Embed Size (px)
DESCRIPTION
Coronary Heart July / August 2009
Citation preview

Treating our Furry Friends in Human Cardiac Cath Labs
coronaryheart.com
July / August 200�Issue 1� July / August 200�Issue 1�
Hot TopicComplex strategies for treating bifurcation stenoses
InterviewDr Charles Knight on how Cardiac CT can improve your practice
Cardiac CTThe BMI London Independent’s new 128-slice CT
Site VisitChristchurch Hospital, New Zealand
PharmaBivalirudin
Echo Case StudyCaseous Mitral Annular Calcifi cation
New TechnologyAccumetrics’ Platelet assessment available in UK EM
PLOYMENT
SubscribeFree
Online
coronaryheart.com

Web based application:High user compliance: Documented results:
Scan Modul System is the world’s leading full-service provider in healthcare logistics.
We cover all your needs from consulting services, cabinets and modules, to software installation and implementation.
Call to set up a LIVE presentation today & learn more about our
introductory offer

ContentsCONTENTS
Disclaimer:Coronary Heart should never be regarded as an authoritati ve peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing arti cles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Therefore it is the reader’s responsibility that any advice provided in this publicati on should be carefully checked themselves, by either contacti ng the companies involved or speaking to those with skills in the specifi c area. Readers should always re check claims made in this publicati on before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their insti tuti on, Coronary Heart Publishing Ltd or the editorial staff .
14 VIP in the Cath Lab- Dogs in human cath labs
Coronary Heart Publishing Ltd145 - 157 St John Street
London, EC1V 4PYUnited Kingdom
Email: [email protected]: +44 (0) 207 788 7967
Web: www.coronaryheart.com
CIRCULATION3800 Cardiac Professionals(Readership of over 12,500 in UK, & downloaded in 122 countries)
Copyright © 2006 -2009 by Coronary Heart Publishing Ltd.
All rights reserved. Material may only be reproduced by prior arrangement and with due acknowledgment of Coronary Heart Publishing. The publication of an
advertisement or product review does not imply that a product is recommended by Coronary
Heart Publishing Ltd.
Low Advertising Budget?
Coronary Heart is widely regarded as the favourite dedicated UK cardiology publicati on for the enti re cardiac department. Each editi on is developed with the reader in mind with interesti ng arti cles and innovati ve designs.
We have a variety of adverti sing opti ons to match your budget, including sponsorships and content matching placements. Our team fi rmly believe in building strong relati onships with all adverti sers which is why our director Tim Larner will personally meet with you to answer any questi ons you have and assist you in achieving your marketi ng goals. The coff ee’s on us!!
See our current adverti sers on page 25.
ADVERTISINGWendy Rose
Rose Media LtdEmail: [email protected]
04 Latest News
05 Hot Topic
06 Journal Trawl
07 New Technology
08 Interview
09 ECG Challenge
10 Cardiac CT
16 Echo Features
20 Pharma
21 Site Visit
25 ECG Challenge Answer
26 Recruitment, Events, & Next Issue
Christchurch Hospital, New Zealand
FEATURES:
COVER STORY:
Page 21
CORONARY HEART ™ 3

LATEST NEWS
- The Team -Mr Tim LarnerDirector/Chief EditorCentral Manchester University Hospitals NHS Foundation Trust
Dr Simon RedwoodChief Clinical EditorGuy’s & St Thomas’ NHS Foundation Trust
Dr Rodney FoaleSenior Clinical EditorImperial College Healthcare NHS Trust
Dr Richard EdwardsConsulting EditorNewcastle upon Tyne Hospitals NHS Trust
Dr Divaka PereraConsulting EditorGuy’s & St Thomas’ NHS Foundation Trust
Dr John PaiseyJournal EditorRoyal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Mr Ian WrightChief EP Consulting EditorImperial College Healthcare NHS Trust
Mr Adam LunghiEcho EditorCVS - CardioVascular Services, Australia
Mr Stuart AllenCRM EditorMonash Medical Centre, Australia
Ms Mojgan SaniPharmaceutical EditorRoyal Berkshire NHS Foundation Trust
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
4 CORONARY HEART ™
hTrak Arrives in UK after Phenomenal Success in Australian Cath LabsFollowing on from its great success in Cath labs in Australia, the hTrak soluti on is now available in the United Kingdom. hTrak is a mobile point of use data capture applicati on specifi cally designed for use in busy high cost procedure areas. Running on the very latest mobile barcode scanning devices, hTrak adds speed & accuracy to the collecti on of criti cal data at the point of use. By eliminati ng the manual, paper based collecti on of informati on, hTrak is able to dramati cally streamline these laborious processes freeing up key staff to concentrate on their clinical roles. hTrak is routi nely used to track prostheses to a pati ent, automate replenishment, cost procedures to a pati ent, manage recalls, manage consignment stock, protect pati ents and provide authorised staff with access to a secure, comprehensive web based reporti ng environment.
For more informati on call 01494 695 630, email: [email protected],or visit the website: www.htrak.com

HOT TOPIC
“With the recent presentation of the BBC-ONE and NORDIC trials, is there ever a role to intentionally use a complex
strategy for treating bifurcations, and if so which
would you choose?”
Cardiologist Hot Topic
Professor Adam TimmisConsultant Interventional Cardiologist, The London Independent Hospital, London
My strategy for bifurcati ons is to stent the main vessel and then do
whatever is necessary to, if anything is necessary to open up the side vessel, usually just with a balloon and a wire, rather than doing any additi onal stenti ng. In the past I have used Crush technique but the long term results have not been good. And if having planned a conservati ve strategy I fi nd I cannot maintain the patency of the side branch I would then be forced into the complex strategy, in eff ect. If I considered the branch to be important in that situati on I would use a culott e technique, by preference. But as I say it is really not oft en necessary to do that and I fi nd that just a conservati ve approach to the side branch is usually all that’s needed.
Dr Rod StablesConsultant Interventional CardiologistLiverpool Heart and Chest Hospital NHS Trust, Liverpool, UK
I might sti ll use complex stent techniques in proximal bifurcati ons, subtending very large branches with substanti al myocardial
distributi on. Left main stem would be a key example. In this setti ng I prefer culott e but also, if the anatomy is favourable (mainly bi-osti al disease), have some experience with simultaneous kissing stents (V-stenti ng)
Trials Explained:
BBC-ONE:
The Briti sh Bifurcati on Coronary Study: Old, New, and Evolving Strategies study showed provisional T-stenti ng using the Taxus stent (compared with crush or culott e) resulted in a lower rate of death, MI, and target-vessel failure at one year. ¹
NORDIC:
Presented fi rst in 2006, this trial suggested that a single-stent approach was bett er than a two-stent approach (including T-stenti ng, crush, or culott e techniques).
Glossary:
Crush Technique:
A small porti on of the side-branch stent extends into the main artery but is crushed against the wall of the main artery when the main-artery stent is expanded.²
Culott e Technique:
Two stents are placed into the diseased vessel, with one positi oned in the main artery and the other in the side branch so that the two stents overlap in the main artery before the branch point. ²
Provisional T-Stenti ng:
Stent placement in the main branch followed by kissing-balloon angioplasty and provisional stent placement in the side branch. ³
htt p://www.theheart.org/arti cle/912611.dohtt p://www.medscape.com/viewarti cle/572220htt p://www.cvspectrum.org/cms/templates/arti cle.aspx?arti cleid=12292&zoneid=48
1.2.3.
Stent image courtesy Boston Scientific Corporation
CORONARY HEART ™ 5

JOURNALS
� CORONARY HEART ™
Cardiac rehabilitation programmes are as varied in their content as they are numerous. Should they
contain a vigorous exercise component? Yes, according to a study of 74 post MI patients randomised to the usual advice with or without an exercise program involving 3000 to 3500 kcal/wk. The higher energy expenditure group lost more weight and had better metabolic profiles, the benefits maintained for at least a year.
Philip Ades and others Circulation. 2009;119:2671-2678
Outcome data is difficult to obtain in cardiopulmonary resuscitation so the changes made to protocols emphasising chest compressions with defibrillation and airway support taking second place were developed from non clinical studies and surrogate endpoints. It is therefore reassuring to see that a comparison of outcomes pre- and post- change in protocol demonstrated a clear improvement in outcomes with survival to hospital discharge rising from 22 to 44%.
Alex Garza and others Circulation. 2009;119:2597-2605
It is always difficult to know what the frequency of events is in the rarer arrhythmogenic syndromes. A useful observational study of 100 patients with catecholamine dependant ventricular tachycardia has shown an event rate of 32% overall (58% without beta blockers; 27% with beta blockers). Fatal or near fatal events occurred in 13% over 8 years.
Meiso Hayashi and others Circulation. 2009;119:2426-2434
Two studies recently published have examined the value of bone marrow derived stem cells in coronary disease. In a proof -of- concept study a statistically significant though small reduction in ischaemic burden was seen after intramyocardial injection of stem cells.In a separate study of acute infarcts,
intracoronary injection of stem cells resulted in an improvement of local myocardial function and quality of life measures.
Jan van Ramshorst and others JAMA. 2009;301(19):1997-2004Muhammad Yousef and others J Am Coll Cardiol, 2009; 53:2262-2269
Ischaemic mitral regurgitation is associated with poor outcomes if treated conservatively whilst surgery is challenging and high risk. A series of 44 patients with severe MR and haemodynamic compromise undergoing annuloplasty and Bovine patch posterior leaflet extension did well with 90% of survivors free from significant MR and symptomatic heart failure. The operative/early mortality was 11%.
Benoit de Varennes and Circulation. 2009;119:2837-2843
Ventricular reconstruction surgery has been touted for a while. A randomised study of 1000 patients with EF <35% undergoing CABG found no endpoint difference between those randomised to ventricular reconstruction and those randomised to CABGs only, despite a reduction in ventricular volume in the intervention group.
Robert Jones and others N Engl J Med. 2009 Apr 23;360(17):1705-17
In low flow aortic stenosis some have advocated contractile reserve on dobutamine stress echo as a selector for suitable surgical candidates. A study of 81 patients without contractile reserve undergoing AVR was compared to medically managed propensity matched controls. Although operative mortality was high at 22%; 5 year survival was significantly better in the operated group (54 vs. 13%). Conclusion-AVR should not be withheld on the grounds of lack of contractile reserve.
Christophe Tribouilloy and others J Am Coll Cardiol, 2009; 53:1865-1873
A registry of 291 patients undergoing drug eluting stent placement for left main stem disease has demonstrated good outcomes at two years. A wide range of haemodynamically stable patients were included with a provisional T stent approach to distal bifurcation lesions. Angiographic success was achieved in >99% with 95% 5 year survival and target lesion revascularisation of 8.7%
Beatriz Vaquerizoand others Circulation. 2009;119:2349-2356
What to do with in stent restenosis? Until recently the answer would have been deployment of a drug eluting stent but it may be preferable to dilate the lesion with a Paclitaxel coated balloon. In a randomised comparison of 131 patients those treated by coated balloon did at least as well as those treated by stenting with a trend toward lower recurrent events in the balloon group.
Bruno Scheller and others Circulation. 2009;119:2986-2994
Lead extraction is an agricultural process at the best of times. It is therefore not surprising that the tricuspid valve may be damaged during the process. In a series of over 200 extractions tricuspid regurgitation was seen in 9% with a high incidence of significant right sided heart failure symptoms amongst these. Use of the laser sheath and female gender were associated with a higher incidence of TR.
Frédéric Franceschi and others J Am Coll Cardiol, 2009; 53:2168-2174
It has been established that aspirin and clopidogrel in combination is an inferior treatment to warfarin where stroke prevention in atrial fibrillation is concerned. Is there though a logic to adding clopidogrel to aspirin in patients who cannot take warfarin? In the ACTIVE study stroke was cut from 3.3 to 2.4% whilst major bleeding was increased from 1.3 to 2%.
The ACTIVE Investigators N Engl J Med. 2009; 360:2066-2078
Dr John PaiseyConsultant Cardiologist and
ElectrophysiologistRoyal Bournemouth Hospital
- Scanning the world’s cardiology journals
Journal Trawl

