Embed Size (px)
Citation preview
Crise aigue drépanocytaire
Pr Armand Mekontso Dessap
Réanimation Médicale Centre de référence hémoglobinopathies
Hôpital Henri Mondor Université Paris Est Créteil
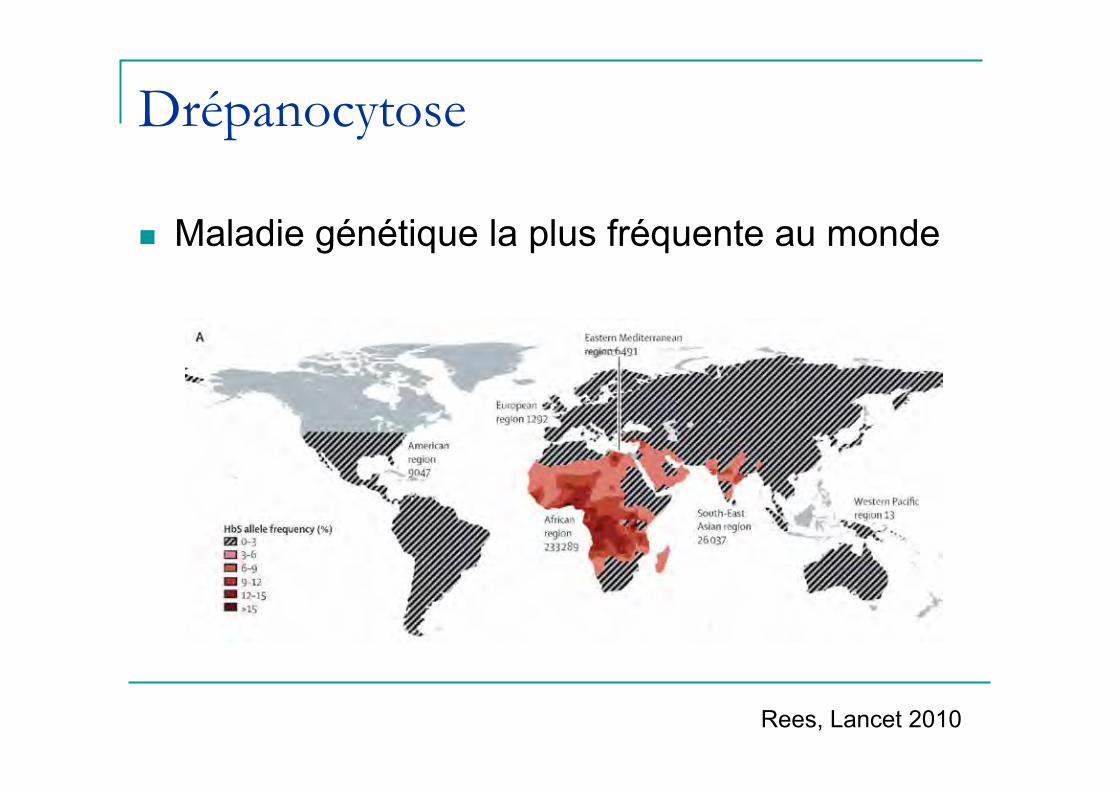
Drépanocytose
n Maladie génétique la plus fréquente au monde
Rees, Lancet 2010

Bases moléculaires et classification
Rees, Lancet 2010

Phénotypes cliniques
Gladwin, NEJM 2008

Admissions en réanimation
STA 70%
CVO hyperalgique
16%
SDMV 7%
Autres 7%
.
Tawfic, SQU Med J, May 2012
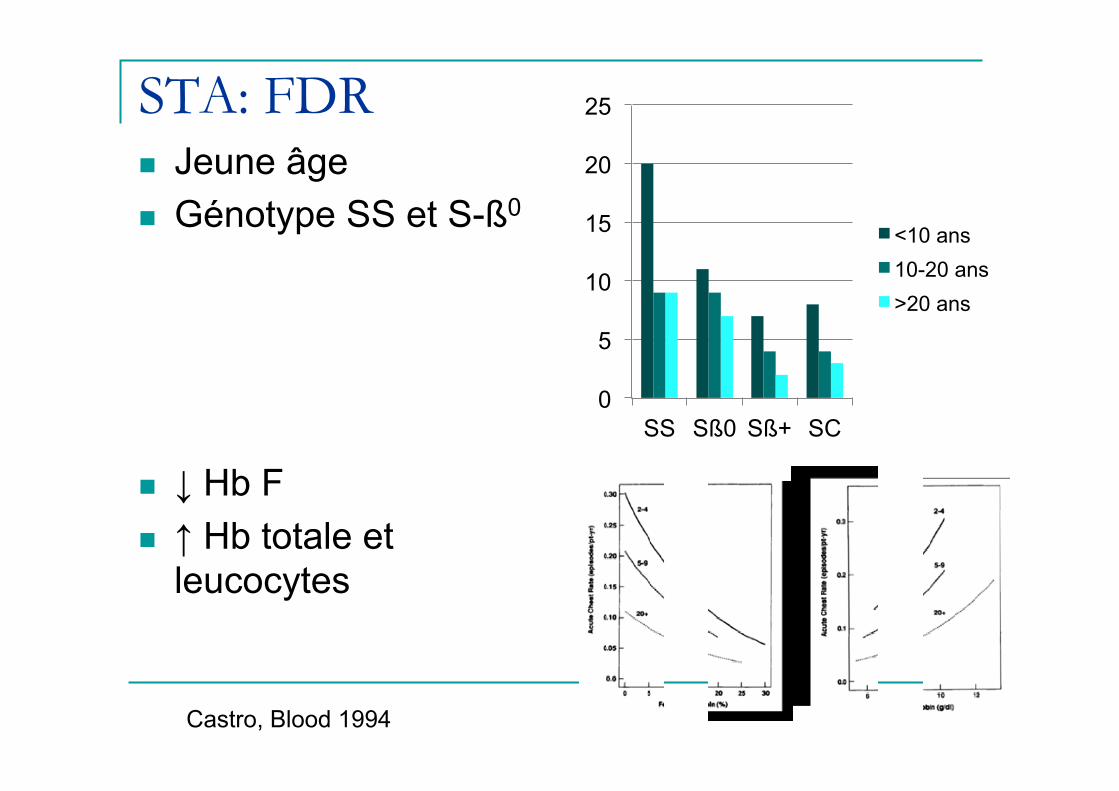
STA: FDR n Jeune âge n Génotype SS et S-ß0
