-
8/14/2019 Cope Study
1/9
ORIGINAL CONTRIBUTION
A Biobehavioral Home-Based Interventionand the Well-being of
PatientsWith Dementia and Their CaregiversThe COPE Randomized
TrialLaura N. Gitlin, PhD
Laraine Winter, PhD
Marie P. Dennis, PhD, EdM
Nancy Hodgson, PhD, RNWalter W. Hauck, PhD
AMONG THE MORE THAN 5 MIL-lion dementia patients in theUnited
States, most live athome, cared for by family
members.1 Functional decline, a coredisease feature, represents
a risk fac-tor for poor quality of life, high healthcare
costs,institutionalization, and mor-tality.2-4Withdisease
progression, fami-lies increasingly provide hands-on
physical assistance with activities ofdaily living (ADLs) and
instrumentalADLs (IADLs). This often results inheightened caregiver
distress,a riskfac-tor for patient nursing home place-ment.5
Few large randomized trials evalu-ate treatments for supporting
physicalfunction of patients with dementia.Trials of antidementia
medicationsshow few if any benefits for physicalfunction or
caregiver burden and havesubstantial adverse effects.6-8 In 1
study,twice-yearly comprehensive care plan-ning in memory clinics
showed no ad-ditional positive effects on functionaldecline.9
Previous nonpharmacologicintervention trials (exercise, use
ofpleasant activities, home environmen-tal modifications) had
promising find-ings, yet studies reported small effectsizes and
outcomes other than func-
Author Affiliations:Jefferson Center for Applied Re-search on
Aging and Health, Thomas Jefferson Uni-versity, Philadelphia,
Pennsylvania (Drs Gitlin, Win-ter, Dennis,and Hodgson); Sycamore
Consulting, NewHope, Pennsylvania (Dr Hauck).
Corresponding Author:Laura N. Gitlin, PhD, Jeffer-son Center for
Applied Research on Aging andHealth, Thomas Jefferson University,
130 S NinthSt, Ste 513, Philadelphia, PA 19130
([email protected]).
Context Optimal treatment to postpone functional decline in
patients with demen-tia is not established.
Objective To test a nonpharmacologic intervention realigning
environmental de-
mands with patient capabilities.Design, Setting, and
Participants Prospective 2-group randomized trial (Care ofPersons
with Dementia in their Environments [COPE]) involving patients with
demen-tia and family caregivers (community-living dyads) recruited
from March 2006 throughJune 2008 in Pennsylvania.
Interventions Up to 12 home or telephone contacts over 4 months
by health pro-fessionals who assessedpatient capabilities and
deficits; obtainedblood and urine samples;and trained families in
home safety, simplifying tasks, and stress reduction. Controlgroup
caregivers received 3 telephone calls and educational
materials.
Main Outcome Measures Functional dependence, quality of life,
frequency of agi-tated behaviors, and engagement for patients and
well-being, confidence using ac-tivities, and perceived benefits
for caregivers at 4 months.
Results Of 284 dyads screened, 270 (95%) were eligible and 237
(88%) random-ized. Data were collected from 209 dyads (88%) at 4
months and 173 (73%) at 9months. At 4 months, compared with
controls, COPE patients had less functional de-pendence (adjusted
mean difference, 0.24; 95% CI, 0.03-0.44; P=.02; Cohen d=0.21)and
less dependence in instrumental activities of daily living
(adjusted mean differ-ence, 0.32; 95% CI, 0.09-0.55; P=.007; Cohen
d=0.43), measured by a 15-item scalemodeled after the Functional
Independence Measure; COPE patients also hadimproved engagement
(adjusted mean difference, 0.12; 95% CI, 0.07-0.22; P =.03;Cohen
d=0.26), measured by a 5-item scale. COPE caregivers improved in
their well-being (adjusted mean difference in Perceived Change
Index, 0.22; 95% CI, 0.08-0.36;P =.002; Cohend=0.30) and confidence
using activities (adjusted mean differ-ence, 0.81; 95% CI,
0.30-1.32; P=.002; Cohen d=0.54), measured by a 5-item scale.By 4
months, 64 COPE dyads (62.7%) vs 48 control group dyads (44.9%)
eliminated1 or more caregiver-identified problems (21=6.72,P =
.01).
Conclusion Among community-living dyads, a nonpharmacologic
biobehavioral en-vironmental intervention compared with control
resulted in better outcomes for COPE
dyads at 4 months. Although no group differences were observed
at 9 months forpatients, COPE caregivers perceived greater
benefits.
Trial Registration clinicaltrials.gov Identifier:
NCT00259454
JAMA. 2010;304(9):983-991 www.jama.com
2010 American Medical Association. All rights reserved.
(Reprinted) JAMA,September 1, 2010Vol 304, No. 9 983
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
2/9
tional dependence or required replica-tion.10,11 Recent
psychosocial care-giver interventions showed caregiverimprovements,
but benefits either didnot extend to patients with dementiaor did
not address functional depen-
dence.
12,13
Building on previous nonpharma-cologic approaches and best
clinicalpractices,14 we designed the Careof Persons with Dementia
in theirEnvironments (COPE) trial to test anonpharmacologic,
biobehavioralapproach to support physical func-tion and quality of
life for patientswith dementia and the well-being oftheir
caregivers. The COPE programtargeted modifiable
environmentalstressors to decrease sensorial, physi-cal, and
cognitive demands and align
with patient capabilities and alsoruled out underlying medical
condi-tions that could lead to reducedpatient functioning. The
interventionsought to re-engage patients in dailyactivities and
increase functionality,thereby alleviating caregiver burden.
We hypothesized that COPE pa-tients, compared with those in a
con-trol group, would show reduced func-tional dependence, improved
quality oflife, and enhanced engagement in ac-tivities at 4 months
(main study end
point). We also hypothesized thatCOPE caregivers, compared with
con-trol caregivers, would report im-proved well-beingand
confidence usingactivities at 4 months. Also consid-ered was
whether COPE reduced oc-currences of agitated behavior
andeliminated problem areas identified bycaregivers.Because the
COPE study in-cluded a brief medical screento rule outundiagnosed
medical conditions, preva-lence of these conditions are reportedfor
intervention patients. Secondarily,
we evaluated long-term effects (at 9months).
