Embed Size (px)
Citation preview
EER quand, comment ? Pr. Nicolas Lerolle Département de réanima5on médicale et médecine hyperbare
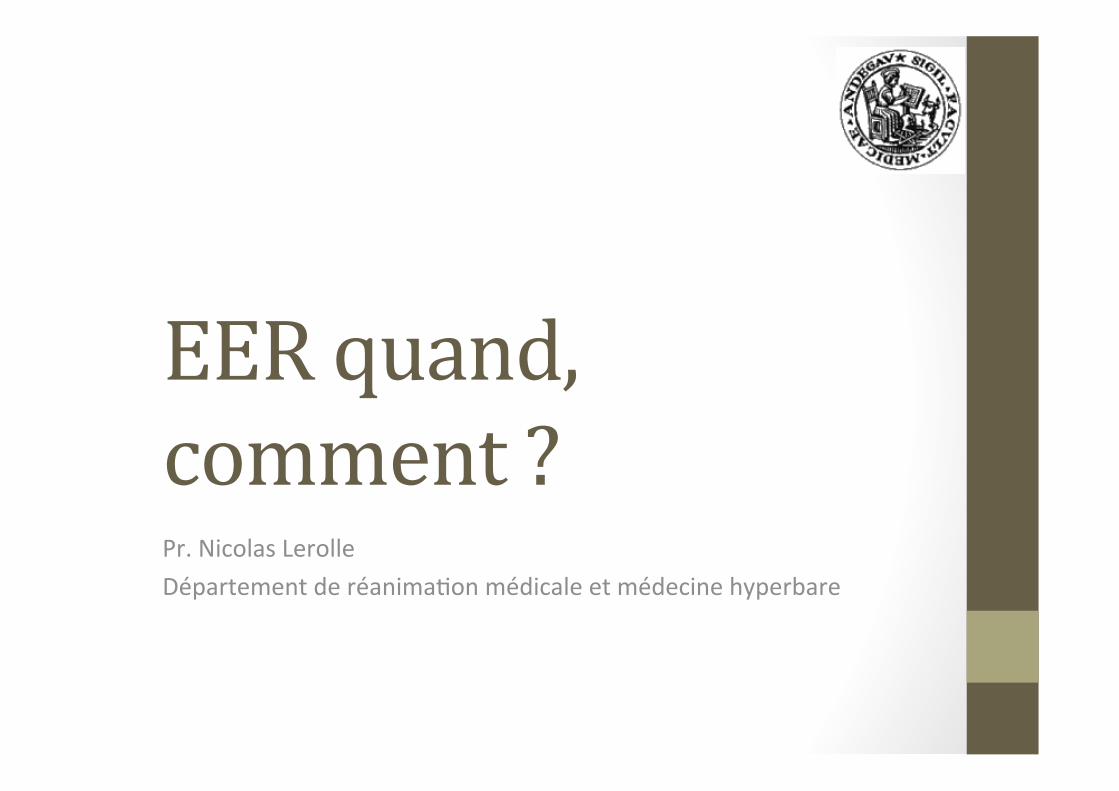
Duration of hypotension before initiation of effective antimicrobialtherapy is the critical determinant of survival in human septic shock*
Anand Kumar, MD; Daniel Roberts, MD; Kenneth E. Wood, DO; Bruce Light, MD; Joseph E. Parrillo, MD;Satendra Sharma, MD; Robert Suppes, BSc; Daniel Feinstein, MD; Sergio Zanotti, MD; Leo Taiberg, MD;David Gurka, MD; Aseem Kumar, PhD; Mary Cheang, MSc
on. (Crit Care Med 2006; 34:1589 1596)Y WORDS: sepsis; antimicrobial; timing; de
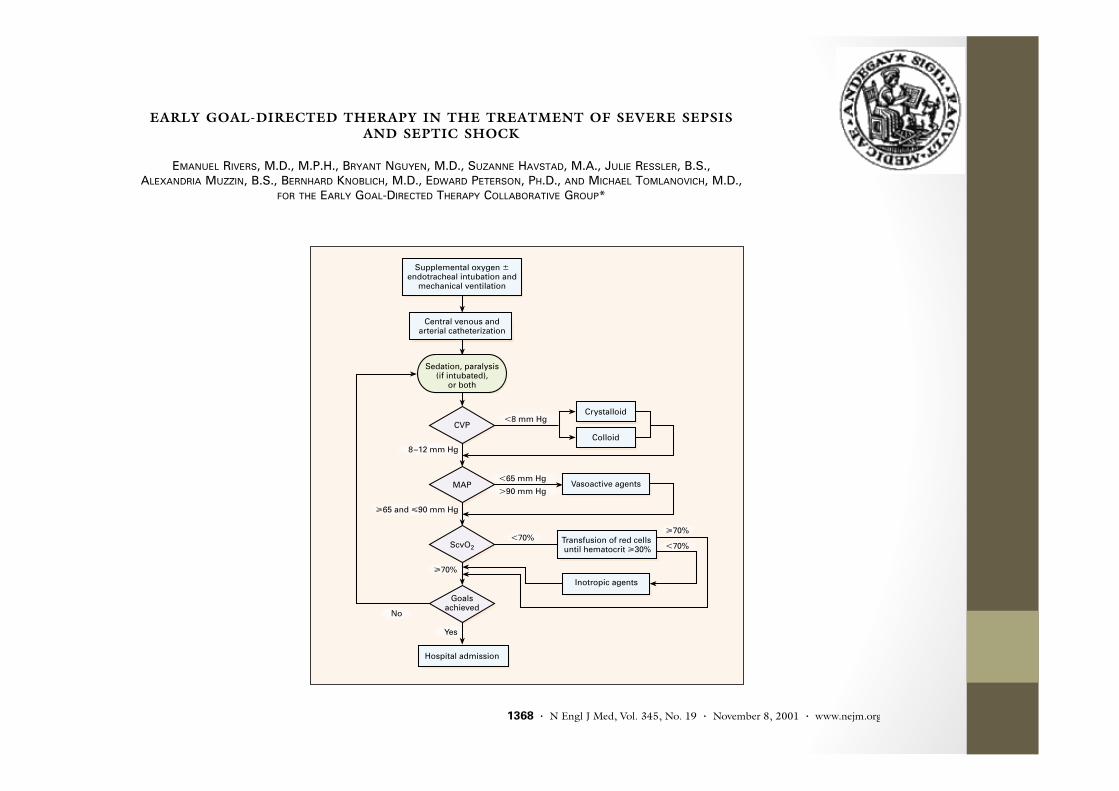
EARLY GOAL-DIRECTED THERAPY IN THE TREATMENT OF SEVERE SEPSIS AND SEPTIC SHOCK
E
MANUEL
R
IVERS
, M.D., M.P.H., B
RYANT
N
GUYEN
, M.D., S
UZANNE
H
AVSTAD
, M.A., J
ULIE
R
ESSLER
, B.S., A
LEXANDRIA
M
UZZIN
, B.S., B
ERNHARD
K
NOBLICH
, M.D., E
DWARD
P
ETERSON
, P
H
.D.,
AND
M
ICHAEL
T
OMLANOVICH
, M.D.,
FOR
THE
E
ARLY
G
OAL
-D
IRECTED
T
HERAPY
C
OLLABORATIVE
G
ROUP
*
<8 mm Hg
Supplemental oxygen ±endotracheal intubation and
mechanical ventilation
Central venous andarterial catheterization
Sedation, paralysis(if intubated),
or both
CVP
MAP
ScvO2
Goalsachieved
Hospital admission
Crystalloid
Colloid
Vasoactive agents
Transfusion of red cells until hematocrit »30%
Inotropic agents
<65 mm Hg
>90 mm Hg
8–12 mm Hg
»65 and «90 mm Hg
No
Yes
<70%<70%
»70%
»70%
1368
·
N Engl J Med, Vol. 345, No. 19
·
November 8, 2001
·
www.nejm.org
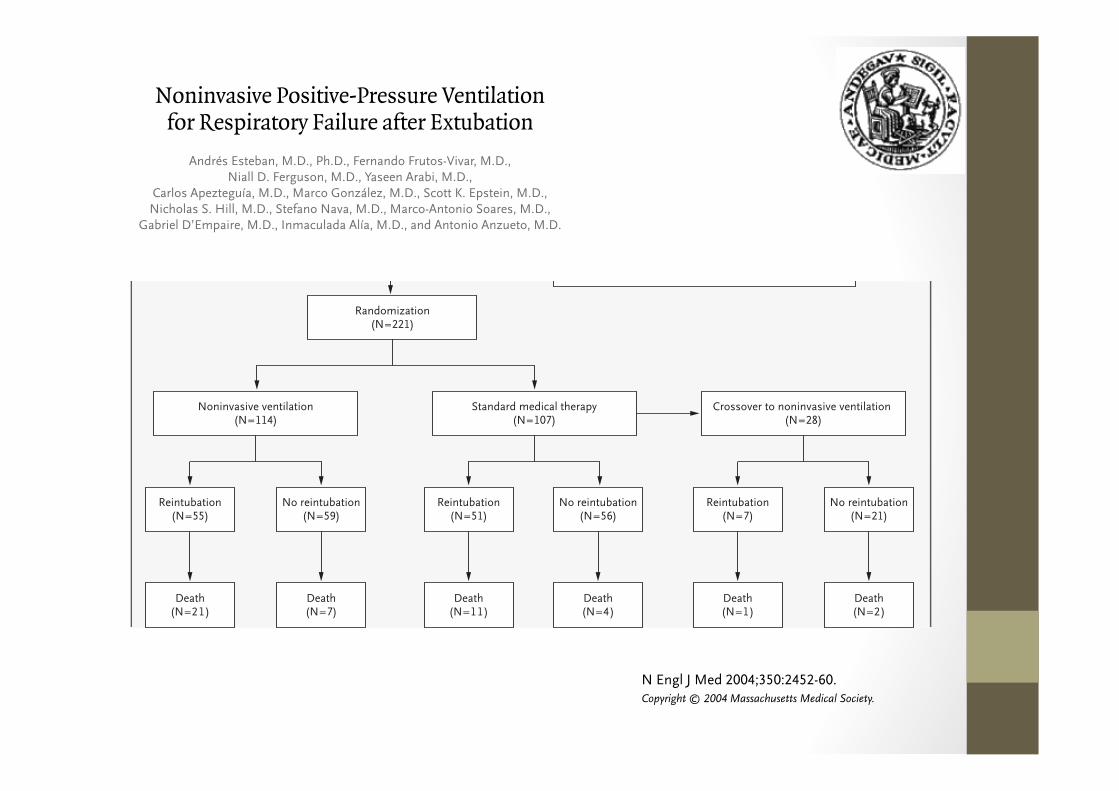
Randomization(N=221)
Noninvasive ventilation(N=114)
Standard medical therapy(N=107)
Crossover to noninvasive ventilation (N=28)
Reintubation(N=55)
No reintubation(N=59)
Reintubation(N=51)
No reintubation(N=56)
Reintubation(N=7)
No reintubation(N=21)
Death(N=21)
Death(N=7)
Death(N=11)
Death(N=4)
Death(N=1)
Death(N=2)
Noninvasive Positive-Pressure Ventilation for Respiratory Failure after Extubation
Andrés Esteban, M.D., Ph.D., Fernando Frutos-Vivar, M.D., Niall D. Ferguson, M.D., Yaseen Arabi, M.D.,
Carlos Apezteguía, M.D., Marco González, M.D., Scott K. Epstein, M.D., Nicholas S. Hill, M.D., Stefano Nava, M.D., Marco-Antonio Soares, M.D.,
Gabriel D’Empaire, M.D., Inmaculada Alía, M.D., and Antonio Anzueto, M.D.
