Embed Size (px)
Citation preview

COMPARATIVE LITERATURE SURVEY OF HEALTH TECHNOLOGY ASSESSMENT IN
BRAZIL, CHINA AND INDIAPOTENTIAL TRANSFERABLE LESSONS FROM BRAZIL
TO EMERGING COUNTRIES
Stuwe LT1, Bellanger MM2, Picon PD3, Chen Y45, Wie Y5, Chi X5, Mathew J6
1Pierre-and-Marie-Curie University, Paris, France, 2EHESP French School of Public Health, Rennes, France, 3Federal University of Rio Grande do Sul,
Porto Alegre - RS, Brazil, 4Key Lab of Health Technology Assessment (Ministry of Health), China 5Fudan University, China, 6Advanced Pediatrics
Centre Post Graduate Institute of Medical Education and Research (PGIMER) Chandigarh, India
Contact e-mail:

Structure
1. Background
2. Study objective
3. Methods
4. Results
5. Discussion
6. Conclusion

Background• Health ministers of BRICS States, a political alliance comprising Brazil,
China, India, Russia and South Africa, have started to strengthencollaboration in their shared objective to implement Universal HealthCoverage (UHC) (Rao et al. 2014)
• HTA is considered an important tool for priority-setting and guiding reimbursement decisions (Busse et al. 2002)
• The key role of HTA has been underlined in the progressive attainment of UHC, since it enables the efficient and equitable allocation of healthcare and other resources (Chalkidou et al., 2013).
• Emerging countries often face similar challenges in introducing Health Technology Assessment (HTA) frameworks
• Such a reality highlights the potential to share insights and strategies
• Network of researchers available in Brazil, China and India which allowedto use these countries for a comparative assessment

Study objectives
Primary objective:
– To compare Brazil, China and India according to their level of HTA influence in decision-making regarding public medicines list management.
Secondary objectives:
– To provide an overview of the influence of HTA in decision-making related to public medicines lists in Brazil, China and India.
– To identify transferable lessons learned from one country to another in terms of HTA processes and implementation.
.

Methodology
1) Published literature survey• A systematic literature search for published articles for the time-period
2005 - early 2015
– In English in international databases: PubMed (MEDLINE), ScienceDirect, and EBSCO-host databases (Academic Search Premier, CINAHL Plus with Full Text)
– In local languages (Portuguese, Chinese and English) in national databases
• Search equation : (<country> AND [“health technology assessment”])
AND ([medicine] OR [pharmaceutical] OR [drug] OR [vaccine] OR [“health technology”])
• Results entered into PRISMA flow diagram
Methodology
2) Grey literature survey
• Scope (Schöpfel 2010): “manifold document types produced on all levels of government, academics, business and industry in print and electronic formats that are protected by intellectual property rights, of sufficient quality to be collected and preserved by library holdings or institutional repositories, but not controlled by commercial publishers”
• Grey literature search in local languages (Portuguese, Chinese and English), according to selected grey literature categories (cf. next slide)

Methodology : Grey literature sources
Grey literature category Subcategory
Central Government and agencies : Ministry of Health, HTA agency/ commission, National Medicines Agency
HTA and medicines evaluation policy / HTA regulations, ordinances, decrees / HTA reports for medicines / Medicines incorporation decisions / HTA policy documents and reports / HTA doctrine / HTA methodology / Clinical guidelines /National medicines list / Bilateral or multilateral HTA statements/ MoU / Statements during interviews, public hearings
State or municipal government : Local secretaries of health
Regulations, ordinances / HTA reports / Medicines incorporation decisions / HTA methodology / Clinical guidelines / State or municipal medicines lists / Statements during interviews
Academia and university hospitals
HTA abstracts for congresses / Written expertise / HTA studies /Methodology / Existence of HTA degree or specialization programmes / Academic workshops / Statements during interviews, public hearings / HTA hospital networks / Specialized academic HTA centers
Doctors, healthcare professionals
Written expertise / HTA studies / Implementation of HTA / Statements during interviews / public hearings / Participation rates in continued education or specialization courses
ParliamentHTA legislation / Parliamentary debates on HTA / Statements during interviews / Public hearings
Judiciary Judicial decisions / Right to health litigation / Public hearings
Private sector (consulting and pharmaceutical industry)
HTA incorporation requests / Statements / News articles / HTA abstracts for congresses / HTA powerpoint presentations for congresses
Civil society and patient associations HTA incorporation requests / HTA-related Statements
International organizations
Communiqués related to participation in international HTA networks / International or regional recommendations for HTABilateral cooperation / International organizations (WHO, World Bank, EU, etc.)

