Embed Size (px)
Citation preview

Cost-effectiveness analysis and policy choices:investing in health systemsC.J.L. Murray,1 J. Kreuser,2 & W. Whang3
The role of health systems infrastructure in studies of cost-effectiveness analysis and health resourceallocation is discussed, and previous health sector cost-effectiveness analyses are cited. Two sub-stantial difficulties concerning the nature of health system costs and the policy choices are presented.First, the issue of health system infrastructure can be addressed by use of computer models such asthe Health Resource Allocation Model (HRAM) developed at Harvard, which integrates cost-effective-ness and burden of disease data. It was found that a model which allows for expansion in health infra-structure yields nearly 40% more total DALYs for a hypothetical sub-Saharan African country than amodel which neglects infrastructure expansion. Widespread use of cost-effectiveness databases forresource allocations in the health sector will require that cost-effectiveness analyses shift from reportingcosts to reporting production functions. Second, three distinct policy questions can be treated usingthese tools, each necessitating its own inputs and constraints: allocations when given a fixed budgetand health infrastructure, or when given resources for marginal expansion, or when given a politicallyconstrained situation of expanding resources. Confusion concerning which question is being addressedmust be avoided through development of a consistent and rigorous approach to using cost-effective-ness data for informing resource allocations.
IntroductionCost-effectiveness analysis of health sector interven-tions was first applied in the 1960s based on meth-ods developed to analyse military investments (1).Since 1970, the number of published studies usingcost-effectiveness analysis has been steadily rising,reflecting a growing concern for the appropriate useof scarce health sector resources (2). Initially, mostcost-effectiveness studies reported results using indi-cators such as the cost per case diagnosed and treat-ed of a particular disease or the cost per fully immu-nized child. These studies using outcome or benefitmeasures that are very disease or context specifichave been gradually replaced by studies using moregeneral measures of health outcome. With morewidespread reporting of results in terms of costs perquality-adjusted life year (QALY) or other generalhealth measure, comparisons of the cost-effectivenessof interventions targeting different health problems
I Associate Professor of International Health Economics, HarvardCenter for Population and Development Studies, 9 Bow Street,Cambridge, MA 02138, USA. Requests for reprints should besent to this author.2 Information Officer, Information Engineering Unit, Organizationand Business Practices Department, The World Bank, WashingtonDC, USA.3 Columbia University College of Physicians and Surgeons, NewYork NY, USA.
Reprint No. 5513
have become possible. League tables of the cost-effectiveness of different interventions are a naturalconsequence (3-8).
Two landmark policy analyses have provided animpetus to using cost-effectiveness to compare awide range of health interventions. These exercisesprovide enough information so that cost-effective-ness analysis for the first time can be used to informresource allocations across the entire health sector.First, the Oregon Health Services Commission (9-18)examined 714 condition-treatment pairs (called inter-ventions in the rest of the following discussion) andcalculated the cost per QALY. The valuation of out-comes from medical intervention and the rankingsfrom cost-effectiveness analysis were then subject toextensive public review through a series of townmeetings. The rank list of interventions from thisprocess can then be used for selecting the interven-tions that Medicaid will finance in the State, whichplans to fund (in order of the rank list) each interven-tion maximally until the budget runs out. This sector-al application of cost-effectiveness is now beingimplemented (18). The second major policy reviewwas the Health Sector Priorities Review undertakenby the World Bank from 1987 to 1993 (7). Twenty-six major health problems of developing countrieswere reviewed by teams of economists, public healthspecialists and epidemiologists. The cost-effectivenessof more than 50 specific health interventions wereevaluated using a standard methodology for costs
Bulletin of the World Health Organization, 1994, 72 (4): 663-674 © World Health Organization 1994 663

C.J.L. Murray et al.
and benefits.a These databases provide useful infor-mation on cost-effectiveness which will help deter-mine resource allocations across the entire healthsector.
Building largely on the Health Sector PrioritiesReview, the World Bank has promoted in the Worlddevelopment report 1993: investing in health (WDR)the concept of using cost-effectiveness of health sec-tor interventions and the burden of disease of healthproblems to develop essential packages of clinicaland preventive care (23). The WDR also proposesthat cost-effectiveness analysis be used to determinethe package of services covered by insuranceschemes and to inform health research priorities. Inthis issue of the Bulletin, Bobadilla et al. (24) pro-vide details on the method and rationale for selec-tion and of interventions and their quantities in theproposed package. In brief, estimates of the cur-rent burden of disease are combined with a cost-effectiveness rank list of interventions, to derivepackages of services that, for a given budget, willpurchase the largest improvement in health asmeasured by DALYs (disability-adjusted life years).Given the considerable attention gamered by theWDR, it is important to examine carefully the impli-cations of this new and more extensive application ofcost-effectiveness analysis.
Limitations of sectoral cost-effectiveness
In recent years, the theoretical basis for using cost-effectiveness analysis to guide health sector resourceallocations has been discussed: the validity of DALYor QALY maximization as a goal for the health sec-tor (25-30), the nature of individual preferences forhealth states and how these preferences are incorpo-rated into QALYs (31-35), the importance of margi-nal costs that change as a function of output (36, 37),the effect of intervention-specific fixed costs (36,38), and the sensitivity of conclusions to abstractconcepts such as discounting (39-51). These techni-cal issues are important and likely to be vigorouslydebated for many years but probably do not have aprofound effect on the sectoral application of cost-effectiveness to policy choice, although furtherresearch may indicate important modifications andrefinements are needed in the methods.
