Embed Size (px)
Citation preview

CSP04 Topics in Hematopathology: Flow Cytometry and Molecular Genetics as Tools for Understanding, Diagnosing, and Treating
Hematolymphoid Malignancy
William Morice MD, PhD Horatiu Olteanu MD, PhD
Andrew Feldman MD John Frater MD
2011 Annual Meeting – Las Vegas, NV
AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600
Chicago, IL 60603

CSP04 Topics in Hematopathology: Flow Cytometry and Molecular Genetics as Tools for Understanding, Diagnosing, and Treating Hematolymphoid Malignancy The aim of this session is to introduce to the audience emerging areas of scientific knowledge in the pathogenesis and identification of hematologic malignancies and illustrate how this knowledge is being used to shape and improve patient care. Along these lines, the speakers will present topics in T-cell lymphoma pathogenesis and treatment, advanced flow cytometry in the diagnosis of myeloid neoplasms and plasma cell proliferative disorders, and the pathogenesis and diagnosis of extramedullary blastic myeloid neoplasm (myeloid sarcomas). Each of the speakers will be discussing from their own published work as well as the published literature, but the presentations will emphasize the practical, day-to-day implications of the findings for practicing pathologists and laboratorians. As such, these studies will not only be informative for the individual topic, but will also provide a tangible context for how advances in scientific knowledge are effecting our daily clinical practice. Therefore the topics should be of keen interest to a broad audience. Each presenter will deliver the content in a 45 minute lecture followed by a 10 minute question and answer session with the audience.
• Recognize how identifying disease pathogenesis provides opportunity for disease specific treatments. • Identify the role of ancillary studies such as immunohistochemistry, flow cytometry, and molecular
pathology in disease diagnosis and prognostication. • Recognize how scientific discovery has direct impact on patient care.
FACULTY: William Morice MD, PhD Horatiu Olteanu MD, PhD Andrew Feldman MD John Frater MD Practicing Pathologists Hematopathology New Techniques 3.0 CME/CMLE Credits Accreditation Statement: The American Society for Clinical Pathology (ASCP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians. This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME). Credit Designation: The ASCP designates this enduring material for a maximum of 3 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. ASCP continuing education activities are accepted by California, Florida, and many other states for relicensure of clinical laboratory personnel. ASCP designates these activities for the indicated number of Continuing Medical Laboratory Education (CMLE) credit hours. ASCP CMLE credit hours are acceptable to meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. All ASCP CMLE programs are conducted at intermediate to advanced levels of learning. Continuing medical education (CME) activities offered by ASCP are acceptable for the American Board of Pathology’s Maintenance of Certification Program.

1
Myeloid SarcomaMyeloid Sarcoma
John L Frater, MDDepartment of Pathology and ImmunologyWashington University School of Medicine
St Louis, Missouri
Disclosure Information
I have no relevant conflicts of interest.
Myeloid sarcomaThe World Health Organization defines myeloid sarcoma (synonyms: granulocytic sarcoma, chloroma) as “a tumor mass consisting of myeloid blasts with or without maturation occurring at an anatomical site other than theoccurring at an anatomical site other than the bone marrow.” Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press; 2008.

2
Myeloid sarcoma• Also referred to as
granulocytic/monoblasticsarcomas or extramedullary myeloid tumors
• Originally termed chloromas because of the greenish color (Gr. Χλωρός = “green”) imparted on gross examination due to the production of myeloperoxidase
Sauter (2008)
Myeloid sarcoma• Wide age distribution; more common in the pediatric age group with
an incidence of up to 30% in some studies of pediatric AML versus 2-5% in adults
• Most commonly presents concurrently with a new diagnosis of AML or as evidence of disease recurrence, a significant subset of myeloid sarcomas (27% in one large study) will present as de novo diseasesarcomas (27% in one large study) will present as de novo disease
• Studies that define outcomes and treatment response are limited and there are no established guidelines for clinical decision-making.
• Therapies typically include local radiation, systemic chemotherapy, immunotherapy and donor lymphocyte infusions.
• Outcomes are usually poor, although may be slightly better than outcomes of primary or relapsed AML without extramedullaryinvolvement
Myeloid sarcoma
• Reported at nearly every anatomic site, but are most frequently encountered in the skin and soft tissues, lymph nodes, and gastrointestinal tractgastrointestinal tract
• clinical symptoms are largely dependent on the site of involvement
Photos: University of Virginia Medical School

3
Myeloid sarcoma• May occur in the presence or absence of bone marrow
disease• Its presence is sufficient to establish a clinical diagnosis
of AML• Bone marrow involvement will become detectable in
nearly all patients who originally presented with isolated myeloid sarcoma, with a mean interval of 10 months
• Isolated myeloid sarcoma also appears to be more common at relapse in patients who have undergone allogeneic stem cell transplantation, occurring in 8-20% of transplanted patients (graft-vs-leukemia surveillance or the biology of high risk AML treated with transplantation?)
Myeloid sarcoma• Due to the aggressive nature
of the disease, necrosis may be present, as well as areas with numerous mitotic figures and tingible-body macrophages.
• The pattern of infiltration is phighly dependent on the tissue involved
Large intestine
Pileri (2007)
Myeloid sarcoma• Leukemic blasts will diffusely
infiltrate tissue within extranodalsites.
• Can appear to be cohesive when there are areas with dense fibroconnective tissue or a prominent stromal reaction, thus mimicking metastatic carcinoma.
• Infiltrates within lymph nodes may obliterate the entire nodal architecture or be confined to the paracortex or sinuses with occasional residual germinal centers.
Lymph node paracortex
Pileri (2007)

4
Myeloid sarcoma
Klco JM et al, Int J Lab Hematol (2011), in press
Myeloid sarcoma
• Though myeloblasts, or blast equivalents such as promonocytes, are the predominant cell population, varying degrees of myeloid maturation may bedegrees of myeloid maturation may be present within the leukemic infiltrate.
• Transformation of a myeloproliferativeneoplasm can demonstrate evidence of more than one lineage.
Myeloid sarcoma• Previously subdivided by
morphologic features into granulocytic sarcomas and monoblasticsarcomas.
• Granulocytic sarcomas were further divided based on the extent of maturation into blastic, immature or differentiated variants.
Klco JM et al, Int J Lab Hematol (2011), in press

5
Myeloid sarcoma
• Myelomonocytic forms, similar to acute myelomonocytic leukemia, are also common and myeloid sarcomas with erythroid and megakaryoblasticdifferentiation have also rarely been reported. C f t d ll t• Cases of extramedullary acute promyelocytic leukemia are rare and the majority occur at relapse with a preference for central nervous system involvement
Megakaryoblastic AML (lymph node)CD41 (bottom)Hirose Y (2001)
Myeloid sarcoma
Klco JM et al, Int J Lab Hematol (2011), in press
Myeloid sarcoma
• “Aleukemic” myeloid sarcomas can morphologically be easily confused with other hematologic malignancies:
• Aggressive B cell lymphomas• Aggressive B-cell lymphomas• Non-hematolymphoid tumors

6
Myeloid sarcoma
Klco JM et al, Int J Lab Hematol (2011), in press
Myeloid sarcomaImmunohistochemistry
• CD43 and lysozyme– most sensitive markers as they are expressed in
nearly 100% of cases in most studies– neither is specific
M l id d CD68 ti l f tl• Myeloperoxidase and CD68 antigen are also frequently expressed; the KP-1 clone of anti-CD68 has higher sensitivity but lower specificity than PG-M1
• CD34 immunoreactivity is not a consistent finding– present in 40/92 cases– frequently negative in cases with monocytic
differentiation
Myeloid sarcomaImmunohistochemistry
• Immunohistochemistry for CD45 is variable; in one study only 14 of 24 cases demonstrated positivity for CD45.
• Other commonly used myeloid markers• Other commonly used myeloid markers include CD33 and CD117 (C-kit).

7
Myeloid sarcomaImmunohistochemistry – Monocytic Differentiation
• Frequently negative for CD34 and/or CD117. • Although myeloperoxidase is classically negative in
acute monocytic leukemia, immunoreactivity for anti-myeloperoxidase is not sufficient for the exclusion of monocytic differentiationmonocytic differentiation
• CD68, CD43, CD33, and lysozyme are expressed by neoplastic monocytes within the bone marrow and in extramedullary sites.
• Immunohistochemistry for the hemoglobin scavenger receptor CD163 can also be positive in some cases with monocytic differentiation
Myeloid sarcomaImmunohistochemistry – Monocytic Differentiation
• CD56 (N-CAM) expression has been associated with monocytic differentiation, extramedullary disease, or t(8;21); however, this has not been a consistent finding.
• CD4 is also commonly expressed by monocyticleukemias however CD4 expression lacks specificity forleukemias, however, CD4 expression lacks specificity for myeloid sarcomas.
• As expected, myelomonocytic myeloid sarcomas will demonstrate a mixed pattern of immunoreactivity for the above-mentioned myeloid and monocytic markers.
Myeloid sarcomaImmunohistochemistry – Monocytic Differentiation
Our group has also recently shown the usefulness of immunohistochemistry for CD14 and Kruppel-like factor 4 (KLF4) in monocytic leukemias.
Histologic features and expression pattern in acute monoblastic leukemia. A, H&E. B, CD34. C, Krüppel-like factor 4 (KLF4). D, CD68. E, CD163. F, CD14. Case demonstrates positivity for CD68, KLF4, CD14, and CD163 with no expression of CD34.
Klco JM, et al. Am J Clin Pathol (2011) 135:720-730

8
Myeloid sarcomaImmunohistochemistry
• Erythroid differentiation: glycophorin A, hemoglobin, or CD71 (transferrin receptor), although many of these markers may only show variable positivity.
• Occasional erythroid precursors can also show expression of CD117.
• CD71 expression from formalin fixed paraffin embedded (FFPE)• CD71 expression from formalin fixed paraffin embedded (FFPE) tissue may be the most useful as its expression decreases during erythroid maturation, allowing for easier interpretation.
• Megakaryocytic differentiation: CD61 (platelet glycoprotein IIIa), CD41 (platelet glycoprotein IIB), CD42b (glycoprotein Ib, alpha polypeptide), linker for activation of T cells (LAT), vWF (factor VIII-related antigen) or CD31.
• CD31 is the least specific within this group, as it is expressed by endothelial cells, plasma cells and a subset of granulocytic elements.
Cutaneous myeloid sarcoma• In the skin, lesions most
commonly present as multiple papules, plaques, or nodules.
• Most common region of involvement is the torsoinvolvement is the torso, although the head and neck regions and extremities are also involved in many cases
Photos: MY Hurley, MD, Saint LouisUniversity
Cutaneous myeloid sarcoma
• Retrospective study of 83 patients presenting with CMS over a 19 year period at 2 tertiary care institutions in the midwestUnited StatesUnited States.
• We emphasized the demographics, clinical presentation, and pathologic workup of these patients, and their response to therapy. Hurley MY, et al, submitted

9
Materials and methods• A search of the electronic databases of the Department of
Dermatology, Section of Dermatopathology, Saint Louis University, and the Section of Anatomic and Molecular Pathology, Department of Pathology and Immunology, Washington University, was performed
• Patient inclusion criteria for our search were less than 90 years of age and also a diagnosis of CMS from January 1st 1990 to June 1st 20092009
• Typical patient demographic data was collected (date of birth, gender, and race) along with dermatologic clinical CMS presentation regarding lesion size, character, and anatomical site
• We also collected data concerning other anatomical involvement including liver, lymph node, and central nervous system, etc. both during clinical treatment and at autopsy when available.
• Patient survival status was also recorded
Hurley MY, et al, submitted
Materials and methods
• This study also described bone marrow in comparison with cutaneous involvement of myeloid blast cells
• Whenever available we also included• Whenever available, we also included karyotype and fluorescence in-situhybridization results
Hurley MY, et al, submitted
Results
• CMS appears to affect genders randomly (p>0.05) but there is a male predominance (1.51:1)
•The disease appears to affect primarily Caucasians
Hurley MY, et al, submitted

10
Results
• The mean age is 52 y with 4 patients being less than 1 year old
•The upper extremities are involved more frequently than would be predicted by body surface area (P<0.05)•The most common region involved is the torso•CMS most commonly presents as multiplepapules, nodules, or plaques
Hurley MY, et al, submitted
Results
• 19 pts had involvement of sites outside the bone marrow and skin
• CNS and lymph node are the most commonly involved extramedullary anatomic sites in ypatients with CMS
• Most (15/19) were from cases with monocytic differentiation
• Lower % than that reported by Kaddu et al (1999, 26 pts)
Hurley MY, et al, submitted
Results
• AML most commonly preceded the diagnosis of CMS (57%) or presented concurrently (34%) with CMS
• Most patients with a diagnosis of CMS were eventually diagnosed with AML (86%)
Hurley MY, et al, submitted

11
Bone marrow biopsy
• 70/83 (84%) patients had at least one bone marrow biopsy available for review.
• Lower percentage of M4/M5 cases than previously reported (Kaiserling et al [1994, 16 pts],
Diagnosis Number of cases
Acute myeloid leukemia (AML) with minimal differentiation (FAB: M0)
4
AML without maturation (FAB: M1)
4
AML with maturation (FAB: M2)
6
Acute myelomonocytic leukemia (FAB: M4)
15
Acute monocytic/ monoblastic 13( g [ , p ],Kaddu et al [1999, 26 pts])
leukemia (FAB: M5a/b)
Acute megakaryoblastic leukemia (FAB: M7)
1
AML, unclassifiable* 6
AML, myelodysplasia-related** 3
Biphenotypic acute leukemia (B-myeloid)
1
Chronic myelogenous leukemia 1
Chronic myelomonocytic leukemia***
5
Myelodysplastic syndrome**** 4
Juvenile myelomonocytic leukemia
1
No evidence of malignancy 6
* Not classified due to lack of enzyme cytochemical analysis of blasts** Includes 2 cases of myelodsplastic syndrome which ultimately progressed to AML and 1 case presenting de novo with multilineage dysplasia*** Includes 2 cases which progressed to acute myeloid leukemia**** All cases presented with increased bone marrow blasts; 1 represented a therapy-related myelodysplastic syndrome
Hurley MY, et al, submitted
Cytogenetics and molecular genetics
• Cytogenetics abnormal in 23/28 (82%) of cases– 2 patients with loss of chromosome 7– 2 patients with loss of the long arm of chromosome 7– 7 patients with trisomy of chromosome 8– 5 patients with abnormalities of chromosome 11q23 involving the
MLL locus– 7 patients had multiple nonspecific structural and/or numerical
chromosomal abnormalities– 5 patients had normal conventional cytogenetic analysis
• Fluorescence in situ-hybridization confirmed the findings of MLL rearrangement in 4 patients and trisomy of chromosome 8 in 4 patients, and revealed low-level abnormal loss of AML1 locus in one patient with normal conventional cytogenetics.
Hurley MY, et al, submitted
ResultsSkin biopsy - workup
• 19 cases with involved skin biopsies and a prior bone marrow diagnosis of acute myeloid leukemia were evaluated by a hematoxylin and eosin-stained section without additional studies
• An additional 19 patients, all with a prior history of bone i l t b t l id l k i h dmarrow involvement by acute myeloid leukemia, had
skin biopsies evaluated by a hematoxylin and eosin-stained section and a Leder stained section, in which the blasts were Leder negative
• The remaining 45 cases had immunohistochemistry analysis as part of their workup
Hurley MY, et al, submitted