N Engl J Med 2004;350:2452-60.
Copyright © 2004 Massachusetts Medical Society.
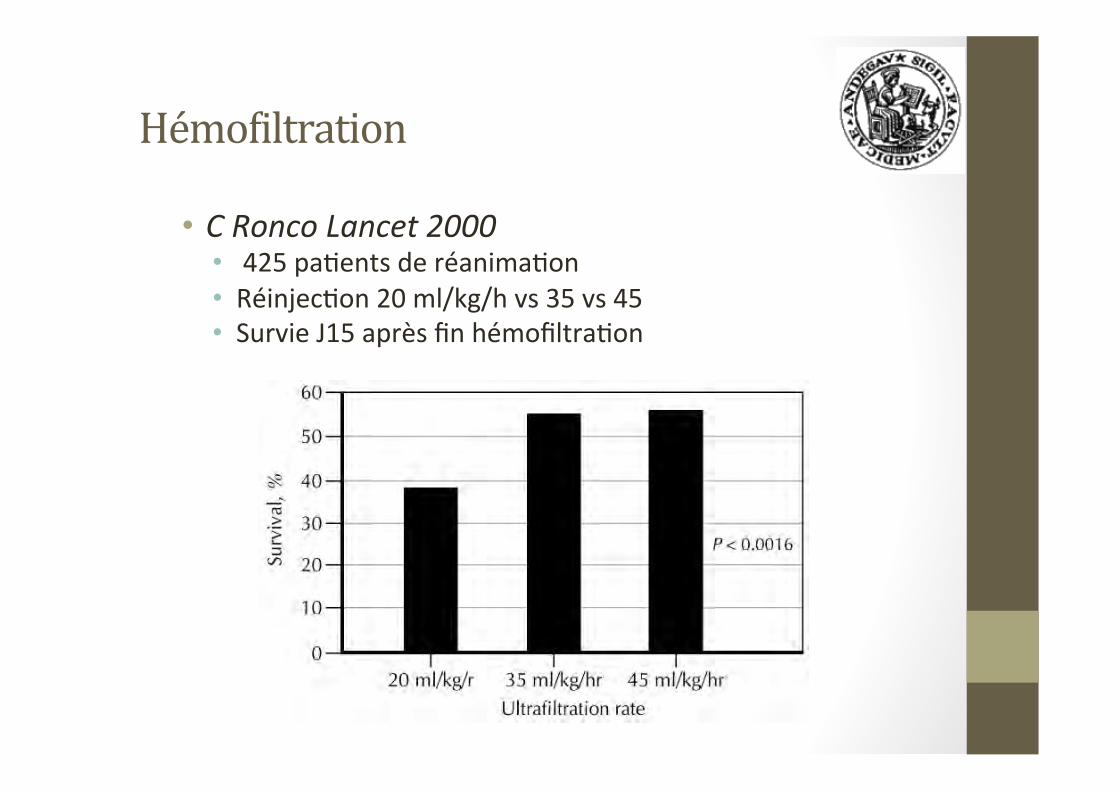
Hémo2iltration
• C Ronco Lancet 2000 • 425 pa5ents de réanima5on • Réinjec5on 20 ml/kg/h vs 35 vs 45 • Survie J15 après fin hémofiltra5on
RESEARCH Open Access
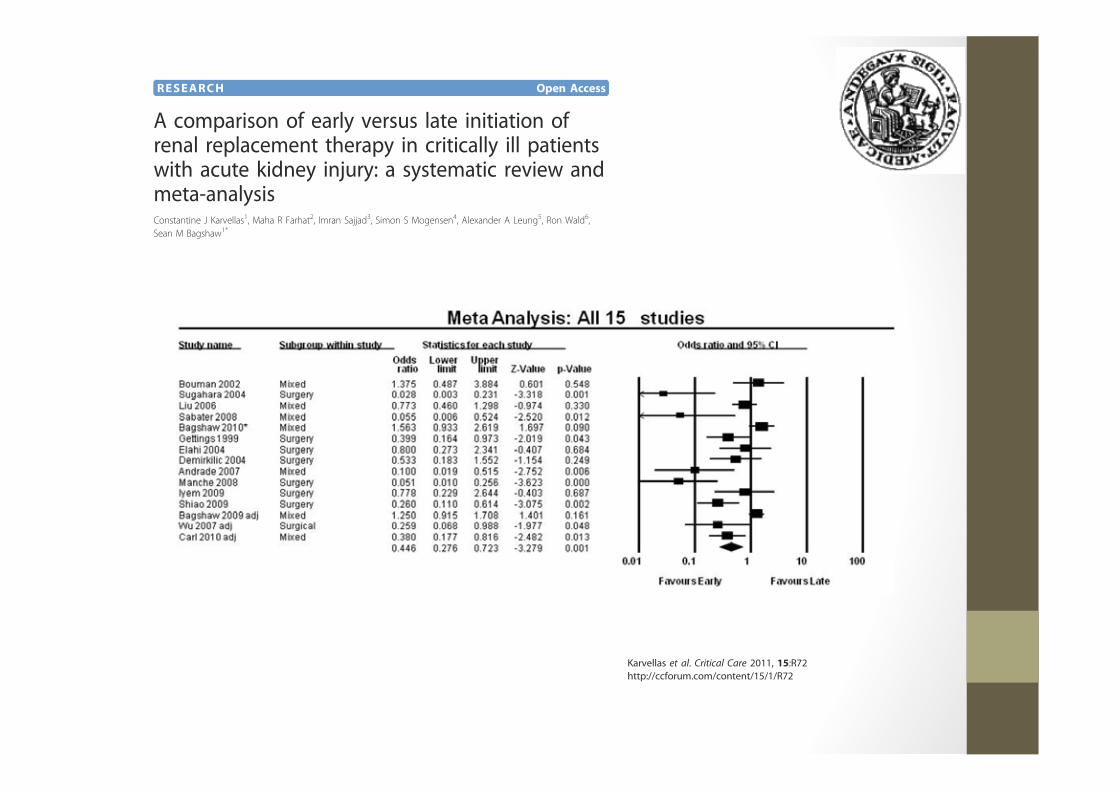
A comparison of early versus late initiation ofrenal replacement therapy in critically ill patientswith acute kidney injury: a systematic review andmeta-analysisConstantine J Karvellas1, Maha R Farhat2, Imran Sajjad3, Simon S Mogensen4, Alexander A Leung5, Ron Wald6,Sean M Bagshaw1*
Karvellas et al. Critical Care 2011, 15:R72http://ccforum.com/content/15/1/R72

louise
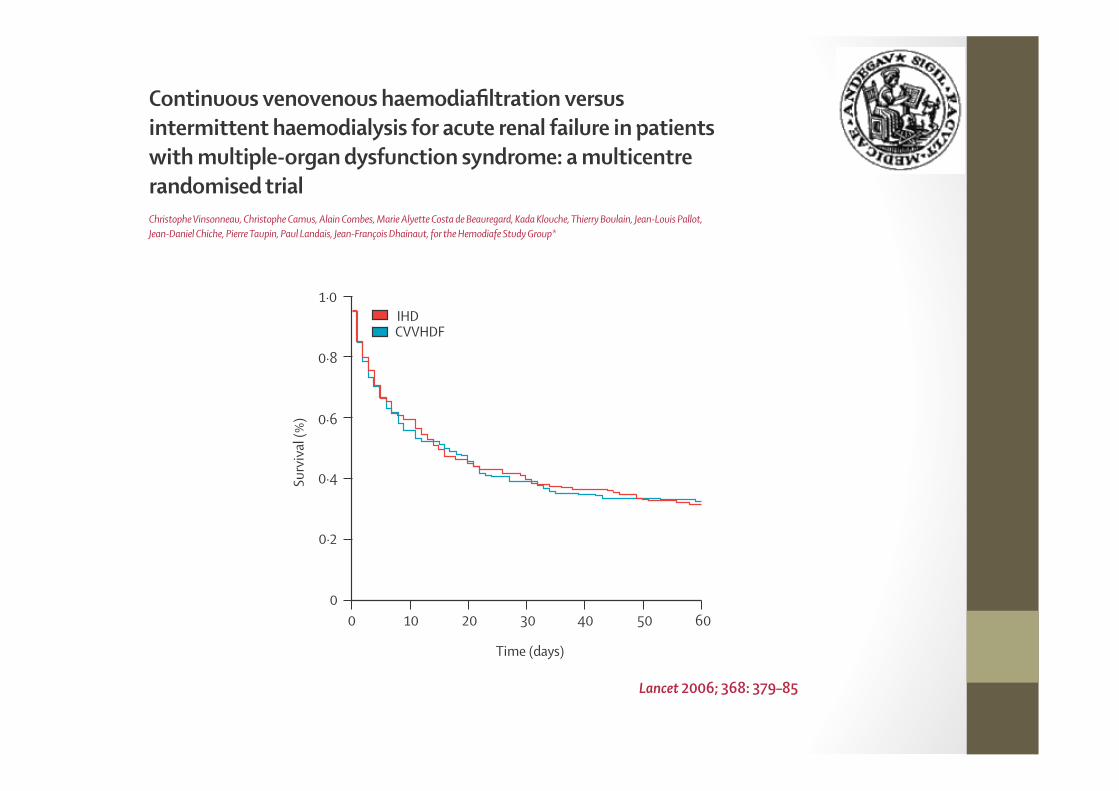
Continuous venovenous haemodiafi ltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: a multicentre randomised trialChristophe Vinsonneau, Christophe Camus, Alain Combes, Marie Alyette Costa de Beauregard, Kada Klouche, Thierry Boulain, Jean-Louis Pallot, Jean-Daniel Chiche, Pierre Taupin, Paul Landais, Jean-François Dhainaut, for the Hemodiafe Study Group*
00
0·2
0·4
0·6
0·8
1·0
10 20 30 40 50 60
Surv
ival
(%)
Time (days)
CVVHDFIHD
Lancet 2006; 368: 379–85
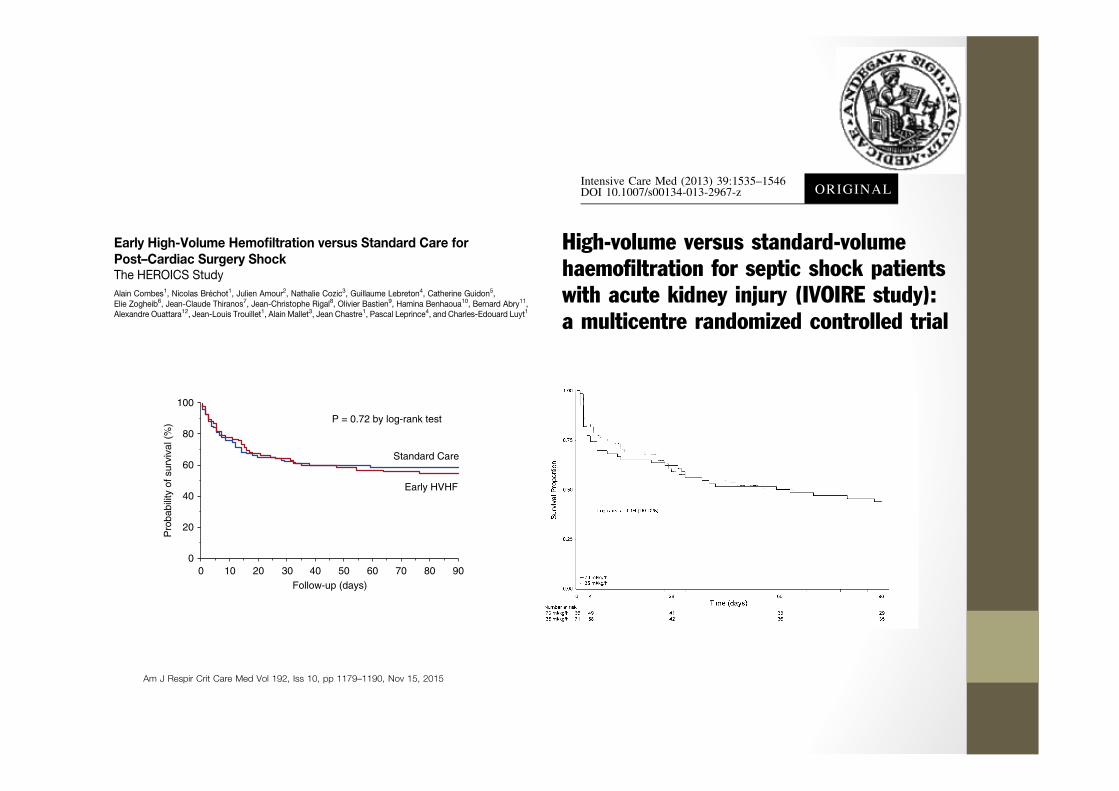