n ↓ Hb F n ↑ Hb totale et
leucocytes
Castro, Blood 1994
0
5
10
15
20
25
SS Sß0 Sß+ SC
<10 ans 10-20 ans >20 ans
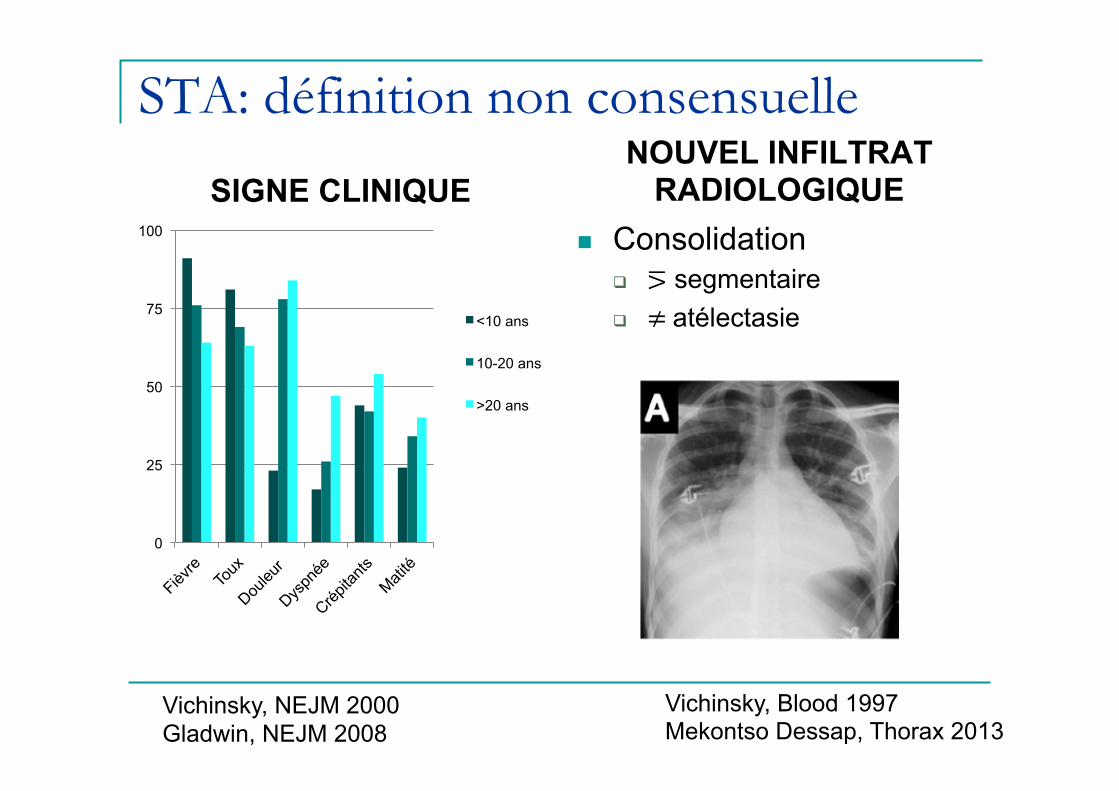
STA: définition non consensuelle
SIGNE CLINIQUE NOUVEL INFILTRAT
RADIOLOGIQUE n Consolidation
q ⋝ segmentaire q ≠ atélectasie
Vichinsky, NEJM 2000 Gladwin, NEJM 2008
Vichinsky, Blood 1997 Mekontso Dessap, Thorax 2013
0
25
50
75
100
<10 ans
10-20 ans
>20 ans
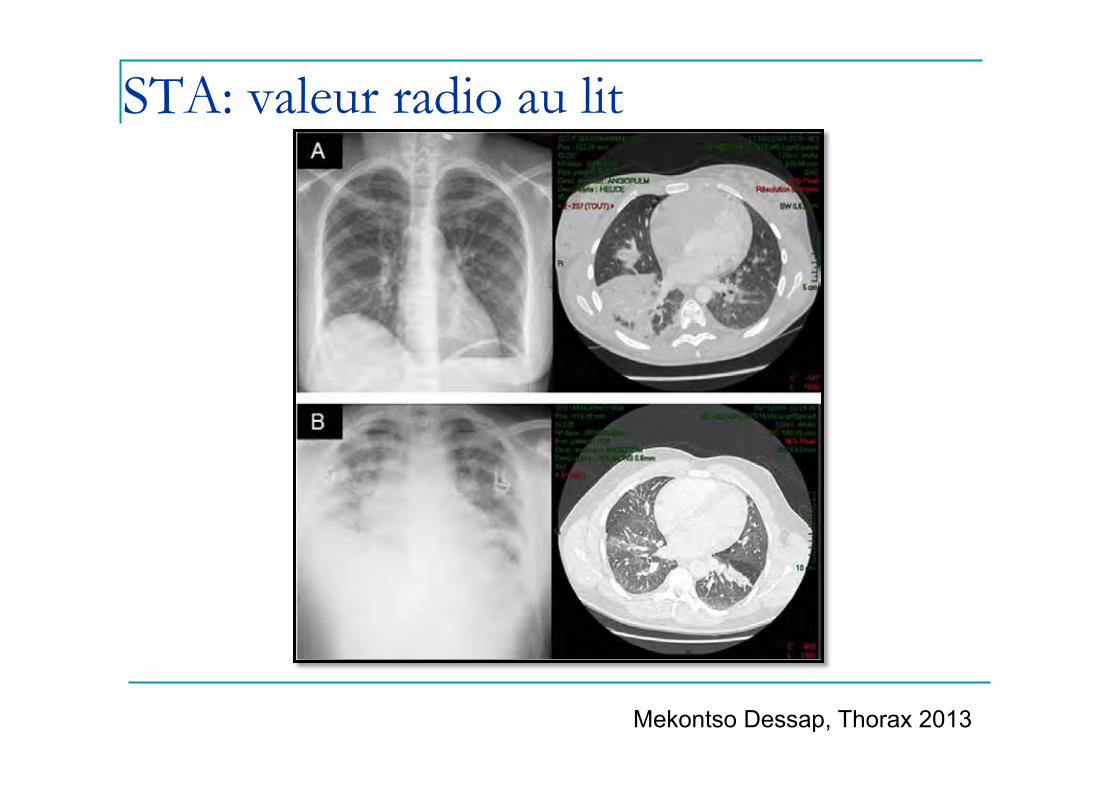
STA: valeur radio au lit
Mekontso Dessap, Thorax 2013
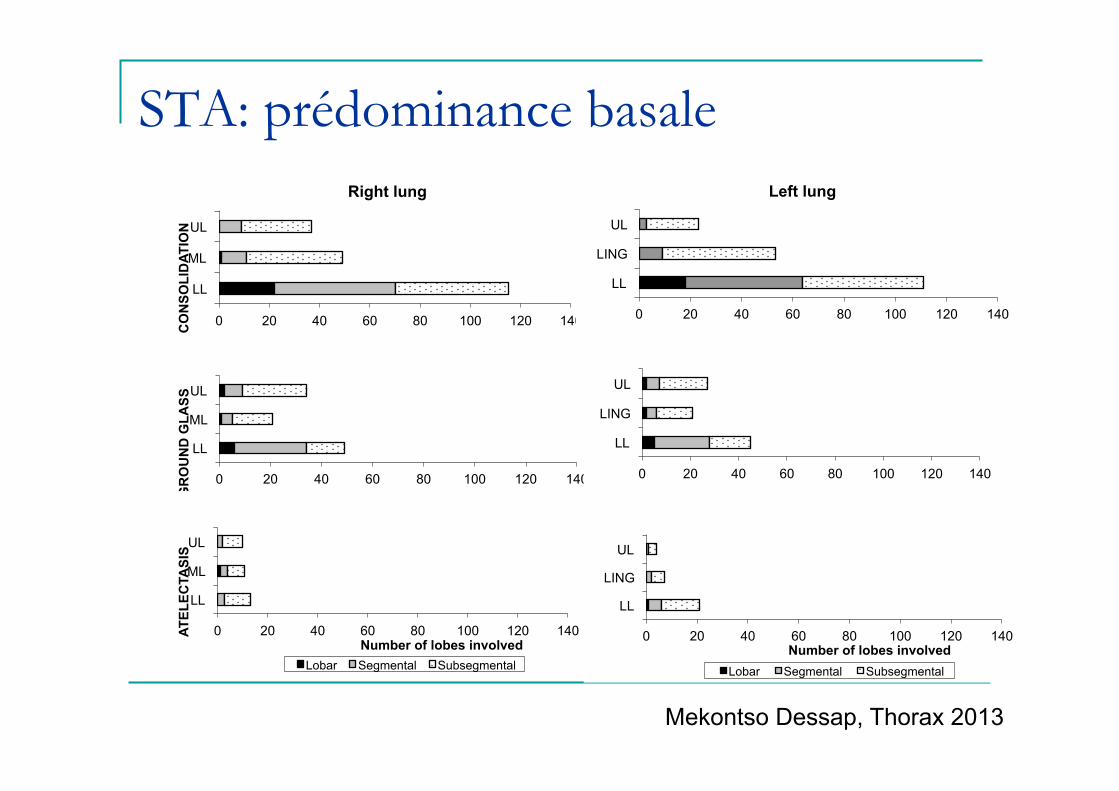
STA: prédominance basale