METHODS
Study Population
Patients with dementia and familycare-givers were recruited from
March 2006to June 2008 through media announce-ments and mailings by
social agencies
targeting caregivers. Study proce-dures wereexplained to
interested care-givers contacting the research team(telephone,
return postcard),and a brieftelephone eligibility screen was
admin-istered. Eligible patients had a physi-
cian diagnosis of probable dementia(using criteria from
NINCDS/ADRDA[National Institute of Neurological andCommunicative
Disorders and Stroke/Alzheimers Disease and Related Dis-orders
Association]) or a Mini-MentalState Examination (MMSE)15 score
lessthan 24; theyalso were 21years or olderand English speaking,
needed helpwithdaily activities or had behavioral symp-toms, and
lived with or within 5 milesof family caregivers. Eligible
care-givers provided oversight or care for 8or more hours weekly,
planned to live
in the area for 9 months, were not seek-ing nursing home
placement, and re-ported difficultymanaging patientfunc-tional
decline or behaviors.
Exclusioncriteria for dyads were ter-minal illnesses with life
expectancy ofless than 9 months, active treatmentsfor cancer, more
than 3 acute hospital-izations in the past year, or involve-ment in
another caregiver trial. Pa-tients were excluded if they
hadschizophrenia or bipolar disorder, haddementia secondary to
probable head
trauma, orhad an MMSEscore of0 andwere bed-bound.
Written informed consent was ob-tained from caregivers prior to
base-line interviews using forms approvedby the institutional
review board. Care-givers provided proxy patient consentand patient
assentwas obtained for eachpatient-related assessment
usingscriptsapproved by the institutional reviewboard. Families
were compensated $20at each interviewfor their participation.
Following baseline interviews, dy-
ads were randomized to the COPE orcontrol group and reassessed
by tele-phone at 4 and 9 months by interview-ers masked to
participant group. Con-sistent with other trials,13,16 caregiversof
patients placed in nursing homesprior to 4 months (n=7) were
reas-sessed at 4 months (but not 9 months)in areas amenable to
reporting. Care-
givers of patientswho died (n= 21) werenot reassessed at 4
months (n=9) or 9months (n= 12) nor included in analy-ses, as
outcome measures were not rel-evant.
Randomization
Dyads were stratified by living arrange-ment (alone/together)
and random-ized within each stratum using ran-dom permuted blocks
to control forpossible changesin participant mixovertime. The
blocking number was devel-oped by the project statistician and
un-known to others. Randomization listsand 2 sets of randomization
forms wereprepared using opaque envelopes. Theproject director
randomized each dyadwithin 48 hours of the baseline inter-view.
Treatment Conditions
The COPE program sought to supportpatient capabilities by
reducing envi-ronmental stressors and enhancingcaregiver skills. In
this multicompo-nent intervention, all COPE dyads re-ceived
exposure to each treatment ele-ment: assessments (patient deficits
andcapabilities, medical testing, home en-vironment, caregiver
communication,and caregiver-identified concerns);caregiver
education (patient capabili-
ties, potential effects of medications,pain, constipation,
dehydration); andcaregiver training to address caregiver-identified
concerns and help themreduce stress. Training in problem-solving,
communication, engaging pa-tients in activities, and simplifying
taskswas tailored to address caregiver-identified concerns and
patientcapabilities.
COPE dyads received up to 10 ses-sions over 4 months with
occupationaltherapists and 1 face-to-facesession and
1 telephone session with an advancepractice nurse. Occupational
thera-pists initially interviewed caregivers toidentify patient
routines, previous andcurrent roles, habits and interests,
andcaregiver concerns. They also con-ducted cognitive and
functional testingto identify patient strengths and defi-cits in
attention, initiation and perse-
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
984 JAMA,September 1, 2010Vol 304, No. 9 (Reprinted) 2010
American Medical Association. All rights reserved.
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
3/9
veration, construction, conceptualiza-tion, and memory.17,18
Occupationaltherapists then trained caregivers tomodify home
environments, daily ac-tivities, and communications to sup-port
patient capabilities; use problem-
solving to identify solutions forcaregiver-identified concerns;
and re-duce stress. For each targeted concern,a written action plan
was provided11,13,16
describing treatment goals, patientstrengths, and specific
strategies. In ahome visit, the nurse provided care-givers
health-related information (paindetection, hydration), obtained
patientblood and urine samples, and exam-ined patients for signs of
dehydration.Laboratory evaluations included com-plete blood cell
count, blood chemis-try, thyroid testing of serum samples,
and culture and sensitivity testing ofurine samples.
Patientmedications werereviewed for appropriateness, polyphar-macy,
and dosing using publishedguidelines.19 Caregivers were informedof
results by telephone and mailedcopies to share with the
patientsphysicians.
Dyads assigned to the control groupreceived up to three
20-minute tele-phone calls from trained research staffmembers (not
occupational therapistsor nurses). Using scripts, staff asked
caregivers about carechallenges,mailedrelevant informational
brochures, andreviewed the materials in subsequentcalls. Materials
included tips from theAlzheimers Association and govern-ment
agencies on home safetyand man-aging patient behaviors, functional
de-cline, and caregiver stress. Thiscontrolledfor professional
attention andtailoring of information.
Treatment Implementation
Interventionists for both treatment
groups were independently trained inprotocols through readings,
didacticsessions, and practices. For the COPEgroup, treatment
fidelity was moni-tored through twice-monthly supervi-sion and
audiotapes submitted by in-terventionists, which were reviewed
byinvestigators. For the control group,randomly selected telephone
calls were
monitored for protocol adherence inreal time. In both groups,
intervention-ists completed documentation of du-ration and delivery
content for eachcontact, which was reviewed for ad-herence.The COPE
interventionistsdid
not have contact with the control groupinterventionists.
Measures
Characteristics of dyads that were as-sessed included living
arrangement(alone/together), sex, education, race,age, financial
difficulty (1, not very dif-ficult, to 3, very difficult paying for
ba-sics like food), and use of 10 formal ser-vices (eg, home health
aide). Todescribe the racial background of par-ticipants,
caregivers identified them-selves and the patient with dementia
as
Caucasian/white, black/African Ameri-can, or other.
