Embed Size (px)
Citation preview

Coronary inflow after systemic-to-coronary artery anastomosis in dogs
Hans H. Schuldt, M.D.* Harm Krause, Ph.D.
Berlin, Germany
B ecause of the fact that the morbidity and mortality of stenosing coronary
diseases recorded in the statistics on heart troubles have been increasing at an alarm- ing rate in almost all industrialized coun- tries since World War II, therapy research in this field has been intensified during the last decade. Since the prerequisites for a coronary-dilating, collateral-circulation-in- ducing effect by drugs are mostly limited in the case of advanced structural lesions of the walls with a reduced flexibility and high-grade narrowing, the demand for adequate surgical measures to be ap- plied to such patients is becoming more urgent.
Whereas indirect methods for the revas- cularization of the ischemic myocardium, such as cardiopexy with extracardiac struc- tures containing vessels, hyperemization of the cardiac surface by producing a sterile epicarditis, arterialization of the coronary venous system, implantation of the internal mammary artery into the myocardium, or bilateral ligature of the latter, have not yet yielded any convincing results in ani- mal experiments and in clinical practice, direct surgical interventions on the coro- nary arteries appear to promise more suc- cess, in so far as the segmental stenoses of main branches are concerned. In addition
Received for publication Dec. 16, 1965. *Address: Department of Experimental Cardiac and
Friedrichshain. Berlin 1017, Germany.
359
to efforts made toward removing stenosis of the lumen by curettage, endarterectomy, and dilation of the stenotic ring by means of a patch graft, numerous experiments have been aimed at overcoming the seg- mental narrowing by creating an anasto- mosis between an arterial branch of the arotic arch and the coronary stem beyond the stenosis. The shunting was made via mobilized arteries, 1-22 arterial or venous vascular grafts,2,4-6,10,12,23 or prosthetic vessels? ,24 Although such experiments have partially led to satisfactory laboratory re- sults, a clinical application has hitherto been condemned to failure because of the high percentage of thrombosis occurring in the vascular shunts of small caliber. This may well account for the fact that, so far, experimenters in this field have almost invariably confined themselves to the surgical problem of the suturing technique to be applied, whereas the functional be- havior of anastomoses was dealt with merely in a general clinical respect. Thus, no publication yet exists which describes the peculiar hemodynamic conditions in systemic-to-coronary artery anastomoses.
This paper reports on experiments in which the coronary inflow in dog hearts was examined prior to and after the shunt- ing with systemic arteries.
Vascular Surgery, German Academy of Sciences, Hospital am

360 S c h u l d t a n d K r a u s e A,,. Hera J. September, 196~;
Methods The studies were performed on 25 mon-
grel dogs weighing 24 to 28 kilograms. Morphine was applied as a preanesthetic, and anesthesia was induced with sodium barbital (approximately 30 mg. per kilo- gram). The respiration was maintained by means of a mechanical insufflator via a cuffed endotracheal tube using fresh air. The thorax was opened in the fifth left intercostal space, with the animal on its right side. After the pericardium had been opened above the auriculoventricular sul- cus, the Circumflex branch of the left coro- nary ar tery was exposed from its origin to the site of branching of the ramus marginis obtusi anterior. This resulted in a segment of about 4 cm. in length which was freed from small tributaries, as well as from the ramus descendens ventriculi sinistri. If the latter was of large size, which would have meant the formation of an extensive area of infarction, the animal was used for other experimental purposes. The main branch to the septum and the proximal auricular branch were carefully spared. The coronary anastomosis was performed with the left subclavian ar tery mobilized directly or via the left internal mammary ar tery or a rubber tube having a 3-ram. inner diameter, which was joined with the left subclavian ar tery at the site of branching of the mam- mary ar tery via a short prosthetic tube of the same diameter. The wall of this model vascular tube was shaped in such a fashion that , in the coronary region of measure- ment, identical formal criteria of the pres- sure and flow pulses were fulfilled as in shunting with the subclavian ar tery or mammary artery, so that similar volume elastic effects could be assumed in the ar- terial pressure region. After the vessels selected had been dissected free, the dog was heparinized intravenously in order to maintain a constant level (initial dose 5 rag. per kilogram).
The anastomosis was applied to the nor- really beating heart, using a thin-walled brass tube, the diameter of which was adapted to the smallest of the two shunt- ing vessels (varying in these experiments between 2.2 and 3 mm.), and the length of which was 18 ram. This tube served at the same time for both pressure and flow measurements, according to the differential
pressure method. For this purpose it was provided with two lateral pipes, 0.8 rnm. in diameter and 10 ram. in length, which were at tached 8 to 10 ram. apar t and connected each with the measuring chamber of Sta tham P23Gb transducers via flexible in- elastic tubes. The transmission of pressure from the blood channel to the recipient membranes of the strain gauges was thus accomplished through the lateral pipes, the inelastic tubes, and the measuring cham- bers of the transducers; this system was filled with physiologic saline free of bubbles. With the given diameters of tile measuring tubes, the distance of 8 to 10 mm. between the pipes was sufficient to obtain measur- able pressure differentials with arterial blood speeds. The pressure differentiation was accomplished by compensation of the two Sta tham transducers, which were of similar pressure sensitivity. The flow zero was determined mechanically by means of two three-way stopcocks which were ar- ranged between the inelastic tubes and the measuring chambers, and which could be changed over in such a way that the strain gauges became adjusted to atmospheric pressure, and the column of fluid between the blood channel and the transducer was simultaneously interrupted. The nat- ural frequency of the manometric system amounted to 500 c.p.s.
