Embed Size (px)
Citation preview
1
COPD:Disease Trajectory and Hospice
Eligibility
Terri L. Maxwell PhD, APRN
VP, Strategic Initiatives
Weatherbee Resources
Hospice Education Network
Course Handouts &
Disclosure
� To download presentation handouts, click on the attachment icon
� Presenter discloses no financial relationships with a commercial entity producing healthcare-related products and/or services. Conflict of interest disclosure and resolution statement is on file with HEN.
� This presentation is for educational and informational purposes only. It is not intended to provide legal, technical or other professional services or advice.
Learning Objectives
� List the stages and clinical course of COPD
� State symptoms experienced by patients with COPD
� Identify “secondary” and “co-morbid” conditions
commonly associated with COPD
� Explain end-of-life issues experienced by COPD
patients and their caregivers
� Describe the basic management and treatment of
COPD
� Name the clinical data points necessary to substantiate
hospice eligibility for patients with COPD
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
2
Chronic Obstructive Pulmonary
Disease (COPD)
� Respiratory disorder characterized by
chronic airway obstruction and lung
hyperinflation
� 12 million diagnosed with COPD
� 4th leading cause of death in the US
�Death rate for COPD has doubled over
past 30 yrs, largely due to exposure to
tobacco smoke and is expected to climb to
3rd by 2020
Jemal, Ward, Hao, Thun. JAMA. 2006, 295(4): 393-394.
Key Attributes of COPD
1. Airway obstruction
2. Not fully reversible
3. Progressive disease that generally
