Embed Size (px)
Citation preview

88 (2006) 265–274www.elsevier.com/locate/schres
Schizophrenia Research
Cortical serotonin7, 1D and 1F receptors: Effects of schizophrenia,suicide and antipsychotic drug treatment
Brian Dean a,c,d,e,⁎, Geoffrey Pavey a, David Thomas f, Elizabeth Scarr a,b
a The Rebecca L. Cooper Research Laboratories, The Mental Health Research Institute, The University of Melbourne, Australiab Centre for Neuroscience, Monash University, Clayton, Victoria, Australiac Department of Pathology, Monash University, Clayton, Victoria, Australia
d Psychiatry, Parkville, Monash University, Clayton, Victoria, Australiae Department of Psychological Medicine, Monash University, Clayton, Victoria, Australia
f GlaxoSmithKline Pharmaceuticals, Psychiatry Centre of Excellence for Drug Discovery, New Frontiers Park (North), Third Avenue, Harlow, UK
Received 19 March 2006; received in revised form 30 June 2006; accepted 5 July 2006Available online 17 August 2006
Abstract
Abnormalities in serotonergic function are thought to be important in the pathology of schizophrenia. Postmortem CNS studiessuggest that levels of serotonin receptors may be altered in the cortex of subjects with schizophrenia. Seeking to expand thishypothesis we have examined the effect of schizophrenia and antipsychotic drug treatments on the levels of cortical serotonin7, 1Dand 1F receptors. There was a significant decrease in the binding of [
3H]SB 269970 to the serotonin7 receptor in Brodmann's area 9from subjects with schizophrenia compared to controls (Mean±S.E.M.: 8.3±0.76 vs. 11.0±0.64 fmol/mg ETE; pb0.05) and anincrease in the binding of that radioligand in the cortex of rats treated with haloperidol (p=0.03). There were no significantdifferences in [3H]sumatriptan binding to the serotonin1D or serotonin1F receptor in Brodmann's area 9 from subjects withschizophrenia. There was a significant increase in [3H]sumatriptan binding to the serotonin1D in binding Layer 2 from subjects whohad potentially died by suicide that was not present in other binding layers or for the serotonin1F or serotonin7 receptors. There wasdecrease in [3H]sumatriptan binding to the serotonin1D, but not serotonin1F, receptors across all cortical binding layers in ratstreated with haloperidol. These data would be consistent with the hypothesis that decreased levels of serotonin7 receptors inBrodmann's area 9 may be involved in the pathological processes of schizophrenia and that levels of cortical serotonin7 and 1D
receptors can be affected by antipsychotic drug treatment.© 2006 Elsevier B.V. All rights reserved.
Keywords: Schizophrenia; Serotonin7 receptor; Serotonin1D receptor; Serotonin1F receptor; Dorsolateral prefrontal cortex; Human postmortem
⁎ Corresponding author. The Rebecca L. Cooper Medical ResearchLaboratories, The Mental Health Research Institute of Victoria,Locked Bag 11, Parkville, Victoria 3052, Australia. Tel.: +61 3 93892940; fax: +61 3 9397 5061.
E-mail address: [email protected] (B. Dean).
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.07.003
1. Introduction
Cognitive deficits are now recognised as the mostdebilitating symptom of schizophrenia (Friedman et al.,1999). Given the key role of the human prefrontal cortexin cognition (Leonard et al., 2006) abnormalities in thefunctioning of this CNS region in subjects withschizophrenia could well underpin the cognitive defi-cits associated with the disorder (Weinberger, 1988).

266 B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
Importantly, the serotonergic systems in the CNS havelong been implicated in the pathology of schizophrenia(Meltzer, 1987) and in maintaining normal cognition(Cassel and Jeltsch, 1995); therefore changes in corticalserotonergic function in schizophrenia could be a contri-butor to cognitive deficits associated with that disorder.
Serotonin (5-HT) signals through a family of 13receptors (Hoyer et al., 2002) which constitute keyfunctional components of serotonergic pathways. Themost direct approach to assessing changes in 5-HTreceptors in schizophrenia is by measuring levels of thereceptor in either postmortem CNS tissue or usingneuroimaging. Technical limitations associated withneuroimaging has meant that the most comprehensivestudies of 5HT receptors in schizophrenia have beencompleted using postmortem CNS and have shownchanges in cortical 5HT2A (Dean, 2003a) and 5HT1A
(Burnet et al., 1996) receptors in subjects with thedisorder. However, these findings are not associated withglobal changes in cortical 5HT receptors in schizophre-nia as the 5HT4 receptor is not altered in cortex fromsubjects with the disorder (Dean et al., 1999). Signifi-cantly, data now suggest that the 5HT1D, 5HT1F and5HT7 receptors may be particularly important in main-taining normal levels of cognition (Meneses, 1999),making these receptors particularly worthy of study inthe cortex of subjects with schizophrenia.
There is a paucity of studies on the 5-HT7, 5-HT1D and5-HT1F receptors in schizophrenia. Genetic studies havesuggested a positive association of the 5HT7 receptor geneand schizophrenia in a Japanese population (Ikeda et al.,2006) that was not detected in an earlier study in apolygenetic population (Erdmann et al., 1996). A study onthe 5-HT1D gene also failed to show any significantassociation between that receptor and schizophrenia(Ambrosio et al., 2004). However, these findings mustbe viewed in the light of extensive genetic studies on the5-HT2A receptor in schizophrenia failing to show con-vincing associations between that gene and schizophreniawhereas a decrease in the level of that receptor has beenextensively reported in postmortem studies (for reviewsee: Dean, 2003a). Thus, a failure to show an associationbetween sequence variation in a receptor gene andschizophrenia does not preclude studies using post-mortem CNS which can provide important informationon the possible role of these receptors in abnormal corticalserotonergic function in subjects with schizophrenia. Thisargument is particularly important given that changedlevels of cortical 5HT1D, 5HT1F and 5HT7 receptors inschizophrenia would increase the importance of thesereceptors as potential drug targets for the treatment ofcognitive deficits associated with the disorder.