Since the pressure and inflow conditions of the left circumflex ar tery had to be ex- amined al ternatively for comparison under original and extracardiac blood supply, the anastomosing measuring tube had to be shaped in such a manner tha t it could con- nect the peripherial portion of the coronary ar tery with both the central portion and the systemic shunting vessel. The measur- ing tube used consisted of two parts, each provided with a lateral pipe and fitted into one another by means of a gap-less joint. The two parts when fitted together formed the measuring tube of the above-stated di- mensions. The central component tube existed in duplicate, one being inserted into the extracardiac shunting vessel, and the other into the central portion of the coro- nary artery. Thus, it was possible to adjust the pa thway of the coronary blood supply as desired by a simple plugging over of the peripherial component tube to one of the two others; tile free supply ar tery was

Volume 72 Coronary inflow after systemic-to-coronary artery anastomosis 3 61 Number 3
clamped during this time. Particular care had to be taken that the measuring tube was always in a horizontal position on the surface of the heart.
In order to minimize the time of inter- ruption of blood flow when the tubes were being joined, the composite measuring tube was at first connected with the extracardiac vessel. Then, the circumflex branch was ligated in two places in the middle third of the mobilized distance and was inter- sected between these, and the free end of the measuring tube was inserted into the peripherial stump. In general, this pro- cedure took no more than 60 seconds. Finally, the remaining central component tube could be inserted easily into the clamped central stump of the circumflex branch.
In addition to the absolute and differen- tial coronary pressure, the pressure of the left ventricle, that of the aortic bulb, and that of the coronary sinus were optically recorded via puncturing needles or short catheters which were inserted intrathoraci- cally.
Since the relationship between speed and pressure differentials is not the same in phasic flows as in stationary ones, 25 a gaug- ing under dynamic conditions was neces- sary. For this purpose we used an artificial partial circulatory system which permitted simulation of the hemodynamic situations of the arterial system and, in addition, the recording of outflow measurements. This arrangement produced a pulsating flow, the amplitude, shape, and time course of which were similar to the original coronary flow pulse of the tested animal.* Gauging was based on the relationship between the integral of the recorded flow curve and the outflow of blood during the registration. Since the measurement of the differential pressure is particularly sensitive in response to changes in viscosity, gauging was car- ried out immediately after the experiment
*The ad jus t ing device was constructed as described previously by Ph. Broemser (Ztschr. Biol. 88:296, 1929). However , the rhy thmic inflow of Mood was not controlled by a ro- t a t i ng stopcock, bu t by an e lectromagnet ic in te r rup te r which could be opened and closed at var iable periods. The changes in the outflow resistance were not accomplished in the original r igid way by v a r y i n g degrees of opening a cock, bu t by a te rmina l spr ing-supported throt t le flap which exerts an adius tahle elast ic counteract ion.
with the arterial blood of the still-living dog.
Critique of methodology In so far as the determination of the
phasic flow of heterogeneous fluids from the static differential pressure is concerned, neither a generally valid theory nor any physical experiments exist from which the expected precision of measurement can be calculated. The respective theoretical con- siderations are based on the fundamental equations of hydrodynamics according to Euler (1755) and Navier-Stocke (1845), the former referring to ideal fluids, the latter to viscous fluids. Frank 25 developed his func- tional equations for measuring the dif- ferential pressure from Euler's fundamental equations, whereas the equations formu- lated by Navier-Stocke led to the Hagen- Poiseuille law which is valid for stationary flows in rigid tubes. Thus, these equations represent but starting points for the com- plicated case of measuring the phasic flow of viscous fluids from the differential pres- sure. Therefore, this method can be judged only empirically at present. In agreement with Gregg and his associatesy ,2s we were able to conclude from comparative meas- urements in the laboratory, using electro- magnetic flow meters, that a sufficient time-resolving power and an acceptable reproduction of the amplitudes can be achieved, although this measuring and gauging method does not give absolute evidence of the actual flow conditions. For the present experiments, the measurement of the differential pressure, as opposed to the electromagnetic method, offered the advantage of simultaneous recording of the flow and pressure pulses in the same area of blood flow.
Since the internal cross section of the measuring tube corresponds to the lumen of the shunting vessels, no essential dy- namic repercussions on local circulation can arise. In order to prevent inflow dis- turbances, the arterial inflow and outflow distances must be located in one and the same straight line. With extracardiac blood sources in the region of the aortic arch this is only possible if the circumflex branch of the left coronary artery is shunted (see Fig. 1).
