Embed Size (px)
DESCRIPTION
Essential reading for the Acquired Brain Injury arena
Citation preview

CHILDREN SPECIAL:
Nature & nurtureTransforming ABI services for today's youth
Inside: SMART future: Accurate diagnosis of ABI 3 United Kingdom of Acquired Brain Injury Forum demands change 4
New start: Clinical Commissioning Groups uncovered 6Shocking effects of undiagnosed brain injury 8Model pupil: Life after injury 15
Issue No.2
Winter 2012produced by Enable Publishing
Essential reading for the Acquired Brain Injury arena
Editorial/Comment2
If you find Cortext an interesting and informative read, let us know by getting in touch at [email protected]
Please also send in any suggestions on topical subjects you would like to see covered in future issues.
Acquiring a brain injury is harrowing for anyone but when it strikes children, it can be heartbreaking. A thought-provoking feature on page 8 looks at how half of the youth offenders in the UK may have turned to a life of crime as a result of an undiagnosed ABI.
Page 10 focuses on a new website launched by The Children's Trust, which is providing much needed support to parents wanting to know more about their child’s ABI. Page 11 pays homage to the notoriously forgotten group – siblings that are affected by their brother or sister’s ABI.
Page 3 sees Helen Gill-Thwaites from the Royal Hospital of Neuro-disability talk about a diagnostic tool that uses sensory stimuli to accurately pinpoint the true extent of ABI.
Editorial
Welcome Welcome to our Winter issue of Cortext magazine – a special emphasis on how Acquired Brain Injury (ABI) can have a devastating effect on youngsters and their families.
Jane Heath, Editor Head of Business Relations, Enable Care
The Acquired Brain Injury (ABI) arena is constantly evolving and developing. Cortext actively encourages knowledge sharing and debate. Here, experts comment on their favourite articles in this edition.
Comment
How the introduction of the Clinical Commissioning Groups in April 2013 will have a huge impact on the way ABI services are commissioned going forward is featured on page 6.
Music therapy (page 12) doesn’t just add a fun element to ABI rehab but helps solve memory and cognitive problems among others. Meanwhile, Yoki Mekuria’s road to recovery in just two years following an ABI on page 15 is a truly inspiring story. We hope our magazine has given you some food for thought on some of the issues happening right now in the world of ABI.
Karen Rullo BAppSc Occupational (Therapy) Managing Director & Case Manager
Liz Shipperlee Speech and Language Therapist
Karen Rullo was keen to read about how Gary Smith conquered his challenge in getting back to work following a brain injury on page 14.
“Gary appears fortunate to have had some brain injury specific input during his vocational rehabilitation, but unfortunately this is not always so commonplace. The challenges faced by individuals with ABI in returning to any kind of vocation are complex and unique, and require specialist input from those supporting the client back into the workplace.
“Work is also needed to provide education and guidance to the individual’s employer and colleagues, so they have an awareness of their difficulties, and how these can be best accommodated. This is particularly important in ABI, which is a ‘hidden’ disability often overlooked and especially if accompanied by more obvious, physical injuries.”
Enthusiastic about how music adds another dimension to conventional therapy, Liz Shipperlee was thrilled to see it featured on page 12.
“Music therapy has been recognised in improving mood, decreasing depression and reducing anxiety. It has been long established as a therapy allied to health professionals. Its use with children and adults, and particularly those with ABI, is beneficial. Music helps with responsiveness, even with severely affected individuals.
“Music Therapist Eirini Alexiou has specialised in working with those with ABI, and along with speech and language therapy, gives another dimension to conventional therapy. Dysarthria is a condition that can be difficult to treat but the use of music and singing can encourage rhythm and a decreased pace of speech, which will help towards the level of intelligibility. The article and case study highlights an established, but sometimes little known therapy, and its effectiveness in helping those with an ABI.”

spontaneous and purposeful behaviour. The sensory assessment then uses 29 different techniques to observe reactions to vision, taste, smell, sound, touch and motor function. The programme involves 10 one-hour sessions within a one-to-three-week period.”
This uniformed approach ensures the patient’s abilities are fully explored, followed by a suggested diagnosis to support the expert physician and team, and formulation of a bespoke rehab programme.
Attention to detailHelen said: “When assessing vision, for one technique we shine a pencil torch in front, to the left and to the right of each eye and record reactions – however small.” Therapists assess sound by recording if a patient looks towards the sound or if they can follow a range of verbal instructions. Another technique explores if the patient can respond to simple instructions by pressing a switch for a yes/no response.
Helen said: “It’s all about repetition of techniques – doing each one 10 times helps us identify patterns. Is the patient sleepier in the afternoon? Are they more responsive sitting up in a chair than in bed? Do they respond better to a photograph? Do they look to the left but not the right?
3 Feature/ SMART Assessment
Detecting even the tiniest response has a positive impact on a patient’s future. And, that’s where the Sensory Modality Assessment & Rehabilitation Technique (SMART) comes in.
Patients with disorders of consciousness are difficult to diagnose. In 1993, the Royal Hospital for Neuro-disability published a paper reviewing 60 patients who were all admitted with a diagnosis of a vegetative state. A staggering 43 per cent was misdiagnosed.
SMART was designed as an intuitive tool to determine the level of response a patient has through a structured sensory programme. Helen recently won an MBE for developing SMART at the hospital.
She said: “SMART assesses sensory motor and communicative responses using a range of sensory stimuli, which encourages positive and meaningful responses.”
SMART has two components. The formal part focuses on sensory techniques and behavioural observation, while the informal part captures information from family and carers.
