Embed Size (px)
Citation preview

U. Joseph Schoepf, MDPhilip Costello, MD
Index terms:Computed tomography (CT),
angiographyComputed tomography (CT), multi–
detector rowEmbolism, pulmonary, 60.72, 944.77Pulmonary arteries, CT, 944.12911,
944.12912, 944.12915,944.12916, 944.12918
State of the Art
Published online10.1148/radiol.2302021489
Radiology 2004; 230:329–337
Abbreviations:DVT � deep venous thrombosisECG � electrocardiographyPE � pulmonary embolism
1 From the Department of Radiology,Brigham and Women’s Hospital, Har-vard Medical School, 75 Francis St,Boston, MA 02115. Received Novem-ber 14, 2002; revision requested Jan-uary 8, 2003; revision received January22; accepted March 4. Addresscorrespondence to U.J.S. (e-mail:[email protected]).© RSNA, 2004
CT Angiography for Diagnosisof Pulmonary Embolism:State of the Art1
In daily clinical routine, computed tomography (CT) has practically become thefirst-line modality for imaging of pulmonary circulation in patients suspected ofhaving pulmonary embolism (PE). However, limitations regarding accurate diagno-sis of small peripheral emboli have so far prevented unanimous acceptance of CT asthe reference standard for imaging of PE. The development of multi–detector rowCT has led to improved visualization of peripheral pulmonary arteries and detectionof small emboli. The finding of a small isolated clot at pulmonary CT angiography,however, may be increasingly difficult to correlate with results of other imagingmodalities, and the clinical importance of such findings is uncertain. Therefore, themost realistic scenario to measure efficacy of pulmonary CT angiography when PEis suspected may be assessment of patient outcome. Meanwhile, the high negativepredictive value of a normal pulmonary CT angiographic study and its associationwith beneficial patient outcome has been demonstrated. While the introduction ofmulti–detector row technology has improved CT diagnosis of PE, it has also chal-lenged its users to develop strategies for optimized contrast material delivery,reduction of radiation dose, and management of large-volume data sets created atthose examinations.© RSNA, 2004
Supplemental material: rsnajnls.radiology.org/cgi/content/full/2302021489/DC1
Where do we stand now with regard to the optimal diagnostic imaging tool for pulmonaryembolism (PE)? Increasingly sophisticated clinical algorithms for bedside exclusion of PEare being developed. These algorithms are based mainly on negative results of a D-dimertest (1–4), which is a highly sensitive, albeit nonspecific, means for ruling out PE. Still,there is a high and increasing demand for imaging tests when PE is suspected, althoughactual numbers are difficult to establish.
Some still regard conventional pulmonary angiography as the standard technique fordiagnosis of PE, but in reality it is infrequently performed (5–8). Conventional angiogra-phy is an invasive procedure, although the incidence of complications with contemporarytechnique is low (9,10). More important, there is accumulating evidence illustrating thelimitations of this technique for unequivocal diagnosis of isolated peripheral pulmonaryemboli: Two recent analyses of the interobserver agreement rates for detection of subseg-mental emboli with selective pulmonary angiography ranged from only 45% to 66%(11,12). Given such limitations, use of this method as an objective and readily reproduc-ible tool for the verification of findings at competing imaging modalities regarding thepresence of PE seems questionable, and the status of pulmonary angiography as thestandard of reference for diagnosis of PE is in doubt (11,12).
Use of nuclear medicine imaging, once the first study in the diagnostic algorithm for PE,is in decline (13,14) owing to the high percentage of indeterminate studies (73% of allstudies performed [15]) and poor interobserver correlation (16). Revised criteria for theinterpretation of ventilation-perfusion scans (17,18) and newer technologies in nuclearmedicine, such as single photon emission computed tomography, (19,20) can help de-crease the ratio of indeterminate scintigraphic studies but cannot offset the limitationsinherent to a functional imaging test (21).
Contrast material–enhanced magnetic resonance (MR) angiography has been evaluated
State of the Art
329
Ra
dio
logy

for use in the diagnosis of acute PE (22–25). However, the acquisition protocolsthat are currently available for pulmo-nary MR angiography lack sufficient spa-tial resolution for reliable evaluation ofperipheral pulmonary arteries (24,25).More important, this modality has notseen widespread use in acutely ill patientssuspected of having PE, owing to lack ofgeneral availability, relatively long exam-ination times, and difficulties in patientmonitoring.
That leaves us with computed tomog-raphy (CT), which for most practical pur-poses has become the first-line imagingtest in daily clinical routine for patientssuspected of having PE. The most impor-tant advantage of CT over other imagingmodalities is that both mediastinal andparenchymal structures can be evaluated,and thrombus can be directly visualized(26,27) (Fig 1). Investigators have shownthat up to two-thirds of patients inwhom there is an initial suspicion of PEreceive another diagnosis (28), includingsome potentially life-threatening diseasessuch as aortic dissection, pneumonia,lung cancer, and pneumothorax (29).Most of these diagnoses are amenable toCT demonstration so that, in many cases,a specific origin for the patient’s symp-toms and important additional diagnosescan be established (21).
Interobserver agreement for CT is bet-ter than that for scintigraphy (30). In astudy published in 2000 (16), the inter-observer agreement for the diagnosis of
PE was excellent for spiral CT angiogra-phy (� � 0.72) and only moderate forventilation-perfusion lung scanning (� �0.22). Moreover, a diagnostic algorithmfor PE that includes CT appears to bemore cost-effective than algorithms thatdo not include CT but are based on otherimaging modalities (ultrasonography[US], scintigraphy, pulmonary angiogra-phy) (31). In addition, there are someindications that CT not only may be usedfor evaluating thoracic anatomy in caseswhere PE is suspected but also could, tosome degree, allow derivation of physio-logic parameters on lung perfusion at sin-gle–detector row electron-beam and mul-ti–detector row CT (32–34).