0 20 40 60 80 100 120 140
LL
ML
UL
CO
NSO
LID
ATIO
N
Right lung
0 20 40 60 80 100 120 140
LL
LING
UL
Left lung
0 20 40 60 80 100 120 140
LL
ML
UL
GR
OU
ND
GLA
SS
0 20 40 60 80 100 120 140
LL
LING
UL
0 20 40 60 80 100 120 140
LL
ML
UL
Number of lobes involved
ATEL
ECTA
SIS
Lobar Segmental Subsegmental
0 20 40 60 80 100 120 140
LL
LING
UL
Number of lobes involved Lobar Segmental Subsegmental
Mekontso Dessap, Thorax 2013
Physiopathologie STA
Embolie graisseuse

Embolie graisseuse
Godeau AJRCCM 1996 Maitre, Chest 2000 Lechapt, AJRCCM 2003
Phospholipides
Acides gras libres
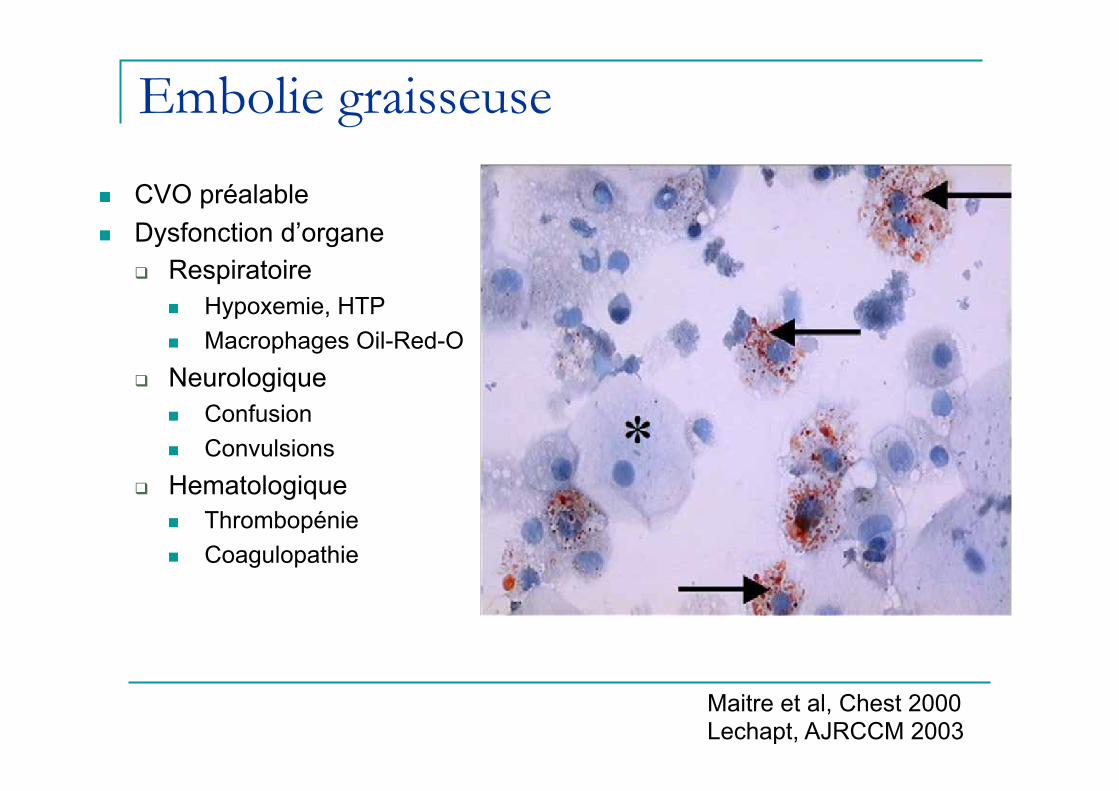