Helen said: “The formal assessment begins with a 10-minute quiet period, where the assessor categorises the patient’s reflexive,
“One patient was admitted having been in bed for ten years. When provided with a bespoke wheelchair and the right stimuli, the change was incredible. He became more responsive and was able to communicate with his wife for the first time by using technology.”
Family inputA unique feature of SMART is the involvement of relatives, friends and carers. The assessor records their views and observations of the patient’s responses to day-to-day activities. Their unique relationship helps provide an insight into interests and preferences.
Training The Royal Hospital of Neuro-disability offers a specially tailored training programme for others to learn the skill. Health professionals from doctors to occupational therapists across Europe and even Australia attend the course. Once completed, individuals become accredited SMART assessors.
What does the future hold?Helen added: “We are developing a shorter, cost-effective SMART training course for health professionals (who already have accredited assessors in their workplace) to provide support.
“We are also developing a shorter assessment called SMART tracker for use in acute units, prior to a full SMART assessment, and for monitoring patients who have had the full assessment but require regular reviews.”
For further information: www.rhn.org.uk
SMART response to rehab“One patient was admitted having been in bed for ten years. When provided with a bespoke wheelchair and the right stimuli, the change was incredible.”
A SMART assessment is the height of sophistication when it comes to pinpointing evidence of awareness in patients with an Acquired Brain Injury (ABI). Development Consultant Helen Gill-Thwaites (pictured above) discusses how it is helping a condition notoriously difficult to diagnose.

4 Feature/ UKABIF
Manifesto of change
Held at the House of Lords, the manifesto outlined the necessity of acute and early access to rehabilitation for adults with an ABI to ensure optimal recovery; the need for specialist neuro-rehabilitation teams to manage care pathways and the cost implications of not providing adequate rehabilitation.
Lord Walton of Detchant, Crossbench Peer and Neurologist, chaired the launch campaign and spoke at length in support of the manifesto demands. Professor Michael Barnes, Chair of UKABIF, described how the variability of rehabilitation services around the UK is having a detrimental impact on the outcomes of people with an ABI and immediate action and change is required.
An audience of health professionals, MPs and interested charities listened avidly to three people who talked about their very different experiences of rehabilitation programmes.
Ron Payne spoke emotionally on behalf of his wife Heather, who was unable to attend the launch.
He said: “In June 2001, we had just returned from a holiday in Spain when my wife Heather noticed a pain in her left leg. On investigation, it became clear this was a circulation problem and deep vein thrombosis was diagnosed. Unfortunately, a catalogue of events occurred resulting in Heather having hypoxic brain damage.
“Heather’s subsequent rehabilitation in our home county was so inadequate that we eventually moved to Northumberland, where Heather could receive specialist rehabilitation, and I could access the support I needed.
“Heather’s improvement was miraculous. If she could have been discharged into the care of such a service earlier, life could have been so much better.”
Tony Hart from the Surrey-based Queen Elizabeth Foundation (QEF) represented Julie Curtis, who also found it difficult to attend the launch.
Tony said: “Julie’s brain injury was undiagnosed for two years and resulted from a diabetic hypoglycaemic episode. During that time, she lived in chaos and lost her job. Life was very difficult and she didn’t understand why.
“I enlisted Julie on a vocational rehabilitation programme at the QEF, where she started to learn how to deal with her condition.”
James Heather was a pilot for British Airways when he fell eighteen feet over a hotel balcony on to a marble floor. After an emergency operation, James remained in a coma for several weeks and took some time to regain consciousness. He received some physiotherapy and hydrotherapy in hospital and was eventually transferred into a wheelchair.
James moved to Northwick Park Hospital and stayed there for almost a year. He had more intensive physiotherapy treatment, as well as speech therapy and psychological intervention. As a transitional step to returning home, James moved to the transitional living unit at The Royal Hospital for Neuro-disability, in Putney, and followed a goal-centred programme.
James supplemented his therapy with swimming lessons and he worked hard on his speech, taking various private speech and singing lessons. Thanks to a good co-ordinated rehabilitation programme and his own drive and determination, James has made a remarkable recovery. He lives in his own flat, can walk almost normally and works voluntarily for a local charity.
Heart-breaking stories about individuals that struggled to get the help they needed, when they needed it, supported a new hard-hitting campaign ‘Life after brain injury? Improve services now’.
“Heather’s improvement was miraculous. If she could have been discharged into the care of such a service earlier, life could have been so much better.”
Launched at the United Kingdom Acquired Brain Injury Forum (UKABIF) conference earlier this year, this also presented a platform to introduce its manifesto ‘Life after Brain Injury – A Way Forward’.
Attendees at the conference: (from left to right) Professor Michael Barnes, James Heather, Lord Walton, Tony Hart, Ron Payne and Sam Shephard

UKABIF MANIFESTO DEMANDS The manifesto makes
four demands:
5
Acute and early access to specialist neurological services, including specialised neurological rehabilitation at local level, is crucial to ensure optimal recovery. The clinical evidence supports this but the words ‘specialist’ and ‘local’ are not adhered to. Commissioning specialist services has to be carried out by someone with the appropriate knowledge and expertise, like a neurological lead.
Appropriate commissioning for specialist brain injury rehabilitation should be made compulsory and each Cinical Commissioning Group should have a named neurological lead.
Building neuro networks throughout the UK would lead to better commissioning for people with an ABI. A good network is commission led and works collaboratively across agencies, professional groups, user and carer groups and the voluntary and independent sector to help develop a more integrated service. Networks should focus on ensuring appropriate services are routinely commissioned and long-term savings are made.