The main impediment to the unani-mous acceptance of CT as the modality ofchoice for the diagnosis of acute PE hasbeen the limitation of this modality foraccurate detection of small peripheralemboli. Results of early studies (35–38) inwhich single–detector row CT was com-pared with selective pulmonary angiog-raphy demonstrated the high accuracy ofCT for detection of PE to the segmentalarterial level but suggested that subseg-mental pulmonary emboli may be over-looked on CT scans. The degree of accu-racy that can be achieved for thevisualization of subsegmental pulmonaryarteries and for the detection of emboli inthese vessels with single–detector row,dual–detector row, and electron-beamCT scanners was found to range from61% to 79% (37,39–41), limitations that
have been overcome by developments inCT technology.
ADVANTAGES OFMULTI–DETECTOR ROW CTFOR IMAGING PE
The past few years have seen decisive dy-namic developments in CT technology,mainly brought about by the advent ofmulti–detector row CT (42,43). The cur-rent generation of four–, eight–, and 16–detector row CT scanners now allow forcoverage of the entire chest with 1-mmor submillimeter resolution within ashort single breath-hold—now less than10 seconds in the case of 16–detector rowCT (Fig 2; Movie 1, rsnajnls.radiology.org/cgi/content/full/2302021489/DC1).
The ability to cover substantial ana-tomic volumes with high in-plane andthrough-plane spatial resolution hasbrought a number of clear advantages.Shorter breath-hold times have beenshown to benefit imaging of patients sus-pected of having PE and underlying lungdisease by reducing the percentage ofnondiagnostic pulmonary CT angiographicstudies (44). The near isotropic nature ofhigh-spatial-resolution multi– detectorrow CT data lends itself to two- and three-dimensional visualization. This may, insome instances, improve diagnosis of PE(45) (Fig 3) but is generally of greaterimportance for conveying information to
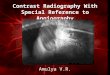
Figure 1. Extensive acute central PE with “saddle embolus” extending into both central pulmonary arteries in a 72-year-oldman. Contrast material–enhanced 16–detector row CT yielded coronal volume renderings in (a) anterocranial and (b) an-terior perspectives, which allow intuitive visualization of the location and extent of embolus (arrows).
330 � Radiology � February 2004 Schoepf and Costello
Ra
dio
logy
helsenet.info

referring clinicians on the location andextent of embolic disease in a more intu-itive display format (Fig 1). Probably themost important advantage is improveddepiction of small peripheral emboli. Ithas been shown that single–detector rowCT with thinner sections (eg, 2 vs 3 mm)can provide superior demonstration ofsegmental and subsegmental pulmonaryarteries (39). With single–detector rowCT, however, the range of coverage withthin section widths within one breathhold was limited (39,41). The high spatialresolution of 1-mm- or submillimeter-collimation data sets now allows evalua-tion of pulmonary vessels down to sixth-order branches (46) and substantiallyincreases the detection rate of segmentaland subsegmental pulmonary emboli
(47). This improved detection rate islikely due to reduced volume averagingand accurate analysis of progressivelysmaller vessels by use of thinner sections.These results are most striking in periph-eral arteries with an anatomic course par-allel to the scan plane; such vessels tendto be most affected by volume averagingwhen thicker sections are used (47). Thehigh spatial resolution along the scanaxis of a thin-collimation multi–detectorrow CT data set, however, allows an ac-curate evaluation of the full course ofsuch vessels (Fig 4). The interobservercorrelation for confident diagnosis ofsubsegmental emboli with thin-sectionmulti–detector row CT by far exceeds thereproducibility of selective pulmonaryangiography (11,12,47).
THE QUANDARY OF THEISOLATED SUBSEGMENTALEMBOLUS
While traditional technical limitations ofCT in the diagnosis of PE appear to havebeen successfully overcome by multi–de-tector row CT, we are now facing newchallenges that are a direct result of ourhigh-resolution imaging capabilities. Inour recent experience, small peripheralclots that might have gone unnoticed inthe past are now frequently detected, of-ten in patients with minor symptoms(Figs 5, 6).
Although there may be no doubt in themind of the interpreting radiologist as tothe presence of a small isolated clot on agood quality multi–detector row CTscan, such a finding will be increasinglydifficult to prove in a correlative manner.Animal experiments with artificial em-boli used as an independent standard in-dicate that thin-collimation four–detec-tor row CT is at least as accurate asconventional pulmonary angiographyfor the detection of small peripheral em-boli (48). However, it appears highly un-likely that pulmonary angiography willbe performed in a patient merely to provethe presence of an isolated small (2–3-mm) embolus. In addition, given the lim-ited interobserver correlation for pulmo-nary angiography discussed earlier (11,12), it appears doubtful that this test,even if performed, would provide proofas useful and conclusive as that of thin-section multi–detector row CT. Investi-gators in broad-based studies such as theProspective Investigation of PulmonaryEmbolism Diagnosis II study, who set outto establish the efficacy of multi–detectorrow CT in cases where PE is suspected,account for this latter fact by using acomposite reference test based on venti-lation-perfusion scanning, US of thelower extremities, pulmonary angiogra-phy, and venography to establish the PEstatus of the patient (49).
