Embed Size (px)
Citation preview

CPAn Official Publication of the National Conference of Gerontological Nurse Practitionersand the National Gerontological Nursing Association
December 2007 Volume 1, Number 3
Sponsored by:
This activity is supported by an educational grant from Ortho-McNeil Neurologics, Inc., administeredby Ortho-McNeil Janssen Scientific Affairs, LLC.
Neurodegenerative Diseasesand Seizure Disorder
Part 3 of a 3-Part Continuing Education Series
Counseling Points™

2COUNSELING POINTS™
Faculty:
Nannette Brower, RN-C, BSN,BSW
Staff NurseATC HealthcareCherry Hill, New Jersey
Nancy D. Henry, RN, PhD-CGeriatric Nurse PractitionerGeriatric & Rehabilitative CareServices—NHCU
Greater Los Angeles VAHealthcare System
Assistant Clinical Professor, UCLASchool of Nursing
Los Angeles, California
Barbara Resnick, PhD, CRNP,FAAN, FAANP
ProfessorUniversity of Maryland School ofNursing
Baltimore, Maryland
Faculty Disclosure Statements:Nannette Brower, Nancy Henry,and Barbara Resnick have nothingto disclose.
Publishing Information:
PublishersJoseph J. D’OnofrioDelaware Media Group66 South Maple AvenueRidgewood, NJ 07450201-612-7676Fax: 201-612-8282www.delmedgroup.com
Editorial DirectorNancy Monson
Art DirectorJames Ticchio
Cover photo credit:© Carol Donner/PhototakeUSA.com
© 2007, Delaware Media Group, Inc. Allrights reserved. None of the contents maybe reproduced in any form without priorwritten permission from the publisher. Theopinions expressed in this publication arethose of the faculty and do not necessarilyreflect the opinions or recommendations oftheir affiliated institutions, the publisher, theNational Conference of GerontologicalNurse Practitioners, the National Geronto-logical Nursing Association, or Ortho-McNeilNeurologics, Inc.
Counseling Points™Neurodegenerative Diseases and Seizure Disorder
Continuing Education Information
Target AudienceThis educational activity is designed to meet the needs of busy gerontological nursesand advanced practice nurses, as well as neuroscience nurses, who are on the frontlines of managing elderly patients with seizures, in an effort to help them stay abreastof the latest research, treatment, and management options.
Learning ObjectivesUpon completion of this educational activity, the participant should be able to:
• Describe the prevalence and impact of seizure disorder in elderly patients with neu-rodegenerative disorders.
• Detail why neurodegenerative disorders combined with the aging physiologyincrease the risk of seizure disorder in the elderly.
• Describe the altered presentation of seizure disorder in the elderly with neurode-generative diseases.
• List the risks and benefits of antiepileptic drugs in elderly patients with seizure dis-order and neurodegenerative diseases.
Continuing Education CreditThis continuing nursing education activity was approved by the National Confer-ence of Gerontological Nurse Practitioners. Successful completion of this activityawards 1.2 contact hours.
The National Conference of Gerontological Nurse Practitioners is accredited as aprovider of continuing nursing education by the American Nurses CredentialingCenter’s Commission on Accreditation.
This program expires December 31, 2009.
Disclosure of Unlabeled UseThis educational activity may contain discussion of published and/or investigationaluses of agents that are not indicated by the FDA.The National Conference of Geron-tological Nurse Practitioners, the National Gerontological Nursing Association, Ortho-McNeil Neurologics, Inc., and Delaware Media Group do not recommend the use ofany agent outside of the labeled indications.The opinions expressed in the educationalactivity are those of the faculty and do not necessarily represent the views of theNational Conference of Gerontological Nurse Practitioners, the National Gerontologi-cal Nursing Association, Ortho-McNeil Neurologics, Inc., or Delaware Media Group.
DisclaimerParticipants have an implied responsibility to use the newly acquired information toenhance patient outcomes and their own professional development.The informationpresented in this activity is not meant to serve as a guideline for patient management.Any medications, diagnostic procedures, or treatments discussed in this publicationshould not be used by clinicians or other healthcare professionals without first evalu-ating the patient’s condition, considering possible contraindications or risks, reviewingany applicable manufacturer’s product information, and comparing any therapeuticapproach with the recommendations of other authorities.

3DECEMBER 2007
Dear Colleague,
Neurodegenerative diseases are of increasing concern to geriatric nurses and advancedpractice nurses as the American population ages. So, too, are seizures, which increase inprevalence as patients grow older.
In this issue of Counseling Points™ on seizures in the elderly, we explore the relation-ship between neurodegenerative diseases and seizure disorder. Neurodegenerative dis-eases such as dementia, stroke, and Parkinson’s disease enhance the risk of seizure dis-order in the elderly, information that is crucial to effective geriatric nursing. Nursesand advanced practice nurses need to know how to recognize seizure disorder in olderpatients with neurodegenerative diseases, because they may display behavioral symp-toms rather than involuntary motor signs and symptoms. Finally, these clinicians alsoneed to know how seizure treatment will impact concurrent medication regimens forneurodegenerative diseases.
Counseling Points™ on seizures in the elderly is an official publication of the NationalConference of Gerontological Nurse Practitioners (NCGNP) and the NationalGerontological Nursing Association (NGNA).We would like to thank Ortho-McNeilNeurologics, Inc. for sponsoring this publication under an educational grant.
We encourage you to send us your comments about the content of this and the othertwo issues in this series on seizure disorder, and we welcome your suggestions for top-ics you would like to see covered in future issues.A space is provided for your input onthe evaluation form on page 15.We also hope you’ll consider becoming involved withthe NCGNP and NGNA, if you’re not already; please visit our websites atwww.ncgnp.org and www.ngna.org for information on membership.
Sincerely,
Debra Bakerjian, PhD, MSN, RN, FNPPRESIDENT, NCGNP
Judith E. Hertz, PhD, RNPRESIDENT, NGNA
welcome