Funded national neuro networks should be established to ensure neurological pathways are available throughout the stages of recovery (patient journey).
There is very little accurate and reliable data on the provision of healthcare services for people with an ABI. The National Institute for Clinical Excellence estimates the acute hospital care costs for traumatic brain injury are £1 billion annually (this does not include all types of ABI) and Gustavsson et al (2011) stated the overall cost of traumatic brain injury in the UK (and again an underestimate for ABI) was approximately £4.1 billion. Published studies show, by providing rehab the savings made offset the costs, even when rehab is not carried out immediately after injury.
A national audit of rehabilitation should be carried out and the collection and reporting of accurate data on new ABIs made compulsory by all providers along the patient journey, from acute to community services.
In 2001, The Health Select Committee published its third report into head injury (Health Committee 2000-1) with a list of 28 conclusions and recommendations; most have not been acted upon. Although the National Service Framework for Long-term Neurological Conditions has been in place since 2005, very little progress has been made and rehabilitation services continue to vary hugely around the UK.
A review is required of The Health Select Committee Report and the National Service Framework (NSF) for Long-term Neurological Conditions.
Your help is needed To support the campaign, you can ask whether your local Clinical Commissioning Group has a named neurological services lead and if not, request one. Consider joining your local ABI forum – see www.ukabif.org.uk/regional-groups and join in activities to raise the profile of ABI locally. And lastly, make a declaration of your support on www.ukabif.org.uk, clicking on the banner ‘Life After Brain Injury’.
For further information on how to support this campaign, contact: Chloe Hayward T: 0845 608 0788 E: [email protected]

6 Feature/ Clinical Commissioning Groups
What the doctor ordered
Brand new Clinical Commissioning Groups (CCGs) will replace Primary Care Trusts in April 2013, but how it will affect the commissioning of services for people with Acquired Brain Injury (ABI) is yet to be made clear. Cortext starts the conversation by examining how GPs will be at the heart of this.

7
The new CCGs will be led by local clinicians who know their local populations’ needs, and health and wellbeing boards, who will help join up the commissioning of health and social care services.
CCGs are a direct result of the Health & Social Care Act in April 2012, promising a new reform that reduces the layers of bureaucracy and increases clinicians’ influence. With a combined budget of £60 billion, the GP-led CCGs will commission and buy healthcare services, including elective hospital care and emergency care, along with rehabilitation, mental health, learning disability and community health services.
Martin McShane, Director for Domain 2 (enhancing quality of life for people with long-term conditions) at the NHS Commissioning Board, said: “The focus is to have clinicians at the heart of the decision-making process. To look at how money should be used to invest in services – delivering the best possible outcome for people. Putting clinicians at the forefront – giving them the opportunity to influence and make decisions.”
Creative proposition Natasha Curry, a Fellow in health policy at the Nuffield Trust, was involved in a simulation exercise for the new system in her former role at the King’s Fund. She said: “The idea behind
CCGs is to support the development of a more imaginative and creative patient pathway informed by clinicians. The premise is that as the closest link to patients and local communities, GPs have a better understanding of where to allocate services more effectively and the best areas to concentrate the budget.”
Depth of experienceOne burning question is will GPs want more responsibility added to their already stacked workload?
Martin answered: “I believe I can add value because of my GP background, and my GP colleagues have the ability to do this both locally and at the centre. Any reform runs the risk of confusion. But it’s about utilising good people and managing expectations. GPs can bring richness and depth of experience – adding real value to CCGs.”
Natasha believes one real advantage is the potential for collaboration between CCGs – pooling together to commission in a way that supports the integration of services.
She said: “There’s a potential for collaborating across different services, so a patient can go to the same place instead of different departments. It is recognised CCGs might not have the expertise in every form of care and networks
will be formed to bring in specialist expertise.ABI experts, for example, will not sit on each CCG and it is likely groups will work together to buy in more specialist services where necessary.”
How will ABI services be commissioned? Martin answered: “Commissioning of ABI services is an area the NHS Commissioning Board is working on. The idea is to ensure local knowledge and expertise is brought to bear. There’s a lot of work to do to fine tune CCGs and it would be inappropriate to speculate what will happen before they pick up the reins in April 2013.”
Fast forward into the future – what could we see for CCGs? Martin said: “An organisation recognised by local people and local health professionals, supporting the delivery of quality care and meeting the challenges of a health and care system in the 21st century.”
A simulation exercise was conducted two years ago to give a real sense of what the new system might feel like.
The intensive one-day exercise took place in Lincolnshire, assigning approximately 60 people in specific roles, from GPs and hospital managers to roles within CCGs, health and wellbeing boards and local government. The group played out a year, with a different scenario and problem to resolve month by month.
Natasha said: “There were many interesting insights. GPs had to work with financial data on a scale they hadn’t previously been accustomed to, so some weren’t very adept at renegotiating contracts in their favour. One CCG got into financial trouble. And, CCGs were slow in exploring opportunities for collaboration, for example, clubbing together to commission specific services.”
Martin added: “The simulation exercise was a great way of showing people the sheer scale of the task and challenges ahead. It was a helpful exercise. The job now is to encourage professionals to realise their potential and seize the opportunity to help sustain and improve NHS services, by working together and with the NHS Commissioning Board.”
Simulation exercise
“There is a brief opportunity, between now and when CCGs go live, for us to positively influence the way they commission neuro rehab.”