Embolie graisseuse
n CVO préalable n Dysfonction d’organe
q Respiratoire n Hypoxemie, HTP n Macrophages Oil-Red-O
q Neurologique n Confusion n Convulsions
q Hematologique n Thrombopénie n Coagulopathie
Maitre et al, Chest 2000 Lechapt, AJRCCM 2003

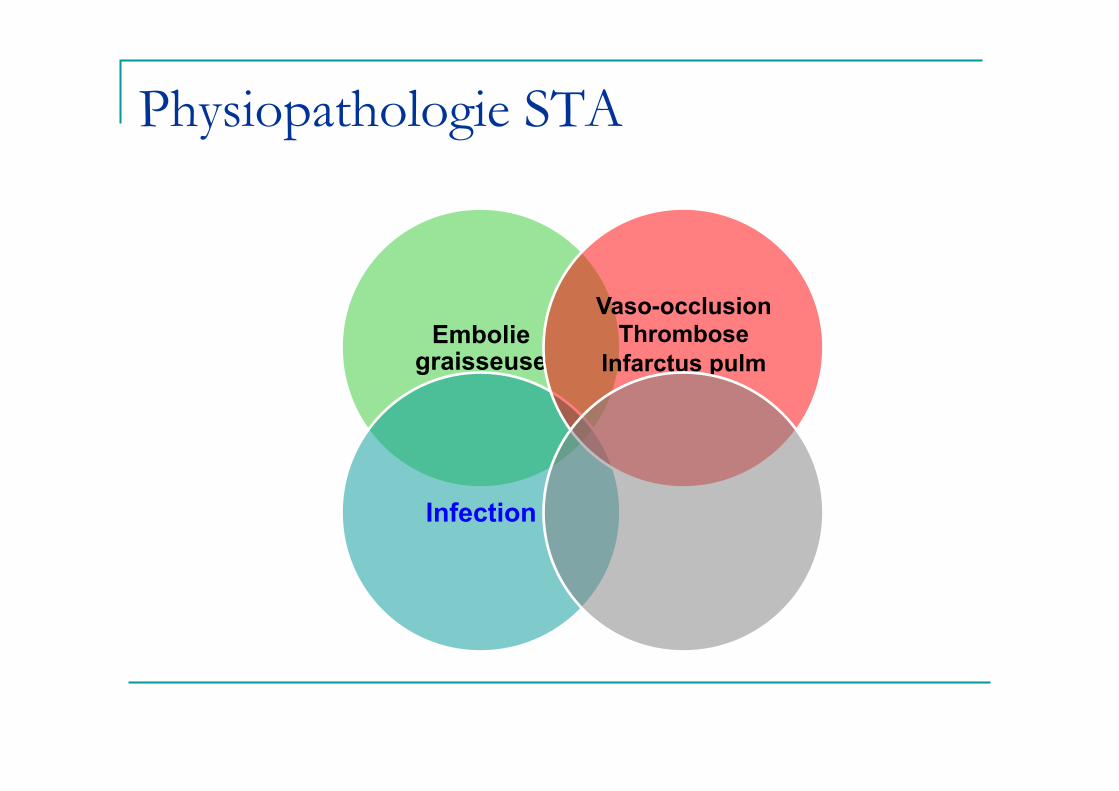
Physiopathologie STA
Embolie graisseuse
Vaso-occlusion Thrombose
Infarctus pulm
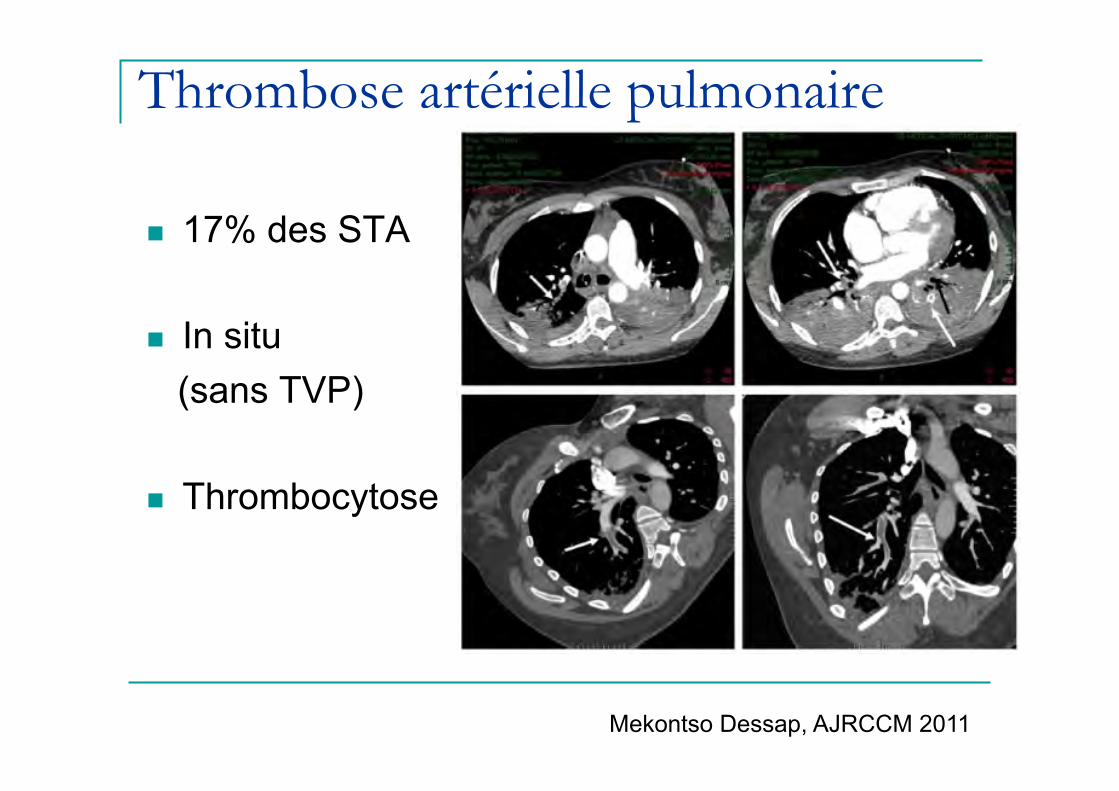
Thrombose artérielle pulmonaire
n 17% des STA
n In situ (sans TVP)
n Thrombocytose
Mekontso Dessap, AJRCCM 2011
Physiopathologie STA
Embolie graisseuse
Infection
