Embed Size (px)
Citation preview

Vol. 3, 999-1007, June 1997 Clinical Cancer Research 999
3 The abbreviations used are: CSF- 1 . macrophage colony-stimulatingfactor; LMP, low malignant potential.
Overexpression of Epithelial Macrophage Colony-stimulating Factor
(CSF-1) and CSF-1 Receptor: A Poor Prognostic Factor in
Epithelial Ovarian Cancer, Contrasted with a
Protective Effect of Stromal CSF-1’
Setsuko K. Chambers,2 Barry M. Kacinski,
Christina M. Ivins, and Maria L. Carcangiu
Departments of Obstetrics and Gynecology [S. K. C.. B. M. K..
C. M. I.. M. L. Cl, Therapeutic Radiology [B. M. K.l. Dermatology
lB. M. K.l, and Pathology IM. L. Cl, Yale University School of
Medicine. New Haven, Connecticut ()6520-8063
ABSTRACT
Markedly elevated levels of macrophage colony-stimu-
lating factor (CSF-1) in the serum and ascites of epithelial
ovarian cancer patients have been previously associatedwith a poor prognosis. However, measurements of circulat-
ing CSF-1 cannot separate CSF-1 originating in the cancer
cell from that originating in stromal macrophage or fibro-
blast. To study the prognosis related to expression of CSF-1
and its receptor in primary and metastatic ovarian cancers
and to compare the significance of epithelial versus stromal
CSF-1 expression, an immunohistochemical study of 130
ovarian carcinomas was performed.
Twenty-two stage I and II and 108 stage Ill and IV
primary tumors were studied. Metastatic lesions were also
studied in 96 of these 130 cases, 90 of which came from those
cases with advanced-stage disease. The intensity and extent
of staining for CSF-1 in epithelium and stroma and forepithelial CSF-1 receptor was scored. Kaplan-Meier curves
of survival were compared with the log-rank test. The Cox
regression model was used for multivariate analysis.
In the primary tumors, there was strong expression of
CSF-1 receptor in 65%, epithelial CSF-1 in 36%, and stro-
mal CSF-1 in 22%. In the metastases, there was strong
staining for CSF-l receptor in 65%, epithelial CSF-1 in
41 %, and stromal CSF-1 in 15%; strong staining for both
CSF-1 receptor and epithelial CSF-1 was noted in 26% of
the cases. When the metastases expressed both CSF-1 recep-
tor and epithelial CSF-1 strongly, a significant decrease in
disease-free survival in stage III invasive ovarian cancers
was observed (P 0.043), which was found to be an inde-
pendent prognostic factor (P = 0.007), with an increased
relative risk of recurrence of 2.3-fold. Although strong stain-ing for stromal CSF-1 in the primary tumor was not found
to have prognostic value, for all stages and for the subsets of
stages III and IV and for stage III alone, the finding of any
degree of stromal CSF-1 expression in the ovary was a
favorable prognostic factor for disease-free (P = 0.046) and
overall (P = 0.015) survival. This finding was associated
with younger patients (P = 0.007) and low-grade tumors
(P = 0.033) and was not an independent prognostic factor on
multivariate analysis. Among the primary tumors, there was
a significant association (P 0.022) between stromal CSF-1
staining and lack of strong coexpression of CSF-1 receptor
and epithelial CSF-1; 67 of 94 cases shared these features in
the primary tumors. In the metastases of invasive stage III
cases, strong staining for stromal CSF-1 was a favorable
prognostic factor for overall survival in the absence of
strong CSF-1 receptor staining (P = 0.033) and was associ-
ated with low-grade tumors (P = 0.0002).
We report that strong expression of epithelial CSF-I
along with its receptor in the metastases of ovarian cancer
patients appears to be a strong independent poor prognostic
factor for outcome. We find that expression of the same
cytokine (CSF-l) in the stroma of the primary tumors is
associated with low-grade tumors and lack of strong coex-
pression of CSF-1 receptor and epithelial CSF-l, leading to
an improved long-term outcome. This study may help ex-
plain the previous observations that elevated levels of CSF-1
in serum and ascites are associated with a worse prognosis in
advanced ovarian cancer patients; the results suggest that
the source of secreted CSF-1 may largely be the epithelium.
The results of this study suggest that paracrine effects of
stromal CSF-1 on tumor behavior contrast with those dem-
onstrated when the tumor cell is capable of autocrine intra-
cellular or extracellular interactions between CSF-I and its
receptor.
Received 12/4/96: revised 2/17/97: accepted 3/5/97.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with I 8 U.S.C. Section 1734 solely to
indicate this fact.
t Supported by NIH Grants HD 27446 and CA 60665 (to S. K. C.). and
NIH Grant CA 47292 (to B. M. K.).2 To whom requests for reprints should be addressed, at Division of
Gynecologic Oncology. Department of Obstetrics and Gynecology.Yale University School of Medicine, 333 Cedar Street, P. 0. Box
208063, New Haven, CT 06520-8063. Phone: (203) 785-5778; Fax:
(203) 785-6782.
INTRODUCTIONFor the past 10 years. attention has been focused by our-
selves and others on the role of CSF- � and its receptor in
epithelial malignancies, including those of breast, lung, pancre-
atic, endometrial, and ovarian origin ( 1-10). In ovarian carci-
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Mean survival(mo)
P = 0.0001
69.3 ± 4.1
54.2 ± 4.8
17.4 ± 2.7
NS”
Mean disease-freesurvival (mo)
P = 0.0001
58.3 ± 5.7
25.3 ± 2.9
4.8 ± 1.6
NS
P = 0.0002
51.1 ± 5.1
16.6 ± 2.0
21.4 ± 2.5
P = 0.0001
34.9 ± 3.1
7.4 ± 1.9
NS
P = 0.01128.3 ± 2.7
10.1 ± 4.1
P = 0.000169.1 ± 3.9
52.3 ± 6.344.9 ± 4.0
P = 0.0001
64.9 ± 5.129.1 ± 3.7
NS
P = 0.00657.6 ± 4.3
26.7 ± 7.2
mucinous, clear cell,
1000 CSF-l and CSF-l Receptor in Ovarian Cancer
nomas, we have previously shown that high levels of CSF- 1
receptor (c-fins) transcripts and protein (as measured by in situ
hybridization and immunohistochemistry on tissues) correlate
strongly with high-grade and advanced clinical presentations,
prognostic of poor outcome (2, 3). Although some CSF-l is
occasionally expressed by normal ovarian surface epithelium
( I 1 ) and benign ovarian neoplasms, intense staining is apparent
only in invasive neoplasms (2, 6). Coexpression of CSF- 1 and
its receptor is also often detected in ovarian cancer metastases,
even when such expression is not observed in the primary tumor
(6). Tumor-derived cell lines have been shown to synthesize
significant quantities of biologically active CSF-l (5, 12), and
tumor derived CSF- I contributes to the elevated circulating
serum CSF- 1 levels found in ovarian cancer patients. We and
others have also shown that serum CSF- 1 is a sensitive and
useful tumor marker in these patients, because elevations in
CSF- 1 levels frequently heralds disease recurrence or progres-
sion (12-14). Recently, others have shown that the finding of
markedly elevated serum CSF-l levels at diagnosis in ovarian
cancer patients is correlated with a poor outcome (15). In the
ascites of patients undergoing primary surgery for stage III and
IV ovarian cancer, we have also demonstrated that elevated
levels of CSF-l are independently predictive of poor overall
survival (16).