12
ResultsSkin biopsy
• Diffuse architecture -18 cases
• Destruction of dermal microanatomy y
Leder
CD7 CD117 CD34
Hurley MY, et al, submitted
ResultsSkin biopsy
• Focal architecture – 38 cases
• Perivascular• Periadnexal• InterstitialInterstitial
The microscopic features of skin disease are variable and do not correlate with clinical appearance of lesions.
Hurley MY, et al, submitted
Results
• The recent paper by Benet et al notes similar patterns of involvement of the skin: certain histologic patterns are associated with specific leukemia types, such as the association of acute myelomonocytic leukemia and acute monoblastic/ monocyticleukemia with a granuloma annulare-type histology.
• Although Benet et al do not report survival data the extent andAlthough Benet et al do not report survival data, the extent and pattern of involvement do not correlate with survival.
• The 1-year mortality status was could be determined for 59 (or 71.1%) of cases
• Of these 59 cases, 86.4% were deceased 1-year after the diagnosis date
• Of the cases who died during the observed period, the mean number of survival days after the diagnosis date was 227 + 319 (range 14 to 1561).
• Survival does not appear to be impacted by more recent chemotherapeutic regimens
Hurley MY, et al, submitted

13
Immunohistochemistry analysis of involved skin biopsies
Antibody # Cases % Positive cases
CD2 2 0%
CD3 16 0%
CD4 10 50%
CD43 12 100%
CD45 19 84%
CD45RO 3 33%
CD56 6 83%
CD68 14 100%
CD5 2 50%
CD7 4 25%
CD8 4 0%
CD10 2 0%
CD20 20 0%
CD23 1 0%
CD30 6 0%
CD34 16 19%
CD99 1 100%
CD79a 5 0%
CD117 6 33%
TdT 4 25%
Vimentin 3 100%
Pan-cytokeratin 1 0%
Myeloperoxidase 36 56%
Lysozyme 29 97%
Chloroacetate esterase
19 53%
Hurley MY, et al, submitted
Immunohistochemistry analysis of involved skin biopsies
Antibody # Cases % Positive cases
CD2 2 0%
CD3 16 0%
CD4 10 50%
CD43 12 100%
CD45 19 84%
CD45RO 3 33%
CD56 6 83%
CD68 14 100%
CD5 2 0%
CD7 4 25%
CD8 4 0%
CD10 2 0%
CD20 20 0%
CD23 1 0%
CD30 6 0%
CD34 16 19%
CD99 1 100%
CD79a 5 0%
CD117 6 33%
TdT 4 25%
Vimentin 3 100%
Pan-cytokeratin 1 0%
Myeloperoxidase 36 56%
Lysozyme 29 97%
Chloroacetate esterase
19 53%
Hurley MY, et al, submitted
Lysozyme Myeloperoxidase CD68
DxPositive Negative Positive Negative Positive Negative
M0 1
M1 1 1
M2 2
M4 5 3 4 2
M5 3 1 3 2
M7 1
CMML 3 2 1
MDS 1 3
JMML 1 1
Unkn 12 1 8 5 9
Unclass 3
Totals 28 1 19 17 14 0
Lysozyme is very sensitive for the detection of myeloid disease but is relatively nonspecific for distinction of malignancies with monocyticdifferentiation (e.g. M4, M5 CMML) from other leukemias without monocyticDifferentiation (e.g.M1, M2).Hurley MY, et al, submitted

14
Lysozyme Myeloperoxidase CD68
DxPositive Negative Positive Negative Positive Negative
M0 1
M1 1 1
M2 2
M4 5 3 4 2
M5 3 1 3 2
M7 1
CMML 3 2 1
MDS 1 3
JMML 1 1
Unkn 12 1 8 5 9
Unclass 3
Totals 28 1 19 17 14 0
MPO is frequently negative due to the high frequency of AML with monocytic differentiation
Hurley MY, et al, submitted
Lysozyme Myeloperoxidase CD68
DxPositive Negative Positive Negative Positive Negative
M0 1
M1 1 1
M2 2
M4 5 3 4 2
M5 3 1 3 2
M7 1
CMML 3 2 1
MDS 1 3
JMML 1 1
Unkn 12 1 8 5 9
Unclass 3
Totals 28 1 19 17 14 0
CD68 is reportedly similar to lysozyme in sensitivity, and is similarly nonspecific for distinction of malignancies with monocytic differentiation (e.g. M4, M5 CMML)from other leukemias without monocytic differentiation (e.g.M1, M2).
Hurley MY, et al, submitted
Immunohistochemistry of CMSAnalysis using CD14, CD33, KLF4, CD163
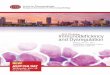
Case with monocytic differentiation and a bone marrow diagnosis of acute myelomonocytic leukemia (FAB-M4) showing positivity for lysozyme (A), CD14 (E) and KLF-4 (nuclear) (G), and negativity for the remaining markers (B, myeloperoxidase; C, CD163; D, CD117; F,myeloperoxidase; C, CD163; D, CD117; F, CD34; H, CD33)
Amador-Ortiz C, et al. J Cutan Pathol (2011), in press.

15
Immunohistochemistry of CMSAnalysis using CD14, CD33, KLF4, CD163
Case with non-monocytic differentiation and a bone marrow diagnosis of AML with maturation (FAB-M2) showing positivity for lysozyme (A), myeloperoxidase (B), CD117 (D) and CD33 (H), and negativity for the remaining markers (C CD163 E
Amador-Ortiz C, et al. J Cutan Pathol (2011), in press.
for the remaining markers (C, CD163; E, CD14; F, CD34; G, KLF-4)
Immunohistochemical findings of cutaneous myeloid sarcomas AML (n=44) CMS-
only n=3
MDS n=5
MPN n=5
Total n=57
M0 n=3
M1 n=5
M2 n=7
M4 n=11
M5 n=13
M7 n=1
NS n=4
+/n (%)2/3 (67)
5/5 (100)
6/7 (86)
9/11 (82)
13/13 (100)
1/1 (100)
4/4 (100)
2/3 (66)
5/5 (100)
5/5 (100)
52/57 (91)
CD33 +/n (%)
2/3 (67)
3/5 (60)
5/7 (71)
9/11 (82)
7/13 (54)
0/1 (0)
3/4 (75)
2/3 (66)
1/5 (20)
2/5 (40)
34/57 (60)
MPX +/n (%)
2/3 (67)
3/5 (60)
6/7 (86)
6/11 (55)
4/13 (30)
0/1 (0)
2/4 (50)
2/3 (66)
4/5 (80)
2/5 (40)
31/57 (54)
CD34 +/n (%)
2/3 (67)
2/5 (40)
3/7 (43)
6/11 (55)
4/13 (30)
0/1 (0)
2/4 (50)
0/3 (0)
1/5 (20)
2/5 (40)
22/57 (39)
CD117 +/n (%)
1/3 (33)
3/5 (60)
2/7 (29)
7/11 (64)
3/13 (23)
0/1 (0)
1/4 (25)
1/3 (33)
1/5 (20)
1/5 (20)
20/57 (35)
CD14 +/n (%)
0/3 (0)
0/5 (0)
3/7 (43)
9/11 (82)
10/13 (77)
0/1 (0)
4/4 (100)
2/3 (66)
3/5 (60)
4/5 (80)
34/57 (60)
CD163 1/3 3/5 4/7 7/11 8/13 0/1 3/4 2/3 2/5 2/5 33/57
Regardless of AML subtype, a panel of antibodies that included lysozyme, CD117 and CD33, identified all cases, including those with monocyticdifferentiation.
Amador-Ortiz C, et al. J Cutan Pathol (2011), in press.
CD163 +/n (%)
1/3 (33)
3/5 (60)
4/7 (57)
7/11 (64)
8/13 (62)
0/1 (0)
3/4 (75)
2/3 (66)
2/5 (40)
2/5 (40)
33/57 (58)
KLF-4 +/n (%)
0/3 (0)
0/5 (0)
2/7 (29)
7/11 (64)
5/13 (38)
1/1 (100)
3/4 (75)
2/3 (66)
1/5 (20)
3/5 (75)
23/57 (40)
MDS, myelodysplastic syndrome; MPN, myeloproliferative neoplasm; , lysozyme; MPX, myeloperoxidase; NS, unclassified
Lysozyme was expressed in 52 (91%), CD33 in 34 (60%), myeloperoxidase in 31 (54%), CD34 in 22 (39%) and CD117 in 20 cases (36%).
Monocytic markers in monocytic related AML casesAML
IHC stainsM4+M5 (n=24)+ (%)
M0-M2(n=15)+(%) p Sens. Spec. PPV NPV
CD14 19 (79%) 3 (20%) <0.001 79% 80% 86% 71%
KLF-4 12 (50%) 2 (13%) <0.05 50% 87% 86% 52%
CD163 15 (63%) 8 (53%) NS 63% 47% 65% 44%
CD14 or KLF-4 20 (83%) 4 (27%) <0.001 83% 73% 83% 73%
CD14 or CD163 19 (79%) 8 (53%) NS 79% 47% 70% 58%
KLF-4 or CD163
19 (79%) 8 (53%) NS 79% 47% 70% 58%
CD14 or KLF-4 20 8 (53%) <0 05 83% 47% 71% 64%or CD163 (83%) 8 (53%) <0.05 83% 47% 71% 64%
PPV, positive predictive value; NPV, negative predictive value
In AML cases with monocytic differentiation (M4 and M5), CD14 and KLF-4 were significantly more commonly expressed than in AML cases of granulocytic lineage (M0, M1 and M2) (79% vs. 20%, p<0.001 and 50% vs. 13%, p<0.05, respectively).
The addition of CD163 immunohistochemistry did not enhance the detection of monocytic leukemias, as the combination of CD14 and KLF-4 detected the same proportion of monocytic related AMLs (83%) as when all three monocytic markers were used.
The sensitivity and specificity for both markers (KLF-4 and CD14) combined were 83% and 73%, respectively.Amador-Ortiz C, et al. J Cutan Pathol (2011), in press

16
Flow cytometry vs IHC• For CD33, CD34, CD117 and CD14 there was agreement between the
bone marrow and skin antigen expression in 66%, 60%, 72% and 41% of the cases, respectively.
• In cases in which there was disagreement, the antigen expression was more commonly present in the bone marrow than in the skin for CD33 and CD117 (83 vs. 17% and 71 vs. 29%, respectively).
• Conversely, CD34 and CD14 were more commonly expressed in the skin than in the bone marrow (57 vs. 43% and 94 vs.6%, respectively).
Amador-Ortiz C, et al. J Cutan Pathol (2011), in press
Differential diagnosis
• Commonly influenced by the clinical history, including the patient’s age and history of a possible antecedent or concurrent myeloid neoplasm.
• Ideally: fresh material will be sent for flow cytometric, cytogenetic and molecular studies.
• Clinical suspicion is very important in establishing the correct diagnosis; in one study of 26 cases of myeloid sarcoma, all 14 cases in which there was no antecedent myeloid neoplasm were initially misdiagnosed!
Skin biopsyCD4 and CD56 expression
• CD56 expressed in 5/6 tested cases
• Coexpressed with CD4 in 3 cases: ddx includes blastic plasmacytoid dendritic cell neoplasm (blastic NK-cell lymphoma, agranular CD4+CD56+ hematodermic neoplasm)p )
• All 3 cases also expressed CD68 and lysozyme and had a history of acute myelomonocytic leukemia (2 cases) or relapsed acute myeloid leukemia (1 case) CD4 CD56
CD68 LysozymeHurley MY, et al, submitted

17
Differential diagnosisBlastic plasmacytoid dendritic cell neoplasm
Photos: JA Kozel, MD,Saint Louis University
Blastic plasmacytoid dendritic cell neoplasm
Photo: JA Kozel, MD,Saint Louis University
Blastic plasmacytoid dendriticcell neoplasm
Photo: JA Kozel, MD,Saint Louis University

18
Blastic plasmacytoid dendriticcell neoplasm
CD4CD4
CD56
Photos: JA Kozel, MD,Saint Louis University
Blastic plasmacytoid dendriticcell neoplasm
• Typically evolve to leukemic stage; may present with predominantly cutaneous disease
• Workup should include myeloperoxidase, lysozyme, CD33 (negative); CD43, CD123 (positive)
• Caveats: weak CD123 expression in some AMLs; CD43• Caveats: weak CD123 expression in some AMLs; CD43 is nonspecific
• BPDCN are occasionally CD68+ (dot-like peri-Golgi pattern)
• TCL1 more frequently positive in BPDCN vs. AML• CMML may be associated with PDC proliferations
Histiocytic sarcoma
Frater JL, et al. J Cutan Pathol (2006); 33; 437-442.