Perhaps more important, there is agrowing sense of insecurity within the clin-ical community as to how to care for pa-tients in whom a diagnosis of isolated pe-ripheral embolism has been established. Ithas been shown that 6% (15) to 30% (50)of patients with documented PE have clotsonly in subsegmental and smaller arteries,but the clinical importance of small pe-ripheral emboli in subsegmental pulmo-nary arteries in the absence of a centralembolus is uncertain. It is assumed thatone important function of the lung is toprevent small emboli from entering the ar-
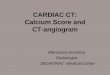
Figure 2. Normal pulmonary vessels in a 56-year-old man who presented with mild chest painafter a long-distance flight. A contrast-enhanced 16–detector row CT examination covers theentire chest within 10 seconds, allowing analysis of even the most peripheral pulmonaryvessels with exquisite detail. Coronal reconstruction using (a) maximum intensity projectionand (b) volume-rendering techniques. The entire scanned volume is shown in Movie 1(rsnajnls.radiology.org/cgi/content/full/2302021489/DC1).
Volume 230 � Number 2 CT Angiography of Pulmonary Embolism � 331
Ra
dio
logy
helsenet.info

terial circulation (26). Such emboli arethought to form even in healthy individu-als, although this notion has never beensubstantiated (51). Controversy also existsregarding whether the treatment of smallemboli, once detected, may result in a bet-ter clinical outcome for patients (38,52,53).There is little disagreement though, thatthe presence of peripheral emboli may bean indicator of concurrent deep venousthrombosis (DVT), thus potentially herald-ing more severe embolic events (28,50,54).A burden of small peripheral emboli mayalso have prognostic relevance in individ-uals with cardiopulmonary restriction(26,50,53) and for the development of
Figure 3. Contrast-enhanced pulmonary CTangiography in a 43-year-old woman sus-pected of having acute PE. Lymphatic tissue(arrows) in mediastinum and pulmonary hi-lum may be misinterpreted as embolic fillingdefects in central pulmonary vessels by lessexperienced observers if (a) transverse sectionsalone are used for diagnosis, while (b) coronalmultiplanar reformations from four–detectorrow CT allow better differentiation of lym-phatic tissue and vessels and may reducesources of diagnostic error.
Figure 4. Contrast-enhanced thin-section pulmonary CT angiography in a 52-year-old manafter right lung transplantation. Transverse 1-mm-thick sections show isolated pulmonary emboli(arrows) in segmental and subsegmental arteries in the right middle lobe of the lung and allowdetailed visualization of course of obliquely oriented vessels and of isolated filling defects insegmental and subsegmental branches.
Figure 5. (a) Transverse contrast-enhanced 16–detector row CT image obtained with 0.75-mmcollimation in a 62-year-old man with chest pain. Isolated peripheral pulmonary embolus (arrow)in sixth-order pulmonary arterial branch in segment 8 of the right lung is shown. (b) Lungwindow display of more caudal transverse section from same study shows subsequent pulmonaryinfarct (arrow) in the corresponding vascular territory in the right lower lobe. (c) Coronalvolume-rendered display (anterior view) shows isolated peripheral filling defect (arrow) in oth-erwise normal pulmonary vascular tree.
332 � Radiology � February 2004 Schoepf and Costello
Ra
dio
logy
helsenet.info

chronic pulmonary hypertension in pa-tients with thromboembolic disease (50).
Perhaps the most practical and realisticscenario for studying the efficacy of CTfor the evaluation of patients in whomPE is suspected is to assess patient out-come. There is a growing body of experi-ence concerning the negative predictivevalue of a normal CT study and patientoutcome if anticoagulants are subse-quently withheld (16,44,53,55–59). Ac-cording to these retrospective investiga-tions, the negative predictive value of anormal CT study is high, approaching98%, regardless of whether multi–detectorrow technology was used (44) or underly-ing lung disease was present (58). The fre-quency of a subsequent clinical diagnosis
of PE or DVT after a negative pulmonaryCT angiogram is low; the frequency is evenlower than that after a negative or low-probability ventilation-perfusion scan (53).Thus, even single–detector row CT appearsto be a reliable imaging tool for excludingclinically relevant PE, and it appears thatanticoagulants can be safely withheldwhen the CT scan is normal and of gooddiagnostic quality (53,59).
PROBLEMS AND LIMITATIONSOF CT FOR DIAGNOSIS OF PE
Contrast Material Injectionand Artifacts
Despite advances in CT technology,there are still several factors that can ren-
der pulmonary CT angiographic imagesinconclusive. The most common reasonsfor nondiagnostic CT images are poorcontrast enhancement of pulmonary ves-sels, patient motion, and increased imagenoise due to excessive patient obesity.
The advent of multi–detector row CTnecessitates an extensive revision of con-trast material injection protocols. Fasterscanning times allow acquisition duringmaximal contrast enhancement of pul-monary vessels (41) but pose an in-creased challenge for precise timing ofthe contrast material bolus. Strategiesthat have the potential to improve thedelivery of contrast material for high andconsistent vascular enhancement duringpulmonary CT angiography currently in-
Figure 6. Contrast-enhanced 16–detector row CT study obtained with 0.75-mm collimation in a 57-year-old man with mildpleuritic chest pain. (a) Consecutive transverse sections show isolated peripheral pulmonary embolus (arrows) in a subseg-mental pulmonary artery in segment 9 of the left lung. (b) Oblique sagittal multiplanar reformation also shows embolus(arrow). (c) Coronal volume-rendered display (posterior view) shows isolated peripheral filling defect (arrow) in otherwisenormal pulmonary vascular tree.
Volume 230 � Number 2 CT Angiography of Pulmonary Embolism � 333
Ra
dio
logy
helsenet.info

clude use of a test bolus or automatedbolus-triggering techniques (60). Salinechasing (61,62) has been used for effec-tive utilization of contrast material andfor reduction of streak artifacts arisingfrom a dense concentration of contrastmaterial in the superior vena cava. Mul-tiphasic injection protocols have provedto be beneficial for general CT angiogra-phy (63,64) but, to our knowledge, havenot been scientifically evaluated for thepulmonary circulation.