Patient Outcomes
For functional dependence, we used a15-item measure modeled
after theFunctional Independence Measure,20
previously shown as psychometricallysound and corresponding to
objectivedeterminations of dependence and as-sistance
required.21,22 Items included 8IADLs (telephone, shopping,
mealpreparation, housework, laundry,
travel, medicine, managing finances)and 7 self-care ADLs
(bathing, dress-ing upper/lower body, toileting, groom-ing, eating,
getting in/out of bed). Foreach item, caregivers chose a score
toindicate the following: patients werecompletely independent (a
score of 7);there was a safety concern, excessivetime required, or
assistive devices used(6); patients needed supervision, set-up, or
cueing but no physical help (5);or patients needed physical help (4
fora little help, 25% assistance; 3 for mod-
erate, 50% assistance; 2 for a lot of help,75% assistance; or 1
for complete help,75% assistance). A total mean func-tional
dependence score was derived bysumming across items and dividing
bynumber of items(actual range of means,1.0-6.3). Lower scores
representedgreater dependence (=.92). Sub-scale scores for IADL
dependence
(=.81) and ADL dependence (=.93)were similarly derived.
We us ed th e 12 -i te m va li da te dQuality of LifeAlzheimer
Diseasescale to assess caregiver perceptions ofpatient quality of
life (1, poor, to 4,
excellent).
23
Overall mean responsewas calculated by summing acrossitems and
dividing by number ofitems. Higher scores indicated betterquality
of life (=.78).
Activity engagement was measuredusing a validated 5-item scale24
(eg,showed signs of pleasure/enjoy-ment), with items rated 1 for
never to3 for often.Scores were derived by sum-ming across items
and dividing by num-ber of items, with 1 item reverse coded(actual
range of means, 1.0-2.8). Higherscores indicated greater
engagement
(=.62).We used the 16-item Agitated Be-
havior in Dementia scale to assess agi-tated behaviors in the
past month.25 Atbaseline, caregivers indicated whetheragitated
behaviors occurred (yes/no)and, if yes, the number of times.
Totalnumber of agitated behaviors was de-rived by summingyes items;
a mean fre-quency score was derived by sum-ming across items and
dividing bynumber of items (actual range, 0.0-121.1). Higher scores
indicated greater
number of agitated behaviors and fre-quency.
Caregiver Outcomes
Caregiver well-being (improvement/worsening) was evaluated using
the13-item Perceived Change Index,26
fashioned after pharmacologic trialmeasures and shown to have
strongpsychometric properties. Caregiversrated change in ability to
manage de-mentia, emotional status (anger, dis-tress), and somatic
symptoms (en-
ergy, sleep quality) in the past monthusing 5-point
scales(1,gotmuch worse,to 5, improved a lot). Total mean scorewas
derived by summing across itemsand dividing by number of
items.Higher scores indicated greater im-provement (=.86).
Caregiver confidence using activi-ties over the past month was
mea-
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
2010 American Medical Association. All rights reserved.
(Reprinted) JAMA,September 1, 2010Vol 304, No. 9 985
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
4/9
sured by 5 investigator-developeditems (identify daily
activities patientcan do, involve patient in activities,use
activities to distract patient, man-age boredom, set up activities)
withratings from 0 for not confident to 10
for very confident.
27
Mean scores werederived across items (actual range ofmeans,
0.60-10.00), with higherscores indicating greater
confidence(=.87).
We used a targeted measurement ap-proach employed in medical,
pharma-cologic, psychotherapeutic, and behav-ior management trials
to capture themost challenging problems (eg, behav-
iors, dependence, respite) for care-givers.28,29 For each
identified prob-lem at baseline, caregivers indicated at4 months
whether that problem hadbeen eliminated.
At 9 months, we evaluated care-
giver appraisal of study benefits usingan 11-item
survey.13,16,29 Items con-cerned satisfaction (yes/no) with
par-ticipation (study clearly explained,treated respectfully,
effort required, rec-ommend to others); and used ratingsof not at
all, some, and a great deal forperceived benefits (overall benefit,
de-mentiaunderstanding,confidence man-aging care, enhanced skills,
life easier)
and perceived patient benefits (im-proved daily life, helped
keep patienthome).
Statistical Analysis
Based on previous research, we based
sample size calculation on assump-tionsof 25.0% attrition by 4
months andstudy hypothesis tested at 90% powerto detect
moderateeffect sizes(d=0.45).We used =.05 level test. Given
ex-pected attrition, we planned to ran-domize 230 dyads.2
andWilcoxon rank-sum tests were
used to compare intervention and con-trol participants on
baseline character-
Table 1.Characteristics of Patients With Dementia and Their
Caregivers Who Completed 4-Month Assessment
Characteristic
Control Group
(n = 107)
Intervention Group
(n = 102)
Total
(N = 209) 2
Z
P
ValuePatients with dementia
Age, mean (SD), y 81.8 (9.9) 83.1 (7.8) 82.4 (8.9) 1.00 .33
Sex, No. (%) 3.42 .06
Male 40 (37.4) 26 (25.5) 66 (31.6)
Female 67 (62.6) 76 (74.5) 143 (68.4)
Race, No. (%) 2.18 .34
White 72 (67.3) 75 (73.5) 147 (70.3)
African American 31 (29.0) 26 (25.5) 57 (27.3)
Other 4 (3.7) 1 (1.0) 5 (2.4)
Living arrangement, No. (%) 0.07 .79
Alone 5 (4.7) 4 ( 3.9) 9 ( 4.3)
With caregiver 102 (95.3) 98 (96.1) 200 (95.7)
No. of agitated behaviors, mean (SD) 6.0 (3.0) 6.8 (3.0) 6.4
(3.0) 1.98 .048
MMSE score, mean (SD) 13.6 (7.9) 13.1 (8.2) 13.4 (8.1) 0.51
.61Caregivers
Age, mean (SD), y 62.4 (11.7) 62.0 (12.4) 62.2 (12.0) 0.31
.83
Sex, No. (%) 0.62 .43
Male 10 (9.3) 13 (12.7) 23 (11.0)
Female 97 (90.7) 89 (87.3) 186 (89.0)
Race, No. (%) 5.27 .07
White 71 (66.4) 75 (73.5) 146 (69.9)
African American 31 (29.0) 27 (26.5) 58 (27.8)
Other 5 (4.7) 0 5 (2.4)
Relationship to patient, No. (%) 1.69 .19
Spouse 45 (42.1) 34 (33.3) 79 (37.8)
Nonspouse 62 (57.9) 68 (66.7) 130 (62.2)
Education, No. (%) 7.06 .03
High school 26 (24.3) 38 (37.3) 64 (30.6)Some college 42 (39.3)
24 (23.5) 66 (31.6)
College 39 (36.4) 40 (39.2) 79 (37.8)
Time caregiving, mean (SD), y 3.9 (2.8) 4.0 ( 4.4) 4.0 ( 3.7)
0.57 .84
Financial difficulty, mean (SD) a 2.2 (1.0) 2.2 (1.0) 2.2 (1.0)
0.65 .52
No. of formal services used,mean (SD)
2.39 (1.3) 2.45 (1.27) 2.42 (1.28) 0.38 .70
Abbreviation: MMSE, Mini-Mental State Examination.aValue
represents median response category with 2 indicating not very
difficult paying for basics like food, housing, medical care
(range, 1-3).