3 62 S c h u l d t a n d K r a u s e ..i,,. He~,.t J
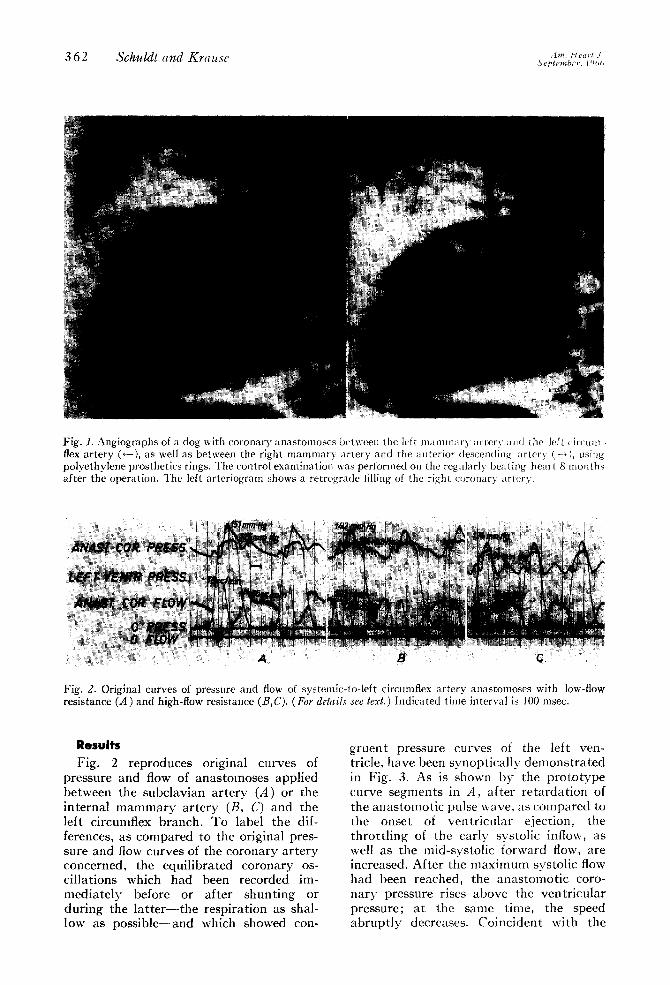
Fig. 1. Angiographs of a dog with coronary anastomoses between the left mammary artcr 5 and the left cir~ tim - flex artery (~-), as well as between the right mammary artery and the anterior descendin~ artery (-~), usi~lg polyethylene prosthetics rings. The control examination was performed on the regularly beatil~g heart 8 mouths after the operation. The left arteriogram shows a retrograde filling of the right coronary artery.
Fig. 2. Original curves of pressure and flow of systemic-to-left circumflex artery anastomoses with low-flow resistance (A) and high-flow resistance (B,C). (For details see text.) Indicated time interval is 100 msec.
Results Fig. 2 r e p r o d u c e s o r ig ina l cu rves of
p ressu re and flow of a n a s t o m o s e s a p p l i e d be tween the s u b c l a v i a n a r t e r y (A) or the i n t e rna l m a m m a r y a r t e r y (/3, C) and the lef t c i rcumflex b ranch . T o labe l the dif- ferences, as c o m p a r e d to the or ig ina l pres- sure and flow curves of the c o r o n a r y a r t e r y conce rned , the equ i l i b r a t ed c o r o n a r y os- c i l l a t ions which had been recorded im- m e d i a t e l y before or a f t e r s h u n t i n g or d u r i n g the l a t t e r - - t h e r e sp i r a t i on as shal- low as p o s s i b l e - - a n d which showed con-
g r u e n t p ressure curves of the lef t ven- tr icle, h a v e been s y n o p t i c a l l y d e m o n s t r a t e d in Fig . 3. As is shown b y the p r o t o t y p e curve s e g m e n t s in A , a f t e r r e t a r d a t i o n of the a n a s t o m o t i c pulse wave , as c o m p a r e d to the onse t of v e n t r i c u l a r e jec t ion , the t h r o t t l i n g of the ea r ly sys to l ic inflow, as well as the mid - sys to l i c fo rward flow, a re increased . A f t e r the m a x i m u m sys to l i c flow had been reached , the a n a s t o m o t i c c o r o - n a r y p re s su re r ises a b o v e the v e n t r i c u l a r p ressure ; a t the s ame t ime , the speed a b r u p t l y decreases . C o i n c i d e n t wi th the
Volume 72 Coronary inflow after systemic-to-coronary artery anastomosis 3 63 Number 3
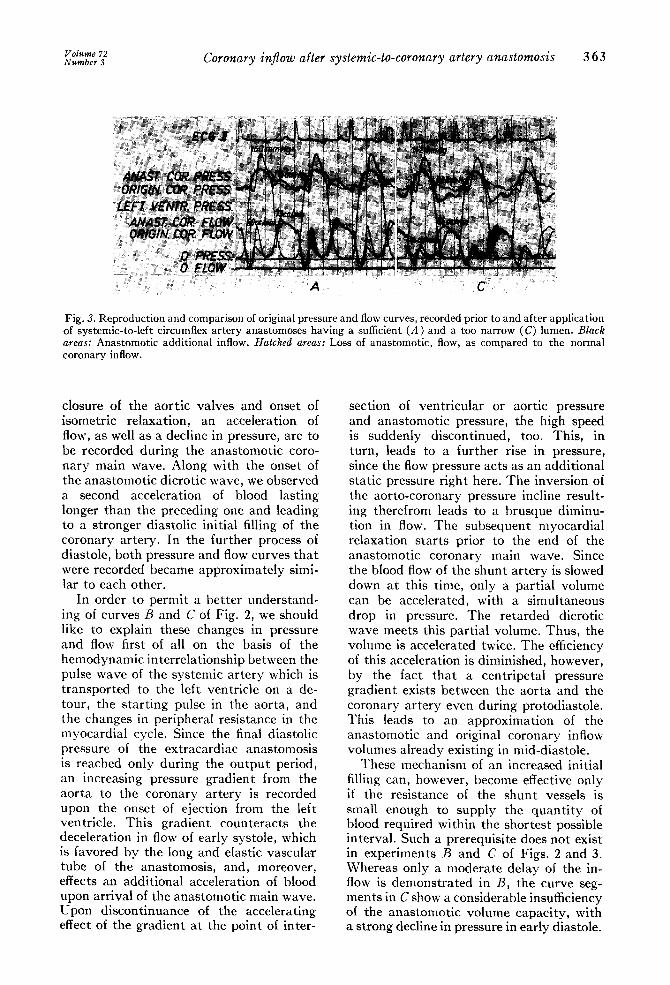
Fig. 3. Reproduction and comparison of original pressure and flow curves, recorded prior to and after application of systemic-to-left circumflex artery anastomoses having a sufficient (A) and a too narrow (C) lumen. Black areas: Anastomotic additional inflow. Hatched areas: Loss of anastomotic, flow, as compared to the normal coronary inflow.