That’s the opinion of Mike Hope, Case Management Co-ordinator for Optua UK and a member of the executive committee for United Kingdom Acquired Brain Injury Forum.
He said: “We are encouraging our members everywhere to attend their local CCG public engagement launch meetings, and raise ABI needs in the context of commissioning a better and more specific neuro rehab pathway. And, to offer to help CCGs design their pathway." Mike believes the problem is many areas are still unclear. What will the specialised National Commissioning Board commission centrally? How will ABI be commissioned under specialised commissioning networks at regional level? What will be left for the CCGs to do? Acute (complex)cases will be commissioned centrally but how will CCGs deal with cases, whose needs are complex but don't meet the central commissioning criteria?
Areas of concern Mike continued: “We are pretty sure there will be a problem with the better commissioning of
services for mild or minor traumatic brain injuries – the 'bumps on the head'. These are those that may not even be admitted to hospital – 70 per cent of which make excellent recoveries.
“There is a specific issue with the 30 per cent who don’t recover, and go on to develop serious behavioural, mental health, criminal justice and social exclusion issues. This is a large group of people, very often not even diagnosed at the time. “There is also a big problem in commissioning services for the 60 plus per cent of ABIs whose brain injury is non-traumatic in origin, and who are very heterogeneous in presentation. They are frequently not adequately diagnosed until some time after the injury – typically getting lost in the system.”
In terms of children and young people, large numbers of cases are under diagnosed or given the wrong diagnosis.
Mike explained: “The very wrong assumption is that often children make better recoveries, when actually the reverse is often the case. Developmental stages are missed due to brain injury, but can stay masked until adolescence and then emerge with a vengeance. There is an extreme lack – even by adult ABI standards – of appropriate rehab resources especially those that work with the family, the school and the child.”
We can make a difference

8 Feature/ Children
Justice for the young
Staggering statistics state more than fifty per cent of youth offenders may have suffered traumatic brain injury – many undiagnosed at some point in their childhood.
Louise Wilkinson, Co-Founder of a UK consortium addressing the issues of brain injury and offending behaviour, spoke candidly about the dire consequences if we don’t act now.
These shocking figures are the result of a research study conducted by Professor Huw Williams – the first of its kind in the UK.
Louise, Child Brain Injury Trust Training Manager, is excited about what this could do for an issue hugely disregarded. She said: “The evidence reinforces what we have known for some time. Brain injury can affect behaviour, and in some cases, lead to offending and/or anti-social behaviour.
“There has been lots of research on an international scale but this is the first time we have real statistics to refer to. It gives us the tools to help create more awareness.”
Typical scenarioImagine a child is involved in a road accident, contracts meningitis or is tragically thrown against a wall at a young age. After spending time in hospital recovering, they are often discharged physically well, with a clean bill of health. They start primary school and do relatively well in their normal mainstream school setting. Their academic performance is typical and they have developed friendships. However, as they move in to Year 7, and to a bigger school, cracks may soon start to appear in their behaviour and performance.
Louise explained: “A child’s brain takes up to 21 years to fully develop. When children reach adolescence, more planning and organisational skills are called upon as they’re expected to go to different classes, manage a homework load, deal with different noisier environments and concentrate for longer periods of time.
“A child with an undiagnosed mild to moderate Acquired Brain Injury (ABI) may struggle with this. They might forget which class they are supposed to be in; get lost; not fully process
all the aspects of homework; forget to hand it in and become tired more quickly.”
If unsupported, their behaviour may start to be affected and they may start getting into trouble, which can lead to fractured relationships with schoolteachers and the child’s peers. In some cases, the deterioration in behaviour can lead to exclusion from school and be the start of greater problems including criminality. It’s not until you start looking back at the child’s history and find that an accident or illness might be a contributing factor to their behaviour.
Louise said: “Part of the issue is there is little awareness of brain injury and how it affects a young person’s behaviour in school. Educational professionals like teachers and special needs co-ordinators receive no specific ABI training, which means that unless you know about ABI, it’s very difficult to address the issues appropriately.”
Symptoms Signs of mild to moderate ABI can be subtle. 90 per cent have no physical traces of disability. On the outside they look like every other child. Typically, it’s how our cognitive and behavioural abilities manifest themselves that cause the majority of the issues. Behaviours, such as being very impulsive, not understanding the consequences of one’s actions, being forgetful and displaying little empathy, are common factors in someone with a mild/moderate brain injury. It is these subtle changes, that if unsupported, may lead a young person to take more risks and enter into the world of antisocial and criminal behaviour.
Louise said: “If a youth offender with an ABI is given a Community Order, their lack of planning and organisational skills means they might forget to go, lose their way or even turn up on a different day. If they breach this, it could result in a custodial sentence.”
Creating awareness Louise was Co-Founder of the Criminal Justice and ABI interest group, chaired by Lord David Ramsbottom, Ex Chief Inspectorate of Prisons. The diverse group brings together the expertise of 15 different organisations including Headway, Prison Reform Trust, Brain Injury Rehabilitation Trust and the Disability Trust. It also boasts a human rights lawyer and specialised ABI defence lawyer.
“There has been lots of research on an international scale but this is the first time we have real statistics to refer to. It gives us the tools to help create more awareness.” The group works with a primary goal of creating awareness of the issues where it matters – across education, health, social care, youth offending services and magistrates.
Louise said: “We work with educators to improve their knowledge and awareness of ABI, behaviours associated with it, strategies they can use in the classroom and what to look out for. Quite often, ABI can be mistaken for ADHD or even Autism. Since 2005, the Child Brain Injury Trust has trained approximately 6,000 professionals across education. In the last three and a half years, we have been creating awareness in the youth offending service.”