Methodology• Policy objectives of the HTA system, its legal status, and its relationships with the remainder
of the health system, with other public sector bodies and stakeholders• The existence of an HTA commission (yes/no)
• Specific methodology used/ doctrine published by HTA commission (yes/no(NA)
• Policies, laws and regulation regarding HTA for medicines evaluation and list incorporation (yes/no)
• Policies, laws and regulation regarding clinical guidelines and implementation (yes/no)
• Existence of HTA networks (yes/no)
• Membership in international HTA networks (INATHA) (yes/no)
• Participation in international HTA congresses (ISPOR, HTAi) (yes/no
• International (bilateral, multilateral, academic) collaborations in the area of HTA (yes/no)
• Publications in HTA (yes/no/specify)
1) HTA Policy implementation
level (adapted from Hutton et al.)
• HTA Stakeholder mapping• Government (Ministry of Health and HTA commission/ agency)
• Academia and university hospitals
• Doctors, hospitals, healthcare professionals
• Parliament
• Judiciary
• Private sector (consulting and pharmaceutical industry)
• Civil society and patient associations
• International organizations (e.g. Mercosur, PAHO/WHO)
2) Identification and weight of
different stakeholders in
HTA process (adapted from
Varvasovszky et al.)
• Influence of HTA on policy and administrative decisions : effective dissemination of HTA reports and recommendations, translation of recommendations into decisions, quality of HTA reports, accessibility of HTA reports, timeliness
• Influence of HTA on administrative action
• Influence of HTA on delivery of health care and on the health status of patients: access to medicines policy linked to HTA, changes to health care and/or health outcomes
3) Assessment of influence of
HTA on decision-making
(INAHTA)

PRISMA flow diagram for published literature
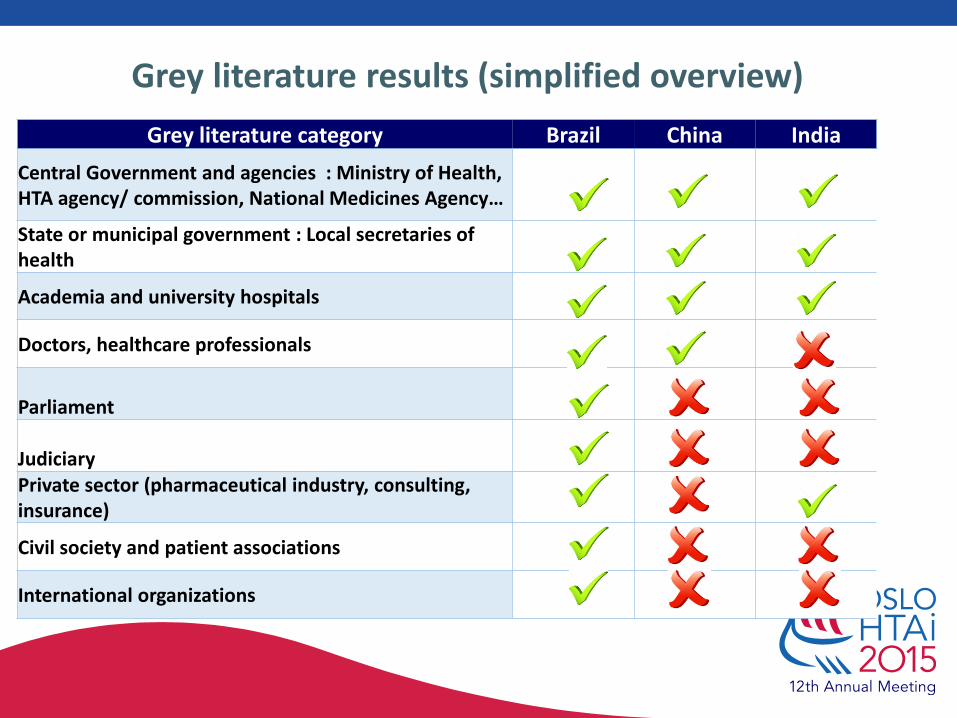
Grey literature results (simplified overview)
Grey literature category Brazil China India
Central Government and agencies : Ministry of Health, HTA agency/ commission, National Medicines Agency…
State or municipal government : Local secretaries of health
Academia and university hospitals
Doctors, healthcare professionals
Parliament
JudiciaryPrivate sector (pharmaceutical industry, consulting, insurance)
Civil society and patient associations
International organizations