worsens over time, even with treatment
4. Abnormal inflammatory response
Celli BR et al. Eur Respir J. 2004;23:932-946.
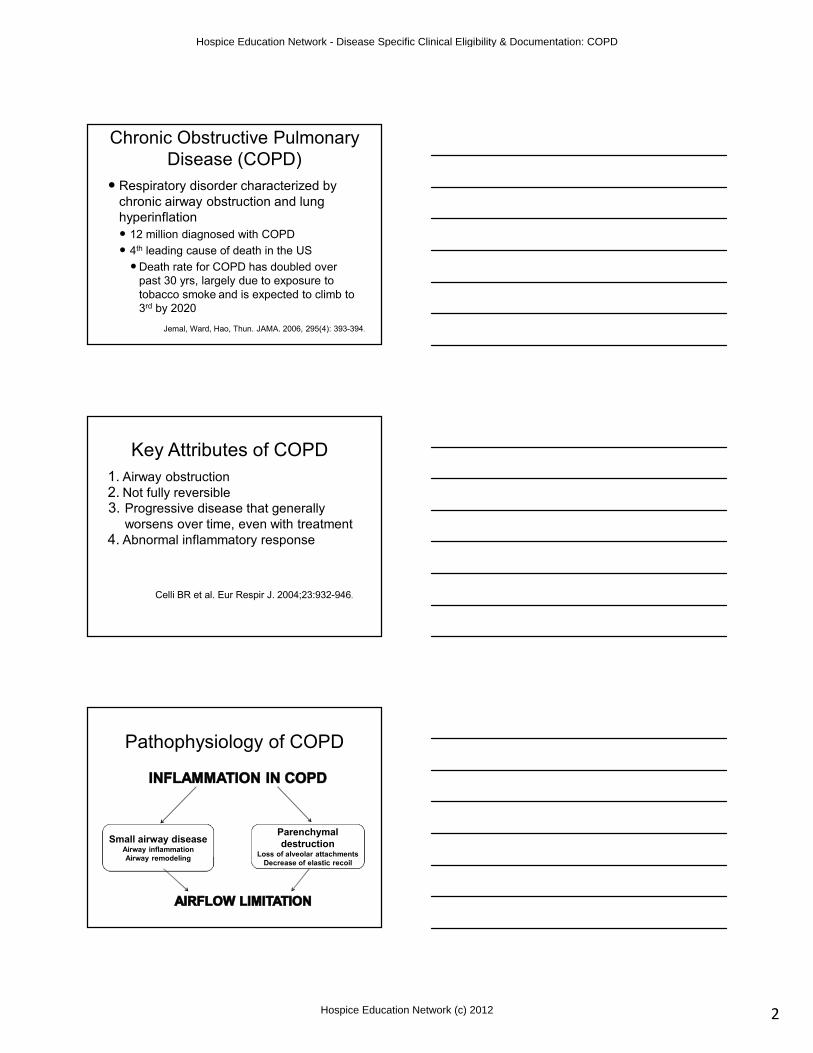
Pathophysiology of COPD
Small airway diseaseAirway inflammation
Airway remodeling
Parenchymal
destructionLoss of alveolar attachments
Decrease of elastic recoil
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
3
Factors Determining
COPD Severity
� Degree of symptoms
� Frequency and severity of exacerbations
� Presence of co-morbidities that can lead to complications
� General health status
� Number of medications needed to manage disease
� Severity of spirometric abnormality/airflow limitation
COPD Severity
Severity of airflow
obstruction
FEV1 % Predicted
Mild 50-80%
Moderate 30-40%
Severe <30%
Spirometry is the gold standard for
diagnosing COPD; severity is
measured by FEV1
Note: FEV= Forced Expiratory Volume
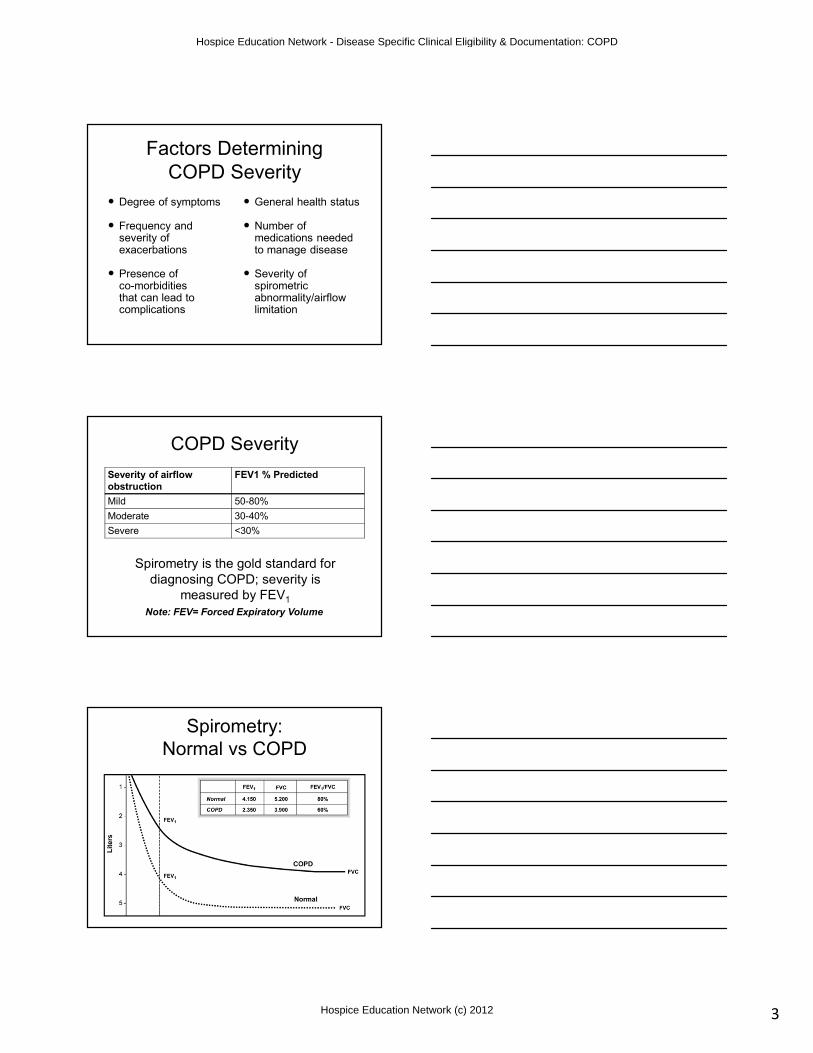
Spirometry:
Normal vs COPD
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
4
Stages of COPD
Stage I: Mild COPD:
� FEV1/FVC < 0.70; FEV1 ≥ 80% predicted.
Patient unaware lung function is abnormal
Stage II: Moderate COPD:
� FEV1/FVC < 0.70; 50% ≤ FEV1 < 80%
predicted. Patient typically seeks medical
attention because of pulmonary symptoms
Adapted from GOLD Guidelines, 2007
Stages of COPD (cont’d)
Stage III: Severe COPD:
� FEV1/FVC < 0.70; 30% ≤ FEV1 < 50% predicted. Greater shortness of breath, reduced exercise tolerance, decreased quality of life
Stage IV: Very Severe COPD:
� FEV1/FVC < 0.70; 30% ≤ FEV1 < 50% predicted plus the presence of chronic respiratory failure. May have signs of cor pulmonale and usually oxygen dependent.
