Embed Size (px)
Citation preview

CPPW: A First Step in Transforming Public Health in the United States
Jeffrey Levi, PhD
Executive Director
June 2, 2010
Overview
CPPW is the largest single non-emergency commitment to public health the federal government has ever made How did we get here: Why community prevention? Why
now? What is Congress expecting of you? What’s the evidence base – why do policy makers believe
you can meet their expectations? How does CPPW relate to some of the prevention and
public health investments in health reform? How should we measure success of CPPW two years
from now?

Why now? Public health has traditionally focused on
communicable diseases with biomedical interventions – treatment or a vaccine
However, the biggest drivers of illness and death (and lower productivity and competitiveness) are chronic diseases for which there are not effective clinical preventive measures Challenge: combine community level (more efficient)
public health perspective with focus on diseases generally treated in the clinical setting but for which there aren’t effective medical preventive interventions
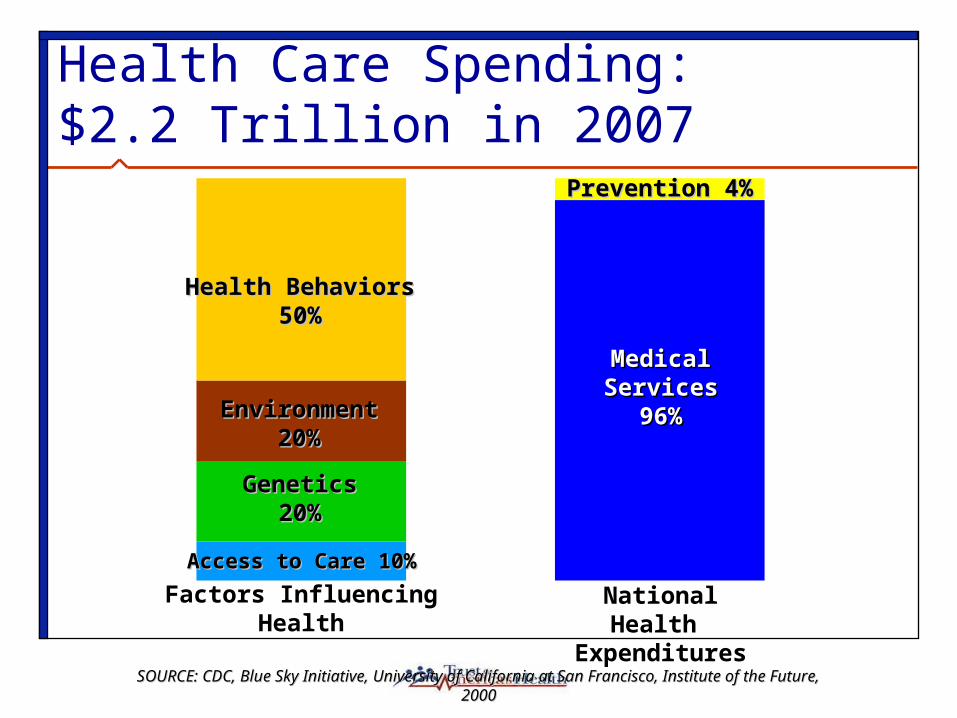
Health Care Spending: $2.2 Trillion in 2007
Health BehaviorsHealth Behaviors50%50%
EnvironmentEnvironment20%20%
Access to Care 10%Access to Care 10%
GeneticsGenetics20%20%
Prevention 4%Prevention 4%
Medical ServicesMedical Services96%96%
Factors InfluencingHealth
National Health Expenditures
SOURCE:SOURCE: CDC, Blue Sky Initiative, University of California at San Francisco, Institute of the Future, 2000CDC, Blue Sky Initiative, University of California at San Francisco, Institute of the Future, 2000
American Recovery and Reinvestment Act: Downpayment on Health Reform $650 million to “carry out evidence-based clinical
and community-based prevention and wellness strategies…that deliver specific, measurable health outcomes that address chronic disease rates.”
“a historic commitment to wellness initiatives will keep millions of Americans from setting foot in the doctor's office in the first place -- because these are preventable diseases and we're going to invest in prevention.” – President Barack Obama, Feb. 17, 2009