Vaso-occlusion Thrombose
Infarctus pulm
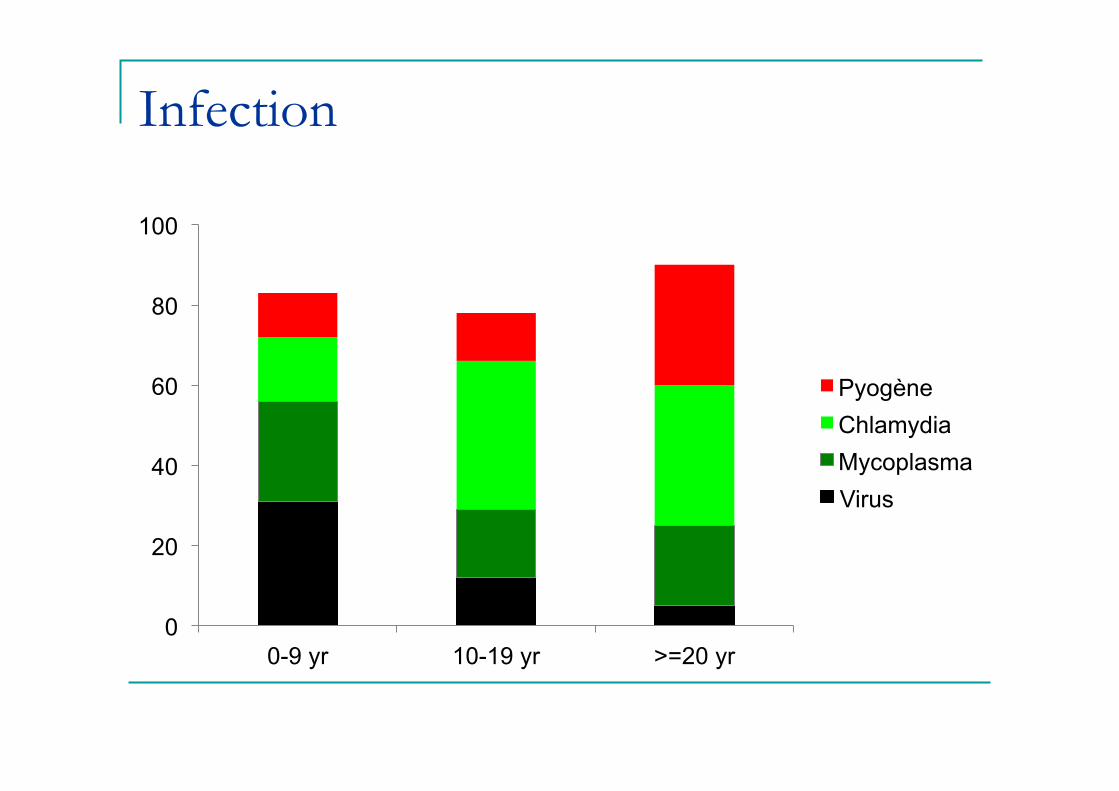
Infection
0
20
40
60
80
100
0-9 yr 10-19 yr >=20 yr
Pyogène Chlamydia Mycoplasma Virus

Physiopathologie STA
Embolie graisseuse
Infection
Vaso-occlusion Thrombose
Infarctus pulm
Infarctus costal Hypoventilation

Mécanismes du STA
42 47 52
36 21 26
15 23 10
7 9 12
0
20
40
60
80
100
0-9 yr 10-19 yr >=20 yr
Embolie graisse Infarctus Infection Inconnue
*Ni graisse ni infection Vichinsky, NEJM 2000
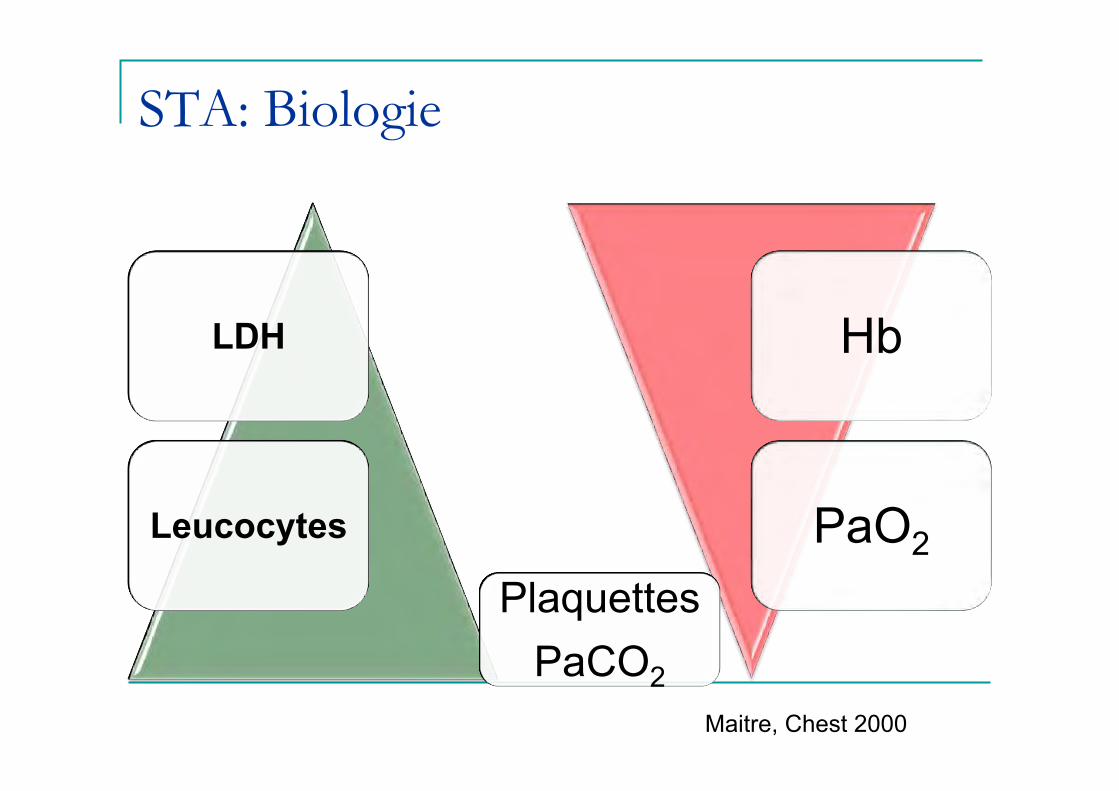
STA: Biologie
Hb
PaO2
LDH
Leucocytes
Maitre, Chest 2000
Plaquettes PaCO2