Two more general and potentially importantcriticisms are concemed with the focus of cost-effec-tiveness analysis. First, cost-effectiveness analysis ofhealth interventions, which are more often than not
a To make the results of the Health Sector Priorities Reviewconsistent with the Global Burden of Disease, benefits weremeasured using disability-adjusted life years. See Murray et al.(19-22) for details of the method of calculating benefits.
disease specific, tends to neglect the role of thehealth system in delivering these interventions.There are no explicit analyses of the cost-effective-ness of improving the physical or human infrastruc-ture of the health system, which provide for directcomparisons between investing in the deliverysystem and purchasing more specific interventionsdelivered by the health system. Some may be con-cemed that the intervention focus of cost-effective-ness analysis may shift the focus of policy debatefrom who delivers health services to satisfying spe-cific targets or goals for particular activities. In theextreme, some accuse cost-effectiveness analysis offostering a vertical approach to disease control asopposed to the horizontal approach embodied in theprimary health care movement. Second, there is apotential for considerable confusion, including in theWDR, on the policy choice that should be informedby cost-effectiveness analysis. For example, shouldcost-effectiveness analysis be used to suggest thereallocation of resources between programmes thatwill lead to the greatest improvement in health orshould it only be used to suggest how marginalincreases in health sector resources could best beallocated to improve health?
In this paper, we present in brief a proposedmethod by which the cost-effectiveness of investingin the physical and human infrastructure of thehealth system can be evaluated. A resource alloca-tion model, the technical details of which aredescribed elsewhere (36), is illustrated with an appli-cation to sub-Saharan Africa. The model is then usedto address the second issue of the range of policyquestions that can be addressed with cost-effective-ness analysis. Finally, some implications for futurecost-effectiveness studies are highlighted.
Cost-effectiveness of investing inthe health systemThe accepted standard for reporting the results ofcost-effectiveness studies in the literature and un-published reports is to provide information on theaverage cost per unit of health output (such as aDALY) at one level of production. Average costequals the sum of general or infrastructure fixedcosts, programme-specific fixed costs, and vari-able costs divided by total output. Arbitrary rules arepromulgated to allocate the general infrastructurefixed costs, such as the costs of hospitals and healthcentres to specific interventions undertaken in thosefacilities. These arbitrary divisions of joint produc-tion costs are usually based on some proxy measureof activity, such as staff hours, bed-days, or square-feet occupied. The treatment of the costs of maintain-
664 WHO Bulletin OMS. Vol 72 1994

Cost-effectiveness analysis and health sector policy choices
ing the physical and human infrastructure of thehealth system in this arbitrary manner leads to twomajor problems with the cost-effectiveness approachwhen applied to sectoral decisions.
First, the average cost-list approach used in theWDR (23) ignores existing infrastructure and implic-itly assumes that hospitals and health centres can bebuilt in infinitely divisible quantities.b The averagecost of an intervention includes a component due tothe general fixed costs divided by the volume of out-put at the time of the assessment. Allocating resourc-es according to average unit costs implies that frac-tions of facilities, e.g., 2% of a health centre, can bebuilt as required. Concomitantly, existing facilitiescan be used in shares less than one while the costsfor the rest of the facility are not incurred. Aresource allocation based on an average cost list mayinclude only the costs of running 45% of district hos-pitals, ignoring the fact that hospitals and health cen-tres come in indivisible units. For example, the pack-age of essential clinical services proposed by theWorld Bank for low-income countries does notinclude all the costs of maintaining and operating theexisting referral and district hospitals. Even the frac-tional costs of facilities depend on operating eachnew fraction at the same level of output as wasincluded in the analysis. Otherwise the general fixedcosts divided by output, which figures in averagecost, would be different.
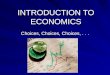
Second, even if shares of facilities could be builtor closed at will, the joint costing rules artifactuallypenalize interventions that are more technically effi-cient. Fig. 1 shows a production function for a healthcentre that undertakes only two activities: the expand-ed programme of immunization (EPI) and prenatalcare. The area within the curve shows all possiblecombinations of the two activities, given the currentstaffing levels and operating budget for the healthcentre. The production possibilities frontier which isthe curved line shows what could be achieved withmaximal technical efficiency for both activities.
Many health centres operate far from theproduction possibilities frontier. Consider a healthcentre at point A in Fig. 1; joint costing rules wouldallocate equal shares of the health centre's overheadcosts to EPI and prenatal care. Imagine a newregional manager who works to increase the efficien-cy of EPI such that at no extra cost to the healthcentre it now operates at point B. Joint costing ruleswould now attribute a much higher share of the over-
b While the cost-effectiveness analysis methods used in devel-oping the packages of care for the WDR do not explicitlyaddress the health system, the WDR devotes the whole ofChapter 6 to the need for developing health systems.
Fig. 1. Production function for hypothetical health cen-tre undertaking only two activities-prenatal care andexpanded programme on immunization; misallocationof overhead costs through use of joint-costing rules.Point A represents a typical level of output and point B theincreased level achieved through improved management.
co
0 Expanded programme on immunization
head costs to EPI than before. Clearly, fixed costshave not increased; only productivity has increased.The joint costing approach to calculating averagecosts entails a very real risk of penalizing with high-er estimated unit costs those programmes that aremore efficient.
To examine investments in human and physicalhealth infrastructure in a cost-effectiveness frame-work, a more sophisticated approach to resourceallocation questions is required. Correa (52) and Tor-rance et al. (38) developed hypothetical planningmodels to choose health maximizing mixes of inter-ventions under various constraints. Torrance et al.(38) discussed the possibility of designing a resourceallocation model that would directly incorporate thelimits on service delivery imposed by the currenthealth system infrastructure and the possibility ofimproving the health system. At least four optimiza-tion models for the health sector applied to specificinterventions that maximize a measure of health stat-us given a budget constraint and a variety of possibleinterventions have been developed (37, 53-55).None of these applications, however, attempted toincorporate the health system into the modellingexercise.
