Embed Size (px)
Citation preview

CroniconO P E N A C C E S S EC DENTAL SCIENCE
Review Article
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian
Patients with Obstructive Sleep Apnea
Mayank Gahlot*Specialist Orthodontist, Primacare Speciality Clinic, Dubai, UAE
*Corresponding Author: Mayank Gahlot, Specialist Orthodontist, Primacare Speciality Clinic, Dubai, UAE.
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fu-sion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Received: December 13, 2018; Published: January 29, 2019
Abstract
Keywords: Obstructive Sleep Apnea (OSA); Orthopantomogram (OPG); Cone Beam CT (CBCT)
Introduction
Obstructive sleep apnea (OSA) is an under-recognized and under-diagnosed medical condition often termed as a “silent killer” that effects more than 5% of the individuals in the United states as well as 7% worldwide. Symptoms range from daytime sleepiness, loud snoring, and restless sleep. While the “gold standard” of its diagnosis still remains the overnight sleep study also known as poly-somnography, a detailed history and focused physical examination along with various skeletal and soft tissue markers, may help in the early diagnosis of the condition. Essential diagnostic records for any Orthodontic treatment consists of a number of skeletal and soft tissue assessments in the form of Orthopantomogram (OPG) and Lateral Cephalogram which are imperative for the commence-ment of the treatment. Also, Cone beam CT (CBCT) evaluation is done for certain specific cases. Several modalities exist for treating obstructive sleep apnea, including continuous positive airway pressure, oral appliances, and several surgical procedures. With more and more people becoming vigilant about OSA, there is an ever increasing demand in the medical and dental field to establish a rela-tionship between the Craniofacial pattern, cervical vertebrae with airway volumetric dimensions with Body Mass Index, neck circum-ference etc. in order to effectively diagnose the syndrome and provide additional methods of diagnosis along with Polysomnography.
Obstructive sleep apnea syndrome (OSAS) is a sleep disorder characterized by recurrent episodes of partial or complete collapse of the upper airway during sleep leading to oxygen desaturation and sleep fragmentation. Apnea, derived from the Greek word meaning “without breath”, is defined by the American Academy of Sleep Medicine (AASM) as the cessation of airflow for at least 10 seconds [1]. The health consequences of hypoxemia and sleep disruption due to obstructive sleep apnea leads to excessive daytime sleepiness, impaired memory, cognitive dysfunction, effecting work performance, and demoting the health-related quality of life.
OSA is prevalent, in both adult and child with an increase with advancing age. The estimated prevalence is 2% for women and 4% for men in the European population [2,3] with similar data from epidemiologic study from the United States [4,5]. Recent research indicates increasing prevalence with 4% for women and 9% for men [6]. A population-based survey from North India estimated the prevalence of OSAS at 3.6% with 4.9% for males and 2.1% for females [7]. In another study the estimated population prevalence of OSA and OSAS was 9.3% and 2.8% respectively [8].
Predisposing factors like gender, age, narrow airway, craniofacial deformities, muscular hypotony, sleep posture, and fatty deposits in the tissues of the upper airway are some of the important considerations. Studies indicate a co-relation between BMI, Neck circumference and Mallampati index and the severity of OSA [9-11]. Neck circumference has been suggested to be predictive of obstructive sleep apnoea than general obesity. Combining neck circumference with other signs and symptoms may allow the clinical diagnosis or exclusion of sleep apnoea to be made with reasonable confidence [11,12].
The relationship between structure and function along with the upper airway anatomy is an important consideration in the patho-physiology of OSA. Reduced posterior airway space may be associated with abnormally long soft palate, low position of the hyoid bone, and extended head posture [13,15]. It is generally agreed that the jaws are more retrognathic than normal and the vertical dimension of the jaws is increased in patients with sleep apnea [14].