Given the limited data on the 5-HT7, 5-HT1D and 5-HT1F receptors in schizophrenia we decided to measurethe levels of these receptors in the cortex of subjects withschizophrenia and a cohort of age and sexmatched controlsubjects. These studies utilised the newly availableradioligand [3H]SB 269970 which radiolabels 5-HT7receptors (Varnas et al., 2004) and [3H]sumatriptan whichlabels the 5-HT1D and 5-HT1F receptors (Scarr et al.,2004) in the human cortex. As with all studies usingpostmortem CNS from subjects with schizophrenia, theeffects of antipsychotic drugs received during life is apotential confounding factor. To address this issue weinvestigated the levels of cortical 5HT7, 5HT1D and5HT1F receptors in rats treated for 1 month with halo-peridol. Haloperidol was chosen as the drug of choice forthis study because all subjects with schizophrenia fromwhom tissue had been obtained had received typicalantipsychotic drugs at some point before death.
2. Materials and methods
2.1. Materials and methods
[3H]sumatriptan and [3H]microscales™ wereobtained from Amersham Biosciences. [3H]SB 269970was kindly donated by GlaxoSmithKline. BAS-TR©plates came from Fuji Photo Film Co. Ltd., Tokyo,Japan. Serotonin hydrochloride, methiothepin hemiox-alate and pimozide were purchased from Sigma AldrichPty. Ltd, as were all other laboratory reagents.
2.2. Tissue collection and processing
2.2.1. Human tissueFollowing approval from the North-Western Health
Care Human Ethics Committee, tissue includingBrodmann's area (BA) 9 was collected from the leftCNS hemisphere, at autopsy, from 24 individuals whohad a preliminary diagnosis of schizophrenia and from27 individuals, closely matched for age and sex, whohad no history of mental illness (controls). Tissue wasrapidly frozen and stored at −70 °C.
Using a structured case history review, the Diagnos-tic Instrument for Brain Studies (Hill et al., 1996), adiagnosis of schizophrenia was confirmed according toDSMIV criteria (American Psychiatric Association,1994), by a psychiatrist and a senior psychologist. Inaddition, whenever possible, toxicology screening wasconducted to exclude the presence of psychotropicdrugs in blood or urine at death.
From case history reviews, the duration of illness(DOI: the interval between the first hospital admission

267B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
to the time of death) and the final recorded antipsychoticdrug dose (FRADD: expressed as chlorpromazineequivalents) (Foster, 1989) were calculated (Table 1).The post-mortem interval (PMI) was calculated as thetime between death and autopsy, except where deathwas not witnessed, in which case the PMI was taken asthe interval halfway between the individual last beingseen alive and being found dead. All cadavers wererefrigerated within 5 h of death. The agonal status of thebrain was assessed by measuring the pH of cerebellartissue (Kingsbury et al., 1995).
The blocks of tissue collected were from BA 9, aregion defined by the lateral surface of the frontal lobeincluding the middle frontal gyrus superior to the inferiorfrontal sulcus (Garey, 1994). Twelve sections (20 μm) ofBA 9 were cut at −20 °C for each schizophrenic andcontrol subject that were included in both radioligandstudies whereas either 5 or 7 were cut for subjectsincluded in only one of the studies, depending whichradioligand was used (see below). All sections weremaintained at −70 °C until required. Radioligandbinding studies were completed with the experimenterblind to diagnosis until all data were analysed.
2.2.2. Rat tissueAfter obtaining consent from the University of
Melbourne Animal Experimental Ethics Committee, alldrug administration procedures and experimental proto-cols were performed at The Mental Health ResearchInstitute in accordance to the Australian Code of Practicefor the Care and Use of Animals for Scientific Purposes(1990) set out by the National Health and MedicalResearch Council of Australia. Six week old maleSprague–Dawley rats (100–150 g; n=5 per group)were treated for 1 month with either vehicle orhaloperidol (0.1 mg/kg/day) in drinking water. Thisdose of haloperidol was chosen because a neuroimagingstudy in live rats has shown that such a dose gives adopamine D2 receptor occupancy close to the occupancyin humans required to give optimal therapeutic effectswithout inducing extrapyramidal side-effects (Kapur etal., 2000). The animals were kept on a 12-h light cyclewith free access to food and water. The brains were thenremoved; frontal cortex was dissected and frozen inisopentane on dry ice, and stored at−70 °C until required.
2.3. Measurement of [3H]SB 269970 and[3H]sumatriptan binding
The binding of [3H]SB 269970 to human cortex andrat CNS was based on a previously described protocol(Thomas et al., 2002). Thus, total radioligand binding
was measured by incubating three sections with 7 nM[3H]SB 269970 in 50 mM Tris–HCl (pH 7.4) containing4 mM CaCl2, 1 mM ascorbic acid, 100 μM pargylinefor 60 min at room temperature. Non-specific binding(NSB) was measured by incubating 2 tissue sectionsunder the same conditions but in the presence of 10 μMpimozide, which selectively binds to the 5-HT7 receptorwith high affinity (Mahe et al., 2004; Roth et al., 1994).Following incubation with the radioligands all sectionswere processed for exposure to tritium imaging plates asdescribed below.
The binding of [3H]sumatriptan was essentially asdescribed previously (Scarr et al., 2004). Specifically,sections were incubated for 30 min at room temperaturein 170 mM Tris–HCl (pH 7.6) prior to being incubatedwith [3H]sumatriptan (4.5 nM) in the presence (NSB) orabsence (TB: 3 sections) of either methiothepin (1 μM: 2sections) or 5-HT (1μM:2 sections) in 170mMTris–HCl(pH 7.6), containing 4 mM CaCl2, 0.01% ascorbic acidand 10 μM pargyline, for 60 min at room temperature.
Following incubationwith the appropriate radioligands,all tissue sections were washed 3×10min in ice-cold assaybuffer and dipped in ice-cold water before being dried in astream of cool air. Tissue sections were partially fixed byovernight storage at room temperature in a desiccatorcontaining paraformaldehyde powder. The fixed sectionswere apposed to BAS-TR2025© imaging plates with [3H]microscales ™ until quantifiable images were obtained.The length of exposure required was dependent upon boththe specific activity of the radioligand and the density ofbinding sites in the tissue. The plates were scanned in aBAS 5000 phosphoimager (high resolution) and phos-phorescence of the images was detected as photo-stimulated luminescence (psl). Using the AIS software, astandard curve was generated using the psl of the [3H]microscales ™. The psl from the sections incubated withradioligand was then quantified as dpm/mg estimatedtissue equivalent (ETE) by comparison with the standardcurve. Using the specific activities of the appropriateradioligand, the values were converted to fmol/mg ETE.