closure of the aort ic valves and onset of isometric relaxation, an acceleration of flow, as well as a decline in pressure, are to be recorded during the anastomotic coro- nary main wave. Along with the onset of the anastomotic dicrotic wave, we observed a second acceleration of blood lasting longer than the preceding one and leading to a stronger diastolic initial filling of the coronary artery. In the further process of diastole, both pressure and flow curves tha t were recorded became approximately simi- lar to each other.
In order to permit a be t te r understand- ing of curves B and C of Fig. 2, we should like to explain these changes in pressure and flow first of all on the basis of the hemodynamic interrelationship between the pulse wave of the systemic ar tery which is t ransported to the left ventricle on a de- tour, the start ing pulse in the aorta, and the changes in peripheral resistance in the myocardial cycle. Since the final diastolic pressure of the extracardiac anastomosis is reached only during the ou tpu t period, an increasing pressure gradient from the aorta to the coronary ar tery is recorded upon the onset of ejection from the left ventricle. This gradient counteracts the deceleration in flow of early systole, which is favored by the long and elastic vascular tube of the anastomosis, and, moreover, effects an additional acceleration of blood upon arrival of the anastomotic main wave. Upon discontinuance of the accelerating effect of the gradient at the point of inter-
section of ventr icular or aortic pressure and anastomotic pressure, the high speed is suddenly discontinued, too. This, in turn, leads to a further rise in pressure, since the flow pressure acts as an additional static pressure right here. The inversion of the aorto-coronary pressure incline result- ing therefrom leads to a brusque diminu- tion in flow. The subsequent myocardial relaxation starts prior to the end of the anastomotic coronary main wave. Since the blood flow of the shunt ar tery is slowed down at this time, only a partial volume can be accelerated, with a simultaneous drop in pressure. The retarded dicrotic wave meets this partial volume. Thus, the volume is accelerated twice. The efficiency of this acceleration is diminished, however, by the fact tha t a centripetal pressure gradient exists between the aorta and the coronary ar tery even during protodiastole. This leads to an approximation of the anastomotic and original coronary inflow volumes already existing in mid-diastole.
These mechanism of an increased initial filling can, however, become effective only if the resistance of the shunt vessels is small enough to supply the quant i ty of blood required within the shortest possible interval. Such a prerequisite does not exist in experiments B and C of Figs. 2 and 3. Whereas only a moderate delay of the in- flow is demonstra ted in B, the curve seg- ments in C show a considerable insufficiency of the anastomotic volume capacity, with a strong decline in pressure in early diastole.

364 S c h u ~ t and K r a u s e A., n~=. s Y e p t e m b e r , 1 9 6 6
So as to be able to estimate the influence of the distance of the shunt pa thway upon coronary inflow, the planimetry values of the anastomotic flow curves and the cor- responding time values of the aorto- coronary pulse re tardat ion ascertained by 74 individual measurements made in 6 suitable dogs were put into relationship with one another. Three of these animals belonged to an experimental series in which the model vascular tube with an internal diameter of 3 ram. was inserted between the origin of the left internal mammary ar tery and the left circumflex branch, being systematically shortened after each double measurement. The other 3 dogs were taken from a second experi- mental group in which analogous measure- nlents were made. Here, the mammary ar tery served as the shunt vessel. As for the physical parameters which may spon- taneously change the coronary inflow in the reproduction experiments having a regular supply of oxygen to the myocar- dium, these above all had to be approxi- mately constant: the aortic and coronary- venous pressure, the systolic and diastolic inflow periods, the coronary inflow under natural conditions, as well as the coronary resistance, which can be est imated from the mean diastolic aortic pressure minus the "critical closing pressure," and the myocardial circulation per minute per 100 gramsY The mean durat ion of a cardiac cvcle approximated 523 msec. (4- 3.8 per
cent). The diastolic aortic pressure effective for the coronary perfusion ranged from 75 to 79 ram. t lg, with amplitudes from 37 to 42 ram. Hg. The mean coronary sinus pressure amounted to 8.8 mln. Hg 4- 9 per cent (max.) or 2.l rain. Hg 4- 28 per cent (rain.), respectively, under natural arterial inflow conditions, so as to part ly rise again after application of the anasto- mosis. (The behavior of the coronary- venous blood flow in the case of extra- cardiac anastomoses is now 1)eing investi- gated in detail.)