What is Community-Level Prevention?
Interventions that promote healthy environments and behaviors – making it easier for people to make healthy choices, such as: Changing community norms and growing community
empowerment Coalition and social network building Social marketing campaigns
Changing the physical and social environments Organization practices and governmental policies Facilities and programs These changes cut across diseases

Why community prevention? Coverage is important, but what surrounds (or precedes)
coverage is also important Achieving good health outcomes requires healthy
communities, not just healthy individuals Drivers of health care costs (chronic disease, injuries) can often
be effectively prevented in the community as opposed to managed in the health care setting Reducing costs as a critical policy outcome
Disparities in chronic diseases related to disparities in the “health” of communities Poverty, race/ethnicity and obesity Poor communities provide less support for healthy lifestyles
(food, physical activity)

What makes us think this will work?

Prevention for a Healthier America

Prevention for a Healthier America: Financial Return on Investment?
INVESTMENT: $10 per person per year
HEATH CARE COST NET SAVINGS:
$16 Billion annually
within 5 years
RETURN ON INVESTMENT
(ROI):
$5.60 for every $1
With a Strategic Investment in Proven Community-Based Prevention Programs to Increase Physical Activity and Good Nutrition and
Prevent Smoking and Other Tobacco Use

Key Findings1. Are there community-level interventions that could reduce
chronic disease levels – and thus affect the biggest driver of increased disease, disability, and cost?
Yes. Regardless of chronic condition targeted, most interventions fell into 4 categories: physical activity, nutrition, obesity, and smoking cessation.
Reduced or delayed incidence of disease; mitigation of disease
2. If we increased funding for community-level interventions, we could see a return on investment and more than break even in terms of ROI.
3. Savings can be shown by payer – with private payers and Medicare the biggest “winners.”

Or Are We Just Delaying High End-of-Life Costs? Compression of morbidity: extending healthy life
expectancy more than total life expectancy – literally compressing chronic disease and disability into a smaller proportion of life Primary prevention delays or prevents disability vs.
management of disability (current focus of health care system) Preventing obesity – delaying or avoiding a knee replacement Managing disability – providing a knee replacement Obesity results in more chronic conditions, but not shorter life

Multiplier Effect

What did the successful programs have in common? Multi-faceted approach: no magic bullet
MAPPS-type approach Adapted to individual community needs Leadership from the community Broad engagement of multiple sectors of the
community Focus on changing policies and the environment that
were sustainable and could achieve long-term change These factors help assure success, but create a challenge
since one size does not fit all

Thinking across stove-pipes Building healthier, more resilient communities able to face
multiple health challenges is the goal Funding sources should provide flexibility for the most
appropriate interventions Community interventions aren’t limited to one disease
Physical activity and youth Obesity, depression, sexual risk, educational performance, tobacco use
Alcohol taxes Alcoholism, motor vehicle accidents, domestic violence, STDs
Organizing done through CPPW will change perspectives on health of the community beyond nutrition, physical activity and tobacco.

Lessons for policy makers Making healthy choices easy choices can improve
health and reduce costs We need to create an environment and policies
where it is possible to expect individuals to exercise personal responsibility
Community prevention only works if all who affect, or are affected by, the health environment are at the table – public health cannot do this alone This is the vision that drove CPPW and prevention in
health reform

What happens next? Health reform
National Prevention Strategy Health in all policies
Community Transformation Grants Policy, environmental, programmatic and
infrastructure changes to promote healthy living and reduce disparities
Prevention and Public Health Fund (short and long term) National menu labeling requirement
Lessons from CPPW will drive the development of the Community Transformation Grants

The End is the Beginning March 2010: CPPW Awards
By September 30, 2010 – Prevention Fund = $500 m. By September 30, 2011 – Prevention Fund = $750 m.
March 2012: CPPW projects wind down By September 30, 2012 – Prevention Fund = $1 billion Community Transformation Grants underway?
2014 – Full health reform access begins October 1, 2014 – Prevention Fund reaches $2 billion

What will success look like? You will have made a measurable impact on disease and, by
extension, costs, in your communities. National and local recognition that creating healthy
communities (public health) is a shared responsibility Communities (public and private sectors) have a responsibility to
create the opportunity for individuals to make healthy choices – so the exercise of personal responsibility is a viable option
Leadership must come from more than the public health community, and include the public and private sectors
Use CPPW experience and apply to other challenges, including Community Transformation Grants





