NEW TECHNOLOGY
CORONARY HEART ™ 7
It is considered well known that the use of Clopidogrel in conjuncti on with Aspirin lowers the rate of thromboti c
events in pati ents undergoing percuta-neous coronary interventi on (PCI) with coronary stenti ng. However, a number of clinical studies in which platelet response is measured have demonstrated that the pati ent response to Aspirin and Clopidog-rel is not uniform, and “poor response” has been associated with an increased risk for cardiovascular events.
Light Transmitt ance aggregometry (LTA) is considered by most to be the gold standard for determining the eff ects of anti platelet therapy on platelet functi on, but the logisti cal demands make it almost impossible to use in daily practi ce. Now, the “Verifynow” platelet functi on ana-lyser from Accumetrics Inc gives clinicians a true point of care (POC) opportunity to monitor their pati ents on anti platelet therapy.
Marketed in the UK by Elitech UK Ltd, spe-cialists in POC haemostasis monitoring, “Verifynow” is able to accurately monitor pati ent’s individual response to every cur-rent major anti platelet medicati on includ-ing the recently released competi tor to Clopidogrel, “Efi ent” marketed by Eli Lily and Daiichi-Sankyo.
“The Verifynow system is extremely ac-curate, has excellent correlati on and is very simple to use” states Tim Watson, Managing Director of Elitech UK. “And it fi ts perfectly into our current portf olio of specialist Cath Lab products which include the Hemochron range of anti coagulati on analysers for ACT results, the IRMA True-Point Blood Gas analyser and fi nally the Avox 1000E Oximetry analyser used pri-marily by cardiologists performing Right Heart procedures”.
There are now a total of 3 diff erent Veri-fynow assays – Aspirin, P2Y12 (Clopidog-rel and Efi ent) and IIb/IIIa (ReoPro® and
Integrilin®) so all of the current major an-ti platelet medicati ons are covered.
Samples to be tested can be whole blood collected from an indwelling catheter or by using direct venipuncture and col-lected in a Greiner tube containing either 3.2% Sodium Citrate (Aspirin or P2Y12) or Lithium Heparin (IIb/IIIa). Following a short incubati on period (30 mins – Aspi-rin, 10 mins - P2Y12) the sample is good to go and is introduced to the analyser. The analyser draws the sample into the previ-ously placed assay cartridge and your re-sult appears 3-5 minute later. It really is that simple!
Tim Watson goes on to say “There is now a considerable amount of published evi-dence for improved outcomes and ongo-ing pati ent management if the pati ent has been monitored by the Verifynow system. I personally believe that the ti me is now right for the introducti on of routi ne moni-toring of pati ents on anti platelet medica-ti on especially when considering the use of Efi ent as a possible replacement for Clopidogrel in poor responders. However, the benefi t of possible increased pati ent response has to be balanced with the possible increased risk of bleeding when considering changing between the two medicati ons.” ¹
For Further Informati on on the Verifynow system please contact:
Elitech UK Ltd, Unit 6, River Park Industrial Estate, Billet Lane, Berkhamsted HP4 1HLTel: 01442 86 93 20 [email protected]
References:Acute coronary syndrome - prasugrel: appraisal consultati on document. www.nice.org.uk
1.
Advertorial for Elitech UK Ltd
- Breakthrough technology making platelet assessment easy for patients receiving antiplatelet therapy.
Accumetrics VerifyNow

INTERVIEW
� CORONARY HEART ™
How has the use of cardiac CT improved your cardiac practice in regards to throughput and patient care?
I think there are two groups of patients really where it is useful. Firstly are those who are at high risk of multiple cardiac risk factors, particularly younger people who maybe have a very bad family history, with a whole load of family members having heart attacks in their forties and fifties. It is a very good technique to be able to give them a non-invasive coronary angiogram and to calcium score, to be able to either reassure them or to really maximise their secondary prevention. So I think it is that group who come and see you where their father has had a heart attack at 45. Previously we didn’t really know what test to do, because you didn’t want to have to do a full blown angiogram, and
an exercise test wasn’t really going to be that helpful. Now we can do this and if it shows minimal atheroma they can be highly reassured.
I guess the other group of patients are the patients who have had bypass surgery. It is a very good way of looking at graft patency, non-invasively. So if they come back with funny symptoms after a bypass we can quite easy take a look and see which grafts are patent and which aren’t.
Is the extra radiation dosage from cardiac CT a cause for concern?
Any radiation bothers you, but I think you have to balance the risk and benefit as with any test. I think the radiation is the main problem with the technique and does limit it. You would prefer a technique that you could follow-up patients year on year on year to keep an eye on things, but I am not sure we can quite do that because of the accumulative radiation dose being pretty huge. So that is a problem if you are looking at a longitudinal follow-up. But for a one-off investigation to say to somebody “you are alright” or “you are not alright” it is a good test.
Do you think in the future cardiac CT will become the first test for patients whom present with chest pain rather than performing a coronary angiogram?
At Bart’s and The London we are
certainly working on incorporating a similar machine into a low risk chest pain pathway. So in other words when patients go into casualty, and present with high risk features – elevated troponin, ECG changes, they will obviously need conventional angiography. If they don’t, a lot of those patients languish in hospital for days waiting for an exercise test or waiting for something to emerge. What we are hoping to do is to be able to discharge those patients straight home with an outpatient appointment the next day where they can have a CT and see a cardiologist. And that way hopefully we can reassure 95%, but catch the 5% that actually have a problem. So I think it is really the low risk groups presenting with chest pain to A&E that these will become very useful machines.
How have you found the accuracy compared with diagnostic angiograms?
So far pretty good. If it says there is a problem it is always there. If it says there is a 50% stenosis, it might, and it is difficult to know who is right. But the angiogram might show something a bit less. That may well be because this is showing plaque in the outside of the artery, and the lumen actually isn’t that bad. So it might overestimate things a tiny bit. Once or twice it might underestimate, but it tells you that you need to do a proper angiogram, so is very reliable. If a stenosis is seen as 40% or 60% there maybe a little variation, but overall the accuracy is very good.
Cardiac CT in Clinical Practice
Dr Charles Knight Lead Consultant CardiologistBarts and The London NHS Trust London United Kingdom
- Coronary Heart Director, Tim Larner interviews Dr Charles Knight at the BMI London Independent Hospital
INTERVIEW
CORONARY HEART ™ �
In the USA the cardiologists do the reporting for the CT’s compared to just the radiologists here in the UK. Do you think that will change with cardiologist involved with the reporting?
I think they have to be. The BCIS group I think is working on a position paper, and without wanting to say what they are going to say, it is almost certain they are going to say it needs to be joint reported. So you will have a cardiologist and a radiologist reporting the images.
The radiologist is vital, because if you do a CT of the chest, there is all sorts of non-cardiac things, incidental lung cancers etc you might miss. This is different from cardiac MR, where I think that cardiologists just can report them as long as they are specialist enough, but with a CT of the chest and heart you do need both and I am sure that is the way forward.
History: 12 lead ECG of patient with previous multiple AF ablations
Question: What is the rhythm?
Answer: See page: 25
Ian Wright’s ECG Challenge
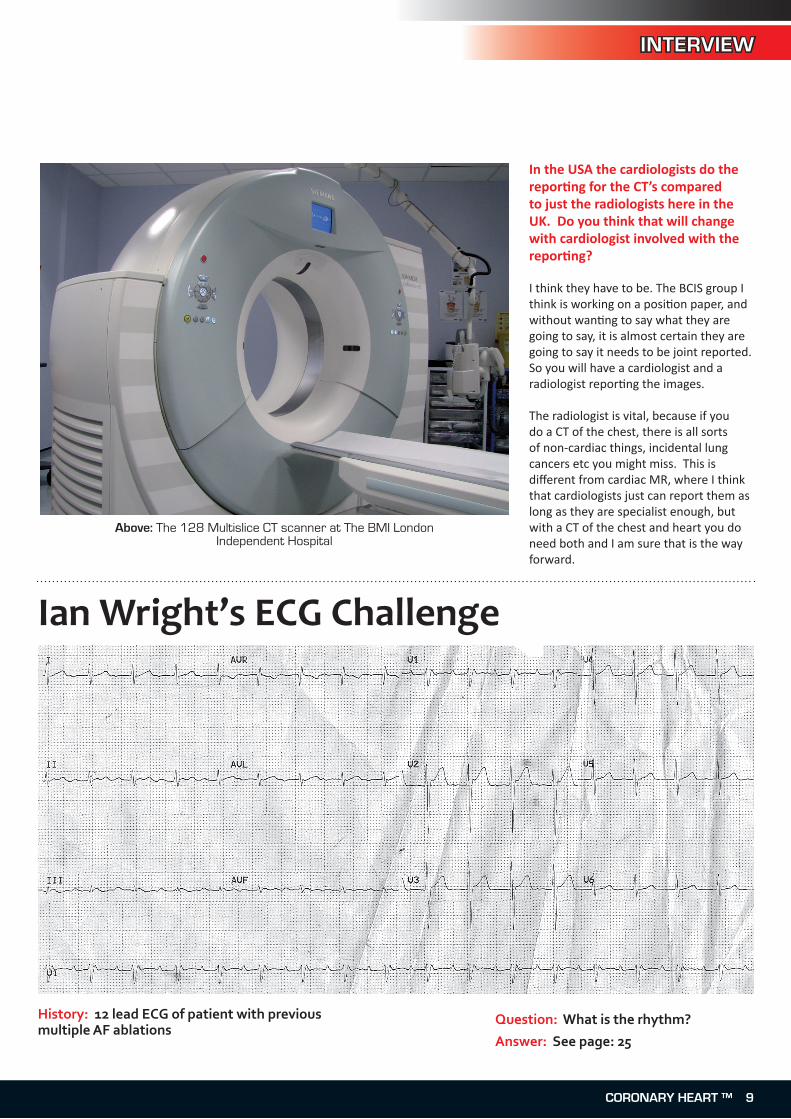
Above: The 128 Multislice CT scanner at The BMI London Independent Hospital