High-volume versus standard-volumehaemofiltration for septic shock patientswith acute kidney injury (IVOIRE study):a multicentre randomized controlled trial
Intensive Care Med (2013) 39:1535–1546DOI 10.1007/s00134-013-2967-z ORIGINAL
Early High-Volume Hemofiltration versus Standard Care forPost–Cardiac Surgery ShockThe HEROICS StudyAlain Combes1, Nicolas Brechot1, Julien Amour2, Nathalie Cozic3, Guillaume Lebreton4, Catherine Guidon5,Elie Zogheib6, Jean-Claude Thiranos7, Jean-Christophe Rigal8, Olivier Bastien9, Hamina Benhaoua10, Bernard Abry11,Alexandre Ouattara12, Jean-Louis Trouillet1, Alain Mallet3, Jean Chastre1, Pascal Leprince4, and Charles-Edouard Luyt1
Am J Respir Crit Care Med Vol 192, Iss 10, pp 1179–1190, Nov 15, 2015
C i ht © 2015 b th A i Th i S i t
0
20
40
60
80
100
Follow-up (days)
Pro
babi
lity
of s
urvi
val (
%)
Standard Care
P = 0.72 by log-rank test
Early HVHF
100 20 30 40 50 60 70 80 90
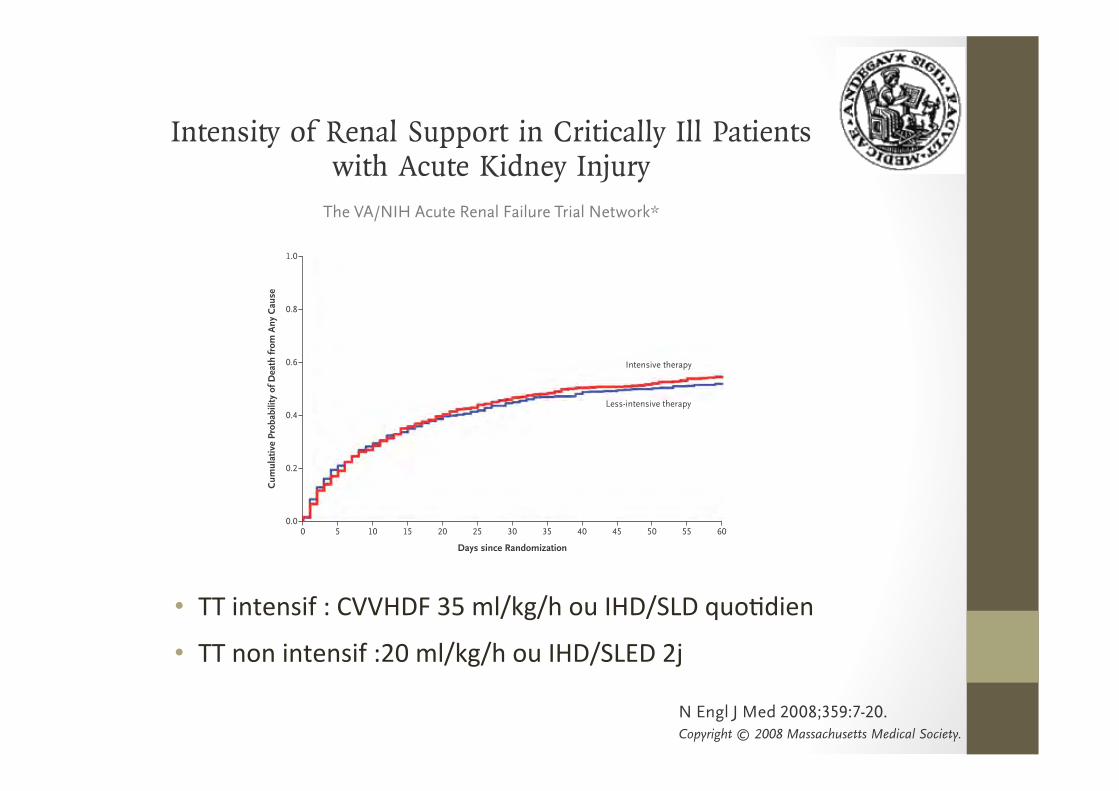
• TT intensif : CVVHDF 35 ml/kg/h ou IHD/SLD quo5dien
• TT non intensif :20 ml/kg/h ou IHD/SLED 2j
Intensity of Renal Support in Critically Ill Patients with Acute Kidney Injury
The VA/NIH Acute Renal Failure Trial Network*
1.0
0.8
0.6
0.4
0.2
0.00 10 20 30 40 50 605 15 25 35 45 55
Intensive therapy
Less-intensive therapy
N Engl J Med 2008;359:7-20.Copyright © 2008 Massachusetts Medical Society.