Not only do approximately one-half of ovarian cancer
specimens coexpress CSF-l along with its receptor (2), but
CSF-l is also expressed by the stromal fibroblasts and infiltrat-
ing macrophages (1). Consequently, in vivo, a tumor (epithelial)
origin of elevated levels of CSF- 1 in the serum or ascites cannot
be easily distinguished from one of macrophage or fibroblast
origin. To study the prognostic significance of CSF-l and its
receptor in primary and metastatic epithelial ovarian cancer
tissues and to contrast the importance of CSF- 1 expression by
epithelial cells from that by the stroma, an immunohistochem-
ical study of CSF- 1 and CSF- I receptor antigen staining in
tissues from I 30 epithelial ovarian cancer patients was under-
taken.
MATERIALS AND METHODS
Patients and Samples. Our study group consisted of 130
patients operated upon for ovarian carcinoma and managed by
the faculty of the Division of Gynecologic Oncology, between
May 1982 and October 1990 at the Yale-New Haven Medical
Center (New Haven, CT). All patients therefore received corn-
plete surgical staging and uniform treatments. The clinicopath-
ological characteristics and their prognostic significance for the
whole group of patients are listed in Table I . Of 1 30 patients,
106 (81 .5%) received platinum-based chemotherapy as adjuvant
treatment. The majority of the 18 patients who received either
alkylating agents (n 12) or no adjuvant therapy (n 6) had
LMP or grade 1 carcinomas. The remaining 6 patients received
whole-abdominal radiation therapy. Of the 99 patients with
invasive stage III and IV disease, only 6 patients did not receive
primary platinum-based chemotherapy. Their mean survival of
39.2 ± 3.7 months was not different from the mean survival of
the whole group of invasive stage III and IV patients of 39.3 ±
3.6 months. Only 25 of the I 18 patients with invasive carcino-
mas ( 14 stage I and II and I I stage III and IV) and 10 of the I 2
Table 1 Patient characteristics and prognostic significance (n = 130)
Characteristic No.
Stage
landIl 22
III 82
IV 26
Age�60 yr 69>6Oyr 61
GradeLMP 12I 12
2and3 106
Residual disease<2cm 92
�2cm 38
Histology
Nonserous” SOSerous or 80surface serous
Performance status
Oandl 118�2 12
a NS, not significant.
b Includes histological types: cndomctrioid,
undifferentiated, and mixed cpithclial.
patients with LMP tumors were still alive at the time of this
analysis. The median follow-up (until death or date last seen) for
the study group was 37 months (range, 1-136 months). The
following factors were abstracted from each chart: International
Federation of Obstetrics and Gynecology stage, residual disease
at the end of primary surgery, patient age, Eastern Cooperative
Oncology Group performance status, treatment, date of recur-
rence, status, and date last seen.
Immunohistochemical Studies. Formalin-fixed, paraf-
fin-embedded tissue was available from at least one neoplastic
ovary for each case. In addition, in 62 cases, paraffin blocks
were available from the contralateral neoplastic ovary. For the
I 1 stage II primary tumors, paraffin blocks were available from
6 metastases (no LMP implants). Among the 108 stage III and
IV primary tumors, paraffin blocks were available from 86
metastases and 4 LMP implants. Rarely, the tissue section
stained from primary or metastatic lesions did not contain ma-
lignant cells; therefore, the number of cases studied per antibody
varied slightly. The 130 tumors studied included 1 18 invasive
carcinomas (61 papillary serous, 7 surface serous, 25 endometn-
oid, 2 mucinous, 7 clear cell, 8 undifferentiated, and 8 mixed
epithelial carcinomas) and 12 tumors of LMP (I 1 serous and I
mixed epithelial type). Of the invasive papillary serous tumors,
8 were histologically grade 1 , 10 grade 2, and 43 grade 3. Of the
invasive tumors of surface serous type, all were grade 3. Of the
invasive tumors of endometnoid type, 3 were grade 1 , 5 grade
2, and 17 grade 3. Of the invasive tumors of mucinous type, one
was grade 1 and the other grade 3. All invasive clear cell
carcinomas were grade 3. Of the mixed epithelial carcinomas, 2
were grade 2 and 6 grade 3. The histological classification was
based on the typing criteria of the WHO. All tissue specimens
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

�‘%\ ,, ‘ -. �
‘4� .�
:�:- .
,; II
;�‘\. �
s� � �
were obtained in accordance with Yale Human Investigations
Committee protocols 3303 and 7027.
Six-p.m sections were prepared on poly-lysine-coated
slides and heated at 60#{176}Cfor 1 h, deparaffinized in xylene, and
rehydrated in solutions of decreasing ethanol concentration.
Endogenous peroxidase was quenched by a 30-mm incubation
with 0.3% hydrogen peroxide in methanol. The slides to be
assayed for CSF- I receptor antigen expression were treated
three times in 70 ml of 10 mrvi citrate buffer (pH 6.0) in the
microwave at 700 W for 5 mm to enhance antigen retrieval.
After being washed in 1% BSA in PBS (pH 7.4), all slides were
preincubated with 1 .5% normal horse or rabbit serum for 1 h to
block nonspecific antibody binding. The slides were incubated
overnight at 4#{176}Cwith a 1 : 100 dilution of a rabbit antifeline
v-fms antibody (OA-l 1-816, Cambridge Research Biochemi-
cals Ltd., Cheshire, United Kingdom) or a I :500 dilution of a
mouse monoclonal antihuman CSF-l IgG (HM 7/7.7.10, kindly
provided by the Immunology Department of Genetics Institute,
Cambridge, MA). Negative controls were run in parallel with an
irrelevant mouse monoclonal IgG (Sigma Chemical Co.) or
rabbit IgG (Sigma) or with PBS in place of the primary anti-
body. Specificities of these primary antibodies have been pre-
viously established by competition experiments (17). There was
complete competition for the signal when a 10-fold molar cx-
cess of human recombinant CSF- I was added, with no residual
staining evident (17). After a PBS wash, the slides were incu-
bated for 30 mm with biotinylated horse antimouse or goat
antirabbit antibody, washed with PBS, and then incubated for
1 h in an avidin-horseradish peroxidase complex solution (ABC
Elite kit, Vector Corp., Burlingame, CA). After another PBS
wash, the slides were incubated in 0.02% hydrogen peroxide
and 0. 1% diaminobenzidine in 0. 1 M Tris buffer (pH 7.2, Vec-
tor), washed in tap water, counterstained with hematoxylin,
dehydrated in 100% ethanol, cleared in xylene, and mounted.