Health Resources AllocationModel (HRAM)In order to deal with these problems, we have devel-oped at Harvard an optimization model for the healthsector based on the burden of disease, the cost-effec-tiveness of available health interventions, and theavailable health system infrastructure. Our model hasbeen developed in the General Algebraic ModelingSystem (GAMS), a computer system which facili-
WHO Bulletin OMS. Vol 72 1994 665

C.J.L. Murray et al.
tates the development of algebraic models in days,which previously took months (56). GAMS has beenextensively used in other fields such as agriculture,education and industry to deal with complex non-linear optimization problems. Our model, HRAM,has also been designed to address technical problemsrelated to intervention fixed costs, rising marginalcosts, and regional heterogeneity. The details on thelatter and the technical specifications of the modelare provided elsewhere (36) and are not discussed inthis paper in detail. The following discussion de-scribes the general strategy used to incorporate thehealth system into a cost-effectiveness framework.
In order to put the appraisal of infrastructure incost-effectiveness terms, we have defined severalbudget constraints that include interchangeable dol-lars and a series of constraints reflecting the currentcapacity of the health system to deliver various typesof services. While there is flexibility in the design ofthe model to specify various types of budget con-straints, we have so far included constraints for ser-vices delivered at referral hospitals, district hospitalsand health centres. Given current facilities and staff-ing levels, the Ministry of Health begins with a con-straint on the volume of services it can providethrough referral hospitals, district hospitals andhealth centres. For referral and district hospitals, wehave used bed-days as the unit of service delivery,and for health centres we have used patient-contactequivalents.
Each intervention or activity may consumereferral hospital bed-days, district hospital bed-daysor health centre contacts in addition to interchange-able dollars. In other words, the use of the generalhealth system infrastructure is captured in terms ofunits of service rather than using arbitrary joint cost-ing rules. Table 1 provides examples of productionfunctions for several health interventions. In choos-ing an optimal allocation of health resources acrossactivities, when the available budget of district hos-pital bed-days is exhausted, no further interventionsusing district hospitals can be bought. The same lim-itation would apply to referral hospital bed-days andhealth centre contacts. However, the govemmentmay choose to build new referral hospitals, districthospitals or health centres in order to relax the ser-vice constraint. In addition to the set of interventionsincluded in the model, three more are added: con-struction and staffing of a referral hospital, districthospital or health centre. For health centres, we havealso included a geographical access constraint. It isnot sufficient to have an adequate total number ofhealth centre contacts for the population; health cen-tres must be positioned close enough to the commu-nity so that they can use them. In the simulations forsub-Saharan Africa, expanding geographical access
to health centres, particularly in remote areas, is amajor force driving the expansion of infrastructure inan optimal resource allocation. While not included sofar, geographical access constraints could also beadded for district hospitals.
At each budget level, the resource allocationmodel searches to see if the total output of thesystem in terms of DALYs avoided could be in-creased by using some resources to expand thehealth system rather than spending it on particularactivities delivered with the current health infrastruc-ture. In other words, the ability of computers toundertake repetitive calculations at high speed isused to test if the total output of the health sector interms of DALYs would be higher or lower byimproving the health system. Improvements in thehealth system can be undertaken in this model bybuilding, staffing and operating new referral hospi-tals, district hospitals or clinics.c In this framework,infrastructure investments can be evaluated in termsof the increase in the number of DALYs or equiva-lent measure of health status.
As one purchases an intervention such as meas-les immunization at the point where all children areimmunized, the marginal cost per DALY reachesinfinity because no more health benefits are gainedby expanding coverage beyond 100%. While techni-cally correct in micro-economic jargon, it is a cum-bersome approach to capturing the practical limits ofeach intervention. More intuitive is to constrain thepurchase of each intervention by the total amount ofDALYs that can be addressed with a particular inter-vention in a particular community. The link betweenthe burden of disease or the total number of DALYslost due to a particular health problem and cost-effectiveness is thus established. The example of themodel, which is described below, makes use of theGlobal Burden of Disease study results (19) for sub-Saharan Africa. The estimates of the current burdenof disease had to be modified to remove the impactof currently financed health interventions on themeasured burden of disease.
To explore the use of such an optimizationmodel, we have used the World Bank's Health Sec-tor Priorities Review database on the cost-effective-ness of some 50 interventions (7), the same databaseutilized by Bobadilla et al. (24). Each estimate of
c In this version of the model, we are able to build new infra-structure and use it in the same time period. The costs of open-ing and operating new units of infrastructure are the annualoperating fixed costs plus the equivalent annual capital cost. Asthe model is not a multi-period model, we do not take intoaccount the necessary time lag between the decision to improvethe physical or human infrastructure of the health system and itsimplementation.
666 WHO Bulletin OMS. Vol 72 1994

Cost-effectiveness analysis and health sector policy choices
Table 1: Data for the Health Resource Allocation Model for five interventionsPer DALY
Programme- Marginal Referral District Healthspecific fixed cost func- hospital hospital centre
Intervention Segmenta costs (US $) tion (US $) (bed-days) (bed-days) (contacts)
ARI screening 0 40 000 24.23 0 0.20 4.001 27.262 30.293 33.324 36.35
Poliomyelitis immunization 0 60 000 9.17 0 0 5.521 14.662 18.333 36.664 183.30
School-based 0 100 000 4.79 0 0 0anti-helminthic 1 4.79chemoprophylaxis 2 5.99
3 7.194 7.19
Short-course chemotherapy 0 53 000 1.71 0 3.85 0for sputum smear-positive 1 2.74tuberculosis 2 3.42
3 6.844 34.20
Tetanus referral 0 200 000 24.08 2.29 0 01 32.102 40.133 48.164 56.18
a To approximate the increasing marginal cost, the nonlinear marginal cost curve for each intervention within a region is broken up intofive linear segments numbered from 0 to 4.