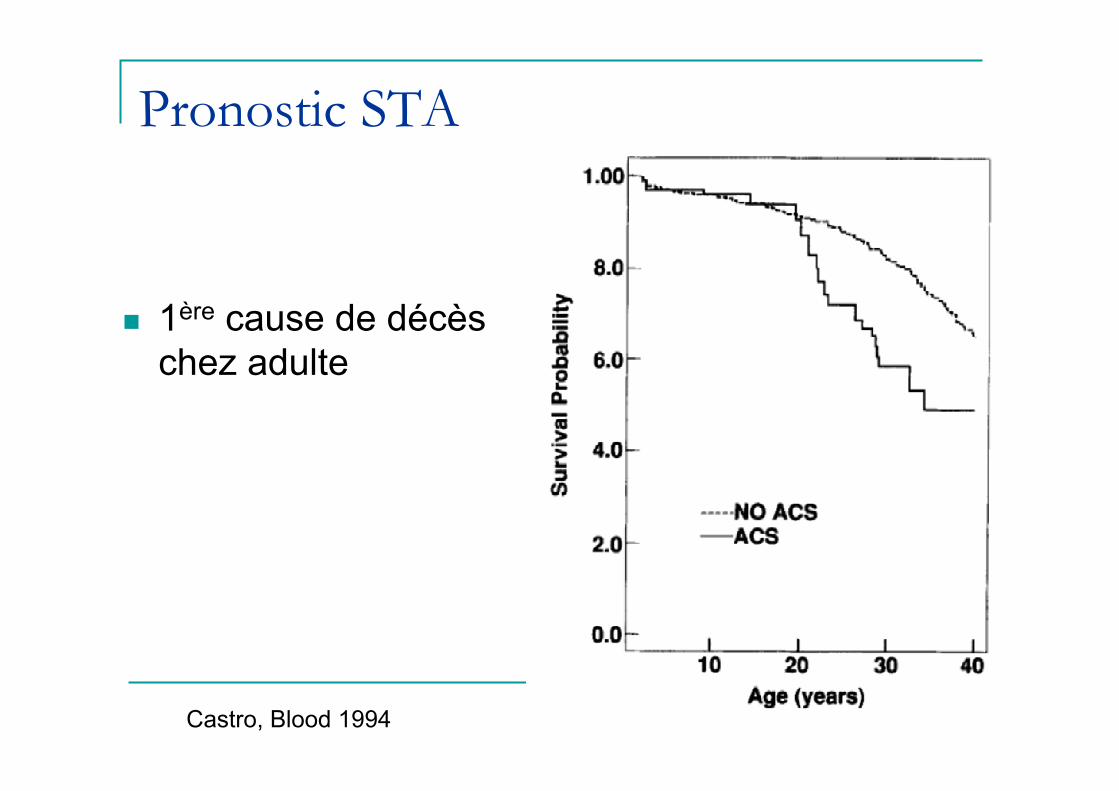
Pronostic STA
n 1ère cause de décès
chez adulte
Castro, Blood 1994
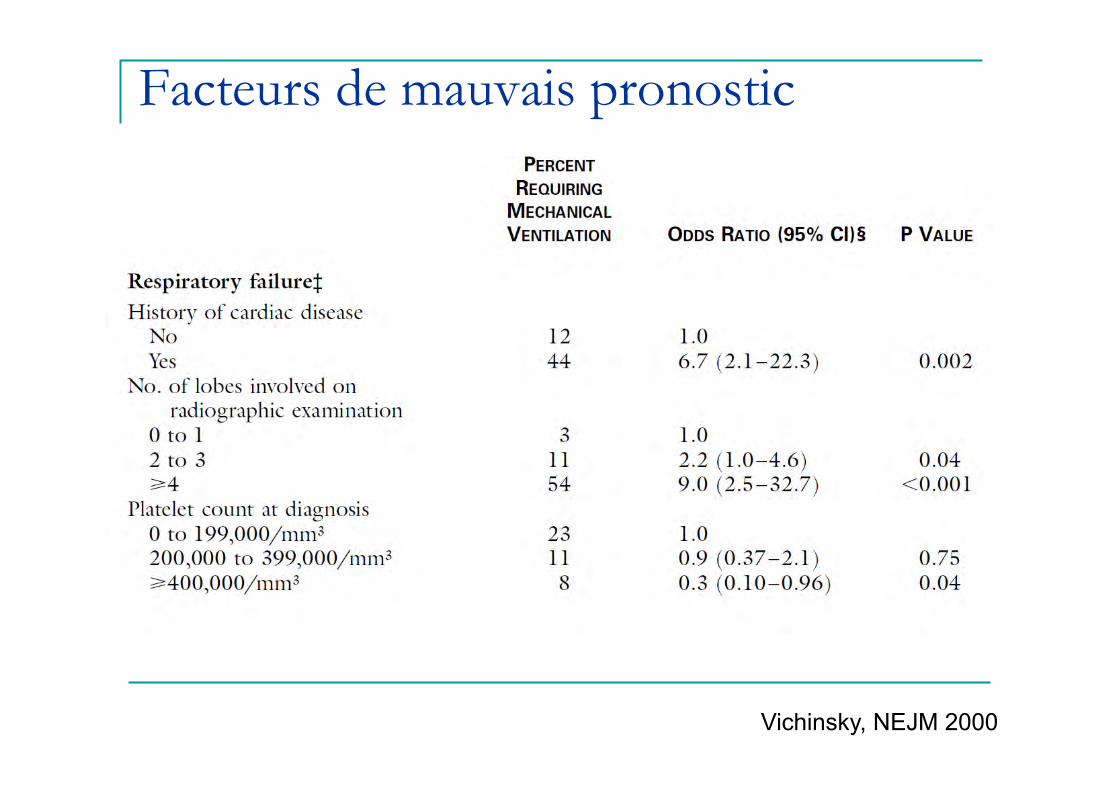
Facteurs de mauvais pronostic
Vichinsky, NEJM 2000

Mekontso Dessap, AJRCCM 2008
HTP aigue du STA
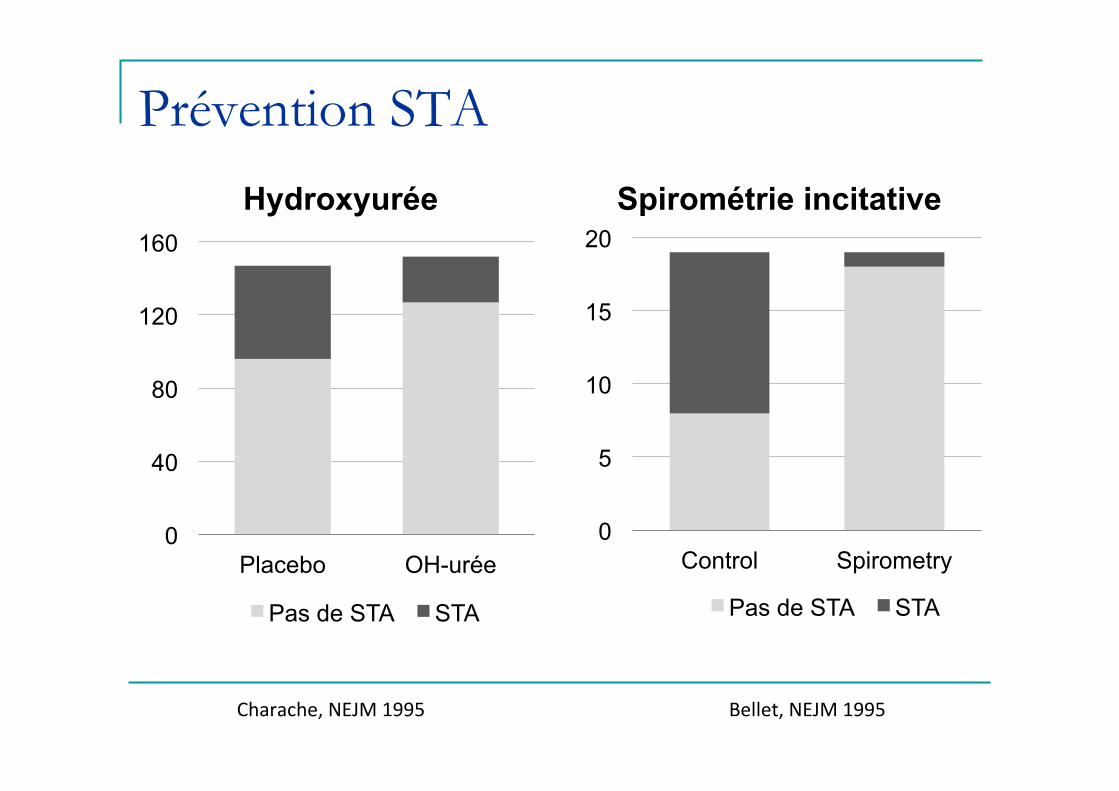
Prévention STA
Hydroxyurée Spirométrie incitative
0
5
10
15
20
Control Spirometry
Pas de STA STA
Bellet, NEJM 1995 Charache, NEJM 1995
0
40
80
120
160
Placebo OH-urée
Pas de STA STA
Traitement STA
n Hydratation n Oxygène±VNI n Analgésie n Transfusion /
Echange transfusionnel
n Antibiotiques n Stéroïdes ? n iNO ?

