Embed Size (px)
Citation preview

COPD Management in 2017
Leonardo Seoane M.D., F.A.C.P.
Associate Professor
Head of School
UQ-Ochsner Clinical School

Objectives
• Review the new 2017 GOLD
guidelines
• Define COPD and classify by
severity
• Apply the treatment guidelines to
clinical case
• Develop COPD quality indicators
for your clinic


Risk Factors for COPD
Nutrition
Infections
Socio-economic
status
Aging Populations
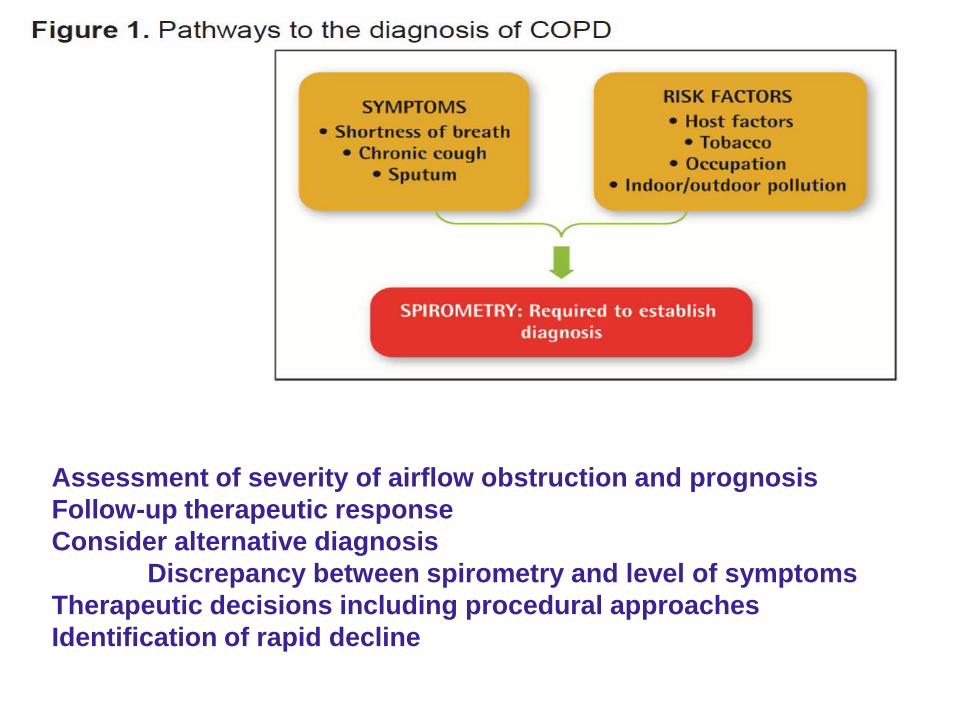
Assessment of severity of airflow obstruction and prognosis
Follow-up therapeutic response
Consider alternative diagnosis
Discrepancy between spirometry and level of symptoms
Therapeutic decisions including procedural approaches
Identification of rapid decline

Spirometry: Normal and
Patients with COPD
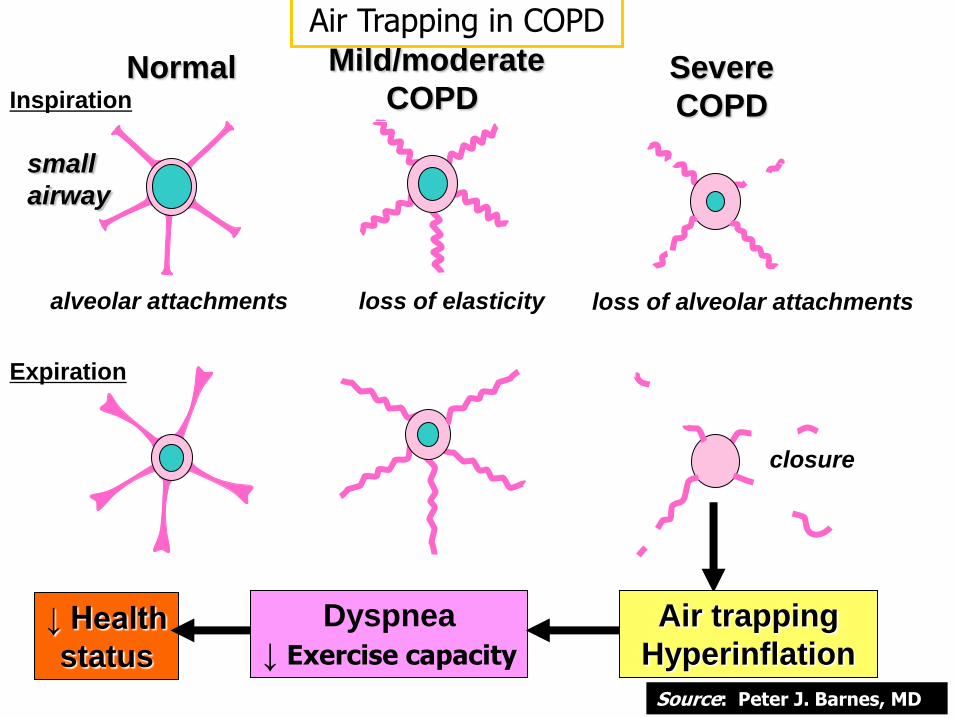
Normal Inspiration
Expiration
alveolar attachments
Mild/moderate
COPD
loss of elasticity
Severe
COPD
loss of alveolar attachments
closure
small
airway
Dyspnea
↓ Exercise capacity
Air trapping
Hyperinflation ↓ Health
status
Air Trapping in COPD
Source: Peter J. Barnes, MD