One particularly potent story for Louise was meeting a forensic economist whose son, now 22, went through shocking behavioural problems during his adolescent years.
She said: “After eighteen months of suffering, the family paid to see a private neurologist. He discovered the son had suffered a fractured skull aged two. The condition had gone undiagnosed for years!”

9
Commissioning services The new commissioning structure, which replaces Primary Care Trusts and Health Authorities from April 2013, has not yet addressed specific health needs for children with mild to moderate ABI. Louise feels this may lead to more children falling through the gaps without the provision they need to reach their full potential.
In addition, as far as we can see there is no provision for mild to moderate ABI, despite the fact that approximately 89 per cent of children who have an ABI have just this.
Effects to society The lack of provision for non-acute ABI doesn’t just affect the child – it has a wider impact on society.
Louise said: “The group received a grant to produce a policy document on this very topic. From an extreme perspective, a child whose behaviour leads to expulsion from school, time spent in youth offending services, repeat
offending and finally the adult prison system, can cost the state anywhere between £150,000 to £240,000 per year. It’s easy to see how the costs can spiral out of control.
“We need to be intervening earlier and ensuring a continuity of support to put a stop to the current ‘pillar to post mentality’ that appears to be used at the moment. Providing appropriate help and support when and where it is needed is key to finding the right tools and interventions to put in place.”
It’s about creating awareness wherever you can and sometimes it’s the small wins that make all the difference.
Louise said: “In one training session this rang true with a participant who was dealing with a case of grievous bodily harm. She knew the person had a brain injury but didn’t realise the implications. We worked together on the report to present to the magistrates, and rather than a custodial sentence, he received a Community
Childhood acquired brain injury
Order allowing him to access the help and support he badly needed.”
Wish list What’s in store for the future? Louise added: “If I had a wish list, I would like to see education, healthcare and social services combining forces for better provision for young people with an ABI. I’d like better awareness of the condition in the education service; and to make speech and language therapy available when needed not just at pre-school level. Finally, I would like to see more specialist ABI rehab centres for children.
“Family support, along with educational support, are not being considered under the new Clinical Commissioning Groups. The current structure is not great but the new one is likely to meet these needs even less. It could fall to the voluntary sector to fill in the gaps.”
For further information: www.childbraininjurytrust.org.uk
Environmental factors
Well supported
Education (rehabilitation)
Poorly supported
Well supported
Youth offending
Poor neuro and cognitive
rehab
Maximum outcomes achieved
Good neuro and cognitive
rehab
Poorly supported

10 Feature/ Children10
Every corner of life as they know it dramatically changes and families need all the help they can get. That’s where the Brain Injury Hub comes in.
Created by the Children’s Trust, Director of Fundraising and Communication, Liz Haigh-Reeve explained the thinking behind the charity’s new online resource.
Liz said: “We wanted to develop something that helped parents, friends, siblings and educators better understand what Acquired Brain Injury (ABI) is, and the impact it can have.
“The online support centre brings together some 100,000 words of information on childhood brain injury, alongside a forum for parents to share experiences and offer mutual support.”
Top Gear presenter Richard Hammond – who suffered a brain injury during filming – recently gave his backing to the site, incorporating expertise developed over two decades. The project funded entirely by charitable income was a direct response to research with families in the Trust’s care.
Liz said: “Parents of children with an ABI were telling us they couldn’t find the information they needed. We want to make parents the
best advocates for their child, so making help accessible was essential. ”
The hub is set out as a ‘journey’, which breaks down material into different stages – the hospital, rehabilitation, education and teenage years.
“Parents want the basics in the early days of their child’s injury – understanding what is going on at the hospital. But over time, their needs change. They want detailed information about their child’s injury, with practical advice.”
The site has won praise from healthcare professionals in the USA, and was recently accredited with the Department of Health’s ‘kite mark’. Academically referenced throughout, the site features ‘easy read’ versions of its factsheets and is optimised for smartphones. Factsheets on childhood brain injury have begun to go out to neurology centres at hospitals. Each leaflet has a Quick Response code, which is a bar code that parents can scan on their phone to access information.
Liz said: “The site wouldn’t have been what it is without real-life case studies. It’s impossible not to be taken aback by parents’ capacity to cope with enormous changes to their lives with optimism, humour and dignity.”
Parent Katie Moore believes the resource would have been useful when her daughter Molly had a stroke aged six. She said: “We had so many questions about her prognosis, but were given few answers. Having a place to go for support would have made a world of difference – not just to us, but to our daughters, grandparents, teachers and extended family.”
Parents like Katie have begun to congregate on the forum, discussing everything from Bradley Wiggins’s call for compulsory cycle helmets to difficulties of self-awareness. There’s also specific information for education professionals, including practical strategies for the classroom – a place where ABI can often be misunderstood.
The next step is to bring articles from the NHS Choices information site into the Hub, including information on benefits and home adaptations.
Liz concluded: “Our ultimate ambition for the site is to see parents take it over and really make it their own.”
For further information: www.braininjuryhub.co.ukEmail: [email protected]
Hub of help at your fingertipsWhen a child acquires a brain injury, it hits a family like a domino effect. And it doesn’t stop there, but ripples through relationships with grandparents, teachers and friends.
“Our ultimate ambition for the site is to see parents take it over and really make it their own.”