The concentrations of radioligands used in this studywere at least three times the Kd for the binding of theradioligand to human and rat cortex and therefore repre-sent single-point saturation analysis studies. In suchstudies, subtracting NSB from total binding provides agood estimate of the number of binding sites available ineach tissue section.
2.4. Statistical analysis
The D'Agostino and Pearson omnibus normality testwas used to determine whether the data were normally

Table 1Demographic, case history and tissue collection data on subjects with schizophrenia and control subjects used in the study of [3H]SB 269970 or [3H]sumatriptan
Age (years) Sex PMI (h) Cause of death SUID pH DOI (years) FRAD FRADD
Schizophrenia 40 F 61.0 Poisoning; welding solvent Y 5.71 24 Fluphenazine 55022 M 48.5 Asphyxia; plastic bag Y 6.29 2 Fluphenazine,
Chlorpromazine2920
27 F 41.0 Asphyxia; plastic bag Y 5.85 10 Haloperidol 750[3H]SB 269970 46 M 42.0 Ischaemic heart disease 5.53 12 Haloperidol 160[3H]SB 269970 42 M 34.5 Drowning 6.26 15 Flupenthixol,
Chlorpromazine610
61 M 37.5 Ischaemic heart disease 6.46 38 Fluphenazine 74534 F 42.0 Drowning 6.23 2 Risperidone 120022 M 37.0 Combined drug toxicity 6.17 3 Pimozide 20035 F 15.0 Coronary arterial
thrombosis6.26 7 Haloperidol 300
48 F 52.5 Pulmonarythromboembolism
6.21 22 Fluphenazine,Chlorpromazine
700
65 M 41.0 Ischaemic heart disease 6.57 35 Fluphenazine 15065 M 42.0 Bronchopneumonia 6.29 36 Trifluoperazine,
Haloperidol460
[3H]SB 269970 31 F 27.0 Cardiomegaly 6.27 13 Clozapine 87565 F 50.0 Ruptured abdominal
aneurysm6.35 18 Fluphenazine,
Haloperidol550
38 M 40.0 Mediastintis 5.52 15 Haloperidol 160[3H]sumatriptan 41 M 31.0 Combined drug toxicity 6.20 11 Fluphenazine,
Trifluoperazine500
53 M 9.0 Coronary artery atheroma 6.29 9 Trifluoperazine,Chlorpromazine
300
57 M 24.0 Coronary artery atheroma 6.06 28 Fluphenazine 15069 M 48.0 Carbon monoxide poisoning Y 6.44 6 Haloperidol 65047 F 50.0 Pneumonia 6.31 20 Risperidone 600
[3H]sumatriptan 30 F 48.0 Hanging Y 6.37 10 Thiothixene 600[3H]sumatriptan 48 M 30.0 Bronchopneumonia 6.62 24 Flupenthixol,
Thioridazine1250
48 M 30.0 Incised wrist injury Y 6.38 9 Risperidone 15079 F 26.0 Hypothermia 6.27 Fluphenazine 330
[3H]SB 269970Mean 47 38.0 6.20 17 618S.E.M. 3.7 2.9 0.07 2.6 137
[3H]sumatriptanMean 48 38.0 6.23 17 601S.E.M. 3.6 2.9 0.06 2.6 137
Controls Age (years) Sex PMI (h) Cause of death pH
43 M 45.0 Drowning 6.25[3H]SB 269970 25 M 50.0 Exsanguination 6.48[3H]SB 269970 53 M 44.5 Ischaemic heart disease 6.56
62 F 40.0 Ischaemic heart disease 6.45[3H]SB 269970 22 F 42.0 Multiple injuries 6.31[3H]SB 269970 68 F 42.0 Ischaemic heart disease 5.73ST 2 26 M 46.5 Electrocution 6.37[3H]SB 269970 42 M 63.0 Cardiomegally 6.34
48 M 52.0 Ischaemic heart disease 5.99[3H]sumatriptan 21 F 58.0 Myocarditis 6.03
27 M 45.0 Coronary artery atheroma 6.4632 F 56.0 Coronary artery atheroma 6.1630 M 27.0 Coronary artery atheroma 5.86
[3H]SB 269970 42 M 43.0 Coronary artery atheroma 6.61[3H]sumatriptan 48 M 24.0 Coronary artery atheroma 6.37
57 M 27.0 Ischaemic heart disease 6.43
268 B. Dean et al. / Schizophrenia Research 88 (2006) 265–274

Table 1 (continued )
Controls Age (years) Sex PMI (h) Cause of death pH
56 F 24.0 Pericard tamponade 5.8868 M 41.0 Aortic stenosis 6.0647 F 24.0 Pulmonary embolism 5.89
[3H]SB 269970 68 M 69.0 Coronary artery atheroma 6.59[3H]sumatriptan 52 M 22.0 Pulmonary thromboembolism 5.98
38 M 46.0 Trauma/asphyxia 6.42[3H]sumatriptan 67 M 32.0 Acute myocardial infarction 6.14[3H]sumatriptan 43 M 51.0 Coronary artery atheroma 6.43
39 F 65.0 Mitral valve prolapse 6.38[3H]sumatriptan 39 F 65.0 Coronary artery atheroma 6.32
77 F 17.0 Hypertensive heart disease 6.32[3H]SB 269970
Mean 47 43.0 6.30S.E.M. 3.7 3.2 0.07
[3H]sumatriptanMean 46 40.4 6.21S.E.M. 3.4 3.3 0.05
Abbreviations: [3H]SB 269970=[3H]SB 269970 binding only, [3H]sumatriptan=[3H]sumatriptan binding only, PMI=postmortem interval,DOI=duration of illness, FRAD=final recorded antipsychotic drug, FRADD=final recorded antipsychotic drug dose (chlorpromazine equivalents),SUID=suicide.