19
Histiocytic sarcoma
• Have overlapping histologic, clinical, and immunophenotypic features with AML
• CD163, CD68, lysozyme postive like AMLCD13 CD33 ti• CD13, CD33 negative
Granuloma annulare
“Generalized” – ddxIncludes AML
“Classic” – ddx doesn’t Include AML
Photos: N Burkemper, MD, Saint Louis University
Granuloma annulare
Photos: MY Hurley, MD, Saint Louis University

20
Differential diagnosisMelanoma
S100 antigen, Melan-A (MART-1), HMB-45 and a pan-keratin marker, such as cytokeratin AE1/AE3, are usually sufficient for this distinction. However, rare AMLs have beenrare AMLs have been reported to show scattered dot-like cytokeratinpositivity
AE1/AE3 (+) AML, Torlakovic (2009)
Differential diagnosisExtramedullary hematopoiesis
Extramedullary hematopoiesis: can clinically present as a mass-forming lesion. Multilineage proliferation, or only erythroid if unilineage, and consists predominantly of mature terminally differentiated cells.
It is important to report the finding of EMH, especially when there are atypical cytomorphologic features and aggregates of immature cells, as this finding may precede the eventual development of an acute leukemia.
EMH, spleenO’Malley DP (2007)
Differential diagnosis
• B-NHL: CD20+, CD79a+ (rare AML cases with t(8;21) are weakly CD9a/ Pax5+)
• T-NHL: are CD43+/ CD45+ like AML; some AMLs are CD4+/ CD7+; rare AMLssome AMLs are CD4+/ CD7+; rare AMLs have clonal TCRs
• ALCL: are occasionally CD13/ CD33+; AMLs are rarely CD30+
• Use myeloperoxidase, lysozyme, CD68, ALK to distinguish

21
Differential diagnosisPediatric cases
• Ddx frequently includes Ewing sarcoma, PNET, medulloblastoma, other SRBCTs
• Workup includes CD99Workup includes CD99, MPO, lysozyme, CD43
• Beware: TdT (+) AMLs; CD99(+) AMLs –coexpressd in ~20% of AMLs! AML: TdT(+) (2A and B) and CD99(+)
(2C and D)Kang (2006)
Differential diagnosisRecommended IHC
• CD43, lysozyme – positive in nearly all AMLs
• CD33, CD34, CD117Id tifi l id i i– Identifies myeloid origin
– Excludes NHLs, etc.• Add other IHC as noted if warranted by
clinical history, site
Molecular findings• Trisomy 8, monosomy 7, MLL
rearrangements most common
• Clinical Associations– AML1-ETO (RUNX1-
RUNX1T1) translocationsRUNX1T1) translocations [t(8;21)(q22;q22)]:orbital region in children
– inv(16)(p13.1q22)/t(16;16) (p13.1;q22):gastrontestinaltract or breast in adults
– Trisomy 8: Skin involvement?
Bonig (2002)

22
Molecular findings• Rare cases of BCR-ABL1 positive
myeloid sarcoma have been reported in which there is no systemic disease
• Myeloid and lymphoid neoplasmswith FGFR1 abnormalities/8p11
d h l h dsyndrome can have lymph node involvement by myeloid sarcoma, although involvement by T-lymphoblastic leukemia/lymphoma is more common in this disorder. Bilineal (T/Myeloid) extramedullarydisease is also common in this syndrome with the myeloid component frequently in a perivascular distribution
Vega (2008)
Molecular findings• Myeloid sarcomas associated
with FIP1L1-PDGFRA have also been reported.
• Increased local and peripheral eosinophilseosinophils
• Sensitive to treatment with tyrosine kinase inhibitors, such as imatinib.
Vedy (2010)
Molecular findings• Small studies investigating the prevalence of Fms-like tyrosine kinase -3
(FLT3) and nucleophosmin (NPM1) mutations in myeloid sarcomas have been reported.
• FLT3-ITD (internal tandem duplication) in 3/20 cases with no D835 mutations. Lack of stability of the FLT3 mutation as cases with discrepancies either between the bone marrow and extramedullary site or th i d t ithe primary and recurrent specimens.
• NPM1 mutations have been found in 15% of myeloid sarcomas.• The incidence of other recurring AML-associated mutations such as WT1,
N/K-Ras, CEBPA, IDH1, IDH2 or DNMT3a have not been reported for myeloid sarcoma.

23
Molecular findings
• High-resolution genomic studies are limited for myeloid sarcoma.
• Deeb et al., array CGH of 7 cases: most common werecommon were– Gains involving chromosome 8 or 21q21.1-
q21.3 – Loss of 5q31.2-q31.3 C– Concordant findings between bone marrow
and extramedullary disease.
ConclusionsAreas of Uncertainty
• What are the molecular events that allow some AMLs to have a predilection for extramedullary sites?
• What is the molecular relationship of the extramedullarytumor to the bone marrow disease?
• Does myeloid sarcoma represent clonal evolution of the• Does myeloid sarcoma represent clonal evolution of the original leukemia?
• Why do some AMLs originally manifest as extramedullary disease?
ConclusionsFuture Research
• What is the incidence of the known genetic lesions associated with AML (i.e. IDH1, IDH2, DNMT3a, FLT3, NPM) in a large series of myeloid sarcomas and are these mutations stable when comparing the medullaryand extramedullary tumors?y
• High-resolution genomic studies (including whole genome sequencing) of a series of myeloid sarcomas with paired normal DNA and bone marrow disease to determine the molecular alterations associated with myeloid sarcoma.

24
ConclusionsRecommendations to the pathologist
• When possible, flow cytometric analysis of the specimen should be performed, since the challenges associated with diagnosis of myeloid sarcoma are compounded by the limitations of immunohistochemicalanalysis for AMLs with monocytic differentiation.y y
• A concurrent bone marrow biopsy is recommended to compare the immunophenotypic and morphologic features and to determine the extent of disease.
• Prudent use of immunohistochemistry is important to minimize the risk of misdiagnosis: e.g. CD7, CD4/ CD56
ConclusionsRecommendations to the pathologist
• Cytogenetic abnormalities are identified in a large percentage of tested cases. Identification of an AML-associated abnormality is helpful in arriving at the correct diagnosis.g
• Correlation with past medical history is particularly important, since many patients have a concurrent or antecedent AML, simplifying the diagnosis and analysis of extramedullary disease.
Atlas of Genetics and Cytogeneticsin Oncology and Haematology
AcknowledgementsWashington University Department of Pathology and
ImmunologyJM Klco, MD, PhDC Amador-Ortiz, MDS i t L i U i it D t t f D t lSaint Louis University Department of DermatologyMY Hurley, MDS Frisch, MDN Burkemper, MDJA Kozel, MDSaint Louis University School of MedicineGK Ghahramani

25
??Questions??

Flow cytometry in acute and chronic myeloid neoplasms
Hora%u Olteanu, MD, PhD
Assistant Professor of Pathology Director, Flow Cytometry Laboratory
Medical College of Wisconsin

Disclosure informa%on
• I do not have any relevant financial rela%onships with any commercial interests.

Overview
• Flow cytometric immunophenotyping of myeloblasts
• Chronic myeloid neoplasms – MPN diagnosis
• Acute myeloid leukemias – diagnosis
• Acute myeloid leukemias – MRD analysis

Overview
• Flow cytometric immunophenotyping of myeloblasts
• Chronic myeloid neoplasms – MPN diagnosis • Acute myeloid leukemias – diagnosis • Acute myeloid leukemias – MRD analysis
• Ra%onale • Technical aspects

Overview
• Flow cytometric immunophenotyping of myeloblasts
• Chronic myeloid neoplasms – MPN diagnosis
• Acute myeloid leukemias – diagnosis
• Acute myeloid leukemias – MRD analysis

FC in MPN diagnosis -‐ Ra%onale
• Integrated diagnos%c approach – Morphology
– Immunophenotype – Cytogene%cs – Molecular analysis
– Clinical data

Technical aspects in FC of MPN
• Specificity of IP altera%ons in myeloblasts • Heterogeneity of the CD45/SSC “blast gate”

Immunophenotype of normal blasts
CD7(-‐) CD11b(-‐) CD13(v +) CD14(-‐) CD15(predom -‐) CD16(-‐) CD33(+) CD34(+) CD36(-‐) CD38(mod br +) CD45(mod +) CD56(-‐) CD64(-‐) CD117(+) HLA-‐DR(mod br +)

ANNUAL MEETING ABSTRACTS 301ADesign:
presence of genetic aberrations affecting BCL11b in situ
Results:
in TCR / / and BCL11b loci. Genomic gain in BCL11b
of an underlying genetic aberration.Conclusions:
1345 A Dissection of the CD45/Side Scatter (SS) Blast Gate in Non-Acute Myeloid Disorders and Non-Neoplastic Bone MarrowsAM Harrington, H Olteanu, SH Kroft.WI.Background:
expression. We thus evaluated the contents of the CD45/SS BG in a variety of bone
Design:
based on conventions derived from standard FC literature.Results:
Conclusions:
the BG in CMMLs and MPNs. Our data highlight pitfalls in using a traditional BG
robust methods.
1346 Incidental, Immunophenotypically Aberrant Cytotoxic T-Cell Clones in Patients with Other Hematologic MalignanciesAM Harrington, H Olteanu, SH Kroft.WI.Background: Clonal or oligoclonal expansions of immunophenotypically normal
hematologic malignancies.Design:
population.Results:
L (median
Conclusions: The abnormal cytotoxic T-cell populations in this series are distinct from
they did not satisfy numeric criteria for LGLL. Presumed to originate as an immune
1347 The Nature and Frequency of Atypical Phenotypic Features Detected by Flow Cytometry in CLL: Correlation with Prognostic Markers CD38 and ZAP70NM Hassanein, E Kulbacki, E Wang, JB Weinberg, AS Lagoo. Duke University Medical
Background: Prognostic markers in chronic lymphocytic leukemia (CLL) have garnered
“atypical CLL” cases is unclear.Design:
Laboratory at our Institution.Results:
Conclusions:
CLL prognostically.
1348 An Algorithm for the Efficient Flow Cytometric Diagnosis of Acute LeukemiaN Haycocks, L Lawrence, JW Cain, XF Zhao.
Background:
of acute myeloid leukemia (AML) from acute lymphoblastic leukemia (ALL). In an
effectively triaging specimens to select more tailored panels could reduce unnecessary
limited immunological markers.Design:
tabulated for analysis.Results:
CD45/SSC 1) AML detailed AML studies; 2) ALL detailed ALL studies; 3) Indeterminate detailed ALL
labor) for analysis of the 104 leukemias.
Mod Pathol (2010) 23;S1: 301A

CD45/SSC “Blast gate”
• Most common approach for defining blasts (Stelzer, et al Ann N Y Acad Sci, 1993) (Borowitz, et al Am J Clin Pathol, 1993 )
• Imprecise, due to presence of other contamina%ng popula%ons (Harrington, et al Am J Clin Pathol, 2010 )
• “Cluster analysis”: flexible, itera%ve analy%c strategy; more robust (Krof and Karandikar Flow Cytometry in Clinical Diagnosis, 2007 )

Tradi%onal ga%ng vs. cluster analysis
• Tradi%onal ga%ng: based on rela%vely rigid quad marker applica%on, dictated by pre-‐supposed an%gen expression / light scaher characteris%cs of a popula%on of interest
• Cluster analysis: detec%on of a “cluster” (popula%on) residing in an abnormal loca%on of the mul%dimensional flow space, based on global paherns of aberrant an%gen expression

Granulocytes, monocytes, lymphocytes, erythroids, basophils, blasts, hematogones.
(Harrington, et al Mod Pathol, 2010)

Granulocytes, monocytes, lymphocytes, erythroids, basophils, blasts, hematogones.
(Harrington, et al Mod Pathol, 2010)
~20%

“Blast gate” composi%on
(Harrington, et al Mod Pathol, 2010)

Granulocytes, monocytes, lymphocytes, basophils, blasts, hematogones.
(Harrington, et al Am J Clin Pathol, 2010)

