Embed Size (px)
DESCRIPTION
Criteria for Any Epileptic Event. Clinical Phenomena Something has to happen Paroxysmal Nature It is an attack, not a permanent condition EEG Correlate There is a change in the EEG. Epileptic Seizure. Transient excessive discharge of nerve cells resulting in an seizure. - PowerPoint PPT Presentation
Citation preview
Criteria for Any Epileptic Event
• Clinical Phenomena– Something has to happen
• Paroxysmal Nature– It is an attack, not
a permanent condition
• EEG Correlate– There is a change in
the EEG
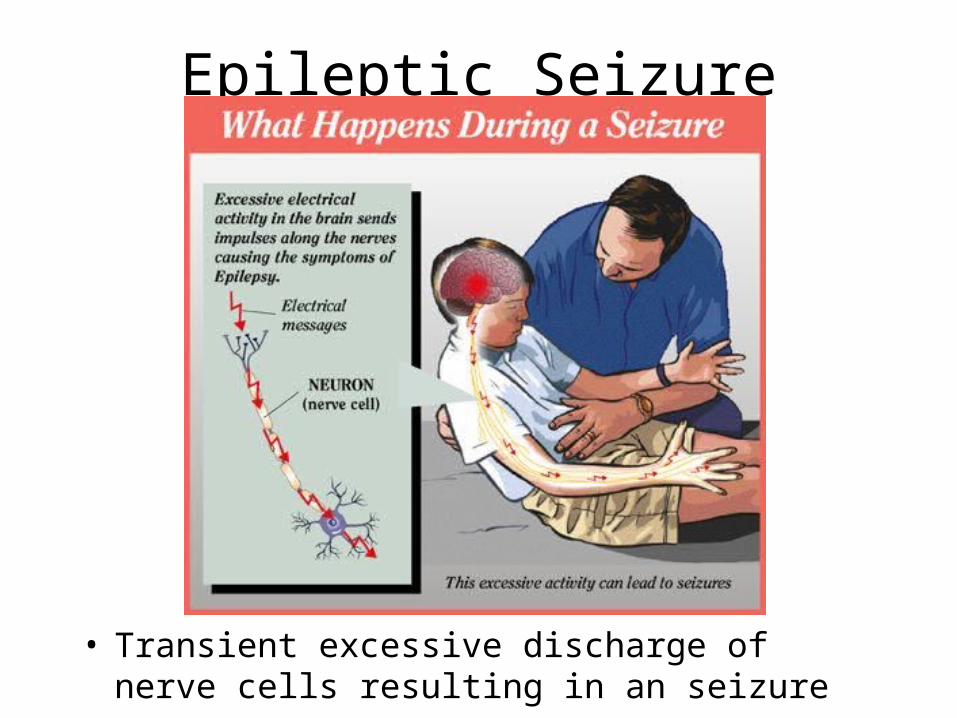
Epileptic Seizure
• Transient excessive discharge of nerve cells resulting in an seizure
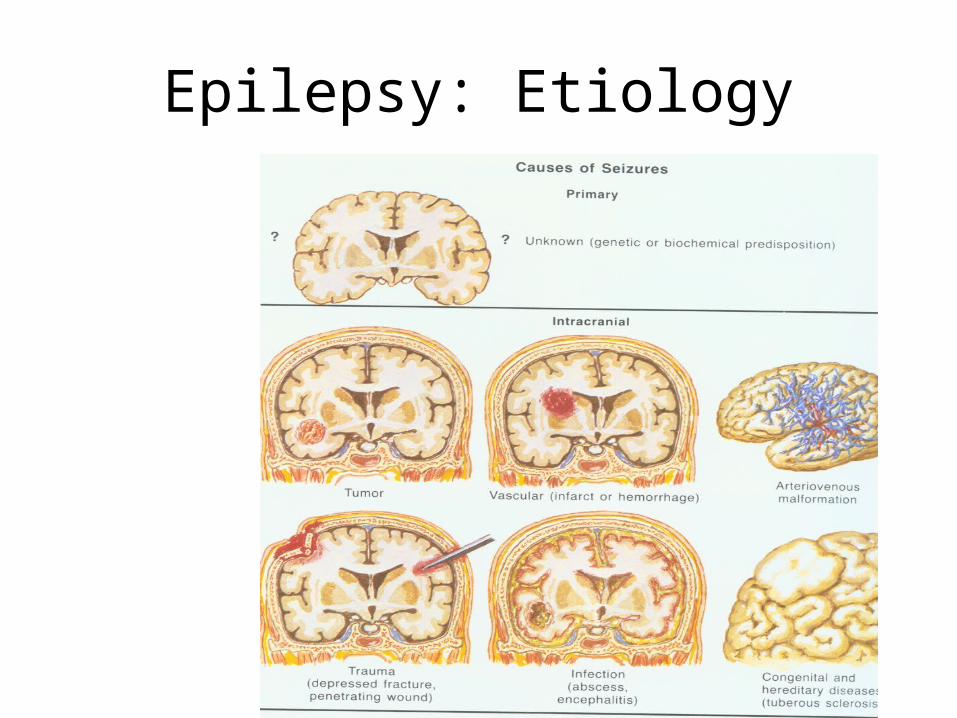
Epilepsy: Etiology
ILAE Classification of Seizures
1. Localization-relateda. Idiopathicb. Symptomatic
2. Generalizeda. Idiopathicb. Idiopathic and/or symptomaticc. Symptomatic
3. Undetermined4. Special Syndromes
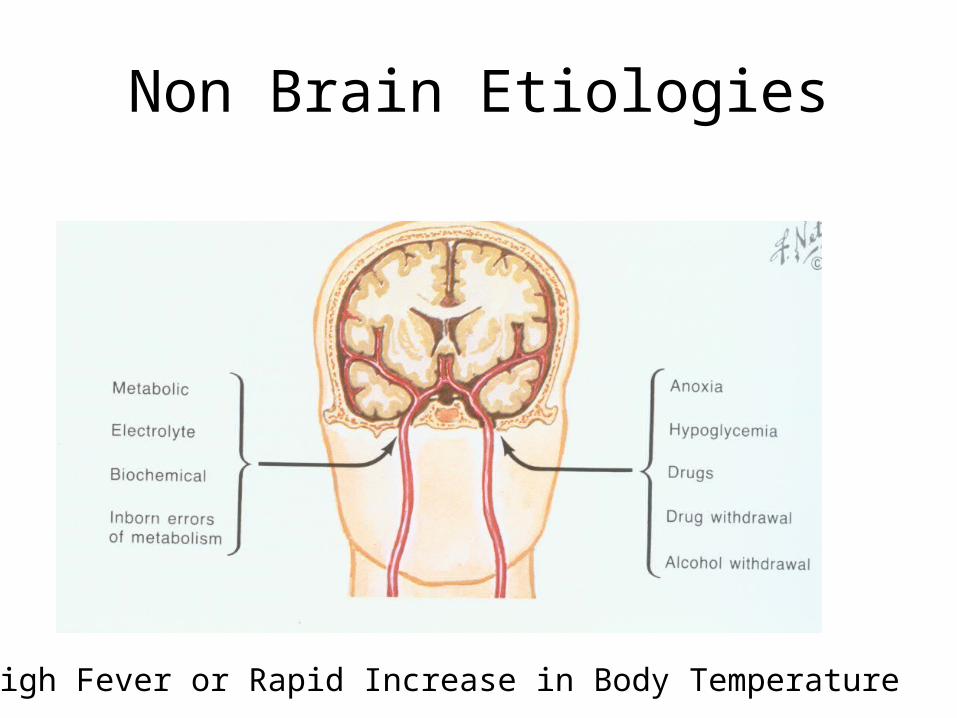
Non Brain Etiologies
High Fever or Rapid Increase in Body Temperature
Febrile Seizures
• Ages: 4months to 6 years• Most common sz disorder in children
– (2-4% of all children)
• Sz are generally short, generalized but may be focal
• Febrile sz do not cause brain damage• Recurrence: 25-40%• Prevalence:
– USA 2-5%– Japan 8.3%
Risk for recurrent febrile seizures
1. Family history of febrile seizures
2. Age younger than 18 months
3. Height of peak temperature-the lower the temperature the higher risk of recurrence
4.Duration of febrile illness-the shorter the duration the Higher risk of recurrence
Febrile Seizures & Epilepsy
• Recurrent FS, even multiple recurrences, are not important predictors of epilepsy.
• No known long term benefits from trying to prevent recurrent FS.
• 15% of children with epilepsy had FS• 2-4% of children with FS will develop epilepsy• 96-98% of children with FS will NOT develop
epilepsy.
Risk for epilepsy
1.Complex febrile seizure:
more than 15 minutes
focal
recurrence in 24 hours.