Another limitation that, in some in-stances, results in suboptimal diagnosticquality of pulmonary CT angiographicimages is motion artifact due to patientrespiration or transmitted cardiac pulsa-tion. The shorter breath-hold times thatare possible with multi–detector row CTshould facilitate investigation in dys-pneic patients (44) and reduce the occur-rence of respiratory motion artifacts.Similarly, artifacts arising from transmit-ted cardiac pulsation appear amenable todecreased temporal resolution with fastCT acquisition techniques (41). Electro-cardiographic (ECG) synchronization ofthe CT acquisition allows effective reduc-tion of cardiac pulsation artifacts thatmight interfere with the unambiguousevaluation of cardiac structures, the tho-racic aorta, and pulmonary structures(65,66).
However, the spatial resolution that
could be achieved with, for example, aretrospectively ECG–gated techniquewith the previous generation of four–de-tector row CT scanners was limited bythe relatively long scanning duration in-herent to data oversampling (66). Thus, athin-section acquisition could only beachieved for relatively small volumes (eg,coronary arterial tree) but not for ex-tended coverage of the entire chest. Theadvent of 16–detector row scanners noweffectively eliminates these previoustradeoffs. With 16–detector row CT, it isnow possible to cover the entire thoraxwith submillimeter resolution in a singlebreath hold with retrospective ECG gat-ing, effectively reducing transmitted pul-sation artifacts (Fig 7). This way, poten-tial sources of diagnostic pitfalls arisingfrom cardiac motion can be averted. Itneeds to be shown whether this technol-ogy will be able to further increase theaccuracy of CT for detection of small em-boli in the vicinity of the heart.
Radiation Dose
Use of thin-section multi–detector rowCT protocols has been shown to improvethe visualization of pulmonary arteries(46) and the detection of small subseg-mental emboli (47). When PE is sus-pected, the establishment of an unequiv-ocal diagnosis regarding the presence of
emboli or other disease on the basis ofhigh-quality multi–detector row CTscans may reduce the overall radiationburden in patients, since further work-upwith other tests that involve ionizing ra-diation may be less frequently required.However, if a four–detector row CT pro-tocol with 1-mm collimation is chosen toreplace a single–detector row CT proto-col with 5-mm collimation, the increasein radiation dose ranges between 30%(67) and 100% (42).
Similar increases in radiation dose,however, are not to be expected with theintroduction of 16 – detector row CTtechnology with submillimeter resolu-tion capabilities. The addition of detectorelements should improve tube outpututilization, compared with that of cur-rent four–detector row scanners, and re-duce the ratio of excess radiation dosethat does not contribute to image gener-ation (68). As sophisticated technical de-vices become part of clinical practice—devices that modulate and adapt tubeoutput relative to the geometry and x-rayattenuation of the scanned object (ie, thepatient) (69–71)—substantial dose sav-ings can be realized without compromis-ing diagnostic quality (72). The specificeffect of such devices on the detection ofPE, however, has not been scientificallyevaluated to date, to our knowledge.
The most important factor for ensuring
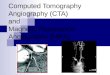
Figure 7. Contrast-enhanced retrospective ECG–gated 16–detector row pulmonary CT angiography study in a 35-year-oldman suspected of having PE. Sagittal volume-rendered images show paracardiac pulmonary vessels in left lower lung lobe.(a) During systole, severe stair-step artifacts (arrows) occur along the course of pulmonary vessels owing to transmittedcardiac motion. (b) During diastole, cardiac pulsation artifacts are substantially reduced, and almost motion-free depictionof paracardiac pulmonary vessels (arrows) can be achieved.
334 � Radiology � February 2004 Schoepf and Costello
Ra
dio
logy

responsible utilization of the technicalprowess of multi–detector row CT is in-creased awareness by technologists andradiologists with regard to radiation ex-posure to patients. It has been shownthat the diagnostic quality of chest CT isnot compromised if tube output is ad-justed to the body type of the individualpatient (73). Also, with multi–detectorrow CT, radiologists are increasinglyadapting to the concept of volume imag-ing. There is a trade-off between in-creased spatial resolution and image
noise when thinner and thinner sectionsare acquired with fast CT techniques.Given the great flexibility and diagnosticbenefit that a thin-section, nearly isotro-pic multi–detector row CT data set pro-vides, radiologists are increasingly will-ing to compromise on the degree ofimage noise that they are willing to ac-cept on an individual transverse thin sec-tion in order to keep radiation dosewithin reasonable limits.
Data Management
Multi–detector row CT increases ourdiagnostic capabilities; however, the mas-sive amount of data that are generatedwith this technique puts a substantialstrain on any image analysis and archivingsystem. A thin-section 16–detector row CTstudy in a patient suspected of having PEroutinely results in 500–600 transverse im-ages. Three-dimensional display of multi–detector row CT data in such a patient mayaid diagnosis in some instances and helpprevent diagnostic pitfalls, allowing, forexample, correct interpretation of hilarlymphatic tissue adjacent to central pul-monary arteries (74) (Fig 3). There are in-dications that focal lung disease can be di-agnosed accurately by using maximumintensity projection reconstructions thatbeneficially “condense” large-volume multi–detector row CT data sets (75). In con-trast, a diagnosis of PE is usually mostbeneficially established on the basis ofindividual transverse sections, althoughextensive (Fig 1) or isolated findings of PE(Figs 5, 6), as well as normal pulmonaryvasculature (Fig 2, Movie 1 [rsnajnls.radiology.org/cgi/content/full/2302021489/DC1]), canbe visualized in a comprehensive mannerby means of three-dimensional reconstruc-tions based on thin-section multi–detectorrow CT data. Interpretation of such large-volume studies is only feasible with use ofdigital workstations that allow viewing in“scroll-through” or cine modes.
