestions for Practice
Brochures/handouts in TagalogSmall group discussion of FA womenCommunity liaisons/ social supportEmphasis on lifestyle, diet, exercise Word of mouth through friends and relatives is
effective
But… who pays?
Affordable Care Act aka “Obamacare”PPO and HMO usually100% coveredNo co-pay after August 1, 2012CA- CDP: Every Woman Counts
Private health plans, Medicaid, Medicare in CA:
baseline for ages 35-39, every 2 years for 40s, each year or physician recommendation
CDP:EWC State Program
are 40 years old or older are low income have medical insurance that does not cover breast
cancer screening have a high insurance deductible or co- payment are not getting these services through Medi-Cal or
another government-sponsored program live in California

Benefits to Stakeholders
Increased preventive health care visitsIncreased knowledge Increased adherence to screening mammoCultural sensitivity careEarly detection reduces morbidity and mortality
Potential Problems
If they don’t come, no screening mammogram recommendation
Lack of engagement Non-adherence despite intervention Strong and persistent cultural factors Guideline confusion
“ An ounce of prevention is worth a pound of cure.”
~ Ben Franklin
References• American Cancer Society. (2011). What are the key statistics about breast cancer? Retrieved from
http://www.cancer.org/Cancer/BreastCancer/DetailedGuide/breast-cancer-key-statistics• American Nurses Association (ANA). (2001). Code of ethics for nurses with interpretive statements. Silver Spring,
MD: Author.• California Department of Public Health. Cancer detection program: every woman counts. Retrieved from
www.cdph.ca.gov/programs/cancerdetection/pages/cancerdetectionprogramseverywomancounts.aspx• California state data center: Demographic profiles. (2011, August 25). Retrieved from
http://www.dof.ca.gov/research/demographic/state_census_data_center/census_2010/view.php• Centers for Disease Control and Prevention. (2007). Breast cancer statistics. Retrieved from
http://www.cdc.gov/cancer/breast/statistics/• Chang, E., Clarke, C., Cockburn, M., Glaser, S., Gomez, S., Horn-Ross, P., & Keegan, T. (2010). Hidden breast
cancer disparities in Asian women: disaggregating incidence rates by ethnicity and migrant status. American Journal of Public Health. doi:10.2105/AJPH.2009.163931
• County of Los Angeles Public Health. (2010, February).Health indicators for women in Los Angeles county. Retrieved from www.publichealth.lacounty.gov/owh/docs/Health-Indicators-2010.pdf
• Han, H.-R., Kim, K., Kim, M., & Lee, H. (2009). Tailored lay health worker intervention improves breast cancer screening outcomes in non-adherent Korean-American women. Health Education Research, 24(2), 318-329.
• Ho, R., Muraoka, M., Cuaresma, C., Guerrero, R., & Agbayani, A. (2010, July). Addressing the excess breast cancer mortality in Filipino women in Hawaii through AANCART, an NCI Community Network Program. Hawaii Medical Journal 69(7), 164-166.
• Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington DC: National Academies Press. Retrieved from http://www.nap.edu/catalog/10027.html
• Ju, E., Lee, H., Lundquist, M., & Vang, P. (2010). Breast and cervical cancer screening among Asian American women and Latinas: Does race/ethnicity matter? Journal of Women’s Health 19(10), 1877-1884. doi:10.1089/jwh.2009.1783
References• Ko, C., Sadler, G., Ryujin, L., & Dong, A. (2003, August). Filipina American women’s breast cancer knowledge,
attitudes, and screening behaviors. Public Health, 3(27). Retrieved from http://www.biomedcentral.com/1471-2458/3/27
• Maxwell, A., Bastani, R., & Warda, U. (1997, September). Breast cancer screening and related attitudes among Filipino-American women. Cancer Epidemiology, Biomarkers & Prevention, 6, 719-726. Retrieved from http://cebp.aacrjournals.org/content/6/9/719.long
• Maxwell, A., Bastani, R., & Warda, U. (2000). Demographic predictors of cancer screening among Filipino and Korean immigrants in the United States. Amercian Journal of Preventive Medicine, 18(1), 62-68.
• Maxwell, A., Bastani, R., Vida, P., & Warda, U. (2005, June). Strategies to recruit and retain older Filipino-American immigrants for a cancer screening study. Journal of Community Health, 30(1), 167-179. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1810967/
• Peek, M. & Han, J. (2004). Disparities in screening mammography. Journal of General Internal Medicine, 19, 184-194. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1492136/
• Sohl, S. & Moyer, A. (2007, October). Tailored interventions to promote mammography screening: A meta-analytic review. Preventive Medicine, 45(4), 252-261.
• Surveillance Research Center Control and Population Sciences: Joint regression program. Retrieved from www.surveillance.cancer.gov/joinpoint/
• Susan G. Komen Breast Cancer Foundation: Los Angeles County 10/2010 Breast Cancer Statistics. Retrieved from www.komenlacounty.org/assets/get.../bc.../bcam-presentation.pdf
• Trends in cancer incidence, mortality, risk factors, and health behaviors in California.(2010, January). Retrieved from www.ccrcal.org/pdf/Reports/09TrendReport-2-24-10.pdf
• United States Preventative Task Force. Assessing evidence at the individual study level. Retrieved from http://www.uspreventiveservicestaskforce.org/uspstf08/methods/procmanual4.htm





















![Filipino sa Konstitusyon [Filipino in the Constitution] (Fil 40)](https://img.pdfslide.us/doc/110x75/558caf97d8b42a27188b4731/filipino-sa-konstitusyon-filipino-in-the-constitution-fil-40.jpg)