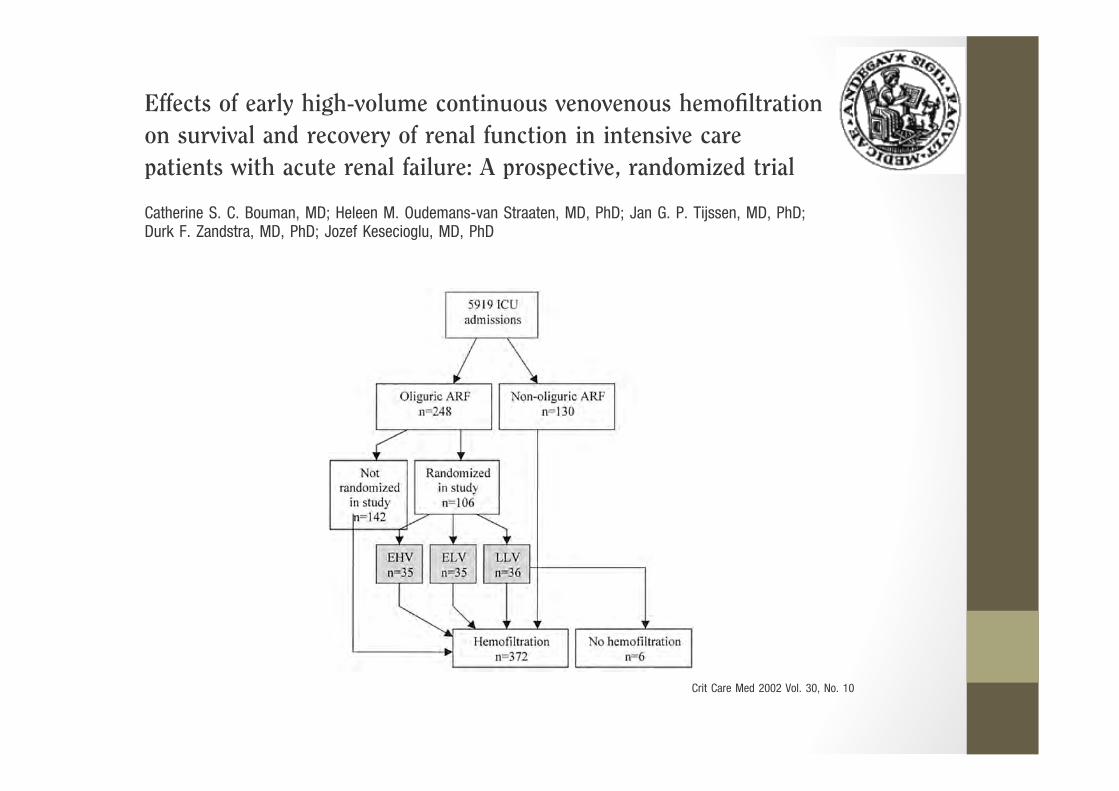
Effects of early high-volume continuous venovenous hemofiltrationon survival and recovery of renal function in intensive carepatients with acute renal failure: A prospective, randomized trial
Catherine S. C. Bouman, MD; Heleen M. Oudemans-van Straaten, MD, PhD; Jan G. P. Tijssen, MD, PhD;Durk F. Zandstra, MD, PhD; Jozef Kesecioglu, MD, PhD
Crit Care Med 2002 Vol. 30, No. 10
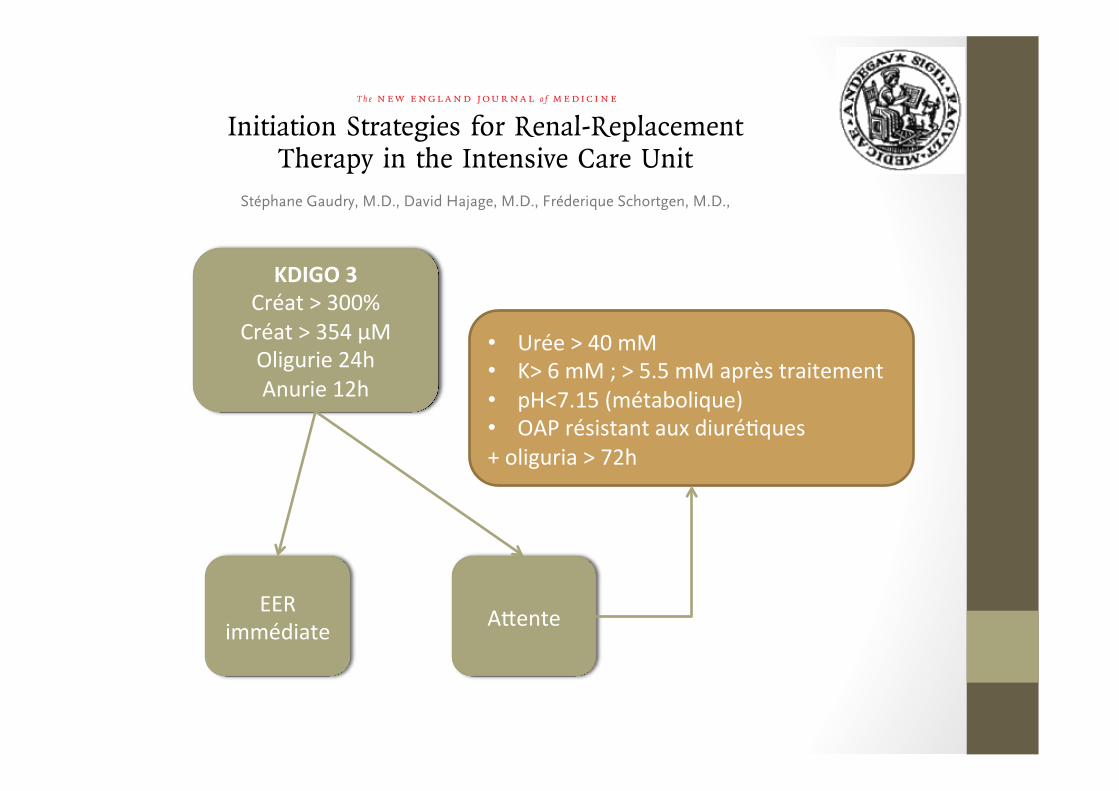
Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit
Stéphane Gaudry, M.D., David Hajage, M.D., Fréderique Schortgen, M.D.,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
KDIGO 3 Créat > 300% Créat > 354 µM Oligurie 24h Anurie 12h
• Urée > 40 mM • K> 6 mM ; > 5.5 mM après traitement • pH<7.15 (métabolique) • OAP résistant aux diuré5ques + oliguria > 72h
EER immédiate Adente
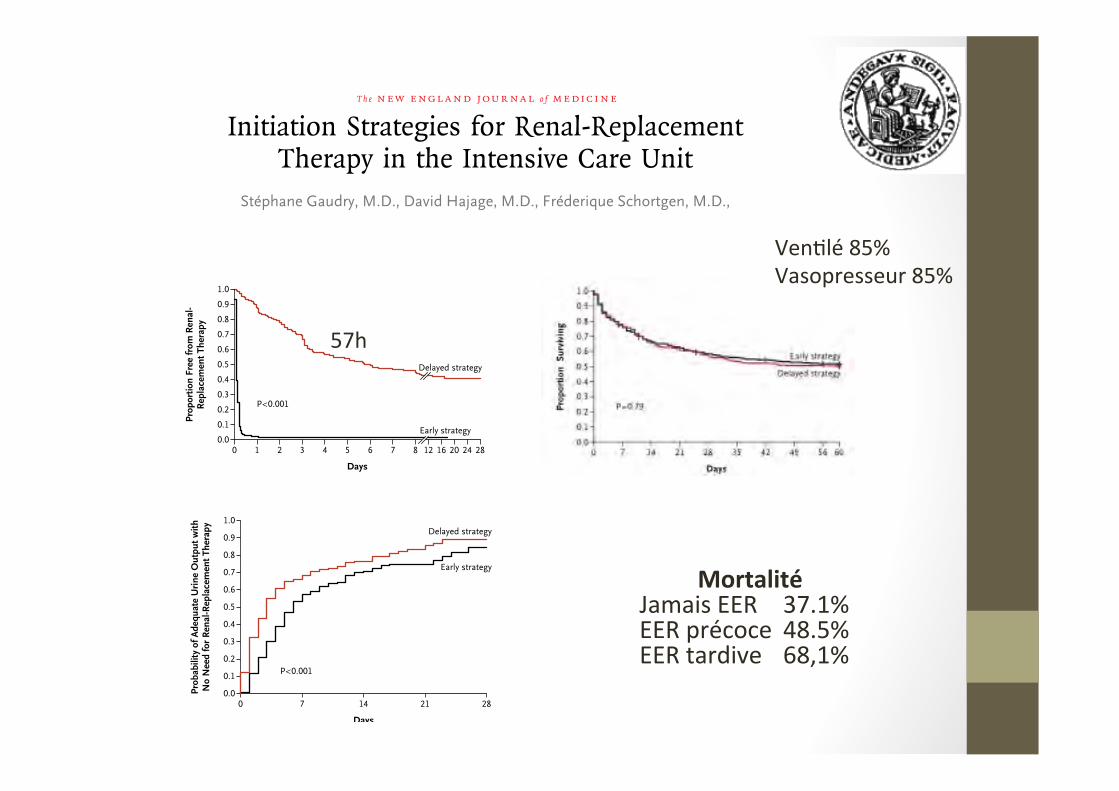
Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit
Stéphane Gaudry, M.D., David Hajage, M.D., Fréderique Schortgen, M.D.,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Prop
ortio
n Fr
ee fr
om R
enal
-R
epla
cem
ent T
hera
py
1.0
0.8
0.9
0.7
0.6
0.4
0.3
0.1
0.5
0.2
0.00 1 2 3 4 6 28
Days
P<0.001
5 247 8 12 16 20
Early strategy
Delayed strategy
Prob
abili
ty o
f Ade
quat
e U
rine
Out
put w
ithN
o N
eed
for
Ren
al-R
epla
cem
ent T
hera
py
1.0
0.8
0.9
0.7
0.6
0.4
0.3
0.1
0.5
0.2
0.00 7 14 21 28
Days
P<0.001
Early strategy
Delayed strategy
Mortalité Jamais EER 37.1% EER précoce 48.5% EER tardive 68,1%
57h
Ven5lé 85% Vasopresseur 85%

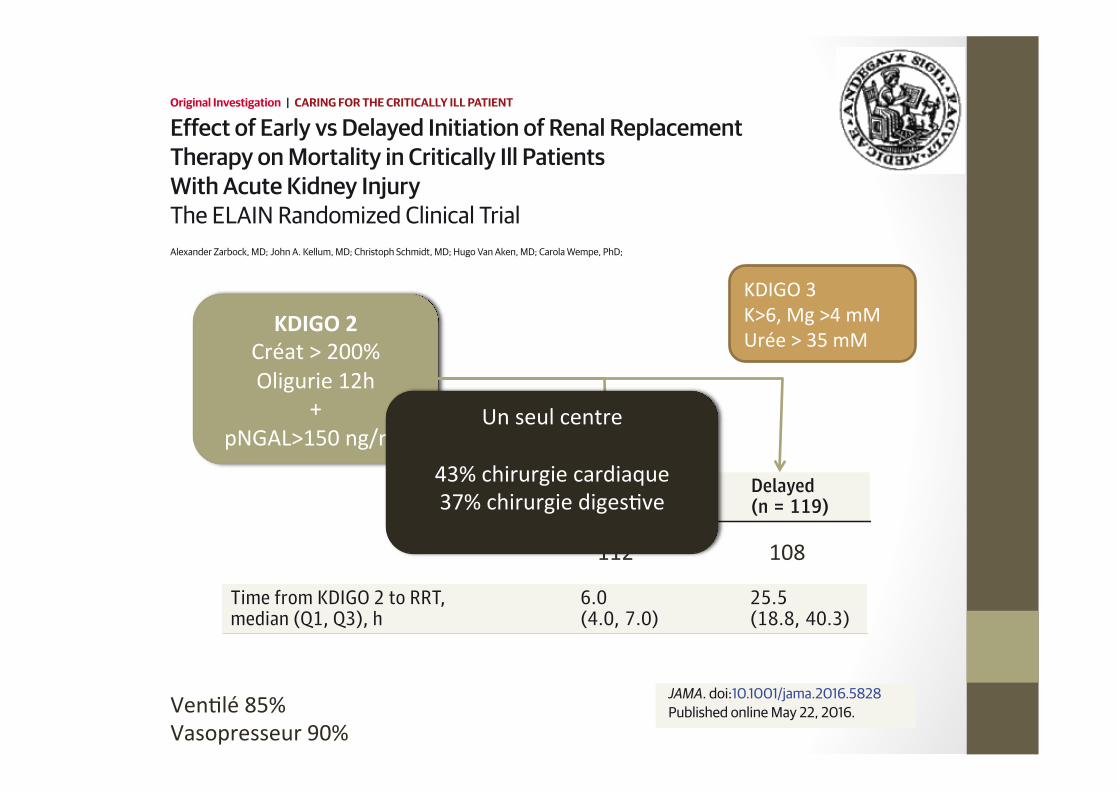
Effect of Early vs Delayed Initiation of Renal ReplacementTherapy onMortality in Critically Ill PatientsWith Acute Kidney InjuryThe ELAIN Randomized Clinical TrialAlexander Zarbock, MD; John A. Kellum, MD; Christoph Schmidt, MD; Hugo Van Aken, MD; Carola Wempe, PhD;
Original Investigation | CARING FORTHE CRITICALLY ILL PATIENT
JAMA. doi:10.1001/jama.2016.5828Published online May 22, 2016.