304
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea
Aims and Objectives
Consensus exists that patients with sleep apnea have an extended head posture which improves airway space in the pharyngeal area [16-21]. Literature reports states cervical spine development to be related to craniofacial malocclusions [20,22,23]. The fusion anomalies of the cervical column occurred significantly more often in the sleep apnea group compared with subjects with neutral occlusion and normal craniofacial morphology [24,25].
The sample was equally divided into three groups, Group 1, 2 and 3, on the basis of severity of OSA into mild, moderate and severe respectively, with no gender bias. Severity of OSA was established by examining the Apnea-Hypopnea Index (AHI) of patients on the ba-sis of the results of sleep study. AHI of < 15 was considered mild, 15 - 30 as moderate and > 30 as severe Obstructive sleep apnea (Table 1). 05 patients with no airway related issues were randomly selected from the imaging centre. This group was designated as “Group 0” and treated as the control group. Care was taken to ensure they were North Indian but full confidentiality of their personal details was achieved as the imaging centre masked the relevant information.
Traditionally, airway assessment was conducted in an orthodontic office on a 2D cephalogram which provided limited information re-stricted to the sagittal dimension only with no inputs on the important transverse dimension. With the recent advent of CBCT technology into dentistry, the airway can now be assessed with increased accuracy in all dimensions [26-33].
A lacuna of knowledge exists on information related to the North Indian population affected with OSA. Volumetric 3D assessment of airway and its relationship to the craniofacial and cervical morphology has not been reported on this population type. The critical char-acteristics of neck circumference, BMI and Mallampati index have not been correlated with craniofacial and cervical vertebra morphology with airway dimensions.
Hence, this study was undertaken to assess the relationship between the airway volumetric dimensions with BMI, neck circumference and Mallampati index. The study also aimed to ascertain if co-relation existed between severity of OSA, craniofacial pattern, cervical ver-tebra fusion and volumetric dimensions of the airway. The differences between a control (Non OSA group) and the OSA affected patients was also studied.
1. To assess the cross-sectional area and volume of airway and establish minimal axial area in patients with mild, moderate and severe obstructive sleep apnea and control group.
2. To assess the skeletal craniofacial parameters and cranio-cervical angulations of patients with mild, moderate and severe obstructive sleep apnea and control group.
3. To evaluate BMI, Neck Circumference and Mallampati Index of patients with mild, moderate and severe obstructive sleep apnea and control group.
4. To evaluate the length and width of soft palate and tongue in patients with mild, moderate and severe obstructive sleep apnea and control group.
5. Evaluate the cervical vertebrae morphology with emphasise on fusion anomalies in patients with mild, moderate and severe obstructive sleep apnea and control group.
6. To evaluate if differences existed between the three OSA affected groups and non OSA (Control group) and if diagnostic parameters for OSA could be identified for North Indian population.
Materials and Methods
The study was conducted at Dept. of Orthodontics and Dentofacial Orthopaedics, of a prominent North Indian Dental College as well as a Sleep Centre in New Delhi was selected for patient’s to undergo overnight sleep study, and finally Dental and Maxillofacial Diagnostics was considered for the various radiological inferences that were to made. The study was commenced after appropriate ethical clearance by the Institutional Ethical Committee (Ref. No: DJD/IEC/01/2009), and obtaining informed consent from each patient prior to the study. A total of 15 pre-diagnosed OSA patients, in the age group of 30 - 50 years with a mean age group of 40 year were included in the study. The patients were diagnosed for OSA with the help of an overnight sleep study by using Polysomnography.

305
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
1. Height of the patients was measured using Stadiometer and weight with digital weighing scale (TAYLOR) with high accuracy (Figure 1).
2. Neck circumference (In Inches) of the patients was measured (at the level of cricothyroid cartilage) using a standard roll up non-distensible measuring tape (Figure 2).
3. Intra-Oral photographs were captured with a high precision SLR camera (NIKKON D60) (Figure 3). The photographs were used to score the Mallampati Index.
General extra and intra oral records
Group (n = 15) Apnea-Hypopnea Index Score (AHI) Severity of OSA1 (n = 5) < 15 Mild2 (n = 5) 15 - 30 Moderate3 (n = 5) > 30 Severe0 (n = 5) - Control
Table 1: Sample distribution.
Figure 1: Height measurement instrument: stadiometer.
Figure 2: Neck circumference.
Figure 3: Digital SLR camera (Nikon D60).
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

306
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
The polysomnographic reports for all the patients were obtained after overnight Polysomnography which provided inputs on AHI, SPO2, PaO2, Total sleep time (REM and NREM) and Apenic and Hypopnic events (Figure 4). A total 11 parameters were assessed during the overnight polysomnographic evaluation. The AHI score was obtained from the polysomnography.
Polysomnography records
Figure 4: Patient undergoing overnight polysomnography.
The CBCT scans of the study subjects were obtained using CS 3000 (Care Stream 3000) hardware (Figure 5). A standardized field of view (FOV) of 17 cm x 30 cm and voxel size of 300 mm was maintained for all the scans. The patients were positioned upright, with chin rest for the support in maximum intercuspation (MIP). CBCT generated axial, coronal and sagittal sections were captured and analyzed with the help of Xelis 3D software (version 4.0, U. S.) with the minimum thickness of the slice being 0.3 mm and Dolphin3D software (ver-sion 11.7, Dolphin Imaging and Management Solutions, Chatsworth, Calif).
Cone beam computerized tomography (CBCT) records
Figure 5: Carestream 3000.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

307
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Figure 6: Mallampati index.
Evaluation of the diagnostic recordsGeneral extra and intra oral records
• Body Mass Index: The body mass index (BMI), or Quetelet index, is a heuristic proxy for human body fat based on an individual’s weight and height. The values for height and weight of each patient were placed in the formulae for the BMI calculator and BMI score was obtained.
• Neck circumference: Neck circumference of the patients was measured using a standard roll up measuring tape and tabulated. The measurement was done below the submental/submandibular region, approximately middle of the neck.
• Mallampati Index: The intra-oral photographs were assessed to designate the grades of Mallampati index for the patients included in the study (Figure 6).
CBCT evaluation
Craniofacial morphology, airway, tongue, soft palate and cervical vertebra fusion anomalies of each patient were assessed on the Axial, Coronal and Sagittal sections on the DICOM images captured by the CBCT scans.
To measure the transverse, sagittal and vertical dimensions on the CBCT generated lateral cephalogram, Axial Multiplaner Reconstruc-tion (MPR) and Maximum intensity projection (MIP) images were formatted.
These images were studied with the help of a Xelis software and Dolphin 3D and cross-sectional, linear and angular measurements were done with the help of tools provided with the software.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