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
986 JAMA,September 1, 2010Vol 304, No. 9 (Reprinted) 2010
American Medical Association. All rights reserved.
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
5/9
istics and to compare those who stayedin vs those who dropped
out by 4months (main end point). These pro-cedures were also used
to examine po-tential differences at screening be-tw een el i g i b
l e dy ads w i l l i ng to
participate and those not willing.Means, standard deviations,
and rangesfor outcome measures were com-puted. The normality
assumption foreach dependent measure was tested byexamining the
distribution of residuals.
For main treatment effects, the out-come measure was 4-month
score withdesign variable, living arrangement(alone/together), and
baseline value ofthe outcome measure entered as covar-iates. For
the 4-month sample, wefound statistically significant differ-ences
between treatment groupsat base-
line for caregiver education and num-ber of agitated behaviors
(TABLE 1).Weran additional analyses of covariancewith these
variables as covariates. As re-sults did not differ from the
primaryanalyses, they are not reported. Co-hendwas calculated to
measure effectsize.
Consistent with other trials, to evalu-ate clinical significance
for outcomesreaching statistical significance at 4
months, we used the criterion of a0.50-SD improvement from
baseline tofollow-up.13 This also represents theup-per endof
thedistribution of effect sizesreported in the literature. We
calcu-lated number of dyads improving by
0.50 SD or more from baseline to 4months and compared
proportions be-tween treatment groups using Mantel-Haenszel2
analyses, controlling for liv-ing arrangement. We also
comparedproportion of COPE and control groupcaregivers eliminating
1 or more care-giver-identified problem by 4 monthsusing 2
analysis, controlling for liv-ing arrangement.
To evaluate 9-month effects, inter-vention and control groups
were com-pared on adjusted mean differences(baseline to 9 months)
for each out-
come using the same procedures as for4-month effects. We also
compared in-tervention and control group care-giver perceived
benefit at 9 monthsusing Mantel-Haenszel2 analyses, con-trolling
for living arrangement.
Statistical analysis was performedwith SPSS version 17.0 (SPSS
Inc, Chi-cago, Illinois) with the significance levelset atP.05. All
analyses were 2-sided.Analyses included all caregivers ac-
tively caregiving (not bereaved) andproviding 4-month data.
Following in-tention-to-treat principles, we in-cluded participants
regardless of expo-sure level to treatment.
We adjusted for 6 outcome mea-
sures (functional dependence, activityengagement, quality of
life, frequencyof agitated behaviors, and caregiverwell-being and
confidence) using amethod controlling for false discoveryrate (ie,
proportion of rejected hypoth-eses expected to be erroneous).30
Be-cause .05 significance wasused, we con-trolled the false
discoveryrate to be notmore than 5%. Reported numerical Pvalues
were not corrected for multipleend points, but impact of
adjustmentis noted in TABLE 2.
RESULTSOf 284 screened, 270 dyads (95.1%)were eligible, of whom
237 (87.8%)were willing to participate. No statis-tically
significant demographic differ-ences were found between the
en-rolled dyads and the 33 dyads eligiblebut unwilling to
participate. Study at-trition was low, with 28 dyads (11.8%)lost by
4 months. A higher percentageof male caregivers (n=12, 34.3%)
Table 2. Comparison of Intervention (n = 102) and Control (n =
107) Group Patients and Caregivers at 4 Months a
Mean (SD) Score
AdjustedMean DifferenceBetween Groups
(95% CI)P
ValueCohen
d
Baseline 4-Month Follow-up
Control GroupIntervention
Group Control GroupIntervention
Group
Patient outcomesOverall functional
dependenceb2.8 (1.3) 3.0 (1.2) 3.3 (1.3) 3.7 (1.3) 0.24 (0.03 to
0.44) .02 0.21
IADL dependence 1.8 (1.0) 1.8 (1.0) 2.5 (1.1) 2.8 (1.2) 0.32
(0.09 to 0.55) .007 0.43
ADL dependence 4.1 (1.8) 4.3 (1.7) 4.3 (1.7) 4.6 (1.6) 0.16
(0.09 to 0.42) .21
Activity engagement 2.0 (0.4) 1.9 (0.4) 1.9 (0.5) 2.0 (0.4) 0.12
(0.07 to 0.22) .03 0.26
QOL-AD score 2.1 (0.5) 2.1 (0.4) 2.1 (0.5) 2.2 (0.5) 0.10 (0.00
to 0.20) .06 0.14
ABID score 9.8 (10.7) 11.0 (14.6) 5.5 (8.0) 6.7 (10.6) 0.65
(3.05 to 1.74) .59
Caregiver outcomesPerceived change in
well-being
2.8 (0.5) 2.7 (0.5) 2.9 (0.5) 3.1 (0.6) 0.22 (0.08 to 0.36) .002
0.30
Confidence usingactivitiesc
7.0 (2.2) 6.6 (2.1) 6.9 (2.5) 7.5 (1.9) 0.81 (0.30 to 1.32) .002
0.54
Abbreviations: A BID, Agitated Behaviors in Dementia scale; ADL,
activities of daily living; CI, confidence interval; IADL,
instrumental activities of daily living; QOL-AD, Quality
ofLifeAlzheimer Disease scale.
a Refer to the Methods section for descriptions of the scales
used in all outcome measures. All analyses controlled for living
arrangement (alone vs with caregiver) and baselinevalue of
dependent variable. After adjustment for multiple comparisons by
the method of Benjamini and Hochberg, 30 thePvalues for the 6
primary measures (not counting ADLand IADL subscales) were .006 for
perceived change in well-being and confidence using activities, .04
for overall functional dependence and activity engagement, .07 for
qualityof life, and 0.59 for ABID score.
bThis measure was assessed for 202 patients because 7 patients
were placed in nursing homes and the caregivers were not asked
functional dependence items at 4 months.cThis measure was assessed
for 106 caregivers in the control group because 1 caregiver was
unable to respond to items.
