Embed Size (px)
Citation preview

CRUSH SYNDROMECRUSH SYNDROMEICD 10: ICD 10: T79.5T79.5
Mohit ChhabraRoll no. : 47

OBJECTIVESOBJECTIVESDefine and understand the
pathophysiology of Crush Syndrome
Clinical diagnosis and relevant investigation
Management

A Case of Crush A Case of Crush Syndrome….Syndrome….

Clinical FeaturesClinical Features
Lower limb injury with pain and swelling, which later on developed anesthesia and motor disturbance
Signs of hypovolemic shockTea-colored urine, maybe oliguriaNausea and confusion
Pathophysiology


On Investigating further….On Investigating further….
Hyperkalemia & hypocalcaemiaECG changes secondary to
hyperkalemiaMetabolic acidosisRaised Creatine KinaseElevated UREA and CREATININEMyoglobinuriaEvidence of D.I.C.

Diagnosis: Crush Diagnosis: Crush SyndromeSyndromeDefinition:
◦ A severe, often fatal condition that follows a severe crushing injury, particularly involving large muscle masses, characterized by fluid and blood loss, shock, hematuria, and renal failure. Also known as compression syndrome. (McGraw Hill Dictionary)
◦ In a nutshell: TRAUMATIC RHABDOMYOLYSIS due to crushing
◦Also known as Bywaters Syndrome/ Reperfusion injury

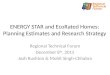
PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Clinical Features

KIDNEY IS IN DANGER AS SOON AS WE RELIEVE THE COMPRESSION
Renal hypoperfusion + Renal Tubular Necrosis = Renal Failure

MANAGEMENTMANAGEMENTInitial Management:
1. Follow the usual criteria of A-B-C as injuries are massive and high chances of poly-trauma
2. Early and rapid rehydration3. Venous access preferably before the limb is
decompressed4. CVP and urinary catheterization for monitoring

Further Management1. Large amount of saline infusion with forced
diuresis2. Debridement of crushed tissue and a
fasciotomy for compartment syndrome3. Dialysis if renal failure sets in4. Amputation as the last resort if massive
limb injury is there and we have to prevent crush syndrome