CARDIAC CT
10 CORONARY HEART ™
The 128 Multislice CT Scanner At London Independent HospitalDr Carl Shakespeare MD FRCP FACC [email protected] Cardiologist, South London Hospitals Trust, WoolwichClinical Director, SE London Cardiac Network
There is an increased array of diagnostic tools used in the diagnosis and evaluation of
prognosis of coronary artery disease. They can be divided into functional assessments: including exercise testing, nuclear perfusion imaging, stress echocardiography, and more recently cardiac MRI perfusion imaging; and anatomical assessment: coronary angiography and cardiac CT angiography (CTA).
Up to now, coronary angiography (CA) has been the gold standard in the diagnosis of coronary disease. Anatomical confirmation is increasingly sought for both symptomatically limiting and non-limiting angina. However, despite numerous NHS initiatives, access to CA is suboptimal and there remains a small but finite morbidity (0.1%) and mortality (0.2%) risk. There has also been a paradigm shift in recent times away from a purely anatomical diagnosis of coronary disease; to a prognostic approach focused on patients subsequent cardiac risk and management (1). This is increasingly relevant as at best, only 50% of diagnostic procedures proceed to intervention. As the degree of angiographic coronary narrowing has not been shown to correlate with future cardiac events, more relevant investigations offering prognostic information could include stress echocardiography or nuclear myocardial perfusion imaging (2).
The Evolution of Cardiac Computed Tomography:
Computed tomography (CT) scanning provides a non-invasive technique of imaging cardiac structures. In the process, an X-ray beam is attenuated while passing through the tissues of the heart, and this is measured by detectors and translated into images. Numerous technical advances have resulted in freezing cardiac motion (temporal resolution) to obtain excellent image quality and minimizing artefacts. Certainly fast rotation times (up to 0.3 seconds) of the X-ray source around the gantry have significantly improved temporal resolution. Spatial resolution
(the degree of blurring and the ability to discriminate small objects) has been optimized by having small multiple detectors (0.6 mm width), thin slice thicknesses and small X-ray focal spots.
Multi slice spiral CT scanning involves a rotating X-ray tube with a simultaneously moving table (hence spiral imaging) and multiple rows of detectors (16, 32, 64, 128, 256…). With this combination of a greater number of detector rows, simultaneous acquisition of a greater number of axial slices can be made per rotation. Thus a greater coverage of the heart can be made per rotation, resulting in a short breath hold. With the Siemens Somatom 128 multislice CT
- Enhancing patient treatment with the latest technology
Above: Ms Sa Memon, Deputy Imaging Manager at The London Independent Hospital
CARDIAC CT
CORONARY HEART ™ 11
scanner recently installed at the London Independent Hospital (LIH), the whole heart can be scanned in 7-10 seconds.
The Siemens Somatom 128 multislice CT scanner at LIH:
This was installed exactly one year ago and involves both cardiac and non-cardiac applications. The technology has lived up to its promise of being “adaptive” to a variety of scenarios that challenge this type of imaging. Most importantly, obesity is a major challenge
for CT imaging and the scanner benefits from a weight limit of up to 300kg, with a large gantry width of 78 cm and most importantly a powerful generator of 100kW.
This scanner with its arrangement of alternating focal spots where the X-ray beams overlap results in a resolution of 0.24mm. The 128 rows of detectors provide excellent volume coverage. A major concern for CT imaging is radiation dose that patients are exposed to. This
Siemens scanner is equipped with several features designed to reduce the radiation to about 4.9mSv (3). This includes: adaptive Dose Shield that removes unnecessary exposure at the beginning and end of acquisition, Dose adaption to the patient, ECG pulsing, dose modulation (that lowers the dose during non-acquisition periods), and adaptive features to arrhythmia.
Cardiac Applications of Cardiac CT:
The major applications of cardiac CT include: calcium scoring, coronary angiography, and visualization of other cardiac structures. Additionally with the large volume of data, left ventricular function can be assessed by as a moving image from reconstructions throughout the cardiac cycle.
Calcium Scoring:
In asymptomatic patients the American Heart Association suggests a role for calcium scoring in patients with intermediate risk for coronary disease (5). Electron Beam CT (EBCT) and more recently Coronary Calcium Scoring (CCS) using the Multi-Slice CT scanner have demonstrated the association of coronary calcification and subsequent cardiovascular risk. The absence of coronary calcium is associated with normal coronary arteries. CT coronary calcification does provide the most accurate method currently available for the early detection of coronary artery disease. The presence of a score > 100 (Agatston Score) is associated with a 10x risk of future cardiovascular events. It provides independent and incremental information over risk factors for predicting extent of angiographic CAD. It is perhaps logical with increasing attention to coronary risk, early detection of atherosclerosis may help select patients for earlier and more aggressive treatment.
Coronary calcification is usually present in all angiographically significant coronary disease (>50% diameter stenosis). Thus it can be applied to evaluate the long term risk of atherosclerosis in
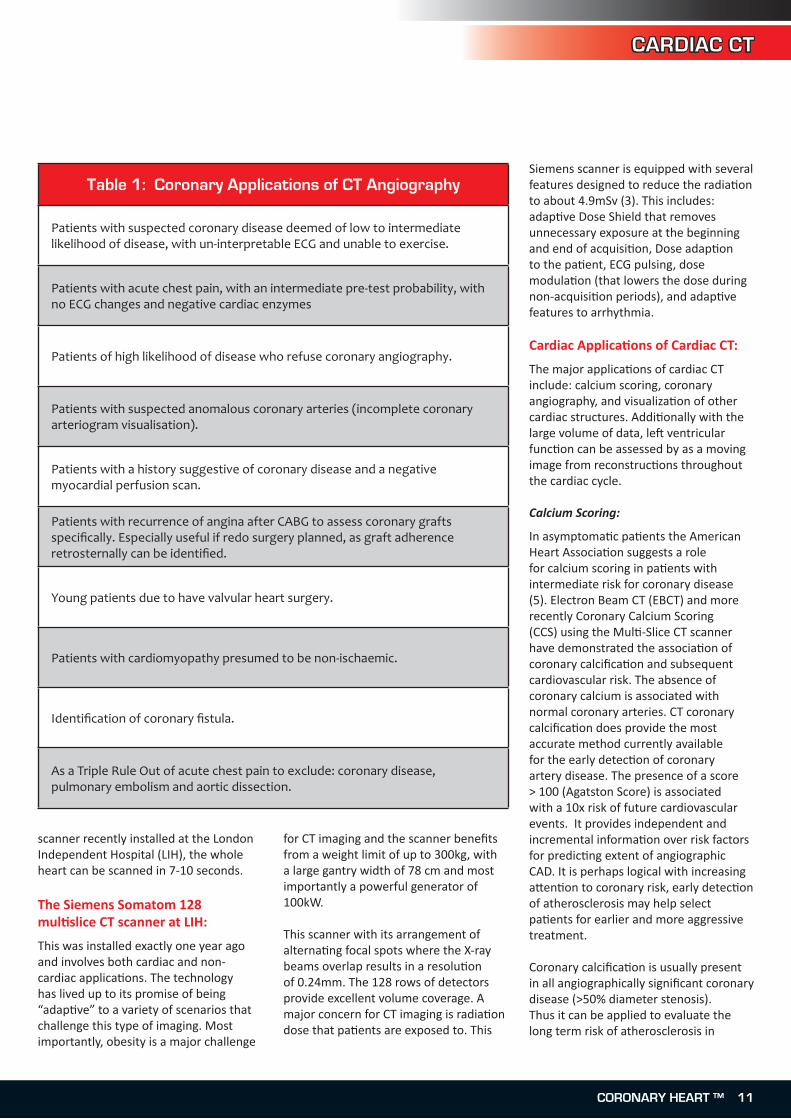
Table 1: Coronary Applications of CT Angiography
Patients with suspected coronary disease deemed of low to intermediate likelihood of disease, with un-interpretable ECG and unable to exercise.
Patients with acute chest pain, with an intermediate pre-test probability, with no ECG changes and negative cardiac enzymes
Patients of high likelihood of disease who refuse coronary angiography.
Patients with suspected anomalous coronary arteries (incomplete coronary arteriogram visualisation).
Patients with a history suggestive of coronary disease and a negative myocardial perfusion scan.
Patients with recurrence of angina after CABG to assess coronary grafts specifically. Especially useful if redo surgery planned, as graft adherence retrosternally can be identified.
Young patients due to have valvular heart surgery.
Patients with cardiomyopathy presumed to be non-ischaemic.
Identification of coronary fistula.
As a Triple Rule Out of acute chest pain to exclude: coronary disease, pulmonary embolism and aortic dissection.