Adapted from GOLD Guidelines, 20072
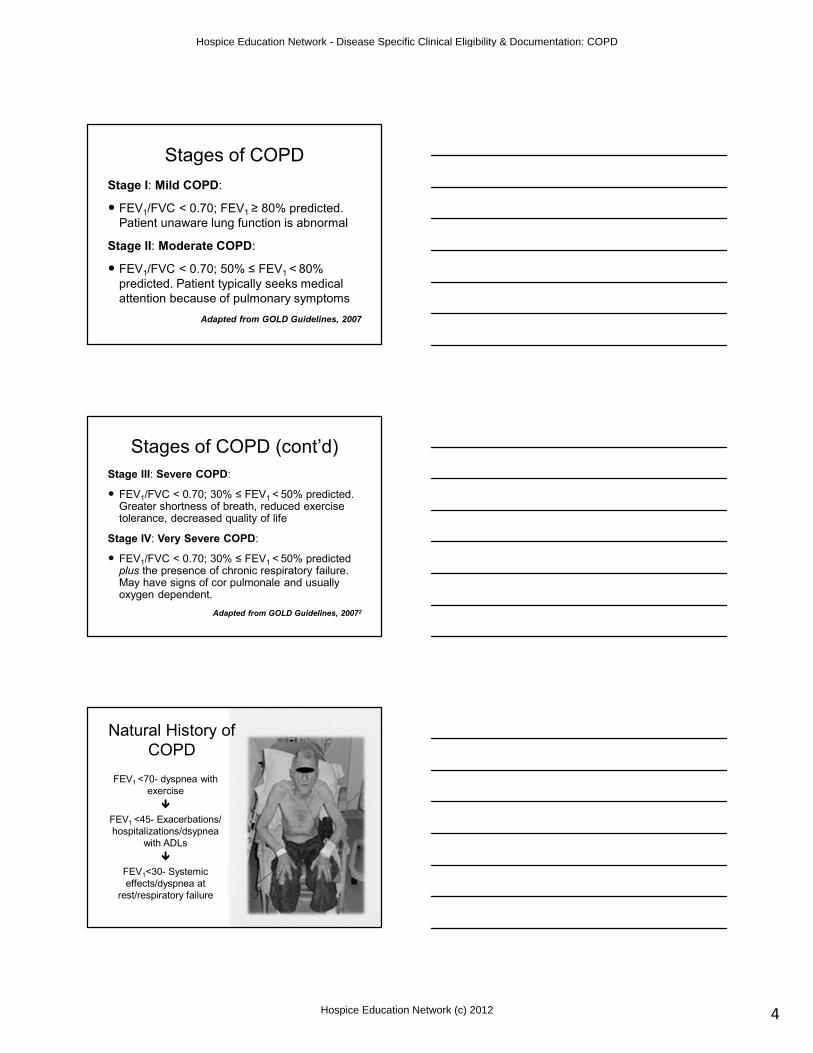
Natural History of
COPD
FEV1 <70- dyspnea with
exercise
�
FEV1 <45- Exacerbations/
hospitalizations/dsypnea
with ADLs
�
FEV1<30- Systemic
effects/dyspnea at
rest/respiratory failure
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
5
COPD and Co-morbid
ConditionsCommon co-morbids:
• Cardiovascular
disease
• Lung cancer
• Osteoporosis
• Musculoskeletal
disorders
• Depression/anxiety
• Obesity/type II
diabetes
Systemic Effects of COPD
�Peptic ulceration
�Lung infections/lung cancer
�Weight loss/muscle wasting and
weakness
�Osteoporosis
�Depression
NOTE: If caused by the COPD, these could be
considered “secondary ” (RELATED) conditions.
