Embed Size (px)
Citation preview

Couple-Based HIV Interventions: A Gender Specific Approach
Nabila El-BasselColumbia University
International AIDS Conference July 2012, Washington, DC

Presentation Will Cover:
• State of the science of couple-based behavioral HIV interventions from a recent systematic review (El-Bassel and Jiwatram, March, 2012)
• Lessons learned: advantages/benefits of couple modality and what makes it gender-specific
• Project Connect (New York) and Renaissance (Kazakhstan) for couples who use drugs

Women and HIV
• Worldwide, 80% of new HIV cases among women are transmitted heterosexually, usually from a steady partner (UNAIDS, 2010)
• In Sub-Saharan Africa, the majority of HIV transmissions occur among serodiscordant co-habiting or married couples (UNAIDS, 2012)
• Outside Sub-Saharan Africa, the majority of HIV transmissions among women occur from steady partners who inject drugs and the woman’s own intravenous drug use (UNAIDS, 2010)
i

HIV Prevention for Couples
Although most HIV infections occur in dyadic relationships (USAIDS, 2010), the majority of behavioral HIV prevention efforts for women:
• Target the women individually
• Rarely include the woman AND her partner together in the intervention

Couple-Based HIV Intervention Studies Globally (N=23)
Africa46%
(n=11)
U.S.37% (n=8)
Asia9% (n=2)
Multi-Country8% (n=2)

% of Studies, by Type
Biomedical17% (n=4)
Behavioral83% (n=19)

Couple-Based HIV Intervention Studies
Behavioral: Couple HIV Test-ing & Counseling (CHTC)
(n=8)
Behavioral: Couple-based HIV/STI Prevention (n=10)
Behavioral: Couple-based Adherence to ART (n=1)
Biomedical: ART (n=4)
% of studies, by type
0.348 0.435 0.043 0.174
3%
8%
13%
18%
23%
28%
33%
38%
43%