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
2010 American Medical Association. All rights reserved.
(Reprinted) JAMA,September 1, 2010Vol 304, No. 9 987
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
6/9
dropped out compared with femalecaregivers (n =16, 7.9%; 21
=19.9;P .001) (FIGURE 1).
By 9 months, an additional 36 dy-ads (17.2% from 4 months) were
lostto follow-up. Total study attrition by 9
months was 64 dyads (27.0%). This in-cluded 20 deaths (13
control group pa-tients [65%], 7 intervention patients[35%]) and 10
nursing home place-ments (5 control patients [50%], 5intervention
patients [50%]); groupdifferences were not statistically
sig-nificant.
For the 4-month sample, patientshada mean (SD) age of
82.4(8.9)years anda mean (SD) MMSE score of 13.4 (8.1).Most were
female (n =143, 68.4%) andlived with caregivers (n=200,
95.7%).Caregiversreported managingmanyagi-
tated behaviors (mean [SD], 6.4 [3.0])and high functional
dependence(mean[SD],2.9 [1.3]). Most patientswere tak-ing
medications: 95 were taking antide-pressants (40.1%); 77,
medications tomanage behavioral symptoms (32.5%);108, pain
medications (45.6%); and173,memory enhancers (73.3%).
Caregivers were a mean (SD) age of62.2 (12.0) years. Most were
female(n= 1 8 6 , 8 9 .0 %), w hi te (n= 1 4 6 ,69.9%), and
nonspouses (n =130,62.2%; primarily adult sons anddaugh-ters [n=
115, 88.5%]) (Table 1).
Treatment Implementation
Of 102 COPE dyads, 80 (78.4%) com-pleted 8 to 12 sessions; 3
dyads (2.9%)had fewer than 3 sessions. Overall, dy-ads received a
mean (SD) of 9.31 (1.54)face-to-face sessions (mean [SD]
length,68.24 [38.34] minutes) and3.25 (0.79)telephone sessions
(mean [SD] lengths,20.15 [13.12] minutes for occupa-tional
therapists; 6.27 [16.50] min-utes for nurses). Intervention cost
wasestimated as $537.05 per dyad based onnational hourly salary or
fringerates for
occupational therapists ($42.83) andnurses ($74.41), patient
laboratorycosts($120),and themean number andlength of contacts.31
Control group dy-ads received a mean (SD) of 2.83 (0.42)telephone
contacts lasting 15 (8.39)minutes as per protocol.
Undiagnosed Medical Conditions
Among 117 COPE patients, nurse as-sessments were obtained for
107 pa-tients (91.4%) and blood or urinesamples for 92 patients
(85.9%; 3 re-
fused and samples were unattainablefrom 12). Undiagnosed
illnesses oc-curred in 40 patients (37.3%); 3 pa-tients (2.8%) had
2 or more coexist-ing undiagnosed medical illnesses.Conditions
included bacteriuria (n= 6;15%), anemia (n=4; 9%), and
hyper-glycemia (n=2; 5%). For the 40 pa-tients with undiagnosed
medical ill-nesses, 39 caregivers (97.5%) followedup with
physicians; 1 refused. Amongthe 39 caregivers following up
withphysicians, 1 patient was admitted to
a hospital and 29 patients were outpa-tients.
4-Month Outcomes
Statistically significant improvementswere observed in
functional depen-dence for COPE patients (baseline to4 months)
compared with controlgroup patients (adjusted mean differ-
Figure 1.Flowchart of Study Design
284 Patients with dementia andfamily caregiver dyads screenedfor
eligibility
270 Eligible
237 Randomized
117 Randomized to receive intervention 120 Randomized to control
group
102 Included in primary analysis(4-month follow-up)
15 Excluded (did not complete4-month follow-up)
107 Included in primary analysis(4-month follow-up)
13 Excluded (did not complete4-month follow-up)
9-Month follow-up
85 Assessed
22 Discontinued study participation7 Patient died
10 Caregiver refused4 Nursing home placement before
4 months so 9-month assessmentnot offered
1 Nursing home placement andcaregiver refused
9-Month follow-up
88 Assessed
14 Discontinued study participation5 Patient died
3 Nursing home placement before4 months so 9-month assessmentnot
offered
6 Caregiver refused
4-Month follow-up
102 Assessed
15 Discontinued study participation3 Patient died
6 Caregiver refused1 Caregiver changed
2 Nursing home placement andcaregiver refused
3 Dissatisfied with study
4-Month follow-up
107 Assessed
13 Discontinued study participation6 Patient died
3 Caregiver refused1 Caregiver changed
3 Dissatisfied with study
14 Excluded7 Nursing home placement planned1 Nursing home
placement before
baseline2 MMSE score too high2 No dementia (had stroke)1 Patient
died before baseline1 No caregiver distress
33 Excluded (unwilling to participate)
Of the 102 dyads in the intervention group, 3 patients were
placed in nursing homes and caregivers receiveda modified 4-month
assessment. Of the 107 dyads in the control group, 4 patients were
placed in nursinghomes andcaregiversreceived a modified
4-monthassessment. MMSE indicates Mini-MentalStateExamination.
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
988 JAMA,September 1, 2010Vol 304, No. 9 (Reprinted) 2010
American Medical Association. All rights reserved.