308
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Figure 7a and 7b: Measurement of soft palate and tongue.
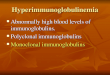
Mid-sagittal section of the DICOM image was assessed for the evaluation of tongue. The length of the tongue was measured as the linear distance from point E (epiglottis) to the tip of the tongue. The width of tongue was recorded as the linear distance between the midpoint of E-TT (tongue length) and the most prominent point on the dorsum of the tongue (Figure 7b).
The Mid-Sagittal Plane was established by coordinating the horizontal and vertical grid in all the three planes on axial, coronal and sagittal section of the 3D images. Once all the three sections were coordinated, the vertical arm of the grid was placed on the three dimen-sional CBCT image and the tool of MIP was selected to obtain a CBCT generated Lateral Cephalogram.
Assessment of cervical vertebrae fusion anomalies
• C1, C2, C3 and C4 were assessed visually for fusion anomalies on the 3D image and the CBCT generated lateral cephalogram. The image was assessed from the right and left lateral along with image rotation for clear observation from the posterior and basal aspect.
• Fusion anomalies were recorded as - a) Fusion of the body of the second and third cervical vertebrae (C2 and C3), b) Block fusion- when two or more vertebrae bodies were fused and c) Occipitalization - when occipitalization of C1 and the occipital bone occurred (Figure 13).
Assessment of shape of the soft palate
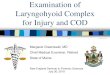
Soft palate measurements were made on the mid-sagittal slice on the CBCT, for the evaluating the shape of the soft palate (Figure 7a). The shape of the soft palate was assessed form the PNS till the Valleculae. The outline of the soft palate was traced and the shape assessed and classified into any of the six morphological varieties, i.e. “Leaf”, “Rat tail”, “Butt Like”, “Straight Line”, “S-Shaped” and “Crook Shaped” (Figure 8).
Assessment of tongue
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

309
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Figure 8: Classification of soft palate.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

310
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
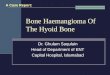
Pharyngeal airway dimensions were measured for all patients at four levels - ranging from the point on the soft palate closest to the dorsal pharyngeal wall to the vallecula of the epiglottis (Figure 9). The areas measured were - a) Soft palate closest to the dorsal pharyn-geal wall between anterior and posterior and Valem palati (Ve-PVe), b) Tip of the uvula and posterior border on airway (Uv-PUv), c) Radix linguae to the posterior border (Rl-PRl) and d) From the Vallecula epiglottis to the posterior border (Va-PVa) (Figure 9).
Figure 9: Pharyngeal airway dimensions.
• The DICOM images of the subjects were imported in Dolphin3D software (version 11.7, Dolphin Imaging and Management Solutions, Chatsworth, Calif.).
• Upper airway volumes were measured at (1) Nasopharynx (OP) and (2) Oropharynx (NP). In addition, the area of maximum constriction of airway was identified and the constricted volume measured to assess the most compromised airway volume.
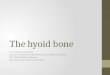
• The nasopharyngeal (NP) volume was measured between the last slice before the nasal septum fused with the posterior wall of the pharynx and the palatal plane (which was the superior limit of the OP airway). Hence, the image was manipulated such that the superior border of the NP was defined on the axial slice first and then it was reflected to the sagittal plane (Figure 10).
• The oropharyngeal (OP) volume was defined as volume between the palatal plane (ANS-PNS) extending to the posterior wall of the pharynx and the plane parallel to the palatal plane that passes from the most anterioinferior point of the second cervical vertebrae. This was also established in the similar manner (Figure 11).
• The software capability was extended to identify the region of maximum constriction and a volumetric measure of the same was done in order to ascertain the extent of airway compromise (Figure 12 and 13).
All measurements were conducted by a single investigator. The measurements were repeated randomly for five cases at a 4 week in-terval by the same operator to check for intra operator errors. No significant intra operator error was found.
Cross sectional area assessment of airway
Volumetric assessment of airway
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

311
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Figure 10: 3D reconstruction of nasopharyngeal airway.
Figure 11: 3D reconstruction of oropharyngeal airway.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

312
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Figure 12a and 12b: Area and volumetric reconstruction of airway.
Figure 13: Measurement: cranio-cervical angle.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