CHTC and AdherenceAuthors Publication Title and Journal
Couple HIV Testing and Counseling
Kamenga et al.AIDS, 1991
Evidence of marked sexual behavior change associated with low HIV-1 seroconversion in 149 married couples with discordant HIV-1 serostatus:
experience at an HIV counselling center in Zaire
Allen et al.BMJ, 1992
Effect of serotesting with counselling on condom use and seroconversion among HIV discordant couples in Africa
The Voluntary HIV-1 Counseling and Testing Efficacy Study Group - Coates et al.
The Lancet, 2000
Efficacy of voluntary HIV-1 counselling and testing inindividuals and couples in Kenya, Tanzania, and Trinidad: a randomised trial
Roth et al.International Journal of STD and AIDS, 2001
Sexual Practices of HIV discordant and concordant couples in Rwanda: effects of a testing and counselling programme for men
Allen et al.AIDS, 2003
Sexual behavior of HIV discordant couples after HIV counseling and testing
Farquhar et al.Journal of Acquired Immune Deficiency Syndrome, 2004
Antenatal Couple Counseling Increases Uptake of Interventions to Prevent HIV-1 Transmission
Mehendale et al.Journal of Acquired Immune Deficiency Syndrome, 2006
Low HIV-1 Incidence Among Married Serodiscordant Couples in Pune, India
Becker et al.AIDS Behavior, 2010
Comparing Couples and Individual Voluntary Counseling and Testing for HIV at Antenatal Clinics in Tanzania: A Randomized Trial
Couple-based Adherence to ART
Remien et al.AIDS, 2005
Couples-focused support to improve HIV medication adherence: a randomized controlled trial
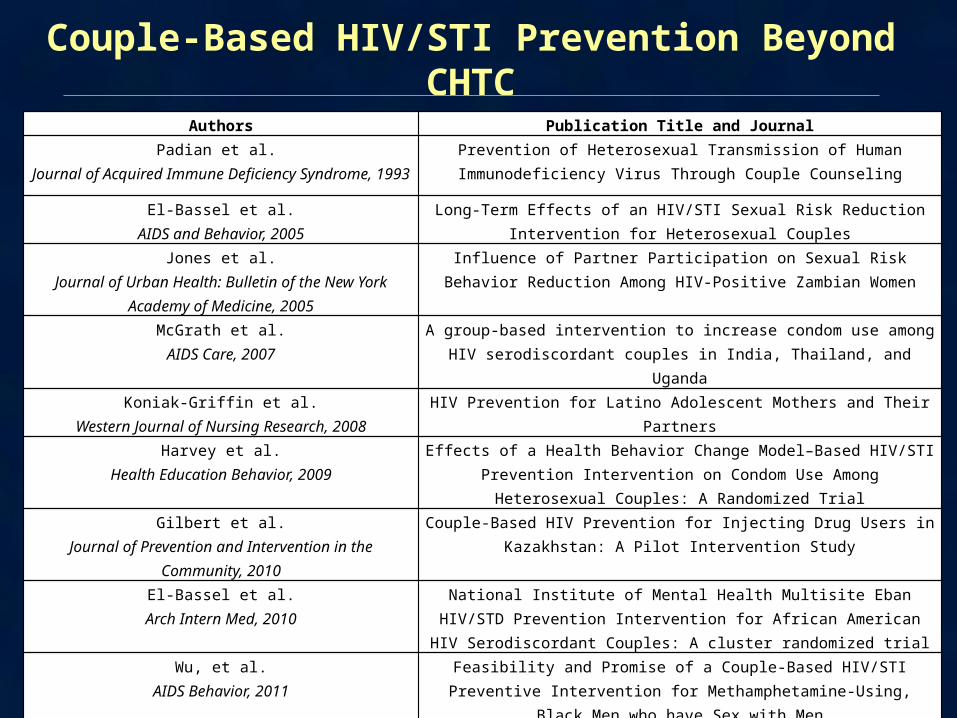
Couple-Based HIV/STI Prevention Beyond CHTC
Authors Publication Title and JournalPadian et al.
Journal of Acquired Immune Deficiency Syndrome, 1993Prevention of Heterosexual Transmission of Human Immunodeficiency Virus
Through Couple Counseling
El-Bassel et al.AIDS and Behavior, 2005
Long-Term Effects of an HIV/STI Sexual Risk Reduction Intervention for Heterosexual Couples
Jones et al.Journal of Urban Health: Bulletin of the New York Academy of
Medicine, 2005
Influence of Partner Participation on Sexual Risk Behavior Reduction Among HIV-Positive Zambian Women
McGrath et al.AIDS Care, 2007
A group-based intervention to increase condom use among HIV serodiscordant couples in India, Thailand, and Uganda
Koniak-Griffin et al.Western Journal of Nursing Research, 2008
HIV Prevention for Latino Adolescent Mothers and Their Partners
Harvey et al.Health Education Behavior, 2009
Effects of a Health Behavior Change Model–Based HIV/STI Prevention Intervention on Condom Use Among Heterosexual Couples: A Randomized Trial
Gilbert et al.Journal of Prevention and Intervention in the Community,
2010
Couple-Based HIV Prevention for Injecting Drug Users in Kazakhstan: A Pilot Intervention Study
El-Bassel et al.Arch Intern Med, 2010
National Institute of Mental Health Multisite Eban HIV/STD Prevention Intervention for African American HIV Serodiscordant Couples: A cluster
randomized trial
Wu, et al.AIDS Behavior, 2011
Feasibility and Promise of a Couple-Based HIV/STI Preventive Intervention for Methamphetamine-Using, Black Men who have Sex with Men
El-Bassel et al.Journal of Acquired Immune Deficiency Syndrome, 2011
Couple-Based HIV Prevention for Low-Income Drug Users From New York City: A Randomized Controlled Trial to Reduce Dual Risks

Biomedical
Authors Publication Title and Journal
Bunnell et al.AIDS, 2006
Changes in sexual behavior and risk of HIV transmission after antiretroviral therapy and prevention interventions in
rural Uganda
Celum et al. The New England Journal of Medicine,
2011
Acyclovir and Transmission of HIV-1from Persons Infected with HIV-1 and HSV-2
Cohen et al.The New England Journal of Medicine,
2011
Prevention of HIV-1 Infection with Early Antiretroviral Therapy
Reynolds et al.AIDS, 2011
HIV-1 transmission among HIV-1 discordant couples before and after the introduction of antiretroviral therapy

Couple-Based Studies, by Sexual Orientation
83%(n=19)
4% (n=1)
9%(n=2)
4% (n=1)
Heterosexual MSM Both Not Defined

Couple-Based HIV Intervention Studies, by Serostatus
Serodiscordant (n=13) Negative Concordant (n=3) Other (including at-risk, unaware, etc.) (n=7)
% of studies 0.565000000000004 0.13 0.304
5.0%
15.0%
25.0%
35.0%
45.0%
55.0%

Advantages of HIV Couple-Based Behavioral Intervention
Bringing the couple together for behavioral HIV prevention sessions sends the message that:
• Both members of the dyad can bring HIV to the relationship
• Both are responsible for HIV risk reduction
Bringing the couple together:
• Increases male involvement and encourages male responsibility for risk reduction
• Increases the opportunity to integrate HIV, STI, and reproductive health issues