CARDIAC CT
12 CORONARY HEART ™
asymptomatic patients or those with suspected coronary disease who are deemed to have low or intermediate likelihood of disease. In asymptomatic patients with an Agatston score > 400; would indicate the need for further functional assessment for ischaemia. Specifically in the asymptomatic diabetic population, the fact that a 20% incidence of myocardial infarction occurs within 7 years has led the American Diabetic Association to recommend early screening. Radiation dose is very low at 1 mSv.
Coronary Angiography:
The main coronary angiographic applications are seen in Table 1 (adapted from the AHA/ACC guidelines of 2006 (4)). The main coronary application is in symptomatic patients who have low to intermediate probability of disease (5). Ideally patients should be in sinus rhythm with stable heart rates. More recent software (applicable in our Siemens scanner) can obviate the rhythm problems. With the exception of Dual Source CT angiography, most coronary imaging requires optimizing heart rate to 60 beats per minute or less (see later). Compared to cardiac catheterization which only identifies the coronary lumen, CT angiography looks at the entire vessel. In early stages of coronary
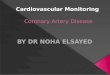
disease, the lumen is normal in diameter, as the active pathological process involves thickening of the wall. As seen in Figure in 1 where coronary stents are in place, the extent of disease extends beyond the stent insertion. Increasing attention is being paid to the consistency of the plaque that might yield prognostic value. Certainly, CT angiographic estimation of the volume bulk of coronary lesions does offer prognostic value over angiography.
Cardiac Structures:
In addition to the coronary anatomy, numerous other cardiac structures are well visualized, and described in Table 2.
Practical Issues:
The main practical issue in performing CT angiography is maintaining the heart rate at about 60 beats per minute. This can be achieved by pre-medicating the patient in outpatients with oral beta blockers. At the London Independent Hospital, we do not pre-medicate the patient, but assess the need for rate reduction just prior to the procedure. We use iv metoprolol in in 5mg aliquots (half life 5-7 minutes), and when optimal heart rate is achieved, the patient is scanned. In patients undergoing calcium scoring alone, neither beta blockade nor contrast media is required. From a reporting perspective, we follow the wide held view that dual
The 128 Multislice CT Scanner at The London Independent Hospital (cont...)
Table 2: Non-Coronary Cardiac CT applications
To evaluate left ventricular hypertrophy, or abnormal myocardial thinning
To demonstrate atrial and ventricular septal defects and patent foramen ovale.
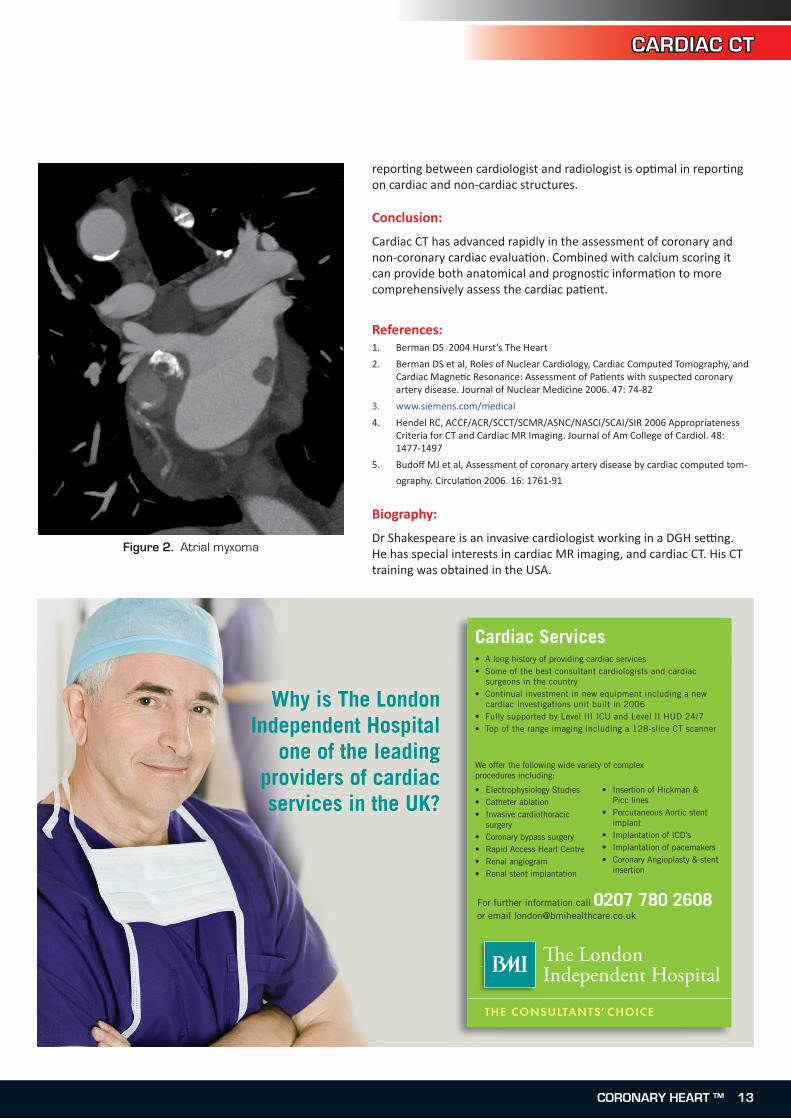
Demonstrate ventricular clot. Atrial clot (especially in the left atrial appendage and other atrial masses can be identified. (see Figure 2)
Visualisation of the pulmonary vein insertion to exclude anomalous pulmonary drainage, and other abnormal communication (e.g. SVC to pulmonary veins)
Assessment of aortic regurgitation by plenimetry
Assessment of pericardial disease. In this way, effusions and more importantly pericardial thickening can be visualized
Evidence of gastric reflux can be shown in the evaluation of atypical chest pain.
Figure 1. Mixed plaque between two stents
CARDIAC CT
CORONARY HEART ™ 13
reporting between cardiologist and radiologist is optimal in reporting on cardiac and non-cardiac structures.
Conclusion:
Cardiac CT has advanced rapidly in the assessment of coronary and non-coronary cardiac evaluation. Combined with calcium scoring it can provide both anatomical and prognostic information to more comprehensively assess the cardiac patient.
References:Berman DS 2004 Hurst’s The Heart
Berman DS et al, Roles of Nuclear Cardiology, Cardiac Computed Tomography, and Cardiac Magnetic Resonance: Assessment of Patients with suspected coronary artery disease. Journal of Nuclear Medicine 2006. 47: 74-82
www.siemens.com/medical
Hendel RC, ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 Appropriateness Criteria for CT and Cardiac MR Imaging. Journal of Am College of Cardiol. 48: 1477-1497
Budoff MJ et al, Assessment of coronary artery disease by cardiac computed tom-
ography. Circulation 2006. 16: 1761-91
Biography:
Dr Shakespeare is an invasive cardiologist working in a DGH setting. He has special interests in cardiac MR imaging, and cardiac CT. His CT training was obtained in the USA.
1.
2.
3.
4.
5.
• A long history of providing cardiac services • Some of the best consultant cardiologists and cardiac surgeons in the country• Continual investment in new equipment including a new cardiac investigations unit built in 2006• Fully supported by Level III ICU and Level II HUD 24/7• Top of the range imaging including a 128-slice CT scanner
Why is The London Independent Hospital
one of the leading providers of cardiac services in the UK?
Cardiac Services
We offer the following wide variety of complex procedures including:
• Electrophysiology Studies• Catheter ablation• Invasive cardiothoracic surgery• Coronary bypass surgery• Rapid Access Heart Centre• Renal angiogram• Renal stent implantation
• Insertion of Hickman & Picc lines • Percutaneous Aortic stent implant• Implantation of ICD’s• Implantation of pacemakers• Coronary Angioplasty & stent insertion
For further information call 0207 780 2608 or email [email protected]
Figure 2. Atrial myxoma