cost-effectiveness was reviewed and modified toincrease the comparability across interventions.Despite our attempts to unearth details, frequentlyonly average cost results are reported in the literatureor reports on cost-effectiveness. Where necessary,expert judgement was used to develop the interventionproduction functions and form of the marginal costcurve, examples of which are provided in Table 1.d
The model was run for a hypothetical sub-Saha-ran African country with a population of 10 millionand a GDP per capita of $340, using the regionalGBD results adjusted to the total population to deter-mine the DALY limits for each disease. A digressionon the burden of disease is necessary. The results ofthe Global Burden of Disease study provide an esti-mate of the current burden of disease. Current or
d Table 1 provides a stepped marginal cost function for fiveinterventions. For convenience, we divided non-linear marginalcost functions into five linear steps or segments which are sum-marized in the Table.
measured burden incorporates the impact of current-ly financed health interventions; for example, if mea-sles immunization coverage is 70%, then a signifi-cant share of the burden of measles has already beenavoided. There are three levels of the burden of dis-ease relevant to this discussion of resource alloca-tion: first, the current burden of disease; second, theburden of disease that would be present if currentlyfinanced health interventions were stopped; andthird, the lowest achievable burden given a technicaland allocative efficiency within a budget constraint.The resource allocation model used as an input esti-mated the burden in the absence of currently fi-nanced health interventions in order to calculate thelowest achievable burden of disease for a given budget.
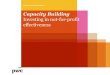
Fig. 2 shows the expansion path for the optimalallocation of health resources to maximize DALYsaverted at each budget level. For reference, currentexpenditure in sub-Saharan Africa excluding SouthAfrica is US$ 14 per capita. The equivalent annualcapital cost of the existing health infrastructure andthe fixed operating costs of the health system are
WHO Bulletin OMS. Vol 72 1994 667

C.J.L. Murray et al.
Fig. 2. DALY retrieval expansion path for sub-SaharanAfrica.
3000
o 2500'as
2000
15001. 75 2.5 3.25 4 4.75
Spending (% of GDP)5.5 6.25
US$ 3.27 per capita. This health sector productionfunction indicates that with increasing expenditurethe marginal cost of each DALY purchased increasesrapidly. For all budget ranges included, the marginalcost per DALY is higher than average cost. Table 2shows the number of new referral hospitals, districthospitals and health centres bought at three budgetlevels. Even at current levels of health expenditure,nearly 25% of the budget should be spent on expand-ing the health system. The remainder should be spenton the set of interventions listed. The Table also pro-vides the utilization rates of the three types of facil-ities modelled at each budget level. Referral hospitalbed-occupancy is less than 1%. The implication isthat there is excess referral hospital capacity but ashortage of district hospital capacity. If closure ordown-sizing of referral hospitals were politically fea-sible, this desirable option could be added as anadditional intervention in the model.
Table 3 shows the allocation to specific inter-ventions at three budget levels. Some highlights areworth discussing. Comparison with the WDR's $12per capita package for low-income countries is diffi-cult, as their package is based on a marginal increaseof $12 per capita, given current expenditures. At cur-rent budget levels, the most important interventionsby expenditure are screening and treatment of acuterespiratory infections (ARI), malaria control, tuber-culosis chemotherapy, measles immunization, oralrehydration therapy, breast-feeding, tetanus immu-
nization, and hygiene promotion. With increasesover current budget levels, the major gainers arechemotherapy for sputum smear-negative tuberculo-sis cases, oral rehydration therapy, malaria controland hygiene promotion.
Fig. 2 shows two expansion paths. The top lineis the expansion path for the complete model. Thesecond line is the expansion path when the optionsof adding infrastructure are removed from the model.Simple inspection shows that expanding the infra-structure is a tremendously important component ofhealth improvement. At current expenditure levels insub-Saharan Africa, expanding the health systemproduces nearly 40% more total DALYs.
Policy choice and sectoral cost-effectivenessHaving illustrated a model that incorporates healthsystem investment choice into a cost-effectivenessframework, we can return to the nature of policyquestions that can be treated with these analyticaltools. Three distinct policy questions using burden ofdisease and cost-effectiveness results can be framed.(1) Ground-zero. Given a fixed budget and healthinfrastructure, how can non-fixed resources be spentso as to maximally reduce the burden of disease?(2) Marginal expansion. Given an existing healthinfrastructure and a set of currently financed activ-ities, none of which can be changed, how best canmarginal increases in the health sector resources bespent so as to maximally reduce the burden of dis-ease?(3) Politically constrained ground-zero. Given anexisting health infrastructure, for political or otherreasons there may be a set of services or activitiesthat are deemed to be 'protected' from changes inbudget and a set of other services or activities thatcould be expanded or contracted. For a fixed healthsector budget, how can health resources be reallocat-ed to maximally reduce the burden of disease with-out reducing the resources allocated to 'protected'activities?