313
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
The orthodontic interest to the airway is related to the dramatic effect that nasorespiratory function has on craniofacial growth and development of the dentofacial complex. It probably dates back to the first description of adenoid hypertrophy. Adenoidectomy was first performed in Copenhagen by Wilhelm Meyer [34], a Danish physician. Rubin RM [35] in his article described the term Adenoid Facies or Long Face Syndrome which was coined by CV Tomas in 1872, which describe dentofacial changes associated with chronic nasal airway obstruction along with mouth breathing. Osler W [36] coined the term “Pickwickian” after Charles Dickens’s description of Joe in refer-ring to obese, hyper somnolent patients and stated “an extraordinary phenomenon in excessively fat young people is an uncontrollable tendency to sleep” [37].
Review of Literature
Sato K., et al. [41] in their study examined the effectiveness of craniofacial morphology and pharyngeal airway morphology analysis and found significant posterior position and backward rotation of the mandible and stenosis of the nasopharyngeal airway and an elon-gated soft palate compared with controls. In another study by Lowe AA., et al. [42] interaction between airway and tongue structures were quantified. They concluded that tongue volume increased rapidly than airway volume in subjects with OSA. Grauer D [43] conducted a study to assess differences in airway shape and volume. No differences in airway volumes related to vertical facial proportions were found. Skeletal Class II patients often had forward inclination of the airway, whereas skeletal Class III patients had amore vertically ori-ented airway.
Sonnesen L and Kjær I [44] were one of the first to examine and compare the cervical column morphology of adults. They found that the most important factor for posterior arch deficiency was mandibular inclination. Arntsena T, Sonnesen L [23] conducted a study in pre-orthodontic children. In their study, new associations were found between cervical column morphology, craniofacial morphology, and head posture.
A population-based survey from North India was conducted by Sharma SK, Kumpawat S, Banga A, Goel A [7] which estimated the prevalence of OSAS at 3.6% (males and females being 4.9 and 2.1% respectively). The prevalence of OSA in the same study was 13.7 percent. However, this prevalence study was conducted in a semi-urban Indian population with a small sample size without adequately studying different socio-economic strata. Another study by Reddy EV, Kadhiravan T, Mishra HK, Sreenivas V, Handa KK, Sinha S, Sharma SK [8] determined the prevalence and risk factors of OSA in middle-aged urban Indian population. The study was conducted as a two-stage, cross-sectional, community-based study in four different socioeconomic zones of the South Delhi district, India, from April 2005 to June 2007. A linear trend was observed in the prevalence of OSA across the socioeconomic strata. OSA is a significant public health problem in the middle-aged Indian population across the socioeconomic spectrum.
Cephalometrics were used to evaluate the posterior airway space by Guilleminault C [38] and Ceylan I and Oktay H [39], whereas John-ston CD and Richardson A [40] conducted a cephalometric study and investigated morphological changes occurring in the pharynx. The nasopharyngeal skeletal dimensions were unchanged but a tendency towards longer and thicker soft palate and narrower oropharynx during adulthood was seen.
Liistro G., et al. [45] measured nasal patency, Mallampati Index (MI), neck circumference and body mass index of OSA patients and concluded that high Mallampati score represents a predisposing factor for OSAS, especially if it is associated with nasal obstruction. A similar study was conducted by Nuckton TJ., et al. [46], to assess the clinical usefulness of the Mallampati score in patients with OSA. They concluded that a scoring system will have practical value in clinical settings Kawaguchi Y [47] conducted a study to investigate the significance of neck circumference (NC) on the presence and severity of obstructive sleep apnea (OSA). In conclusion, NC was found to be associated with the severity of OSA independently of visceral obesity, especially in non-obese patients.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

314
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Data was subjected to various statistical tests like One-Way Anova, T-Test, Kruskall Wallis Test and Mann Whitney Test. Descriptive statistics were applied to all the groups together which showed that the patients affected with severe OSA had anteclination of maxilla, retrognathic mandible with increased ANB (Table 2). One-way Anova was applied on all the three groups which showed a significant dif-ference (P < 0.05) in the effective length of maxilla and posterior position of maxilla between the mild, moderate and severe groups (Table 3). Mann- Whitney test shows a very high significant difference (P < 0.01) in effective length and posterior position of maxilla in mild and severe groups (Table 4). Mann- Whitney test showed a high significance (P < 0.01) in the effective length of mandible and significant dif-ference (P < 0.05) in saddle angle between mild and moderate groups (Table 5).
Results
Mild Moderate Severe ControlMean SD SE Mean SD SE Mean SD SE Mean SD SE
SNA 30.7300 2.7306 1.2435 32.1200 2.4243 1.0342 33.6600 4.7643 2.1309 33.1000 1.9761 .3337MAX. P.
POS.14.0600 1.1233 .5046 17.1300 2.1033 .9431 14.5600 23954 1.0713 15.7300 3.1523 1.4093
EL 39.9000 2.5603 1.1450 34.9400 2.5735 1.1509 35.6400 3.6473 1.6311 33.5200 3.4230 3.7669ANGLE OF INC.
68.6400 33.8420 15.1346 35.3000 2.2353 1.0223 83.1600 .9915 .4434 87.2600 1.3012 .5819
SNB 79.0200 2.3164 1.2595 73.4400 .6139 .2763 73.4400 3.9935 1.7332 30.7600 1.2992 .5310SN
(Go-Gn)
27.7400 3.7166 1.6621 29.7400 2.0912 .9352 27.3600 3.2476 3.6334 23.5000 2.3627 1.2302
MAND. EL
119.1200 1.4305 .6621 105.3000 6.0667 2.7131 87.5800 42.5412 19.0250 109.1800 7.5374 33708
MPA 19.1200 6.7906 3.0363 22.2300 3.7793 1.6904 22.5300 2.9440 1.3166 22.3200 3.7446 1.6746LOW. Go.
63.6400 1.9731 .3324 67.4600 3.1037 1.3330 64.6200 9.5290 4.2615 69.2200 5.6322 2.5133
SAD-DLE
127.6000 2.3022 1.0296 123.0000 3.5355 1.5811 124.2000 4.7645 11307 121.0000 7.7136 3.4496
ANB 1.8400 2.0852 .9325 3.6800 1.8180 .S399 5.2200 1.5659 .7003 2.3400 1.8501 .8274
Table 2
ANOVASum of Squares df Mean Square F Siq.
SNA Between Groups 20.769 2 10385 258 .448Within Groups 145.248 12 12.104
Total 166.017 14Po P Between Groups 28.081 2 14.041 3.676 .057
Within Groups 45.832 12 3.819Total 73.913 14
EL Between Groups 72.065 2 36.033 4.082 .044Within Groups 105.924 12 8227
Total 177.989 14ANGLE Between Groups 821.609 2 410.805 1.070 .373
Within Groups 4605.944 12 383.829Total 5427.553 14
Table 3: One way anova: maxilla.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