SPECIAL FEATURE
VIP in the Cath Lab
A Cardiac Catheterisati on suite is an environment full of expensive technology and staff ed with highly qualifi ed people. But what about the pati ents? Are they all the
same? Are gender, ethnicity or socio-economic background relevant factors which might infl uence our behaviour? Do we someti mes give VIP services to pati ents?
I have, during the course of my work, witnessed VIP treatment off ered to pati ents. The irony is that the recipients of this fi rst class service were not requesti ng such a level of att enti on. In fact, although the pati ents were by no means intellectually challenged, they could not understand what the procedure was all about. This was due simply to the fact that they all belong to the canine species.
Balloon valvuloplasty on dogs is a proper technique for relief of valvular pulmonic stenosis which is occasionally performed in “Homo Sapien” Cath Labs.
Cardiologists are, from ti me to ti me, approached by Veterinarians requesti ng access to their Cath Lab to treat dogs requiring pulmonic valvuloplasty. I had the opportunity to be involved in one of these cases. While working in general radiography I had in the past x-rayed cats and dogs (usually performed aft er-hours and with a certain level of discreti on), nevertheless a valvuloplasty under GA is not a procedure that can go unnoti ced.
Balloon valvuloplasty of pulmonic stenosis is a minimally invasive procedure associated with fewer complicati ons and a shorter recovery ti me than other surgical opti ons. This procedure oft en has an excellent outcome. The ideal result is a gradient that is to near normal pressures (<20 mmHg); this is achieved approximately 70-80% of the ti me.
Case Study
An 11 month old Kelpie (Narla) initi ally presented with two episodes of collapse while doing minimal exercise. On her fi rst visit her pressure gradient across the pulmonic valve was 100 mmHg compared to 120 mmHg 4 months later. She had been on atenolol for 3 months.
Brief Technical Descripti onNarla was anaestheti sed and placed on left lateral decubitus positi on. The initi al plan was to perform a cut down to gain access to the RJV but aft er discussion with the Interventi onal Cardiologist a percutaneous approach was selected and a 9 F introducer sheath was inserted. A Swan Ganz/balloon catheter was then introduced and haemodynamic measurements were made in the RVOT. Pull back from PA to RV to RA was performed. The next step was to use a Maxi LD
Above from left to right:Dr Richard Clugston (interventional Cardiologist) and his
daughter, Narla (patient), andDr Josephine Dandrieux (Cardiologist Veterinarian)
Above: Narla anaesthetised on the cath lab table
- Opening up Human Cath Labs to our Furry Friends
14 CORONARY HEART ™
SPECIAL FEATURE
Does you department perform interesting procedures? Send them to us at [email protected]
balloon from Cordis 18 x 40 mm to reduce the pulmonic stenosis. Repeat pull back was done followed by a second inflation with a Maxi LD 20 x 40 and a final inflation with a 22 x 40 mm Maxi LD balloon. The sheath was removed and the dog was awake without any complications.
Staff involved
1 Interventional Cardiologist3 Veterinarians (Cardiologist, Anaesthetist, Internist)1 Veterinary Nurse1 Radiographer1 Monitoring Technician
Outcome
The pressure gradient was reduced by half (from 100 mmHg to 50 mmHg) immediately following the procedure. Narla is now doing wonderfully well! Her pressure gradient is 55 mmHg.
Anecdotal
Narla is a farm dog and her male owner was not keen to spend money on expensive procedures but luckily the daughter and wife of the farmer were able to secretly save money for Narla’s treatment. All the Cath Lab staff donated their time and Cordis Australia supplied the balloons free of charge. This VIP patient will be remembered for a long time and has made me discover an interesting facet of interventional cardiology.
Authors details and location withheld upon request
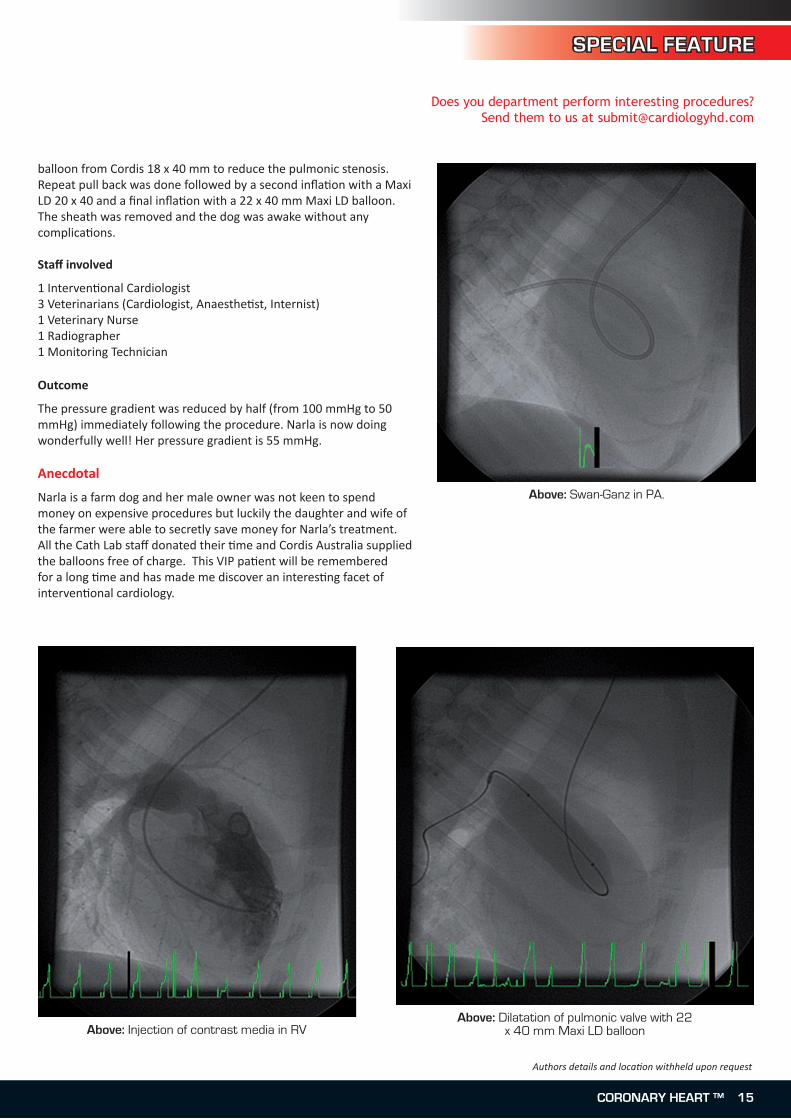
Above: Swan-Ganz in PA.
Above: Injection of contrast media in RVAbove: Dilatation of pulmonic valve with 22
x 40 mm Maxi LD balloon
CORONARY HEART ™ 15
ECHO
The NHS Institute for Innovation and Improvement recently published its ‘Focus on: Heart Failure’ document
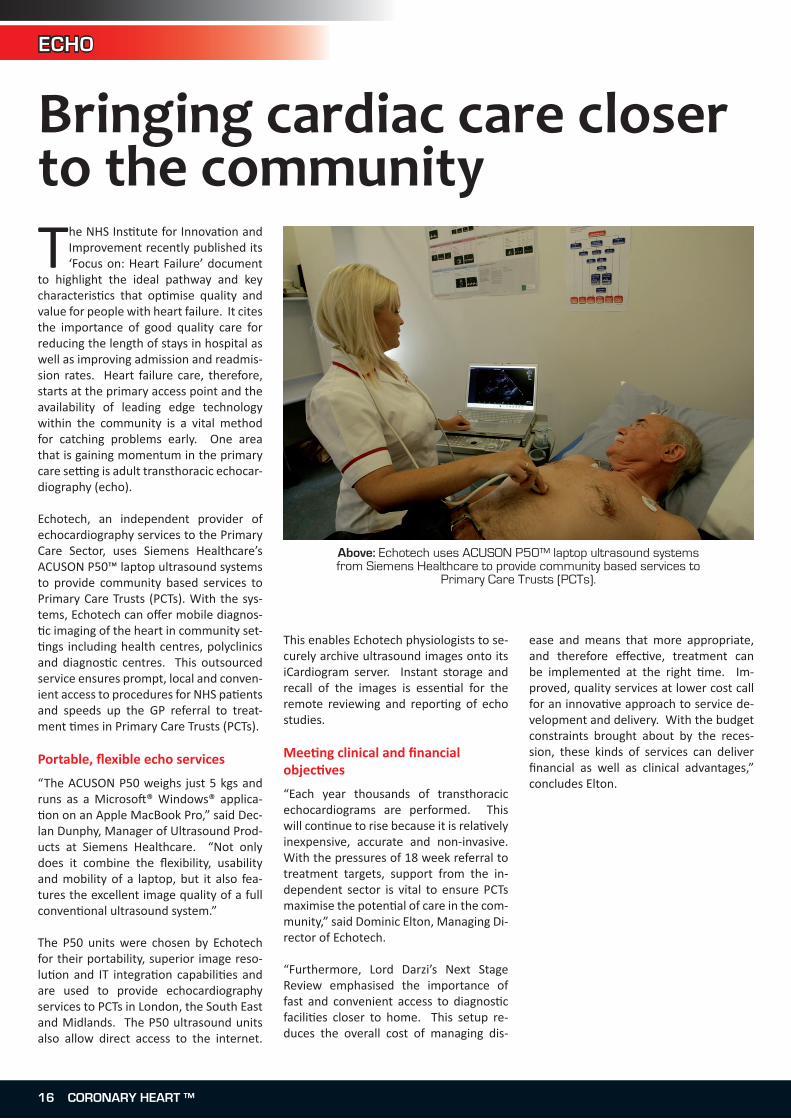
to highlight the ideal pathway and key characteristics that optimise quality and value for people with heart failure. It cites the importance of good quality care for reducing the length of stays in hospital as well as improving admission and readmis-sion rates. Heart failure care, therefore, starts at the primary access point and the availability of leading edge technology within the community is a vital method for catching problems early. One area that is gaining momentum in the primary care setting is adult transthoracic echocar-diography (echo).
Echotech, an independent provider of echocardiography services to the Primary Care Sector, uses Siemens Healthcare’s ACUSON P50™ laptop ultrasound systems to provide community based services to Primary Care Trusts (PCTs). With the sys-tems, Echotech can offer mobile diagnos-tic imaging of the heart in community set-tings including health centres, polyclinics and diagnostic centres. This outsourced service ensures prompt, local and conven-ient access to procedures for NHS patients and speeds up the GP referral to treat-ment times in Primary Care Trusts (PCTs).
Portable, flexible echo services
“The ACUSON P50 weighs just 5 kgs and runs as a Microsoft® Windows® applica-tion on an Apple MacBook Pro,” said Dec-lan Dunphy, Manager of Ultrasound Prod-ucts at Siemens Healthcare. “Not only does it combine the flexibility, usability and mobility of a laptop, but it also fea-tures the excellent image quality of a full conventional ultrasound system.”
The P50 units were chosen by Echotech for their portability, superior image reso-lution and IT integration capabilities and are used to provide echocardiography services to PCTs in London, the South East and Midlands. The P50 ultrasound units also allow direct access to the internet.
This enables Echotech physiologists to se-curely archive ultrasound images onto its iCardiogram server. Instant storage and recall of the images is essential for the remote reviewing and reporting of echo studies.
Meeting clinical and financial objectives
“Each year thousands of transthoracic echocardiograms are performed. This will continue to rise because it is relatively inexpensive, accurate and non-invasive. With the pressures of 18 week referral to treatment targets, support from the in-dependent sector is vital to ensure PCTs maximise the potential of care in the com-munity,” said Dominic Elton, Managing Di-rector of Echotech.
“Furthermore, Lord Darzi’s Next Stage Review emphasised the importance of fast and convenient access to diagnostic facilities closer to home. This setup re-duces the overall cost of managing dis-
ease and means that more appropriate, and therefore effective, treatment can be implemented at the right time. Im-proved, quality services at lower cost call for an innovative approach to service de-velopment and delivery. With the budget constraints brought about by the reces-sion, these kinds of services can deliver financial as well as clinical advantages,” concludes Elton.
Bringing cardiac care closer to the community
Above: Echotech uses ACUSON P50™ laptop ultrasound systems from Siemens Healthcare to provide community based services to
Primary Care Trusts (PCTs).
1� CORONARY HEART ™
We call it Echo in a HeartbeatTake your workflow to a new dimension with Echo in a HeartbeatTM Instantaneous Volume Imaging.
Knowledge based Workflow for rapid access to complete data.
For further information: www.siemens.com/echoinaheartbeat or 0800 512128
ACUSON SC2000 Echocardiography System
Answers for life. s
Can you see the shape of tomorrow?
SC 2000 A4 advert:Layout 1 15/10/2008 12:01 Page 1

