Embed Size (px)
Citation preview

10/9/14
1
By: Pascal Bernatchez
Providence!Heart + Lung Institute!at St. Paul’s Hospital!
University of!British Columbia!
Smooth muscle pharmacology & interventional cardiology
LAST LECTURE
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
High blood pressure
Blood pressure control
Atherosclerosis Endothelial Injury
Thrombus
CABG
PTCA
Stent
Drug eluting stents Scaffolds
Classic Vascular pharmacology -chronic -systemic
Local Vascular pharmacology -acute -targeted
Patient burden
Restenosis
In-sent restenosis
Lipid lowering drugs Platelet/SMC pharmacology

10/9/14
2
Cath lab patients / surgery
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
blood pressure management lipid management Coagulation Diabetes Macrophage
accumulation Formation of necrotic core
Formation of fibrous cap
CABG

10/9/14
3
PTCA
What is PTCA?
Restenosis

10/9/14
4
Stenosis and angioplasty
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Medication?
Damage
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Plaxitaxel Cirrolimus\ Cobalt chromium

10/9/14
5
Restenosis
Restenosis: multi step process (lecture X)
Angioplasty injury
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Platelet adhesion

10/9/14
6
Angioplasty injury
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
pdgf
Angioplasty injury
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia

10/9/14
7
Stents
Stenosis and stenting
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia

10/9/14
8
Restenosis
Paclitaxel/Taxol
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia

10/9/14
9
Paclitaxel/Taxol
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
-Anti-cancer agent -Anti-mitotic
-As a potent stabilizer of microtubules. Microtubule disassembly is essential for the transition from the G2 to the M phase and migration - less SMC less leukocytes
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Sirolimus/Rapamycin

10/9/14
10
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
-Immunosuppressant possesses anti-proliferative properties -Stent: The metal of the stent has a soft, plastic coating
It slowly releases Sirolimus into the artery wall around the stent Eighty percent (80%) of the sirolimus is released during the first 30 days. The rest is released by the end of 90 days
Controlled-release, nonresorbable, elastomeric polymer coating
Sirolimus/Rapamycin
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 368;3 nejm.org january 17, 2013256
stenosis, which is manifested as myocardial in-farction in 10 to 20% of patients.28,29
Everolimus-Eluting StentsIn randomized trials, everolimus-eluting stents improved clinical outcomes as compared with paclitaxel-eluting stents, reducing the risks of re-
peat revascularization, myocardial infarction, and stent thrombosis.30,31 Randomized comparisons showed similar outcomes for stents releasing everolimus and those releasing sirolimus with respect to rates of death, myocardial infarction, and repeat revascularization.32-34 A large trial showed lower rates of stent thrombosis with
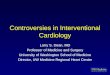
Bare-metal stent
Inhibition
Binding toFKBP12
Inhibition ofmTOR
Binding to !-tubulinsubunit of microtubules
Polymerizationof tubulin
Up-regulation ofp27Kip1
Inhibition of microtubuledisassembly
Drug-eluting stent
Cell cycle
G0 phase
S phase
G2 phase
M phase(cell division)
G1 phase
Stentplatform
Stentplatform
Polymer coating
Antiproliferative
Drug release Polymer coating
biodegradation
PaclitaxelC47H51NO47
MW 854
SirolimusC51H79NO13
MW 914
EverolimusC53H83NO14
MW 958
ZotarolimusC52H79N5O12
MW 966
OOO OOO
OO
OOOOOOO
OOO
OOOOOO
OH
OHOHOH
OHOHOO
OHOHOH
NHNHNHNH
OH OOOO OOOOO OHHH
NNN
HOHO
OOOOOO
OO
OOOOOOO
OOOOOOOOO
OOOOOOOO
OHOH
OOOOO
OO
HOHO
NNN
HOHO
OOOOOO
OO
OOOOOOO
OOOOOOOOO
OOOOOOOO
OHOH
OOOOO
OO
HOHOHO
OH
NNN
HOHO
OOOOOO
OO
OOOOOOO
OOOOOOOOO
OOO
OHOH
NNNNNNN
NNNNNNN
H3CO
H3COCO
OCHOCH3
C
A B
Polymer coatingPolymer coating
platform
Restenosis
Arterial injury
Activation of vascularsmooth-muscle cells
Proliferation and migrationof vascular smooth-muscle
cells and extracellular-matrix formation
12/17/2012
1/17/2013
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
AuthorFig #Title
DEMEArtistPub Date
COLOR FIGURE
Draft 3
Drug-Eluting CoronaryArtery Stents
1
NameWilliams
Holmes ra1210816
Ingelfinger
The New England Journal of Medicine Downloaded from nejm.org by Pascal Nicolas Bernatchez on January 17, 2013. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.