2.Neurologic disease, developmental delay etc…
3. Family history of epilepsy
Febrile Seizures: Assessment
• Indication for lumbar puncture – Deteriorating condition of child– Neck stiffness– Photophobia– Continuing fever without obvious reason
Febrile Seizures: Treatment?
• Anti-pyretics do not reduce no. of FS• AED: Phenobarbital produces unclear
results but replete with adverse effects• AED: Not effective• Diazepam PR: May be effective in
stopping FS in the home• Diazepam PO: Apparently not effective• Best Treatment: Reassurance
What to do!
• Keep Calm!• Only move person if in danger• Turn the head to one side if possible• Do not try to stop the seizure• DO NOT FORCE ANYTHING INTO MOUTH• Call ambulance if sz lasts more than 5 minutes,
there are multiple sz or person is hurt or has difficulty breathing
• Stay with person and allow to rest and recover from the seizure
What to do!
Case Report
• 18 month old previously healthy baby• Parents refused vaccinations• Two day history of irritability, and on day of
admission 2 events of tonic movements on left side of body
• Examination: 39˚, somnolence, stiff neck• Diagnosis?• Recommendations?
Epilepsy Syndromes
• Types of seizures
• EEG patterns
• Characteristic course and prognosis
• Age-dependant
• Some syndromes have idiopathic and symptomatic forms
.בת שש וחצי שנים פנתה למרפאה עקב הפרעת קשב ורכוז
מחלה נוכחית: מזה ארבעה חדשים המורה שמה לב לשינוי התנהגותי הכולל ירידה בהקשבה נטיה לחלום במהלך השיעור ולא להקשיב. מדי פעם שמדברים אליה לא
מגיבה, מבט לעיתים בוהה.
אבחנה מבדלת בשלב זה:
) כחלק מהפרעת קשב ורכוז.day-dreamingחולמנות(1.
.2Complex partial seizure
.3Petit - Mal Epilepsy
עוד במחלה נוכחית:
ברקע:
הריון ולידה תקינים. ללא סבוכים פרינטלים.שניה משלושה להורים ילידי הארץ ללא קרבה
משפחתית. התפתחות מוטורית ושפתית תקינה. חסונים כמקובל, ללא רגישות לתרופות.
בבדיקה:
לחץ דם ודופק תקינים. בדיקה גופנית ונוירולוגית תקינה.
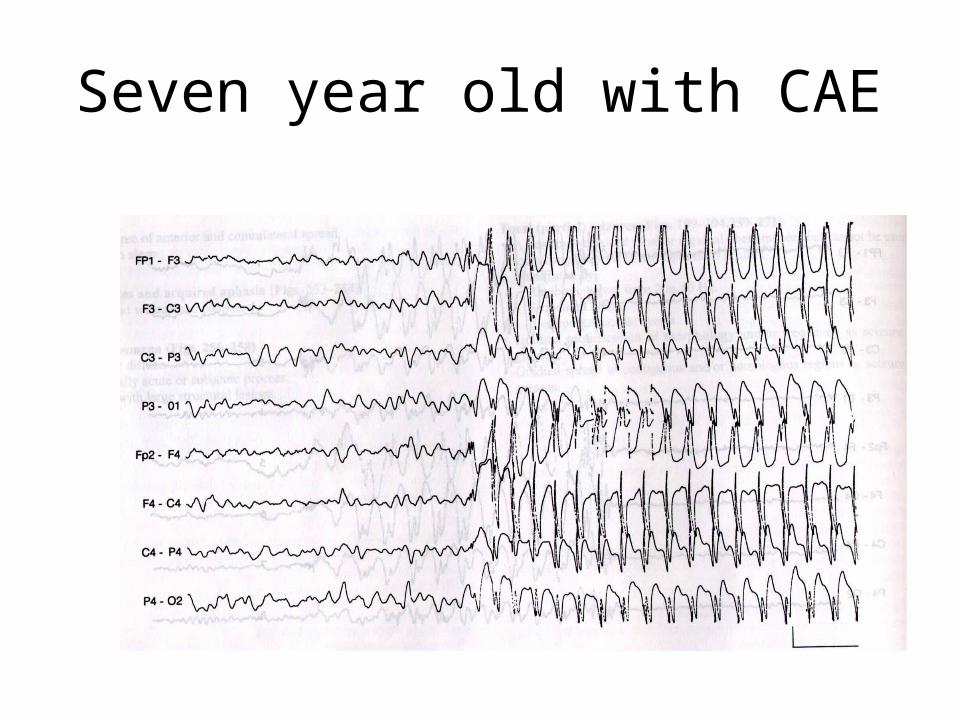
Seven year old with CAE
המשך ברור:
: פעילות הרקע תקינה. כוללת פעילןת בטא קדמית ואלפא אחורית .EEGבדיקת הרץ. מוגברת בנישום יתר.3לאורך התרשים מדי פעם פעילות כללית של זיז וגל בתדירות
Childhood absance epilepsy
ILAE Classification of Seizures
1. Localization-relateda. Idiopathicb. symptomatic
2. Generalizeda. Idiopathicb. Idiopathic and/or symptomaticc. Symptomatic
3. Undetermined4. Special Syndromes

A 5 year old boy wakes his parents in the middle of the night. He is unable to talk. He is drooling.