COPD Signs & Symptoms
�Dyspnea
�Wheezing
�Cough
�Hypoxemia and rising CO2 levels
�Pulmonary hypertension that may
progress to right ventricular
hypertrophy and cor pulmonale
(right-sided heart failure)
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
6
Acute COPD Exacerbation
� Definition: Sustained worsening of symptoms from
patient’s usual condition; acute in onset
� Symptoms
� Increased shortness of breath
� Increased sputum production and/or increase in
purulence
� Increase cough
� Increased wheeze/chest tightness
� Decreased exercise tolerance
� Increased fatigue
� Altered mental statusNICE GUIDELINES 2004
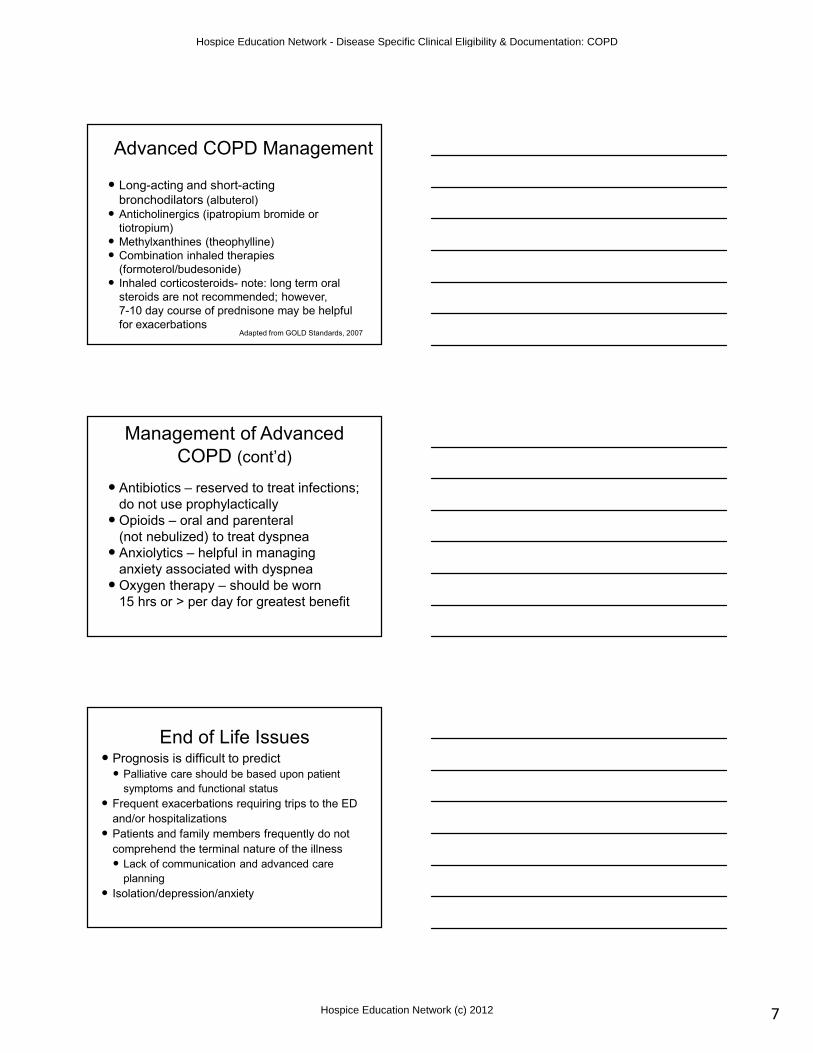
IV: Very SevereIII: SevereII: ModerateI: Mild
Therapy at Each Stage of COPD
• FEV1/FVC < 70%
• FEV1 > 80%
predicted
• FEV1/FVC < 70%
• 50% < FEV1 <
80%
predicted
• FEV1/FVC <
70%
• 30% < FEV1 <
50% predicted
• FEV1/FVC < 70%
• FEV1 < 30%
predicted
or FEV1 < 50%
predicted plus
chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccination
Add short-acting bronchodilator (when needed)
Add long term oxygenif chronic respiratory
failure. Consider
surgical treatments
Adapted from GOLD Guidelines.
http://www.goldcopd.com/Guidelineitem.asp?