269B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
distributed. For [3H]sumatriptan binding, comparisons ofbinding densities across diagnostic groups and corticallayers, with suicide and cortical layers or with drugtreatment across binding layers in rats were assessed usinga two-way ANOVAwith Bonferroni post test to identifyspecific sources of variance. For [3H]SB 269970 bindingdifferences between diagnostic cohorts and with drugtreatments in rats were assessed using unpaired t-tests. Theeffects of the potential confounding factor of death bysuicide were assessed by comparing levels of radioligandbinding in the cortex of subjects who had or had not diedby suicide. These analyses were completed first with onlysubjects where suicide was confirmed and again includingsubjectswhere suicidewas possible but not confirmed (i.e.the three subjects with death by drowning). For bothradioligands, relationships between experimental para-meters and the potential confounding factors of PMI, age,pH, chlorpromazine equivalents and DOI were analysedusing Pearson single product moment correlationscalculated using an assumed straight line fit. All statisticalanalyses were completed using GraphPad Prism Version4.0 for Windows (GraphPad Software Inc., San Diego,California, USA).
3. Results
There were no significant differences in the mean age([3H]SB 269970: p=0.98; [3H]sumatriptan: p=0.69),PMI ([3H]SB 269970: p=0.27; [3H]sumatriptan:p=0.61) or pH ([3H]SB 269970: p=0.19; [3H]suma-triptan: p=0.79) between diagnostic cohorts (Table 1).
4. Studies of [3H]SB 269970 binding
The binding of [3H]SB 269970 was homogeneouslydistributed across all cortical layers of both human(Fig. 1A) and rat cortex. Therefore, for this study, anintegrated measure of binding across all layers wastaken as the measure of radioligand binding.
There was a significant decrease in the binding of[3H]SB 269970 to BA 9 from subjects with schizophre-nia compared to controls (Mean±S.E.M.: 8.3±0.76 vs.11.0±0.64 fmol/mg ETE; pb0.05: Fig. 1B). There wasno significant difference in [3H]SB 269970 bindingto BA 9 from subjects who had not died by suicide(Mean±S.E.M.: 9.54±0.59 fmol/mg ETE) comparedto either subjects who had died by confirmed (Mean±S.E.M.: 9.56±1.5 fmol/mg ETE; p=0.99) or uncon-firmed suicide (Mean±S.E.M.: 9.41±1.16 fmol/mgETE; p=0.92). There were no significant correlationsbetween [3H]SB 269970 and age, PMI or brain pH ineither cohort and with DOI and FRADD for subjectswith schizophrenia.
There was a significant increase in [3H]SB 269970binding in the cortex of rats treated with haloperidol( p=0.03: Table 2).
5. Studies of [3H]sumatriptan binding
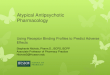
In humans (Fig. 1C–D), both methiothepin-sensitiveand -insensitive [3H]sumatriptan binding was detectedin BA 9 in three distinct layers. Microscopic examina-tion of the tissue sections used for autoradiography after

Fig. 1. A: Typical autoradiographs showing the binding of [3H]SB 269970 to human (A) cortex, the non-specific binding of the radioligand in thepresence of 10−5 M pimozide is shown as the insert. B: The binding of [3H]SB 269970 (Mean±S.E.M.) to cortex (Brodmann's area 9) from subjectswith schizophrenia and control subjects. C–D: Typical autoradiographs showing the binding of [3H]sumatriptan alone (C) to human cortex(Brodmann's area 9) and in the presence of 10−5 M methiothepin (D) or 10−5 M serotonin (E). F: A summary (Mean±S.E.M.) of methiothepin-sensitive and -insensitive [3H]sumatriptan binding to Brodmann's area 9 from control subjects and subjects with schizophrenia. *pb0.05.
270 B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
Nissl staining (Disbrey and Rack, 1970) showed that theouter binding layer (Layer 1) encompassed corticallaminae I to III, the middle layer of radioligand binding(Layer 2) was over laminae IVand Vand the inner layer(Layer 3) was over lamina VI.
For both methiothepin-sensitive and -insensitive [3H]sumatriptan binding there was significant variance inbinding between layers (sensitive: F=8.49, df=2, 114,pb0.0005; insensitive: F=45.90, df=2, 114, pb0.0001)but not with diagnosis (sensitive: F=0.14, df=1, 114,

Table 2The binding of [3H]SB 269970 (Mean±S.E.M.) to the 5-HT7R and[3H]sumatriptan (Mean±S.E.M.) to the 5-HT1DR and 5-HT1FR in thecortex of rats treated for 1 month with either vehicle or haloperidol(0.1 mg/kg/day) in drinking water
Receptor Binding Layer Vehicle Haloperidol(fmol/mg ETE)
p
5-HT7 N/A 4.9±0.83 8.8±1.4 b0.05
5-HT1D 1 2.99±0.28 1.47±0.15 b0.0012 5.48±0.37 2.63±0.05 b0.0013 1.94±0.4 2.17±0.24 n.s.
5-HT1F 1 5.87±0.26 5.69±0.23 n.s.2 11.54±0.46 10.40±0.34 n.s3 5.85±0.27 6.43±0.34 n.s.
Abbreviations: N/A=not applicable, n.s.=not significant, ETE=esti-mated tissue equivalents.
271B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
p=0.71; insensitive: F=2.58, df=2, 114, p=0.11) andthere was no significant interaction between thesevariables (sensitive: F=0.31, df=2, 114, p=0.73; insen-sitive: F=0.09, df=2, 114, p=0.92. Fig. 1F).
Analysis of methiothepin-sensitive [3H]sumatriptanbinding across layers revealed that this variance to be dueto radioligand binding being higher in Layer 1 (pb0.05)and 2 (pb0.001) compared to that in Layer 3 in controlsubjects. By contrast, methiothepin-sensitive [3H]suma-triptan binding did not vary significantly between layers intissue from the subjects with schizophrenia. For bothschizophrenia and controls, the levels of methiothepin-insensitive binding showed the same rank order of bindingin that Layer 2N (pb0.001) Layer 3N (pb0.05) Layer 1.