All slides were reviewed and scored by a senior gynecologic
pathologist (M. L. C., who was blinded to the clinical and out-
come data) using a modified H score ( 18), with a score of 0
implying no staining in the slide and 400 reflecting intense
staining over the whole slide. The degree of staining for CSF-l
in the epithelial cancer cells was evaluated separately from that
in the stroma for each tissue section. For statistical analysis, the
degree of antigen staining was subdivided into three groups: H
scores of 0-99, 100-199, and �200. Any staining refers to a
score of � 100 and strong staining refers to a score �200. In this
paper, we refer to CSF- 1 expression by stromal cells as “stromal
CSF-l”; similarly, CSF-l expressed by epithelial cells is re-
ferred to as “epithelial CSF- I .“
Statistical Analysis. Statistical analysis was performed
by using the SAS statistical package (Cary, NC); a P of <0.05
was considered significant. The Mann-Whitney U test was used
as a nonparametric test of association. Kaplan-Meier survival
curves were compared with the log-rank test. A multivariate
Cox regression model was used to assess independence of
prognostic factors.
RESULTS
Our study group appears to be representative of epithelial
ovarian cancers in general, as the standard risk factors of stage,
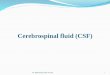
��tI_Fig. I Strong staining (score � 200) of epithelial CSF-1 receptor inthe primary tumor of a patient with stage IV, grade 2 papillary serouscarcinoma of the ovary.
grade, residual disease, and performance status retained prog-
nostic significance for both disease-free and overall survival
(Table 1). The proportions of patients having each patient char-
acteristic (Table 1 ) is also representative of the disease in
general.
CSF-1 Receptor, Epithelial CSF-1, or Stromal CSF-1
Expression in Epithelial Ovarian Cancer
Primary Tumors. CSF- I receptor staining was seen pre-
dominantly in the cancer cells (Fig. I ), but it was also seen in
stromal macrophages. CSF-l staining was seen in both the
stroma [primarily in the fibroblasts but also in macrophages (2)]
and the neoplastic cells, where it was predominantly cytoplas-
mic. When tissues from both neoplastic ovaries were available,
there tended to be concordance in the degree of staining between
one ovary and its contralateral partner. There was agreement for
44 of 55 paired sets of ovaries for CSF- I receptor staining (P =
0.08), for 44 of 62 paired sets for stromal CSF- 1 staining (P =
0.006), and for 46 of 62 paired sets for strong staining of
epithelial CSF-l (P 0.07). Thus, for the rest of the analysis,
the degree of antigen staining in the ovary was represented by
the ovary in each case that stained most strongly.
Expression for both CSF-l and its receptor (score � 100)
was a common finding in the primary ovarian tumors. For the
whole group, 92% (117 of 127) of the ovarian specimens cx-
pressed CSF-l receptor, 75% (97 of 129) expressed epithelial
CSF- 1 , and 74% (96 of I 29) expressed stromal CSF- I . Strong
staining (score � 200) for CSF-l receptor was seen in 65% (83
of 127) of the ovarian primary tumors; strong staining was seen
for epithelial CSF-l in 36% (46 of 129) and for stromal CSF-l
in 22% (28 of 1 29) of the primary lesions. Coexpression of
strong staining for both CSF-l receptor and epithelial CSF-l in
the primary invasive carcinomas was seen 26% (30 of I 16) of
the time, with no such coexpression seen in any of the 1 2 tumors
of LMP.
Metastases. Where the metastases are concerned, the
same relationships described for the primary tumors exist.
CSF-l receptor was expressed (score � 100) by 83% (74 of 89)
of metastases or implants, epithelial CSF-l by 69% (66 of 96),
Clinical Cancer Research 1001
.� -
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

cDloo
�80Cl)
Cl)
V40
C
g20
O_0
- fms&CSF-1- (N=44)
1002 CSF-l and CSF-l Receptor in Ovarian Cancer
�
� � ��: : : �
h�4��? \
-‘ *, . ..-�..........- S..
4,, � �
4::� � � �:#{176}: � .t�()
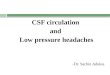
Fig. 2 Coexpression of strong staining (score � 200) for both epithe-hal CSF-l receptor (A) and epithelial CSF-l (B) in the omentum of a
patient with stage IIIC. grade 3. mixed cpithclial (papillary scrous and
clear cell) ovarian carcinoma.
and strornal CSF-l by 56% (54 of 96) of metastatic lesions or
implants. Strong staining (score � 200) in the metastases or
implants was seen for CSF-l receptor in 65% (58 of 89), for
epithelial CSF-l in 41% (39 of 96), and for stromal CSF-l in
15% (14 of 96). In the invasive cases, coexpression for strong
staining of CSF-l receptor and epithelial CSF-1 in the metas-
tases (Fig. 2) was seen in 29% ( 1 8 of 62) of stage III cases and
in 27% (22 of 83) of stage III and IV cases. There were only
three cases seen of coexpression of strong staining for CSF- 1
receptor and stromal CSF- 1 in the metastases, but none were
seen in the absence of strong staining for epithelial CSF-l . For
the whole group, for both the primary tumors (P = 0.026) and
metastases or implants (P 0.0002), strong epithelial CSF-l
staining (score � 200) was closely associated with the presence
of strong stromal CSF- I staining. In the metastases or implants,
only two cases of strong staining of stromal CSF- I were seen in
the absence of strong staining for epithelial CSF-l. Thus, it
appears that strong epithelial CSF-l expression is essentially a
necessary prerequisite for strong stromal CSF- 1 expression.
Significance of Coexpression of CSF-1 Receptor and
Epithelial CSF-1
Because strong coexpression of CSF-l receptor and epi-
thelial CSF- I was not seen in any of the primary tumors of
0 20 40 60 80
Time (months)Fig. 3 Disease-free survival of patients with invasive stage III epithe-
hal ovarian cancer by cocxprcssion of strong staining for CSF- 1 receptorand cpithclial CSF-l in the metastases (a = 62). Patients who had
coexpression of strong staining for CSF- I receptor and cpithclial CSF- 1
had a significantly shorter disease-free survival than those who did not.