Advantages of Bringing Couples Together for a Behavioral Intervention
Provides a safe, non-judgmental, and supportive environment with a third party in order to:
• Discuss gender roles and expectations around safer sex, condom use, and reproductive heath
• Disclose and discuss sensitive issues:
– Sexual concurrency, survival sex, bisexuality
– Disclosure of HIV and STIs
– Fear and experience of IPV, contexts that lead to IPV, and explore and learn ways to deal with them
Advantages of HIV Couple-Based Behavioral Intervention
Provides a safe environment to:
• Learn ways to strengthen and improve the couple’s relationship
• Learn and practice communication skills
• Promote the use of female condoms
• Learn drug risk reduction skills together, learn to help each other cope with drug overdose in order to save each other’s life

Findings from CHTC Couple-Based Studies
• Promotes the couple to disclose their HIV status and encourages support for each other if one or both are HIV positive
• Increases uptake and adherence to ART
• Reduces HIV infection rates and risk sexual behavior
Recent systematic review (El-Bassel and Jiwatram, March, 2012)
Findings: Couple-Based
Behavioral Studies Beyond CHTC
• Increased condom use and reduced sexual and drug risks (e.g., sharing syringes and injection equipment)
• Increased communication, problem solving, help-seeking skills and promoted joint responsibility, and better informed reproductive health decisions regarding conception
• Reduced sexual and physical IPV
• Improved testing and access to care
• None of the behavioral studies demonstrated a reduced incidence of HIV/STI because of lack of statistical power
Recent systematic review (El-Bassel and Jiwatram, March, 2012)

Project Connect II: Aims
• Efficacy trial on HIV prevention with couples who use drugs to reduce sexual and drug risk behavior (NIDA funded)
• HIV prevention intervention is more efficacious in reducing sexual and drug risks when both members of the couple receive the intervention together than when one member receives it alone
El-Bassel et al. JAIDS, 2011

Project Connect II: DesignScreened 1616
Individuals 865 Eligible Individuals (54%)
Couple HIV Risk Reduction
7 Sessions (95)
Individual HIV Risk Reduction
7 Sessions (92)
Couple Wellness Promotion
7 Sessions (95)
• Immediately Post-Treatment (IPT)
• 6-Month Follow-Up• 12-Month Follow-Up
• Immediately Post-Treatment (IPT)
• 6-Month Follow-Up• 12-Month Follow-Up
Baseline346 Couples (80%)
Randomization282 Couples (82%)
• Immediately Post-Treatment (IPT)
• 6-Month Follow-Up• 12-Month Follow-Up

SociodemographicsTotal (n = 564) Women (n = 282) Men (n = 282)
Mean age 36 yrs. 35 yrs. 38 yrs.
African American 49% 45% 53%
Latino/a 26% 25% 28%
Never married 45% 45% 45%
Married 43% 43% 43%
High school or GED 63% 56% 71%
Employed 19% 15% 23%
Homeless 26% 27% 25%
In prison or jail (past 90 days)
21% 15% 27%
Mean monthly income (SD) $389 ($489) $404 ($539) $374 ($433)
Major Hypothesis
• To determine whether the relationship-based prevention intervention is more efficacious when both members of the couple receive the intervention together than when one member receives it alone
vs.Couple
Wellness Promotion
Randomization
Couple Risk Reduction
Individual Risk Reduction

Multilevel Poisson and Logistic Regression Models
Number of unprotected acts of intercourse (Incidence rate ratio and 95% confidence intervals at 12-month follow-up)
Poisson regression
With Study Partner
Modality (Couple Risk vs. Individual Risk)0.71 *
[0.51, 0.97]
Across All Partners
Modality (Couple Risk vs. Individual Risk)0.74 *
[0.56, 0.99]
Shared needles and works (Odds ratio and 95% confidence intervals at 12-month follow-up)
Logistic regression
Modality (Couple Risk vs. Individual Risk) 0.28 †
[0.07, 1.03]
† p<0.1; * p<0.05; ** p<0.01
Project Renaissance:Almaty, Kazakhstan

Central Asia
Source: Russia-Ukraine-Travel.com

Project Renaissance
• RCT to test an integrated overdose and HIV prevention delivered to couples (NIDA funded, underway, to be completed October 2012)
Outcomes:
• Reduction of sexual and drug risk behavior, reduce incidence of overdose, of HIV and other STIs
• Improve access to harm reduction programs and HIV treatment and care