ECHO
Introduction
Caseous mitral annular calcification is considered to be a rare and incidental echocardiographic finding with no ‘mass-related events’ detected by Harpaz et al. They describe diagnosis of caseous calcification had little impact on patient symptoms and morbidity. In this case study however, extrusion of the caseous mass was associated with an episode of acute pulmonary oedema with new significant mitral regurgitation.
Caseous calcification of the mitral annulus has been reported as an uncommon variation of mitral annular calcification. Described previously in the literature as a soft, periannular extensive calcification, it can be readily picked up on both transthoracic and transoesophageal echo. Commonly misdiagnosed on echocardiography as a tumour or myocardial abscess in cases where cardiotomy has been performed, the entity has been discovered to contain a mixture of calcium, fatty acids and cholesterol with a toothpaste like texture.
Transthoracic echocardiography cases describe a large round mass sometimes with central echolucencies, situated in the posterior mitral annulus. Concluding that this impressive lesion appeared to carry a benign prognosis, conservative treatment was recommended. When the patient presented with acute pulmonary oedema, serial echocardiograms described an undocumented finding.
Case Report:
An 82y.o asymptomatic female presented to our clinic for assessment of a suspected left atrial mass. First detected on routine transthoracic echo five years earlier, assessment of any progression in mass morphology was requested.
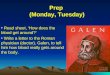
Transthoracic echocardiography revealed a large homogenous circumscribed and echo dense mass arising from the posterior mitral annulus. The mass was well demarcated with mitral chordal attachment, suggesting incorporation and replacement of the posterior mitral leaflet. The mass was measured from 2D echocardiography as 2.9 x 2.2 x 3.5cm. Other echocardiographic
findings included normal left ventricular function (EF 55%) with moderate left ventricular hypertrophy (LV mass index 139gm/m2). Mild pulmonary hypertension (PASP 44mmHg) centrally directed mitral regurgitation and normal left atrial volume were also recorded (20cc/m2).
The mass was identified as severe posterior mitral annular calcification and referred back to the patients local doctor. No intervention was deemed necessary.
Caseous Mitral Annular Calcification
- by Narelle Cranston Adams , Senior Echocardiographer for CVS formerly known as Echo Services, Australia
Figures 1 & 2 (above and below): Pre-rupture, Parasternal Long Axis Vews
1� CORONARY HEART ™

ECHO
Three weeks later the patient presented to the emergency centre of a major public hospital with shortness of breath. Echocardiography showed the mitral annular mass was now an echodense sclerotic capsule with echolucent interior. A mobile echodensity was observed on the posterior leaflet which was determined unlikely to be chordal rupture or a flail mitral leaflet.
The left ventricular function was normal and the pulmonary artery pressure was 70mmHg. There was also a dilated left atrium and severe mitral regurgitation. The patient developed pulmonary oedema which settled after treatment with oxygen and Frusimide. Repeated blood cultures were negative as were all other stigmata for infective endocarditis.
Discussion
Caseous mitral annular calcification has been defined in a rare subgroup of patients that is yet to be widely recognised nor described by echocardiographers. The diagnosis of caseous mitral annular calcification is difficult based on patient clinical symptoms due to the lack of correlation between its presence and clinical findings. Incidence in the general population has been reported as very low but until this classification is more widely recognised and reported, its true incidence is uncertain.
Echocardiography immediately following the development of acute pulmonary oedema showed the development of significant mitral regurgitation. The predominantly anteriorly directed jet with broad spray pattern suggested an acute event involving the posterior mitral valve leaflet and its support structures. The discovery of the small mobile echodensity attached to the posterior annular mass following patient symptoms was another interesting development detected on the transthoracic echocardiogram. Its appearance was not suggestive of a flail mitral leaflet nor a ruptured chordae tendinae. Initially it was thought likely to be a vegetation, however all other indications of infective endocarditis were absent. Hence it was proposed that this mobile echodensity may represent part of the ruptured capsule of the mitral annular mass. Further echocardiogram studies showed no significant change over time.
Transthoracic echo has proved a good tool for diagnosing caseous calcification of the mitral annulus and its delineation from more common mitral annular calcification. In diagnosed cases where transoesophageal echocardiography has been undertaken for further entity assessment, results determined that transoesophageal echo produced clearer images of the structure and the central liquefaction, but did not provide significant additional information to influence in patient treatment.
ReferencesHarpaz D, Auerbach I, Vered Z, Motro M, Tobar A, Rosenblatt S. Caseous calcification of the mitral annulus: A neglected, unrecognised diagnosis. J Am Soc Echocardiogr 2001;14:825-31.
Teja k, Gibson RS, Nolan SP. Atrial extension of mitral annular calcification mimicking intracardiac tumor Clin Cardiol 1987;10:546-8.
Borowski A, Korb H, Voth E, de Vivie ER. Asymptomatic myocardial abscess. Thorac Cardiovasc Surg 1988;36:338-40.
Gilbert HM, Grodman R, Chung MH, Hartman G, Krieger KH, Hartman BJ. Sterile, caseous mitral valve “abscess” mimicking infective endocarditis. Clin Infect Dis 1997;24:1015-6.
Kautzner J, Vondracek V, Jirasek A, Belohlavek M. Tumor-like mitral annular calcification with central liquefaction. Echocardiography 1993;10:459-63.
Pomerance A. Pathological and clinical study of calcification of the mitral valve ring. J Clin Pathol 1970;23:354-61
Kronzon I, Winer HE, Cohen ML. Sterile, caseous mitral annular abscess. J am Coll Cardiol 1983;2:186-90
1.
2.
3.
4.
5.
6.
7.
Figures 3 & 4 (above and below): Post, Parasternal Long Axis Vews
CORONARY HEART ™ 1�

PHARMA
Objectives:Review & update multidisciplinary Practitioners in the latest therapeutic data available following the International Cardiology Conferences and Clinical Trial Results. Network with delegates throughout the UK
Cardiovascular Therapeutic Update 200926th & 27th November 2009, London
Further information from [email protected] or [email protected]
CCO National Conference
Bivalirudin is a direct thrombin inhibitor (acti ng independently of the cofactor anti thrombin III),
inhibiti ng both clot-bound and free circulati ng thrombin. It has a much more predictable pharmacokineti cs than heparin.
Bivalirudin in Unstable Angina and NSTEMI
There are a number of clinical trials investi gati ng bivalirudin in UA and NSTEMI. The ACUITY trial was the largest of the studies, recruiti ng over 13,000 pati ents with moderate to high risk NSTEMI. The study investi gated the use of unfracti onated heparin (UFH) or enoxaparin plus Glycoprotein IIb/IIIa inhibitor, against bivalirudin plus Glycoprotein IIb/IIIa inhibitor against
bivalirudin monotherapy. The study concluded that there was no stati sti cally signifi cant diff erence in the 30 day composite ischaemia endpoints between UFH/Enoxoparin plus GP IIB/IIIa inhibitor versus bivalirudin monotherapy. There was however, a signifi cant reducti on in 30 day net clinical outcome (death, MI, unplanned revascularisati on and major bleed) (p= 0.015). Bivalirudin monotherapy showed an advantage in terms of signifi cant reducti on in major bleeding (p<0.0001) (1).
Bivalirudin in STEMI
The HORIZONS-AMI trial investi gated over 3,000 pati ents with STEMI undergoing PCI. Pati ents were randomised to bivalirudin or UFH plus GP IIb/IIIa inhibitor. Bivalirudin signifi cantly reduced rates of 30 day major bleeding (p<0.001) and demonstrated that bleeding had a signifi cant impact on early and long term mortality. Despite the bleeding benefi t and clear mortality
advantage in bivalirudin group, there was a higher rate of acute (<24hour) stent thrombosis in this group compared with heparin plus GP IIb/IIIa inhibitors (p=0.0002) (2).
References
Stone GW, McLaurin BT, Cox DA. ACUITY Investi gators. Bivalirudin for pati ents with acute coronary syndromes. N Engl J Med 2006; 355: 2203-2216.
Stone GW, Witzenbichler B, Guagliumi G, et al. HORIZONS-AMI Trial Investi gators. Bivalirudin during primary PCI in acute myocardial infarcti on. N Engl J Med 2008; 358: 2218-2230.
Readers are recommended to consult the European Heart Journal Supplement Volume 11, Supplement C, June 2009 for further details.
1.
2.
Dr Mojgan H Sani, DPharm, MBA, MRPharmSHead of Clinical Pharmacy, Royal Berkshire Foundation NHS Trust.
Bivalirudin- Does the new anti-thrombotic off er an advantage in bleeding in coronary revascularisation?
20 CORONARY HEART ™

