Embed Size (px)
Citation preview

CRIC
Coronary Angioplasty and Healthy Innovation
Systems
J.S. Metcalfe, Ramlogan, R., Mina, A., and Tampubolon, G.
PREPARED FOR THE IHT at the HTAi CONFERENCEROME, ITALY - JUNE 20-21, 2005.
QUESTIONS
High level policy debates in health driven by the ageing population and the paradox of health care innovations: innovation is cost reducing per intervention but not so in the aggregate.
• How does innovation take place and how does it diffuse? And how do innovation systems emerge?
• What is the role of public and private institutions? Who are the key intermediators?
• Are there unanticipated consequences?
• What kind of general policy instruments facilitate innovation system building?
Methodology• Large-scale and multi-technique analysis of one problem area (probe) • Secondary literature reviews, clinical reports and policy documents.• Descriptive statistics of global scientific research, inventive activities and clinical practice• Empirical Network Analysis of citations, co-authorships, geographical origin and institutional affiliation of authors/inventors.• Data: ISI and USPTO Citation Networks
Papers 11240 94442
Patents 5136 22095
+ FDA Interventional Cardiology products dataset.
• Clustering algorithms embedded in Pajek to structure and visualise large networks
• Expert Interviews in UK and US.
• The Medical Problem: Coronary Artery Disease
- causes severe disability and more death than any other disease, including cancer, in affluent societies.
- medical conditions associated with it are angina, ischemia, unstable angina, myocardial infarction, arrhythmias, heart failure and sudden death.
Treatment Options:
- Before1960s: nitrogylcerine, rest and hope
- Late 1960s: coronary artery by-pass surgery
- Late 1970s: percutaneous transluminal coronary angioplasty (PTCA); one of the most significant medical advances in medical practise over the last thirty years
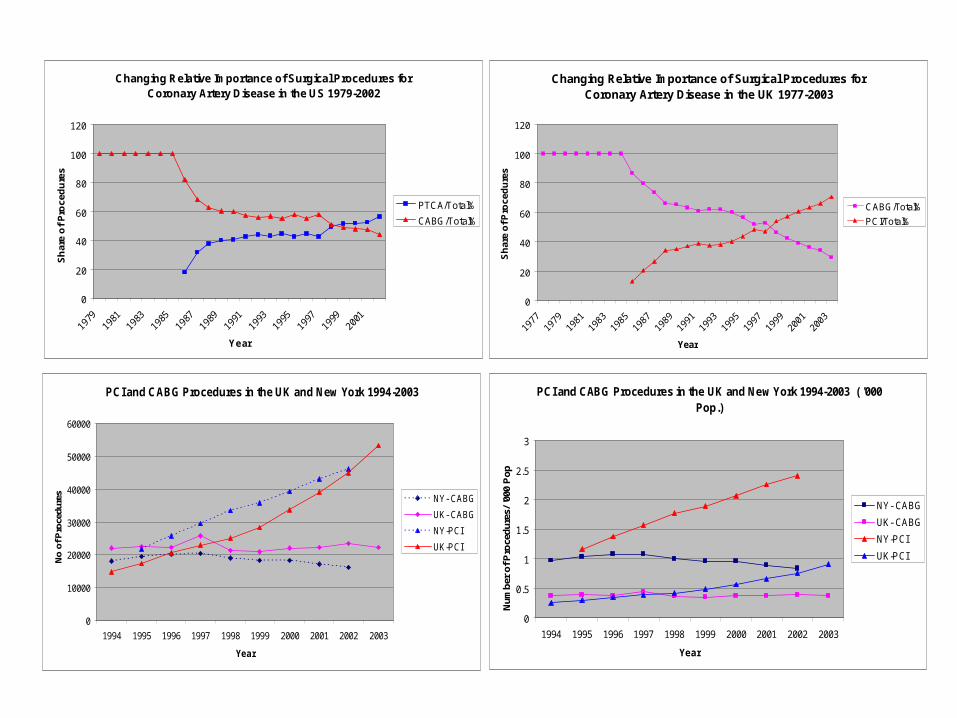
Changing Relative Importance of Surgical Procedures for Coronary Artery Disease in the US 1979-2002
0
20
40
60
80
100
120
Year
Sh
are
of
Pro
ced
ure
s
PTCA/Total%
CABG/Total%
Changing Relative Importance of Surgical Procedures for Coronary Artery Disease in the UK 1977-2003
0
20
40
60
80
100
120
Year
Sh
are
of P
roce
du
res
CABG/Total%
PCI/Total%
PCI and CABG Procedures in the UK and New York 1994-2003
0
10000
20000
30000
40000
50000
60000
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
No
of P
roce
dure
s NY- CABG
UK- CABG
NY-PCI
UK-PCI
PCI and CABG Procedures in the UK and New York 1994-2003 ( '000 Pop.)