315
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
T-Test showed a significant difference (P < 0.05) i.e. at the level of tip of the uvula of the soft palate and the posterior border on airway (SAG2), Radix linguae to the posterior border on airway (SAG3), its corresponding area measurement of the axial section (AREA3) and from the Vallecula epiglottis to the to the posterior border on airway (SAG4) between the mild and severe groups. A Significant difference (P < 0.01) was seen between AREA1, AREA2, AREA3 and AREA4 and (P < 0.05) at SAG1 in severe and control groups (Table 6).
Test Statistic b
SNA PoP EL ANGLEMann-Whitney U
Wilcoxon W
Z
Asymp. Sig. (2-tailed)
Exact Sig. [2*(1-tailed Sig.)]
7.000 22.000 -1.149
.251
.310a
.000
15.000
-2.619
.009
.008a
.000
15.000
-2.611
.009
.008a
4.500
19.500
-1.676
.094
.095a
Table 4: Mann-Whitney test: Maxilla.a: Not corrected for ties.b: Grouping Variable: GR.
Test Statisticsb
EL SNB SN Go Gn MPA GON SADOMann-Whitney U
Wilcoxon W
Z
Asymp. Sig. (2-tailed)
Exact Sig. [2*(1-tailed Sig.)]
.000
15.000
-2.611
.009
.008a
6.500
21.500
-1.257
.209
.222a
10.000
25.000
-.524
.600
.690a
7.500 22.500 -1.048
.295
.310a
4.000
19.000
-1.776
.076
.095a
2.500
17.500
-2.102
.036
.032a
Table 5: Snake Wallis Test: Mandible: Mild vs Moderate.a: Not corrected for ties.
b: Grouping Variable: Group.
Levant’s Test for Equality of Variances
t-test for Equality of Means
F Sig. t df Sig. (2-tailed)
Mean Difference
Std. Error Difference
95% Confidence interval of the
DifferenceUpper Lower
AREAl Equal variances assumed 2.291 .169 3.649 8 .007** -152.4800 41.7843 -248.834 -56.1252
AREA2 Equal variances assumed .134 .723 3.860 8 .005** -165.3600 42.8359 -264.139 -66.5803
AREA3 Equal variances assumed 3.523 .097 -2.904 8 .020 -152.4200 52.4832 -273.446 -31.3936AREA4 Equal variances assumed 1.992 .196 -2.336 8 .048* -111.7000 47.8194 -221.971 -1.4284
SAG1 Equal variances assumed .657 .441 3.436 8 .009** -4.8200 1.4030 -8.0553 -1.5847SAG2 Equal variances assumed 1.607 .241 -2.146 8 .064 -5.8600 2.7307 -12.1570 .4370SAG3 Equal variances assumed .006 .941 -1.728 8 .122 -3.5000 2.0260 -8.1720 1.1720SAGO Equal variances assumed 7.127 .028 -2.162 8 .063 -5.3400 2.4698 -11.0354 .3554
Table 6: Inter group comparison: independent T-Test: severe v/s control.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