Ven5lé 85% Vasopresseur 90%
Time from KDIGO 2 to RRT,median (Q1, Q3), h
6.0(4.0, 7.0)
25.5(18.8, 40.3)
Early(n = 112)
Delayed(n = 119)
108 112
KDIGO 2 Créat > 200% Oligurie 12h
+ pNGAL>150 ng/mL
KDIGO 3 K>6, Mg >4 mM Urée > 35 mM
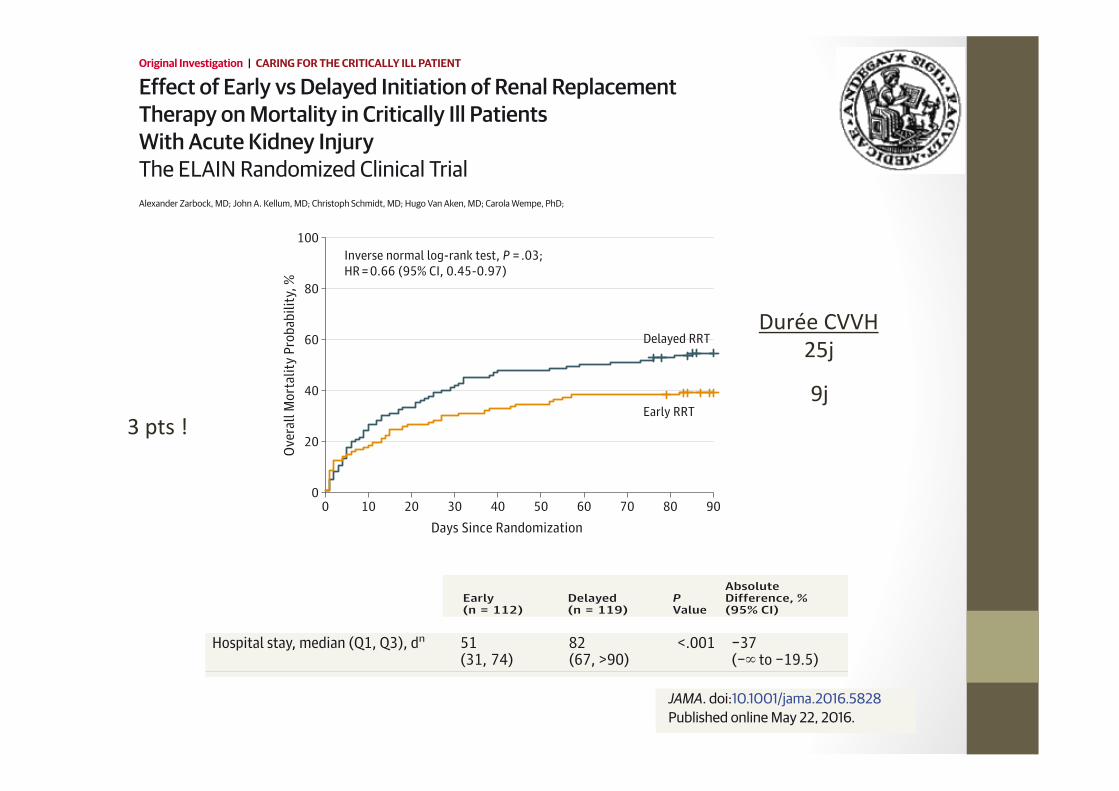
Effect of Early vs Delayed Initiation of Renal ReplacementTherapy onMortality in Critically Ill PatientsWith Acute Kidney InjuryThe ELAIN Randomized Clinical TrialAlexander Zarbock, MD; John A. Kellum, MD; Christoph Schmidt, MD; Hugo Van Aken, MD; Carola Wempe, PhD;
Original Investigation | CARING FORTHE CRITICALLY ILL PATIENT
JAMA. doi:10.1001/jama.2016.5828Published online May 22, 2016.
Ven5lé 85% Vasopresseur 90%
Time from KDIGO 2 to RRT,median (Q1, Q3), h
6.0(4.0, 7.0)
25.5(18.8, 40.3)
Early(n = 112)
Delayed(n = 119)
108 112
KDIGO 2 Créat > 200% Oligurie 12h
+ pNGAL>150 ng/mL
KDIGO 3 K>6, Mg >4 mM Urée > 35 mM
Un seul centre
43% chirurgie cardiaque 37% chirurgie diges5ve
Effect of Early vs Delayed Initiation of Renal ReplacementTherapy onMortality in Critically Ill PatientsWith Acute Kidney InjuryThe ELAIN Randomized Clinical TrialAlexander Zarbock, MD; John A. Kellum, MD; Christoph Schmidt, MD; Hugo Van Aken, MD; Carola Wempe, PhD;
Original Investigation | CARING FORTHE CRITICALLY ILL PATIENT
JAMA. doi:10.1001/jama.2016.5828Published online May 22, 2016.
100
80
60
40
20
00 10 20 30 40 50 60 70 80 90
Ove
rall
Mor
talit
y Pr
obab
ility
, %
Days Since Randomization
Early RRT
Delayed RRT
Inverse normal log-rank test, P = .03; HR = 0.66 (95% CI, 0.45-0.97)
Hospital stay, median (Q1, Q3), dn 51(31, 74)
82(67, >90)
<.001 −37(−� to −19.5)
D ti f h i l til ti 125 5 181 0 002 60 0
Early(n = 112)
Delayed(n = 119)
PValue
AbsoluteDifference, %(95% CI)
Durée CVVH 25j
9j 3 pts !