30 seconds later he falls to the ground with a tonic-clonic seizure
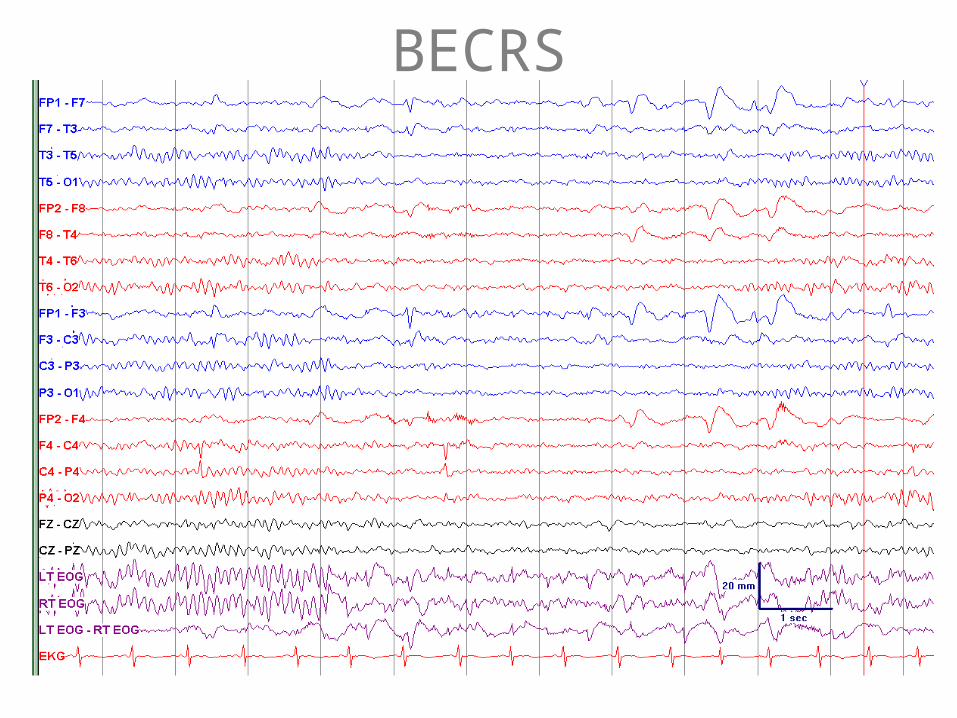
BECRS
BECRS
• Benign Rolandic Epilepsy• 3-12 years• Seizures disappear (majority) during
adolescence• Focal motor and/or secondarily generalized• Seizures tend to occur during sleep, last hour or
first 2 hours• EEG: Spikes over the central region and/or
adjacent midtemporal and parietal
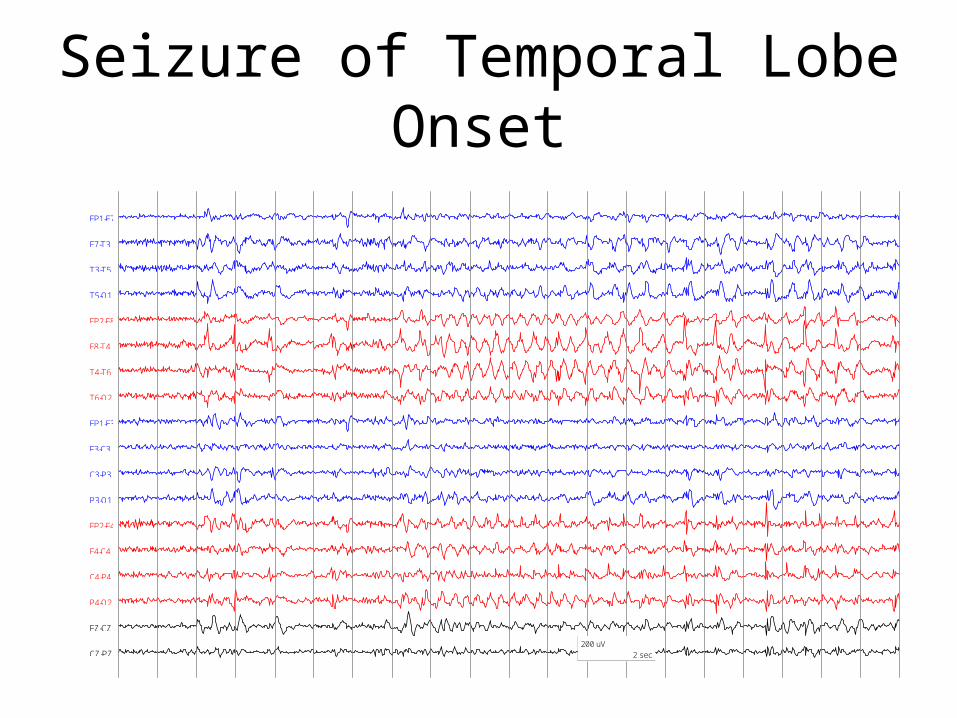
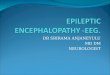
Seizure of Temporal Lobe Onset
FP1-F7
F7-T3
T3-T5
T5-O1
FP2-F8
F8-T4
T4-T6
T6-O2
FP1-F3
F3-C3
C3-P3
P3-O1
FP2-F4
F4-C4
C4-P4
P4-O2
FZ-CZ
CZ-PZ200 uV
2 sec
בן תשעה חדשים.
תלונה עיקרית: תנועות מוזרות.
מחלה נוכחית: מזה שבועיים ההורים שמו לב לכפוף הזרועות קדימה במקביל לכיפוף הראש מספר פעמים רב ביום. כמו כן מתיחת ידיים לאחור שחוזרת על עצמה שוב ושוב באופן מוגזם.