LMP, the analysis of clinical significance of this feature was
limited to the invasive cases (n = I 18).
Primary Tumors. Coexpression of strong staining
(score � 200) for CSF-l receptor and epithelial CSF-l in the
primary invasive tumors did not find prognostic significance
among all, early, or advanced stages. Strong coexpression in the
primary tumors was significantly associated with strong CSF-l
receptor staining in the metastases (P = 0.005). Of 21 primary
invasive tumors that demonstrated strong coexpression of
CSF-l receptor and epithelial CSF-l, 19 had strong CSF-l
receptor staining in the corresponding metastasis. There was a
trend (P = 0.08) toward an association between strong coex-
pression of CSF-l receptor and epithelial CSF-l in the primary
tumor and coexpression in the metastases. Fifty of 65 cases that
lacked strong coexpression of CSF- I receptor and epithelial
CSF- 1 in the primary tumor also lacked such coexpression in the
metastases. There was no association between strong coexpres-
sion in the primary tumors and standard factors, such as stage,
histological type, grade, residual disease, age, or performance
status, nor was strong staining for CSF-1 receptor alone or
epithelial CSF-l in the primary tumors a significant prognostic
factor on analysis of this data set.
Metastases. Coexpression of strong staining for CSF- 1
receptor and epithelial CSF-l in the metastases of stage III
invasive carcinomas was significantly predictive (P = 0.043)
of a short disease-free survival (Fig. 3) but not of overall
survival on univariate analysis. The mean disease-free sur-
vival of 13.5 ± 4.0 months for the 18 patients who strongly
coexpressed CSF- I receptor and epithelial CSF- I was cx-
tended to 24. 1 ± 3.9 months for the 44 patients who did not
evince such coexpression. When the subset of patients who
received platinum-based chemotherapy was analyzed in this
manner, the results did not change (P = 0.035). Table 2 lists
the results of univariate analysis of prognostic significance of
various factors in stage III cases. Notably, expression of
either factor alone (epithelial CSF- I or CSF- I receptor) in the
metastases exerts no significant prognostic impact in the
same group in which the combination of cytokine and recep-
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1003
Table 2 Univariate analysis for disease-free survival
stage III cases”
in invasive
Disease-free
survival
Factor Significance (mo)
Grade P = 0.0451 and 2 12.0 ± 2.2
3 19.8 ± 2.7
Residual disease P 0.0001
<2 cm 27.8 ± 3.7
�2 cm 9.4 ± 2.6
Performance status P 0.043
0 and 1 23.2 ± 3.0
�2 8.1 ± 3.8
Age NS5
Histology NS
Expression in Ovary
CSF-l receptor NSEpithelial CSF- 1 NS
Stromal CSF-l NS
Any staining (score � 100) P = 0.042
<100 12.6±2.7�l00 25.1 ± 3.6
CSF-l receptor and epithelial CSF-l NSCSF-l receptor and stromal CSF-l NSEpithelial and stromal CSF-l NS
Expression in metastasis
CSF-1 receptor NSEpithelial CSF-l NS
Stromal CSF-1 NS
<200 19.1 ± 2.8
�200 36.3 ± 10.6
CSF-l receptor and epithelial CSF-l P = 0.043<200 13.5 ± 4.0�200 24.1 ± 3.9
CSF-l receptor and stromal CSF-l NSEpithclial and stromal CSF-l NS
“ Strong antigen staining (score � 200) reported unless otherwise
noted.
‘, NS, not significant.
tor finds significance. For stage III and IV cases, stage, grade,
residual disease, and performance status, but not coexpres-
sion of strong staining for CSF-1 receptor and epithelial
CSF-l in the metastases (P = 0.09) were significant factors
for disease-free survival on univariate analysis.
On multivariate analysis of metastases, the finding of
strong coexpression of CSF-l receptor and epithelial CSF-l of
stage III cases analyzed separately (P = 0.007), or of stage III
and IV cases (P = 0.010), was found to be an independent poor
prognostic factor for disease-free survival (Table 3). These
results were the same when these analyses were performed in
the subset of patients who received platinum-based chemother-
apy (P = 0.005 for stage III; P = 0.007 for stages III and IV).
Among stage III cases, the level of significance of this finding
was only surpassed by that for residual disease (P = 0.004), and
among stage III and IV cases, this factor was only surpassed by
that for stage (P = 0.0004). The relative risk for recurrence if
the metastases strongly expressed both CSF- 1 receptor and
epithelial CSF-1 was increased 2.3-fold in stage III cases and
2.0-fold in stage III and IV cases. Similar (but not as strong)
findings were observed when overall survival was studied by
Table 3 Multivariate analysis for disease-free survival
Relative
Factor Significance risk
Invasive stage III
Grade NS”
Residual disease P = 0.004 1.55
Performance status NS
CSF-l receptor and epithelial CSF-l P = 0.007 2.31
(metastasis)
Invasive stages III and IV
Stage P = 0.0004 2.87
Grade NSResidual disease P 0.032 1.32
Performance status NS
CSF-l receptor and epithelial CSF-l P = 0.010 2.00
(metastasis)
a NS, not significant.
Table 4 Multivariate analysis for overall survival
Factor Significance Relative risk
Invasive stage III
Grade NS#{176}
Residual disease NS
Performance status NS
CSF-l receptor and epithelial CSF-l P = 0.062 1.82
(metastasis)
Invasive stages III & IVStage P = 0.0001 4.01
Grade NS
Residual disease NSPerformance status P 0.077 1 . I 8
CSF- 1 receptor and epithelial CSF- I P = 0.050 1.73(metastasis)
a NS. not significant.
multivariate analysis (Table 4). There was a trend for strong
coexpression of CSF-l receptor and epithelial CSF-l in the
metastases to be an independent poor prognostic factor in stage
III cases (P = 0.062) and also in stage III and IV cases (P =
0.050). These findings did not change when the analysis was
restricted to the patients who received platinum-based chemo-
therapy (P = 0.061 for stage III; P = 0.050 for stages III and
IV). The relative risk for death if the metastases strongly cx-
pressed both CSF-l receptor and epithelial CSF-1 was increased
by 1 .8-fold in stage III cases and by 1 .7-fold in stage III and IV
cases.
Coexpression of strong staining (score � 200) for CSF- 1
receptor and epithelial CSF-l in the metastases was not associ-
ated with any other factor (stage, histological type or grade.
residual disease, age, performance status, stromal CSF- 1 in the
metastasis, or stromal or epithelial CSF-l in the ovary) with the
exception of a significant association with strong expression
(score � 200) of CSF-1 receptor in the ovary (P 0.0 14).