10/9/14
11
Drug eluting stents
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
-Decrease rate of restenosis by 40-70% compared to BMS -% Stenosis/total lumen diameter: Sirolimus: 3.5% of diameter
BMS: 18.5% of diameter
Paclitaxel: 3.3% 5100 patients study BMS: 12.2%
Delayed restenosis
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
-Work well for a year -Delayed reendothelialization because of taxol/rapamycin affects endoth. -Your vessel is never healed unless your endothelial layer regrows, and becomes functional (not dysfunctional, which is the case mostly) -Thrombosis causes Death or MI so HUGE ANTI PLATELET THERAPY

10/9/14
12
Stent thrombosis
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Aspirin: should not be interrupted Clopidogrel: no longer that day -5 to day +2 if other surgery
Normally a month of clopidogrel after PTCA or stent, now increased at 6 to 12mo
Reopro:
-Other types of surgeries need cessation of platelet therapy
Scaffolds / Resorbable stents
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
-Metal (Mg) -Polymer (polylactic acid) -Biggest advantage? -Biggest question marks?
expansion was observed in the first 3 months of follow-up.The mean stent cross-sectional area increased from7.42!1.51 mm2 at baseline to 8.18!2.42 mm2 (P"0.086) at3 months and 8.13!2.52 mm2 at 6 months.65 A second, largerstudy of 50 elective patients (63 lesions, 84 stents) alsoshowed promising results. IVUS performed at the 3-yearfollow-up demonstrated the complete absence of stent struts,and angiographic analysis demonstrated a mean diameterstenosis of 25% compared with 38%, 29%, and 26% at 6, 12,and 24 months, respectively. Clinical outcomes at 4-yearfollow-up showed rates of overall and MACE-free survivalrates of 97.7% and 82.0%, respectively.66
At the 10-year clinical follow-up, freedom from cardiacdeath, noncardiac death, and MACEs was 98%, 87%, and48%, respectively.67 In the limited cases with serial angio-graphic follow-up, the minimum lumen diameter was stable:the mean minimum lumen diameter was 2.01 mm at 1 yearand 2.06 mm at 10 years. There were 2 ST events: 1 subacuteevent occurring at day 5 possibly as a result of inadequateheparinization at the time of percutaneous coronary interven-tion and 1 very late ST event occurring in the sirolimus-
eluting metallic stent that was later implanted proximal to thepreviously placed Igaki-Tamai stent. Serial angiographic andOCT images of the stent struts out to the 10-year follow-up in1 anecdotal case are shown in Figure 4.
Despite these impressive results, the failure of the stent toprogress was related primarily to the use of heat to induceself-expansion. There were concerns that this could causenecrosis of the arterial wall, leading to excessive intimalhyperplasia or increased platelet adhesion, leading to ST.68
None of these concerns were substantiated in the initialstudies; however, only low-risk patients were enrolled. Aftercompletion of the Biodegradable peripheral Igaki-Tamaistents PERSEUS study,69 the stent became available in Europefor peripheral use; however, there are plans to review itsuse in coronary arteries. At present, the stent has no drugelution, although preclinical studies of the polymeric stenteluting the tyrosine kinase antagonist ST 638 showedpromising results.52
Magnesium AlloyMagnesium (Mg) is the fourth-most-common cation withinthe human body; the total body content is #20 g, with 350 mg
Figure 3. OCT and histology at 28 daysand 2, 3, and 4 years after stent implan-tation. At 28 days, OCT shows pre-served box appearance (A), correspond-ing to the voids not stained by AlcianBlue (B and C). At 2 years, OCT stillshows struts as preserved box appear-ance (D), but the persistent voids (E) arenow replaced by proteoglycan (hyalinematerial), which stained positively withAlcian Blue (F). At 3 years, only 2 strutsat 6 o’clock remained detectable as pre-served box (G). Otherwise, connectivetissue cells are now infiltrated in the strutfootprints (H, hematoxylin and eosinstaining; I, Alcian Blue). At 4 years, strutsare no longer discernible by OCT (J); thestrut footprints are hardly detectable inMovat staining (K) and Alcian Blue (L)and are characterized by paucity of con-nective tissue cells and a small amountof calcification.