Am J Clin Pathol 2010;134:749-761 749749 DOI: 10.1309/AJCPFNF5MN1GDWKU 749
© American Society for Clinical Pathology
Hematopathology / B!"#$ A!$%&"$'()# ') N()"*+$% M,%!('- D'#(&-%&#
The Specificity of Immunophenotypic Alterations in Blasts in Nonacute Myeloid Disorders
Alexandra Harrington, MD, Horatiu Olteanu, MD, PhD, and Steven Kroft, MD
Key Words: Blasts; Immunophenotype; Myelodysplastic syndromes; Myeloproliferative neoplasms; Flow cytometry
DOI: 10.1309/AJCPFNF5MN1GDWKU
A b s t r a c tData regarding flow cytometry (FC) in nonacute
myeloid disorders is confounded by variable gating strategies and controls limited to normal bone marrow (BM) samples. Blasts in diagnostic BM samples of myelodysplastic syndromes (MDSs), myeloproliferative neoplasms (MPNs), and chronic myelomonocytic leukemias (CMMLs) were compared with 20 nonneoplastic cytopenias/cytoses (CCs) and negative staging BM samples using 4-color FC. Blasts in 10 of 20 CCs showed immunophenotypic differences vs control samples. Immunophenotypic alterations were identified in 18 of 21 MDSs, 11 of 14 MPNs, and 7 of 7 CMMLs vs control samples and 13 (62%) of 21 MDSs, 7 (50%) of 14 MPNs, and 3 (43%) of 7 CMMLs vs CCs. Neoplastic-specific blast immunophenotypic changes included expression of CD7, CD11b, CD15, CD36, and CD56; CD34 overexpression; HLA-DR variability; lack of CD13 and CD33; underexpression of CD13, CD33, CD45, and HLA-DR; and partial loss of CD13, CD33, CD38, and CD117. In all cases, blasts were CD34+. Several blast immunophenotypic alterations are shared in neoplastic and nonneoplastic BM samples. Approximately 40% to 60% of neoplastic BM samples exhibited aberrancies not seen in reactive BM samples.
There is a large and complex literature describing the immunophenotypic features of myelodysplastic syndromes (MDSs) and to a considerably lesser extent myeloproliferative neoplasms (MPNs).1-13 These studies have focused on aber-rant antigen expression and maturation patterns of various cell populations, primarily granulocytes, monocytes, and blasts. For MDSs, scoring systems have been developed based on these descriptions in attempts to aid in diagnosis and guide therapeutic options for patients.1-8 Studies that have focused on blast populations2-8 have described various abnormalities, including decreased CD45 expression; underexpression and overexpression of CD13, CD33, CD38, and HLA-DR; lack of CD34; aberrant expression of CD2, CD10, CD11b, and CD15; and expression of the lymphoid-associated antigens CD2, CD5, CD7, CD19, and CD56. However, the specif-ics of these abnormalities are not always well described. In addition, many of these studies are confounded by variable gating strategies, suboptimal control groups, and skewed and/or poorly characterized patient cohorts.
CD45/side scatter (SS) gating, the most common approach to blast isolation,14,15 is imprecise because many other cell populations contaminate this gate, including mature and immature monocytes, basophils, granulocytes, hematogones, lymphocytes, and erythroid precursors !Image 1!.16 In fact, blasts in such a gate frequently represent only a minority of events.17 Using such a gating strategy may lead to inac-curate reporting of antigen expression patterns on blasts. For example, failure to identify basophils contaminating this gate may result in erroneous identification of CD11b expression on blasts. Flexible, iterative analysis strategies that seek to discriminate distinct population clusters in multidimensional flow cytometry space based on differential patterns of antigen
Am J Clin Pathol 2010;134:749-761 749749 DOI: 10.1309/AJCPFNF5MN1GDWKU 749
© American Society for Clinical Pathology
Hematopathology / B!"#$ A!$%&"$'()# ') N()"*+$% M,%!('- D'#(&-%&#
The Specificity of Immunophenotypic Alterations in Blasts in Nonacute Myeloid Disorders
Alexandra Harrington, MD, Horatiu Olteanu, MD, PhD, and Steven Kroft, MD
Key Words: Blasts; Immunophenotype; Myelodysplastic syndromes; Myeloproliferative neoplasms; Flow cytometry
DOI: 10.1309/AJCPFNF5MN1GDWKU
A b s t r a c tData regarding flow cytometry (FC) in nonacute
myeloid disorders is confounded by variable gating strategies and controls limited to normal bone marrow (BM) samples. Blasts in diagnostic BM samples of myelodysplastic syndromes (MDSs), myeloproliferative neoplasms (MPNs), and chronic myelomonocytic leukemias (CMMLs) were compared with 20 nonneoplastic cytopenias/cytoses (CCs) and negative staging BM samples using 4-color FC. Blasts in 10 of 20 CCs showed immunophenotypic differences vs control samples. Immunophenotypic alterations were identified in 18 of 21 MDSs, 11 of 14 MPNs, and 7 of 7 CMMLs vs control samples and 13 (62%) of 21 MDSs, 7 (50%) of 14 MPNs, and 3 (43%) of 7 CMMLs vs CCs. Neoplastic-specific blast immunophenotypic changes included expression of CD7, CD11b, CD15, CD36, and CD56; CD34 overexpression; HLA-DR variability; lack of CD13 and CD33; underexpression of CD13, CD33, CD45, and HLA-DR; and partial loss of CD13, CD33, CD38, and CD117. In all cases, blasts were CD34+. Several blast immunophenotypic alterations are shared in neoplastic and nonneoplastic BM samples. Approximately 40% to 60% of neoplastic BM samples exhibited aberrancies not seen in reactive BM samples.
There is a large and complex literature describing the immunophenotypic features of myelodysplastic syndromes (MDSs) and to a considerably lesser extent myeloproliferative neoplasms (MPNs).1-13 These studies have focused on aber-rant antigen expression and maturation patterns of various cell populations, primarily granulocytes, monocytes, and blasts. For MDSs, scoring systems have been developed based on these descriptions in attempts to aid in diagnosis and guide therapeutic options for patients.1-8 Studies that have focused on blast populations2-8 have described various abnormalities, including decreased CD45 expression; underexpression and overexpression of CD13, CD33, CD38, and HLA-DR; lack of CD34; aberrant expression of CD2, CD10, CD11b, and CD15; and expression of the lymphoid-associated antigens CD2, CD5, CD7, CD19, and CD56. However, the specif-ics of these abnormalities are not always well described. In addition, many of these studies are confounded by variable gating strategies, suboptimal control groups, and skewed and/or poorly characterized patient cohorts.
CD45/side scatter (SS) gating, the most common approach to blast isolation,14,15 is imprecise because many other cell populations contaminate this gate, including mature and immature monocytes, basophils, granulocytes, hematogones, lymphocytes, and erythroid precursors !Image 1!.16 In fact, blasts in such a gate frequently represent only a minority of events.17 Using such a gating strategy may lead to inac-curate reporting of antigen expression patterns on blasts. For example, failure to identify basophils contaminating this gate may result in erroneous identification of CD11b expression on blasts. Flexible, iterative analysis strategies that seek to discriminate distinct population clusters in multidimensional flow cytometry space based on differential patterns of antigen

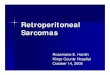
Percentage of IP changes in cytopenias/cytoses (CCs), MDSs, MPNs, and CMMLs.
(Harrington, et al Am J Clin Pathol, 2010)

Control samples (A, D, G, and J) and cytopenias/cytoses (B, E, H, and K)
(Harrington, et al Am J Clin Pathol, 2010)
Variable CD33 Bright CD13 Bright CD117 Variable CD38

Blast IP changes Shared with reacTve BMs
• CD13(bright +) • CD33(variably +) • CD34(slightly bright +) • CD38(variably +) • CD117(bright/dim/variably +)
• HLA-‐DR(bright +)
Neoplasia-‐specific
• CD7(par%al +) • CD11b(bright +) • CD13(par%al + or -‐) • CD15(par%al +) • CD33(par%al + or -‐) • CD34(bright/variably +) • CD36(par%al +) • CD38(par%al +) • CD45(dim +) • CD56(par%al +) • CD117(par%al +) • HLA-‐DR(dim/variably +) (Harrington, et al Am J Clin Pathol, 2010)

Neoplasia-‐specific IP altera%ons in MPNs
• Expression of CD7, CD36, CD56
• Variable expression of HLA-‐DR
• Loss of CD13 • Underexpression of CD45 and HLA-‐DR
• Par%al loss of CD13, CD33, and CD117
(Harrington, et al Am J Clin Pathol, 2010)

Abnormal blast IP in non-‐CML MPNs
(Kussick and Wood Am J Clin Pathol, 2003)
PV
MPN, NOS

Overview
• Flow cytometric immunophenotyping of myeloblasts
• Chronic myeloid neoplasms – MPN diagnosis
• Acute myeloid leukemias – diagnosis
• Acute myeloid leukemias – MRD analysis

Role of FC in diagnosing AML
• Allows dis%nc%on between AML and ALL • Certain immunophenotypes correlate with the presence of recurrent cytogene%c or molecular abnormali%es
• Establishes an immunophenotypic fingerprint for MRD analysis at follow-‐up

AML with minimal differen%a%on
MPO

AML with minimal differen%a%on

AML with t(8;21)(q22;q22)

AML with t(8;21)(q22;q22)

AML with t(15;17)(q22;q12)

AML with t(15;17)(q22;q12)

AML with “cup-‐like” inclusions

AML with “cup-‐like” inclusions NPM1 mut(+)

AML with t(1;22)(p13;q13)

Overview
• Flow cytometric immunophenotyping of myeloblasts
• Chronic myeloid neoplasms – MPN diagnosis
• Acute myeloid leukemias – diagnosis
• Acute myeloid leukemias – MRD analysis

MRD detec%on in AML -‐ Ra%onale
• Standard of care: induc%on chemotherapy + consolida%on (chemotherapy and/or SCT) (Dohner, et al Blood, 2010)
• Pa%ents with AML show heterogeneous response to therapy, ranging from cure to refractory disease
• CR is formally defined based on BM morphology (<5% blasts) – low sensi%vity (Cheson, et al J Clin Oncol, 2003)

MRD detec%on in AML -‐ Ra%onale
• Risk stra%fica%on includes cytogene%c and molecular abnormali%es (2008 WHO classifica%on)
• Other risk factors: – Drug efflux transporters
– Pharmacologic resistance – BM environment
(Ossenkoppele, et al Br J Haematol, 2011)

MRD detec%on in AML -‐ Ra%onale
• Prognosis in individual pa%ents cannot be es%mated accurately – Very good risk pa%ents may relapse – Very poor risk pa%ents may be cured
• MRD analysis may poten%ally guide treatment – More chemotherapy for high risk pa%ents – Less chemotherapy for low risk pa%ents
• MRD analysis may offer a short-‐term surrogate endpoint for assessing new therapies

Toward Optimization of Postremission Therapy forResidual Disease–Positive Patients With AcuteMyeloid LeukemiaLuca Maurillo, Francesco Buccisano, Maria Ilaria Del Principe, Giovanni Del Poeta, Alessandra Spagnoli,Paola Panetta, Emanuele Ammatuna, Benedetta Neri, Licia Ottaviani, Chiara Sarlo, Daniela Venditti,Micol Quaresima, Raffaella Cerretti, Manuela Rizzo, Paolo de Fabritiis, Francesco Lo Coco, William Arcese,Sergio Amadori, and Adriano Venditti
From the Hematology, Policlinico TorVergata and Ospedale S. Eugenio,Rome, Italy.
Submitted January 3, 2008; acceptedMay 14, 2008; published online aheadof print at www.jco.org on July 7,2008.
Supported in part by Ministero dellaSalute (Ricerca Finalizzata Istituto diRicovero e Cura a Carattere Scientificoand “Alleanza contro il Cancro”), Rome,Italy.
Presented in part at the 48th AnnualMeeting of the American Society ofHematology, December 9-12, 2006,Orlando, FL.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Corresponding author: Adriano Venditti,MD, Cattedra di Ematologia–UniversitaTor Vergata, Viale Oxford 81, 00133Roma, Italia; e-mail: [email protected].
© 2008 by American Society of ClinicalOncology
0732-183X/08/2630-4944/$20.00
DOI: 10.1200/JCO.2007.15.9814
A B S T R A C T
PurposeDespite the identification of several baseline prognostic indicators, the outcome of patients withacute myeloid leukemia (AML) is generally heterogeneous. The effects of autologous (AuSCT) orallogeneic stem-cell transplantation (SCT) are still under evaluation. Minimal residual disease(MRD) states may be essential for assigning patients to therapy-dependent risk categories.
Patients and MethodsBy multiparametric flow cytometry, we assessed the levels of MRD in 142 patients with AML whoachieved complete remission after intensive chemotherapy.
ResultsA level of 3.5 ! 10"4 residual leukemia cells (RLCs) after consolidation therapy was establishedto identify MRD-negative and MRD-positive cases, with 5-year relapse-free survival (RFS) rates of60% and 16%, respectively (P # .0001) and overall survival (OS) rates of 62% and 23%,respectively (P $ .0001). Of patients (n $ 77) who underwent a transplantation procedure (56AuSCT and 21 SCT procedures); 42 patients (55%) were MRD positive (28 patients whounderwent AuSCT and 14 patients who underwent SCT) and 35 patients (45%) were MRDnegative (28 patients who underwent AuSCT and seven who underwent SCT). MRD-negativepatients had a favorable prognosis, with only eight (22%) of 35 patients experiencing relapse,whereas 29 (69%) of 42 MRD-positive patients experienced relapse (P # .0001). In this high-riskgroup of 42 patients, we observed that 23 (82%) of 28 of those who underwent AuSCT experiencedrelapse, whereas six (43%) of 14 who underwent SCT experienced relapse (P $ .014). Patients whounderwent SCT also had a higher likelihood of RFS (47% v 14%).
ConclusionA threshold of 3.5 ! 10"4 RLCs postconsolidation is critical for predicting disease outcome.MRD-negative patients have a good outcome regardless of the type of transplant they receive. Inthe MRD-positive group, AuSCT does not improve prognosis and SCT represents the pri-mary option.
J Clin Oncol 26:4944-4951. © 2008 by American Society of Clinical Oncology
INTRODUCTION
The use of modern intensive induction chemother-apies leads to complete remission (CR) in 60% to80% of adult patients with acute myeloid leukemia(AML).1-6 However, without additional chemother-apies, including intensive consolidation,4,5,7 less in-tensive maintenance,8,9 autologous (AuSCT), orallogeneic stem-cell transplantation (SCT),1,2,4
nearly all cases of AML will eventually relapse.The goal of these additional treatments is to erad-icate leukemia cells surviving the cytotoxic effectsof the therapy that are undetectable by conven-
tional light microscopy surveys. These cells, calledminimal residual disease (MRD) units, are re-sponsible for recurrence.
Although a number of baseline prognostic fac-tors (including age, performance status, AML oc-curring as secondary disease, and WBC count) havebeen identified, the prognosis of patients withinrespective subgroups defined by these parametersis still quite heterogeneous. Acquired clonal chro-mosomal abnormalities are considered the mostrelevant prognosticators in patients with AML,who are then stratified by cytogenetics into good-,intermediate-, and high-risk AML.10-12 Using
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
VOLUME 26 ! NUMBER 30 ! OCTOBER 20 2008
4944 © 2008 by American Society of Clinical Oncology
from 192.227.62.1Information downloaded from jco.ascopubs.org and provided by at MEDICAL COLLEGE OF WISCONSI on August 18, 2011
Copyright © 2008 American Society of Clinical Oncology. All rights reserved.