Among stage III and IV, 19 of 22 cases with such coexpression
in the metastasis had strong CSF-l receptor staining in the
primary tumor. Despite this association, strong staining for
CSF- 1 receptor in the ovary alone was not found to be prog-
nostically significant on univariate analysis (Table 2).
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

B- p
. , /
� t1.� /
�
-‘:� �:-� , �.r. �
‘_.�_./ � � � .
1004 CSF- I and CSF- I Receptor in Ovarian Cancer
Significance of Expression of Stromal CSF-1
Primary Tumors. For the entire study group. expression
of stromal CSF-l in the ovary (Fig. 4) was associated with
low-grade tumors (tumors of LMP or grade 1 invasive carcino-
mas: P = 0.033). Among LMP tumors, 92% evinced some
degree (score � 1(X)) of stromal CSF-l staining. Moreover, 31
of the 33 primary ovarian tumors in the study group with no
stronial CSF-l staining (score < 100) were grade 3 invasive
carcinomas. Of the 96 patients whose ovaries had stromal CSF- I
expression, 72 had residual disease <2 cm (P = 0.06), and 89
had residual disease �5 cm (P 0.028). Younger age was
significantly associated with stromal CSF-l expression in the
ovary (P = 0.0()7). Fitly-eight of 69 patients ages �6() years
had strornal CSF- I staining in their primary tumors. Stromal
CSF- I expression was not significantly associated with stage.
perforniance status, histology. or expression of CSF- I receptor
in the primary tumor or metastases. The finding of stromal
CSF-l expression [but not the subset of strong (score � 200)
stromal CSF- I staining] in the ovary was a significant prognos-
tic factor for both disease-free (P 0.046: Fig. 5) and overall
(P = 0.OIS: Fig. 6) survival. The mean disease-free survival of
14.9 ± 2.6 months for the 33 patients with no stromal CSF-l
staining was extended to 30.1 ± 3.1 months for the 96 patients
with stromal CSF-l staining (Fig. 5). Similarly, the mean sur-
vival 0f41 ± 7 months was extended to 49.3 ± 3.3 months for
those with stromal CSF-l staining (Fig. 6). The finding of
stromal CSF- I expression in the ovary retained significance in
the subset of stage III and IV cases (P = 0.014 for disease-free
survival, and P = 0.017 fbroverall survival), as well as for stage
III alone (P = 0.008 fordisease-free survival. and P = 0.012 for
overall survival). However, stromal CSF-l expression (score
� 1(X)) in the primary tumor was not tbund to be an independent
prognostic factor on multivariate analysis for either disease-free
or overall survival.
The significance of the findings of coexpression of CSF- 1
receptor and epithelial CSF-l in the metastases (Fig. 3) contrasts
with that of stromal CSF- 1 expression in the primary tumor: the
latter imparts a protective effect, improving long-term outcomes
(Figs. 5 and 6). The association between stromal CSF-l staining
in the primary tumor and lack of strong coexpression of CSF-l
receptor and epithelial CSF- I in the metastases was not signif-
icant, although the majority of cases (44 of 64) of stromal CSF- I
staining in the primary tumor lacked strong coexpression of
CSF- I receptor and epithelial CSF- I in the metastases. Where
the primary tumors were concerned, there was a significant
association (P = 0.022) between stromal CSF-l staining and
lack of strong coexpression of CSF-l receptor and epithelial
CSF- I : 67 of 94 cases shared those features in the primary
tumors.
Metastases. The significance of stromal CSF- I expres-
sion in the metastases of invasive carcinomas was also evalu-
ated. There were only two LMP implants in which sutTicient
tumor stroma was present to allow for evaluation of stromal
CSF-l staining: in both cases, strong strornal CSF-l staining
was demonstrated. Expression of stromal CSF-l (score � 100)
in the metastases was not found to be a significant prognostic
factor among all stages, among the subsets of stages III and IV,
or among stage III alone. However, strong staining (score
A��’
4T2i:: � :: �I�5�’ ‘I’.,d,/.: � � ,� , �
‘- , .� � ..�-
I � ‘ ,� �:. � ;
� � � #{149} “� #{149} # .)a � � �‘1 b
I � -� � � . ‘
I ,, � � �
�
1.
.� �
44 � � ..,- �‘
:5 1 rn/ : . � ,‘#{149}�..
-� ‘: . � .�, 1,
. ‘. #{149}�5\ �� ,,�. �
- ‘:)law ‘s”�’\’.
% ‘.
Fig. 4 Expression of stromal CSF-l (score � 100) in primary ovarian
carcinomas: A. stromal CSF-l staining in the ovary of a patient with
stage IIIC. LMP papillary serous carcinoma: B, stromal CSF-l staining
in the ovary of a patient with stage lIC. grade I . papillary serous
carcinoma.
� 200) for stromal CSF- 1 in metastases was found to have a
trend toward significance for improved disease-free survival in
stage III cases (P = 0.053: Table 2) but not in stage III and IV
cases. This finding was not found to be a significant factor (P =
0.075) for favorable overall survival in stage III cases, except
when the analysis was restricted to the metastases that evinced
little to no CSF- I receptor expression (P = 0.033). Among stage
III cases, strong stromal CSF- I expression in the metastases was
associated with histological type (P = 0.022) and grade (P =
0.0002) but not with age, residual disease, performance status,
strong staining for CSF- 1 receptor in the metastases, or strong
coexpression of CSF- 1 receptor and epithelial CSF- I in the
metastases. Of 59 cases in which strong stromal CSF- 1 staining
was not expressed in the metastasis, 56 were grade 3. All seven
cases of strong strornal CSF- I staining in the metastases were of
serous or surface serous histology. Of I 8 cases of strong coex-
pression of CSF-l receptor and epithelial CSF-l in the metas-
tases, only 3 metastases also had strong stromal CSF- 1 staining.
DISCUSSION
Despite prior reports of expression of both CSF- 1 and its
receptor in epithelial ovarian cancer specimens, the prognostic
significance of this observation has not been previously inves-
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

ci) 60Cl)
�0 40
C
- stromal CSF-1 + (N=96)
.---- stromal CSF-1 - (N-33)
�P�04�=.046
__ stromal CSF-1 + (N=96)
0 20 40 60 80 100
Time (months)Fig. 6 Overall survival of patients in the entire study group (a I 30)
by stromal CSF-l staining in the primary tumor. Patients with stromal
CSF-l staining (score � 1(X)) in the primary tumor had a significantly
improved overall survival compared to those who did not have stromal
CSF-l staining.