4
Introduction….John is a 77-year-old nursing home resident who is
known for his easy-going demeanor. The nursing home
staff is puzzled by his occasional episodes of intense anger.
Sudden and unprovoked, this behavior is totally out of
character for John.
….Margaret is an 85-year-old woman with severe dementia
who has frequent, sudden muscle contractions. Often, these
brief muscle contractions only affect one of her arms, but at
times her whole body is involved.
….Eleanor is a 69-year-old woman with Parkinson’s disease
residing in the community with her daughter, who is her
primary caregiver. At times, she is noted to stare and is
apparently unaware of her surroundings. At other times,
she will repeatedly blink her eyes. During these periods,
she shows no response when someone tries to get her
attention. Eleanor’s daughter states she is confused after
these episodes.
….Jeanie is a 60-year-old woman with Down syndrome
and dementia who recently moved into a long-term care
facility. The nurse entered her room this evening to find
Jeanie on the floor unconscious and experiencing rhythmic
twitching of her arms and legs.
Despite the differing presentations, each of the indi-
viduals described in the vignettes above is having
seizure activity.Whatever form it takes, seizure activity
negatively impacts on the quality of life and well-being
of the older adult. Thus, it is important for nurses
working with older adults to have an understanding of
the altered presentation of seizures in this population.
Older adults have the highest incidence of seizures
of any age group, although obtaining an accurate diag-
nosis and initiating appropriate treatment is often
delayed.1 Identifying seizures in this population can be
particularly challenging due to an altered presentation:
Behavior changes, increased confusion, and vague
complaints such as dizziness associated with seizures in
the elderly can easily be attributed to a variety of other
conditions.2-4
Overview of Seizure DisorderA seizure is a sudden alteration in normal brain activity
that results in distinct changes in behavior and/or body
function.Acute symptomatic (provoked) seizures occur
when there has been an acute insult to the central
nervous system (CNS). The risk of having an acute
symptomatic seizure rises each decade after the age of
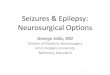
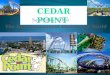
60 (Figure 1).1,5,6 Stroke is the cause of nearly half of
such seizures and typically these seizures will occur
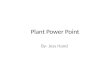
within 24 hours of a stroke event (Figure 2).8 Neu-
rodegenerative disorders are also implicated in pro-
voked seizures. Ten to 22% of those with Alzheimer’s
disease will experience at least one seizure, usually in
the later stages of the disease.9 Other causes of acute
symptomatic seizures in older adults include metabolic
disturbances, drug/alcohol withdrawal, trauma, brain
tumors, and infection.4 In approximately 50% of cases,
COUNSELING POINTS™
Neurodegenerative Diseasesand Seizure Disorder
Figure 1. Incidence of acutesymptomatic and unprovoked seizuresin the elderly.1,6
300
250
200
150
100
50
00 20 40
Age (yrs)
Inci
den
ce/1
00,0
00
Acute symptomatic Unprovoked
60 80
Used with permission from Epilepsia.

5
seizure disorder in older adults is idiopathic—that is,
no cause can be determined.5
The term epilepsy (seizure disorder) is used when
seizures are recurrent and unprovoked.While onset of
epilepsy can occur at any age, there is an increased risk
of both provoked and unprovoked seizures associated
with aging.5,6 In the United States, nearly a quarter of
the 2.3 million persons with epilepsy are over the age
of 65.7 New-onset epilepsy occurs in approximately
60,000 people over age 65 each year.7
While older adults often have chronic health prob-
lems such as cerebrovascular disease that put them at
increased risk of developing seizures, it is likely that the
process of aging itself also increases the risk of seizure
development.4 There are numerous changes in the
aging brain, including the loss of neurons, alterations in
brain chemistry, and histologic changes including lipo-
fuscin and amyloid deposits, that may predispose
patients to seizures.10 Amyloid deposition may play a
role in the development of both Alzheimer’s disease
and seizures. People with Down syndrome have a par-
ticularly high risk of developing Alzheimer’s disease:
This form of dementia occurs in more than half of
those over age 50 in this population, and up to 84% of
those with the combined Down syndrome and
Alzheimer’s disease presentation will have seizures.11 It
appears that what makes those with Down syndrome
highly susceptible to both Alzheimer’s disease and
seizures is that they have an extra copy of chromosome
21, which is involved in the production of amyloid
precursor protein.12
The most common type of seizure in older adults is
the complex partial seizure; however, the presentation
of these seizures can be very different from that seen in
the general population.3 In the general population,
these seizures usually originate in the temporal lobe
and are accompanied by a distinct aura. In older per-
sons, in contrast, complex partial seizures generally
originate in the frontal lobe of the brain, which is
involved in personality, intellect, speech, and move-
ment. Older adults often have a vague complaint such
as dizziness rather an aura. Another difference in
seizure presentation in this population is that automa-tisms (involuntary automatic behaviors such as lipsmacking or picking at clothing) do not occur as fre-quently as in younger persons. Post-ictal confusion,which is often present, also takes longer to resolve inolder versus younger adults.3
In most cases, seizures are brief and self-limiting.Prolonged seizure activity is indicative of status epilep-ticus, a life-threatening event. Status epilepticus isdefined as a single seizure lasting more than 5 minutesor a series of seizures occurring without regainingconsciousness. Status epilepticus is described as convul-sive or non-convulsive activity depending upon thepresentation. In convulsive status epilepticus, tonic-clonic seizure activity is seen, while in non-convulsivestatus epilepticus, behavior and cognition are affected.Non-convulsive status epilepticus is more difficult torecognize for this reason. Older adults are at greaterrisk of developing status epilepticus and face a greatermortality rate than the general population; thisincreased risk and poor outcome rises significantly inthose over age 80.13 Like other seizure activity in olderadults, stroke is often the precipitating factor for statusepilepticus. Other causes include low anti-epilepticdrug (AED) levels, hypoxia or anoxia, metabolic distur-
DECEMBER 2007
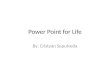
Figure 2. Epilepsy etiology in people>64 years of age.8
Trauma3.3%
Congenital0.5%
Idiopathic49.0%
Degenerative11.5%
Neoplastic2.7%
Infection0.5%
Vascular32.5%
Used with permission from Epilepsia.