The time-volume relationships of the anastomoses with the model vascular tubes (~l) and with the mammary ar tery (b) are graphically demonstrated in l:ig. 4. The ordinates state the percentage surface dif- ference, as compared to the original coro- nary flow curve; this comparat ive value is assumed to anlount to 100 per cent. I t turned out that in both experimental groups the systolic inflow was relatively more strongly affected by retardat ion of the anastomotic pulse wave than by the diastolic blood flow. Because of the con- siderable acceleration of blood in mid- systole the blood flow recorded during the ou tpu t period in the tubes amounted to a pulse lag of 55 msec., and in the narrow- lumen arteries, pulse lags of 36 to 43 msec. al/ove the corresponding coronary value. ()nly after these times have been exceeded does the prolonged duration of the early systolic thrott l ing of the blood flow have a
140
120
;4100
80 i....
so
%
a =-e.2
~',.~ -..., . . . . . . . . . . . . .
o 8,
~ o
No
I / i 1 I 20 ~0 60 80 100 20
PHASIC DISPLACEMENT-ms
T T ~ I
"-.~'k,,
60 80 100
Fig. 4. Graph indicating, as percentage, the changes in flow of coronary-to-systemlc ar tery anastomoses in systole (dashed lines) and in diastole (solid lines) with different phase displacement between the pulse waves of the aorta and those of the coronary artery, a, Anastomoses with low-flow resistance, b, Anastomoses with high- flow resistance.
Vot, m~ 72 Coronary inflow after systemic-to-coronary artery anastomosis 3 65 N u m b e r 3
100 , , , , ,
(~
so
o~
o;:
Io
0 3 0 0
/ . f
i i i i i i i i i
400 5 0 0 600 7 0 0 8 0 0 H E A R T RATE - m s
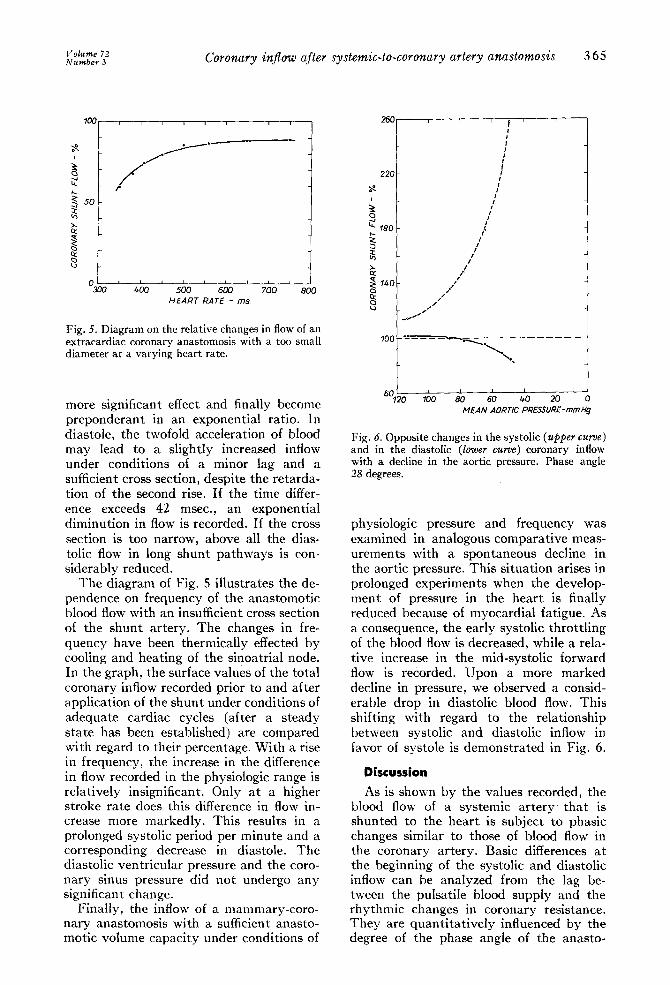
Fig. 5. Diagram on the relative changes in flow of an extracardiac coronary anastomosis with a too small diameter at a varying heart rate.
more significant effect and finally become preponderant in an exponential ratio. In diastole, the twofold acceleration of blood may lead to a slightly increased inflow under conditions of a minor lag and a sufficient cross section, despite the retarda- tion of the second rise. If the time differ- ence exceeds 42 msec., an exponential diminution in flow is recorded. If the cross section is too narrow, above all the dias- tolic flow in long shunt pathways is con- siderably reduced.
The diagram of Fig. 5 illustrates the de- pendence on frequency of the anastomotic blood flow with an insufficient cross section of the shunt artery. The changes in fre- quency have been thermically effected by cooling and heating of the sinoatrial node. In the graph, the surface values of the total coronary inflow recorded prior to and after application of the shunt under conditions of adequate cardiac cycles (after a steady state has been established) are compared with regard to their percentage. With a rise in frequency, the increase in the difference in flow recorded in the physiologic range is relatively insignificant. Only at a higher stroke rate does this difference in flow in- crease more markedly. This results in a prolonged systolic period per minute and a corresponding decrease in diastole. The diastolic ventricular pressure and the coro- nary sinus pressure did not undergo any significant change.