(Maurillo, et al J Clin Oncol, 2008)

(Maurillo, et al J Clin Oncol, 2008)

Articles
www.thelancet.com/oncology Vol 11 June 2010 543
Lancet Oncol 2010; 11: 543–52
Published OnlineMay 6, 2010DOI:10.1016/S1470-2045(10)70090-5
See Refl ection and Reaction page 502
St Jude Children’s Research Hospital and the University of Tennessee Health Science Center, Memphis, TN, USA (Prof J E Rubnitz MD, H Inaba MD, Prof R C Ribeiro MD, S Pounds PhD, B I Razzouk MD, X Cao PhD, Prof S C Raimondi PhD, M Onciu MD, E Coustan-Smith MS, Prof J R Downing MD, Prof W Leung MD, Prof C-H Pui MD, Prof D Campana MD); Lucile Packard Children’s Hospital and Stanford Cancer Center, Palo Alto, CA, USA (Prof G Dahl MD, N J Lacayo MD); Cook Children’s Medical Center, Fort Worth, TX, USA (Prof W P Bowman MD); Children’s Hospital of Michigan, Detroit, MI, USA (J Taub MD); Fred Hutchinson Cancer Research Center, Seattle, WA, USA (S Meshinchi MD); Dana-Farber Cancer Institute, Boston, MA, USA (B Degar MD); and Texas Children’s Cancer Center, Houston, TX, USA (G Airewele MD)
Correspondence to:Prof Je! rey E Rubnitz, Department of Oncology, St Jude Children’s Research Hospital, 262 Danny Thomas Place, Memphis, TN 38105-2794, USAje! [email protected]
Minimal residual disease-directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trialJe! rey E Rubnitz, Hiroto Inaba, Gary Dahl, Raul C Ribeiro, W Paul Bowman, Je! rey Taub, Stanley Pounds, Bassem I Razzouk, Norman J Lacayo, Xueyuan Cao, Soheil Meshinchi, Barbara Degar, Gladstone Airewele, Susana C Raimondi, Mihaela Onciu, Elaine Coustan-Smith, James R Downing, Wing Leung, Ching-Hon Pui, Dario Campana
SummaryBackground We sought to improve outcome in patients with childhood acute myeloid leukaemia (AML) by applying risk-directed therapy that was based on genetic abnormalities of the leukaemic cells and measurements of minimal residual disease (MRD) done by fl ow cytometry during treatment.
Methods From Oct 13, 2002, to June 19, 2008, 232 patients with de-novo AML (n=206), therapy-related or myelodysplasia-related AML (n=12), or mixed-lineage leukaemia (n=14) were enrolled at eight centres. 230 patients were assigned by block, non-blinded randomisation, stratifi ed by cytogenetic or morphological subtype, to high-dose (18 g/m!, n=113) or low-dose (2 g/m!, n=117) cytarabine given with daunorubicin and etoposide (ADE; induction 1). The primary aim of the study was to compare the incidence of MRD positivity of the high-dose group and the low-dose group at day 22 of induction 1. Induction 2 consisted of ADE with or without gemtuzumab ozogamicin (GO anti-CD33 monoclonal antibody); consolidation therapy included three additional courses of chemotherapy or haematopoietic stem-cell transplantation (HSCT). Levels of MRD were used to allocate GO and to determine the timing of induction 2. Both MRD and genetic abnormalities at diagnosis were used to determine the fi nal risk classifi cation. Low-risk patients (n=68) received fi ve courses of chemotherapy, whereas high-risk patients (n=79), and standard-risk patients (n=69) with matched sibling donors, were eligible for HSCT (done for 48 high-risk and eight standard-risk patients). All 230 randomised patients were analysed for the primary endpoint. Other analyses were limited to the 216 patients with AML, excluding those with mixed-lineage leukaemia. This trial is closed to accrual and is registered with ClinicalTrials.gov, number NCT00136084.
Findings Complete remission was achieved in 80% (173 of 216 patients) after induction 1 and 94% (203 of 216) after induction 2. Induction failures included two deaths from toxic e! ects and ten cases of resistant leukaemia. The introduction of high-dose versus low-dose cytarabine did not signifi cantly lower the rate of MRD-positivity after induction 1 (34% vs 42%, p=0·17). The 6-month cumulative incidence of grade 3 or higher infection was 79·3% (SE 4·0) for patients in the high-dose group and 75·5% (4·2) for the low-dose group. 3-year event-free survival and overall survival were 63·0% (SE 4·1) and 71·1% (3·8), respectively. 80% (155 of 193) of patients achieved MRD of less than 0·1% after induction 2, and the cumulative incidence of relapse for this group was 17% (SE 3). MRD of 1% or higher after induction 1 was the only signifi cant independent adverse prognostic factor for both event-free (hazard ratio 2·41, 95% CI 1·36–4·26; p=0·003) and overall survival (2·11, 1·09–4·11; p=0·028).
Interpretation Our fi ndings suggest that the use of targeted chemotherapy and HSCT, in the context of a comprehensive risk-stratifi cation strategy based on genetic features and MRD fi ndings, can improve outcome in patients with childhood AML.
Funding National Institutes of Health and American Lebanese Syrian Associated Charities (ALSAC).
IntroductionWith improvements in risk-directed therapy and supportive care, event-free survival (EFS) for children with acute lymphoblastic leukaemia (ALL) now approaches 90%.1 By contrast, EFS for children with acute myeloid leukaemia (AML) ranges from 49% to 62%.2–4 Improving clinical results in AML requires not only the development of new drugs and better supportive care, but also a more precise application of risk-directed therapy.
It is well known that genetic abnormalities of leukaemic blasts are associated with clinical outcome in patients with AML.5 Methods for detecting minimal residual
disease (MRD) allow much more precise assessments of early reduction in leukaemic burden than were possible in the past, and the results of these tests are powerful and independent predictors of relapse in adults and children with AML.6–10 We therefore designed a multicentre study, AML02, that relied on presenting genetic features and sequential assessment of MRD to establish the fi nal risk assignment and treatment of children with AML. Additionally, because earlier studies suggested that higher doses of cytarabine during induction therapy might be associated with lower relapse rates,11–13 we investigated whether high-dose cytarabine (18 g/m!) would lead to better results than a lower dose (2 g/m!).

• 232 pa%ents • MRD levels used to allocate gemtuzumab and to determine
%ming of 2nd induc%on
• MRD and cytogene%c abnormali%es were combined to determine final risk stra%fica%on
(Rubnitz, et al Lancet Oncol, 2010)

InducTon 1
InducTon 2

Event-‐free survival Overall survival
HR (95% CI) p value HR (95% CI) p value
Treatment group 0·∙83 (0·∙50–1·∙39) 0·∙483 0·∙83 (0·∙46–1·∙53) 0·∙554
Induc%on 1 MRD ≥1% 2·∙41 (1·∙36–4·∙26) 0·∙003 2·∙11 (1·∙09–4·∙11) 0·∙028
CBF 0·∙32 (0·∙13–0·∙79) 0·∙013 0·∙37 (0·∙12–1·∙12) 0·∙079
Age at diagnosis* 1·∙65 (0·∙92–2·∙95) 0·∙095 2·∙55 (1·∙23–5·∙27) 0·∙012
Other 11q23 2·∙05 (0·∙96–4·∙34) 0·∙062 3·∙29 (1·∙34–8·∙04) 0·∙009
M7 without t(1;22) 2·∙17 (0·∙86–5·∙45) 0·∙099 5·∙64 (1·∙99–16·∙0) 0·∙001
FLT3-‐ITD 1·∙64 (0·∙82–3·∙27) 0·∙163 1·∙93 (0·∙84–4·∙44) 0·∙123
(Rubnitz, et al Lancet Oncol, 2010 )

Significance of MRD in AML
• “MRD detec%on methods… should be part of the rou%ne management of AML pa%ents to guide therapy.”
(Ossenkoppele, et al Br J Haematol, 2011) (Bene and Kaeda Haematologica, 2009) (Grimwade, et al Curr Opin Oncol, 2010) (van Rhenen, et al Curr Hematol Malig Rep, 2007) (Kern, et al Best Pract Res Clin Haematol, 2010)

Techniques for MRD detec%on in AML
• PCR and FC • Real-‐%me quan%ta%ve RT-‐PCR (RQ-‐PCR) has clinical u%lity in direc%ng treatment in APL (Grimwade, et al J Clin Oncol, 2009)
• FC is useful for MRD detec%on and quan%fica%on, and can provide prognos%c informa%on (Maurillo, et al J Clin Oncol, 2008) (Kern, et al Cancer, 2008) (Buccisano, et al Curr Opin Oncol, 2009)

MRD analysis by RQ-‐PCR
• Advantages: – Very sensi%ve (10-‐6) – Quan%ta%ve
• Disadvantages: • Applicable to a limited number of molecular targets
– PML-‐RARA – CBF leukemias
– NPM1
(Perea, et al Leukemia, 2006) (Schnihger, et al Blood, 2009)

MRD analysis by FC
• Advantages: – Sensi%ve (10-‐4) – Rapid – Quan%ta%ve – Applicable in ≥95% pa%ents
• Disadvantages: – Lacks standardiza%on – Immunophenotypic stability of LAIP

Technical aspects in FC of AML
• MRD analysis – How to gate? – Beware of blast autofluorescence – What an%body combina%ons to use? – How many colors (4, 6, 8)?
– What MRD cut-‐off values to use / how many events are required?
– Immunophenotypic shifs

Leukemia-‐associated immunophenotype
• Sum of aberrant an%gen expression on blasts • Type of IP aberrancies: – Asynchronous an%gen expression – Cross-‐lineage an%gen expression – An%gen over-‐ / underexpression – Abnormal forward / side scaher proper%es

Asynchronous an%gen expression
CD34 and CD15 coexpression

Asynchronous an%gen expression
CD34 and CD15 coexpression

Cross-‐lineage an%gen expression
Par%al CD7 and CD56 expression

Cross-‐lineage an%gen expression
Par%al CD2 expression

Cross-‐lineage an%gen expression
Dim CD19 and par%al CD56 expression

An%gen over-‐ / underexpression
Bright CD34, CD33 and CD117 Dim HLA-‐DR

An%gen over-‐ / underexpression
Par%al CD34, CD117

Abnormal FSC / SSC
Increased side scaher

Abnormal FSC / SSC
Increased side scaher

Technical aspects: How to gate?
• CD45/side scaher (“blast gate”) • Back ga%ng with CD34 and/or CD117 for refinement of “blast gate”
• “Cluster analysis” is more powerful, but poten%ally %me consuming

Blasts ante portas

Technical aspects: Autofluorescence
• Blasts tend to have high autofluorescence • Include appropriate nega%ve isotype control an%body tube

CD10(+) vs. CD10(-‐)

CD10(+) vs. CD10(-‐)

Technical aspects: An%bodies
• LAIP found in 75-‐100% of cases; depends on: – Number of an%bodies
– Comparison with “normal”/reac%ve BM blasts – Individual laboratory thresholds for LAIP defini%on
• 5-‐color FC shows increased sensi%vity vs. 4-‐color FC
• Suggested an%body panels are highly variable (Campana and Coustan-‐Smith Cytometry, 1999) (Al-‐Mawali, et al Am J Clin Pathol, 2009) (Al-‐Mawali, et al Am J Clin Pathol, 2008)

LAIP type and frequencies
Am J Clin Pathol 2009;131:16-26 1919 DOI: 10.1309/AJCP5TSD3DZXFLCX 19
© American Society for Clinical Pathology
Hematopathology / REVIEW ARTICLE
100 101 102
CD117+CD15+
24%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD34+CD7+
32%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.12%
G2G1
G4G3
CD7 FITC
BM: AML at Diagnosis After Induction After Consolidation I After Consolidation II Follow-up
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.15%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.13%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.09%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD117+CD15+
0.78%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
0.42%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
0.64%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
52%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
24%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD34+CD7+
32%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.12%
G2G1
G4G3
CD7 FITC
BM: AML at Diagnosis After Induction After Consolidation I After Consolidation II Follow-up
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.15%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.13%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD34+CD7+
0.09%
G2G1
G4G3
CD7 FITC
CD
34 P
E
103
100
101
102
103
100 101 102
CD117+CD15+
0.78%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
0.42%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
0.64%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
100 101 102
CD117+CD15+
52%
C2C1
C4C3
CD15 FITC
CD
117
PE
103
100
101
102
103
A
B
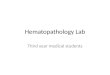
Image 1 Detection of minimal residual disease (MRD) in consecutive bone marrow (BM) samples from a patient with relapse (A) and a patient still in remission (B). Cells from acute myeloid leukemia (AML) at diagnosis and follow-up BM samples are stained with a combination of monoclonal antibodies, which identifies a leukemia-associated phenotype (LAP). The gating strategy starts by defining the WBC compartment characterized by CD45 expression and SS Log. A, On these selected cells, the cell population with a primitive marker expression, in this case CD117, and low side scatter (SSC) is subsequently gated for detection of the cells with aberrant phenotypes. The patient experienced relapse within 6 months after achieving complete remission (CR). The aberrant phenotype was CD117+/CD15+ expression on the CD34+/CD117+ cells. The MRD percentages were 0.78%, 0.42%, and 0.64% after induction and consolidation I and consolidation II chemotherapy, respectively. The dot plot at the extreme right shows relapsed material with LAP expression similar to that at diagnosis. B, On these selected cells, the cell population with a primitive marker expression, in this case CD34, and low SSC is subsequently gated for detection of the cells with aberrant phenotypes. The patient was still in CR after 24 months. The LAP includes CD34+/CD7+ expression. The MRD percentages were 0.12%, 0.15%, 0.13%, and 0.09% after induction, consolidation I and consolidation II chemotherapy, and at follow-up, respectively. FITC, fluorescein isothiocyanate; PE, phycoerythrin; SS, side scatter.
Table 2Various LAPs and Their Frequencies
Asynchronous Lineage Antigen Aberrant Absence of No. of MFC LAPs Antigen Infidelity Overexpression Light-Scatter Lineage-Specific Report Colors Used (%) Expression (%)* (%)* (%)* Properties (%)* Antigens (%)*
Al-Mawali et al14 3 64 52 35 ND ND 35Al-Mawali et al11 5 94 73† 20† ND ND 7†
Babusíková et al‡ 2 56 13 42 1 NR NRBahia et al20 3 89 82.4 34.3 NR NR NRDrach et al21 2 51 13 32 NR NR 16Macedo et al7 2 and 3 73 62.5 37.5 17.5 32.5 NRReading et al9 2 and 3 85 70 54 NR NR NRLaane et al‡ 3 93.5 83 55 16 NR 9San Miguel et al17 3 NR 78 29 21 17 NRFeller et al22 4 60 55 45 2.5 NR NRVoskova et al23 2 82 50 64.3 14.3 50 27.8Kern et al10 3 100 14.2† 26.4† 32.9† NR 26.4†
AML, acute myeloid leukemia; LAPs, leukemia-associated phenotypes; MFC, multiparameter flow cytometry; ND, not done; NR, not reported.* Percentage of total AML cases unless otherwise indicated.† Percentage of total number of LAPs.‡ Babusíková O, Glasová M, Koníková E, et al. Leukemia-associated phenotypes: their characteristics and incidence in acute leukemia. Neoplasma. 1996;43:367-372. Laane E,
Derolf AR, Björklund E, et al. The effect of allogeneic stem cell transplantation on outcome in younger acute myeloid leukemia patients with minimal residual disease detected by flow cytometry at the end of post-remission chemotherapy. Haematologica. 2006;91:833-836.
(Al-‐Mawali, et al Am J Clin Pathol, 2009)