6
bances, brain tumors, infection, drug/alcohol with-
drawal, and trauma.5 The immediate concern in status
epilepticus is to stop the seizure activity and maintain
cardiopulmonary functioning.
Stroke and SeizuresCerebrovascular disease, which includes cerebrovascu-
lar accident (CVA), hypertension, and vasculitis, is a
large contributor to disability and death. Annually,
about 700,000 people experience a new or recurrent
stroke.14 Many authorities consider seizure secondary
to stroke as a major cause of epilepsy in the elderly
population.8,15
According to Benbir et al, hemorrhagic and venous
infarctions are more commonly encountered in post-
stroke seizure patients than atherosclerotic or cardioem-
bolic strokes.16 These authors suggest that “strokes rep-
resent the most common etiology of epilepsy in
patients over the age of 60 years, with an incidence of
2-4% occurring in different studies.” Seizures can occur
early (within 7 days) or late (beyond 7 days) after a
stroke, and can be focal or generalized, but are usually
brief and associated with loss of consciousness when
they occur in the presence of hemorrhage.17
Status Epilepticus and Stroke
When remote symptomatic CVAs are combined with
acute stroke cases, stroke represents about 40% of eld-
erly patients with status epilepticus.18 Hence, stroke,
acute or remote, represents a major cause of status
epilepticus in the elderly.19 In a study of 342 patients
with status epilepticus who had their first seizure after
age 60, it was found that cerebrovascular disease was
the primary cause followed by head trauma.20 Hauser
described a retrospective population-based study in
which calculations revealed that almost 0.4% of people
who survive to age 75 will have had a previous episode
Many authorities consider seizure secondary
to stroke as a major cause of epilepsy in the
elderly population.
of status epilepticus.18
Etiology is a strong determinant of status epilepticus
mortality in the elderly. It is likely that the increased
risk of the elderly to develop CVA, systemic metabolic
disease, and progressive symptomatic conditions
(tumor, dementia) makes them more susceptible to
developing status epilepticus. The fact that stroke and
status epilepticus both have high mortality rates raises
the question of whether that high death rate is attrib-
utable to the severity of the underlying CVA or to the
effect of status epilepticus itself.
Dementia, Parkinson’s Disease, andSeizuresThe term “neurogenerative diseases” refers to a large,
clinically and pathologically heterogeneous group that
comprises all of the neurologic disorders leading to
dysfunction and eventual death of subsets of neurons in
highly specific functional anatomic systems of the body.
The most common neurodegenerative diseases of the
brain are Alzheimer’s disease (AD) and Parkinson’s dis-
ease, but also include Lewy body dementia, Hunting-
ton disease, and amyotrophic lateral sclerosis (ALS).21
According to Ramsay, et al, the second most common
cause of seizures in the elderly after cerebrovascular
disease is neurodegenerative diseases.22
Dementia
Degenerative dementias, such as Alzheimer’s disease, are
associated with an increased incidence of seizures.The
prevalence of seizures in patients with dementia ranges
from 10%-20%.23 McAreavey and colleagues deter-
mined in a survey of dementia inpatients that those
with seizure were younger and, according to one meas-
ure of mental status, significantly more cognitively
impaired than control group patients with dementia
only.24
Thomas indicates that Alzheimer’s-type dementia
and amyloid angiopathy are major causes of seizure,
while Romanelli et al identify Alzheimer’s disease as a
risk factor for new-onset generalized tonic-clonic
seizures in older adults.9,25
COUNSELING POINTS™

7
Sirven and Ozuna describe elderly persons as havingseizure presentation characterized by dementia-relatedsymptoms such as confusion, memory loss or delirium,and episodes of staring or disorientation.26 In addition,elderly persons can have unwitnessed seizures whenthey live alone or have limited social interactions.27
In a case study described by Ramsay et al, a primeexample of how cognitive assessment may aid in prop-er diagnosis and treatment of seizures is described asfollows: A 72-year-old woman living alone was admit-ted with a diagnosis of dementia due to episodes ofbeing “fuzzy” without a significant past medical histo-ry.22 On close examination, her electroencephalogram(EEG) revealed a dynamic change from a build-up ofpolymorphic delta activity followed by an abruptchange to a normal recording. The EEG recordingappeared to depict epilepsy, although it did not havethe morphology of epilepsy. Other than the atrophyseen on the CT scan, the clinical evaluation was unre-markable. Only after a video evaluation of the patientwas viewed did what appear to initially be dementialater become evident as seizures.
According to Bergey, the impact of epilepsy on thephysical health status of older adults is substantial andcompounded by co-morbidities found in this popula-tion.28 Given the limited information available on theincidence of seizures and that no reports exist ofseizure predictors in Alzheimer’s patients, Amatniek etal conducted a study to determine cumulative inci-dence and predictors of new-onset seizures in subjectswith mild Alzheimer’s disease in a cohort followedprospectively.29 The study replicated the observation ofearlier studies that an increased risk for unprovokedseizures exists in individuals with Alzheimer’s diseasecompared with others of the same age. This findingsupports the theory that seizures can be a part of thenatural history of Alzheimer’s disease.29-33
Elderly persons can have unwitnessed
seizures when they live alone or have
limited social interactions.
Seizure Semiology in the Elderly
Kellinghaus et al observe that the degenerative processes
of the aging brain do not influence the symptoms of
seizures in the same way as the myelinating and matu-
ration processes do in the first years of life.34 There are
no major differences in the frequency of seizure types
between the elderly and a younger control group
matched according to location of the epileptogenic
focus. Seizures with auras, automotor seizures with typ-
ical orofacial automatisms, and all seizure types with
complex, semi-purposeful movements occur equally in
both groups.
The notion that a different seizure semiology exists
in the elderly is based primarily on the findings of a
few hospital-based studies and one population–based
study.8,35-40 These studies used the current classification
of the International League Against Epilepsy (ILAE) of
1981 and distinguished only between simple partial,
complex partial, and generalized seizures. The specific
signs of seizure in the elderly reported in these studies
may have been due to the use of a less-adequate seizure
classification, the lack of an adequate control group
eliminating location-inherent differences in semiology,
and, especially in the case-population study, a different
recruitment setting.
Kellinghaus et al also note that simple motor
seizures like focal clonic seizures, versive seizures, and
bilateral asymmetric tonic seizures are seen less fre-
quently in elderly patients, a difference that might be
attributed to the higher number of patients with
generalized cerebral atrophy and white matter
lesions.34 Therefore, one could speculate that the
aging brain is less able to prevent the spread of focal
seizure activity.
Seizures and Epilepsy in the OlderAdult: When to Initiate SeizureTreatmentThe decision to initiate treatment with medication for a
seizure should be based on evidence of recurrent
seizures, onset of epilepsy as status epilepticus, or the
presence of a clear structural predisposition for seizures.10
DECEMBER 2007