784 Circulation February 22, 2011
by guest on September 18, 2014http://circ.ahajournals.org/Downloaded from
expansion was observed in the first 3 months of follow-up.The mean stent cross-sectional area increased from7.42!1.51 mm2 at baseline to 8.18!2.42 mm2 (P"0.086) at3 months and 8.13!2.52 mm2 at 6 months.65 A second, largerstudy of 50 elective patients (63 lesions, 84 stents) alsoshowed promising results. IVUS performed at the 3-yearfollow-up demonstrated the complete absence of stent struts,and angiographic analysis demonstrated a mean diameterstenosis of 25% compared with 38%, 29%, and 26% at 6, 12,and 24 months, respectively. Clinical outcomes at 4-yearfollow-up showed rates of overall and MACE-free survivalrates of 97.7% and 82.0%, respectively.66
At the 10-year clinical follow-up, freedom from cardiacdeath, noncardiac death, and MACEs was 98%, 87%, and48%, respectively.67 In the limited cases with serial angio-graphic follow-up, the minimum lumen diameter was stable:the mean minimum lumen diameter was 2.01 mm at 1 yearand 2.06 mm at 10 years. There were 2 ST events: 1 subacuteevent occurring at day 5 possibly as a result of inadequateheparinization at the time of percutaneous coronary interven-tion and 1 very late ST event occurring in the sirolimus-
eluting metallic stent that was later implanted proximal to thepreviously placed Igaki-Tamai stent. Serial angiographic andOCT images of the stent struts out to the 10-year follow-up in1 anecdotal case are shown in Figure 4.
Despite these impressive results, the failure of the stent toprogress was related primarily to the use of heat to induceself-expansion. There were concerns that this could causenecrosis of the arterial wall, leading to excessive intimalhyperplasia or increased platelet adhesion, leading to ST.68
None of these concerns were substantiated in the initialstudies; however, only low-risk patients were enrolled. Aftercompletion of the Biodegradable peripheral Igaki-Tamaistents PERSEUS study,69 the stent became available in Europefor peripheral use; however, there are plans to review itsuse in coronary arteries. At present, the stent has no drugelution, although preclinical studies of the polymeric stenteluting the tyrosine kinase antagonist ST 638 showedpromising results.52
Magnesium AlloyMagnesium (Mg) is the fourth-most-common cation withinthe human body; the total body content is #20 g, with 350 mg
Figure 3. OCT and histology at 28 daysand 2, 3, and 4 years after stent implan-tation. At 28 days, OCT shows pre-served box appearance (A), correspond-ing to the voids not stained by AlcianBlue (B and C). At 2 years, OCT stillshows struts as preserved box appear-ance (D), but the persistent voids (E) arenow replaced by proteoglycan (hyalinematerial), which stained positively withAlcian Blue (F). At 3 years, only 2 strutsat 6 o’clock remained detectable as pre-served box (G). Otherwise, connectivetissue cells are now infiltrated in the strutfootprints (H, hematoxylin and eosinstaining; I, Alcian Blue). At 4 years, strutsare no longer discernible by OCT (J); thestrut footprints are hardly detectable inMovat staining (K) and Alcian Blue (L)and are characterized by paucity of con-nective tissue cells and a small amountof calcification.
784 Circulation February 22, 2011
by guest on September 18, 2014http://circ.ahajournals.org/Downloaded from

10/9/14
13
Endothelial dysfunction and restenosis
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Endothelial dysfunction and restenosis
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Flow mediated dilation