Table 2: Infrastructure expansion and rising budget levels
At 3% of GDP At 4% of GDP At 5% of GDP
Additional Utilization Additional Utilization Additional UtilizationFacility type facilities rate (%) facilities rate (%) facilities rate (%)
Referral hospital 0 0 0 0 0 0.61District hospital 41 99 47 100 53 98Clinic 411 56 53 64 578 74
WHO Bulletin OMS. Vol 72 1994
350
HRAM
-.1-- I
-- __ -without infrastructure expansion
668

Cost-effectiveness analysis and health sector policy choices
Table 3: Allocations to specific interventions at varying health budget levels for a hypothetical sub-Saharan Africancountrya
Intervention
Fixed infrastructurebARI screening and referralOral rehydration therapy
BCG added to DPTHepatitis B immunizationlodination of salt or waterMeasles immunizationPoliomyelitis immunizationSemiannual vitamin-A dose for children 0-5 yearsTetanus immunization
Breast-feeding promotion w/education or hospitalroutine for diarrhoeal diseases
Improved weaning practices from educationOral iron supplementation during pregnancy
Chlamydia treatment w/antibioticsGonorrhoea treatment w/antibioticsSyphilis treatment w/antibioticsHIV blood screening
Annual breast examinationsAntibiotics for rheumatic heart diseaseCataract surgeryCVD preventive programmeImproved domestic and personal hygieneInjected insulin and health education for IDDMcLeprosy multidrug clinicLow-cost management of acute MlcPap smear at 5-year intervalsPneumococcal vaccineSchizophreniaSchool-based anti-helminthic chemoprophylaxisShort-course chemotherapy for sputum-negative patients
Short-course chemotherapy for sputum-positive patients
Sugar or salt fortified with ironTetanus referral case managementVector control for malaria
Added infrastructure
At 3.0% of GDP
Spending DALYS('000 $) ('000 $)
32 6976 879 233789 12
920 71391 8249 32
4 986 272907 30577 38
1 651 213
2 564 741 526 46
70 1
107111147911
00
860000
5370
246884248597
6 688
69
15639
009000601
163
12372
3 498 453
1240
12 123
20 713
190
304
At 4.0% of GDP
Spending DALYS('000 $) ('000 $)
32 69911 107 2774 831 53
1 783 80505 9249 32
7 686 2981 232 33881 41
2 042 222
2 755 771 526 46
70 1
107111147962
0388935
05 306
0541
0227
2 543331597
10 208
69
15640
03
100
470702
323
12415
At 5.0% of GDP
Spending DALYS('000 $) ('000 $)
32 69811 107 27715 661 123
2 291 84505 9249 32
12 545 3241 503 34881 41
2 042 222
2 7551 526
70
107111147962
312722935287
9 6582315417804223206331597
14 120
7746
1
69
15640
5102
720732
363
12443
5 018 484 5 218 487
1240
16 587
24 502
190
348
1241 176
18 942
27 238
193
364
Total costs ('000 $)Total cost per capita ($)
102 00010.20
2 435 136 00013.60
2 762 170 00017.00
2 950
a Population is assumed to be 10 million and GDP per capita $340.b Fixed infrastructure reports the costs of construction, maintenance and staffing of the clinics, district hospitals and referral hospitals,which are assumed to have been constructed previously. Assumptions are based on infrastructure data for sub-Saharan African countries.c IDDM: insulin-dependent diabetes mellitus. Ml: myocardial infarction.
All three and combinations of (2) and (3) canbe addressed using the burden of disease and cost-effectiveness information, as described above forsub-Saharan Africa. The inputs to the process, how-ever, to answer each of these questions will be dif-
ferent. Table 4 shows that the budget constraint onthe purchase of interventions is fixed at the currentlevel to answer questions (1) and (3), while for thesecond question there is a marginal increase in thebudget available to buy further interventions.
WHO Bulletin OMS. Vol 72 1994 669

C.J.L. Murray et al.
Table 4: Setting health sector priorities: different Inputs to answer different policy questions
Inputs to optimization or packagingBudget Burden Health system
1. Ground-zero Current budget minus fixed cost Burden in absence of currently Total available capacityof operating current health financed health interventionsinfrastructure
2. Marginal expansion Marginal increase in budget Current burden Unused capacity
3. Politically constrained Current budget minus fixed cost For protected, current burden Total capacity, less capacityground-zero of operating health infrastructure For remainder, burden in used for protected services
and cost of protected activity absence of currently financedhealth interventions
The burden of disease estimates that should beused either in HRAM or in the World Bank packag-ing exercise will be different for the three questions.The first question, which can be labelled the ground-zero exercise, was the one addressed by the HRAMapplied to sub-Saharan Africa. The burden of diseasein the absence of currently financed interventions isthe required input. To allocate marginal increases inresources, maintaining currently financed activities,the currently observed burden of disease is theappropriate input. Finally, to answer the third ques-tion, we would want to use the current burden of dis-ease for those conditions affected by currentlyfinanced and protected activities and the burden ofdisease in the absence of currently financed activitiesfor those activities that are not protected.
Finally, the approach to the infrastructure con-straints would also be different for the three ques-tions. The ground-zero exercise would use totalavailable capacity at each level of the health systemas the constraint on service delivery with the optionfor building new infrastructure. The input to the mar-ginal budget exercise would be the unused capacityat each level with the option of building new infra-structure. The politically constrained exercise woulduse total capacity at each level minus the capacityused to deliver 'protected' services.
In the WDR, the World Bank proposes a pack-age of essential public health and clinical servicesthat would cost $12 in a low-income country. Thispackage is meant to be a marginal package of expen-diture and health gain on top of currently financedactivities. Some confusion is generated when theWorld Bank states, "In fact, in the poorest countriestotal current public spending of $6 per person isabout $6 short of the cost of the package. Total percapita spending, including private spending, is about$14, about the same as the proposed package." (23,page 67). The package, however, has been describedat several junctures as addressing the marginal bur-den of disease and has been calculated using the cur-rent burden, not the burden in the absence of current-
ly financed activities.e In other words, by the natureof its calculation, the World Bank package is a mar-ginal package on top of current expenditure. Payingfor the package in a low-income country is not aquestion of resource reallocation but a question ofincreasing health expenditure by $12 per capita or adoubling of total health sector expenditure in a low-income country; if the increase was to come entirelyfrom the public sector it would entail a tripling ofpublicly financed health expenditure. Potential con-fusion around the policy question that is being askedand the appropriate method of calculation by theWorld Bank highlights the importance of developinga consistent and internally rigorous approach to usingcost-effectiveness for informing sectoral resourceallocation questions.