8
In particular, medical interventions probably should be
initiated if the individual has seizures that impact quality
of life.
Treatment Options
Pharmacologic interventions are the primary manage-
ment of seizure disorder and treatment choices are
generally based on what is known about the seizure
(e.g., simple versus complex partial seizures, tonic
clonic, or myoclonic), the known co-morbidities of the
individual, and drug side effects.10,22 Consistent with
multiple clinical guidelines, it is emphasized that all
AEDs are equally efficacious for seizure control.41,42
The newer AEDS (Table 1), however, are known to
have fewer adverse effects than older agents such as
phenytoin and carbamazepine.41 In general, for older,
medically stable patients with idiopathic, generalized
seizures, lamotrigine and valproic acid are recommend-
ed as first-line treatments.10 Phenytoin and carba-
mazepine are also often used in this setting due to their
lower costs and previously established effectiveness.10
The specific risks and challenges of use of these drugs
in older adults are related to known hepatic changes
and altered drug metabolism that occurs with age, and
an increased likelihood of drug-drug interactions. It is
also challenging to utilize currently advised dosages
and drug serum levels, as these values were developed
in and for younger individuals. Drug choices and
potential side effects are shown in Table 2.
Decisions on drug use must be made based on indi-
vidual needs and side-effect profiles. With regard to
drug dosing, the guideline is to start low and monitor
drug response in terms of prevention of seizure.
Extended-release formulations may be helpful with
regard to drug adherence. Expense can further influ-
ence treatment decisions, with older AEDs generally
being less costly than newer AEDs.43 It is not clear,
however, what the potential costs of drug-drug interac-
tions and other negative outcomes may be that can
occur from use of the older treatment options (e.g.,
falls, fractures, confusion, sedation).
Certain drugs may offer a particular advantage in
select patient populations. For example, topiramate
may be helpful in obese patients as it can result in
weight loss; for the same reason, it should be avoided
in older adults with anorexia. Drugs with a more
favorable cognitive profile in terms of side effects
include gabapentin, tiagabine, lamotrigine, oxcar-
bazepine, and levetiracetam.43
Special Challenges Associated withMedication Management in Older Adults
Age-related physiologic changes in protein binding,
albumin levels, hepatic metabolism, renal clearance, and
absorption may influence AED metabolism and utiliza-
tion.44 Specifically, decreasing renal and hepatic function
with age decreases the body’s ability to eliminate med-
ication. There is also a decrease in oxidative metabolism
via the cytochrome P-450 enzyme system, which fur-
ther influences metabolism. In addition, there is a
decreased ratio of muscle to body fat influencing drug
binding. Therefore, a standard medication dose may
result in higher drug serum concentrations in an older
individual. In light of the reduced protein binding of
drugs that occurs with age, drugs that are highly pro-
tein-bound such as phenytoin and carbamazepine may
have normal or low plasma levels but high levels of free
drug in the plasma, ultimately resulting in toxicity.
Generally, based on their pharmacokinetics, the
COUNSELING POINTS™
Table 1. Older and Newer AEDs
Older AEDs Newer AEDs(Available Prior Year (Available After Year
to 1993) Introduced 1993) Introduced
Phenobarbital 1912 Felbamate 1993
Phenytoin 1938 Gabapentin 1993
Ethosuximide 1960 Lamotrigine 1994
Diazepam 1968 Topiramate 1996
Carbamazepine 1974 Tiagabine 1997
Valproic acid 1978 Levetiracetam 1999
Oxcarbazepine 2000
Zonisamide 2000
Pregabalin 2005

9DECEMBER 2007
Table 2. Medications for Seizure Management*
Drug Indication Advantages Disadvantages Adverse Events
Carbamazepine(Tegretol®)
Partial seizures Minimal sedation andcognitive adverse effects
Ataxia; diplopia; multipledrug interactions
Tremor; hyponatremia; lowerWBC; osteoporosis; rash;cognitive changes; drug-drug interactions
Felbamate(Felbatol®)
Partial seizures—used only inrefractory disease
None Risk of serious adverseevents
Aplastic anemia; weight loss;liver failure; gastrointestinalupset; sleep changes;headache
Gabapentin(Neurontin®)
Partial seizures No hepatic metabolism;drug interaction only withantacids
Dosage modificationneeded in patients withrenal disease; TID dosingrequired
Tiredness
Lamotrigine(Lamictal®)
Partial seizures Interaction with AEDsonly
Dosage modificationneeded in patients withliver disease
Prolonged half life; rash
Levetiracetam(Keppra®)
Partial seizures;myoclonic seizures;tonic-clonicseizures
Effective in the treatmentof multiple types ofseizures
Possible impact onbehavior
Unusual thoughts orbehaviors; fever; chills; bodyaches; flu symptoms;depression
Oxcarbazepine(Trileptal®)
Partial seizures Low side-effect profile Photosensitivity; doseshould be adjusted whenthe glomerular filtrationrate is <30
Hyponatremia; fatigue;altered cognition
Phenytoin(Dilantin®)
Partial seizures Low cost Many drug andfood/nutrient interactions
Peripheral neuropathy;gingival hypertrophy; frozenshoulder; osteoporosis; rash;cognitive changes; drug-drug interactions
Pregabalin(Lyrica®)
Partial seizures;generalizedseizures
Reduced platelet counts;increased blood creatininekinase levels with associatedmuscle pain; sedation;dizziness; edema; weightgain; impaired cognition
Tiagabine(Gabitril®)
Partial seizures None Dosage modificationneeded in patients withliver disease
Slowed thinking; tiredness
Topiramate(Topamax®)
Partial seizures;generalizedseizures
Interaction with AEDsonly; weight loss
Weight loss; dosagemodification required ifcreatinine clearance is <60mL per minute
Weight loss; renal stones;slowed thinking
Valproic acid(Depakene®)
Generalizedseizures; absenceseizures
Broad-spectrum efficacy Extensive protein binding;multiple drug interactions
Tremor; effect on plateletfunction; drug-druginteractions
*Optimal dosage is based on prevention of seizure, not on reaching therapeutic drug levels.AEDs=anti-epileptic drugs; TID=three times a day; WBC=white blood count.