0
0.5
1
1.5
2
2.5
3
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Year
Num
ber
of P
roce
dur
es/ '
000
Pop
NY- CABG
UK- CABG
NY-PCI
UK-PCI
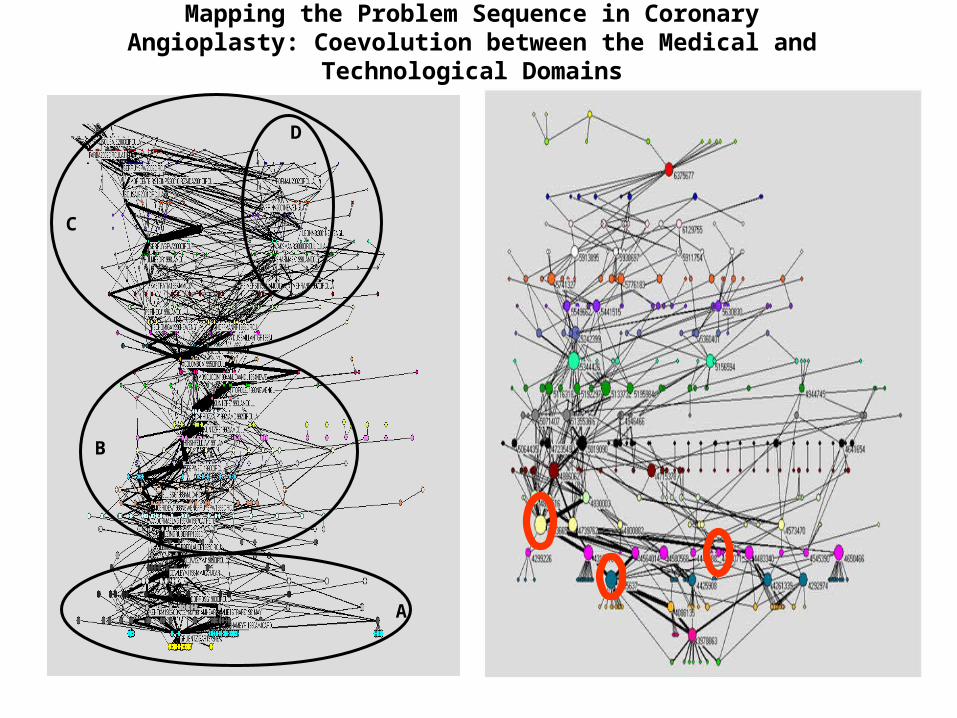
A
C
D
B
Mapping the Problem Sequence in Coronary Angioplasty: Coevolution between the Medical and Technological Domains
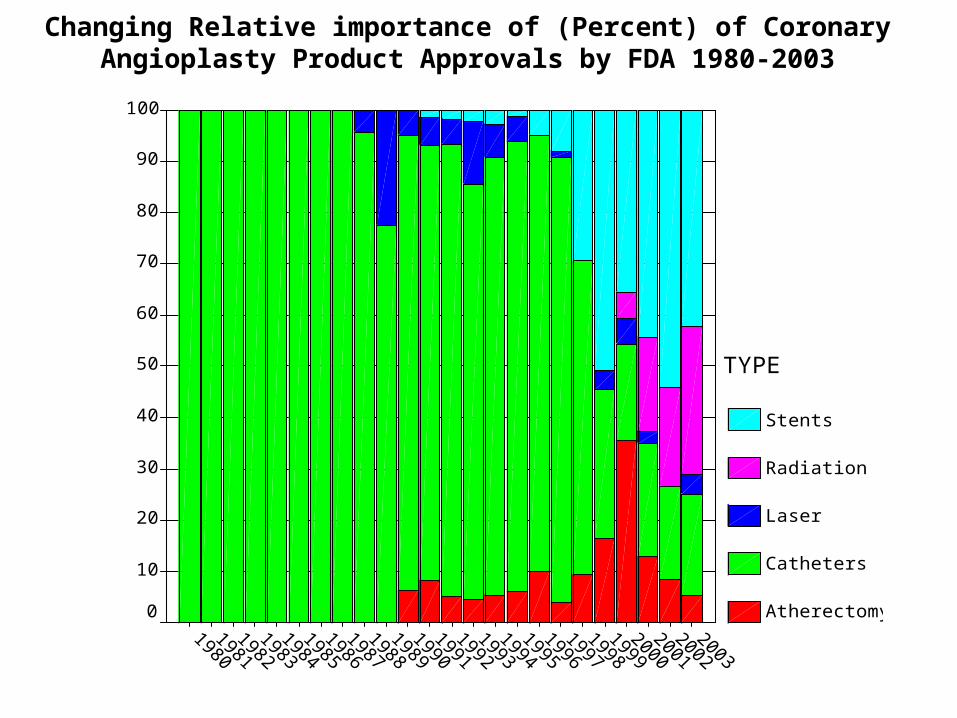
100
90
80
70
60
50
40
30
20
10
0
TYPE
Stents
Radiation
Laser
Catheters
Atherectomy
Changing Relative importance of (Percent) of Coronary Angioplasty Product Approvals by FDA 1980-2003
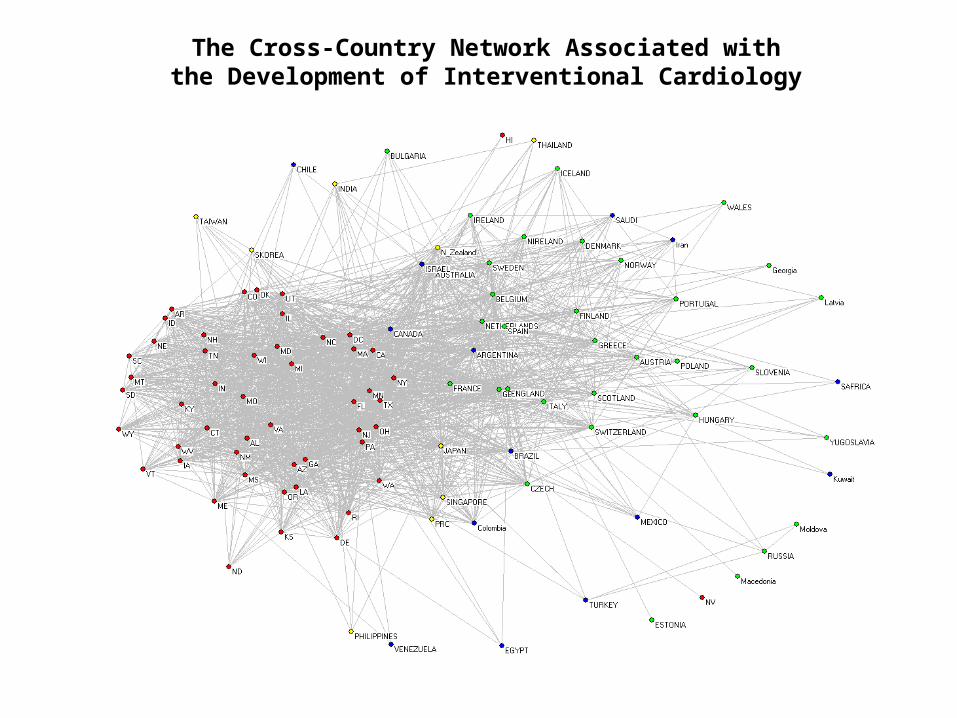
The Cross-Country Network Associated with the Development of Interventional Cardiology
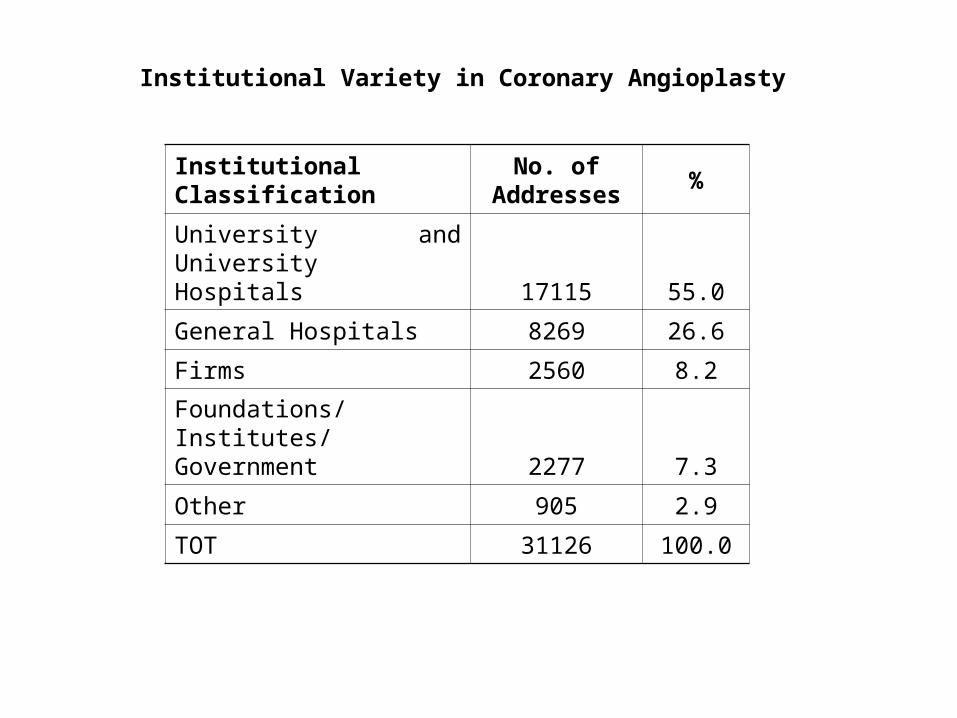
Institutional ClassificationNo. of
Addresses%
University and University Hospitals 17115 55.0
General Hospitals 8269 26.6
Firms 2560 8.2
Foundations/Institutes/Government 2277 7.3
Other 905 2.9
TOT 31126 100.0
Institutional Variety in Coronary Angioplasty
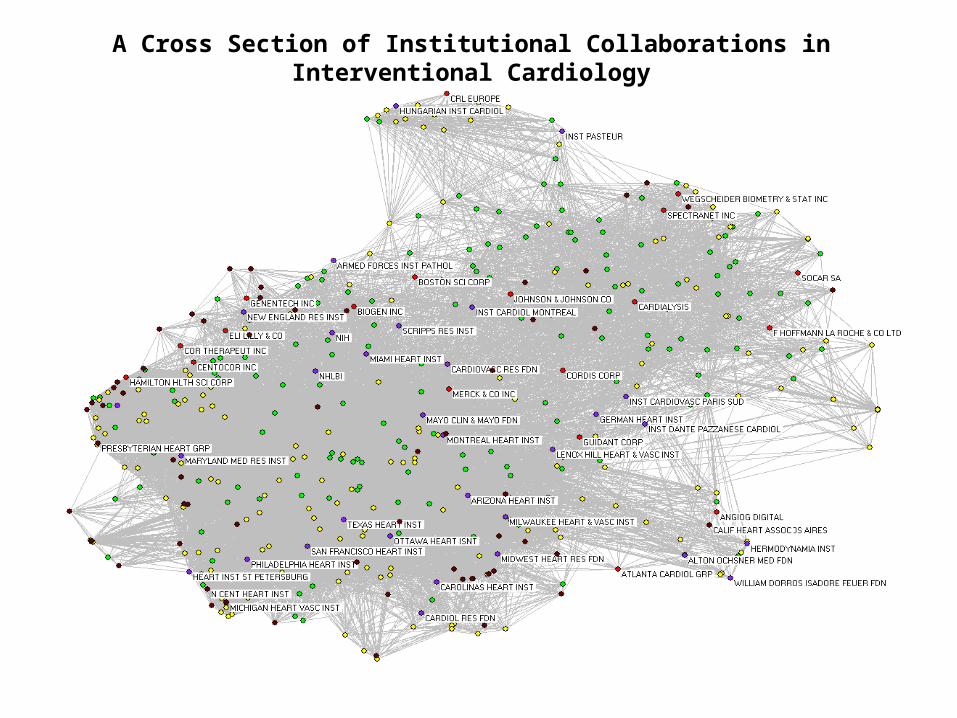