ImplicationsThe cost-effectiveness of interventions, the burden ofdisease, and information on the human and physicalinfrastructure in a health system can be combinedto answer a host of resource allocation questionsincluding variations of protected expenditures andmarginal budget increases. Using a computer pro-gram like the one illustrated here, investments in thehealth system can be directly compared with ex-panding resources for particular interventions for agiven level of the health system. The preliminary workpresented on such models can easily be developedto incorporate other investments in health systemquality or coverage. Investments in health infor-mation systems or training can be included as long
e The method used to calculate the package is different for dif-ferent interventions. Some of the package is based on a costper person receiving a service and an estimate of the desiredcoverage of the service so that this is closer to the ground-zeroanalysis. For others, including most of the clinical services, thepackage is estimated, based on the current burden of diseaseand the cost per DALY averted.
670 WHO Bulletin OMS. Vol 72 1994

Cost-effectiveness analysis and health sector policy choices
as the chain of causation between these investmentsand improvement in health through the delivery ofspecific health interventions can be traced. Moresophisticated versions of such a computer programcould take into account the delay between the deci-sion to improve the health system and the comple-tion of new construction or training. A multi-periodmodel would also allow for incorporating expectedchanges in the burden of disease due to demographicand epidemiological changes (57, 58).
If more widespread use of cost-effectivenessdatabases to inform health sector resource allocationis intended, then it will be important to alter the stan-dards of reporting cost-effectiveness studies in theliterature. Frequently studies report only an averagecost per unit of service delivered or health benefitsuch as a DALY. Details on the component costs areoften not provided. In order to examine the cost-effectiveness of investing in the health system, wemust shift to reporting the different resources used inproviding a health intervention rather than costs.Table 1 illustrates crude forms of such resource useprofiles where the component inputs such as bed-days, clinic contacts, or outreach workers are denom-inated. More detailed resource use profiles could beprovided outlining specific inputs and the necessaryquality of the inputs such as nursing or surgeons'time, etc. There is an urgent need to develop a sim-ple but useful categorization of the inputs to healthservice production that provides sufficient detail forsectoral analysis.
Another major benefit from a shift to reportingproduction functions would be to increase the trans-ferability of cost-effectiveness results from one envi-ronment to another. In the WDR, studies on the cost-effectiveness of a programme in the United Republicof Tanzania are directly compared with results ofstudies in Brazil where the same input such as nurs-ing time can be ten times more expensive in dollarterms; nevertheless, the World Bank is well aware ofthese limitations and the urgent need to refine meth-ods to transfer cost-effectiveness results from onecontext to another. Such comparisons obscure thereal use of resources for health programmes whichwould be transparent if resource use is reporteddirectly. We hope that the World Bank and theWorld Health Organization will take the lead indeveloping a standard approach to reporting healthintervention resource use profiles and ultimately pro-duction functions.
In this paper, we have argued that cost-effective-ness results, information on the burden of disease,and details on the available health system resourcescan be combined to provide useful insights into awide range of questions on allocation of health sec-tor resources. All these questions, however, are com-
plicated and require at present the assistance ofsophisticated computer algorithms to define prefer-able patterns of resource allocation. Given the earlystage of development of this sectoral application ofcost-effectiveness, it appears that computer pro-grams, such as HRAM, will remain an essentialadjunct to policy analysis. Ultimately, as these meth-ods are tested in a range of countries, simpler deci-sion rules may be developed that will allow for morerapid application of the cost-effectiveness and diseaseburden results to questions of resource allocation.
Despite the challenges raised in this paper, themethod proposed by the WDR and others remains amuch better alternative to current practice. We shouldnot let the perfect be the enemy of the good. TheWorld Bank's Health Sector Priorities Review andthe 1993 WDR have advanced technical analysis ofhealth policy choices in developing countries byyears if not decades. On the other hand, we mustalways remain cognizant of the fact that technicalanalysis of health sector priorities using the burdenof disease, the cost-effectiveness of interventions,and the available resources is only one input to thepolicy process and is not intended to be a rigid pre-scription for all health system ailments.
AcknowledgementsWe gratefully acknowledge the extensive efforts of JohnKim and Robert Ashley. Comments and suggestions fromJulio Frenk, Dean Jamison, Jose-Luis Bobadilla, PhilipMusgrove, and Peter Berman have been very helpful.
ResumeInvestigation du secteur de sant6: analysecoOt-efficacite et choix politiquesLes 6tudes actuelles sur l'affectation des res-sources en fonction du rapport cout-efficacit6- notamment l'Oregon State plan et le Rapportsur le d6veloppement dans le monde 1993 de laBanque mondiale - pretent le flanc a deux cri-tiques importantes. Tout d'abord, les analysescout-efficacite tendent a negliger le r6le des infra-structures de sant6. Ensuite, se pose le problemedes choix politiques qui devraient etre documen-t6s par une analyse cout-efficacit6 de I'affectationdes ressources.
En premier lieu, les 6tudes qui negligent ler6le de l'infrastructure dans I'affectation des res-sources d'apres leur cout-efficacit6 supposentimplicitement que l'infrastructure physique est infi-niment divisible. La m6thode utilisant la liste descoOts moyens (comme celle utilis6e dans le rap-
WHO Bulletin OMS. Vol 72 1994 671

C.J.L. Murray et al.
port de la Banque mondiale) suppose que desfractions des installations, 2% d'un h6pital de dis-trict par exemple, peuvent etre construites confor-m6ment aux normes. Une nouvelle difficulte inter-vient avec les effets indesirables de 1'etablissementconjoint des coOts.
Cet effet infrastructure peut etre corrige en utili-sant un modele informatise tel que le HarvardHealth Resources Allocation Model (HHRAM) qui,comme dans le rapport de la Banque mondiale,integre le rapport cout-efficacit6 et le poids de lamorbidit6. Le HHRAM a e applique a un paysd'Afrique subsaharienne fictif, ayant une populationde 10 millions d'habitants et un PIB par habitant deUS$ 340; ce modble, qui tient compte de 1'expan-sion des infrastructures de sante dans I'affectationdes ressources, donne un nombre total de DALYsuperieur de 40% a ce que donne un modele negli-geant l'infrastructure. Au niveau des budgetsactuels - qui pour I'Afrique subsaharienne, a1'exclusion de I'Afrique du Sud, est de US$ 14 parhabitant - les interventions les plus importantescompte tenu des depenses sont le d6pistage et letraitement des infections respiratoires aigues, lalutte antipaludique, la chimioth6rapie antitubercu-leuse, la vaccination antirougeoleuse, la rehydrata-tion orale, I'allaitement au sein, la vaccination anti-tetanique et l'am6lioration de l'hygiene.