10
older AEDs tend to be more difficult to manage thanthe newer AEDs.The older AEDs are mostly metabo-lized by the P-450 enzyme system, which can impactother drugs being used by the individual. Conversely,the newer AEDs are metabolized via the glucuronida-tion system with less risk of drug-drug interactions.For example, gabapentin, levetiractam, and pregabalinare almost 100% cleared by the renal pathway andtherefore have a low risk for drug-drug interactions.
Although a therapeutic range has been establishedfor the older medications, treatment should be drivenby cessation of seizures without side effects from med-ications, rather than based on a recommended thera-peutic range.45 Moreover, older adults can have a totalphenytoin serum concentration that is below the ther-apeutic range, yet have unbound concentrations thatare within the therapeutic range.
Treatment Complications Associated withCo-morbidities
Older adults commonly experience multiple co-morbidities that not only contribute to the incidenceof seizures but likewise impact treatment. Co-morbidities can impact adherence to medications dueto cognitive impairment, degenerative joint diseaseand functional impairment, or vision changes—all ofwhich can make it difficult for patients to rememberhow to manage their medications. Likewise, condi-tions associated with dysphagia, diplopia, and absorp-tive disorders can influence medication management.
Treatment Consequences: Adverse Effectsof AEDs
AEDs can be associated with hypersensitivity, dose-related adverse events, or adverse events related tochronic use. In particular, older adults are more sensi-tive to dose-related events such as ataxia, which canoccur at doses lower than those seen in younger indi-viduals. The major problem with adverse events inolder adults is that they can have a significant impacton function. Associated ataxia, peripheral neuropathy,tremor, hyponatremia, and/or soft-tissue changes caninfluence the individual’s ability to ambulate safely or
engage in activities of daily living. Table 2 providessome of the most common adverse events.
Dosing and Administration Considerations
If the first AED prescribed is not well tolerated at lowdoses or does not stop seizures, an alternative agent canbe tried. If the first drug initiated is well tolerated butdoesn’t control the seizures, then a second drug can beadded. Generally administered via the oral route, theabsorption of carbamazepine is decreased when givenduring nasogastric feeding.To improve absorption, car-bamazepine suspension should be mixed with an equalvolume of dilutant prior to being inserted into thenasogastric feeding tube.
Discontinuation of PharmacologicManagementConsideration can be given to stopping medication ifthe patient is free of seizures for 2 to 5 years.When adecision to withdraw an AED is made, the drug shouldbe tapered no faster than every 4 to 6 weeks in decre-ments of 20%.46 If a subsequent seizure occurs, imme-diate treatment of seizures for institutionalized olderadults can be started with diazepam administered as abuccal squirt or rectal suppository.
The Role of the Nurse and AdvancedPractice NurseThe main concern of the nurse and advanced practicenurse during a seizure is to protect the person experi-encing the episode from harm and to maintain a patentairway. In the event that this is a first seizure or if seizureactivity is prolonged (status epilepticus), immediateemergency medical care is needed. Table 3 describesnursing interventions during seizure activity.47
Seizure Documentation
Seizure documentation is a valuable tool both in mak-ing the diagnosis of seizure disorder and in evaluatingthe efficacy of treatment. Observation and documenta-tion should include the following:• What preceded the seizure• Duration of the seizure
COUNSELING POINTS™

11
• Description of motor movement or rigidity type,where the seizure started, its progression, and partsof the body involved
• Position of eyes, size of pupils, staring, unrespon-siveness
• Position of head• Automatisms (twitching, jerking movements, or
other atypical movements)• Vocalizations (humming, talking, etc.)• Confused or combative or other behavior changes• Stiffness of extremities• Incontinence of bowel or bladder or emesis• Loss of consciousness—when and for how long• Falling to the ground• Injury during the seizure• Behavior after the seizure—confusion, weakness,
paralysis, sleep, or inability to speak.• Medical interventions (medication, oxygen, vagus
nerve stimulation) during the episode.47
Psychosocial ImplicationsThe onset of a seizure disorder in the older adult has anumber of psychosocial implications. Epilepsy, unfortu-nately, remains a stigmatized illness. Older persons mayremember a time when there were many misconcep-tions and limited treatment options available. Educatingolder adults with seizure disorder and their families isimportant. Support groups and resources such as TheEpilepsy Foundation (www.efa.org) will prove helpful.
A seizure disorder diagnosis is a life-altering eventfor an older adult and can compromise his or her qual-ity of life. Seizure-related falls can result in injuriessuch as fractures that, in turn, can limit mobility andself-care activities. The older adult or family membersmay question the safety of the patient continuing tolive on his or her own. Falls and fall-related injuries,seizure-related or not, often lead to nursing homeplacement in the older adult population.48 In addition,independence may be limited when driving privilegesare revoked until it has been established that treatmentis controlling seizure activity.
Older adults with newly diagnosed seizure disordermay curtail previously enjoyed activities. Some activi-
ties such as swimming may be unsafe if seizures are
poorly controlled. In addition, patients may withdraw
from socialization due to fear of embarrassment.
There appears to be a correlation between major
depression and epilepsy.Those who develop epilepsy in
later life tend to report greater anxiety and depression,
and to rate their overall quality of life as lower than
those who have been living with epilepsy for some
time.49 Studies have found that there is a six times
greater incidence for developing epilepsy in those with
major depression.50 Some question the validity of these
retrospective studies. The medications that are com-
monly used in treating people with major depression
in years past included benzodiazepines, which have
themselves been linked to seizure development.51 It
appears that psychiatric co-morbidities, including
depression, worsen with seizures.4
DECEMBER 2007
Table 3. Nursing Interventions DuringSeizure Activity47
• Do not restrain someone during a seizure.
• Protect the person from injury by clearing the immediate
area of any hazards.
• Protect the head as much as possible—e.g., place padded
siderails on the bed and outfit the patient with protective
head gear if he or she is known to have frequent seizures,
especially generalized ones.
• Do NOT place anything in the person’s mouth.
• If possible, turn the person’s head to the side to prevent
aspiration of pooling respiratory secretions. Have suction
equipment readily available in case it becomes necessary
to suction the person.
• Monitor for color changes and administer oxygen if there
is a color change.
• Observe for respiratory depression, which can occur dur-
ing seizures.
• Remain with the person until consciousness is fully
regained. It is not unusual for someone who has had a
seizure to sleep afterwards. Place the person lying on his
or her side (recovery position) if possible.
• Document seizure activity.