Performance Metric
Spirometry
What % of patients seen in your clinic with risk factors
and symptoms of COPD had spirometry done and
documented?
The most available, reproducible, standardized and
objective way to measure exhalation air flow limitation.
Although spirometry is essential to diagnose COPD
it is not indicated in asymptomatic individuals

Case 1
• Danny is a 60 y/o male with a history of COPD and 50 pack year history of tobacco.
He quit smoking 5 years ago and has a good support system at home (His wife). He
is coming in for a routine visit, he states he is annoyed about getting SOB climbing up
a flight of stairs at home or walking up the hill to his garden. His spirometry in the
office demonstrates a FEV1/FVC ratio of 50% and FEV1 of 45% predicted. He has
had to visit the clinic twice in the past year for increasing SOB and cough due to his
COPD.
• What is his GOLD classification using refined ABCD assessment tool?
• A Grade 3
• B Grade 3
• C Grade 3
• D Grade 3
Global Strategy for Diagnosis, Management and Prevention of COPD
Assessment of COPD
Assess spirometry
Assess symptoms
History/future risk of exacerbations
Assess comorbidities
© 2014 Global Initiative for Chronic Obstructive Lung Disease
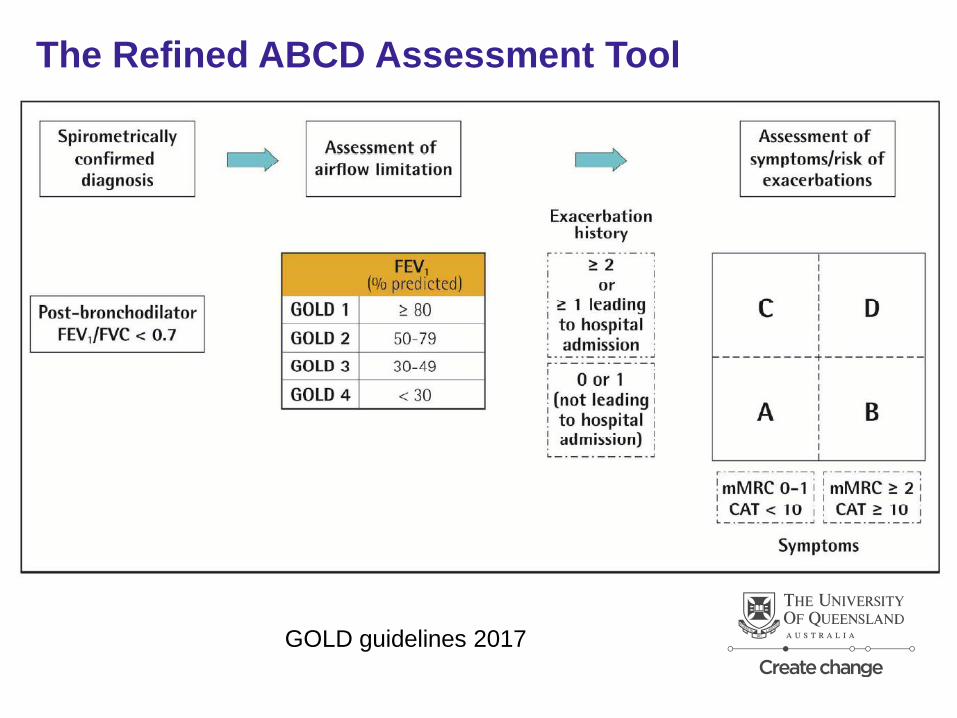
The Refined ABCD Assessment Tool
GOLD guidelines 2017

Modified Medical Research Council (mMRC)
Dyspnea Scale
Grade Description of Breathlessness
0 I only get breathless with strenuous exercise.
1 I get short of breath when hurrying on level ground our walking up a
slight hill.
2 On level ground, I walk slower than people of the same age because of
SOB, or have to stop for breath when walking at my own pace
3 I stop for breath after walking about 100 yards or after a few minutes on
level ground
4 I am too breathless to leave the house or I am breathless when
dressing.