CSF- I -induced secretion of plasminogen activator inhibitor-2
by ovarian cancer cells (21). We have previously found that
elevated levels of plasminogen activator inhibitor-2 in the asci-
tes was associated with a poor prognosis (2 1 ). These represent
at least two mechanisms by which CSF- I could, by binding with
its receptor, enhance neoplastic progression of this disease.
As was observed previously in breast cancers (22). in
ovarian cancers, epithelial CSF- I expression was associated
with some degree of monocytic infiltration. In fact, in this study,
strong epithelial CSF- 1 staining appears to be a prerequisite for
strong CSF- 1 staining in the strornal fibroblasts and monocytes.
Some degree of stromal CSF-l staining in the primary tumors
was a common finding, associated with low-grade tumors and
younger patients, and was significantly predictive of a favorable
prognosis. Importantly, the significance of stromal CSF-l stain-
ing in ovarian cancers contrasts with that of coexpression of
epithelial CSF-l and CSF-l receptor. In the primary tumors.
there was a significant association between stromal CSF- 1 stain-
ing and lack of strong coexpression of CSF-1 receptor and
epithelial CSF-l. It appears that loss of stromal CSF-l in the
primary tumor may be associated with emergence and subse-
quent metastasis of clones that strongly express both CSF- 1
receptor and epithelial CSF- 1 , imparting a poor prognosis. Of
the primary tumors of LMP. 92% evinced some degree of
stromal CSF- I staining, whereas strong coexpression of epithe-
hal CSF- 1 and CSF- I receptor was not seen in any of the cases.
Moreover, strong stromal CSF- 1 staining was also noted in the
LMP implants studied. Thus, although the numbers of LMP
tumors studied are small, our findings in invasive cancers may
relate to the biology of LMP tumors as well.
The fact that enhancement of monocyte migration, differ-
entiation, and activation of macrophages by CSF- I secreted by
tumors cells or stromal fibroblasts may serve to control the
growth of some tumors may in part explain our observations of
the favorable prognostic impact of stromal CSF- 1 expression. In
fact, in mice, an antitumor effect of exogenous CSF- 1 is ob-
served only in the presence of host macrophages activated by
tumor cells (23). However, it is known that the effects of
epithelial CSF-1 on the immunological cells in the stroma can
Clinical Cancer Research 1005
0 20 40 60 80
Time (months)Fig. 5 Disease-free survival of patients in the entire study group (n =
130) by stromal CSF-l staining in the primary tumor. Patients with
stromal CSF-l staining (score � 100) in the primary tumor had a
significantly improved disease-free survival compared to those who did
not have stromal CSF- 1 staining.
tigated. Several reports studying CSF- 1 and CSF- 1 receptor
transcripts in ovarian cancer specimens (6, 19, 20) have corre-
lated their expression with each other; however, neither expres-
sion of CSF-l receptor nor that of CSF-l , in particular, is
restricted to the neoplastic epithelium of those tumors. Reports
using techniques capable of subcellular localization of gene
expression with preservation of the cellular architecture showed
that expression of both epithelial CSF-l and its receptor were
noted in the majority of tumor specimens, along with staining of
the stroma by CSF-l (2, 20). In the current study. we confirm
the observations described previously by us (2): CSF- I receptor
expression is seen in the majority of epithelial ovarian cancers.
and at least one-half coexpress epithelial CSF- 1 . Only 29% of
stromal CSF- I expression was strong. which contrasts with 7 1 (�/�
strong CSF-l receptor staining and 47% strong epithelial CSF- 1
staining. Thus, the effect of autocrine CSF- 1 on epithelial ovar-
ian cancer cells expressing CSF-l receptor may dominate (or
differ from) the paracrine effect of the weaker stromal CSF- 1.
This work describes the independent poor prognostic sig-
nificance of coexpression of strong staining for epithelial CSF- 1
and CSF- I receptor in the metastases both for disease-free and
overall survival. This feature increases the relative risk of re-
currence and of death by 2-fold. Because we believe that bind-
ing of CSF- I to its receptor is relevant to neoplastic progression.
it is notable that the significance of such coexpression is seen in
the metastases and not the primary tumors. Moreover, expres-
sion of either epithelial CSF-l alone or CSF-l receptor alone
exerts no significant prognostic impact in the same group in
which coexpression of cytokine and receptor finds significance.
In addition, coexpression of CSF- 1 receptor and stromal CSF- I
exerted no significant prognostic impact in our study. It appears.
then, that it is the autocrine interactions of receptor and ligand
that impart an aggressive invasive phenotype, rather than the
interaction of epithelial CSF- I receptor and CSF- I from a
paracrine source such as the stroma. We have previously de-
scribed: (a) the enhancement of invasiveness of ovarian cancer
cells by CSF-l (which is mediated through the actions of CSF- I
on urokinase-type plasminogen activator: Ref. 17); and (b) the
I00
C
580
�60Cl)
c40a)C-)
0
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1006 CSF-l and CSF-l Receptor in Ovarian Cancer
be variable. CSF- I has been reported to exert paradoxical im-
munosuppressive effects on macrophages (24); hence, the over-
all picture is complex. Tumor-associated macrophages bearing
the CSF- I receptor served to provide a growth-promoting ac-
tivity for CSF-l-secreting sarcomas (25), and in the op/op
mouse model (in which CSF- I gene mutation leads to a severe
deficiency in macrophage number and function), exogenous
CSF- I enabled macrophages to define stroma to enhance tumor
growth (26).
The results of this study suggest that paracrine effects of
stromal CSF-l on tumor behavior contrast with those dem-
onstrated when the tumor cell is capable of autocrine intra-
cellular or extracellular interactions between CSF-l and its
receptor. Autocrine and exogenous transforming growth fac-
tor �3- I have been described to have opposite effects on gene
expression (27), and in the case of basic fibroblast growth
factor, the different intracellular and extracellular forms can
lead to different phenotypes (28). The secreted forms of
CSF-l may also play different functional roles from the
membrane-bound forms in interacting with the CSF-l recep-
tor (I). In one report, only membrane-bound CSF-l (not the
secreted form) was capable of providing a signal for stimu-
lation of phagocytosis of tumor cells by macrophages (29).
However, although CSF-l expression by the tumor induces
macrophage infiltration, it does not appear to be sufficient to
activate macrophage tumoricidal activity (30). In the sera,
85% of the biologically active CSF- I detected is the long,
secreted form (3 1 ). It is possible that because biologically
detectable CSF- 1 in sera and ascites portends a poor prog-
nosis for ovarian cancer patients and because the bulk of the
tumor burden resides in metastatic sites, the majority of
CSF-l detected may represent CSF-1 from an epithelial
source, rather than from the stroma.