ברקע:ראשון להורים ילידי הארץ ללא קרבה משפחתית. הריון ולידה תקינים.
ללא סבוכים פרינטלים. במשפחה כולם בריאים. התפתחות- מתהפך בטן גב, לא זוחל לא יושב. ממלמל הברות בודדות. חסונים כמקובל, רגישות לתרופות-לא ידועה.
לגיל. ריאות, לב, בטן ב.מ.פ.עור-שלושה כתמים היפופיגמנטרים50%בבדיקה: חיוני ועירני. הקף ראש משוננים בקצה.
נוירולוגית: עדיין צניחת ראש.תנועות עיניים תקינות. ללא רפלקסי ילודאין רפלקסי הגנה, לנדאו גבולי.רפלקסים גידיים תקינים.
בבינסקי סמטרי.טונוס לא מוגבר בגפיים עליונות מופחת בגו ובגפיים תחתונות.

במסגרת הברור:
שהדגים היפסאריתמיה.EEGבוצע
ראש שהדגים נודולים סב-אפנדימלים בגבול החדרים הלטרלים.CTבוצע
אבחנה:
Tuberous sclerosis presenting as Infantile spasms.
תנועות משונות....,לסכום:פגור התפתחותי , כתמים היפופיגמנטרים על העור
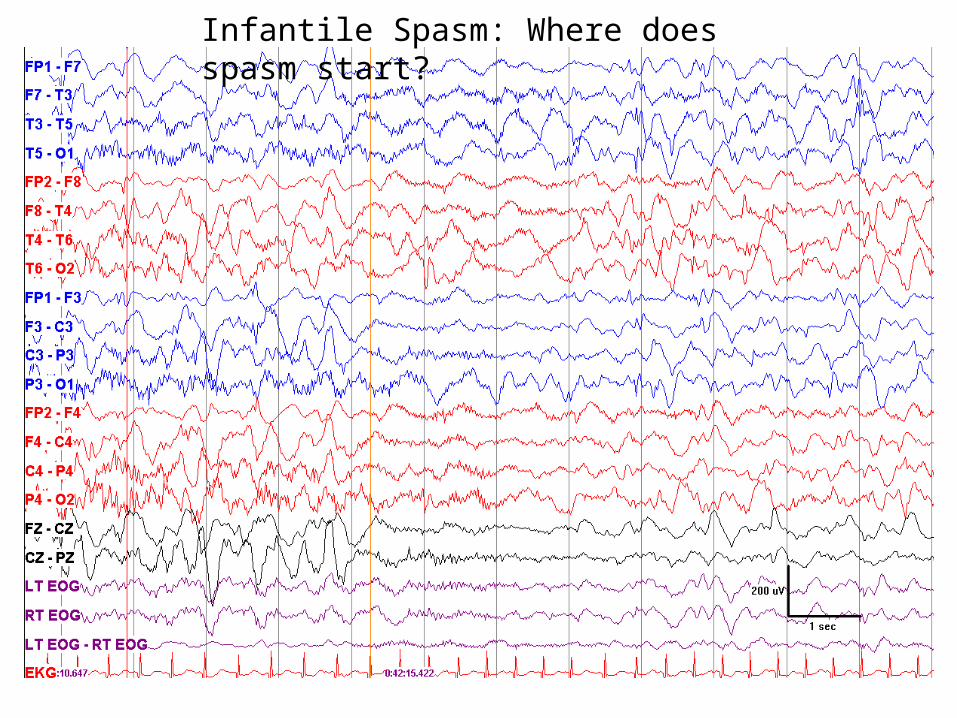
Infantile Spasm: Where does spasm start?