Finally, the inflow of a mammary-coro- nary anastomosis with a sufficient anasto- motic volume capacity under conditions of
2 6 0
2 2 0
is0
to
g
1 0 0
I
I
I
t
/
g
I
/
, # /
. . . . . . . ~, . ~ ,
% ' ' ' ' b 6 0 100 80 60 #0 2
MEAN AORTIC PRESSURE-mmHg
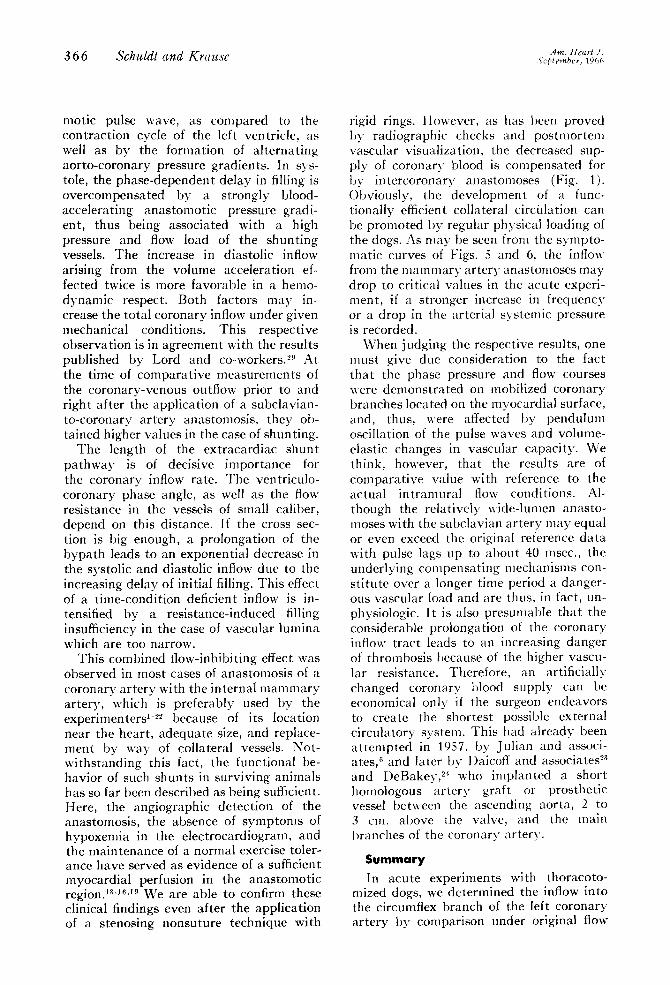
Fig. 6. Opposite changes in the systolic (upper curve) and in the diastolic (lower curve) coronary inflow with a decline in the aortic pressure. Phase angle 28 degrees.
physiologic pressure and frequency was examined in analogous comparat ive meas- urements with a spontaneous decline in the aortic pressure. This situation arises in prolonged experiments when the develop- ment of pressure in the hear t is finally reduced because of myocardial fatigue. As a consequence, the early systolic throt t l ing of the blood flow is decreased, while a rela- tive increase in the mid-systolic forward flow is recorded. Upon a more marked decline in pressure, we observed a consid- erable drop in diastolic blood flow. This shifting with regard to the relationship between systolic and diastolic inflow in favor of systole is demonstrated in Fig. 6.
Discussion
As is shown by the values recorded, the blood flow of a systemic ar tery tha t is shunted to the hear t is subject to phasic changes similar to those of blood flow in the coronary artery. Basic differences at the beginning of the systolic and diastolic inflow can be analyzed from the lag be- tween the pulsatile blood supply and the rhythmic changes in coronary resistance. They are quant i ta t ive ly influenced by the degree of the phase angle of the anasto-
A m . H e a r t .f, 3 6 6 Schuldt and Krause s,,pt~,,b~. 19~,,~
motic pulse wave, as compared to the contraction cycle of the left ventricle, as well as by the formation of alternating aorto-coronary pressure gradients. In sys- tole, the phase-dependent delay in filling is overcompensated by a strongly blood- accelerating anastomotic pressure gradi- ent, thus being associated with a high pressure and flow load of the shunting vessels. The increase in diastolic inflow arising from the volume acceleration ef- fected twice is more favorable in a hemo- dynamic respect. Both factors may in- crease the total coronary inflow under given mechanical conditions. This respective observation is in agreement with the results published by Lord and co-workers. 29 At the time of comparative measurements of the coronary-venous outflow prior to and right after the application of a subclavian- to-coronary artery anastomosis, they ob- tained higher values in the case of shunting.
The length o[ the extracardiac shunt pathway is of decisive importance for the coronary inflow rate. The ventriculo- coronary phase angle, as well as the flow resistance in the vessels of small caliber, depend on this distance. If the cross sec- tion is big enough, a prolongation of the bypath leads to an exponential decrease in the systolic and diastolic inflow due to the increasing delay of initial filling. This effect of a time-condition deficient inflow is in- tensified by a resistance-induced filling insufficiency in the case of vascular lumina which are too narrow.
This combined flow-inhibiting effect was observed in most cases of anastomosis of a coronary artery with the internal mammary artery, which is preferably used by the experimenters ~-2~ because of its location near the heart, adequate size, and replace- ment by way of collateral vessels. Not- withstanding this fact, the functional be- havior of such shunts in surviving animals has so far been described as being sufficient. Here, the angiographic detection of the anastomosis, the absence of symptoms of hypoxemia in the electrocardiogram, and the maintenance of a normal exercise toler- ance have served as evidence of a sufficient myocardial perfusion in the anastomotic regionJ a-1<~9 We are able to confirm these clinical findings even after the application of a stenosing nonsuture technique with
rigid rings. However, as has been proved by radiographic checks and postmortem vascular visualization, the decreased sup- ply of coronary' blood is compensated for by intercoronary anastomoses (Fig. 1). Obviously, the development of a func- tionally efficient collateral circulation can be promoted by regular physical loading of the dogs. As may be seen from the sympto- matic curves of Figs. 5 and 6, the inflow from the mammary artery anastomoses may drop to critical values in the acute experi- ment, if a stronger increase in frequency or a drop in the arterial systemic pressure is recorded.