12
SummarySeizure is an important differential diagnosis to consid-
er in the care of older adults. Decisions to treat or not
to treat the older individual, however, need to be made
carefully based on the impact of the seizure on the
quality of life of the individual balanced against the
side effects of drug management. Using this approach
to facilitate the evaluation and treatment of older adults
for seizure will help nurses and advanced practice nurs-
es optimally manage this potentially devastating clinical
problem.
References
1. Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovokedseizures in Rochester, Minnesota: 1935-1984. Epilepsia. 1993;34:453-468.
2. Sirven J. Funny spells: Recognizing and diagnosing seizures. Slide set from9th Annual Teleconsult in Epilepsy. Accessed 8/9/07 at www.aesnet.org.
3. Sirven J. Management of epilepsy in older adults. Clin Geriatrics.2000;8:1. Accessed 8/9/07 at www.cl inicalgeriatr ics.com/article/1098.
4. Rowan AJ. Epilepsy in older adults: Common morbidities influence devel-opment, treatment strategies, and expected outcomes. Geriatrics.2005;60:30-34.
5. Hauser WA. Epidemiology of seizures and epilepsy in the elderly. In:Rowan AJ, Ramsay RE, eds. Seizures and Epilepsy in the Elderly. New-ton, Ma: Butterworth-Heinemann. 1997;7-18.
6. Annegers JF, Hauser WA, Lee JR, et al. Incidence of acute symptomaticseizures in Rochester, Minnesota: 1935-1984. Epilepsia. 1995;36:327-333.
7. Begley CE, Famulari, Annegers JF, et al. The cost of epilepsy in the Unit-ed States: An estimate from population-based clinical and survey data.Epilepsia. 2000;41:342-351.
8. Hauser WA. Seizure disorders: The changes with age. Epilepsia.1992;33(suppl 4):S5-14.
9. Thomas RJ. Seizures and epilepsy in the elderly. Arch Intern Med.1997;157:605-617.
10. Velez L, Selwa L. Seizure disorders in the elderly. Am Family Physician2003;67:325-332.
11. Porth CM. Pathophsiology Concepts of Altered Health States, 5th ed. Lip-pincott: Philadelphia, Pa. 1998;1321.
12. Menendez, M. Down syndrome, Alzheimers disease, and seizures. BrainDev. 2005;27:246-252.
13. Hessdorfer DC, Logroscino G, Cascino G, et al. Incidence of statusepilepticus in Rochester, Minnesota, 1965-1984. Neurology. 1998;50:735-741.
14. American Heart Association. Heart Disease and Stroke Statistics—2007Update. Accessed 9/27/07 at www.americanheart.org/download-able/heart/1166712318459HS_StatsInsideText.pdf.
15. Annergers JF, Rocca WA, Hauser WA. Causes of epilepsy; contributionsof the Rochester Epidemiology Project. Mayo Clinic Proceedings, MayoClinic. 1996;71:570-575.
16. Benbir G, Ince B, Bozluolcay M. The epidemiology of post-stroke epilep-sy according to stroke subtypes. Acta Neurol Scand. 2006;114:8-12.
17. Feleppa M, DiIorio W, Saracino DM. Early poststroke seizures. Clin ExpHypertens. 2006;28:265-270.
18. Hauser WA. Status epilepticus: Epidemiologic considerations.Neurology. 1990;40:(5suppl 2):9-13.
19. Waterhouse EJ, Delorenzo RJ. Status epilepticus in older patients. DrugsAging. 2001;18:133-142.
20. Sung CY, Chu NS. Status epilepticus in the elderly: etiology, seizure,type and outcome. Acta Neurol Scand.1989;80:51-56.
21. Przedborski S, Vial M, Jackson-Lewis V. Neurodegeneration: what is itand where are we? J Clin Invest. 2003;111:3-10.
22. Ramsay RE, Rowan JA, Pryor FM. Special considerations in treating theelderly patient with epilepsy. Neurology. 2004;62(5suppl2):S24-S29.
23. Ramsay RE, Pryor F. Epilepsy in the elderly. Neurology. 2000;55(5suppl1): S9-S14.
24. McAreavey MJ, Ballinger BR, Fenton GW. Epileptic seizures in elderlypatients with dementia. Epilepsia. 1992;33:657-660.
25. Romanelli MF, Morris JC, Ashkin K, et al.Advanced Alzheimer’s diseaseis a risk factor for late-onset seizures. Arch Neurol. 1990;47:847-850.
26. Sirven JI, Ozuna J.Diagnosing epilepsy in older adults: what does itmean for the primary care physician? Geriatrics. 2005;60:30-35.
27. Van Coll AC. Epilepsy and EEG in the elderly. Epilepsia. 2002;34(suppl 3):94-102.
28. Bergey GK. Initial treatment of epilepsy: Special issues in treating the eld-erly. Neurology. 2004;63(10suppl4):S40-48.
29. Amatniek JC, Hauser WA, DelCastillo-Castaneda C, et al. Incidence andpredictors of seizures in patients with Alzheimer’s disease. Epilepsia.2006;47:867-872.
30. Risse SC, Lampe TH, Bird TD, et al. Myoclonus, seizures, and paratoniain Alzheimer disease. Alzheimer Dis Assoc Disord. 1990;4:217-225.
31. Bjork RJ, Pleumer S, Scandura D. Incidence of seizures in a residentialAlzheimer care facility. Epilepsia. 1995;36:244.
32. Forstl H, Burns A, Levy R, et al. Neurologic signs in Alzheimer’s disease:results of prospective clinical and neuropathologic study. Arch Neurol.1992;49:1038-1042.
33. Lehotovirta M, Soininen H, Helisalmi S, et al. Clinical and neuropsycho-logical characteristics in familial and sporadic Alzheimer’s disease: rela-tion to apolipoprotein E polymorphism. Neurology. 1996;46:413-419.
34. Kellinghaus C, Loddenkemper T, Dinner DS, et al.Seizure semiology inthe elderly: A video analysis. Epilepsia. 2004;45:263-267.
35. Drury I, Selwa LM, Schuh LA, et al. Value of inpatient diagnostic CCTV-EEG monitoring in the elderly. Epilepsia. 1999;40:1100-1102.
36. Lanceman ME, O’Donovan C, Dinner D, et al. Usefulness of prolongedvideo-EEG monitoring in the elderly. J Neurol Sci. 1996;142:54-58.
37. Keranen T, Rainesalo S, Peltola J. The usefulness of video-EEG monitoringin elderly patient with seizure disorders. Seizure. 2002;11:269-272.
38. McBride AE, Shih TT, Hirsch LJ. Video-EEG monitoring in the elderly: areviw of 94 patients. Epilepsia. 2002;43:165-169.
39. Luhdorf K, Jensen LK, Plesner AM. Epilepsy in the elderly: prognosis.Acta Neurol Scand. 1986;74:409-415.
40. Tinuper P, Provini F, Marini C, et al. Partial epilepsy of long duration:changing semiology with age. Epilepsia. 1996;73:162-164.
41. Pugh MJ, Foreman PJ, Berlowitz DR. Prescribing antiepileptics for the eld-erly: differences between guideline recommendations and clinical prac-tice. Drugs Aging. 2006;23 861-875.
42. Glauser T, Ben-Menachem E, Bourgeois B, et al. ILAE treatment guide-lines: Evidence based analysis of antiepileptic drug efficacy and effec-tiveness of initial monotherapy for epileptic seizures and syndromes.Epilepsia. 2006; 47:1094-1020.
43. Asconape JJ. Some common issues in the use of antiepileptic drugs. SemNeurol. 2002;22:27-39.
44. Gidal BE. Drug absorption in the elderly: Biopharmaceutical considera-tions for the antiepileptic drugs. Epilepsy Research. 2006; 68(supp 1):S1-S4.
45. Jannuzzi G, Cian P, Fattore C, et al. A multicenter randomized controlledtrial on the clinical impact of therapeutic drug monitoring in patients withnewly diagnosed epilepsy. Epilepsia. 2000;41:222-230.
46. Lackner TE. Strategies for optimizing antiepileptic drug therapy in elderlypeople. Pharmacotherapy. 2002; 22:329-364.
47. Nettina S. Lippincott Manual of Nursing Practice, 8th ed. Lippincott:Philadelphia, Pa. 2005, 544-550.
48. Tinneti ME, Williams CS. Falls, injuries due to falls, and the risk ofAdmission to nursing home. N Engl J Med. 1997;337:1279-1284.
49. Waterhouse E, Towne A. Seizures in the elderly:nuances in presentationand treatment. Cleve Clin J Med. 2005;75(suppl 3):S26-37.
50. Hesdorffer DC, Hauser WA, Annegers JF, et al. Major depression is arisk factor for seizures in older adults. Ann Neurol. 2000;47:246-249.
51. Chandlee CD. Does major depression increase the risk for seizures inolder adults? J Watch Neurol. Accessed 8/6/07 at www.neurology.jwatch.org/cgi/content/full/2000/501/6.
COUNSELING POINTS™