Analgésie multimodale
n Morphine q Titration q PCA
n Paracétamol n Nefopam n ±Kétamine n ± Protoxyde d’azote
Bartolucci, Blood 2009

Exsanguino-transfusion n Rationnel:
q ⇧ TaO2, ⇩ HbS
n Indications: q signes de sévérité, absence amélioration q Hb < 6g/dl q sepsis q programme transfusionnel chronique q grossesse, post-partum, post-opératoire
n Objectifs: q Hb de base (<10 g/dL) q HbS< 30% dans les cas sévères
n Prévention allo-immunisation: q Iso-groupe, iso Rhesus, phenotypé

Alloimmunisation
n 20-50% des patients n Différences
antigéniques raciales entre donneurs et receveurs: q Rhésus: C, E q Kell: K q Duffy: Fya q Kidd: Jkb (JK) q MNS: S
Yazdanbakhsh, Blood 2012
Hémolyse retardée post transfusionnelle PRESENTATION
n >J3 transfusion
n CVO±STA
n Anémie multifactorielle q Hémolyse (hémoglobinurie, ↑LDH)
n GR transfusés n ±GR autologues n Alloimmunisation parfois
absente ou non-imputable q ± Réticulocytopénie
TRAITEMENT n Eviter nouvelle transfusion
n EPO si reticulocytopénie
n Immunomodulation? q Corticoides q Ig q Rituximab (anti CD20) q Eculizimab (anti C5b-9)

Anémie selon réticulocytes
ELEVES n Hémolyse
q CVO q Paludisme q AHAI q Post transfusionnelle
n Séquestration q splénique q hépatique
n Hémorragie
BAS n Carences (fer, folates) n Inflammation n Insuffisance rénale n Toxicité OH-urée n Nécrose médullaire n Crise aplastique
Anémie selon réticulocytes
BAS n Nécrose médullaire n Crise aplastique n Carences (fer, folates) n Inflammation n Insuffisance rénale n Toxicité OHurée
ELEVES n Hémolyse
q Post transfusionnelle q CVO q Paludisme q AHAI
n Séquestration q splénique q Hépatique
n Hémorragie
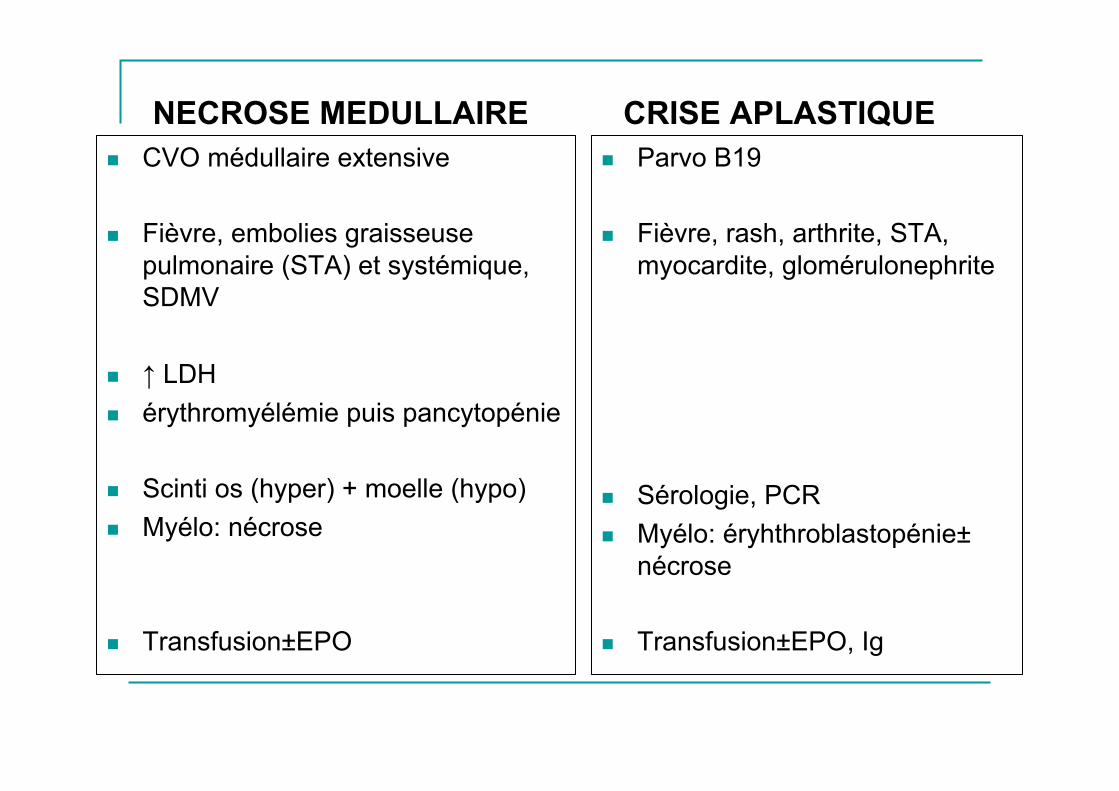
NECROSE MEDULLAIRE n CVO médullaire extensive n Fièvre, embolies graisseuse
pulmonaire (STA) et systémique, SDMV
n ↑ LDH n érythromyélémie puis pancytopénie n Scinti os (hyper) + moelle (hypo) n Myélo: nécrose