When judging the respective results, one must give due consideration to the fact that the phase pressure and flow courses were demonstrated on mobilized coronary branches located on the myocardial surface, and, thus, were affected by pendulum oscillation of the pulse waves and volume- elastic changes in vascular capacity. We think, however, that the results are of comparative value with reference to the actual intramural flow conditions. Al- though the relatively wide-lumen anasto- moses with the subclavian artery may equal or even exceed the original reference data with pulse lags up to about 40 msec., the underlying compensating mechanisms con- stitute over a longer time period a danger- ous vascular load and are thus, in fact, un- physiologic. It is also presumable that the considerable prolongation of the coronary inflow tract leads to an increasing danger of thrombosis because of the higher vascu- lar resistance. Therefore, an artificially changed coronary blood supply can be economical only if the surgeon endeavors to create the shortest possible external circulatory system. This had already been attempted in 19.57, by Julian and associ- ates, 6 and later by Daicoff and associates 2a and DeBakey, 24 who implanted a short homologous artery graft or prosthetic vessel between the ascending aorta, 2 to 3 cm. above the valve, and the main branches of the coronary artery.
Summary In acute experiments with thoracoto-
mized dogs, we determined the inflow into the circumflex branch of the left coronary artery by comparison under original flow
Vol~,~ 72 Coronary inflow after systemic-to-coronary artery anastomosis 3 6 7 ,Vumber 3
c o n d i t i o n s a n d a f t e r a n a s t o m o s i n g wi th s y s t e m i c a r t e r i e s of v a r y i n g l eng th a n d cross sec t ion , us ing the lef t s u b c l a v i a n a r t e r y , t he lef t i n t e r n a l m a m m a r y a r t e r y , or, in l ieu of t he l a t t e r , m o d e l v a s c u l a r t u b e s wi th s imi la r e las t i c p rope r t i e s .
As has been p roved , the p r o l o n g e d p a t h - w a y of the c o r o n a r y pulse wave a n d the r e s i s t a n t a n d a c c e l e r a t i v e forces of the lef t v e n t r i c l e l ead to b o t h a sys to l i c a n d a d i a s to l i c in i t i a l def ic iency of fill ing and to a s u b s e q u e n t a d d i t i o n a l inflow, as c o m p a r e d to the n a t u r a l c o r o n a r y flow. P r o v i d e d t h a t the cross sec t ion of the e x t r a c a r d i a c s h u n t - ing vessel is sufficient , the a lgeb ra i c dif- fe rence b e t w e e n b o t h v a l u e s d e p e n d s on the degree of the phase d i s p l a c e m e n t be tween the o n s e t of the v e n t r i c u l a r o u t p u t pe r iod and the a r r i va l of the c o r o n a r y pulse wave on a de tou r . In the p r e s e n t e x p e r i m e n t s , the v e n t r i c u l o - c o r o n a r y or a o r t o - c o r o n a r y phase angle r equ i red for an a d e q u a t e sys- t e m i c - t o - c o r o n a r y a r t e r y inflow was be low 38 degrees (55 mesc.) for sys to le and below 29 degrees (42 msec.) for d ias to le . W h e n these va lue s a re exceeded , the inflow d r o p s in the shape of an e x p o n e n t i a l func t ion .
W h e n the i n t e r n a l d i a m e t e r of the ex t r a - c a r d i a c s h u n t i n g vessel was too smal l (below, say, 2.5 ram.) , t hen the mid- sys to l i c and p r o t o d i a s t o l i c inflows were r e d u c e d even wi th the s h o r t e s t poss ib le b y p a t h b e t w e e n the s u b c l a v i a n a r t e r y and the c o r o n a r y a r t e r y , caus ing a r e d u c t i o n in t he t o t a l inflow r a t e in c o m p a r i s o n wi th the n a t u r a l va lues . In the chronic e x p e r i m e n t , the phys io log ic r ange of r egu l a t i on of the c o r o n a r y s y s t e m wi th such a n a s t o m o s e s can , however , be m a i n t a i n e d by the for- m a t i o n of c o m p e n s a t i n g co l l a t e ra l chan- nels.
A s t rong rise in f r equency and a spon- t a n e o u s d r o p in a r t e r i a l p ressu re m a y lead to a c r i t i ca l insuff ic iency of flow in t he s y s t e m i c - t o - c o r o n a r y a r t e r y a n a s t o m o s e s of smal l ca l iber .
R E F E R E N C E S
1. Murray, G., Hilario, J., Porcheron, R., and Roschlau, W.: Surgery of coronary disease, Angiology 4:526, 1953.
2. Murray, G., Porcheron, R., Hilario, J., and Roschlau, W. : Anastomosis of a systemic artery to the coronary, Canad. M.A.J. 71:594, 1954.
3. Absolon, K. B., Aust, J. B., Varco, R. L., and Lillehei, C. W.: Surgical treatment of occlusive
coronary artery disease by endarterectomy or anastomotic replacement, Stlrg. Gynec. & Obst. 103:180, 1956.