316
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
According to the descriptive statistics, Soft Palate increased both in length and width and airway was seen to be compromised severely at the retro-palatal region. Width of the tongue also seemed to have a positive co-relation with the severity of OSA (Table 7). Whereas, Intergroup comparison showed a Statistically significance difference (P < 0.05) in soft palate width (Table 8).
Mild Moderate Severe ControlMean SD SE Mean SD SE Mean SD SE Mean SD SE
SPL 38.640 6.3830 2.8546 41.4200 3.8232 1.7098 45.9200 5.0281 2.2486 38.8000 8.0172 3.5854SPW 11.760 1.9540 .8738 14.2200 .2280 .1020 15.3200 2.4884 1.1128 10.0300 1.7936 .8021TW 78.060 6.1052 2.7303 80.5200 9.3106 4.1638 81.3200 4.7851 2.1400 36.0000 4.6293 2.0703TL 30.160 2.4643 1.1021 30.5400 2.7337 1.2225 25.7400 4.6683 2.0877 65.0000 11.7156 5.2394
Table 7: Descriptive statistics: soft palate and tongue.
Levene’s Test for Equality of Variances t-test for Equality of Means
F Sig. t df Sig. (2-tailed)
Mean Difference
Std. Error Difference
95% Confidence Interval of the Difference
Upper LowerSPL Equal variances
assumed.979 .351 -.335 8 .423 -2.7300 3.3275 -10.4531 4.3931
SPCC Equal variances assumed
7.480 .026 -2.796 8 .023* -2.4600 .8798 -4.4888 -.4312
TL Equal variances assumed
3.071 .113 -.494 8 .635 -2.4600 4.9792 -13.9420 9.0220
TW Equal variances assumed
.616 .455 -.231 8 .323 -.3300 1.6460 4.1756 3.4156
Table 8: Inter Group comparison: independent T-Test: mild vs moderate.
The oropharyngeal airway essentially consists of muscles and soft tissue but lacks a rigid or bony support. It is enclosed along its length by nasal turbinates, hard palate, mandible, hyoid and cervical vertebrae and soft tissues which include the tongue, soft palate, ton-sillar pillars, pharyngeal mucosa, muscles, fat pads, epiglottis and blood vessels of the neck.
Discussion
Katz., et al. and Kawaguchi., et al. [47] conducted separate studies to investigate the significance of neck circumference (NC) on the presence and severity of obstructive sleep apnea (OSA) syndrome independent of obesity. The results of the current study were in concur-rence with these studies and showed an increase in the neck circumference with an increase in AHI in all the experimental groups which was statistically significant. Mallampati Index has been used as a guide by anaesthetists and surgeons alike in airway assessment. Liistro., et al. [45] concluded that a high Mallampati score represents a predisposing factor for obstructive sleep apnea syndrome. The results of the current study indicated that the Mallampati index worsened with the increase in severity of AHI.
You., et al. [48] studied variations in velar morphology and classified them into six different types based on the shape related anatomic variations. Literature search did not reveal any previous study where the anatomic shape of the soft palate was correlated with the sever-ity of OSA. Current study concludes that morphology may be responsible for the obstruction due to its increased thickness in the basilar region. Ryan., et al. [49] and Lowe., et al. [42] observed that tongue volume was larger in OSA patients which was associated with reduced airway volumes. In the current study, width of the tongue was found to be significantly increased in the entire OSA group. However, a re-duced tongue length was seen in all the OSA groups compared to the control group.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

317
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Bibliography
Arntsena and Sonnesen., et al. [23] assessed cervical vertebrae morphology in non-syndromic patients and patients with OSA and con-cluded that fusion of the cervical vertebra column is associated with development and function of the craniofacial morphology. Whereas, current study was unable to decipher any cervical vertebrae fusion anomalies in the groups studied. Further studies with large sample size may help in establishing a relationship between the cervical vertebrae fusion anomalies and severity of OSA.
Solow., et al. [50] measured pharyngeal airway diameters at seven different levels starting from the maxillary tuberosity to the val-lecula of the epiglottis. However, in the current study, sagittal airway dimension were measured at four levels and area cross section was assessed in all three OSA groups and compared amongst themselves and against the control. A significant reduction in the width was seen in all 3 OSA Groups where severe OSA group exhibited a significant reduction in mean area cross section at all the four levels.
Intergroup comparison showed that the mild OSA group exhibited a significant increase in the lower gonial angle which is suggestive of patients exhibiting a vertical growth pattern. This group also showed an ante inclination of maxilla which was statistically significant. Additionally, the study also showed opening of the saddle angle and an increase in ANB in the patients with mild OSA. An increase in saddle angle would denote an upward inclined anterior cranial base and/or posteriorly positioned glenoid fossa.
BMI, Neck circumference and Mallampati Index are important diagnostic parameters in the study of sleep related breathing disorders. It may be worthwhile to include these in our orthodontic case assessment sheet in patients suspected to have airway related issues. The length and width of soft palate may be considered as important incriminating factors in effecting OSA in the patients studied. Width of the tongue seemed to have a positive co-relation with the severity of OSA.
Conclusion
Various studies have focused on the association between the craniofacial relationships and OSA on the basis of skeletal class I, II and III. The current study makes an attempt to establish association of various craniofacial parameters with the severity of OSA vis a vis the control group. Baik., et al. [51] and Enache., et al. [52] reported positive correlation of retrognathia, micrognathia, and skeletal Class II with Retro palatal (Rp) airway obstruction. On the other hand, Lamaco., et al. [53] found no difference in the maxillary or mandibular prognathism between the two OSA groups studied. Results of the current study showed a statistically significant increase in the ANB values with increasing severity of OSA. The maxillo-mandibular Sagittal difference (ANB) was indicative of skeletal class II pattern and the OSA patients in the moderate and severe group exhibited skeletal mandibular deficiency. Enlow’s Counterpart Principle explains that maxillary length and nasopharyngeal space are counterparts in the process of growth and development. Hence, the reduction in maxillary effective length would significantly affect the nasopharyngeal airway.
Mild OSA group presented with increased cranio-cervical angulation, increased saddle angle and increased ANB due to retrognathic mandible. Maxilla exhibited ante-inclination additionally there was increased gonial angle showing a vertical growth pattern. Patients affected with severe OSA had anatomically reduced maxillary length and retrognathic mandible with increased ANB. Cross sectional area of airway was significantly reduced in the mild group compared to the controls which further worsened with increasing severity of OSA. Clinical features of increased neck circumference, increased body mass index and severe Mallampati index were seen. The soft palate increased both in length and width and the airway was compromised severely at the retro-palatal region.
1. American Academy of Sleep Medicine. “International Classification of Sleep Disorders”. In: Diagnostic and Coding Manual. Second Edition. Westchester, Ill: American Academy of Sleep Medicine (2005).
2. Young T., et al. “The occurrence of sleep-disordered breathing among middle-aged adults”. New England Journal of Medicine 328.17 (1993): 1230-1235.
3. Centers for Medicare and Medicaid Services. Decision Memo for Continuous Positive Airway Pressure (CPAP) Therapy for Obstruc-tive Sleep Apnea (OSA) (CAG-00093R2). Available from: US Department of Health and Human Services (2010).
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