n Transfusion±EPO
CRISE APLASTIQUE n Parvo B19 n Fièvre, rash, arthrite, STA,
myocardite, glomérulonephrite n Sérologie, PCR n Myélo: éryhthroblastopénie±
nécrose
n Transfusion±EPO, Ig

Antibiotiques et STA n Rationnel
q ⇧ risque infectieux (asplénie) q STA non discernable de la pneumonie q Causes infectieuses rapportées, même si rares en routine clinique
§ Kirkpatrick Am J Med 1991
n Indication q Quasi-systématique, notamment si fièvre
n Objectifs q S. pneumoniae et intracellulaires q Example: amoxicilline+macrolide
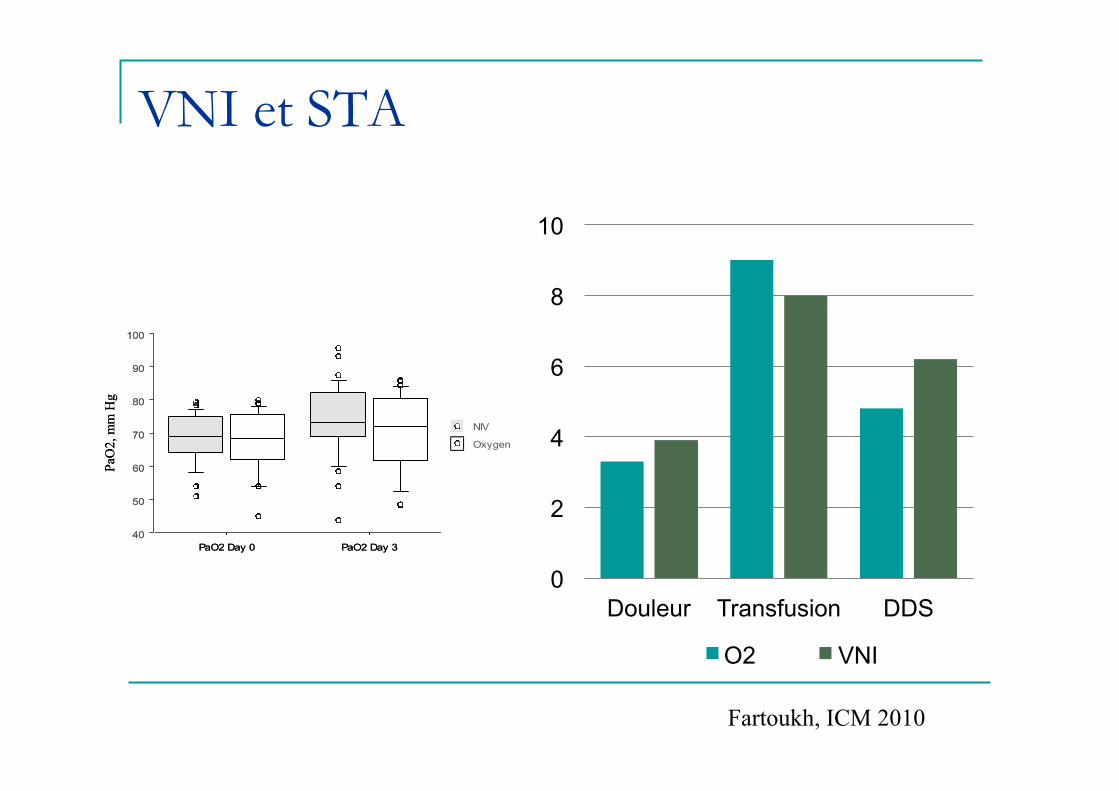
VNI et STA
0
2
4
6
8
10
Douleur Transfusion DDS
O2 VNI
PaO
2, m
m H
g
40
50
60
70
80
90
100
PaO2 Day 0 PaO2 Day 3
Oxygen
NIV
PaO
2, m
m H
g
40
50
60
70
80
90
100
PaO2 Day 0 PaO2 Day 3
Oxygen
NIV
Fartoukh, ICM 2010
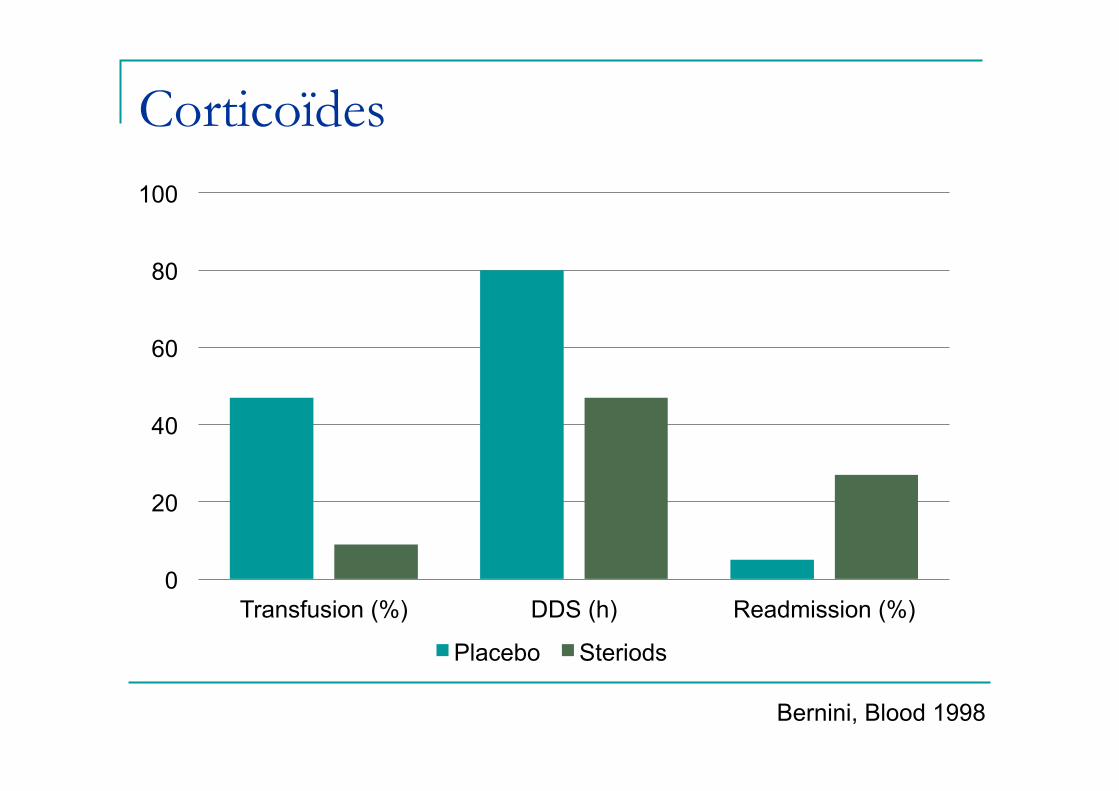
Corticoïdes
0
20
40
60
80
100
Transfusion (%) DDS (h) Readmission (%)
Placebo Steriods
Bernini, Blood 1998
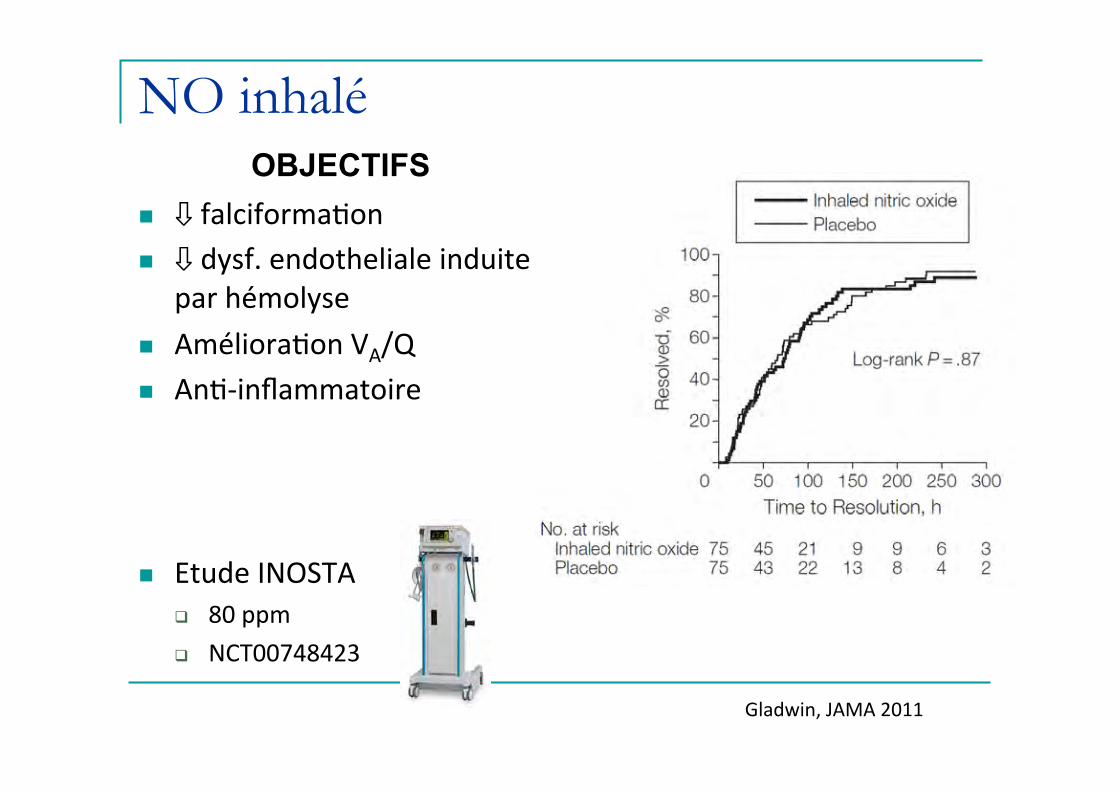
NO inhalé OBJECTIFS
n ⇩ falciforma�on n ⇩ dysf. endotheliale induite
par hémolyse n Améliora�on VA/Q n An�-‐inflammatoire
n Etude INOSTA q 80 ppm q NCT00748423
Gladwin, JAMA 2011
Conclusion
n Signes de sévérité STA q Défaillance cardiaque droite
n Traitement STA q Symptomatique
n Analgésie n Hydratation n Oxygène n Transfusion sauf hémolyse post-transfusionnelle
retardée q Etiologique
n Antibiotiques / Anticoagulants si TAP q En cas d’intubation
n Ventilation protectrice; attention particulière pour HTP



![[PPT]Slide 1 · Web viewLa prévention du paludisme chez le drépanocytaire en Afrique à l’ère des résistances aux antipaludiques Atelier « drépanocytose Monaco» Novotel Hotel,](https://img.pdfslide.us/doc/110x75/5b995e4609d3f210688bce87/pptslide-1-web-viewla-prevention-du-paludisme-chez-le-drepanocytaire-en.jpg)