HTA Policy implementation level (adapted from Hutton et al.)
Involvement in HTA activities (yes = 1, no = 0) Brazil China India
The existence of an HTA commission 1 0 0
Specific methodology used/ doctrine published by HTA commission 0 0 0
Policies, laws and regulation regarding HTA for medicines evaluation and list incorporation 1 0 0
Policies, laws and regulation regarding clinical guidelines and implementation 1 0 0
Existence of HTA networks 1 1 1
Membership in international HTA networks (INATHA) 1 1 0
Participation in international HTA congresses (ISPOR, HTAi) 1 1 0
International (bilateral, multilateral, academic) collaborations in the area of HTA 1 0 0
Publications in HTA 1 1 0
Sum of points / 9 8 4 1
Policy objectives of the HTA system, its legal status, and its relationships with the remainder of the health system, with other public sector bodies and stakeholders

Identification and weight of different stakeholders in HTA process (adapted from Varvasovszky et al.)
Stakeholder involved in HTA (yes = 1, no = 0) Brazil China India
Government (Ministry of Health and HTA commission/ agency) 1 0 0
Academia and university hospitals 1 1 1
Healthcare professionals1 1 1
Judiciary1 0 0
Parliament 1 0 0
Private sector (consulting and pharmaceutical industry) 1 1 1
Civil society and patient associations 1 0 0
International organizations (e.g. Mercosur, PAHO/WHO)1 0 0
Sum of points / 8 8 3 3

Assessment of influence of HTA on decision-making (INAHTA)
Influence of HTA (yes = 1, no = 0) Brazil China India
Influence of HTA on policy and administrative decisions
Effective dissemination of HTA reports and recommendations 1 0 0
Translation of recommendations into decisions 1 0 0
Quality of HTA reports 1 0 0
Accessibility of HTA reports 1 0 0
Timeliness 1 0 0
Influence of HTA on administrative action
Influence of HTA on delivery of health care and on the health status of patients
Access to medicines policy linked to HTA 1 0 0
Changes to health care and/or health outcomes
0 0 0
Sum of points / 8 6 0 0

0 1 2 3 4 5 6 7 8 9
Assessment of influence of HTA ondecision-making (INAHTA)
Identification and weight of differentstakeholders in HTA process (adapted
from Varvasovszky et al.)
HTA Policy implementation level (adaptedfrom Hutton et al.)
Comparison of countries according to HTA implementation measurements
India China Brazil

Discussion : Added value
• No comparative study on HTA status between Brazil, China and India so far conducted
• Same methodology applied to all three countries, involvement of local researchers and languages
• Main finding is that Brazil has established a centralized framework for HTA, whereas it is absent in the other countries
• Advanced situation of Brazil, but progressive steps taken in China and India

Discussion: Transferable HTA in Brazil to China and India
• The institutionalization of HTA by means of a national commission that orients MoH health priority-setting and decision-making regarding public medicines lists management
• More transparent processes represented by consistent online publication of reports
• The effective use of public consultations
• Regional involvement of Brazil within Mercosur, RedETSA, etc…

Discussion : Limitations
• Limitations of the study
Interpretation bias using Brazil as a starting point
Time frame too short for an external assessment
Focus only on medicines and exclusion of medical devices and procedures
Difficulty in assessing grey literature, insufficient results for India may question the results
Comparability of the three countries is questionable
• Transferability of lessons learned
China, HTA might be used in future listing, pricing, and reimbursement of drugs (16), which opens up the possibility to transfer the centralized Brazilian HTA model to China.
• Remaining challenges in Brazil not sufficiently underlined
Lack of transparency in the decision-making process
No cost-effectiveness threshold in the HTA process
Insufficient involvement of the public and of patients in the HTA process
Implementation of HTA via clinical guidelines

Conclusion
• Among the three countries, Brazil is most advanced in terms of HTA implementation
• In China, the national plan for health-care reform has put special emphasis on making appropriate, cost–effective and essential health care and technology available to all people in the country: great potential of HTA to contribute to this reform
• India takes into account HTAs done in other countries but there is no link between HTA and the regulatory process and visible steps towards the implementation of HTA.
• The Brazilian experience shows that HTA can provide information needed for evidence-based policies, and offers lessons transferable to other emerging countries.
• Further analyses should be conducted to test the transferability of these lessons learned at the State level, starting by China, the second most advanced country in terms of HTA development after Brazil.