SITE VISIT
Christchurch Hospital, NZChristchurch Hospital2 Riccarton Avenue, Addington, Canterbury 8011, New Zealand
Largest Tertiary, Teaching, and Research Hospital in the South Island.
2,931 cases performed in 2008.
•
•
Christchurch City is sited on the Canterbury Plains between the Southern Alps and the Pacifi c
Ocean and has a populati on approaching 400,000 people. The surrounds off er beach suburbs, protected bays, and snow-capped mountain ranges for skiing, hiking, mountain biking and climbing. The city itself has a relaxed and cosmopolitan centre with historic trams ratt ling along several streets, a great bar and restaurant scene, theatres, street buskers, museums and art galleries.
Christchurch, named aft er Christ Church College in Oxford University, is the largest city in the South Island of New Zealand and is oft en referred to as the most English of New Zealand’s citi es and the gateway to the South Island. The atmosphere is reminiscent of an English university town, off ering punti ng on the River Avon, a grand Anglican cathedral dominati ng the central square, elegant Victorian architecture and
numerous parks and exquisite gardens. Christchurch City is recognised as New Zealand’s ‘Garden City’ with over 740 parks and an extensive system of rivers, streams and wetlands. It off ers a temperate climate and knows all four seasons, oft en in the one day.
Christchurch Hospital located within a 10 minute walk from the central city and is surrounded by the Avon River, Botanic Gardens and Hagley Park. Hagley Park is renowned for its extensive area of 165 hectares (407 acres) containing a golf course, tennis courts, numerous sports grounds, tree-lined walking and cycling tracks and arti fi cial lakes. Hagley Park is also the locati on for Christchurch Hospital emergency helipad.
The following questi ons were answered by Tina Bailey, Cardiac MRT, in consultati on with the Clinical Director, Charge Radiographer, Charge Tech and Charge Nurse.
What is the size of your Cath Lab facility / Hospital?
Christchurch Hospital is the largest terti ary, teaching and research hospital in the South Island employing 3,400 staff and providing services to over 35,600 inpati ents each year. The hospital operates 600-650 beds. Doctors and specialists from here also travel to major centres in the South Island providing specialist clinics and operati ons. In additi on, Christchurch Hospital has the busiest Emergency Department in Australasia treati ng more than 65,000 pati ents a year.
Currently there are two Cath labs at Christchurch Hospital, one used principally for electrophysiology but also used for diagnosti c angiograms and angioplasti es and the other for diagnosti c coronary, angiograms and PCIs and other interventi onal procedures. There are two cardiology wards (55 beds in total) and one Coronary Care Unit (9 beds).
Fast Facts
Back Row L to RChris Hudson (RN), Dr James Blake, Dr Richard Troughton2nd to Back Row L to RWendy Yesberg (MRT), Greg Cross (RN), Dr Sally Aldous2nd to Front Row L to RShirley Kirby (MRT), Maureen McHenry (RN), Kim Knight (Cardiac Tech), Ruth Cameron (RN), Helen Warwick (RN)Front Row L to RAnna Davis (RN), Dorina Armie (Cardiac Tech), Tina Bailey (MRT), Maxine Rhodes (RN)
CORONARY HEART ™ 21

SITE VISIT
22 CORONARY HEART ™
Christchurch Hospital (cont...)
How many staff? Roles?
Cardiologists: There are 10 cardiologists including 5 interventional specialists and 2 electro-physiologists. There is also 1 EP Fellow, 1 Research Fellow and 3 Advanced Trainees assisting the consultant cardiologists.
Nurses: A total of 16 nurses (12 FTE) are employed on full time, permanent part-time and a casual basis. 2 nurses are assigned to care for the patients in our 7 bed Day Ward attached to the Cath lab; the other nurses are rostered to the labs and are responsible for circulating and scrubbing during procedures. The nurses are also responsible for pre-admission checks. TOEs and DSEs are performed adjacent to the Day Ward and our nurses assist with these procedures also. Some of the nurses participate in a nurse led pre-admission health assessment clinic for EPs patients.
Radiographers (MRT): There are 7 cardiac radiographers (4.8 FTE) employed solely by cardiology to work in the labs. All work on a part-time basis and are responsible for radiation safety, operation of the x-ray
equipment, image archiving and assist with preliminary reporting for the cardiologists. The radiographers also ensure that old studies are transferred from the old GEMNET archiving system to the new ProSolv system.
Cardiac Physiologists: 11 cardiac techs (8.5 FTE) are rostered to the Cath labs on a rotational basis and they also staff the pacing clinic and the ECG department. The techs are responsible for monitoring the ECG and hemodynamic status, as well as recording the equipment used during the procedures. They also assist with IABP management and temporary pacing wire insertions.
For most procedures, the team consists of a cardiologist, 2 registered nurses (1 scrub and 1 circulating), 1 radiographer and 1 cardiac tech.
Types of procedures:
We perform diagnostic C/Angios, PCIs, IVUS, Rotablator, Septal Ablations, Pericardiocenteses, Pericardial windows for malignancy, EP studies, Ablations, Pulmonary Vein Isolations, ICDs, and PPIs including CRT. We are also involved in several ongoing international clinical trials.
We do not officially operate a 24 hour PAMI service as yet due to limited funding. Patients are thrombolysed
Above: Dr James Blake and Dr Sally Aldous
Above: Dr Sally Aldous, Tina Bailey (MRT), and Phyllis Hyde (RN)
SITE VISIT
CORONARY HEART ™ 23
between 2200 and 0600 however; the On Call team are called in for major infarcts, failed thrombolysis, cardiogenic shock and on a case by case basis. Once funding is approved, we will be able to provide a 24 hour PAMI service.
Equipment:
The EP lab has a GE Advantx LC+ x-ray system with a Prucka hemodynamic system. This lab was installed in 2000 and is due for an upgrade in the very near future. The interventional lab was upgraded July 2007 and a Siemens Artis dFC and Sensis hemodynamic system was installed. A ProSolv Cardiovascular archiving and reporting system was implemented at the same time as the lab upgrade and replaced a GEMNET archiving system. An OEC 9600 mobile image intensifier is located in the Coronary Care Unit for insertion of Temp Wires, Swan Ganz and IABPs. We also have a Volcano s5i IVUS system and a RADI Pressure wire system.
Procedures performed per year:
In 2008 we performed 2,931 cases. This included 900 PCIs, 1313 C/Angios, 220
EPs (85 of these were 3D mapping), 80 ICD implants (20 of these were CRT-Ds), 230 PPI (20 of these were CRT-P).
Cross-training of staff:
Not at present but all disciplines assist one another as required. Cross training may be implemented in the future.
New procedures implemented:
One cardiologist has recently started performing PFO closures, Valvuloplasties and the occasional peripheral stenting. We are also about to participate in a clinical research trial involving the use of OCT (Optical Coherence Tomography). We have also recently implemented same day discharges post PCI on suitable patients.
Inventory Management:
Barcodes are removed from the equipment as it is used and the purchasing officer is responsible for ensuring our stock is replaced. Some stents are on consignment.
Haemostasis Management:
The majority of our diagnostic procedures have manual compression. We use Angioseals and Starclose closure
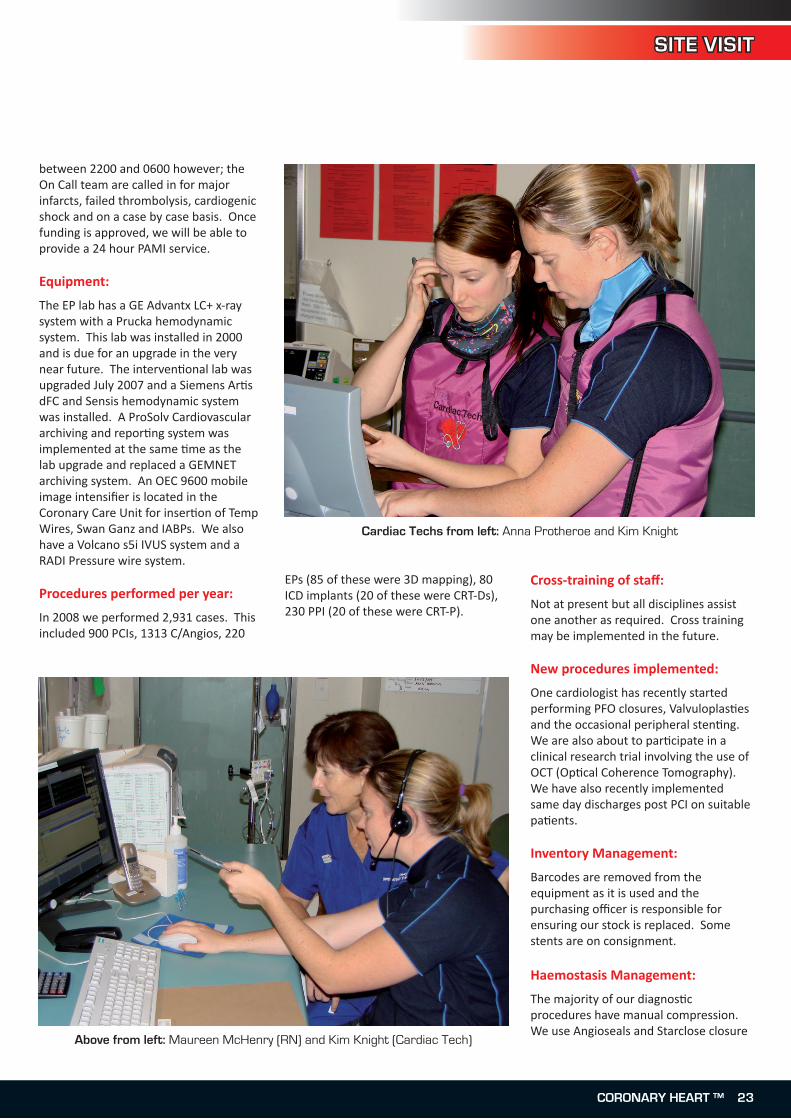
Cardiac Techs from left: Anna Protheroe and Kim Knight
Above from left: Maureen McHenry (RN) and Kim Knight (Cardiac Tech)