Le second point est que I'analyse coOt-efficacite de I'affectation des ressources permetde traiter trois questions de politique distinctes,chacune avec ses propres contraintes budgetaireset infrastructurelles et ses propres estimations dupoids de la morbidite. 1) Affectation a partir duniveau z6ro: etant donnes un budget fixe et uneinfrastructure de sant6, comment des ressourcesnon fix6es peuvent-elles etre d6pens6es de facona diminuer au maximum le poids de la morbidit6?2) Affectation de ressources a 1'expansion margi-nale: etant donn6s une infrastructure de sant6 etun ensemble d'activit6s actuellement financ6es,dont aucune ne peut etre modifi6e, comment lesaugmentations marginales des ressources du sec-teur de sante peuvent-elles etre depens6es defacon a diminuer au maximum le poids de la mor-bidite ? 3) Affectation au niveau zero politique-ment limit6e: le budget du secteur de sant6 etantfixe, comment les ressources pour la sant6 peu-vent-elles etre r6affectees pour diminuer au maxi-mum le poids de la morbidite sans diminuer lesressources affect6es aux activit6s ",prot6g6es,,.Le probleme de savoir quelle est la question trai-tee par une etude doit etre evite en elaborant unemethode coherente et rigoureuse d'utilisation durapport coOt-efficacite pour documenter l'affecta-tion de ressources.
Une consequence de I'analyse ci-dessus estque pour examiner le rapport cout-efficacite del'investigation des systemes de sante, il faut ren-dre compte des fonctions de production des inter-ventions de sant6 plut6t que des couts. Nous sou-haitons que la Banque mondiale et l'Organisationmondiale de la Sante donnent l'exemple en met-tant au point une methode codifi6e pour l'evalua-tion des fonctions de production des interventionsde sant6.
Malgr6 les problemes soulev6s dans cetarticle, la methode propos6e par le rapport de laBanque mondiale et divers auteurs reste la meil-leure alternative a la pratique actuelle. Toutefois,ne pas oublier que I'analyse technique des priori-t6s du secteur de sante ne pr6tend pas etre uneprescription rigide destinee a traiter tous les mauxdes systemes de sant6.
References1. Klarman HE, Francis JOS, Rosenthal G. Cost-
effectiveness analysis applied to the treatment ofchronic renal disease. Medical care, 1968, 6: 48-54.
2. Elixhauser A et al. Health care CBA/CEA: anupdate on the growth and composition of the litera-ture. Medical care, 1993, 31: jsl-jsl 1.
3. Williams AH. Economics of coronary artery bypassgrafting. British medical journal, 1985, 291: 326-329.
4. Torrance GW, Zipursky A. Cost-effectiveness ofantepartum prevention of Rh immunization. Clinicsin perinatology, 1984, 11: 267-281.
5. Schulman KA et al. Cost-effectiveness of low-dosezidovudine therapy for asymptomatic patients withhuman immunodeficiency virus (HIV) infection.Annals of internal medicine, 1991, 114: 798-802.
6. Drummond M, Torrance G, Mason J. Cost-effec-tiveness league tables: more harm than good?Social science and medicine, 1993, 37: 33-40.
7. Jamison DT et al., eds. Disease control priorities indeveloping countries. New York, Oxford UniversityPress, 1993.
8. Allen D, Lee RH, Lowson K. The use of QALYs inhealth service planning. International journal of healthplanning and management, 1989, 4: 261-273.
9. Oregon Health Services Commission. OregonMedicaid priority setting project. Portland, 1991.
10. Brown LD. The national politics of Oregon's ration-ing plan. Health affairs, 1991, 10(2): 28-51.
11. Dixon J, Welch HG. Priority setting: lessons fromOregon. Lancet, 1991, 337: 891-894.
12. Fox DM, Leichter HM. Rationing care in Oregon: thenew accountability. Health affairs, 1991, 10(2): 7-27.
13. Garland MJ, Hasnain R. Health care in common:setting priorities in Oregon. Hastings Center report,September-October 1990: 16-18.
14. Hadorn DC. Setting health care priorities in Ore-gon-cost-effectiveness meets the rule of rescue.Journal of the American Medical Association, 1991,265: 2218-2225.
672 WHO Bulletin OMS. Vol 72 1994

Cost-effectiveness analysis and health sector policy choices
15. KIevit HD et al. Prioritization of health care ser-vices-a progress report by the Oregon Health Ser-vices Commission. Archives of internal medicine,1991, 151: 912-916.
16. 0stbye T, Speechley M. The Oregon formula: abetter method of allocating health care resources.Nordisk medicin, 1992, 107(3): 92-95.
17. Eddy DM. Oregon's methods-did cost-effectivenessanalysis fail? Journal of the American Medical Asso-ciation, 1991, 266: 2135-2141.
18. Kitzhaber JA. Prioritising health services in an eraof limits: the Oregon experience. British medicaljournal, 1993, 307: 373-377.
19. Murray CJL, Lopez AD, Jamison DT. The globalburden of disease in 1990: summary results, sensi-tivity analysis and future directions. Bulletin of theWorld Health Organization, 1994, 72: 495-509.
20. Murray CJL. Quantifying the burden of disease: thetechnical basis for disability-adjusted life years. Bulle-tin of the World Health Organization, 1994, 72:429-445.