Development of dedicated algorithmsfor computer-aided detection (76) maybe helpful in the future for identificationof pulmonary emboli in large-volumemulti–detector row CT data sets. Largeand accessible storage capacity is an es-sential requirement for successful routineperformance of multi–detector row CT ina busy clinical environment. Adaptationof this environment to the new demandsgenerated by the introduction of ever-faster scanning techniques is not a trivialtask. New modalities for data transfer,data archiving, and image interpretationwill have to be devised to make full use of
the vast potential of multi–detector rowCT imaging.
CT ALGORITHM FOREVALUATION OF PATIENTSWHO MAY HAVE PE
We propose a simple CT-based algo-rithm, which is based on our beneficialexperiences with thin-section multi–de-tector row pulmonary CT angiography,for the imaging evaluation of patients inwhom there is clinical suspicion of PE(Fig 8). This algorithm reflects the clinicalreality at our institution and works wellin our hands for establishment of a de-finitive diagnosis in the majority of cases.
Before proceeding to imaging, themost important first-line clinical tool atour institution for diagnosis of PE is D-dimer testing, the results of which, if neg-ative, are usually accepted for ruling outPE (3), especially if other causes for thepatient’s signs and symptoms can be es-tablished during further work-up. In clin-ically stable patients, the same regimenof anticoagulants is usually chosen fortreatment of both PE and DVT. There-fore, if a diagnosis of DVT can be estab-lished (eg, by means of positive findingsat lower extremity US) in a patient inwhom PE is clinically suspected, usuallyno further diagnostic work-up of the pul-monary circulation is pursued (Fig 8). Ifno diagnosis of DVT can be established insuch a patient, CT angiography of thepulmonary circulation is performed and,if the results are positive for PE, the pa-tient is treated accordingly (Fig 8). If agood-quality CT angiographic study doesnot reveal PE, the work-up for PE canordinarily stop at this point (Fig 8), andother diagnostic routes for elucidation ofthe source of the patient’s signs andsymptoms should be pursued.
In the unlikely case of a persistent highclinical suspicion of PE despite a negativegood-quality CT pulmonary angiogram,there is the theoretical option of pursu-ing a definitive diagnosis by means ofconventional pulmonary angiography asthe last resort to exhaust all diagnosticmeans available. To date, however, thishas not occurred in our practice. In thosefew cases where a poor quality CT angio-graphic study does not allow us to estab-lish or rule out with confidence a diagno-sis of PE as the source of the patient’ssymptoms, we usually attempt repeatpulmonary CT angiography, if at all fea-sible in view of the patient’s clinical pre-sentation. In many instances, analysisand remedying of factors for failed pul-
Figure 8. CT-based algorithm for imagingevaluation of patients clinically suspected ofhaving PE. If diagnosis of DVT can be estab-lished in a patient suspected of having PE, thetherapeutic regimen is usually predeterminedand no further diagnostic work-up of pulmo-nary circulation is pursued. If no diagnosis ofDVT can be established, CT angiography (CTA)of pulmonary circulation is performed; if re-sults are positive for PE, the patient is treated.If a good quality CT study does not reveal PE,work-up can usually stop at this point. In theunlikely case of persistent high clinical suspi-cion of PE despite a negative good-quality pul-monary CT angiogram, there is the theoreticaloption of pursuing definitive diagnosis bymeans of conventional pulmonary angiogra-phy to exhaust all diagnostic means available.In cases where a poor-quality CT study doesnot allow one to establish or rule out withconfidence PE or other sources of the patient’ssymptoms, repeat pulmonary CT angiographyis usually attempted.
Volume 230 � Number 2 CT Angiography of Pulmonary Embolism � 335
Ra
dio
logy

monary CT angiography (eg, improvedintravenous access, higher rate of con-trast material injection, use of automatedbolus-triggering techniques, adaptationof tube output to patient’s body type, useof ECG-gated acquisition) result in diag-nostic studies at repeat CT angiography.
CONCLUSION
With multi–detector row CT technology,past limitations of CT for the diagnosis ofPE should be effectively overcome; for allpractical purposes, CT has become thefirst-line modality for imaging in patientssuspected of having PE. CT is now anattractive means for establishing a safe,highly accurate, and cost-effective diag-nosis of PE. The lack of a clinically avail-able reference standard for the diagnosisof PE suggests that the medical commu-nity should replace theoretical and aca-demic discussions on the relative value ofdifferent imaging modalities with morerealistic approaches based on patient out-come. Retrospective studies (16,44,53,55–59) already indicate the high negative pre-dictive value for a normal multi–detectorrow CT pulmonary angiographic study.However, prospectively acquired patientoutcome studies are still needed. Oncethis type of investigation has confirmedthat a negative CT study can be used tosafely rule out PE, we believe use of CT toaid in diagnosis of PE will be unani-mously accepted.
References1. Wells PS, Anderson DR, Rodger M, et al.
Excluding pulmonary embolism at thebedside without diagnostic imaging:management of patients with suspectedpulmonary embolism presenting to theemergency department by using a simpleclinical model and d-dimer. Ann InternMed 2001; 135:98–107.
2. Kruip MJ, Slob MJ, Schijen JH, et al. Use ofa clinical decision rule in combinationwith D-dimer concentration in diagnosticworkup of patients with suspected pul-monary embolism: a prospective manage-ment study. Arch Intern Med 2002; 162:1631–1635.