Feature/ Children11 Feature/ Children
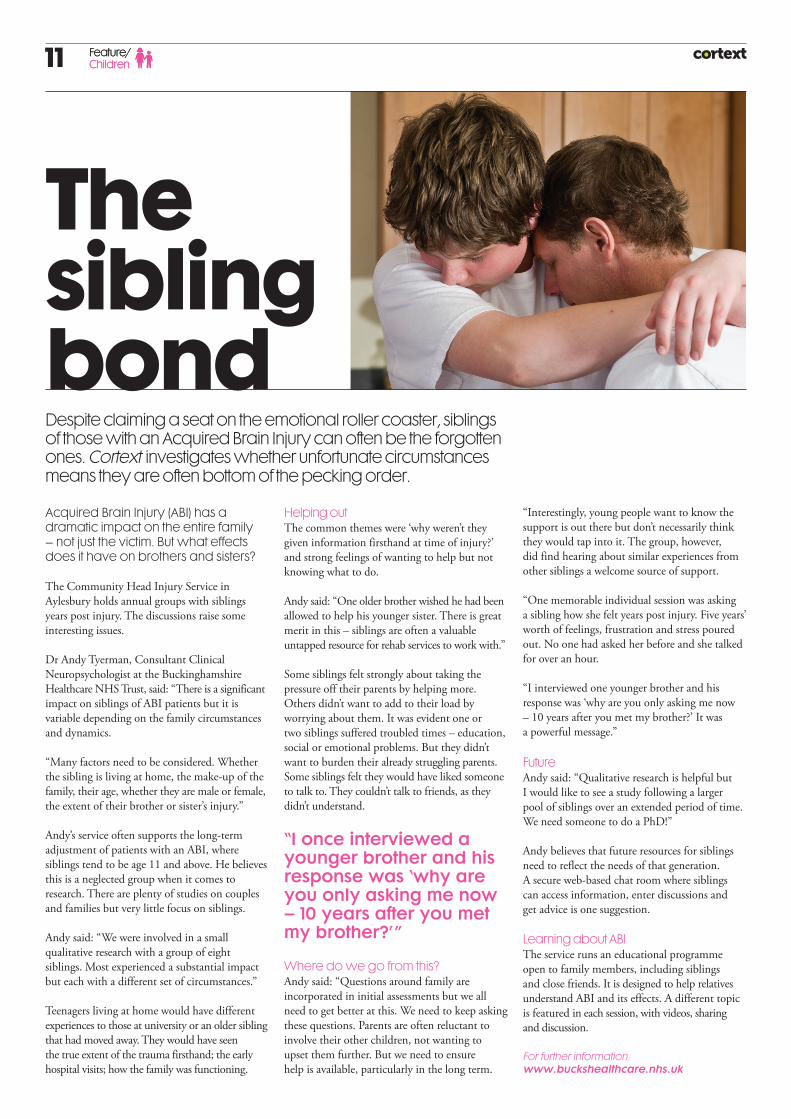
Acquired Brain Injury (ABI) has a dramatic impact on the entire family – not just the victim. But what effects does it have on brothers and sisters?
The Community Head Injury Service in Aylesbury holds annual groups with siblings years post injury. The discussions raise some interesting issues.
Dr Andy Tyerman, Consultant Clinical Neuropsychologist at the Buckinghamshire Healthcare NHS Trust, said: “There is a significant impact on siblings of ABI patients but it is variable depending on the family circumstances and dynamics.
“Many factors need to be considered. Whether the sibling is living at home, the make-up of the family, their age, whether they are male or female, the extent of their brother or sister’s injury.”
Andy’s service often supports the long-term adjustment of patients with an ABI, where siblings tend to be age 11 and above. He believes this is a neglected group when it comes to research. There are plenty of studies on couples and families but very little focus on siblings.
Andy said: “We were involved in a small qualitative research with a group of eight siblings. Most experienced a substantial impact but each with a different set of circumstances.”
Teenagers living at home would have different experiences to those at university or an older sibling that had moved away. They would have seen the true extent of the trauma firsthand; the early hospital visits; how the family was functioning.
Helping outThe common themes were ‘why weren’t they given information firsthand at time of injury?’ and strong feelings of wanting to help but not knowing what to do.
Andy said: “One older brother wished he had been allowed to help his younger sister. There is great merit in this – siblings are often a valuable untapped resource for rehab services to work with.”
Some siblings felt strongly about taking the pressure off their parents by helping more. Others didn’t want to add to their load by worrying about them. It was evident one or two siblings suffered troubled times – education, social or emotional problems. But they didn’t want to burden their already struggling parents. Some siblings felt they would have liked someone to talk to. They couldn’t talk to friends, as they didn’t understand.
“I once interviewed a younger brother and his response was ‘why are you only asking me now – 10 years after you met my brother?’”
Where do we go from this?Andy said: “Questions around family are incorporated in initial assessments but we all need to get better at this. We need to keep asking these questions. Parents are often reluctant to involve their other children, not wanting to upset them further. But we need to ensure help is available, particularly in the long term.
The sibling bondDespite claiming a seat on the emotional roller coaster, siblings of those with an Acquired Brain Injury can often be the forgotten ones. Cortext investigates whether unfortunate circumstances means they are often bottom of the pecking order.
“Interestingly, young people want to know the support is out there but don’t necessarily think they would tap into it. The group, however, did find hearing about similar experiences from other siblings a welcome source of support.
“One memorable individual session was asking a sibling how she felt years post injury. Five years’ worth of feelings, frustration and stress poured out. No one had asked her before and she talked for over an hour.