There were no significant correlations betweenmethiothepin sensitive or insensitive [3H]sumatriptanbinding with any demographic, pharmacological or tissuecollection variable. However, there was significant var-iance in methiothepin-sensitive [3H]sumatriptan bindingbetween subjects who had died by confirmed (F=9.15,df=1,2,111, p=0.003) or confirmed+ unconfirmed sui-cide (F=11.94, df=1,2,114, pb0.001) and those who hadnot died as a result of suicide. The global variance inmethiothepin-sensitive [3H]sumatriptan in confirmed sui-cide was due to non-significant increases in radioligandbinding in each binding layer (Mean±S.E.M. Layer 1:suicide=18.3±0.93 vs. non-suicide 16.6±0.52 fmol/mgETE, pN0.05; Layer 2: suicide=20.0±1.4 vs. non-suicide17.4±0.53 fmol/mg ETE, pN0.05; Layer 3: sui-cide=17.7±1.1 vs. non-suicide 14.9±0.43 fmol/mgETE, pN0.05). For confirmed plus unconfirmed suicidethere was a significant increase in methiothepin-sensitive[3H]sumatriptan binding in Layer 2 (Mean±S.E.M.suicide=20.4±1.2 vs. non-suicide 17.4±0.53 fmol/mgETE, pb0.05) with no significant changes in binding in
Layer 1 (suicide=18.7±0.90 vs. non-suicide 16.6±0.52fmol/mg ETE, pN0.05) and Layer 3 (suicide=17.2±1.0vs. non-suicide 14.9±0.43 fmol/mg ETE, pN0.05). Formethiothepin-insensitive binding there was significantvariance with confirmed (F=4.23, df=1,2,11, p=0.04)but not confirmed+ unconfirmed (F=2.89, df=1,2,114,p=0.09) suicide. The global variance in confirmed suicidewas due to non-significant decreases in methiothepin-insensitive binding in all binding layers (Mean±S.E.M.Layer 1: suicide=10.6±0.69 vs. non-suicide 11.9±0.47fmol/mg ETE, pN0.05; Layer 2: suicide=16.6±1.1 vs.non-suicide 19.0±0.72 fmol/mg ETE, pN0.05; Layer 3:suicide=13.0±1.0 vs. non-suicide 14.4±0.56 fmol/mgETE, pN0.05).
In rats, there was a significant variance in methiothe-pin-sensitive [3H]sumatriptan binding with drug treat-ments (F=40.5, df=2,1,2,24, pb0.0001), acrossradioligand binding layers (F=31.9, df=2,1,2,24,pb0.0001) with a significant interaction between thetwo variables (F=14.8, df=2,1,2,24, pb0.0001). Thevariance with drug treatment was due to decreasesin methiothepin-sensitive [3H]sumatriptan binding inLayer 1 (pb0.001) and 2 (pb0.001) in rats treated withhaloperidol (Table 2).
The density of methiothepin-insensitive [3H]suma-triptan binding did not vary in rat cortex with drugtreatment (F=0.83, df=2,1,2,24, p=0.37) but did varysignificantly across Layers (F=159, df=2,1,2,24,pb0.0001) and there was significant interaction betweenthe variables (F=3.56, df=2,1,2,24, pb0.05) (Table 2).
6. Discussion
This study has shown a significant decrease in [3H]SB 269970 binding in BA 9 from subjects withschizophrenia and a significant increase in binding ofthat radioligand in the cortex of rats treated for 1 monthwith haloperidol. Under the conditions used in thesestudies [3H]SB 269970would bind to the 5-HT7 receptorin both human (Thomas et al., 2000; Varnas et al., 2004)and rat (Thomas et al., 2002) cortex. Therefore, our datawould be consistent with the hypothesis that there is adecrease in 5-HT7 receptor density in BA 9 from subjectswith schizophrenia and that haloperidol treatmentincreases levels of the receptor in rat cortex. We arenot aware of any other radioligand binding studies of 5-HT7 receptors in postmortem CNS from subjects withschizophrenia, but our data show similar levels of re-ceptors in tissue from control subjects as reported in anearlier study (Varnas et al., 2004). Importantly, our studyadds to an earlier study that reported a decrease in levelsof mRNA for the 5-HT7 receptor in BA 9/46 from

272 B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
subjects with schizophrenia (East et al., 2002) suggestingthat a change in 5-HT7 gene expression translates intodifferences in levels of receptor.
The 5-HT7 receptor has been shown to have animportant role in regulating cortical synaptic activity(Beique et al., 2004b), therefore changes in the level ofthe receptor in the dorsolateral prefrontal cortex mightbe predicted to contribute to the abnormal functioning ofthat region in schizophrenia (Weinberger, 1988). More-over, the 5-HT7 receptor has been shown to be importantin affecting learning and memory, hippocampal activity,circadian rhythm and mood (Hedlund and Sutcliffe,2004), all of which have been shown to be affected inschizophrenia (Levinson et al., 1999; Martin et al.,2005; Meltzer, 2004; Scarr et al., 2004). Thus, whilst asequencing study concluded that genetic variation ofthe 5-HT7 receptor did not play a major role in thedevelopment of schizophrenia (Erdmann et al., 1996),our data suggest a possible role for the 5-HT7 receptor inthe pathology of the illness. The focus of this study wason the potential role for specific cortical serotoninreceptors in schizophrenia with the hypothesis thatchanges in these receptors may be targets for drugsdesigned to reverse the cognitive deficits associatedwith the disorder. Given the demonstration that the 5-HT7 receptor is altered in the CNS from subjects withschizophrenia further studies on this receptor, particu-larly in the hippocampus and thalamus, would bewarranted given the important role of the 5-HT7 receptorin learning and memory (Hedlund and Sutcliffe, 2004).