318
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
4. Goetting C and Downey R III. Sick, symptomatic and undiagnosed. San Antonio, TX. Paper to be presented at the Annual Meeting of the Association of Professional Sleep Society (2010).
5. Schwab RJ., et al. “Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic reso-nance imaging”. American Journal of Respiratory and Critical Care Medicine 168.5 (2003): 522-530.
6. Johnson EO and Roth T. “An epidemiologic study of sleep-disordered breathing symptoms among adolescents”. Sleep 29.9 (2006): 1135-1142.
7. Sharma SK., et al. “Prevalence and risk factors of obstructive sleep apnoea syndrome in a population of Delhi, India”. Chest 130.1 (2006): 149-156.
8. Reddy EV., et al. “Prevalence and risk factors of obstructive sleep apnea among middle-aged urban Indians: A community-based study”. Sleep Medicine 10.8 (2009): 913-918.
9. Cakirer B., et al. “The relationship between craniofacial morphology and obstructive sleep apnea in whites and in African-Ameri-cans”. American Journal of Respiratory and Critical Care Medicine 163.4 (2001): 947-950.
10. Dagan Y., et al. “Body Mass Index (BMI) as a first-line screening criterion for detection of excessive daytime sleepiness among profes-sional drivers”. Traffic Injury Prevention 7.1 (2006): 44-48.
11. Davies RJ., et al. “Neck circumference and other clinical features in the diagnosis of the obstructive sleep apnoea syndrome”. Thorax 47.2 (1992): 101-105.
12. Patil SP., et al. “Adult obstructive sleep apnea: pathophysiology and diagnosis”. Chest 132.1 (2007): 325-337.
13. Dempsey JA and Skatrud JB. “A sleep induced apneic threshold and its consequences”. American Review of Respiratory Disease 133.6 (1986): 1163-1170.
14. Kuna ST and Sant’Ambrogio G. “Pathophysiology of upper airway closure during sleep”. Journal of the American Medical Association 266.10 (1991): 1384-1389.
15. Hudgel D. “Mechanisms of obstructive sleep apnea”. Chest 101.2 (1992): 541-549.
16. Solow B and Greve E. “Craniocervical angulation and nasal respiratory resistance”. In: McNamara J A (ed.) Nasorespiratory function and craniofacial growth, Monograph No. 9, Craniofacial Growth Series, Center for Human Growth and Development, University of Michigan, Ann Arbor (1983): 87-119.
17. Hellsing E. “Changes in the pharyngeal airway in relation to extension of the head”. European Journal of Orthodontics 11.4 (1989): 359-365.
18. Solow B and Tallgren A. “Head posture and craniofacial morphology”. American Journal of Physical Anthropology 44.3 (1976): 417-436.
19. Davis PJ. “Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren”. Community Dentistry and Oral Epidemiol-ogy 15.4 (1987): 218 -220.
20. Solow B., et al. “Airway adequacy, head posture, and craniofacial morphology”. American Journal of Orthodontics 86.3 (1984): 214-223.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