Annex

References
• Busse R, Orvain J, Velasco M, Perleth M, Drummond M, Jørgensen T, et al. Best practice in undertaking and reporting health technology assessments. Int J Technol Assess Health Care. 2002;18(02):361–422.
• Chalkidou K, Marten R, Cutler D, Culyer T, Smith R, Teerawattananon Y, et al. Health technology assessment in universal health coverage. The Lancet. 2013 Dec;382(9910):e48–9.
• Hutton J, McGrath C, Frybourg J-M, Tremblay M, Bramley-Harker E, Henshall C. Framework for describing and classifying decision-making systems using technology assessment to determine the reimbursement of health technologies (fourth hurdle systems). Int J Technol Assess Health Care. 2006;22(01):10–8.
• INAHTA Conceptual Paper on the Influence of HTA 2014
• National Information Center on Health Services Research and Health Care Technology (NICHSR), U.S: National Library of Medicine, HTA 101: VII. RETRIEVE EVIDENCE, Accessed May 1, 2015 at: http://www.nlm.nih.gov/nichsr/hta101/ta10109.html#Heading1
• Rao KD, Petrosyan V, Araujo EC, McIntyre D. Progress towards universal health coverage in BRICS: translating economic growth into better health. Bull World Health Organ. 2014 Jun 1;92(6):429–35.
• Schöpfel J. Towards a Prague Definition of Grey Literature. GL 12. Twelfth International Conference on Grey Literature. Prague, Czech Republic. December 2010. Accessed May 29, 2015 at: http://www.textrelease.com/images/GL12_Abstract_S1N1.pdf
• Varvasovszky Z, Brugha R. A stakeholder analysis. Health Policy Plan. 2000 Sep 1;15(3):338–45.

Results : HTA in Brazil
• Brazil established a health technology unit in 2003
• Institutionalization and new framework for HTA in the Brazilian healthcare system with Law 12.401/2011 which resulted from a public hearing in 2011
• New national HTA commission operating from on January 1st 2012: ComissãoNacional de Incorporação de Tecnologias no Sistema Único de Saúde(CONITEC) = National Commission for the Incorporation of Technologies
• CONITEC’s mission : to advise the MoH in the incorporation and management of new technologies
• CONITEC produces studies comparing technologies as well as guidelines for clinical practice and lists of drugs to be reimbursed
• A link between HTA outcomes assembled and recommendations issued by the national HTA commission and MoH health priority-setting and decision-making regarding public medicines lists management
• More transparent processes represented by consistent online publication of reports and the effective use of public consultations

Results : HTA in China
• Even though HTA can be traced back to early 1990s, no national HTA governing structure and system in place
• HTA activities fragmented and inconsistent, not all regulations, reports and methodology are available
• The national plan for health-care reform has put special emphasis on making appropriate, cost–effective and essential health care and technology available to all people in the country: great potential of HTA to contribute to this reform
• Some HTA or pharmacoeconomic evaluation centres at academic institutions:
• National Key Laboratory of Health Technology in Fudan (MOH)
• China National Health Development Research Center are the two specialized academic HTA centers
• “Experiential decision making” preferred over evidence-based decision-making for doctors, healthcare professionals and policy makers
Scattered HTA framework in various authorities, lack of consistency, no national body.

Results : HTA in India
• India takes into account HTAs done in other countries
• Actors: division of Healthcare Technology in the National Health Systems Resource Centre (NHSRC), a technical support institution under the Ministry of Health and Family Welfare and Healthcare Technology Innovation Centre
• Training of professionals in health technology assessment, as part of three fellowship programmes while two more programmes are planned this year
No link between HTA and the regulatory process and visible steps towards the implementation of HTA.


















![[06 - Junho 2011]](https://img.pdfslide.us/doc/110x75/568c0f4c1a28ab955a939c03/06-junho-2011.jpg)