“I interviewed one younger brother and his response was ‘why are you only asking me now – 10 years after you met my brother?’ It was a powerful message.”
Future Andy said: “Qualitative research is helpful but I would like to see a study following a larger pool of siblings over an extended period of time. We need someone to do a PhD!”
Andy believes that future resources for siblings need to reflect the needs of that generation.A secure web-based chat room where siblings can access information, enter discussions and get advice is one suggestion.
Learning about ABIThe service runs an educational programme open to family members, including siblings and close friends. It is designed to help relatives understand ABI and its effects. A different topic is featured in each session, with videos, sharing and discussion.
For further information: www.buckshealthcare.nhs.uk

12 Industry Profile/ Music Therapy12
Maestro of music therapy
Whether it’s waxing lyrical, strumming a guitar or singing to a beat, music therapy can make a huge difference to those with an ABI.
It’s all about tailoring therapy to the needs of the patient according to Eirini, who has worked as a Music Therapist at the Royal Hospital of Neuro-disability since 2009.
She said: “We use all elements of music to meet an individual’s emotional, physical, social and communication needs. Music therapy helps many walks of life – people with emotional problems, those with special needs or disabilities. I specialise in helping those with brain injury.”
Graduating with a music degree at Cardiff University, Eirini trained as a music therapist at the Royal Welsh College of Music and Drama in 2008. Combining her passion for music and helping people has meant the rewards are rich.
The Royal Hospital of Neuro-disability has provided music therapy for the last 20 years, and has grown in size and expertise – with six therapists, therapy assistants and students.
Developing speechTherapists use music to help people overcome difficulties stemming from a disability, like ABI. It’s powerful stuff as therapy can improve memory and cognition through musical and verbal prompting. It helps develop speech, using music to prompt vocal responses and control breathing. It aids the processing of information, improving memory and building physical abilities.
Eirini said: “Patients are referred to us for specific reasons – it could be cognitive, communication or behavioural problems. We do an assessment and form a treatment programme that takes into account language, speech, memory and building physical abilities.
“Sessions can include singing, voice exercises or instrument improvisations. We will ask the patient to choose an instrument to play. We explore sounds through improvisations and create some music together. It’s not about producing a Beethoven piece but simply being creative.”
Emotional expressionThe sessions last 30 to 45 minutes, once or twice per week. It is very dependent on the patient’s attention span.
Eirini continued: “If we want to focus on emotional expression, we write lyrics and choose music. We have a fantastic software programme, which helps patients to compose music with different sounds and instruments. It’s an effective technique in exploring a patient’s memory, attention span and emotional expression.
“Sometimes we do shared listening where patients select the music, we pre-record it and discuss and reflect. It’s a great opportunity for patients to communicate and interact in a facilitated environment.”
Music therapy sees remarkable results. For example, techniques in music therapy can help patients with Dysarthria (a condition where a person loses control of their muscles) slow down and control their speech better.
Therapists often work with different disciplines, like speech therapists, to help patients on their road to recovery. Family members are even welcome to join in.
Eirini added: “It can take time to see the benefits but patients find sessions fun and motivating. There’s a fun element to music therapy unlike any other. It can take the pressure off and relax, motivate and really bring patients out of themselves.” Case studyMusic therapy helped a father improve speech and reconnect with his children, after a cycling accident left him with a traumatic brain injury.
40-year-old Adrian Smith* suffered communication impairments including poor respiratory function and a speech disorder, which resulted in unclear, slurred speech. He was referred to music therapy to help him work on the clarity and volume of his speech. And, as Adrian used to sing to his children, he was keen to do so again.
Eirini said: “Adrian engaged in oral, motor and respiratory exercises, breathing exercises and playing the recorder. These exercises helped Adrian gain control of his respiratory function. A rhythmic speech cueing technique was also adopted to help decrease his rate of speech.
“Each session, I determined the baseline of Adrian’s speech rate. We read and sang lyrics in time to the metronome, and compiled a CD of songs for Adrian’s children. He selected the songs, practised and recorded them on to a CD. This helped Adrian regain his parental role, and his children enjoyed listening to their dad’s songs.”
Music therapy left Adrian highly motivated, helping him to improve his speech. His singing and speaking voice became clearer and louder, and his aspirations to connect with his children were met.
*Actual name changed to protect identity.
For further information: www.rhn.org.uk
The magic of music is a powerful one and is increasingly being used in the rehabilitation of people suffering with an Acquired Brain Injury (ABI). Eirini Alexiou struck a chord when she told Cortext about her work as a Music Therapist.
“It’s not about producing a Beethoven piece but simply being creative.”

“There’s a fun element to music therapy unlike any other. It can take the pressure off, relax, motivate and really bring patients out of themselves.”
13
Music has always been an important part of life at the Royal Hospital for Neuro-disability.
However, it wasn’t until the early eighties that the first music therapy position was established under the guise of the occupational therapy department. The introduction of a dedicated department took place for the first time in 1993.
When Dr Wendy Magee finished her doctoral research in 1998, it resulted in much-needed funding.
The department has since grown in size and stature – with six part-time music therapists now on the team. All posts are funded through voluntary contributions sourced by the hospital’s fundraising committee and through research.
Music Therapist Eirini Alexiou
Journey through music

14 Feature/ Real Life
Getting back to workWhen Carpenter Gary Smith* was pulled under a van following a collision with his moped, his whole life changed before his eyes.
The severity of the road accident left Gary with an Acquired Brain Injury (ABI), shattered hand and injuries to his ankle resulting in unemployment for six years.