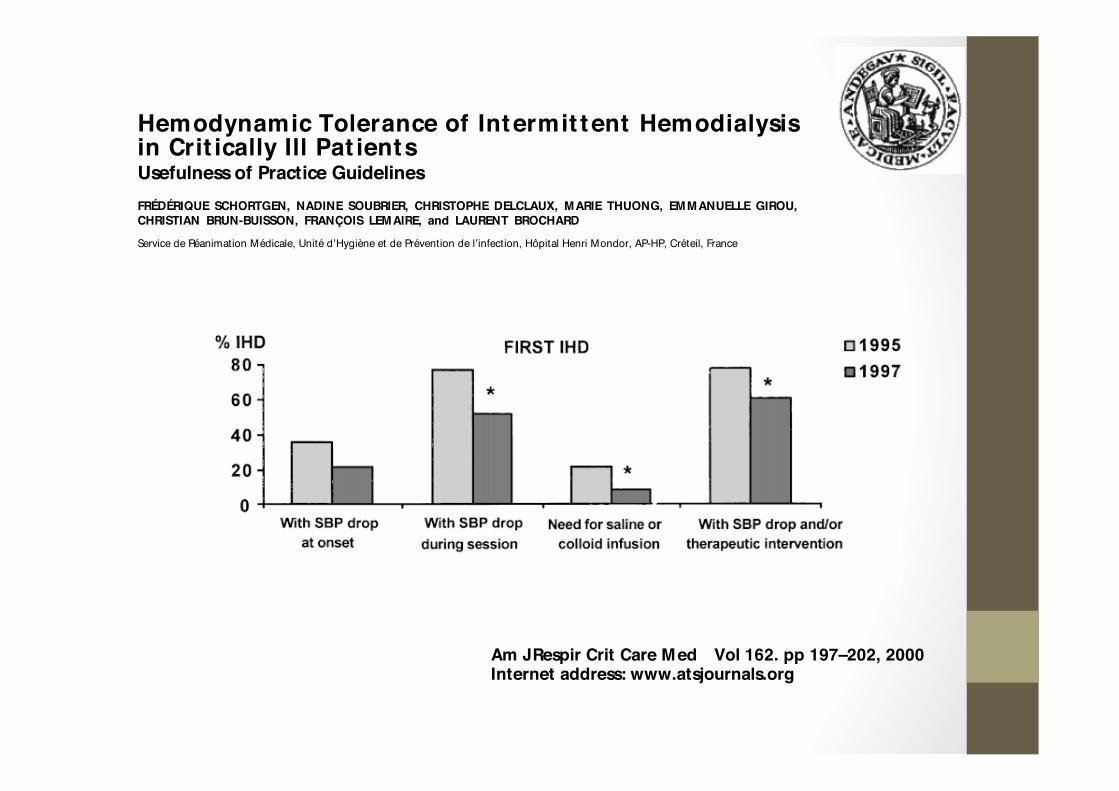
Hemodynamic Tolerance of Intermit tent Hemodialysis in Crit ically Ill Pat ients
Usefulness of Practice Guidelines
FRÉDÉRIQUE SCHORTGEN, NADINE SOUBRIER, CHRISTOPHE DELCLAUX, MARIE THUONG, EMMANUELLE GIROU,CHRISTIAN BRUN-BUISSON, FRANÇOIS LEMAIRE, and LAURENT BROCHARD
Service de Réanimation Médicale, Unité d’Hygiène et de Prévention de l’infection, Hôpital Henri Mondor, AP-HP, Créteil, France
Am J Respir Crit Care Med Vol 162. pp 197–202, 2000Internet address: www.atsjournals.org
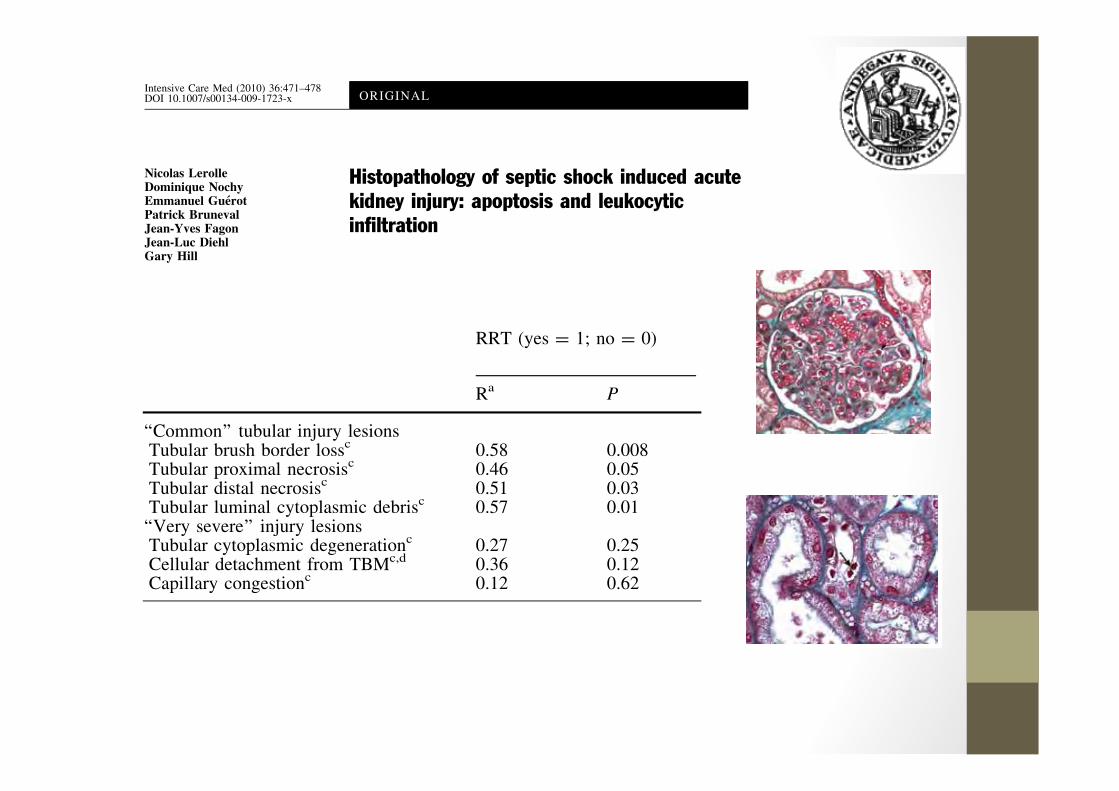
Nicolas LerolleDominique NochyEmmanuel GuerotPatrick BrunevalJean-Yves FagonJean-Luc DiehlGary Hill
Histopathology of septic shock induced acutekidney injury: apoptosis and leukocyticinfiltration
Intensive Care Med (2010) 36:471–478DOI 10.1007/s00134-009-1723-x ORIGINAL
RRT (yes = 1; no = 0)
Ra P
‘‘Common’’ tubular injury lesionsTubular brush border lossc 0.58 0.008Tubular proximal necrosisc 0.46 0.05Tubular distal necrosisc 0.51 0.03Tubular luminal cytoplasmic debrisc 0.57 0.01‘‘Very severe’’ injury lesionsTubular cytoplasmic degenerationc 0.27 0.25Cellular detachment from TBMc,d 0.36 0.12Capillary congestionc 0.12 0.62
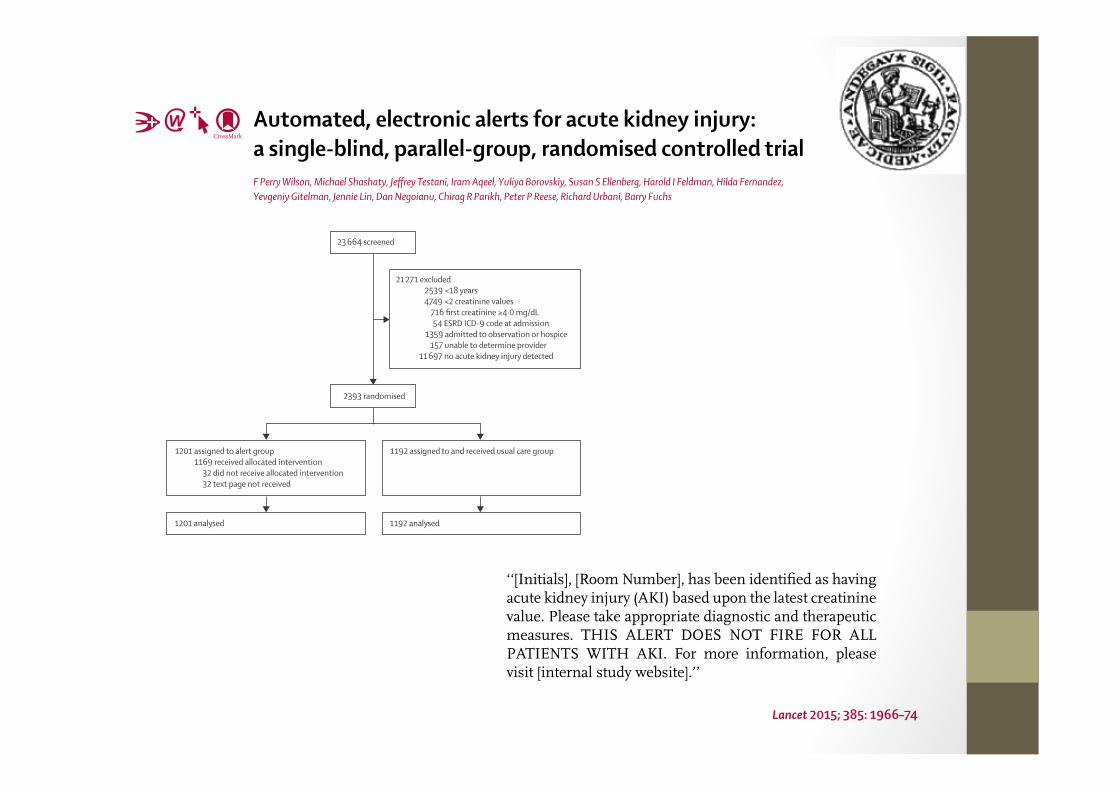
Automated, electronic alerts for acute kidney injury: a single-blind, parallel-group, randomised controlled trialF Perry Wilson, Michael Shashaty, Jeff rey Testani, Iram Aqeel, Yuliya Borovskiy, Susan S Ellenberg, Harold I Feldman, Hilda Fernandez, Yevgeniy Gitelman, Jennie Lin, Dan Negoianu, Chirag R Parikh, Peter P Reese, Richard Urbani, Barry Fuchs
Lancet 2015; 385: 1966–74
1201 assigned to alert group1169 received allocated intervention
32 did not receive allocated intervention 32 text page not received
23 664 screened
21 271 excluded2539 <18 years 4749 <2 creatinine values
716 first creatinine ≥4·0 mg/dL 54 ESRD ICD-9 code at admission
1359 admitted to observation or hospice 157 unable to determine provider
11 697 no acute kidney injury detected
2393 randomised
1192 assigned to and received usual care group
1201 analysed 1192 analysed
‘‘[Initials], [Room Number], has been identifi ed as having acute kidney injury (AKI) based upon the latest creatinine value. Please take appropriate diagnostic and therapeutic measures. THIS ALERT DOES NOT FIRE FOR ALL PATIENTS WITH AKI. For more information, please visit [internal study website].’’