934 Am J Clin Pathol 2008;129:934-945934 DOI: 10.1309/FY0UMAMM91VPMR2W
© American Society for Clinical Pathology
Hematopathology / LEUKEMIA-ASSOCIATED PHENOTYPES IN AML
Incidence, Sensitivity, and Specificity of Leukemia-Associated Phenotypes in Acute Myeloid Leukemia Using Specific Five-Color Multiparameter Flow Cytometry
Adhra Al-Mawali, MD,1,2 David Gillis, MBBS,1 Pravin Hissaria, MD,1 and Ian Lewis, MBBS, PhD2
Key Words: Acute myeloid leukemia; Multiparameter flow cytometry; Leukemia-associated phenotypes
DOI: 10.1309/FY0UMAMM91VPMR2W
A b s t r a c t!"#$%%"%%"&#'("#)%"*)+,"%%#-*#./0-+-1#
2)+'34$1$2"'"1#*+-5#06'-2"'16#'-#&"'"0'#+")7"23$/$%%-03$'"(",-'64"%#89:;%<#3,#'("#=-,"#2$11-5#-*#4$'3",'%#53'(#,"5+6#&3$>,-%"&#$0)'"#26"+-3&#+")7"23$#8:?9<#$,&#&"'"123,"'%#)%"*)+,"%%#*-1#&"'"0'3-,#-*#23,32$+#1"%3&)$+#&3%"$%"#8?@A<B#CD"1$++E#FGH#-*#4$'3",'%#8.IJ.G<#53'(#:?9#($	:;%#$'#&3$>,-%3%B#K("#*1"L)",06#-*#+")7"230#=-,"#2$11-5J2"&3$,#*1"L)",06#-*#9:;%#3,#,-12$+#-1#1">","1$'3,>#=-,"#2$11-5#%$24+"%#)%3,>#2$M32)2#+->#&3**"1",0"#%'$'3%'30%#1"D"$+"&#'($'#NAOE#NA.PE#NAII=E#NAQE#$,&#NAIF#"M41"%%3-,#-,#:?9#=+$%'%#1"41"%",'"&#'("#2-%'#%",%3'3D"#$,"+3$=+"#2$17"1%#*-1#&"'"0'3-,#-*#?@AB#R"13$+#&3+)'3-,$+#"M4"132",'%#%(-5"&#'($'#'("#%",%3'3D3'6#+"D"+#-*#322),-4(",-'643,>#5$%#="'5"",#ISTG#$,&#IST.#$,&#'($'#'("#$441-$0(#5$%#(3>(+6#1"41-&)03=+"B
U22),-4(",-'6430#$,$+6%3%#)%3,>#$#NAG.#>$'3,>#%'1$'">6E#./0-+-1#%'$3,3,>E#$,&#$,#"M'",%3D"#4$,"+#-*#2-,-0+-,$+#$,'3=-&3"%#$++-5"&#'("#3&",'3*30$'3-,#-*#9:;%#3,#FGH#-*#:?9#0$%"%E#$,&#'("%"#322),-4(",-'64"%#0$,#="#)%"&#*-1#?@A#2-,3'-13,>#53'(#$#%",%3'3D3'6#+323'#-*#ISTG#'-#IST.B
!""#$%&'($%)*&+$,-%.-'("/)%0%,+1-"/0+,$/$1+(2-+2-%$(-%.-)'(-"%2)-+"&%3)/$)-10+$+1/0-/&&0+1/)+%$2-%.-.0%4-1*)%"()3*5-!$-3(1($)-*(/326-+)2-#2(-'/2-(7)($8(8-.3%"-10+$+1/0-3(2(/31'-)%-8+/,$%2)+1- 0/9%3/)%3+(25- :(2&+)(- )'(- 4(00;(2)/90+2'(8- #2(.#0;$(22-%.-+""#$%&'($%)*&+$,-.%3-)'(-8+/,$%2+26-10/22+.+1/)+%$6-&3%,$%2)+1-2)3/)+.+1/)+%$6-/$8-"%$+)%3+$,-%.-"+$+"/0-3(2+8#/0-8+2(/2(-<=>:?-+$-/1#)(-0*"&'%90/2)+1-0(#@("+/6-0+"+)(8-8/)/-/3(-/A/+0/90(-%$-+)2-#2(.#0$(22-.%3-=>:-"%$+)%3+$,-+$-/1#)(-"*(0%+8-0(#@("+/-<B=C?5
=>:-+2-8(.+$(8-/2-)'(-&(32+2)($1(-%.-0(#@("+1-1(002-/.)(3-1'("%)'(3/&*-)'/)-1/$$%)-9(-+8($)+.+(8-4+)'-3%#)+$(-"%3&'%;0%,+1-(A/0#/)+%$5-D'(-0(#@("+/;/22%1+/)(8-&'($%)*&(2-<CBE2?-/3(-$%)-&3(2($)-%3-/3(-%$0*-A(3*-+$.3(F#($)0*-&3(2($)-%$-$%3"/0-90%%8- %3- 9%$(-"/33%4- <G=?- 1(0025H;I- J%3-B=C6- &3(A+%#20*-8(213+9(8-/9(33/)+%$2-+$10#8(-)'(-.%00%4+$,K-<H?-/2*$1'3%$%#2-/$)+,($-(7&3(22+%$-<2+"#0)/$(%#2-(7&3(22+%$-%.-(/30*-/$8-0/)(-"/3@(32-+$-H-1(006-2#1'-/2-)'(-1%(7&3(22+%$-%.-L:MN-/$8-L:HI-/$)+,($2?O-<P?-0+$(/,(-+$.+8(0+)*6-4'+1'-+2-(7&3(22+%$-%.-0*";&'%+8;/22%1+/)(8-"/3@(326-+(6-L:P6-L:M6-L:I6-L:Q6-L:HR6-/$8-L:HS6-%$-"*(0%+8-90/2)-1(002O-<M?-/$)+,($-%A(3(7&3(22+%$6-4'+1'-+2-/9$%3"/00*-+$13(/2(8-(7&3(22+%$-%.-/-1(3)/+$-/$)+,($-&(3-1(00O- <N?-/9(33/$)- 0+,');21/))(3-&3%&(3)+(26-4'+1'-+$A%0A(2-)'(-(7&3(22+%$-%.-0*"&'%+8;/22%1+/)(8-/$)+,($2-+$-90/2)-1(002-8+2&0/*+$,-3(0/)+A(0*-'+,'-.%34/38-21/))(3-<JTL?-/$8-2+8(-21/);)(3-<TTL?6-1%33(2&%$8+$,-)%-$%3"/0-"*(0%+8-1(002H6U6QO-/$8-<I?-/92($1(-%.-0+$(/,(;2&(1+.+1-/$)+,($26-4'+1'-+$A%0A(2-/92($1(-%.-(7&(1)(8-/$)+,($-(7&3(22+%$6-2#1'-/2-L:HM-/$8-L:MM6-%$-"*(0%+8-90/2)25V
D'(- (7+2)($1(- %.- CBE2-"/*- 9(- /- A/0#/90(- )%%0- .%3- )'(-8()(1)+%$-%.-=>:-9(1/#2(-$(%&0/2)+1-1(002-1/$-)'#2-9(-8+2)+$;,#+2'(8-.3%"-$%3"/0-'("/)%&%+()+1-&3%,($+)%32-%$-)'(-9/2+2-%.-)'(+3-/9(33/$)-/$)+,($-(7&3(22+%$5S;HH-D'(-&3(2($1(-%.-CBE2-
Am J Clin Pathol 2008;129:934-945 935935 DOI: 10.1309/FY0UMAMM91VPMR2W 935
© American Society for Clinical Pathology
Hematopathology / ORIGINAL ARTICLE
!"#$%&&'$(&)*'#+,"+&($-'$./01213142145
$%6+$+!&-,$,&"7$-'8-(&'8&$
"'($+!&$)*#+$#&'#-+-9&$"'($,&7-"%7&$)",:&,#$;*,$/<=$!"9&$'*+$
%&&'$&#+"%7-#!&($*>-'?$+*$(-#&"#&$!&+&,*?&'&-+@A$B'$"((-+-*'1$
C,&7-)-'",@$,&C*,+#$#6??&#+$+!"+$!-?!$7&9&7#$*;$#&'#-+-9-+@$8"'$
%&$ ,&"8!&($%@$6#-'?$)67+-C",")&+&,$ ;7*>$8@+*)&+,@$ D/EFG$
>!&'$ "CC,*C,-"+&$ (*6%7&H#+&C$ "8I6-#-+-*'$ "'($ )67+-(-)&'H
#-*'"7$"'"7@+-8$C,*8&(6,&#$",&$8*)%-'&(A4JH4K
L!&$"-)$*;$+!&$C,&#&'+$#+6(@$>"#$+*$&MC7*,&$+!&$"CC7-8"H
%-7-+@$"'($#&'#-+-9-+@$*;$NH8*7*,$/EF$-))6'*C!&'*+@C-'?$;*,$
+!&$#+6(@$*;$/<=$-'$C"+-&'+#$>-+!$./0A$L*$"8!-&9&$+!-#$>&$
"'"7@O&($+!&$#&'#-+-9-+@$*;$/EF1$"##&##&($#C&8-;-8-+@$%@$(&+&,H
)-'-'?$-))6'*C!&'*+@C-8$C,*;-7&#$*;$0.P#$*;$./0$9#$+!*#&$
*;$,&?&'&,"+-'?$"'($'*,)"7$Q/$#")C7$"'($(&+&,)-'&($+!&$
-'8-(&'8&$*;$+!&#&$0.P#$-'$"$#&,-&#$*;$NJ$8*'#&86+-9&$C"+-&'+#$
>-+!$'&>7@$(-"?'*#&($./0A
Materials and Methods
!"#$%&'E,&#!$ Q/$ #")C7&#$ ;,*)$ NJ$ 8*'#&86+-9&1$ 6'#&7&8+&($
C"+-&'+#$ >-+!$ ./0$ >&,&$ *%+"-'&($ "+$ (-"?'*#-#$ %&+>&&'$
R"'6",@$ 2SSN$ "'($ .C,-7$ 2SSTA$ L!&$ (-"?'*#&#$ >&,&$ %"#&($
*'$ )*,C!*7*?-8$ ;-'(-'?#1$ -))6'*C!&'*+@C-'?1$ "'($ 8@+*H
?&'&+-8#A4T
$ P"+-&'+$ 8!","8+&,-#+-8#$ ",&$ #!*>'$ -'$ (")%&* + A$
L!&$C"+-&'+#$>&,&$#+,"+-;-&($;*,$,-#:$"88*,(-'?$+*$8@+*?&'&+-8$
"%'*,)"7-+-&#A43
$U*,)"7$Q/$#")C7&#$;,*)$!&"7+!@$9*76'+&&,#$
D'$V$4SG$"'($,&?&'&,"+-'?$Q/$#")C7&#$D'$V$JG$;,*)$C"+-&'+#$
>-+!$'*')@&7*-($)"7-?'"'8-&#$>&,&$6#&($"#$8*'+,*7$#")C7&#$
+*$(&+&,)-'&$+!&$#C&8-;-8-+@$*;$0.P#A$<&?&'&,"+-'?$Q/$#")H
C7&#$>&,&$*%+"-'&($;,*)$J$C"+-&'+#$>-+!$7@)C!*C,*7-;&,"+-9&$
(-#*,(&,#A$L>*$#")C7&#$>&,&$;,*)$C"+-&'+#$ ,&8*9&,-'?$;,*)$
#+"'(",($8!&)*+!&,"C@$"'($+>*$#")C7&#$>&,&$;,*)$C"+-&'+#$
>!*$!"($,&8&-9&($)@&7*"%7"+-9&$8!&)*+!&,"C@$"'($C&,-C!&,"7$
%7**($#+&)$8&77$+,"'#C7"'+"+-*'A$.77$#")C7&#$>&,&$8*77&8+&($*'$
("@$23A
,%-.*/01-#&120B))6'*C!&'*+@C-8$"'"7@#-#$>"#$C&,;*,)&($*'$&,@+!,*H
8@+&H7@#&($>!*7&$Q/$#")C7&#$>-+!$(-,&8+7@$8*'W6?"+&($)*'*H
87*'"7$"'+-%*(-&#$D/*.%#G$ (")%&*3 A$.'+-?&'$&MC,&##-*'$>"#$
"'"7@O&($ %@$ 6#-'?$ NH8*7*,$ 8*)%-'"+-*'#$ *;$ /*.%#$ 8*'W6H
?"+&($>-+!$ ;76*,&-'$ -#*+!-*8@"'"+&$ DEBLFG1$C!@8*&,@+!,-'$
DPXG1$C!@8*&,@+!,-'YL&M"#$,&($DXF=G1$C!@8*&,@+!,-'H8@"'-'$
DPFGHN1$"'($PFHT$"+$(-"?'*#-#A$L>*$/*.%$C"'&7#$>&,&$6#&($
-'$+!&$#+6(@Z$#8,&&'-'?$"'($#&8*'(",@$C"'&7#A$L!&$#8,&&'-'?$
C"'&7$ -#$ *6,$ #+"'(",($ (-"?'*#+-8$ C"'&7$ 6#&($ +*$ (-#+-'?6-#!$
"86+&$ 7@)C!*%7"#+-8$ 7&6:&)-"$ ;,*)$./0A$ [6%#&I6&'+7@1$ -'$
./01$+!&$#&8*'(",@$C"'&7$>"#$6#&($+*$-(&'+-;@$0.P#A$Q7"#+#$
>&,&$ -(&'+-;-&($ %@$ 6#-'?$ "$ F=JN\[[F$ 7*?$ ?"+-'?$ #+,"+&?@A$
Q"8:H?"+-'?$#+,"+&?-&#$6#-'?$F=5J$"'($F=44T$>&,&$6#&($+*$
%&++&,$(&;-'&$ +!&$%7"#+$C*C67"+-*'A$F=JN\F=5J\F=44T$>&,&$
6#&($ -'$ 8*)%-'"+-*'$ >-+!$ (-;;&,&'+$ )@&7*-($ "'($ 7@)C!*-($
)",:&,#$-'$"$NH8*7*,$8*)%-'"+-*'$+*$-'8,&"#&$+!&$#&'#-+-9-+@$*;$
0.P$(&+&8+-*'A$L!-#$>"#$(*'&$+*$*%+"-'$"$)"M-)6)$"(9"'H
+"?&1$-'8*,C*,"+-'?$9",-*6#$C&,)6+"+-*'#$"'($8*)%-'"+-*'#1$*;$
NH8*7*,$/EF$-'$(&;-'-'?$+!&$0.P#A
L!&$#8,&&'-'?$C"'&7$>"#$"#$ ;*77*>#Z$F=THEBLF\F=45H
PX\F=JNHPFHN1$ F=4]HEBLF\F=4SHPX\F=JNHPFHN1$ F=5JH
EBLF\F=55HPX\F=JNHPFHN1$ F=4JHEBLF\F=NKHPX\F=JNH
PFHN1$ ^0.H=<HEBLF\F=JNHPFHN1$ F=4NHEBLF\F=44THPX\
F=JNHPFHN1$ )@&7*C&,*M-("#&\F=JNHPFHN1$ +&,)-'"7$ (&*M@H
'687&*+-(@7$ +,"'#;&,"#&$ DL(LG\F=JNHPFHN1$ "'($ F=JNHPFHN\
[-)67+&#+$ F*'+,*7$4\
2$ D"$ 8*)%-'"+-*'$ *;$ EBLFHB?_4$ "'($
PXHB?_2%G$DQ&8+*'$=-8:-'#*'1$["'$R*#&1$F.GA$L!&$#&8*'(",@$
C"'&7$-#$#!*>'$-'$ (")%&*4 A
.CC,*C,-"+&$-#*+@C&H)"+8!&($'&?"+-9&$8*'+,*7#$>&,&$6#&($
-'$ +!&$ C"'&7$ *;$ /*.%#$ +*$ "##&##$ %"8:?,*6'($ ;76*,&'8&$
-'+&'#-+@A$ L!&$ ,&#C&8+-9&$ 8*)%-'"+-*'#$ *;$ "'+-%*(-&#$ >&,&$
"((&($+*$"CC,*M-)"+&7@$4SK$)*'*'687&",$8&77#$"'($-'86%"+&($
(")%&*+/5"2"61&27'176'*-8*9:*;"17&<1'*=715*>&.%0*?7"@<-'&A*BCD**)0*E'7<@*9F/-%-2*!1"7<7<@G
/5"2"61&27'176* (-1"%
No. of M/F 37/17Mean (range) age at diagnosis (y) 58 (18-85)Median (range) WBC count at diagnosis (! 109/L) 5.6 (0.26-179)Median (range) hemoglobin level at diagnosis (g/L) 94 (52-143)Median (range) platelet count at diagnosis (! 109/L) 61 (11-241)Median (range) bone marrow blasts (%) By morphologic examination 42 (19-96) By multiparametric flow cytometry 36 (7-86)AML cases De novo 42 (78) Secondary 12 (22)French-American-British classification M0 0 (0) M1 9 (17) M2 11 (20) M3 2 (4) M4 9 (17) M5 5 (9) M6 1 (2) M7 1 (2) Not classified 16 (30)Cytogenetic risk group Favorable 9 (17) Intermediate 25 (46) Poor 17 (31) No metaphases 3 (6)World Health Organization classification AML with recurrent genetic abnormalities 11 (20) AML with multilineage dysplasia 10 (19) AML and myelodysplastic syndromes, 0 (0) therapy-related AML, not otherwise categorized 33 (61)
./01$"86+&$)@&7*-($7&6:&)-"A
`$="+"$",&$?-9&'$"#$'6)%&,$DC&,8&'+"?&G$6'7&##$*+!&,>-#&$-'(-8"+&(A$aQF1$
!&)*?7*%-'1$"'($C7"+&7&+$9"76&#$",&$?-9&'$"#$[@#+b)&$B'+&,'"+-*'"7$6'-+#c$
8*'9&,#-*'#$+*$8*'9&'+-*'"7$6'-+#$",&$"#$;*77*>#Z$aQF$8*6'+$D\d0G1$(-9-(&$%@$
SASS4c$!&)*?7*%-'$D?\(0G1$(-9-(&$%@$4Sc$"'($C7"+&7&+$8*6'+$De$4S5\d0G1$(-9-(&$$
%@$4ASA