Definition of West Syndrome
• Infantile spasms
• Hypsarrhythmia
• Developmental plateau, regression or delay
Etiology
• Symptomatic
• Idiopathic
• Cryptogenic
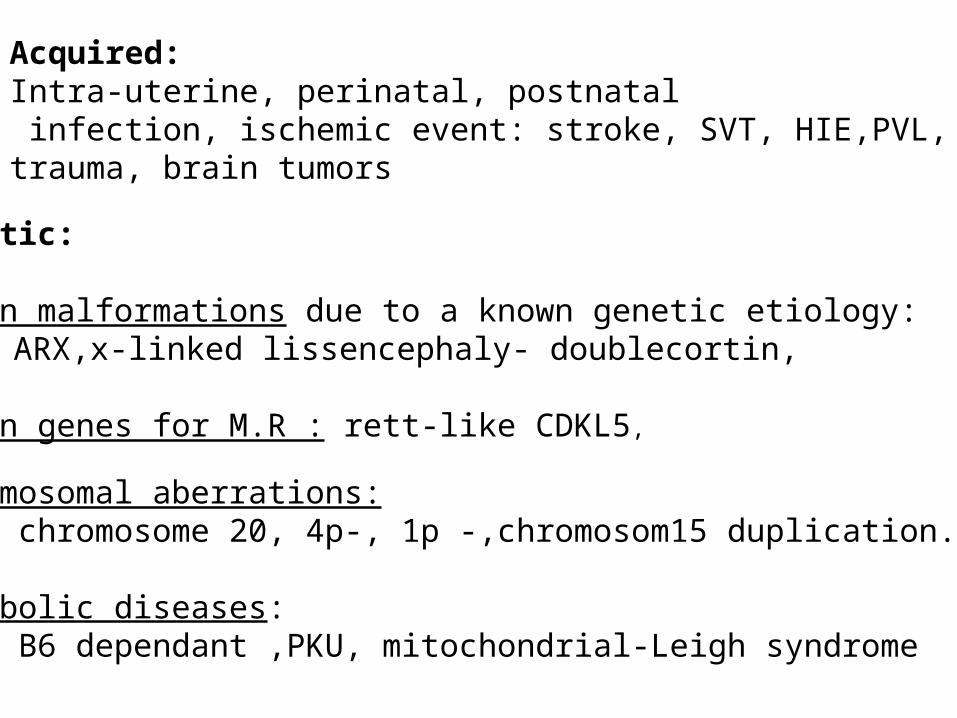
Acquired:Intra-uterine, perinatal, postnatal infection, ischemic event: stroke, SVT, HIE,PVL, trauma, brain tumors
Genetic:
Brain malformations due to a known genetic etiology:T.S, ARX,x-linked lissencephaly- doublecortin,
Known genes for M.R : rett-like CDKL5,
Chromosomal aberrations:Ring chromosome 20, 4p-, 1p -,chromosom15 duplication.
Metabolic diseases:NKH, B6 dependant ,PKU, mitochondrial-Leigh syndrome
ILAE Classification of Seizures
1. Localization-relateda. Idiopathicb. Symptomatic
2. Generalizeda. Idiopathicb. Idiopathic and/or symptomaticc. Symptomatic
3. Undetermined4. Special Syndromes