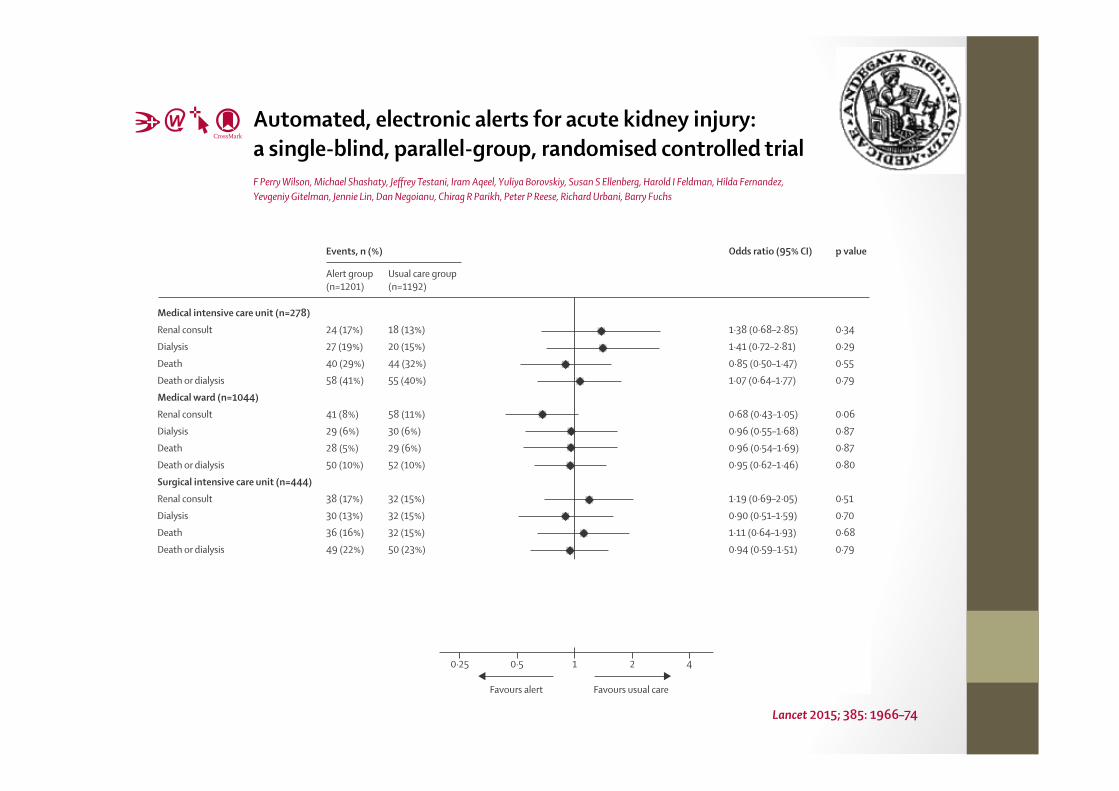
Automated, electronic alerts for acute kidney injury: a single-blind, parallel-group, randomised controlled trialF Perry Wilson, Michael Shashaty, Jeff rey Testani, Iram Aqeel, Yuliya Borovskiy, Susan S Ellenberg, Harold I Feldman, Hilda Fernandez, Yevgeniy Gitelman, Jennie Lin, Dan Negoianu, Chirag R Parikh, Peter P Reese, Richard Urbani, Barry Fuchs
Lancet 2015; 385: 1966–74
Medical intensive care unit (n=278)
Renal consult
Dialysis
Death
Death or dialysis
Medical ward (n=1044)
Renal consult
Dialysis
Death
Death or dialysis
Surgical intensive care unit (n=444)
Renal consult
Dialysis
Death
Death or dialysis
Surgical ward (n=627)
Renal consult
Dialysis
Death
Death or dialysis
1·38 (0·68–2·85)
1·41 (0·72–2·81)
0·85 (0·50–1·47)
1·07 (0·64–1·77)
0·68 (0·43–1·05)
0·96 (0·55–1·68)
0·96 (0·54–1·69)
0·95 (0·62–1·46)
1·19 (0·69–2·05)
0·90 (0·51–1·59)
1·11 (0·64–1·93)
0·94 (0·59–1·51)
2·29 (1·22–4·44)
2·49 (1·02–6·67)
2·07 (0·77–6·13)
2·51 (1·17–5·73)
Events, n (%) Odds ratio (95% CI)
0·34
0·29
0·55
0·79
0·06
0·87
0·87
0·80
0·51
0·70
0·68
0·79
0·01
0·03
0·12
0·01
p value
Alert group (n=1201)
Usual care group (n=1192)
Favours alert Favours usual care
0·25 0·5
24 (17%)
27 (19%)
40 (29%)
58 (41%)
41 (8%)
29 (6%)
28 (5%)
50 (10%)
38 (17%)
30 (13%)
36 (16%)
49 (22%)
36 (12%)
19 (6%)
14 (5%)
26 (8%)
18 (13%)
20 (15%)
44 (32%)
55 (40%)
58 (11%)
30 (6%)
29 (6%)
52 (10%)
32 (15%)
32 (15%)
32 (15%)
50 (23%)
17 (5%)
8 (3%)
7 (2%)
11 (4%)
21 4
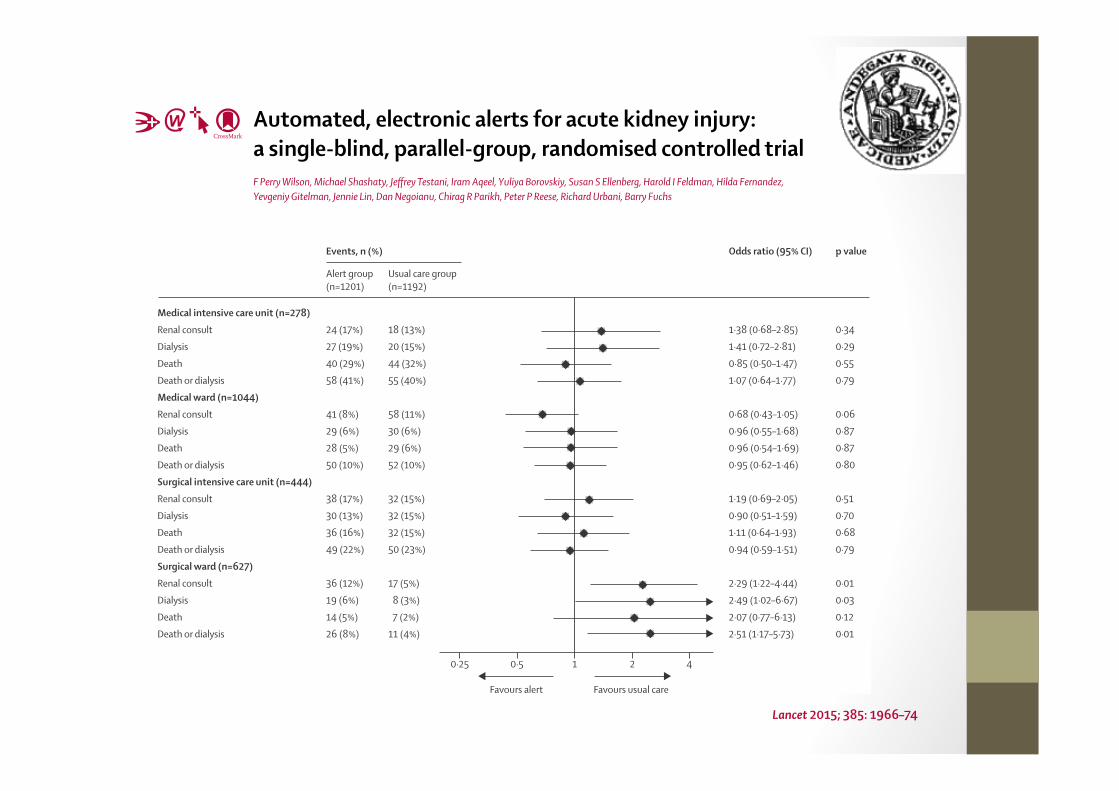
Automated, electronic alerts for acute kidney injury: a single-blind, parallel-group, randomised controlled trialF Perry Wilson, Michael Shashaty, Jeff rey Testani, Iram Aqeel, Yuliya Borovskiy, Susan S Ellenberg, Harold I Feldman, Hilda Fernandez, Yevgeniy Gitelman, Jennie Lin, Dan Negoianu, Chirag R Parikh, Peter P Reese, Richard Urbani, Barry Fuchs
Lancet 2015; 385: 1966–74
Medical intensive care unit (n=278)
Renal consult
Dialysis
Death
Death or dialysis
Medical ward (n=1044)
Renal consult
Dialysis
Death
Death or dialysis
Surgical intensive care unit (n=444)
Renal consult
Dialysis
Death
Death or dialysis
Surgical ward (n=627)
Renal consult
Dialysis
Death
Death or dialysis
1·38 (0·68–2·85)
1·41 (0·72–2·81)
0·85 (0·50–1·47)
1·07 (0·64–1·77)
0·68 (0·43–1·05)
0·96 (0·55–1·68)
0·96 (0·54–1·69)
0·95 (0·62–1·46)
1·19 (0·69–2·05)