3. Dunn KL, Wolf JP, Dorfman DM, Fitz-patrick P, Baker JL, Goldhaber SZ. NormalD-dimer levels in emergency departmentpatients suspected of acute pulmonaryembolism. J Am Coll Cardiol 2002; 40:1475–1478.
4. Brown MD, Rowe BH, Reeves MJ, et al.The accuracy of the enzyme-linked im-munosorbent assay D-dimer test in thediagnosis of pulmonary embolism: ameta-analysis. Ann Emerg Med 2002; 40:133–144.
5. Schluger N, Henschke C, King T, et al.Diagnosis of pulmonary embolism at alarge teaching hospital. J Thorac Imaging1994; 9:180–184.
6. Khorasani R, Gudas TF, Nikpoor N, PolakJF. Treatment of patients with suspectedpulmonary embolism and intermediate-probability lung scans: is diagnostic im-aging underused? AJR Am J Roentgenol1997; 169:1355–1357.
7. Crawford T, Yoon C, Wolfson K, et al. Theeffect of imaging modality on patientmanagement in the evaluation of pulmo-nary thromboembolism. J Thorac Imag-ing 2001; 16:163–169.
8. Prologo JD, Glauser J. Variable diagnosticapproach to suspected pulmonary embo-lism in the ED of a major academic ter-tiary care center. Am J Emerg Med 2002;20:5–9.
9. Stein PD, Athanasoulis C, Alavi A, et al.Complications and validity of pulmonaryangiography in acute pulmonary embo-lus. Circulation 1992; 85:462–468.
10. Zuckerman DA, Sterling KM, Oser RF.Safety of pulmonary angiography in the1990s. J Vasc Interv Radiol 1996; 7:199–205.
11. Diffin D, Leyendecker JR, Johnson SP,Zucker RJ, Grebe PJ. Effect of anatomicdistribution of pulmonary emboli on in-terobserver agreement in the interpreta-tion of pulmonary angiography. AJR Am JRoentgenol 1998; 171:1085–1089.
12. Stein PD, Henry JW, Gottschalk A. Reas-sessment of pulmonary angiography forthe diagnosis of pulmonary embolism: re-lation of interpreter agreement to the or-der of the involved pulmonary arterialbranch. Radiology 1999; 210:689–691.
13. Schibany N, Fleischmann D, ThallingerC, et al. Equipment availability and diag-nostic strategies for suspected pulmonaryembolism in Austria. Eur Radiol 2001; 11:2287–2294.
14. Leveau P. Diagnostic strategy in pulmo-nary embolism. National French survey.Presse Med 2002; 31:929–932.
15. Value of the ventilation/perfusion scanin acute pulmonary embolism: results ofthe Prospective Investigation of Pulmo-nary Embolism Diagnosis (PIOPED). ThePIOPED investigators. JAMA 1990; 263:2753–2759.
16. Blachere H, Latrabe V, Montaudon M, etal. Pulmonary embolism revealed on he-lical CT angiography: comparison withventilation-perfusion radionuclide lungscanning. AJR Am J Roentgenol 2000;174:1041–1047.
17. Stein PD, Relyea B, Gottschalk A. Evalua-tion of individual criteria for low proba-bility interpretation of ventilation-perfu-sion lung scans. J Nucl Med 1996; 37:577–581.
18. Stein PD, Gottschalk A. Review of criteriaappropriate for a very low probability ofpulmonary embolism on ventilation-per-fusion lung scans: a position paper. Ra-dioGraphics 2000; 20:99–105.
19. Palmer J, Bitzen U, Jonson B, Bajc M.Comprehensive ventilation/perfusionSPECT. J Nucl Med 2001; 42:1288–1294.
20. Bajc M, Bitzen U, Olsson B, et al. Lungventilation/perfusion SPECT in the artifi-cially embolized pig. J Nucl Med 2002;43:640–647.
21. Garg K, Welsh CH, Feyerabend AJ, et al.Pulmonary embolism: diagnosis with spi-ral CT and ventilation-perfusion scan-ning—correlation with pulmonary an-
giographic results or clinical outcome.Radiology 1998; 208:201–208.
22. Meaney J, Weg JG, Chenevert TL, Staf-ford-Johnson D, Hamilton BH, PrinceMR. Diagnosis of pulmonary embolismwith magnetic resonance angiography.N Engl J Med 1997; 336:1422–1427.
23. Roberts DA, Gefter WB, Hirsch JA, et al.Pulmonary perfusion: respiratory-trig-gered three-dimensional MR imagingwith arterial spin tagging—preliminaryresults in healthy volunteers. Radiology1999; 212:890–895.
24. Gupta A, Frazer CK, Ferguson JM, et al.Acute pulmonary embolism: diagnosiswith MR angiography. Radiology 1999;210:353–359.
25. Oudkerk M, van Beek EJ, Wielopolski P, etal. Comparison of contrast-enhancedmagnetic resonance angiography andconventional pulmonary angiographyfor the diagnosis of pulmonary embo-lism: a prospective study. Lancet 2002;359:1643–1647.
26. Gurney JW. No fooling around: direct vi-sualization of pulmonary embolism (edi-torial). Radiology 1993; 188:618–619.
27. Woodard PK. Pulmonary arteries must beseen before they can be assessed (edito-rial). Radiology 1997; 204:11–12.
28. Hull R, Raskob GE, Ginsberg JS, et al. Anoninvasive strategy for the treatment ofpatients with suspected pulmonary em-bolism. Arch Intern Med 1994; 154:289–297.