In breast cancers, coexpression of epithelial CSF-l and its
receptor are seen 36% of the time (32). Nuclear staining for
CSF- 1 , in particular, in epithelial breast cancers was found to
correlate with an increased incidence of metastases and poor
survival (22). Because such staining was found to be an mdc-
pendent prognostic factor on multivariate analysis, nuclear
CSF-l expression was hypothesized to reflect activated CSF-l
receptor function in target cells. In our study of ovarian cancer
specimens, the finding of nuclear staining for CSF-l was noted
occasionally but was not a prominent feature and had no clear
prognostic implication. Our finding of the prognostic impor-
tance of coexpression of CSF-l receptor and epithelial CSF-l,
however, demonstrates the biological importance of autocrine
activation of CSF- 1 receptor in ovarian cancers. We are cur-
rently exploring the use of antibodies capable of discriminating
the tyrosine-phosphorylated, activated form of CSF-l receptor
in our ovarian cancer specimens, which may be even a better
indicator of tumor cell autocrine activation of CSF- 1 receptor by
ligand (33).
REFERENCES
I. Sherr, C. J., and Stanley. E. R. Colony-stimulating factor 1 (macro-phage colony-stimulating-factor). In: M. A. Sporn and A. B. Roberts(eds.), Handbook of Experimental Pharmacology, Vol. 95, pp. 667-698.Heidelberg: Springer-Verlag. 1990.
2. Kacinski, B. M., Carter, D., Mittal, K., Yec, L. D., Scata, K. A.,
Donofrio, L., Chambers, S. K., Wang, K., Yang-Feng, 1., Rohrschnei-dcr, L. R., and Rothwcll, V. M. Ovarian adenocarcinomas expressfms-complcmentary transcripts and fms antigen, often with coexpres-sion ofCSF-l. Am. J. Pathol., 137: 135-147, 1990.
3. Kacinski, B. M., Carter, D., Kohorn, E. I., Mittal, K., Bloodgood,
R. S., Donahue, J., Kramer, C. A., Fischer, D., Edwards, R., Chambers,S. K., Chambers, J. 1., and Schwartz, P. E. Oncogenc expression in viva
by ovarian adcnocarcinomas and mixcd-mullcrian tumors. Yale J. Biol.Med., 62: 379-392, 1989.
4. Kacinski, B. M., Carter, D., Mittal, K., Kohorn, E. I., Bloodgood,
R. S., Donahue, J., Donofrio, L., Edwards, R., Schwartz, P. E.,Chambers, J. T., and Chambers, S. K. High level expression of fms
proto-oncogenc mRNA is observed in clinically aggressive human en-
dometrial adenocarcinomas. Int. J. Radiat. Oncol. Biol. Phys., 15: 823-
829. 1988.
5. Ramakrishnan, S., Xu, F. J., Brandt, S. J., Neidel, J. E., Bast, R. C..
and Brown, E. L. Constitutive production of macrophage colony-stim-ulating factor by human ovarian and breast cancer cell lines. J. Clin.Invest., 83: 921-926, 1989.
6. Baiocchi, G., Kavanagh, J. J., Talpaz, M., Wharton, J. T., Guttcrman,J. U., and Kurzrock, R. Expression of the macrophagc colony-stimulat-ing factor and its receptor in gynccologic malignancies. Cancer (Phila.),
67: 990-996, 1991.
7. Rettenmier, C. W., Sacca, R., Furman, W. L., Roussel, M. F., Holt,
J. T.. Nienhuis, A. W., Stanley, E. R., and Shcrr, C. J. Expression of thehuman c-fins proto-oncogene product (colony-stimulating factor- 1 re-ceptor) on peripheral blood mononuclear cells and choriocarcinoma cell
lines. J. Clin. Invest., 77: 1740-1746, 1986.
8. Kacinski, B. M., Scata, K. A., Carter, D., Yce, L. D., Sapi, E., King,
B. L., Chambers, S. K., Jones, M. A., Pirro, M. H., Stanley, E. R., andRohrschncidcr, L. R. FMS (CSF-l receptor) and CSF-l transcripts andprotein arc expressed by human breast carcinomas in viva and in vitro.
Oncogene, 6: 941-952, 1991.
9. Kawasaki, E. S., Ladner, M. B., Wang, A. M., Van Arsdcll, J.,Warren, M. K., Coyne, M. Y., Schwcickart, V. L., Lee, M., Wilson.
K. J., Boosman, A., Stanley, E. R., Ralph, P.. and Mark, D. F. Molecular
cloning of a complementary DNA encoding human macrophagc-spe-
cific colony-stimulating factor (CSF-l ). Science (Washington DC), 230:
291-296, 1985.
10. Chambers, S. K., Wang. Y., Gilmore-Hebert, M., and Kacinski,
B. M. Post-transcriptional regulation of c-fins proto-oncogene exprcs-sion by dexamethasone and of CSF- I in human breast carcinomas in
vitro. Steroids, 59: 514-522, 1994.
II. Lidor, X. J., Xu, F. J., Martinez-Maza, 0., Olt, 0. J., Marks, J. R.,Berchuck, A., Ramakrishnan, S., Berek, J. S., and Bast, R. C., Jr.
Constitutive production of macrophage colony stimulating factor and
intcrleukin-6 by human ovarian surface epithelial cells. Exp. Cell Res.,
207: 332-339, 1993.
12. Kacinski, B. M., Chambers, S. K., Carter, D., Filderman, A. E., and
Stanley, E. R. The macrophage colony stimulating factor CSF-l, anauto- and paracrinc tumor cytokine is also a circulating “tumor marker”
in patients with ovarian, endometrial and pulmonary neoplasms. In: C.A. Dinarello, M. J. Klugcr, M. C. Powanda, and J. J. Oppenheim (eds.).The Physiological and Pathological Effects of Cytokincs, pp. 393-400.New York: Wilcy-Liss, Inc., 1990.
13. Kacinski, B. M., Stanley, E. R., Carter, D., Chambers, J. 1.,
Chambers, S. K., Kohorn, E. I., and Schwartz, P. E. Circulating levelsof CSF-1 (M-CSF) a lymphohematopoictic cytokine may be a usefulmarker of disease status in patients with malignant ovarian neoplasms.
Int. J. Radiat. Oncol. Biol. Phys., /7: 159-164, 1989.
14. Xu, F-J., Ramakrishnan, S., Daly, L., Soper. J. T.. Bcrchuck, A..
Clarke-Pearson, D., and Bast, R. C., Jr. Increased serum levels ofmacrophage colony-stimulating factor in ovarian cancer. Am. J. Obstct.Gynecol., 165: 1356-1362, 1991.