Frequency of LAIPs in 51 AMLs
20 Am J Clin Pathol 2009;131:16-2620 DOI: 10.1309/AJCP5TSD3DZXFLCX
© American Society for Clinical Pathology
Al-Mawali et al / MINIMAL RESIDUAL DISEASE IN AML
The Quality of LAP for MRD DetectionAnalytic sensitivity refers to how good LAP detection by
MFC is at correctly identifying LAPs. Specificity, on the other hand, refers to how good the test is at correctly identifying cells that are normal.
Thus, the quality of LAP for MRD detection depends on the following: (1) Specificity: Specificity depends on the percentage of LAP expression on normal BM cells; a high specificity can be achieved by including primitive markers (CD34, CD133, and CD117) if present on AML. In most cases, LAP expression on normal BM cells is less than 0.1%.7-11 (2) Sensitivity: The sensitivity of MRD detection depends, among other factors, on the percentage of LAP expression on the leukemic blast population at diagnosis and the number of cells analyzed. For this reason only LAPs that are expressed on more than 10% on the leukemic blast population should be con-sidered.9 (3) Stability: LAPs may undergo phenotypic shifts. During the disease, marker expression in AML may disappear, resulting in false negativity. Especially dim expression of mark-ers is susceptible to change. Furthermore, CD19 expression has been shown to disappear on several occasions in the course of disease. (These definitions are adapted from Dutch/Belgium task force for MRD detection in AML in cooperation with the European Working Group on Clinical Cell Analysis.)
Points for Consideration for Detection of LAPsSeveral issues need to be considered for LAPs detection.
There is a need for testing a wide and comprehensive anti-body panel with progenitor markers included (such as CD34, CD117, and CD133). In our experience,11 using maximum log difference analyses from the median frequency in normal and regenerating BM samples resulted in 5 most sensitive LAPs in our series of 54 newly diagnosed AML cases, and these were CD2, CD56, CD7, CD11b, and CD19 in normal BM and CD56, CD11b, CD2, CD7, and CD19 in regenerating BM, in order of their sensitivity based on maximum log difference, which means that these LAPs are the most sensitive markers for tracking MRD when present in AML samples. These markers represented a reasonable percentage of our cohort: CD2 (9%), CD56 (17%), CD7 (28%), CD11b (14%), and CD19 (4%).
Furthermore, our data showed that CD2, CD56, CD7, CD19, and CD11b are potentially the most useful markers for MRD detection because these markers allowed the maxi-mum analytic sensitivity when normal and regenerating BM samples were taken into account as baseline. Of the 54 cases, 24 (44%) expressed at least one of these markers, and, thus, they should be included in any diagnostic panel of AML for MRD monitoring.
The correct interpretation of antigen expression patterns as compared with normal vs regenerating hematopoietic cells also needs to be considered. Another issue for consideration in LAP detection is the concept that the leukemic blasts are
certainly composed by distinct phenotypic clones.12,19,21 In this regard, Macedo et al7 found that most patients with AML with a LAP have more than 1 aberration. Although this find-ing needs to be interpreted with caution, multiple staining assays to confirm the coexistence of more than 1 aberrant phenotype may be a tool to identify the population of interest in a more appropriate way and then to negate the phenomenon of phenotypic switch at relapse.
Level of SensitivityIn theory, MFC may allow a maximum level of sensitiv-
ity of 1 leukemic cell in 106 after an accurate and prolonged cleansing of the fluidics system.15 However, a more realistic figure for practical applications is 1 target cell in 104 normal cells.15 By using serial dilution of leukemic cells in normal peripheral blood and BM cells, it was shown that MFC is able reliably to detect cells displaying LAPs up to a level of 10–4.11 However, it should be noted that the level of sensitivity varies (from 10–3 to 10–5) depending on the type of phenotypes being analyzed, the combination of MoAb reagents used for their detection,15 and the sample under study.
Table 3Frequencies of LAPs in 51 Patients With AML
Range of Positive No. of Cells in AML Bone LAPs (n = 200) Cases Marrow (%)
Lineage infidelity (n = 40) CD34+/CD2+ 5 26-92 CD34+/CD7+ 12 11-88 CD34+/CD10+ 1 22 CD34+/CD19+ 2 24-65 CD117+/CD2+ 5 13-91 CD117+/CD7+ 11 18-90 CD117+/CD10+ 1 17 CD117+/CD19+ 2 15-53 CD34+/Glycophorin A+ 0 0 CD117+/Glycophorin A+ 1 30Asynchronous antigen expression (n = 146) CD34+/CD11b+ 11 11-80 CD34+/CD14+ 0 0 CD34+/CD15+ 20 10-36 CD34+/CD56+ 5 29-84 CD34+/CD64+ 6 10-49 CD34+/CD65+ 15 11-63 CD117+/CD11b+ 10 12-62 CD117+/CD14+ 0 0 CD117+/CD15+ 25 10-55 CD117+/CD56+ 6 11-80 CD117+/CD64+ 9 11-70 CD117+/CD65+ 22 10-62 CD33+/CD15+ 2 80-94 CD33+/CD64+ 5 18-97 CD33+/CD65+ 5 10-99 CD33+/CD11b+ 3 20-26 CD33+/CD56+ 2 10-78Lack of lineage-specific antigen (n = 14) CD33++/CD13– 5 93-99 CD33–/CD13++ 9 25-98
AML, acute myeloid leukemia; LAPs, leukemia-associated phenotypes; +, positive; ++, strong positive; –, negative.
(Al-‐Mawali, et al Am J Clin Pathol, 2008)

Sensi%vity of aberrant LAIPs
940 Am J Clin Pathol 2008;129:934-945940 DOI: 10.1309/FY0UMAMM91VPMR2W
© American Society for Clinical Pathology
Al-Mawali et al / LEUKEMIA-ASSOCIATED PHENOTYPES IN AML
!"#$%&'
()%*+%,-.%/&01&234/&.,&'5&362&7"89$%/:&5;&<0)8"$&=6&7"89$%/:&",>&'&?%@%,%)"A.,@&=6&7"89$%/
& 234/&.,& 40/.A.B%&C%$$/&.,&& & 40/.A.B%&C%$$/&.,&
& 362&DEF& <0)8"$&=6&DEF& 20@&G.11%)%,-%& ?%@%,%)"A.,@&=6&DEF& 20@&G.11%)%,-%
&<0H&01&
& C"/%/&
234& I.AJ&362K& 6.,& 6"L& 6%>.",& 6.,& 6"L& 6.,& 6"L& 6%>.",& 6.,& 6"L& 6.,& 6"L
CD34+/CD2+ 5 26 92 0.001 0.000 0.030 4.41 4.96 0.004 0.000 0.030 3.81 4.36CD34+/CD7+ 12 11 88 0.002 0.000 0.009 3.74 4.64 0.004 0.000 0.005 3.49 4.39CD34+/CD10+ 1 22 22 0.012 0.000 0.185 3.26 3.26 0.035 0.002 0.072 2.79 2.79CD34+/CD19+ 2 24 65 0.002 0.000 0.007 4.08 4.51 0.003 0.000 0.015 3.96 4.39CD117+/CD2+ 5 13 91 0.003 0.000 0.010 3.64 4.48 0.003 0.000 0.019 3.70 4.54CD117+/CD7+ 11 18 90 0.003 0.000 0.033 3.78 4.48 0.006 0.001 0.017 3.48 4.18CD117+/CD10+ 1 17 17 0.001 0.000 0.014 4.23 4.23 0.003 0.001 0.050 3.75 3.75CD117+/CD19+ 2 15 53 0.002 0.000 0.011 3.88 4.42 0.004 0.000 0.004 3.63 4.18CD34+/CD235+ 0 0 0 0.000 0.000 0.006 NC NC 0.053 0.002 0.237 NC NCCD117+/CD235+ 1 30 30 0.001 0.000 0.008 4.48 4.48 0.015 0.003 0.443 3.31 3.31CD34+/CD11b+ 11 11 80 0.002 0.000 0.022 3.74 4.60 0.002 0.001 0.095 3.74 4.60CD34+/CD14+ 0 0 0 0.000 0.000 0.001 NC NC 0.002 0.001 0.005 NC NCCD34+/CD15+† 20 10 36 0.004 0.000 0.024 3.40 3.95 0.012 0.002 0.014 2.92 3.48CD34+/CD56+ 5 29 84 0.001 0.000 0.039 4.46 4.92 0.001 0.000 0.024 4.35 4.81CD34+/CD64+ 6 10 49 0.051 0.000 0.160 2.29 2.98 0.086 0.000 0.105 2.06 2.75CD34+/CD65+ 15 11 63 0.013 0.005 0.047 2.93 3.69 0.057 0.003 0.106 2.29 3.05CD117+/CD11b+ 10 12 62 0.002 0.000 0.048 3.78 4.49 0.001 0.000 0.026 4.08 4.79CD117+/CD14+ 0 0 0 0.000 0.000 0.010 NC NC 0.001 0.000 0.011 NC NCCD117+/CD15+ 25 10 55 0.010 0.000 0.039 3.00 3.74 0.017 0.005 0.093 2.76 3.50CD117+/CD56+ 6 11 80 0.003 0.000 0.037 3.56 4.43 0.002 0.000 0.025 3.74 4.60CD117+/CD64+ 9 11 70 0.067 0.001 0.127 2.22 3.02 0.040 0.002 0.247 2.44 3.24CD117+/CD65+ 22 10 62 0.007 0.001 0.042 3.15 3.95 0.028 0.023 0.266 2.55 3.34Median 11 62 0.002 0.000 0.027 3.74 4.43 0.004 0.001 0.028 3.48 4.18Minimum 0 0 0 0.000 0.001 2.22 2.98 0.001 0.000 0.004 2.06 2.75Maximum 30 92 0.067 0.005 0.185 4.48 4.96 0.086 0.023 0.443 4.35 4.81
!"#$%&'()*%+,*-./0%-*(1*+/&2%3"$%4.5*%+&66.72%#!8$%-*(1*+/&9&::.'/&)*0%;<*5.),;*2%"&=$%+&=/+(+2%"/5$%+/5/+(+2%>?$%5.%'&:*:%@.(50%@.6%)<*%0*@/5*0%&4*66&5)%/++(5.;<*5.),;*A
B%C.+*%'&:*:%<&D*%+.6*%)<&5%E%#!8AF%?GHIJK?GELJK?GHH0/+%7&:%0*@/5*0A
CD34+CD2+
CD34+CD7+
CD34+CD19+
Most Aberrant and Sensitive LAPs
Max
imum
Log
Diff
eren
ce
CD34+CD11b+
CD34+CD56+
4.2
4.3
4.4
4.5
4.6
4.7
4.8
4.9
5.0
CD34+CD7+
CD34+CD19+
CD117+CD2+
CD34+CD11b+
Most Aberrant and Sensitive LAPs
CD34+CD56+
CD117+CD11b+
CD117+CD56+
Max
imum
Log
Diff
eren
ce4.1
4.2
4.3
4.4
4.5
4.6
4.7
4.8
4.9
A B
(.@+)%&5 The most aberrant and most sensitive phenotypes based on maximum log difference in percentage of positive cells of leukemia-associated phenotypes (LAPs) in acute myeloid leukemia samples from normal bone marrow (A) and regenerating bone marrow (B).
M<*% /0*&-% &::&,% :,:)*+% @.6% )<*% 0*)*')/.5% .@% :+&--%5(+4*6:%.@% -*(1*+/'%'*--:% )<&)%;*6:/:)%&@)*6%'<*+.)<*69&;,%/5%3"%.6%4-..0%:&+;-*:%:<.(-0%@(-@/--%)<*%@.--.7/5N%'6/)*6/&O%PEQ%&;;-/'&4-*%/5%+.:)%'&:*:%.@%)<*%0/:*&:*%(50*6%:)(0,$%PRQ%:;*'/@/'%@.6%5*.;-&:)/'%'*--%),;*$%PHQ%:*5:/)/D*$%
&50%PIQ%&--.7:%S(&5)/)&)/.5%.@%)(+.6%4(60*5%@.6%;6.N5.:9)/'%;(6;.:*:ART
M<*%;6*:*5)%:)(0,%4&:*0%.5%(:/5N%L9'.-.6%@-.7%',).+*)6,%&50%&5%*=)*5:/D*%;&5*-%.@%".!4:%/5%!"#%'&:*:%:<.7*0%)<&)%#!8:%7*6*%;6*:*5)%/5%)<*%+&U.6/),%.@%'&:*:%PVIWQA%".6*.D*6$%
(Al-‐Mawali, et al Am J Clin Pathol, 2008)
Compared to normal BMs Compared to reacTve BMs