A Cross Section of Institutional Collaborations in Interventional Cardiology
Understanding Innovation in Medicine:
• A science push or bench to bedside model of medical innovation is unsatisfactory.
• The development of medical know-how is characterised by 1) Systematic Feedback between knowledge and practice2) Dynamic interaction between Epistemic, Organisational, Institutional and Cultural Factors.
• Innovation processes are systemic, involving multiple actors in specifically instituted contexts – need to know how boundaries change and the nature of the connections.
• Innovation systems emerge for a purpose, namely to solve problems. The idea of problem sequences is the central concept around which we can build an understanding of how innovation processes are instituted
• Innovations are rarely if ever uniquely circumscribed events and outcomes. They are better seen as trajectories of improvement sequences in which devices or procedures are progressively refined and extended in their scope of application.
• In PTCA we see a mix of market and non-market modes of inventing and innovation spread across public and private spheres of action, that have evolved according to specific dynamic processes.
• Should policy instruments be geared to those that facilitate collaborative research, incubate University/ Research Hospital ideas and in general to create connections that will not otherwise arise spontaneously?
Problem: You cannot predict which innovation systems will form or who the actors will be; this implies an obvious corollary, that the connection between instruments and their effects will be ‘loose’ with outcomes that may be unanticipated.
• Policy Coordination: When innovation systems transcend national boundaries they are influenced by the different policy jurisdictions. Competition between nation states to have key elements of innovation systems within their national ecologies raises the possibility that policy conflict could stymie innovation system formation. This moves innovation policy coordination higher up the policy agenda.