Project RenaissanceScreened
966 Individuals
Couple HIV Risk Reduction and Overdose 5 Sessions (151 Couples)
Couple Wellness Promotion and Overdose 5 Sessions (141 Couples)
• Immediately Post-Treatment (IPT)
• 6-Month Follow-Up
• 12-Month Follow-Up
• Immediately Post-Treatment (IPT)
• 6-Month Follow-Up
• 12-Month Follow-Up
Baseline732 Individuals (367 Couples)
Randomization 300 Couples (600)
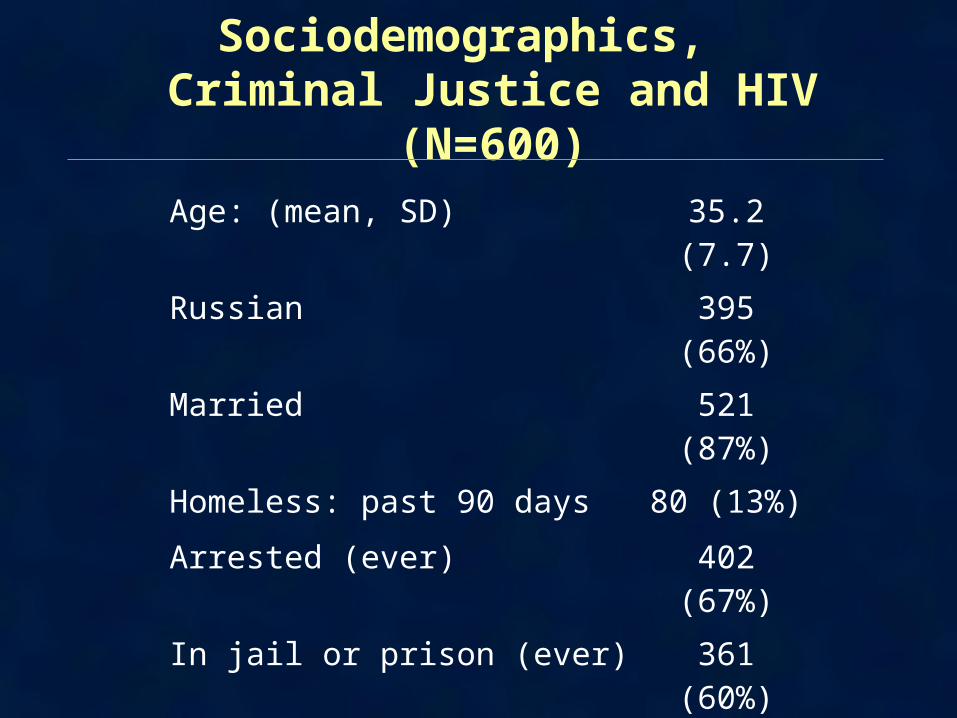
Sociodemographics, Criminal Justice and HIV (N=600)
Age: (mean, SD) 35.2 (7.7)
Russian 395 (66%)
Married 521 (87%)
Homeless: past 90 days 80 (13%)
Arrested (ever) 402 (67%)
In jail or prison (ever) 361 (60%)
Drug-related offense (ever) 340 (57%)
HIV positive 156 (26%)
HCV positive 461 (77%)

Partner Abuse
Female Male
Ever experienced sexual IPV 37% 15%
Experienced sexual IPV (past 6 months)
13% 7%
Ever experienced physical IPV 55% 31%
Experienced physical IPV (past 6 months)
15% 10%

Multiple Regression Models for Sexual Risk Reduction
Number of unprotected vaginal sex acts with study partner (Incidence rate ratio and 95% confidence intervals at 6-month follow-up)
Modality (Couple Risk vs. Health Promotion)0.49*
[0.28, 0.84)
Proportion of protected vaginal sex acts with study partner (proportion at 6-month follow-up)
Modality (Couple Risk vs. Individual Risk)0.18*
[0.11, 0.25]
Consistent condom use with study partner (past 90 days) at 6-month follow-up (Odds ratio and 95% confidence interval)
Modality (Couple Risk vs. Health Promotion)3.03*
[1.51, 6. 09)
* p<0.05; ** p<0.01

Overdose Rates in Past 6 Months
Baseline 6 Months0%
5%
10%
15%
20%
25%
18%
8%
**p<0.05

Conclusions
Although the number of couple-based HIV behavioral studies is small, evidence for their effectiveness is strong in:
• Increasing access to HIV testing and ART
• Reducing sexual and drug risk transmission, and increasing condom use
• Improving communication skills and promoting a healthy relationship
• Reducing sexual and physical IPV among couples

Conclusions
• Scaling up couple-based HIV behavioral interventions is important
• Even though the FDA has approved over-the-counter HT, CHTC is still needed. Couples may need to address negative reactions to disclosure of HIV and risk reduction strategies
• Behavioral HIV couple-based interventions should be integrated with biomedical interventions such as ART, PREP

Acknowledgments
Louisa Gilbert (PhD) Columbia University
Assel Terlikbayeva (MD, MSW) Global Health Research Center
Susan Witte (PhD) Columbia University
Elwin Wu (PhD) Columbia University
Mingway Chang (PhD) Columbia University
Robert Remien (PhD) Columbia University
Sholpan Primbetova (MD, MSW) Global Health Research Center
Chris Beyer (MD, MPH) John Hopkins University
National Institute on Drug Abuse (NIDA)

Team in Kazakhstan