10/9/14
14
Diabetes
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
NEJM 367:25, 2012
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;25 nejm.org december 20, 20122380
tients with myocardial infarction in that group). All the procedural myocardial infarctions in the trial were non–Q-wave events. Myocardial in-farctions that occurred more than 30 days after the index procedures were reported in 81 of 99 patients (82%) in the PCI group and in 29 of 48 patients (60%) in the CABG group.
There were fewer strokes in the PCI group than in the CABG group (P = 0.03) (Table 2, and Fig. 2B in the Supplementary Appendix). The
5-year rates were 2.4% in the PCI group and 5.2% in the CABG group. Of these strokes, the major-ity (87%) were ischemic and 13% were hemor-rhagic. In the first 30 days after the procedure, 3 patients in the PCI group and 16 in the CABG group had a stroke (Table 3). The excess of strokes in the CABG group occurred in the first 30 days after randomization. An NIH Stroke Scale score of more than 4 (severely disabling) at the time of the event was reported in 27% of patients in the PCI group, as compared with 55% of those in the CABG group. A score on the Rankin scale of more than 1 at the time of the stroke was re-ported in 60% of patients in the PCI group, as compared with 70% in the CABG group.
Secondary OutcomesRates of cardiovascular death (63.7% of all deaths) did not differ significantly between the two study groups (P = 0.12 by the log-rank test), nor did rates of major adverse cardiovascular and cerebrovas-cular events at 30 days (P = 0.68 by the log-rank test). However, at 1 year after the procedure, there was a significant difference in rates of major ad-verse cardiovascular and cerebrovascular events, with 16.8% in the PCI group versus 11.8% in the CABG group (P = 0.004) (Table 3, and Fig. 2C in the Supplementary Appendix). This difference was attributed largely to the preponderance of repeat revascularization events by 1 year in the PCI group, as compared with the CABG group, with repeat events in 12.6% and 4.8% of patients in the two groups, respectively (hazard ratio, 2.74; 95% CI, 1.91 to 3.89; P<0.001) (Fig. 2D in the Supplemen-tary Appendix).
Prespecified Subgroup AnalysesThe greater benefit of CABG versus PCI was con-sistent across all prespecified subgroups (Fig. 2). The analysis according to the category of SYNTAX score showed no significant subgroup interac-tion (P = 0.58). At 5 years, the absolute difference in the rate of the primary outcome in the PCI group, as compared with the CABG group, was similar in the three SYNTAX subgroups (6 percentage points for a low SYNTAX score, 10 percentage points for an intermediate score, and 8 percentage points for a high score). The hazard ratios for the PCI group, as compared with the CABG group, according to SYNTAX subgroup were 1.14, 1.46, and 1.46, re-spectively. Similarly, for the rate of major adverse cardiovascular and cerebrovascular events at 1 year,
Dea
th, M
yoca
rdia
l Inf
arct
ion,
or S
trok
e (%
)60
40
30
10
50
20
00 1 2 3 4 5
Years since Randomization
B Death
A Primary Outcome
P=0.005 by log-rank test5-Yr event rate: 26.6% vs. 18.7%
No. at RiskPCICABG
953947
848814
788758
625613
416422
219221
PCI
CABG
Dea
th fr
om A
ny C
ause
(%)
60
40
30
10
50
20
00 1 2 3 4 5
Years since Randomization
P=0.049 by log-rank test5-Yr event rate: 16.3% vs. 10.9%
No. at RiskPCICABG
953947
897855
845806
685655
466449
243238
PCI
CABG
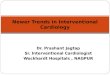
Figure 1. Kaplan–Meier Estimates of the Composite Primary Outcome and Death.
Shown are rates of the composite primary outcome of death, myocardial infarction, or stroke (Panel A) and death from any cause (Panel B) truncated at 5 years after randomization. The P value was calculated by means of the log-rank test on the basis of all available follow-up data.
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF BRITISH COLUMBIA on August 16, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 367;25 nejm.org december 20, 20122380
tients with myocardial infarction in that group). All the procedural myocardial infarctions in the trial were non–Q-wave events. Myocardial in-farctions that occurred more than 30 days after the index procedures were reported in 81 of 99 patients (82%) in the PCI group and in 29 of 48 patients (60%) in the CABG group.