4. Thal, A., Perry, J. F., Miller, F. A., and Wangensteen, O. H.: Direct suture anastomosis of the corollary arteries in the dog, Snrgery 40:1023, 1956.
5. Miller, E. W., Hughes, C. R., and Kolff, W. F.: Angiography of the coronary arteries in the live dog, Cleveland Clin. Quart. 24:41, 1957.
6. Julian, O. C., Lopez-Belio, M., Moorehead, D., and l.ima, A.: Direct surgical procedures on the coronary arteries: Experimental studies, J. Thoracic Surg. 34:654, 1957.
7. Carter, E. L., and Roth, E. J.: Direct uonsuture coronary artery anastomosis in the dog, Ann. Surg. 148:212, 1958.
8. Moore, T. C., and Riberi, A.: Maintenance of coronary circulation during systemic-to- coronary artery anastomosis, Surgery 43:245, 1958.
9. Baker, N. H., and Grindlay, J. H.:Technic of experimental systemic-to-coronary artery anas- tomosis, Proc. Staff Meet. Mayo Clin. 34:497, 1959.
10. Botham, R. J., and Young, W. P.: An experi- mental study of systemic-coronary anastomosis, Surg. Gynec. & Obst. 108:361, 1959.
11. Hall, R. J., Khouri, E. M., and Gregg, D. E.: Nonsuture internal mammary-coronary artery anastomosis, Circulation 20:791, 1959.
12. Miller, E. W., Kolff, W. F., and Groves, L. K.: Experimental coronary artery surgery in dogs employing a pump-oxygenator, Surgery 35:1005, 1959.
13. Rohman, M., Goetz, R. H., and Dee, R.: I)ouble coronary artery-internal mammary artery anastomoses, tautalum ring technique, Surg. Forum 11:236, 1960.
14. Ratan, R. S., Leon, M., Lovette, J. B., Levo- witz, B. S., Magovern, G. J., and Kent, E. M.: Modified nonsuture anastomosis of coronary artery and internal lnamlnary artery in dogs, Surg. Forum 11:238, 1960.
15. Magovern, G. J., Kent, E. M., loevowitz, B.S., Ratan, P,. S., Lovette, J. B., Burman, S. O., and Orwig, V.: A nonsuture method of anastomosis of the left internal mammary artery to the coro- nary artery, J. Thoracic & Cardiovas. Surg. 42:642, 1961.
16. Goetz, R. H., Rohman, M., Hailer, J. D., Dee, R., and Rosenak, St. S.: Internal mammary- coronary artery anastomosis, .l. Thoracic Surg. 41:378, 1961.
17. Burman, S. O., and Orwig, V.: A nonsuture method of anastomosis of the left internal mam- mary artery to the coronary artery, J. Thoracic & Cardiovas. Surg. 42:642, 1961.
18. Ursehel, I-t. C., and Roth, E. J.: Small arterial anastomoses, Am1. Surg. 153:599, 1961.
19. Demichow, W. P.: Die experimentelle Trans- plantation lebenswichtiger Organe, Berlin, 1963, Vertag Volk und Gesundheit, p. 182.
20. Schiller, U.: The problem of vascular anasto- mosis with small-caliber vessels, as demon- strated by experimental studies on the mam- mary-coronary arterial anastomosis, IVth Euro-
368 S c h M d l a n d K r a m ~ c .~,,,. H,.~,,, .: 5,,t,t~.j~!~,r, ] otto
pean Congress on Cardioh,g>, Prague, 1964 (Abstracts).
21. Schamaun, M.: Internal mammar3 alld coro- nary artery stlttlre-anastomosis with use of patch grafting, Angiology 15:.322, 1964.
22. Carrol, S. E.: Experimental anastomosis of the left internal mammary artery to the circumflex coronary artery, using the NRC-Vogelfanger stapling device, Canad J. Surg. 7:463, 1964.
23. Daicoff, G. R., Lancaster, J. R., Stewart, P. B., Siderius, N. J., and Moulder, P. V.: Coronary artery surgery in dogs with veno-veuous coo[- ing and acetylcho/ine arrest, Surg. Forum 11:246, 1960.
24. De Bakey, M. E., and Henly, W. S.: Surgical treatment of angina pectoris, Circulation 23:111, 1961.
25. Frank, O.: Der Ablatff der StrOmungsge-
schwmdigkeit in dell GefSssen, Ztschr. I~;ioL 88:249, 1920.
26. Bretschneider, H. J.: Pharmakotherapie coro- narer l)urchbhmmgsstiirungen mit kreislauf- wirksamen Substanzen, Verhandl. deutsch Gesellsch. inn. Med. 69:583, 1963.
27. Gregg, 1-). E., Khouri, E. M., and Rayford, C. R.: Systemic and coronary energetics in the restillg unanesthetized dog, Circulati(m Res. 16:102, 1965.
28 Olssoa, R. A., and Gregg, 1). E.: M)ocard/al reactive hyperemi;t in the uuane.>thetized dog, Am. J. Physiol. 208:224, 1965.
29. Lord, J. '~\7., Coryllos, g., I.oweulels, A., Dysart, R., Netlnlann, Ch. G., and Hinton, J. w : Evaluation of operations for revasculari- zation of the m3 (x'ardium b3 the use of coronary blood tlow, using extracorporeal circulation, Surgery 43:202, 1958.