13DECEMBER 2007
• Older adults have the highest incidence of seizures of any age group, although obtain-ing an accurate diagnosis and initiating appropriate treatment is often delayed due toan altered presentation of the disorder.
• The risk of having an acute symptomatic seizure rises each decade after the age of 60.
• While older adults often have chronic health problems such as cerebrovascular diseasethat put them at increased risk of developing seizures, it is likely that the process ofaging itself also increases the risk of seizure development.
• The most common type of seizure in older adults is the complex partial seizure. Thepresentation of these seizures can be very different from that seen in the general popu-lation.
• Stroke represents a common cause of seizures and status epilepticus in older adults.
• The second most common cause of seizures in the elderly after cerebrovascular diseaseis neurodegenerative diseases, such as dementia and Parkinson’s disease.
• The decision to initiate treatment with medication for a seizure should be based on evi-dence of recurring seizures, onset of epilepsy as status epilepticus, or the presence of aclear structural predisposition for seizures.
• All antiepileptic drugs are equally efficacious for seizure control, but the newer agentshave fewer adverse effects than the older agents.
• Decisions on drug use must be made based on individual needs and side-effect pro-files.
• Treatment should be driven by cessation of seizures without side effects from medica-tions, rather than based on a recommended therapeutic range.
• Consideration can be given to stopping a medication if the patient is seizure-free for 2to 5 years.
• The main concern of the nurse and advanced practice nurse during a seizure is to pro-tect the person experiencing the episode from harm and to maintain a patent airway.
• Seizure documentation is a valuable tool both in making a diagnosis of seizure disorderand in evaluating the efficacy of treatment.
• There appears to be a correlation between major depression and epilepsy.
Neurodegenerative Diseasesand Seizure Disorder
CPCounseling Points™