21. Murray CJL, Lopez AD. Quantifying disability: data,methods, and results. Bulletin of the World HealthOrganization, 1994, 72: 481-494.
22. Murray CJL, Lopez AD. Global and regional cause-of-death patterns in 1990. Bulletin of the WorldHealth Organization, 1994, 72: 447-480.
23. World Bank. World development report 1993:investing in health. New York, Oxford UniversityPress, 1993.
24. Bobadilla J-L et al. Design, content and financingof an essential national package of health services.Bulletin of the World Health Organization, 1994, 72:653-662.
25. Garber AM, Phelps CE. Economic foundations ofcost-effectiveness analysis. Cambridge MA, NationalBoard of Economic Research, 1992 (NEBR workingpaper 4164).
26. Phelps CE, Mushlin Al. On the (near) equivalenceof cost-effectiveness and cost-benefit analyses.International journal of technology assessment inhealth care, 1991, 7(1): 12-21.
27. Loomes G, McKenzie L. The use of QALYs inhealth care decision-making. Social science andmedicine, 1989, 28(4): 299-308.
28. Birch S, Gafni A. Cost-effectiveness/utility analy-ses-do current decision rules lead us where wewant to be? Journal of health economics, 1992, 11:279-296.
29. Johannesson M, J6nsson B. Economic evaluationin health care: is there a role for cost-benefit analy-sis? Health policy, 1991, 17: 1-23.
30. Hammer JS. Prices and protocols in public healthcare. Washington, World Bank, 1993 (PopulationHealth and Nutrition Working Paper Series).
31. Mehrez A, Gafni A. Quality-adjusted life years, util-ity theory, and healthy-years equivalents. Medicaldecision-making, 1989, 9:142-149.
32. Miyamoto JM, Eraker SA. Parameter estimates fora QALY utility model. Medical decision-making,1985, 5(2): 191-213.
33. Sackett DL, Torrance GW. The utility of differenthealth states as perceived by the general public.Journal of chronic disease, 1978, 31: 697-704.
34. Pliskin JS, Shepard DS, Weinstein MC. Utilityfunctions for life years and health status. Operationsresearch, 1980, 28(1): 206-224.
35. Torrance GW. Measurement of health state utilitiesfor economic appraisal: a review. Journal of healtheconomics, 1986, 5:1-30.
36. Murray CJL, Kreuser J, Whang W. A cost-effec-tiveness model for allocating health sector resourc-es. Cambridge MA, Harvard Center for Populationand Development Studies 1994 (Health TransitionWorking Paper).
37. Forgy L. Cost-effectiveness in child health: a mini-mum information approach to planning and forecast-ing. In: Hill K, ed., Child health priorities for the1990s. Baltimore, Johns Hopkins University Institutefor International Programs, 1992: 309-335.
38. Torrance GW, Thomas WH, Sackett DL. A utilitymaximization model for evaluation of health careprograms. Health services research, Summer 1972:118-133.
39. Daniels N. Just health care. New York, CambridgeUniversity Press, 1985.
40. Lind R. Discounting for time and risk in energy poli-cy. Baltimore, Johns Hopkins University Press, 1982.
41. Little I, Mirrlees S. Project appraisal and planningfor developing countries, London, Heinemann, 1974.
42. Hartman RW. One thousand points of light seekinga number: a case study of CBO's search for a dis-count rate policy. Journal of environmental econom-ics and management, 1990, 18(suppl.):s3-s7.
43. Martens LLM, van Doorslaer EKA. Dealing withdiscounting. International journal of technologyassessment in health care, 1990, 6: 139-145.
44. Hammit J. Discounting health increments. Journalof health economics, 1993, 12: 117-120.
45. Krahn M, Gafni A. Discounting in the economicevaluation of health care interventions. Medicalcare, 1993, 31: 403-418.
46. Olsen J. On what basis should health be discount-ed? Journal of health economics, 1993, 12: 39-53.
47. Viscusi K, Moore M. Rates of time preference andvaluations of the durations of life. Journal of publiceconomics, 1989, 38: 297-317.
48. Johanneson M. On the discounting of gained life-years in cost-effectiveness analysis. Internationaljournal of technology assessment in health care,1992, 8(2): 359-364.
49. Parsonage M, Neuberger H. Discounting andhealth benefits. Health economics, 1992, 1: 71-76.
50. Messing SD. Discounting health: the issue of sub-sistence and care in an underdeveloped country.Social science and medicine, 1973, 7: 911-916.
51. Keeler E, Cretin S. Discounting of life-saving andother nonmonetary effects. Management science,1983, 29: 300-306.
52. Correa H. Health planning. Kyklos internationalreview for social science, 1967, 20(4): 909-923.
53. Feldstein MS, Piot MA, Sundaresan TK. Resourceallocation model for public health planning: a casestudy of tuberculosis control. Geneva, 1973 (supple-ment to vol. 48 of the Bulletin of the World HealthOrganization).
54. Chen MM, Bush JW. Maximizing health system outputwith political and administrative constraints using math-
WHO Bulletin OMS. Vol 72 1994 673

C.J.L. Murray et al.
ematical programming. Inquiry, 1976, 13: 215-227.55. Barnum H. A resource allocation model for child
survival. Cambridge MA, Oelgeschlager, Gunn andHain, 1980.
56. Brooke A, Kendrick D, Meeraus A. GAMS - auser's guide release 2.25. South San Francisco,The Scientific Press, 1992.
57. Omran AR. The epidemiologic transition theory: apreliminary update. Journal of tropical pediatrics,1983, 29: 305-316.
58. Bobadilla JL et al. The epidemiologic transition andhealth priorities. In: Jamison DT et al., eds. Diseasecontrol priorities in developing countries. New York,Oxford University Press, 1993: 673-702.
674 WHO Bulletin OMS. Vol 72 1994