0·90 (0·51–1·59)
1·11 (0·64–1·93)
0·94 (0·59–1·51)
2·29 (1·22–4·44)
2·49 (1·02–6·67)
2·07 (0·77–6·13)
2·51 (1·17–5·73)
Events, n (%) Odds ratio (95% CI)
0·34
0·29
0·55
0·79
0·06
0·87
0·87
0·80
0·51
0·70
0·68
0·79
0·01
0·03
0·12
0·01
p value
Alert group (n=1201)
Usual care group (n=1192)
Favours alert Favours usual care
0·25 0·5
24 (17%)
27 (19%)
40 (29%)
58 (41%)
41 (8%)
29 (6%)
28 (5%)
50 (10%)
38 (17%)
30 (13%)
36 (16%)
49 (22%)
36 (12%)
19 (6%)
14 (5%)
26 (8%)
18 (13%)
20 (15%)
44 (32%)
55 (40%)
58 (11%)
30 (6%)
29 (6%)
52 (10%)
32 (15%)
32 (15%)
32 (15%)
50 (23%)
17 (5%)
8 (3%)
7 (2%)
11 (4%)
21 4
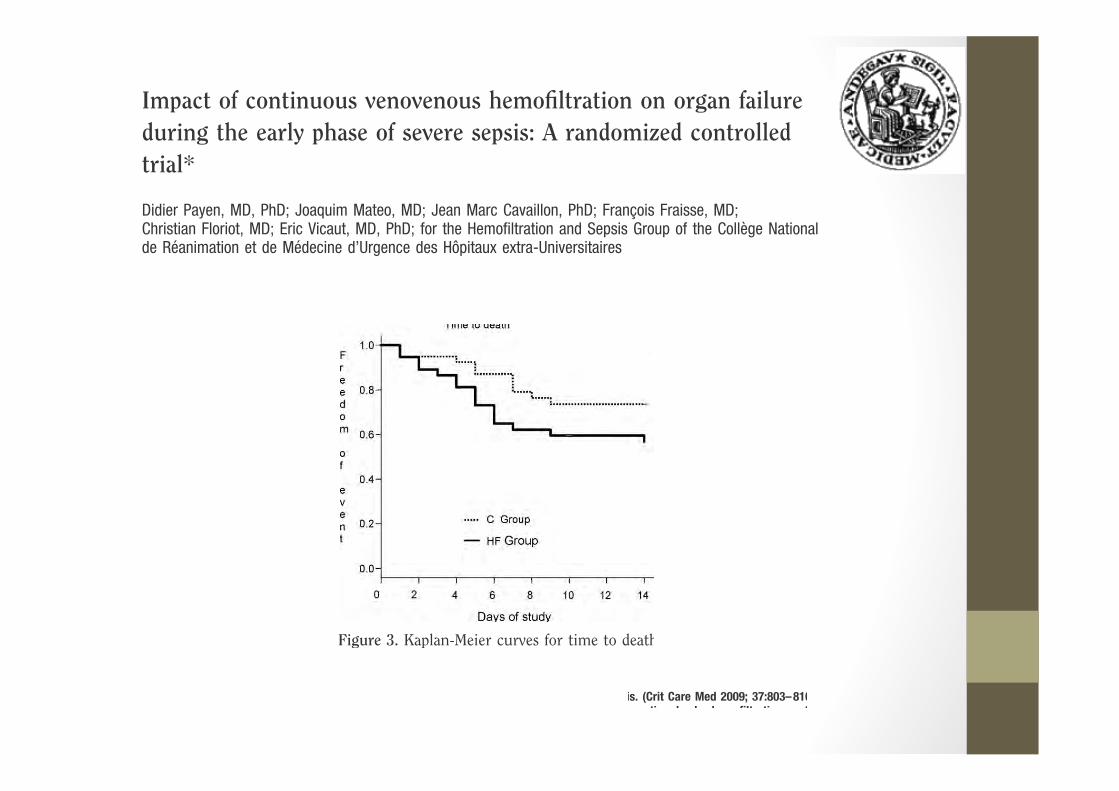
Impact of continuous venovenous hemofiltration on organ failureduring the early phase of severe sepsis: A randomized controlledtrial*
Didier Payen, MD, PhD; Joaquim Mateo, MD; Jean Marc Cavaillon, PhD; Francois Fraisse, MD;Christian Floriot, MD; Eric Vicaut, MD, PhD; for the Hemofiltration and Sepsis Group of the College Nationalde Reanimation et de Medecine d’Urgence des Hopitaux extra-Universitaires
Figure 3. Kaplan-Meier curves for time to death
is. (Crit Care Med 2009; 37:803–810septic shock; hemofiltration; cyt
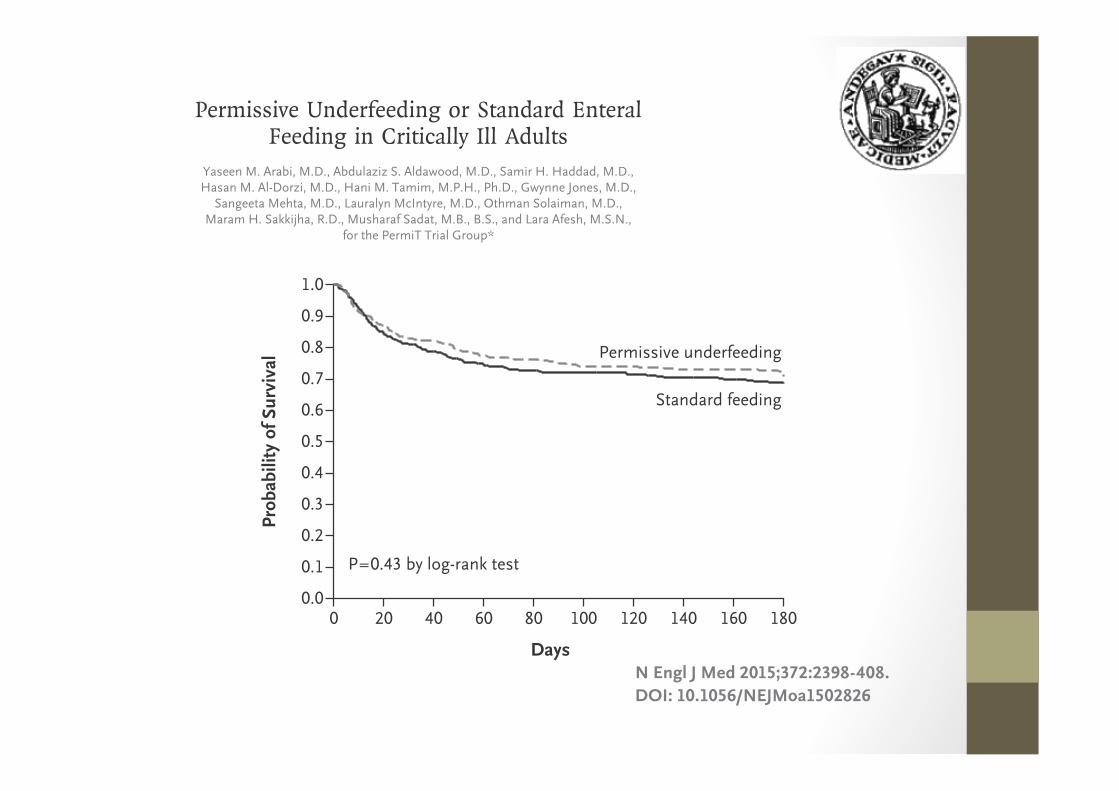
Permissive Underfeeding or Standard Enteral Feeding in Critically Ill Adults
Yaseen M. Arabi, M.D., Abdulaziz S. Aldawood, M.D., Samir H. Haddad, M.D., Hasan M. Al-Dorzi, M.D., Hani M. Tamim, M.P.H., Ph.D., Gwynne Jones, M.D.,
Sangeeta Mehta, M.D., Lauralyn McIntyre, M.D., Othman Solaiman, M.D., Maram H. Sakkijha, R.D., Musharaf Sadat, M.B., B.S., and Lara Afesh, M.S.N.,
for the PermiT Trial Group*
Prob
abili
ty o
f Sur
viva
l1.0
0.8
0.9
0.7
0.6
0.4
0.3
0.1
0.5
0.2
0.00 20 60 1008040 120 140 160 180
Days
P=0.43 by log-rank test
Permissive underfeeding
Standard feeding
N Engl J Med 2015;372:2398-408.DOI: 10.1056/NEJMoa1502826
• Pas de rela5on dose / effet
• Tôt ou tard peu importe
• Pourrait augmenter la mortalité/morbidité chez certains pa5ents
• Pas de rela5on dose / effet
• Tôt ou tard peu importe
• Pourrait augmenter la mortalité/morbidité chez certains pa5ents
Que traite-‐t-‐on avec l’épura5on extra-‐rénale aiguë?
Que traite-‐t-‐on avec l’épura5on extra-‐rénale aiguë?
K pH
Surcharge Urée > 35 mM
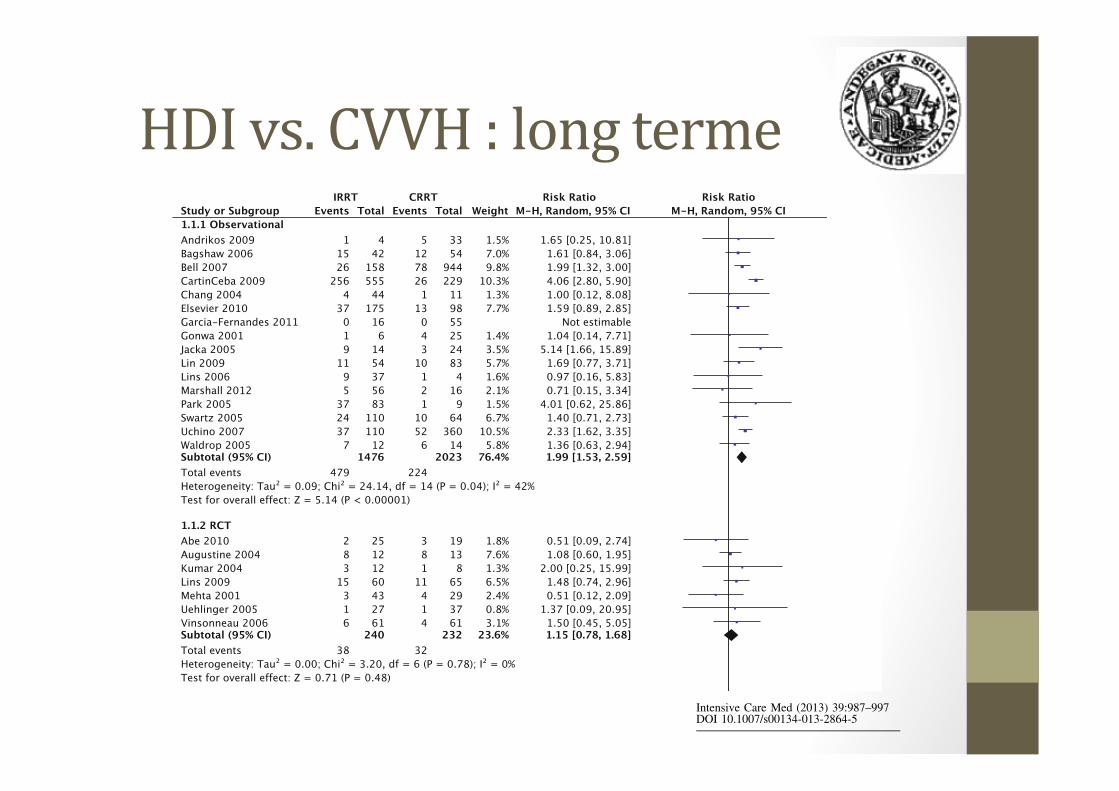
Intensive Care Med (2013) 39:987–997DOI 10.1007/s00134-013-2864-5
HDI vs. CVVH : long terme