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
7/9
ence, 0.24; 95% confidence interval[CI], 0.03-0.44;P=.02;
Cohend=0.21),representing a small effect. Improve-
ment occurred mostly for IADLs (ad-justed mean difference, 0.32;
95% CI,0.09-0.55; P = .007; Cohen d=0.43), amoderate effect. COPE
patients im-proved slightly more in ADL function-ing than controls,
but this was not sta-tistically significant(Table 2). Similarly,we
observed small but statistically sig-nificant improvements in
engagementfor COPE compared with control pa-tients (adjusted mean
difference, 0.12;95% CI, 0.07-0.22; P=.03; Cohend=0.26). We did not
find statistically
significant benefitsfor frequency of agi-tated behaviors or
quality of life.
Compared with control group care-givers, COPE caregivers
reported im-provement in well-being (adjustedmean difference, 0.22;
95% CI, 0.08-0.36;P=.002; Cohend=0.30) and en-hanced confidence
using activities (ad-justed mean difference, 0.81; 95%
CI,0.30-1.32; P=.002; Cohen d=0.54),small to moderate effects
(Table 2).TABLE 3 shows proportions of par-
ticipants with clinically meaningful
changes (0.50 SD)for statistically sig-nificant 4-month
outcomes. Net im-provement across measures favoredCOPE participants
over controls, withdifferences reaching statistical signifi-cance
for all except activity engage-ment. Differences in net
improve-ments ranged from 14.6% to 26.5%. Of112 caregivers (53.8%)
reporting 1 or
more caregiver-identified problemseliminated by 4 months, 64
(62.7%)
were COPE and 48 (44.9%) were con-trol group caregivers
(21=6.72, P=.01).
9-Month Outcomes
We did not find statistically signifi-cant differences between
COPE andcontrol group participants from base-line to 9 months for
any outcome mea-sure. Both intervention and control
group caregivers considered study par-ticipation worthwhile and
not timecon-
suming, felt they were treated respect-fully, and would
recommend the studyto others (allP .14). However, COPEcompared with
control caregivers re-ported a great deal of improvementin their
lives overall (70.9% vs 38.5%,22=20.5,P .001), disease
understand-ing(66.3% vs 43.6%,22=15.0, P=.001),confidence managing
behaviors (72.1%
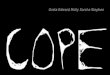
Figure 2.Perceived Benefits of Intervention and Control Group
Caregivers at 9 Months
COPE (n=
88)
Control (n=85)Treated with respect P=.34Study satisfaction
Study clearly explained P=.62
Too much work P=.50
Recommend to others P=.14
Benefited you P
-
8/14/2019 Cope Study
8/9
vs 37.2%,22=25.4, P .001), made lifeeasier (45.3% vs 17.9%, 22
=34.2,P .001), ability to care for patients(54.7% vs 26.9%,
22=25.7, P .001),patients quality of life (32.6% vs 10.3%,22=17.0,P
.001), and ability to keep
patients home (39.5 vs 20.8%,2
2=7.5,P=.02) (FIGURE 2).
COMMENT
These findings addto an increasing evi-dentiary base for
nonpharmacologicmanagement of patients with demen-tia. We tested a
multicomponent inter-vention that helped caregivers attendto
patients medical well-being and sim-plify everyday tasks to align
with pa-tient capabilities. COPE addresses coreelements of dementia
care: optimizingphysical health and function, engag-
ing in daily activities, maintaining qual-ity of life, and
supporting caregivers.32
At 4 months, COPE improved patientfunctioning, especially IADLs;
patientengagement; and caregiver well-beingand confidence using
activities. COPEdidnot improve caregiver ratings of pa-tient
quality of life or frequency of agi-tated behaviors, although
change wasin the right direction.
Improvement in patient function, al-beit small, compares
favorably withpharmacologic trials, yet with no
adverse events or known risks. Al-though different functional
measureswere used, trials of dimebon33 andtarenflurbil6 showed no
functionalimprovement, and benefits reported ford o n e z e p i l w
e r e s m a l l ( C o h e nd0.10)34 compared with COPE (Co-hen
d=0.21 for overall function, Co-hend=0.43 for IADL). Other studies
ofcholinesterase inhibitors show statis-tically significant but
small benefits forIADLs and a trend in ADL improve-ment, as in
COPE.7 A multisite study
found no differences in functioningfrom clinic-based
treatments.9 In con-trast, COPE decreased severity of over-all
dependence by 0.7 points and IADLdependence by 1 point. Control
groupcaregivers also reported small func-tionalgainsof 0.5points
overall and0.7points for IADLs, although differ-ences were
statistically significant fa-
voring intervention. As points on thescale reflect increments of
25%in physi-cal assistance required by caregivers, a1-point
reduction may be clinicallymeaningful. Poor patient functioningis a
predictor of disease progression,
heightening risk of caregiver burdenand nursing home
placement.12 Also,dependencies are associated with in-creased
health care costs.3 Thus, evensmall reductions in physical
depen-dence may ease caregiver burden.
As to caregiver effects, pharmaco-logic interventions have shown
onlysmall benefits in caregiver burden(Cohen d=0.18),8 whereas in
thisstudy COPE participants showedhigher effects compared with
controls,from Cohen d=0.29 for well-beingan d d =0.54 for
confidence using
activities to engage patients. Theseimprovements appear to be
clinicallymeaningful. More intervention dyadsimproved 0.50 SD or
more than con-trols on outcome measures. Also,more COPE caregivers
than controlsreported eliminating at least 1 prob-lem initially
identified as challenging.
Consistent with recent studies,16,35 ahigh prevalence (close to
40%) wasfound of undiagnosed, treatable medi-cal conditions for
intervention pa-tients with all but 1 dyad (97.5%)
following up with physicians for treat-ment. However, effects of
their treat-ment are unclear. A comparison ofCOPE patients with
identified andtreated medical problems (n= 39) withCOPE
patientswithout identified medi-cal problems or treatment
(n=63)showed similar 4-month gains. Never-theless, managing
physical health is animportant aspect of dementia care. Highrates
of untreated conditions suggest theneed for more frequent routine
medi-cal examinations because symptoms
maypresent atypically and patientsmaynot be able to report
adequately.At 9 months, there were no statisti-
cally significant differences in out-come measures.
Nevertheless, per-ceived benefits favored intervention.Compared
with controls, COPE care-givers reported a great deal of
im-provement in many areas, including
managing care better and keeping pa-tients home. Lack of
findings for stan-dardized measures contrasts with per-ceived
benefits, highlighting thecomplexity of measuring improve-ments in
quality of life.36
Of importance is that neither groupreported finding the study
burden-some, and both groups participantswere equally willing to
recommend itto others. Training and telephone edu-cation were
equally well received.