14COUNSELING POINTS™
1. What percentage of patients with Alzheimer’sdisease will experience at least one seizure, usuallyin the later stages of the disease?A) 2%-4%B) 5%-8%C) 10%-22%D) 25%-30%
2. Which of the following changes in the brainpredisposes older adults to seizures?A) loss of neuronsB) changes in brain chemistryC) histologic changes including lipofuscin and amyloid
depositsD) all of the above
3. Older adults with combined Down syndrome andAlzheimer’s disease are at greater risk ofdeveloping seizures than other elderly adults.A) TrueB) False
4. According to Benbir et al, which types of strokesare more commonly encountered in post-strokeseizure patients?A) Hemorrhagic infarctionsB) Venous infarctionsC) Atherosclerotic infarctionsD) Both A and B
5.According to a retrospective study conducted byHauser, what percentage of people who survive toage 75 will have had a previous episode of statusepilepticus?A) 0.4%B) 0.8%C) 1.3%D) 2.0%
6. The second most common cause of seizures in theelderly after cerebrovascular disease is:A) alcohol/drug withdrawalB) neurodegenerative diseasesC) metabolic disturbancesD) brain tumors
7. Which of the following anti-epileptic drugs (AEDs)may be helpful in obese patients as it can result inweight loss?A) GabapentinB) LamotrigineC) OxcarbazepineD) Topiramate
8. Common adverse events associated with manyAEDs include all BUT which of the following?A) TremorB) Peripheral neuropathyC) Low blood glucoseD) Drug-drug interactions
9. When a decision is made to withdraw an AED, thedrug should be tapered no faster than every 4 to 6weeks in decrements of:A) 5%B) 10%C) 20%D) 30%
10. Retrospective studies indicate that there is a ___greater incidence for developing epilepsy in thosewith major depression.A) 3 timesB) 4 timesC) 5 timesD) 6 times
Counseling Points™Neurodegenerative Diseases and Seizure Disorder
Continuing Education PosttestTo receive credit, please read the newsletter in its entirety and answer the posttest and program evaluation ques-tions using the answer key on page 15. Please fax the form to Delaware Media Group at (201)612-8282.A certificate will be awarded for a score of 80% (8 correct) or better and will be mailed to you within 4-6weeks.There is no charge for CE credit.

15DECEMBER 2007
Fax form to (201) 612-8282
Fax form to (201) 612-8282
Counseling Points™: Neurodegenerative Diseases and Seizure DisorderTo assist us in evaluating the effectiveness of this activity and to make recommendations for future educational offerings, please take a few minutes tocomplete this evaluation form. You must complete this evaluation form to receive acknowledgment for completing this activity.
Please answer the following questions by circling the appropriate rating:
1 = Strongly Disagree 2 = Disagree 3 = Neutral 4 = Agree 5 = Strongly Agree
Extent toWhichYou AgreeWith the Following Statements: (Please circle the appropriate number on the scale.)
1. A diagnosis of dementia does not increase the likelihood of a seizure. .......................................................................................................... 1 2 3 4 5
2. Stroke is well-accepted as the most common etiology of epilepsy in the elderly. .......................................................................................... 1 2 3 4 5
3. Seizures rarely occur beyond 7 days after a stroke. .................................................................................................................................... 1 2 3 4 5
4. Parkinson’s disease can sometimes precipitate seizure disorders in the elderly. ..................................................................................... 1 2 3 4 5
Extent toWhich Program Activities Met the Identified Objectives: (After completing this activity, I am now better able to:)
5. Describe the prevalence and impact of seizure disorder in elderly patients with neurodegenerative disorders. ................................. 1 2 3 4 5
6. Detail why neurodegenerative disorders combined with the aging physiology increase the risk of seizure disorder in the elderly. 1 2 3 4 5
7. Describe the altered presentation of seizure disorder in the elderly with neurodegenerative diseases. ................................................. 1 2 3 4 5
8. List the risks and benefits of antiepileptic drugs in elderly patients with seizure disorder and neurodegenerative diseases. .............. 1 2 3 4 5
Overall Effectiveness of the Activity: (The content presented:)
9. Was timely and will influence how I practice.......................................................................................................................................... 1 2 3 4 5
10. Enhanced my current knowledge base .................................................................................................................................................. 1 2 3 4 5
11. Addressed my most pressing questions................................................................................................................................................... 1 2 3 4 5
12. Provided new ideas or information I expect to use .............................................................................................................................. 1 2 3 4 5
13. Addressed competencies identified by my specialty.............................................................................................................................. 1 2 3 4 5
14. Avoided commercial bias or influence .................................................................................................................................................. 1 2 3 4 5
Impact of the Activity
Name one thing you intend to change in your practice as a result of completing this activity:________________________________________________________
______________________________________________________________________________________________________________________________________________________
Please list any topics you would like to see addressed in future educational activities: ________________________________________________________________
______________________________________________________________________________________________________________________________________________________
Additional comments about this activity: ____________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________________________
Follow-up
As part of our continuous quality improvement effort, we conduct postactivity follow-up surveys to assess the impact of our educational interven-tions on professional practice. Please indicate if you would be willing to participate in such a survey:
� Yes, I would be interested in participating in a follow-up survey. � No, I’m not interested in participating in a follow-up survey.
If you wish to receive acknowledgment for completing this activity, please complete the posttest by selecting the best answer to each question,
complete this evaluation verification of participation, and fax to (201) 612-8282.
Posttest Answer Key
Request for Credit
Name _________________________________________________________________ Degree ________________________________________
Organization___________________________________________________________ Specialty ________________________________________
Address_________________________________________________________________________________________________________________
City _____________________________________________________________________________ State __________ ZIP ________________
Phone _____________________________ Fax _____________________________ E-mail __________________________________________
Signature_________________________________________________________________ Date ______________________________________
1 2 3 4 5 6 7 8 9 10
EVALUATION FORM

www.delmedgroup.com
CP


















![P oint-to- P oint T unneling P rotocol [PPTP]](https://img.pdfslide.us/doc/110x75/568145f9550346895db3036c/p-oint-to-p-oint-t-unneling-p-rotocol-pptp.jpg)