There were fewer strokes in the PCI group than in the CABG group (P = 0.03) (Table 2, and Fig. 2B in the Supplementary Appendix). The
5-year rates were 2.4% in the PCI group and 5.2% in the CABG group. Of these strokes, the major-ity (87%) were ischemic and 13% were hemor-rhagic. In the first 30 days after the procedure, 3 patients in the PCI group and 16 in the CABG group had a stroke (Table 3). The excess of strokes in the CABG group occurred in the first 30 days after randomization. An NIH Stroke Scale score of more than 4 (severely disabling) at the time of the event was reported in 27% of patients in the PCI group, as compared with 55% of those in the CABG group. A score on the Rankin scale of more than 1 at the time of the stroke was re-ported in 60% of patients in the PCI group, as compared with 70% in the CABG group.
Secondary OutcomesRates of cardiovascular death (63.7% of all deaths) did not differ significantly between the two study groups (P = 0.12 by the log-rank test), nor did rates of major adverse cardiovascular and cerebrovas-cular events at 30 days (P = 0.68 by the log-rank test). However, at 1 year after the procedure, there was a significant difference in rates of major ad-verse cardiovascular and cerebrovascular events, with 16.8% in the PCI group versus 11.8% in the CABG group (P = 0.004) (Table 3, and Fig. 2C in the Supplementary Appendix). This difference was attributed largely to the preponderance of repeat revascularization events by 1 year in the PCI group, as compared with the CABG group, with repeat events in 12.6% and 4.8% of patients in the two groups, respectively (hazard ratio, 2.74; 95% CI, 1.91 to 3.89; P<0.001) (Fig. 2D in the Supplemen-tary Appendix).
Prespecified Subgroup AnalysesThe greater benefit of CABG versus PCI was con-sistent across all prespecified subgroups (Fig. 2). The analysis according to the category of SYNTAX score showed no significant subgroup interac-tion (P = 0.58). At 5 years, the absolute difference in the rate of the primary outcome in the PCI group, as compared with the CABG group, was similar in the three SYNTAX subgroups (6 percentage points for a low SYNTAX score, 10 percentage points for an intermediate score, and 8 percentage points for a high score). The hazard ratios for the PCI group, as compared with the CABG group, according to SYNTAX subgroup were 1.14, 1.46, and 1.46, re-spectively. Similarly, for the rate of major adverse cardiovascular and cerebrovascular events at 1 year,
Dea
th, M
yoca
rdia
l Inf
arct
ion,
or S
trok
e (%
)
60
40
30
10
50
20
00 1 2 3 4 5
Years since Randomization
B Death
A Primary Outcome
P=0.005 by log-rank test5-Yr event rate: 26.6% vs. 18.7%
No. at RiskPCICABG
953947
848814
788758
625613
416422
219221
PCI
CABG
Dea
th fr
om A
ny C
ause
(%)
60
40
30
10
50
20
00 1 2 3 4 5
Years since Randomization
P=0.049 by log-rank test5-Yr event rate: 16.3% vs. 10.9%
No. at RiskPCICABG
953947
897855
845806
685655
466449
243238
PCI
CABG
Figure 1. Kaplan–Meier Estimates of the Composite Primary Outcome and Death.
Shown are rates of the composite primary outcome of death, myocardial infarction, or stroke (Panel A) and death from any cause (Panel B) truncated at 5 years after randomization. The P value was calculated by means of the log-rank test on the basis of all available follow-up data.
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF BRITISH COLUMBIA on August 16, 2013. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
LAST LECTURE
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
High blood pressure
Blood pressure control
Atherosclerosis Endothelial Injury
Thrombus
CABG
PTCA
Stent
Drug eluting stents
Classic Vascular pharmacology -chronic -systemic
Local Vascular pharmacology -acute -targeted
Patient burden
Restenosis
In-sent restenosis
Lipid lowering drugs Platelet/SMC pharmacology

10/9/14
15
Providence Heart + Lung Institute at St. Paul’s Hospital
University of British Columbia
Conclusion
-Restenosis – In-Stent stenosis – Delayed restenosis -DES have a fantastic effect on restenosis and revascularization (decreased need of second procedure). -Impaired reendothelialization -Exam? [email protected]