l1=2&l2=1&intId=989
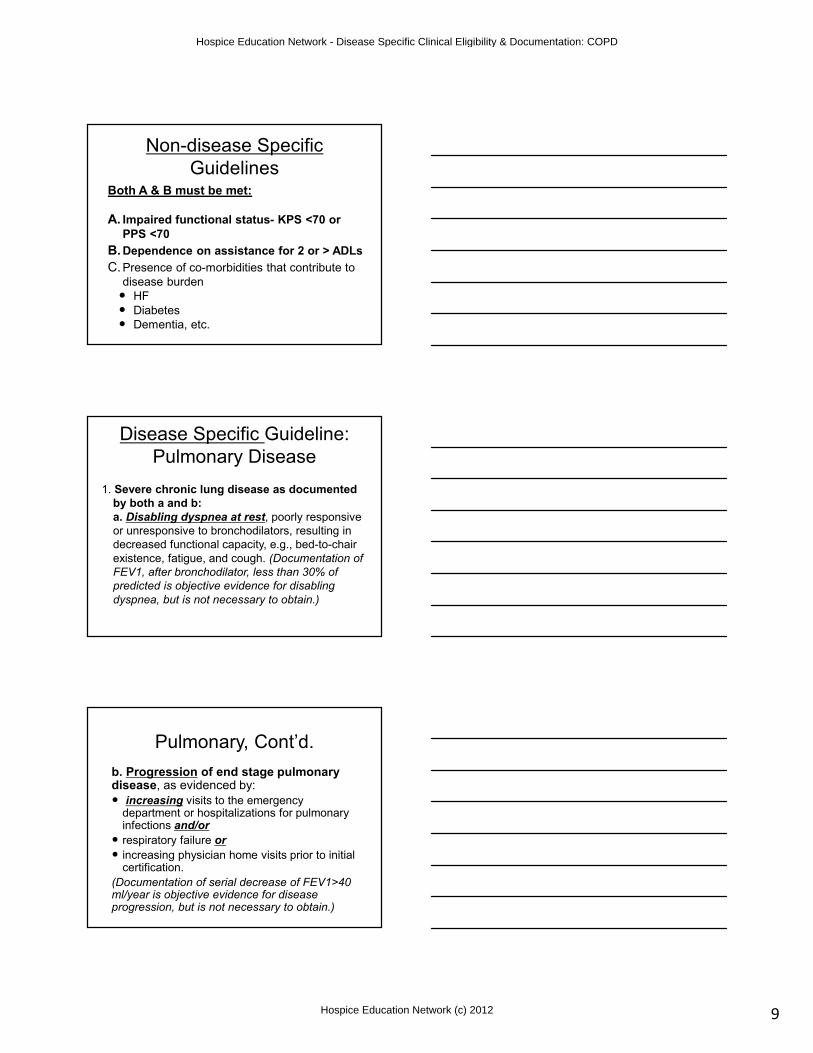
Management of COPD
Stage IV: Very Severe COPD
Characteristics Recommended
Treatment• FEV1/FVC < 70%
• FEV1 < 30%
predicted or FEV1 <
50% predicted plus
chronic respiratory
failure
• Short-acting bronchodilator as needed
• Regular treatment with one or more LA bronchodilators
• Inhaled glucocorticosteroidsif repeated exacerbations
• Treat complications
• Rehabilitation
• Long-term O2 therapy if respiratory failure
• Consider surgical options
Adapted from GOLD
Guidelines, 2007
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
7
Advanced COPD Management
� Long-acting and short-acting
bronchodilators (albuterol)
� Anticholinergics (ipatropium bromide or
tiotropium)
� Methylxanthines (theophylline)
� Combination inhaled therapies
(formoterol/budesonide)
� Inhaled corticosteroids- note: long term oral
steroids are not recommended; however,
7-10 day course of prednisone may be helpful
for exacerbationsAdapted from GOLD Standards, 2007
Management of Advanced
COPD (cont’d)
� Antibiotics – reserved to treat infections;
do not use prophylactically
� Opioids – oral and parenteral
(not nebulized) to treat dyspnea
� Anxiolytics – helpful in managing
anxiety associated with dyspnea
� Oxygen therapy – should be worn
15 hrs or > per day for greatest benefit
End of Life Issues� Prognosis is difficult to predict
� Palliative care should be based upon patient
symptoms and functional status
� Frequent exacerbations requiring trips to the ED
and/or hospitalizations
� Patients and family members frequently do not
comprehend the terminal nature of the illness
� Lack of communication and advanced care
planning
� Isolation/depression/anxiety
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
8
Signs that Patient Requires
Palliative Care
� FEV1 < 30% predicted
� History of 2 or more exacerbations in
past year
� Frequent hospitalizations
� Progressive shortening of intervals
between admissions
� Limited improvement after hospitalization
Supporting
Indicators
• Declining functional
status/homebound
• Presence of
co-morbidities such as
heart failure or diabetes
• On maximum therapy
and dependence on
oxygen
LCD Guidelines for
Hospice Eligibility and
Recertification
for COPD
NGS LCD Number L25678
CGS LCD Number L32015
NHIC LCD Number L29881
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
9
Non-disease Specific
GuidelinesBoth A & B must be met:
A. Impaired functional status- KPS <70 or
PPS <70
B. Dependence on assistance for 2 or > ADLs
C. Presence of co-morbidities that contribute to
disease burden
� HF
� Diabetes
� Dementia, etc.