Technical aspects: How many events?
• Several studies have used an MRD cut-‐off of 0.03 – 0.1% (Kern, et al Haematologica, 2004) (Al-‐Mawali, et al Am J Clin Pathol, 2009) (Buccisano, et al Leukemia, 2006) (Langebrake, et al J Clin Oncol, 2006)
• For a 0.01% (10-‐4) detec%on level, at least 200,000 events are required to detect 20 aberrant blasts
• In prac%ce, up to 1,000,000 events may be necessary

AML -‐ Diagnosis
20% blasts

AML – MRD at day 14
0.06% blasts

Technical aspects: IP stability
• Ques%on: Is the aberrant blast IP rela%vely stable over %me?
• Hematologic malignancies (ALL, PCM, T-‐LGLL, MF / SS) demonstrate temporal IP instability
• May occur in AML at follow-‐up
(San Miguel, et al Blood, 1997)

Issues to consider • Revised defini%on for CR in AML – Similar to plasma cell myeloma
• What level of MRD correlates with cure?
• Role of addi%onal therapy in MRD(+) cases
• MRD detec%on in peripheral blood / stem cells
• MRD analysis in CD34(-‐) AML
• Uniform analy%c strategies
• FC vs. PCR comparison for MRD detec%on

Future developments • Several single-‐ins%tu%on, retrospec%ve studies have been performed
• Standardize LAIP analysis to enable adequate mul%center clinical studies (ini%ated in Netherlands and Switzerland – HOVON/SAKK studies)
• Perform RQ-‐PCR in parallel with FC • Prospec%ve, randomized trials, to determine the clinical value of MRD status as predic%ve biomarker (underway in UK – AML 16 and 17 trials)

Conclusions
• There are technical issues associated with blasts IP in MPN
• Tradi%onal CD45/SSC “blast gate” has a heterogeneous composi%on
• There is IP overlap between reac%ve and neoplas%c blast aberrancies
• FC is useful and diagnosis and assessment of MRD in AML

Conclusions
• Currently, there are numerous technical limita%ons for MRD detec%on by FC
• MRD assessment may help in refining risk stra%fica%on of AML pa%ents
• MRD assessment may apply to individual risk defini%on
• MRD assessment poten%ally cons%tutes a short-‐term surrogate endpoint for determining effec%veness of new therapies

References • Al-‐Mawali, A., Gillis, D., Hissaria, P. & Lewis, I. (2008) Incidence, sensi%vity, and
specificity of leukemia-‐associated phenotypes in acute myeloid leukemia using specific five-‐color mul%parameter flow cytometry. Am J Clin Pathol, 129, 934-‐945.
• Al-‐Mawali, A., Gillis, D. & Lewis, I. (2009) The role of mul%parameter flow cytometry for detec%on of minimal residual disease in acute myeloid leukemia. Am J Clin Pathol, 131, 16-‐26.
• Al-‐Mawali, A., Gillis, D. & Lewis, I. (2009) The use of receiver opera%ng characteris%c analysis for detec%on of minimal residual disease using five-‐color mul%parameter flow cytometry in acute myeloid leukemia iden%fies pa%ents with high risk of relapse. Cytometry B Clin Cytom, 76, 91-‐101.
• Bene, M.C. & Kaeda, J.S. (2009) How and why minimal residual disease studies are necessary in leukemia: a review from WP10 and WP12 of the European LeukaemiaNet. Haematologica, 94, 1135-‐1150.
• Borowitz, M.J., Guenther, K.L., Shults, K.E. & Stelzer, G.T. (1993) Immunophenotyping of acute leukemia by flow cytometric analysis. Use of CD45 and right-‐angle light scaher to gate on leukemic blasts in three-‐color analysis. Am J Clin Pathol, 100, 534-‐540.

• Buccisano, F., Maurillo, L., Gahei, V., Del Poeta, G., Del Principe, M.I., Cox, M.C., Paneha, P., Consalvo, M.I., Mazzone, C., Neri, B., Ohaviani, L., Fraboni, D., Tamburini, A., Lo-‐Coco, F., Amadori, S. & Vendix, A. (2006) The kine%cs of reduc%on of minimal residual disease impacts on dura%on of response and survival of pa%ents with acute myeloid leukemia. Leukemia, 20, 1783-‐1789.
• Buccisano, F., Maurillo, L., Spagnoli, A., Del Principe, M.I., Ceresoli, E., Lo Coco, F., Arcese, W., Amadori, S. & Vendix, A. (2009) Monitoring of minimal residual disease in acute myeloid leukemia. Curr Opin Oncol, 21, 582-‐588.
• Campana, D. & Coustan-‐Smith, E. (1999) Detec%on of minimal residual disease in acute leukemia by flow cytometry. Cytometry, 38, 139-‐152.
• Cheson, B.D., Benneh, J.M., Kopecky, K.J., Buchner, T., Willman, C.L., Estey, E.H., Schiffer, C.A., Doehner, H., Tallman, M.S., Lister, T.A., Lo-‐Coco, F., Willemze, R., Biondi, A., Hiddemann, W., Larson, R.A., Lowenberg, B., Sanz, M.A., Head, D.R., Ohno, R. & Bloomfield, C.D. (2003) Revised recommenda%ons of the Interna%onal Working Group for Diagnosis, Standardiza%on of Response Criteria, Treatment Outcomes, and Repor%ng Standards for Therapeu%c Trials in Acute Myeloid Leukemia. J Clin Oncol, 21, 4642-‐4649.
• Dohner, H., Estey, E.H., Amadori, S., Appelbaum, F.R., Buchner, T., Burneh, A.K., Dombret, H., Fenaux, P., Grimwade, D., Larson, R.A., Lo-‐Coco, F., Naoe, T., Niederwieser, D., Ossenkoppele, G.J., Sanz, M.A., Sierra, J., Tallman, M.S., Lowenberg, B. & Bloomfield, C.D. (2010) Diagnosis and management of acute myeloid leukemia in adults: recommenda%ons from an interna%onal expert panel, on behalf of the European LeukemiaNet. Blood, 115, 453-‐474.

• Grimwade, D., Vyas, P. & Freeman, S. (2010) Assessment of minimal residual disease in acute myeloid leukemia. Curr Opin Oncol, 22, 656-‐663.
• Harrington, A., Olteanu, H. & Krof, S. (2010) The specificity of immunophenotypic altera%ons in blasts in nonacute myeloid disorders. Am J Clin Pathol, 134, 749-‐761.
• Harrington, A.M., Olteanu, H. & Krof, S.H. (2010) A dissec%on of the CD45/SSC (SS) blast gate in non-‐acute myeloid disorders and non-‐neoplas%c bone marrows [abstract]. Mod Pathol, 23, 301A.
• Kern, W., Bacher, U., Haferlach, C., Schnihger, S. & Haferlach, T. (2010) The role of mul%parameter flow cytometry for disease monitoring in AML. Best Pract Res Clin Haematol, 23, 379-‐390.
• Grimwade, D., Jovanovic, J.V., Hills, R.K., Nugent, E.A., Patel, Y., Flora, R., Diverio, D., Jones, K., Asleh, H., Batson, E., Rennie, K., Angell, R., Clark, R.E., Solomon, E., Lo-‐Coco, F., Wheatley, K. & Burneh, A.K. (2009) Prospec%ve minimal residual disease monitoring to predict relapse of acute promyelocy%c leukemia and to direct pre-‐emp%ve arsenic trioxide therapy. J Clin Oncol, 27, 3650-‐3658.
• Grimwade, D., Vyas, P. & Freeman, S. (2010) Assessment of minimal residual disease in acute myeloid leukemia. Curr Opin Oncol, 22, 656-‐663.
• Kern, W., Haferlach, C., Haferlach, T. & Schnihger, S. (2008) Monitoring of minimal residual disease in acute myeloid leukemia. Cancer, 112, 4-‐16.
• Kern, W., Voskova, D., Schoch, C., Schnihger, S., Hiddemann, W. & Haferlach, T. (2004) Prognos%c impact of early response to induc%on therapy as assessed by mul%parameter flow cytometry in acute myeloid leukemia. Haematologica, 89, 528-‐540.

• Krof, S.H. & Karandikar, N.J. (2007) Flow cytometric analysis of acute leukemias, myelodysplas%c syndromes, and myeloprolifera%ve disorders. In: Flow Cytometry in Clinical Diagnosis (ed. by Carey, J.L., McCoy, J.P. & Kere, D.F.). ASCP Press, Chicago.
• Kussick, S.J. & Wood, B.L. (2003) Four-‐color flow cytometry iden%fies virtually all cytogene%cally abnormal bone marrow samples in the workup of non-‐CML myeloprolifera%ve disorders. Am J Clin Pathol, 120, 854-‐865.
• Langebrake, C., Creutzig, U., Dworzak, M., Hrusak, O., Mejstrikova, E., Griesinger, F., Zimmermann, M. & Reinhardt, D. (2006) Residual disease monitoring in childhood acute myeloid leukemia by mul%parameter flow cytometry: the MRD-‐AML-‐BFM Study Group. J Clin Oncol, 24, 3686-‐3692.
• Maurillo, L., Buccisano, F., Del Principe, M.I., Del Poeta, G., Spagnoli, A., Paneha, P., Ammatuna, E., Neri, B., Ohaviani, L., Sarlo, C., Vendix, D., Quaresima, M., Cerrex, R., Rizzo, M., de Fabri%is, P., Lo Coco, F., Arcese, W., Amadori, S. & Vendix, A. (2008) Toward op%miza%on of postremission therapy for residual disease-‐posi%ve pa%ents with acute myeloid leukemia. J Clin Oncol, 26, 4944-‐4951.
• Ossenkoppele, G.J., van de Loosdrecht, A.A. & Schuurhuis, G.J. (2011) Review of the relevance of aberrant an%gen expression by flow cytometry in myeloid neoplasms. Br J Haematol, 153, 421-‐436.
• Perea, G., Lasa, A., Aven%n, A., Domingo, A., Villamor, N., Queipo de Llano, M.P., Llorente, A., Junca, J., Palacios, C., Fernandez, C., Gallart, M., Font, L., Tormo, M., Florensa, L., Bargay, J., Mar%, J.M., Vivancos, P., Torres, P., Berlanga, J.J., Badell, I., Brunet, S., Sierra, J. & Nomdedeu, J.F. (2006) Prognos%c value of minimal residual disease (MRD) in acute myeloid leukemia (AML) with favorable cytogene%cs [t(8;21) and inv(16)]. Leukemia, 20, 87-‐94.

• Rubnitz, J.E., Inaba, H., Dahl, G., Ribeiro, R.C., Bowman, W.P., Taub, J., Pounds, S., Razzouk, B.I., Lacayo, N.J., Cao, X., Meshinchi, S., Degar, B., Airewele, G., Raimondi, S.C., Onciu, M., Coustan-‐Smith, E., Downing, J.R., Leung, W., Pui, C.H. & Campana, D. (2010) Minimal residual disease-‐directed therapy for childhood acute myeloid leukaemia: results of the AML02 mul%centre trial. Lancet Oncol, 11, 543-‐552.
• San Miguel, J.F., Mar%nez, A., Macedo, A., Vidriales, M.B., Lopez-‐Berges, C., Gonzalez, M., Caballero, D., Garcia-‐Marcos, M.A., Ramos, F., Fernandez-‐Calvo, J., Calmun%a, M.J., Diaz-‐Mediavilla, J. & Orfao, A. (1997) Immunophenotyping inves%ga%on of minimal residual disease is a useful approach for predic%ng relapse in acute myeloid leukemia pa%ents. Blood, 90, 2465-‐2470.
• Schnihger, S., Kern, W., Tschulik, C., Weiss, T., Dicker, F., Falini, B., Haferlach, C. & Haferlach, T. (2009) Minimal residual disease levels assessed by NPM1 muta%on-‐specific RQ-‐PCR provide important prognos%c informa%on in AML. Blood, 114, 2220-‐2231.
• Stelzer, G.T., Shults, K.E. & Loken, M.R. (1993) CD45 ga%ng for rou%ne flow cytometric analysis of human bone marrow specimens. Ann N Y Acad Sci, 677, 265-‐280.
• van Rhenen, A., Moshaver, B., Ossenkoppele, G.J. & Schuurhuis, G.J. (2007) New approaches for the detec%on of minimal residual disease in acute myeloid leukemia. Curr Hematol Malig Rep, 2, 111-‐118.