Data from studies using knockout mice and othertechniques have revealed some properties of the 5-HT7receptor. One study has shown an increase in adrenergicα2A receptors in the cortex and adrenergicα2C receptors inthe cortex, thalamus and hypothalamus of the micelacking the 5-HT7 receptor (Bonaventure et al., 2004).These data were interpreted as indicating that anappropriate level of 5-HT7 receptor may be critical fornormal cortical development. This hypothesis is supportedby data suggesting that appropriate interactions betweenthe 5-HT7, 5-HT1A and 5HT2A are critical in maintainingnormal membrane potentials (Beique et al., 2004a) andneuronal cytoarchitecture (Kvachnina et al., 2005) in thedeveloping cortex. It is, therefore, noteworthy that whilstglobal levels of adrenergic α2 adrenergic receptors are notaltered in the cortex of subjects with schizophrenia (Dean,2003b), changes in levels of 5-HT7, 5-HT2A (Dean,2003a) and 5-HT1A (Burnet et al., 1996) have now beenreported in the cortex of subjects with the disorder. Thesechanges may therefore be reflective of abnormalities in 5-HTsignaling that could have led to subtle abnormalities incortical development in subjects with the schizophrenia.
Little is known of the regulation of the 5-HT7 receptorbut haloperidol does not bind to the receptor with highaffinity (Bymaster et al., 1999; Roth et al., 1994). Giventhe high selectivity of haloperidol for the dopamine-D2
like receptors, the 5HT2AR and the α1R (Bymaster et al.,1996) our data suggest that blockade of one or all of thesereceptors is involved in the observed up-regulation ofcortical 5-HT7R in the rat. Whilst it must be acknowl-edged that the treatment regime in rats may not model themulti-year antipsychotic drug treatments received bysubjects with schizophrenia, our current data in rats donot readily support the hypothesis that the decrease in5HT7R in the cortex from subjects with schizophrenia issimply reflecting the effects of antipsychotic drug treat-ments prior to death.
Neither methiothepin-sensitive nor methiothepin-insensitive [3H]sumatriptan binding differed significant-ly in the cortex of subjects with schizophrenia com-pared to that in controls. Under the conditions used,methiothepin-sensitive [3H]sumatriptan binding wouldpredominantly represent the 5-HT1D receptor whilst themethiothepin-insensitive binding would represent bind-ing to the 5-HT1F receptor (Scarr et al., 2004). Our datatherefore suggest that, unlike in the hippocampus wherethere are decreased levels of 5-HT1F receptor inschizophrenia (Scarr et al., 2004), levels of the 5-HT1D and 5-HT1F receptors did not differ in BA 9 fromsubjects with the disorder. Thus, neither postmortemCNS data nor genetic studies (Ambrosio et al., 2004)support a role for the 5-HT1D receptor in schizophrenia.
This study contained tissue from subjects who hadeither died by suicide or forms of death that may haveinvolved suicide. In the case of 5-HT1D and 5-HT1F
receptors the only focal significant effect was an increasein the density of the 5-HT1D in binding Layer 2 insubjects who had died by confirmed suicide and in thetotal population of subjects who may have died bysuicide. With regards to the 5-HT1F receptor, ourfindings agree with a study focused on suicide in depres-sion that reported no change in either the 5-HT1D or 5-HT1F receptors in the cortex of subjects who had died bysuicide (Lowther et al., 1997). However, our findingsdiffer from earlier studies on the cortical 5-HT1D receptorthat reported no difference in that receptor in the cortexof subjects who had died by suicide (Arranz et al., 1994;Lowther et al., 1997). However, these two studiesdiffered in that one reported no change in cortical 5HT1D
receptors in subjects with depression who had died bysuicide (Lowther et al., 1997) whilst the other reportedthat there was a decrease in the affinity of drug binding tothe 5HT1D receptor in depressed suicide whilst thedensity of that receptor was decreased in subjects that did

273B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
not have depression and died by suicide (Arranz et al.,1994). Thus current data would be consistent with theargument that changes in levels of 5-HT1D receptorsassociated with, or preceding, suicide might vary be-tween psychiatric diseases and that any changes in thelevels of that receptor from normal equilibrium increasethe risk of suicide. Alternatively, it might be that the datain suicide subjects with depression support the long heldhypothesis that under activity of that receptor isimportant in the genesis of that disorder (Cleare et al.,1998). Irrespective, our data supports the overarchinghypothesis that changes in the serotonergic pathways inschizophrenia are complex and need further elucidation.
Haloperidol treatment significantly reduced methio-thepin-sensitive, but not methiothepin-insensitive, [3H]sumatriptan binding in the rat cortex; an effect limited tothe outer two cortical binding layers. Using current no-menclature (Hoyer et al., 2002), methiothepin-sensitive[3H]sumatriptan binding would be predominantly to therat 5-HT1D receptor. Thus, our data are consistent with theconclusion that haloperidol treatment decreases levels of5-HT1D receptor in the outer layers of the rat cortex.Significantly, haloperidol does not bind to the 5-HT1Dreceptor with high-affinity (Audinot et al., 2001; Pauwelset al., 1993) but has been shown to indirectly interfere with5-HT1D receptor function (Higgins et al., 1991). It remainsto be determined if this effect of haloperidol is associatedwith any aspect of the drugs clinical efficacy. Importantly,the absence of a decrease in methiothepin-sensitive [3H]sumatriptan binding in the cortex of subjects with schizo-phrenia is further evidence that the changes in radioligandbindingmeasured in tissue fromsubjectswith that disorderare not simply reflecting the effects of antipsychotic drugs.
This study suggests that the ability of haloperidol toalter levels of cortical 5-HT7 and 5-HT1D receptors maybe involved in the mechanism of action of this class ofdrug. In addition, this and other studies from ourlaboratories (Dean, 2002), show that 5-HT receptors areaffected in complex ways by both the pathologicalprocesses underlying schizophrenia (Meltzer, 1987) andthe actions of antipsychotic drugs (Leysen et al., 1978).More specifically, this study strongly suggests thatchanges in cortical 5-HT7 receptors may be involved inthe neurobiology of schizophrenia and the actions ofantipsychotic drugs. Whilst it is presumptive to ascribeany particular function to specific 5-HT receptors, it isknown that serotonin in the prefrontal cortex is particu-larly important in decision making and reversal learning(Clark et al., 2004). Therefore it is possible that changes inthe 5-HT7 receptor in subjects with schizophrenia may becontributing to deficits in these areas of cognition insubjects with the disorder. This hypothesis is supported by
the recent finding that SB 269970 attenuates a PCP-induced deficit in the rat reversal learning model (Neillet al., 2006), this behavioral model is thought tomimic thecognitive deficits associated with schizophrenia.