319
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
21. Woodside DG., et al. “Mandibular and maxillary growth after changed mode of breathing”. American Journal of Orthodontics and Den-tofacial Orthopedics 100.1 (1991): 1-18.
22. Watanabe T., et al. “Contribution of body habitus and craniofacial characteristics to segmental closing prssures of the passive phar-ynx in patients with sleep disordered breathing”. American Journal of Respiratory and Critical Care Medicine 165.2 (2002): 260-265.
23. Arntsena A and Sonnesen L. “Cervical vertebral column morphology related to craniofacial morphology and head posture in pre-orthodontic children with Class II malocclusion and horizontal maxillary overjet”. American Journal of Orthodontics and Dentofacial Orthopedics 140.1 (2011): e1-e7.
24. Sonnesen L and Kjær I. “Anomalies of the cervical vertebrae in patients with skeletal Class II malocclusion and horizontal maxillary overjet”. American Journal of Orthodontics and Dentofacial Orthopedics 133.2 (2008): 189.e15-189.e20.
25. Ryan CM and Bradley TD. “Pathogenesis of Obstructive sleep apnea”. Journal of Applied Physiology 99.6 (2005): 2440-2450.
26. J Huang., et al. “Pharyngeal Cross-Sectional Area and Pharyngeal Compliance in Normal Males and Females”. Respiration 65.6 (1998): 458-468.
27. Solow B and Kreiborg S. “Soft-tissue stretching: A possible factor in craniofacial morphogenesis”. Scandinavian Journal of Dental Research 85.6 (1977): 505-507.
28. Dougherty G and Newman D. “Measurement of thickness and density of thin structures by computed tomography: a simulation study”. Medical Physics 26.7 (1999): 1341-1348.
29. Mori K., et al. “Recognition of bronchus in three-dimensional X-ray CT images with application to virtualized bronchoscopy system”. Proceedings International Conference on Pattern Recognition 7276 (1996): 528-532.
30. Kitasaka T., et al. “A method for segmenting bronchial trees from 3-D chest X-ray CT images”. Lecture Notes in Computer Science 2879 (2003): 603-610.
31. Tschirren J., et al. “Airway tree segmentation using adaptive regions of interest”. Proceedings of SPIE 5369 (2004): 125-131.
32. Malandain G., et al. “Topological segmentation of discrete surfaces”. International Journal of Computer Vision 10 (1993): 183-197.
33. Aylward SR and Bullitt E. “Initialization, noise, singularities, and scale in height ridge traversal for tubular object centerline extrac-tion”. IEEE Transactions on Medical Imaging 21.2 (2002): 61-75.
34. Meyer W. “On adenoid vegetation in the naso-pharyngeal cavity: Their pathology, diagnosis and treatment”. Medico-Chirurgical Transactions 53 (1870): 191-215.
35. Rubin RM. “Effects of Nasal Airway Obstruction on Facial Growth”. Ear, Nose and Throat Journal 66.5 (1987): 212-219.
36. Osler W. “The principle and practice of medicine”. Appleton, New York (1918).
37. Dickens C. “The Posthumous Papers of the Pickwick Club”. London: Chapman and Hall (1837).
38. Guilleminault C. “Natural history, cardiac impact and long term follow-up of sleep apnea syndrome”. Medical Clinics of North America 69 (1985): 1265-1280.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea

320
Citation: Mayank Gahlot. “A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea”. EC Dental Science 18.2 (2019): 303-320.
Volume 18 Issue 2 February 2019© All rights reserved by Mayank Gahlot.
39. Ceylan I and Oktay H. “A study on the pharyngeal size in different skeletal patterns”. American Journal of Orthodontics and Dentofacial Orthopedics 108.1 (1995): 69-75.
40. Johnston CD and Richardson A. “Cephalometric changes in adult pharyngeal morphology”. European Journal of Orthodontics 21.4 (1999): 357-362.
41. Sato K., et al. “Effectiveness of the analysis of craniofacial morphology and pharyngeal airway morphology in the treatment of chil-dren with obstructive sleep apnoea syndrome”. Dentomaxillofacial Radiology 41.5 (2011): 411-416.
42. Lowe AA., et al. “CT reconstructions of tongue and airway in adults with obstructive sleep apnea”. American Journal of Orthodontics and Dentofacial Orthopedics 90.5 (1986): 364-374.
43. Grauer D., et al. “Pharyngeal airway volume and shape from cone-beam computed tomography: Relationship to facial morphology”. American Journal of Orthodontics and Dentofacial Orthopedics 136.6 (2009): 805-814.
44. Sonnesen L and Kjær I. “Cervical column morphology in patients with skeletal Class III malocclusion and mandibular overjet”. Ameri-can Journal of Orthodontics and Dentofacial Orthopedics 132.4 (2007): 427.e7-427.e12.
45. Liistro G., et al. “High Mallampati score and nasal obstruction are associated risk factors for obstructive sleep apnoea”. European Respiratory Journal 21.2 (2003): 248-252.
46. Nuckton TJ., et al. “Physical Examination: Mallampati Score as an Independent Predictor of Obstructive Sleep Apnea”. Sleep 29.7 (2006): 903-908.
47. Kawaguchi Y., et al. “Different Impacts of Neck Circumference and Visceral Obesity on the Severity of Obstructive Sleep apnea Syn-drome”. Obesity 19.2 (2011): 276-282.
48. You M., et al. “Morphological variety of the soft palate in normal individuals: a digital cephalometric study”. Dentomaxillofacial Radi-ology 37.6 (2008): 344-349.
49. Ryan CF., et al. “Three-dimensional Upper Airway Computed Tomography in Obstructive Sleep Apnea: A Prospective Study in Pa-tients Treated by Uvulopalatopharyngoplasty”. American Journal of Respiratory and Critical Care Medicine 144.2 (1991): 428-432.
50. Solow B., et al. “Airway dimensions and head posture in obstructive sleep apnoea”. European Journal of Orthodontics 18 (1996): 571-579.
51. Baik UB., et al. “Relationship between cephalometric characteristics and obstructive sites in obstructive sleep apnea syndrome”. Angle Orthodontist 72.2 (2002): 124-134.
52. Enache AM., et al. “Assessment of sagittal and vertical skeletal patterns in Romanian patients with obstructive sleep apnea”. Roma-nian Journal of Morphology and Embryology 51.3 (2010): 505-508.
53. Lamaco L. “Quelque cas de narcolepsis”. Revue Médicale 17 (1987): 699-714.
A CBCT Study to Assess the Volumetric Analysis of Airway, Craniofacial Morphology and Cervical Vertebral Fusion Anomalies in North Indian Patients with Obstructive Sleep Apnea