SITE VISIT
devices for most of our PCIs but it is very much operator and patient dependent. Syvek, M-Patch and FemoStop are used if there is difficulty obtaining haemostasis. TR bands are used on all radial access patients.
Measures implemented to cut costs:
Budget constraints and constant ‘blow-outs’ are an ongoing concern. We have implemented same day discharge for some PCIs and are considering the purchase of an ACIST device to reduce our contrast budget as 99% of our patients receive Visipaque.
Training for new employees:
Nurses have a 6-8 week preceptorship programme tailored to suit individual needs. Ongoing supervision continues until proficient practice is achieved.Radiographers are paired with an experienced radiographer for on-the-job training and must have competencies signed off before working independently.Cardiac techs have on-the-job training and are expected to complete a Post Grad Diploma in Medical Technology within the first 3 years of employment.
Continuing education programs available to staff:
We try to have weekly in-house training sessions, product training from reps and our clinical nurse educator organises regular study days for all cardiology staff. As many staff as possible attend annual Australian and New Zealand conferences. Each discipline is also responsible for ensuring competencies are kept up to date.
Kinds of competency checks staff have to undergo once employed:
All staff undertake annual CPR training and assessments. Each discipline must supply evidence of participation in ongoing professional development to obtain annual registration with their relative professional body.
Department Management structure.
Nurses report to the Charge Nurse, radiographers report to the Charge Radiographer and techs report to the Charge Cardiac Physiologist. In turn, the Charges report to the Clinical Director and the Cardiology Service Manager
Dealing with late finishing of cases:
Late finishes are becoming more common place as greater demands are put on the Cath lab service. At present, dealing with late finishes relies heavily on the goodwill of staff volunteering to work overtime. Some disciplines call in their On Call person and others alter their shifts to cover the end of the day. We all try to do the best we can to enable patients to get home as early as possible. In addition, planned ‘late lab’
and weekend sessions occur from time to time to cope with increased waiting lists.
Policy for company reps within the labs?
Company reps are generally welcome and are supposed to contact the Charge Nurse and arrange an appointment to visit the labs to ensure that reps from different companies are not present at the same time.
What is the best part of working at your facility?
We have an awesome group of people who all possess a great sense of enjoyment and team ethic. This is reflected by the positive comments from patients who have experienced our professional attitude combined with a wonderful sense of humour.
Above: Wendy Yesberg (Aussie MRT)
Special thanks to Greg Cruickshank, Chairman of the Cardiac Radiographers Advisory Group (CRAG) for
organising this visit and taking the photos.
Christchurch Hospital (cont...)
24 CORONARY HEART ™
ECG ANSWER
ECG Challenge Answer
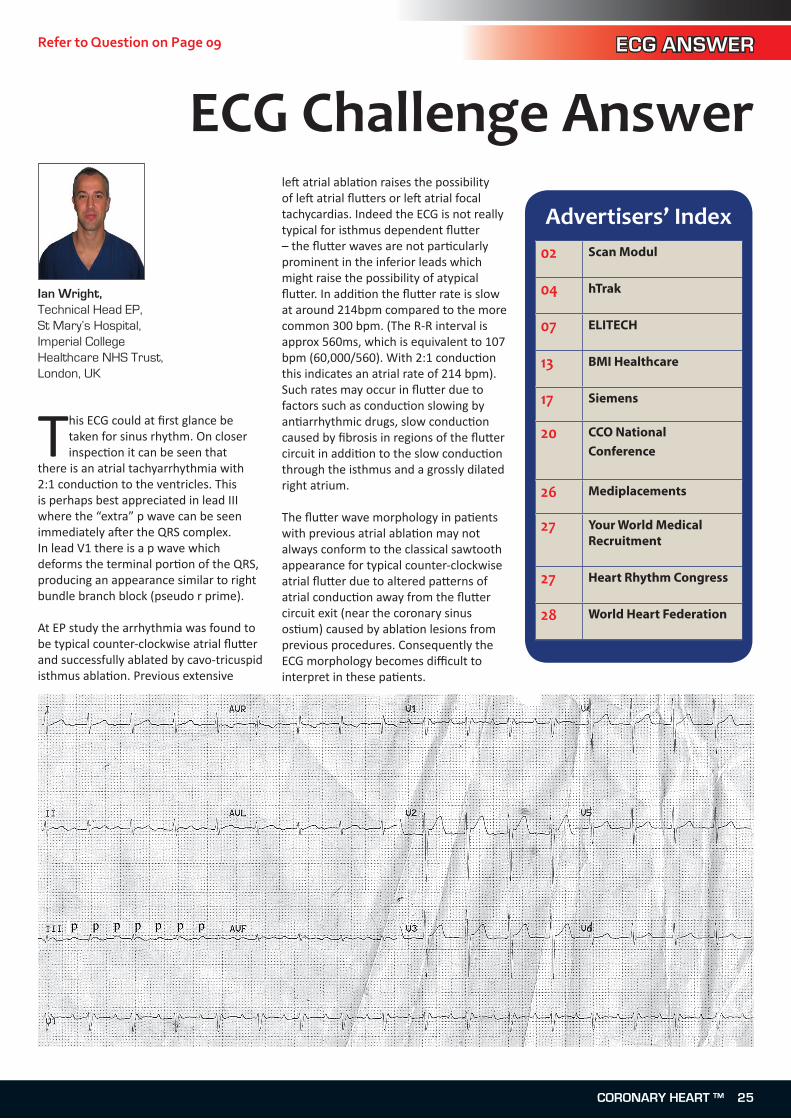
This ECG could at fi rst glance be taken for sinus rhythm. On closer inspecti on it can be seen that
there is an atrial tachyarrhythmia with 2:1 conducti on to the ventricles. This is perhaps best appreciated in lead III where the “extra” p wave can be seen immediately aft er the QRS complex. In lead V1 there is a p wave which deforms the terminal porti on of the QRS, producing an appearance similar to right bundle branch block (pseudo r prime).
At EP study the arrhythmia was found to be typical counter-clockwise atrial fl utt er and successfully ablated by cavo-tricuspid isthmus ablati on. Previous extensive
left atrial ablati on raises the possibility of left atrial fl utt ers or left atrial focal tachycardias. Indeed the ECG is not really typical for isthmus dependent fl utt er – the fl utt er waves are not parti cularly prominent in the inferior leads which might raise the possibility of atypical fl utt er. In additi on the fl utt er rate is slow at around 214bpm compared to the more common 300 bpm. (The R-R interval is approx 560ms, which is equivalent to 107 bpm (60,000/560). With 2:1 conducti on this indicates an atrial rate of 214 bpm). Such rates may occur in fl utt er due to factors such as conducti on slowing by anti arrhythmic drugs, slow conducti on caused by fi brosis in regions of the fl utt er circuit in additi on to the slow conducti on through the isthmus and a grossly dilated right atrium.
The fl utt er wave morphology in pati ents with previous atrial ablati on may not always conform to the classical sawtooth appearance for typical counter-clockwise atrial fl utt er due to altered patt erns of atrial conducti on away from the fl utt er circuit exit (near the coronary sinus osti um) caused by ablati on lesions from previous procedures. Consequently the ECG morphology becomes diffi cult to interpret in these pati ents.
Advertisers’ Index02 Scan Modul
04 hTrak
07 ELITECH
13 BMI Healthcare
17 Siemens
20 CCO National Conference
26 Mediplacements
27 Your World Medical Recruitment
27 Heart Rhythm Congress
28 World Heart Federation
Ian Wright, Technical Head EP, St Mary’s Hospital,Imperial College Healthcare NHS Trust, London, UK
Refer to Question on Page 09
CORONARY HEART ™ 25

Next Issue:
Events Diary:July 20Essentials Of Radial AccessUniversity Hospital of North StaffordshireVisit: www.radi.se/radialaccess
September 24-25Europe AF 2009Hilton London Metropole HotelVisit: www.europeaf.com
October 5-65th She� eld Practical Cath Lab CourseMedical Education Centre, Northern General Hospital, Herries Road, Sheffi eld S5 7AUVisit: www.angioed.com
October 18-21Heart Rhythm Congress 2009Hilton Birmingham Metropole, BirminghamVisit: www.heartrhythmcongress.com
November 26-27CCO National Conference LondonEmail: [email protected]
Edition 20 (September / October 2009)
Electrophysiology
Growing your EP department.
Ian Wright’s Education article
Preview of Heart Rhythm Congess 2009 in Birmingham.
Interview with Mark Hall, EP cardiologist.
Invasive Cardiology
The Amsterdam Project at The Liverpool Heart and Chest NHS Trust and interview with Dr Rod Stables.
Management
Inventory Management for your department.
•
•
•
•
•
•
Like to advertise or submit articles? See page 3
2� CORONARY HEART ™
RECRUITMENT

Heart Rhythm Congress 2009
18 – 21 October 2009 Birmingham
UK
Arrhythmia Alliance PO Box 3697 Stratford upon Avon Warwickshire CV37 8YL UK Telephone: +44 (0) 1789 450 787
Promoting better understanding, diagnosis, treatment and quality of life for individuals with cardiac arrhythmias
HeartRhythm
Congress
www.heartrhythmcongress.comTel: +44 (0) 1789 451822 Email: [email protected]
HRC Advert Landscaped 2009.indd 1 17/04/2009 11:38:51CORONARY HEART ™ 27CORONARY HEART ™ 27
RECRUITMENT
Medical Recruitment
Short &Long termVacanciesAvailableCall the our specialist team direct
020 7426 [email protected]
GENERAL RADIOGRAPHYECHOCARDIOGRAPHYSONOGRAPHYSLEEP STUDIESMRIPACINGCATH LABEPRESPIRATORYEEG’S
Cardiac and RespiratoryRecruitment SpecialistsWe have the latest temporaryand permanent positionsavailable throughout the UKand worldwide.

World Congress of CardiologyScientific Sessions 2010Featuring the 3rd International Conference on Women, Heart Disease and Stroke
16 –19 June 2010 | Beijing, China
www.worldcardiocongress.org
WCC_advert_A4.indd 1 17.3.2009 9:50:36