29. van Rossum AB, Pattynama PM, MallensWM, et al. Can helical CT replace scintig-raphy in the diagnostic process in sus-pected pulmonary embolism? a retrolec-tive-prolective cohort study focusing ontotal diagnostic yield. Eur Radiol 1998;8:90–96.
30. van Rossum AB, van Erkel AR, van Persijnvan Meerten EL, Ton ER, Rebergen SA,Pattynama PM. Accuracy of helical CT foracute pulmonary embolism: ROC analy-sis of observer performance related toclinical experience. Eur Radiol 1998;8:1160–1164.
31. van Erkel AR, van Rossum AB, Bloem JL,Kievit J, Pattynama PN. Spiral CT angiog-raphy for suspected pulmonary embo-lism: a cost-effectiveness analysis. Radiol-ogy 1996; 201:29–36.
32. Groell R, Peichel KH, Uggowitzer MM, etal. Computed tomography densitometryof the lung: a method to assess perfusiondefects in acute pulmonary embolism.Eur J Radiol 1999; 32:192–196.
33. Schoepf U, Bruening R, Konschitzky H, etal. Pulmonary embolism: comprehensivediagnosis using electron-beam computedtomography for detection of emboli andassessment of pulmonary blood flow. Ra-diology 2000; 217:693–700.
34. Wildberger JE, Niethammer MU, Klotz E,et al. Multi-slice CT for visualization ofpulmonary embolism using perfusionweighted color maps. Rofo Fortschr GebRontgenstr Neuen Bildgeb Verfahr 2001;173:289–294.
35. Remy-Jardin M, Remy J, Wattinne L, Gi-raud F. Central pulmonary thromboem-bolism: diagnosis with spiral volumetricCT with the single-breath-hold tech-nique—comparison with pulmonary an-giography. Radiology 1992; 185:381–387.
36. Teigen CL, Maus TP, Sheedy PF 2nd, et al.
336 � Radiology � February 2004 Schoepf and Costello
Ra
dio
logy

Pulmonary embolism: diagnosis withcontrast-enhanced electron-beam CT andcomparison with pulmonary angiogra-phy. Radiology 1995; 194:313–319.
37. Goodman LR, Curtin JJ, Mewissen MW,et al. Detection of pulmonary embolismin patients with unresolved clinical andscintigraphic diagnosis: helical CT versusangiography. AJR Am J Roentgenol 1995;164:1369–1374.
38. Remy-Jardin M, Remy J, Deschildre F, etal. Diagnosis of pulmonary embolismwith spiral CT: comparison with pulmo-nary angiography and scintigraphy. Radi-ology 1996; 200:699–706.
39. Remy-Jardin M, Remy J, Artaud D, et al.Peripheral pulmonary arteries: optimiza-tion of the spiral CT acquisition protocol.Radiology 1997; 204:157–163.
40. Qanadli SD, Hajjam ME, Mesurolle B, etal. Pulmonary embolism detection: pro-spective evaluation of dual–detector rowhelical CT versus selective pulmonary ar-teriography in 157 patients. Radiology2000; 217:447–455.
41. Schoepf UJ, Helmberger T, Holzknecht N,et al. Segmental and subsegmental pul-monary arteries: evaluation with elec-tron-beam versus spiral CT. Radiology2000; 214:433–439.
42. McCollough CH, Zink FE. Performanceevaluation of a multi-slice CT system.Med Phys 1999; 26:2223–2230.
43. Hu H, He HD, Foley WD, Fox SH. Fourmultidetector-row helical CT: imagequality and volume coverage speed. Radi-ology 2000; 215:55–62.
44. Remy-Jardin M, Tillie-Leblond I, SzapiroD, et al. CT angiography of pulmonaryembolism in patients with underlying re-spiratory disease: impact of multislice CTon image quality and negative predictivevalue. Eur Radiol 2002; 12:1971–1978.
45. Remy-Jardin M, Remy J, Cauvain O, et al.Diagnosis of central pulmonary embo-lism with helical CT: role of two-dimen-sional multiplanar reformations. AJRAm J Roentgenol 1995; 165:1131–1138.
46. Ghaye B, Szapiro D, Mastora I, et al. Pe-ripheral pulmonary arteries: how far inthe lung does multi–detector row spiralCT allow analysis? Radiology 2001; 219:629–636.
47. Schoepf U, Holzknecht N, HelmbergerTK, et al. Subsegmental pulmonary em-boli: improved detection with thin-colli-mation multi–detector row spiral CT. Ra-diology 2002; 222:483–490.
48. Baile E, King GG, Muller NL, et al. Spiralcomputed tomography is comparable toangiography for the diagnosis of pulmo-nary embolism. Am J Respir Crit CareMed 2000; 161:1010–1015.
49. Gottschalk A, Stein PD, Goodman LR,Sostman HD. Overview of prospective in-vestigation of pulmonary embolism diag-nosis II. Semin Nucl Med 2002; 32:173–182.
50. Oser RF, Zuckerman DA, Gutierrez FR,Brink JA. Anatomic distribution of pul-monary emboli at pulmonary angiogra-phy: implications for cross sectional im-aging. Radiology 1996; 199:31–35.
51. Tetalman MR, Hoffer PB, Heck LL, Kun-zmann A, Gottschalk A. Perfusion lungscan in normal volunteers. Radiology1973; 106:593–594.
52. Novelline R, Baltarowich O, AthanasoulisC, Greenfield A, McKusick K. The clinicalcourse of patients with suspected pulmo-nary embolism and a negative pulmo-nary angiogram. Radiology 1978; 126:561–567.