Study limitations include an inabil-ity to determine active
treatment com-ponents. The trial was not designed toanswer this
question and COPE re-flects the integration of multiple
com-ponents. COPE may primarily affectcaregiver appraisals. As
outcome mea-sures relied on proxy report, it is dif-
ficult to rule out this pathway.Another limitation is study
general-
izability. Because caregivers volun-teered for participation,
they may havebeen more aware of their role and moremotivated to
learn skills than nonvol-unteers.37 Only 15% of study care-givers
were male and a higher propor-tion of male caregivers than
femalecaregivers dropped out, so it is un-clear how best to address
their needs.1
A concern may be the placebo con-dition. Controls received
information
tailoredto their needs,12
buttheamountof time staff spent providing informa-tion was not
equivalent to that in COPE.Nevertheless, our approach is an
ad-vance over previous studies employ-ing no-treatment comparison
groups.
Because most patients live at homewith functional decline, a
nonpharma-cologic, biopsychosocial-environmen-tal intervention may
positively contrib-ute to disease management. Futureresearch needs
to examine effects ofunderlying medical conditions, ways
to boost treatment effects, cost-effectiveness, COPE in
combinationwith pharmacologic treatments, andtranslational
potential.
Author Contributions:Dr Gitlin had full access to allof the data
in the study and takes responsibility forthe integrity of the data
and the accuracy of the dataanalysis.Study concept and
design:Gitlin, Hauck.Acquisition of data:Gitlin, Winter.
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
990 JAMA,September 1, 2010Vol 304, No. 9 (Reprinted) 2010
American Medical Association. All rights reserved.
wnloaded From: http://jama.jamanetwork.com/ on 10/08/2013
-
8/14/2019 Cope Study
9/9
Analysis and interpretation of data:Gitlin, Winter,Dennis,
Hodgson, Hauck.Drafting of the manuscript:Gitlin, Winter.Critical
revision of the manuscript for important in-tellectual
content:Gitlin, Dennis, Hodgson, Hauck.Statistical analysis:Gitlin,
Winter, Dennis, Hodgson,Hauck.Obtained
funding:Gitlin.Administrative, technical, or material
support:Gitlin,
Winter.Study supervision:Gitlin.Financial Disclosures:None
reported.Funding/Support:Research reported was supportedin part by
funds from the National Institute onAging and the National
Institute on NursingResearch (RO1 AG22254) and the PennsylvaniaDe p
a rtme n t o f He a lth , T o b a cco S e tt le me n
t(SAP100027298).Role of the Sponsor: Funding agencies had no rolein
the design and conduct of the study; in the col-lection, analysis,
and interpretation of the data; orin the preparation, review, or
approval of themanuscript.Additional Contributions:Barry Rovner,
MD, Jeffer-son Hospital for Neuroscience, provided patient
con-sultation, for which he did not receive additional
com-pensation besides his salary. The interventionists
whomadeimportant contributionswere Michele Rifkin, MA,OTR/L, Health
Through Action; Nicole Davis, MS,OTR/L; Lauren Lapin, OTR/L;
Catherine Piersol, MA,OTR/L; Geri Shaw, OTR/L; and Tracey
Vause-Earland, MA, OTR/L, and the nurse interventionist,Kathy
Czekanski,RN, PhD. These individualswereem-ployees or contractors
for Thomas Jefferson Univer-sityand weresupported in part
byfundsfrom thelistedgranting agencies. We also acknowledge the
contri-butions of our interviewing staff and thank the fami-lies
for their study participation.
REFERENCES
1. 2010 Alzheimers disease facts and figures. Alzhei-mers
Association.
http://www.alz.org/documents_custom/report_alzfactsfigures2010.pdf.
Accessed Au-gust 4, 2010.2. AtchisonTB, Massman PJ, Doody RS.
Baselinecog-nitivefunctionpredictsrate of decline in
basic-careabili-
ties of individuals with dementia of the Alzheimerstype. Arch
Clin Neuropsychol. 2007;22(1):99-107.3. HillJ, Fillit H, ThomasSK,
Chang S. Functional im-pairment, healthcare costs and the
prevalence of in-stitutionalisation in patients with Alzheimers
diseaseand other dementias. Pharmacoeconomics.
2006;24(3):265-280.4. Soto ME, Andrieu S, Gillette-Guyonnet S,
CantetC, Nourhashemi F, Vellas B. Risk factors for func-tional
decline and institutionalisation among commu-nity-dwelling older
adults with mild to severe Alzhei-mersdisease:one yearof
follow-up.AgeAgeing. 2006;35(3):308-310.5. Spillman BC, Long SK.
Does high caregiver stresspredict nursing home entry? Inquiry.
2009;46(2):140-161.6. Green RC, Schneider LS, Amato DA, et al;
Taren-flurbil Phase 3 Study Group. Effect of tarenflurbil on
cognitive decline and activities of daily living in pa-
tients with mildAlzheimerdisease: a randomized con-trolled
trial.JAMA. 2009;302(23):2557-2564.7. Trinh NH, Hoblyn J, Mohanty
S, Yaffe K. Efficacyof cholinesterase inhibitors in the treatment
of neu-ropsychiatric symptoms and functional impairmentinAlzheimer
disease: a meta-analysis. JAMA. 2003;289(2):210-216.8. Lingler JH,
Martire LM, Schulz R. Caregiver-specific outcomes in antidementia
clinical drug trials:
a systematic review and meta-analysis.J Am GeriatrSoc.
2005;53(6):983-990.9. Nourhashemi F, Andrieu S, Gillette-Guyonnet
S,et al; PLASA Group. Effectiveness of a specific careplan in
patients with Alzheimers disease: clusterrandomised trial (PLASA
study). BM J. 2010;340:c2466.10. Teri L, Gibbons LE, McCurry SM, et
al. Exerciseplus behavioral management in patients with
Alzhei-merdisease:a randomized controlledtrial.JAMA.
2003;290(15):2015-2022.11. Gitlin LN, Winter L, Corcoran M, Dennis
MP,Schinfeld S, Hauck WW. Effects of the home envi-ronmental
skill-building program on the caregiver-care recipient dyad:
6-month outcomes fromthe Phila-delphia REACH Initiative.