15. Scholl, S., Bascou, C. H., Mosseri, V., Olivares, R., Magdalcnat, H.,Dorval, T., Palangic, T., Validare, P., Pouillart, P., and Stanley, E. R.Circulating levels of colony-stimulating factor I as a prognostic mdi-
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 1007
33. Kacinski, B. M. CSF-l and its receptor in ovarian, endometrial and
breast cancer. Ann. Mcd., 27: 79-85, 1995.
cator in 82 patients with epithelial ovarian cancer. Br. J. Cancer. 62:
342-346, 1994.
16. Price, F. V., Chambers, S. K., Chambers, J. T., Carcangiu. M. L..Schwartz, P. E., Kohorn, E. I., Stanley, E. R., and Kacinski, B. M.
CSF- 1 concentration in primary ascites of ovarian cancer is a significant
predictor of survival. Am. J. Obstct. Gynccol., 168: 520-527, 1993.
17. Chambers, S. K., Wang, Y., Gertz, R. E., and Kacinski, B. M.
Macrophage colony-stimulating factor mediates invasion of ovarian
cancer cells through urokinase. Cancer Res., 55: 1578-1585, 1995.
18. Bacus, S., Flowers, J. L., Press, M. F., Bacus, J. W., and McCarty,K. S., Jr. The evaluation of estrogen receptor in primary breast carci-noma by computer-assisted image analysis. Am. J. Clin. Pathol.. 90:
233-239, 1988.
19. Bauknccht, T., Kiechle-Schwarz, M., du Bois, A., Wolfie, J., andKacinski, B. Expression of transcripts for CSF- I and for the �‘macro-
phage” and “cpithelial” isoforms of the CSF-1R transcripts in humanovarian carcinomas. Cancer Detect. Prey., 18: 231-239, 1994.
20. Kommoss, F., Wolfie, J., Bauknecht, T., Pfistcrcr, J., Kiechle-
Schwartz, M., Pfleidcrcr, A., Sauerbrei, W., Kichl, R., and Kacinski,
B. M. Co-expression of M-CSF transcripts and protein, FMS (M-CSFreceptor) transcripts and protein, and steroid receptor content in adeno-carcinomas of the ovary. J. Pathol.. 174: 1 1 1-1 19, 1994.
21. Chambers, S. K., Gertz, R. E., Ivins, C. M., and Kacinski, B. M. The
significance of urokinase-type plasminogen activator, its inhibitors, and
its receptor in ascites of patients with epithelial ovarian cancer. Cancer
(Phila.), 75: 1627-1633, 1995.
22. Scholl, S. M., Pallud, C., Beuvon, F., Hacenc, K., Stanley, E. R..
Rohrschneider, L., Tang, R., Pouillart, P., and Lidcrcau, R. Anti-colony-stimulating factor-l antibody staining in primary breast adenocarcino-
mas correlates with marked inflammatory cell infiltrates and prognosis.
J. Natl. Cancer Inst., 86: 120-126, 1994.
23. Yoshizawa, H., Ichikawa, K., Yamaguchi, Y., Shinbo, T.,
Takahashi, M., Wakabayashi, M., and Arakawa, M. Cellular interactions
in antitumor efficacy of human macrophage colony stimulating factor
(hM-CSF) in peritoneal tumor dissemination model. Proc. Am. Assoc.Cancer. Res., 37: 450, 1996.
24. Willman, C. L., Stewart, C. C., Miller, V., Tao-Lin, Y., and Tomasi,
1. B. Regulation of MHC class II gene expression in macrophagcs by
hematopoietic colony-stimulating factors (CSF). J. Exp. Med.. 170:
1559-1567. 1989.
25. Bottazzi, B., Erba, E., Nobili, N., Fazioli, F., Rambaldi, A.. and
Mantovani, A. A paracrinc circuit in the regulation of the proliferation
of macrophages infiltrating murinc sarcomas. J. Immunol.. 144: 2409-
2412, 1990.
26. Nowicki, A.. Szenajch, J., Ostrowska, G., Wojtowicz, A.,
Wojtowicz, K., Kruszcwski, A. A., Maruszynski, M., Aukerman, S. L.,
and Wiktor-Jcdrejczak. W. Impaired tumor growth in colony-stimulat-
ing factor I (CSF-I)-dcficicnt, macrophage-deficient op/op mouse: cv-
idcncc for a role of CSF- I dependent macrophages in formation of
tumor stroma. Int. J. Cancer, 65: 1 12-1 19, 1996.
27. Rundhaug, J. E., Park, J., and Fischer, S. M. Autocrinc and exog-
enous transforming growth factor-�3l have opposite effects on the RNA
levels of the 92 kDa type IV collagenase in CH72 cells. Proc. Am.
Assoc. Cancer Res., 37. 92, 1996.
28. Bikfalvi, A.. Klein, S., Pintucci, G., Quarto, N., and Mignatti, P.
Differential modulation of cell phenotype by different molecular
weight forms of basic fibroblast growth factor: possible intracellular
signalling by the high molecular weight forms. J. Cell. Biol., 129:
233-243. 1995.
29. Jadus, M. R., and Wepsic. H. 1. The killing of tumor cells which
express membrane bound M-CSF (mM-CSF) by macrophages. Proc.
Am. Assoc. Cancer Res., 37: 483, 1996.
30. Dorsch, M., Hock, H., Kunzcndorf, U., Diamantstein, T., and
Blankenstein, 1. Macrophage colony-stimulating factor gene transfer
into tumor cells induces macrophage infiltration but not tumor suppres-
sion. Eur. J. Immunol.. 23: 186-190, 1993.
3 1 . Praloran, V. Structure, biosynthesis and biological roles of mono-cyte-macrophage colony stimulating factor (CSF- 1 or M-CSF). Nouv.Rev. Fr. Hematol., 33: 323-333, 1991.
32. Scholl, S. M., Mosseri, V., Tang, R., Beuvon, F., Palud, C.,
Lidereau, R., and Pouillart, P. Expression of colony-stimulating factor- I
and its receptor (the protein product of c-fms) in invasive breast tumor
cells. Ann. NY Acad. Sci.. 698: 131-135, 1993.
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1997;3:999-1007. Clin Cancer Res S K Chambers, B M Kacinski, C M Ivins, et al. stromal CSF-1.epithelial ovarian cancer, contrasted with a protective effect offactor (CSF-1) and CSF-1 receptor: a poor prognostic factor in Overexpression of epithelial macrophage colony-stimulating
Updated version
http://clincancerres.aacrjournals.org/content/3/6/999
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/3/6/999To request permission to re-use all or part of this article, use this link
Research. on March 7, 2021. © 1997 American Association for Cancerclincancerres.aacrjournals.org Downloaded from