53. Goodman LR, Lipchik RJ, Kuzo RS, et al.Subsequent pulmonary embolism: risk af-ter a negative helical CT pulmonary an-giogram—prospective comparison withscintigraphy. Radiology 2000; 215:535–542.
54. Patriquin L, Khorasani R, Polak JF. Corre-lation of diagnostic imaging and subse-quent autopsy findings in patients withpulmonary embolism. AJR Am J Roentge-nol 1998; 171:347–349.
55. Garg K, Sieler H, Welsh CH, et al. Clinicalvalidity of helical CT being interpreted asnegative for pulmonary embolism: impli-cations for patient treatment. AJR Am JRoentgenol 1999; 172:1627–1631.
56. Gottsater A, Berg A, Centergard J, et al.Clinically suspected pulmonary embo-lism: is it safe to withhold anticoagula-tion after a negative spiral CT? Eur Radiol2001; 11:65–72.
57. Ost D, Rozenshtein A, Saffran L, Snider A.The negative predictive value of spiralcomputed tomography for the diagnosisof pulmonary embolism in patients withnondiagnostic ventilation-perfusionscans. Am J Med 2001; 110:16–21.
58. Tillie-Leblond I, Mastora I, Radenne F, etal. Risk of pulmonary embolism after anegative spiral CT angiogram in patientswith pulmonary disease: 1-year clinicalfollow-up study. Radiology 2002; 223:461–467.
59. Swensen SJ, Sheedy PF 2nd, Ryu JH, et al.Outcomes after withholding anticoagula-tion from patients with suspected acutepulmonary embolism and negative com-puted tomographic findings: a cohortstudy. Mayo Clin Proc 2002; 77:130–138.
60. Kirchner J, Kickuth R, Laufer U, et al.Optimized enhancement in helical CT:experiences with a real-time bolus track-ing system in 628 patients. Clin Radiol2000; 55:368–373.
61. Hopper KD, Mosher TJ, Kasales CJ, et al.Thoracic spiral CT: delivery of contrastmaterial pushed with injectable saline so-lution in a power injector. Radiology1997; 205:269–271.
62. Haage P, Schmitz-Rode T, Hubner D, et al.Reduction of contrast material dose andartifacts by a saline flush using a doublepower injector in helical CT of the tho-rax. AJR Am J Roentgenol 2000;174:1049–1053.
63. Bae K, Heiken JP, Brink JA. Aortic andhepatic peak enhancement at CT: effectof contrast medium injection rate—phar-macokinetic analysis and experimentalporcine model. Radiology 1998; 206:455–464.
64. Fleischmann D, Rubin GD, Bankier AA,Hittmair K. Improved uniformity of aor-
tic enhancement with customized con-trast medium injection protocols at CTangiography. Radiology 2000; 214:363–371.
65. Schoepf UJ, Becker CR, Bruening RD, etal. Electrocardiographically gated thin-section CT of the lung. Radiology 1999;212:649–654.
66. Flohr T, Prokop M, Becker C, et al. A ret-rospectively ECG-gated multislice spiralCT scan and reconstruction techniquewith suppression of heart pulsation arti-facts for cardio-thoracic imaging with ex-tended volume coverage. Eur Radiol2002; 12:1497–1503.
67. Schoepf U, Bruening RD, Hong C, et al.Multislice helical CT imaging of focal anddiffuse lung disease: comprehensive diag-nosis with reconstruction of contiguousand high-resolution CT sections from asingle thin-collimation scan. AJR Am JRoentgenol 2001; 177:179–184.
68. Flohr T, Stierstorfer K, Bruder H, et al.New technical developments in multi-slice CT. I. Approaching isotropic resolu-tion with sub-millimeter 16-slice scan-ning. Rofo Fortschr Geb RontgenstrNeuen Bildgeb Verfahr 2002; 174:839–845.
69. Kalender WA, Wolf H, Suess C, et al. Dosereduction in CT by on-line tube currentcontrol: principles and validation onphantoms and cadavers. Eur Radiol 1999;9:323–328.
70. Gies M, Kalender WA, Wolf H, Suess C.Dose reduction in CT by anatomicallyadapted tube current modulation. I. Sim-ulation studies. Med Phys 1999; 26:2235–2247.
71. Kalender WA, Wolf H, Suess C. Dose re-duction in CT by anatomically adaptedtube current modulation. II. Phantommeasurements. Med Phys 1999; 26:2248–2253.
72. Greess H, Nomayr A, Wolf H, et al. Dosereduction in CT examination of childrenby an attenuation-based on-line modula-tion of tube current (CARE dose). Eur Ra-diol 2002; 12:1571–1576.
73. Wildberger JE, Mahnken AH, Schmitz-Rode T, et al. Individually adapted exam-ination protocols for reduction of radia-tion exposure in chest CT. Invest Radiol2001; 36:604–611.
74. Remy J, Remy-Jardin M, Artaud D, Fri-bourg M. Multiplanar and three-dimen-sional reconstruction techniques in CT:impact on chest diseases. Eur Radiol1998; 8:335–351.
75. Gruden JF, Ouanounou S, Tigges S, et al.Incremental benefit of maximum-inten-sity-projection images on observer detec-tion of small pulmonary nodules revealedby multidetector CT. AJR Am J Roentge-nol 2002; 179:149–157.
76. Schoepf UJ, Das M, Schneider AC, Ander-son A, Wood SA, Costello P. Computeraided detection (CAD) of segmental andsubsegmental pulmonary emboli on 1-mmmultidetector-row CT (MDCT) studies (ab-str). Radiology 2002; 225(P):384.
Volume 230 � Number 2 CT Angiography of Pulmonary Embolism � 337
Ra
dio
logy