Once his bones had healed, Gary tried to go back to work in the family business but was unable to do his previous job properly. His insurance company paid for Gary to go on the Papworth Vocational & Medical Rehabilitation programme for 12 weeks. A big Bristol City FC fan, Gary stayed weekdays and travelled home at weekends for matches.
Gary said: "The therapies at Papworth were good and I benefited from the vocational aspects of the programme like career software, personal advice around what sort of job would be suitable for me."
When Gary returned home, his rehab programme continued on an ‘outreach’ basis, with his vocational adviser visiting him regularly. Papworth engaged with local employers to find a suitable work placement for Gary to develop his skills and further improve the confidence gained through the various therapies.
"With the support of Papworth, I have been working at Brandon Tool Hire near my home in Bristol which is great," said Gary.
Brandon Tool Hire National Training Manager Jim MacCall said: “Papworth was very supportive of both client and employer interests with excellent communication maintained at all stages. This support continued after the formal processes were completed. Papworth's commitment regarding the client's welfare is commendable."
About PapworthPapworth Trust Vocational & Medical Rehabilitation service is part of the disability charity, Papworth Trust. The Trust delivers a range of services including housing, employment, personal support as well as rehabilitation supporting disabled people.
The rehabilitation service itself works nationally to provide programmes for people with an acquired disability, like ABI, following an accident.
Instructed as part of a personal injury claim, Papworth’s aim is to get an individual work ready or in work by the end of their programme. The multi-disciplinary team includes everything from occupational therapists and physiotherapists to nutritionists and counsellors. The dedicated centre in Papworth Everard, Cambridgeshire, is equipped with a gym, treatment rooms, vocational delivery area and accommodation.
Programmes are tailored to client needs addressing vocational, medical and life skills rehabilitation, including social therapy and work therapy. Papworth works with clients, their existing healthcare providers and families to overcome difficulties and barriers experienced since their accident.
Funding for services is often difficult to find and Papworth works predominantly within the personal injury arena. It is happy to talk to clients and their families to see if there is a way that an individual can move forward with us.
Additional supportPapworth offers support through centre-based and outreach programmes to assist those affected by ABI. This can be through interventions with existing employers to act as an intermediary facilitating changes to allow an individual to return to the workplace; organise centre-based support to take clients out of their environment and provide support to them and their families to move forward with their lives.
*Actual name changed to protect identity .
For further information:www.papworthtrustrehab.org.ukwww.headway.org.ukwww.apil.org.uk
"With the support of Papworth, I have been working at Brandon Tool Hire near my home in Bristol which is great."

15
Just two years later, Yoki’s life is truly transformed – thanks to her sheer determination and infectious sense of humour.
Diagnosed with an infection, which resulted in a brain injury in 2010, Yoki was treated at the Royal Hospital for Neuro-disability before moving to 1 Sewardstone Close, a specialist Acquired Brain Injury (ABI) home based near Waltham Abbey, Essex. Yoki’s injury caused her to experience weakness, uncontrolled movement, decreased proprioception, moderate dysarthria and a low volume when speaking.
Thanks to 1 Sewardstone Close’s experienced neuro-rehabilitation specialists and modern and spacious accommodation, Yoki settled in immediately.
Yoki required assistance transferring to a bed, wheelchair and toilet. Her reduced strength and fitness meant she could only use a wheelchair independently for short distances indoors, but required help outdoors and during community visits.
Suffering frustration Simon Berrell, Clinical Specialist Physiotherapist, said: “Yoki’s lack of confidence and fear of movement created a dependency on others. She found her aspiration to study law, and engage in a potential career as a model, had been taken away by her neurological damage. Plus, the frustration of not being able to perform everyday tasks independently.”
Simon added: “One of Yoki’s aspirations was to walk independently and achieve independence with daily living activities again. We set realistic
goals together and praised every achievement with positive reinforcement. After a few months, however, Yoki experienced a reduction in confidence and withdrew from therapeutic interventions.”
Through patience, understanding and positive guidance by the clinical psychologist, Yoki was encouraged back into a therapeutic mindset and became re-engaged in the rehabilitation process.
Positive attitude Yoki continues to strive towards her goal of independent walking and works hard using the fully equipped gym, which incorporates parallel bars and specialist cycling machines.
“Yoki’s attitude is more positive. Her newfound confidence has resulted in increased speech volume and improvements with her dysarthria. Yoki is looking into studying for a qualification in law, and has independently registered with a modelling agency.”
Model pupil1 Sewardstone Close is supporting Yoki with attending external appointments for hair, make-up and photo-shoots, which is enhancing her confidence further. Yoki attends some appointments independently now with only distant support when required.
Again due to greater self-belief, Yoki has become independent in all transfers to her wheelchair and with washing and dressing. Her love for shopping continues and Yoki regularly attends girlie shopping trips with the team!
For further information: www.enablecare.co.uk
Life after injury
A traumatic brain injury shattered Yoki Mekuria’s aspirations of modelling and studying law, leading to a downward spiral of reduced confidence and independence.
“Thanks to 1 Sewardstone Close’s experienced neuro-rehabilitation specialists and modern and spacious accommodation, Yoki settled in immediately.”
Profile/ Rehab

Enable Publishing3rd Floor, The Courtyard7 Francis GroveWimbledonLondon SW19 4DW
For further information and all enquiries:Tel. 0845 190 [email protected]
Cortext has been brought to you by Enable Publishing.
Cortext is designed and produced by Design Culture Associates Ltd and is printed on sustainably sourced material, using vegetable and soya based inks.