Gerontologist. 2003;43(4):532-546.12. SrensenS, Duberstein P, Gill
D, PinquartM. De-mentia care:mental health effects, intervention
strat-egies, and clinical implications. Lancet Neurol.
2006;5(11):961-973.13. Belle SH, Burgio L, Burns R, et al;
Resources forEnhancing Alzheimers Caregiver Health (REACH)
IIInvestigators. Enhancingthe qualityof lifeof demen-tia caregivers
from different ethnic or racial groups: arandomized, controlled
trial. Ann Intern Med. 2006;145(10):727-738.14. Ballard
CG,GauthierS, Cummings JL,et al.Man-agement of agitation and
aggression associated withAlzheimer disease. Nat Rev Neurol.
2009;5(5):245-255.15. Folstein MF, Folstein SE, McHugh PR.
Mini-mental state: a practical method for grading thecog-nitive
state of patientsfor theclinician.J Psychiatr
Res.1975;12(3):189-198.16. GitlinLN, WinterL, DennisMP, Hodgson N,
HauckWW. Targeting and managing behavioral symptomsin individuals
with dementia: a randomized trial of anonpharmacological
intervention[published online July
19, 2010].J Am Geriatr Soc.
doi:10.1111/j.1532-5415.2010.02971.x.17. Earhart CA.Allen
Diagnostic Modules: Manual.2nd ed. Colchester, CT: S&S
Worldwide; 2006.18. MillerJM, PliskinNH. Theclinicalutility of
theMat-tis Dementia Rating Scale in assessing cognitive de-cline in
Alzheimers disease. Int J Neurosci. 2006;116(5):613-627.19. Fick
DM, Cooper JW, Wade WE, Waller JL,MacleanJR, Beers MH.Updatingthe
Beers criteria forpotentiallyinappropriate medicationuse in
olderadults:results of a US consensus panel of experts. Arch
In-tern Med. 2003;163(22):2716-2724.20. Guide for the Uniform Data
Set for Medical Re-habilitation (including the FIM instrument),
version5.1. Buffalo, NY:StateUniversity of NewYork at Buf-falo;
1997.21. GitlinLN, Roth DL,Burgio LD,et al.Caregiverap-praisals of
functional dependence in individuals with
dementiaand associated caregiverupset: psychomet-
ricproperties of a newscaleand response patterns bycaregiver and
care recipient characteristics. J AgingHealth.
2005;17(2):148-171.22. Cotter EM, Burgio LD, Roth DL, Gerstle
J,Richardson P. Comparison of caregiver and occupa-tional therapist
ratings of dementia patients perfor-mance of activities of daily
living. J Appl Gerontol.2008;27(2):215-225.23. Logsdon RG, Gibbons
LE, McCurry SM, Teri L.
Assessing quality of life in older adults with
cognitiveimpairment. Psychosom Med. 2002;64(3):510-519.24. Albert
SM,Del Castillo-CastanedaC, Sano M, etal.Quality of life in
patients with Alzheimers disease asreported by patient proxies.J Am
Geriatr Soc. 1996;44(11):1342-1347.25. Logsdon RG, Teri L, Weiner
MF, et al. Assess-ment of agitation in Alzheimers disease: the
Agi-tated Behavior in Dementia scale: Alzheimers Dis-ease
Cooperative Study. J Am Geriatr Soc. 1999;47(11):1354-1358.26.
GitlinLN,WinterL, Dennis MP, Hauck WW.As-sessing perceived change
in the well-being of familycaregivers: psychometric properties of
the PerceivedChange Index and response patterns. Am J Alzhei-mers
Dis Other Demen. 2006;21(5):304-311.27. Gitlin LN, Winter L, Burke
J, Chernett N, DennisMP, Hauck WW. Tailored activities to manage
neu-ropsychiatric behaviors in persons with dementia
andreducecaregiver burden: a randomized pilot study.AmJ Geriatr
Psychiatry. 2008;16(3):229-239.28. BattleCC, ImberSD, Hoehn-SaricR,
Nash ER,FrankJD. Target complaints as criteria of improvement. AmJ
Psychother. 1966;20(1):184-192.29. SchulzR, OBrien A, CzajaS, etal.
Dementia care-giver intervention research: in search of
clinicalsignificance.Gerontologist. 2002;42(5):589-602.30.
Benjamini Y, Hochberg Y. Controllingthe false dis-covery rate: a
new and powerful approach to mul-tiple testing. J R Stat Soc Ser B.
1995;57:1289-1300.31. Chartbook: occupational employment and
wages,May 2006 (2008, bulletin 2703). US Dept of
Labor.http://www.bls.gov/oes/. Accessed June 1, 2010.32. Prince MJ,
Acosta D, Castro-Costa E, Jackson J,Shaji KS. Packages of care for
dementia in low- andmiddle-income countries. PLoS Med.
2009;6(11):e1000176.
33. Pfizer and Medivation announce results fromtwophase 3
studies in dimebon (latrepirdine*) Alzhei-mers diseaseclinical
developmentprogram. Pfizerme-diaroom. March 3, 2010.34. R oman GC,
Wilkinson DG, Doody RS, Black SE,Salloway SP, Schindler RJ.
Donepezil in vascular de-mentia: combined analysis of two
large-scale clinicaltrials.Dement Geriatr Cogn Disord.
2005;20(6):338-344.35. Lppnen MK, Isoaho RE, Rih IJ, et al.
Undi-agnosed diseases in patients withdementia:a poten-tial
targetgroup for intervention.Dement Geriatr CognDisord.
2004;18(3-4):321-329.36. Rabins PV, Black BS. Measuring quality of
life indementia: purposes, goals, challenges and progress.Int
Psychogeriatr. 2007;19(3):401-407.37. Pruchno RA, Brill JE, Shands
Y, et al. Conve-nience samples and caregiving research: how
gener-alizable are the findings? Gerontologist. 2008;
48(6):820-827.
HOME-BASED INTERVENTION FOR PATIENTS WITH DEMENTIA AND THEIR
CAREGIVERS
2010 American Medical Association. All rights reserved.
(Reprinted) JAMA,September 1, 2010Vol 304, No. 9 991