Acknowledgements
BD is a NHMRC Senior Research Fellowship(# 400016) and ES Elizabeth Scarr is the RonaldGriffiths Schizophrenia Research Fellow and holds aNARSAD Young Investigator Award. The study wasalso supported by NHMRC Project Grant # 114253 andThe Rebecca L. Cooper Medical Research Foundation.
References
Ambrosio, A.M., Kennedy, J.L., Macciardi, F., Coelho, I., Soares, M.J.,Oliveira, C.R., Pato, C.N., 2004. Lack of association or linkagedisequilibrium between schizophrenia and polymorphisms in the 5-HT1Dalpha and 5-HT1Dbeta autoreceptor genes: family-basedassociation study. Am. J. Med. Genet., B Neuropsychiatr. Genet.128, 1–5.
American Psychiatric Association, 1994. Diagnostic and StatisticalManual of Mental Disorders, Forth edition. American PsychiatricAssociation, Washington, DC.
Arranz, B., Eriksson, A., Mellerup, E., Plenge, P., Marcusson, J., 1994.Brain 5-HT1A, 5-HT1D, and 5-HT2 receptors in suicide victims.Biol. Psychiatry 35, 457–463.
Audinot, V., Newman-Tancredi, A., Cussac, D., Millan, M.J., 2001.Inverse agonist properties of antipsychotic agents at cloned, human(h) serotonin (5-HT)(1B) and h5-HT(1D) receptors. Neuropsycho-pharmacology 25, 410–422.
Beique, J.C., Campbell, B., Perring, P., Hamblin, M.W., Walker, P.,Mladenovic, L., Andrade, R., 2004a. Serotonergic regulation ofmembrane potential in developing rat prefrontal cortex: coordi-nated expression of 5-hydroxytryptamine (5-HT)1A, 5-HT2A, and5-HT7 receptors. J. Neurosci. 24, 4807–4817.
Beique, J.C., Chapin-Penick, E.M., Mladenovic, L., Andrade, R.,2004b. Serotonergic facilitation of synaptic activity in thedeveloping rat prefrontal cortex. J. Physiol. 556, 739–754.
Bonaventure, P., Nepomuceno, D., Hein, L., Sutcliffe, J.G., Lovenberg,T., Hedlund, P.B., 2004. Radioligand binding analysis of knockoutmice reveals 5-hydroxytryptamine(7) receptor distribution anduncovers 8-hydroxy-2-(di-n-propylamino)tetralin interaction withalpha(2) adrenergic receptors. Neuroscience 124, 901–911.
Burnet, P.W., Eastwood, S.L., Harrison, P.J., 1996. 5-HT1A and 5-HT2A receptor mRNAs and binding site densities are differen-tially altered in schizophrenia. Neuropsychopharmacology 15,442–455.
Bymaster, F.P., Calligaro, D.O., Falcone, J.F., Marsh, R.D., Moore,N.A., Tye, N.C., Seeman, P., Wong, D.T., 1996. Radioreceptorbinding profile of the atypical antipsychotic olanzapine. Neurop-sychopharmacology 14, 87–96.
Bymaster, F., Perry, K.W., Nelson, D.L., Wong, D.T., Rasmussen, K.,Moore, N.A., Calligaro, D.O., 1999. Olanzapine: a basic scienceupdate. Br. J. Psychiatr., Suppl. 36–40.
Cassel, J.C., Jeltsch, H., 1995. Serotonergic modulation of cholinergicfunction in the central nervous system: cognitive implications.Neuroscience 69, 1–41.

274 B. Dean et al. / Schizophrenia Research 88 (2006) 265–274
Clark, L., Cools, R., Robbins, T.W., 2004. The neuropsychology ofventral prefrontal cortex: decision-making and reversal learning.Brain Cogn. 55, 41–53.
Cleare, A.J., Murray, R.M., Sherwood, R.A., O'Keane, V., 1998.Abnormal 5-HT1D receptor function in major depression: aneuropharmacological challenge study using sumatriptan. Psychol.Med. 28, 295–300.
Dean, B., 2002. Understanding the pathology of schizophrenia: recentadvances from the study of the molecular architecture ofpostmortem CNS tissue. Postgrad. Med. J. 78, 142–148.
Dean, B., 2003a. The cortical serotonin2A receptor and the pathologyof schizophrenia: a likely accomplice. J. Neurochem. 85, 1–13.
Dean, B., 2003b. [3H]RX 821002 in human dorsolateral prefrontalcortex: no changes in postmortem tissue from subjects withschizophrenia. Psychiatry Res. 119, 25–31.
Dean, B., Tomaskovic-Crook, E., Opeskin, K., Keks, N., Copolov, D.,1999. No change in the density of the serotonin1A receptor, theserotonin4 receptor or the serotonin transporter in the dorsolateralprefrontal cortex from subjects with schizophrenia. Neurochem.Int. 34, 109–115.
Disbrey, B.D., Rack, J.H., 1970. Histological Laboratory Methods. E& S Livingstone, Edinburgh and London.
East, S.Z., Burnet, P.W., Kerwin, R.W., Harrison, P.J., 2002. An RT-PCR study of 5-HT(6) and 5-HT(7) receptor mRNAs in thehippocampal formation and prefrontal cortex in schizophrenia.Schizophr. Res. 57, 15–26.
Erdmann, J., Nothen, M.M., Shimron-Abarbanell, D., Rietschel, M.,Albus, M., Borrmann, M., Maier, W., Franzek, E., Korner, J.,Weigelt, B., Fimmers, R., Propping, P., 1996. The human serotonin7 (5-HT7) receptor gene: genomic organization and systematicmutation screening in schizophrenia and bipolar affective disorder.Mol. Psychiatry 1, 392–397.
Foster, P., 1989. Neuroleptic equivalence. Pharm. J. 243, 431–432.Friedman, J.I., Temporini, H., Davis, K.L., 1999. Pharmacologic
strategies for augmenting cognitive performance in schizophrenia.Biol. Psychiatry 45, 1–16.
Garey, L.J., 1994. Bordmann's ‘Localisation in the Cerebral Cortex’.Smith-Gordon, London.