Disease Specific Guideline:
Pulmonary Disease
1. Severe chronic lung disease as documented
by both a and b:
a. Disabling dyspnea at rest, poorly responsive
or unresponsive to bronchodilators, resulting in
decreased functional capacity, e.g., bed-to-chair
existence, fatigue, and cough. (Documentation of
FEV1, after bronchodilator, less than 30% of
predicted is objective evidence for disabling
dyspnea, but is not necessary to obtain.)
Pulmonary, Cont’d.
b. Progression of end stage pulmonary disease, as evidenced by:
� increasing visits to the emergency department or hospitalizations for pulmonary infections and/or
� respiratory failure or
� increasing physician home visits prior to initial certification.
(Documentation of serial decrease of FEV1>40 ml/year is objective evidence for disease progression, but is not necessary to obtain.)
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
10
Pulmonary, Cont’d.
2. Hypoxemia at rest on room air as evidenced by:
� pO2 less than or equal to 55 mmHg; or
� oxygen saturation less than or equal to 88%;
or
� hypercapnia as evidenced by pCO2 greater than or equal to 50mmHg.
(These values may be obtained from recent [within 3 months] hospital records.)
Pulmonary (supportive)
3. Cor pulmonale (right heart failure)
secondary to pulmonary disease (e.g., not
secondary to left heart disease or valve
disease)
4. Unintentional progressive weight loss of
greater than 10% of body weight over the
preceding 6 months
5. Resting tachycardia >100/min
Establishing, Evaluating,
and Explaining
Eligibility Based upon Burden of Illness in COPD
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
11
Assessing and Documenting
Disease Burden in COPD
� Sustained tachypnea (RR>30
breaths/min)
� Sustained tachycardia (RR>100
beats/min)
� O2 saturation <88% on room air or
patient’s usual supplemental oxygen
� Hypotension <100mm Hg or 20% lower
than patient’s usual
� Severe impairment of ADLs
ADL Documentation
Describe:
�How much caregiver support?
�None
�Minimal
�Moderate
�Total
�Time-to-completion of tasks
Assessing and Documenting
Disease Burden in COPD
� Inability to speak in full sentences
� Sustained use of accessory muscles of
respiration at rest
� Decreased ability to eat or sleep due to
respiratory distress
� Repeated lung infections/courses of
antibiotic therapy
� Hemoptysis/increased sputum
production/cough
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
12
Assessing and Documenting
Disease Burden in COPD
� Sustained increase in
patient’s usual degree of
dyspnea
� Medication changes-
addition or titration of
opioids, anxiolytics, etc.
� Altered mental status-
lethargy, confusion
� Increased caregiver
stress/burden
Documentation example
“Patient is now completely bed-bound and is having new episodes of urinary incontinence. Caregiver providing maximal assist with all ADLs. Pt now severely dyspneic with minimal activity, including trying to speak. Sleeping on avg18/24 hrs per day. Po intake reduced due to coughing/choking episodes. Using MSO4 q 4 ATC with moderate relief.”
Conclusion
� COPD is the 4th leading non-cancer diagnosis in
hospice
� Although irreversible and progressive, COPD
prognosis is difficult to predict
� Hospice eligibility based on pulmonary function
(FEV1), degree of hypoxemia, dyspnea
unresponsive to therapy, functional status, recent
ED/hospitalization/physician visits for recurrent
infections, or respiratory failure
� Initial and ongoing comprehensive patient
assessment with documentation is necessary for
enrollment and recertification
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012
13
References
1. Jemal, Ward, Hao, Thun. Trends in the leading
causes of death in the United States, 1970-2002.
JAMA. 2006, 295(4): 393-394.
2. Global Initiative for Chronic Obstructive Lung
Disease (GOLD). Global Strategy for the Diagnosis,
Management, and Prevention of Chronic Obstructive
Pulmonary Disease (2007). www.goldcopd.com
3. Poole, PJ, Veale, AG, Black, PN. The effect of
sustained-release morphine on breathlessness and
quality of life in severe chronic obstructive
pulmonary disease. Am J Respir Crit Care Med
1998: 157: 1877-80.
Course Evaluation
& Post Test
Thank you for viewing this course on the
Hospice Education Network
The course evaluation and post test are
available from your course catalog page
Thank You!
Terri Maxwell PhD, APRNVP, Strategic Initiatives
Weatherbee Resources Inc. & Hospice Education Network
Hospice Education Network - Disease Specific Clinical Eligibility & Documentation: COPD
Hospice Education Network (c) 2012