Hedlund, P.B., Sutcliffe, J.G., 2004. Functional, molecular andpharmacological advances in 5-HT7 receptor research. TrendsPharmacol. Sci. 25, 481–486.
Higgins, G.A., Jordan, C.C., Skingle, M., 1991. Evidence that theunilateral activation of 5-HT1D receptors in the substantia nigra ofthe guinea-pig elicits contralateral rotation. Br. J. Pharmacol. 102,305–310.
Hill, C., Keks, N., Roberts, S., Opeskin, K., Dean, B., Mackinnon, A.,Copolov, D., 1996. Problem of diagnosis in postmortem brainstudies of schizophrenia. Am. J. Psychiatry 153, 533–537.
Hoyer, D., Hannon, J.P., Martin, G.R., 2002. Molecular, pharmaco-logical and functional diversity of 5-HT receptors. Pharmacol.Biochem. Behav. 71, 533–554.
Ikeda, M., Iwata, N., Kitajima, T., Suzuki, T., Yamanouchi, Y.,Kinoshita, Y., Ozaki, N., 2006. Positive association of theserotonin 5-HT7 receptor gene with schizophrenia in a Japanesepopulation. Neuropsychopharmacology 31, 866–871.
Kapur, S., Wadenberg, M.L., Remington, G., 2000. Are animal studiesof antipsychotics appropriately dosed? Lessons from the bedside tothe bench. Can. J. Psychiatry 45, 241–246.
Kingsbury, A.E., Foster, O.J., Nisbet, A.P., Cairns, N., Bray, L., Eve,D.J., Lees, A.J., Marsden, C.D., 1995. Tissue pH as an indicator ofmRNA preservation in human post-mortem brain. Brain Res. Mol.Brain Res. 28, 311–318.
Kvachnina, E., Liu, G., Dityatev, A., Renner, U., Dumuis, A., Richter,D.W., Dityateva, G., Schachner, M., Voyno-Yasenetskaya, T.A.,Ponimaskin, E.G., 2005. 5-HT7 receptor is coupled to Galphasubunits of heterotrimeric G12-protein to regulate gene transcrip-tion and neuronal morphology. J. Neurosci. 25, 7821–7830.
Leonard, C.M., Eckert, M.A., Kuldau, J.M., 2006. Exploiting humananatomical variability as a link between genome and cognome.Genes Brain Behav. 5 (Suppl 1), 64–77.
Levinson, D.F., Umapathy, C., Musthaq, M., 1999. Treatment ofschizoaffective disorder and schizophrenia with mood symptoms.Am. J. Psychiatry 156, 1138–1148.
Leysen, J.E., Niemegeers, C.J., Tollenaere, J.P., Laduron, P.M., 1978.Serotonergic component of neuroleptic receptors. Nature 272,168–171.
Lowther, S., Katona, C.L., Crompton, M.R., Horton, R.W., 1997. 5-HT1D and 5-HT1E/1F binding sites in depressed suicides:increased 5-HT1D binding in globus pallidus but not cortex.Mol. Psychiatry 2, 314–321.
Mahe, C., Loetscher, E., Feuerbach, D., Muller, W., Seiler, M.P.,Schoeffter, P., 2004. Differential inverse agonist efficacies of SB-258719, SB-258741 and SB-269970 at human recombinantserotonin 5-HT7 receptors. Eur. J. Pharmacol. 495, 97–102.
Martin, J.L., Jeste, D.V., Ncoli-Israel, S., 2005. Older schizophreniapatients have more disrupted sleep and circadian rhythms than age-matched comparison subjects. J. Psychiatr. Res. 39, 251–259.
Meltzer, H.Y., 1987. Biological studies in schizophrenia. Schizophr.Bull. 13, 77–111.
Meltzer, H.Y., 2004. Cognitive factors in schizophrenia: causes,impact, and treatment. CNS Spectr. 9, 15–24.
Meneses, A., 1999. 5-HT system and cognition. Neurosci. Biobehav.Rev. 23, 1111–1125.
Neill, J., Grayson, B., Jones, D.N.C., Hagan, J.J., Thomas, D.R., 2006.Antagonism at 5-HT7 receptors attenuates a PCP-induced reversallearning deficit in the rat. Schizophr. Res. 81 (suppl.), 233.
Pauwels, P.J., Palmier, C., Briley, M., 1993. Identification of 5-hydroxytryptamine1D binding sites in sheep caudate nucleusmembranes. Biochem. Pharmacol. 46, 535–538.
Roth, B.L., Craigo, S.C., Choudhary, M.S., Uluer, A., Monsma Jr., F.J., Shen, Y., Meltzer, H.Y., Sibley, D.R., 1994. Binding of typicaland atypical antipsychotic agents to 5-hydroxytryptamine-6 and 5-hydroxytryptamine-7 receptors. J. Pharmacol. Exp. Ther. 268,1403–1410.
Scarr, E., Pavey, G., Copolov, D., Dean, B., 2004. Hippocampal 5-hydroxytryptamine receptors: abnormalities in postmortem brainfrom schizophrenic subjects. Schizophr. Res. 71, 383–392.
Thomas, D.R., Atkinson, P.J., Ho, M., Bromidge, S.M., Lovell, P.J.,Villani, A.J., Hagan, J.J., Middlemiss, D.N., Price, G.W., 2000.[(3)H]-SB-269970—a selective antagonist radioligand for 5-HT(7) receptors. Br. J. Pharmacol. 130, 409–417.
Thomas, D.R., Atkinson, P.J., Hastie, P.G., Roberts, J.C., Middlemiss,D.N., Price, G.W., 2002. [3H]-SB-269970 radiolabels 5-HT7receptors in rodent, pig and primate brain tissues. Neuropharma-cology 42, 74–81.
Varnas, K., Thomas, D.R., Tupala, E., Tiihonen, J., Hall, H., 2004.Distribution of 5-HT7 receptors in the human brain: a preliminaryautoradiographic study using [3H]SB-269970. Neurosci. Lett. 367,313–316.
Weinberger, D.R., 1988. Schizophrenia and the frontal lobe. TrendsNeurosci. 11, 367–370.