COPD Assessment Test (CAT)
Score
I have cough I cough all the time
I have no phlegm My chest is full
My chest does My chest feels very
Not feel tight tight
When I walk up When I walk up a
Stairs I am not f light of stairs I am very
Breathless breathless
I am not limited I am very limited
doing home activities
I am confident I am not confident leaving
Leaving my home
I sleep soundly I don’t sleep soundly
I have lots of I have no energy at all
energy
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5

Patient Characteristic Spirometric
Classification
Exacerbations
per year
CAT mMRC
A Low Risk
Less Symptoms GOLD 1-2 ≤ 1 < 10 0-1
B Low Risk
More Symptoms GOLD 1-2 ≤ 1 > 10 > 2
C High Risk
Less Symptoms GOLD 3-4 > 2 < 10 0-1
D High Risk
More Symptoms GOLD 3-4 > 2 > 10
> 2
Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or
exacerbation history. One or more hospitalizations for COPD exacerbations should
be considered high risk.)
© 2014 Global Initiative for Chronic Obstructive Lung Disease

Case 1 continues
• What treatment options would you recommend to Danny at this stage?

Goals for Treatment of Stable COPD
GOLD guidelines 2017

Principles of COPD Management
1. Individualized approach based on symptom severity and quality of life
2. Smoking status and risk factors addressed with intervention to improve
cessation
3. Appropriate inhaler technique
4. Screen for Depression and co-morbidities
5. Exercise and rehabilitation (strength & condition)
6. Vaccine, Influenza and Pneumococcal

Fletcher C and Peto R. BMJ. 1977;1:1645-1648.
severe

Smoking and smoking cessation in relation to
mortality in women JAMA 2008;299(17):2037-47
• Tobacco use remains the leading preventable cause of
death in the U.S.
• Background
– WHO projects 10 million tobacco related death annually by year 2030
– Determine the rate of mortality risk reduction after quitting smoking
• Methods
– Nursing health study
– Population based cohort study 104,519

Smoking Health Effects (>1 ½ packs/day)
• 114 (CI 42-306) times higher risk of COPD
• 40 (CI 30-52) times greater risk of developing lung cancer
• Risk of dying from COPD
– 14 X greater if a current smoker
– 155 X greater (CI 59 to 408) >1 ½ packs/day
• After cessation of smoking
• hazard ratios decline for COPD and lung cancer to rates of
non-smokers after 20 years
• 13% reduction in risk of all-cause mortality within 5 years of
quitting
Performance Metric
Smoking Cessation • Tobacco cessation counseling is recommended for all
who smoke.
• Incorporate tools to Identify smokers who received
smoking cessation counseling during an office visit
• Especially COPD patients who still smoke


Performance Metric
Assessment and Documentation of Pneumococcal
and Influenza Immunizations
CDC recommends that all patients with chronic diseases of the pulmonary system should
be vaccinated.
Influenza vaccination reduces: serious illness, death, and exacerbations
Vaccinations decrease the incidence of lower respiratory tract infections
Pneumococcal vaccinations PCV13 and PPSV23 are both effective

Case 1 continues
• What pharmacologic treatment options would you recommend to Danny at this
stage?
• A) Short acting β-agonist four times a day
• B) Inhaled corticosteroid (ICS) daily
• C) Long acting β-agonist (LABA) daily
• D) Long acting muscarinic Agent daily

Patient Characteristic Spirometric
Classification
Exacerbations
per year
CAT mMRC
A Low Risk
Less Symptoms GOLD 1-2 ≤ 1 < 10 0-1
B Low Risk
More Symptoms GOLD 1-2 ≤ 1 > 10 > 2
C High Risk
Less Symptoms GOLD 3-4 > 2 < 10 0-1
D High Risk
More Symptoms GOLD 3-4 > 2 > 10
> 2
Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or
exacerbation history. One or more hospitalizations for COPD exacerbations should
be considered high risk.)
© 2014 Global Initiative for Chronic Obstructive Lung Disease
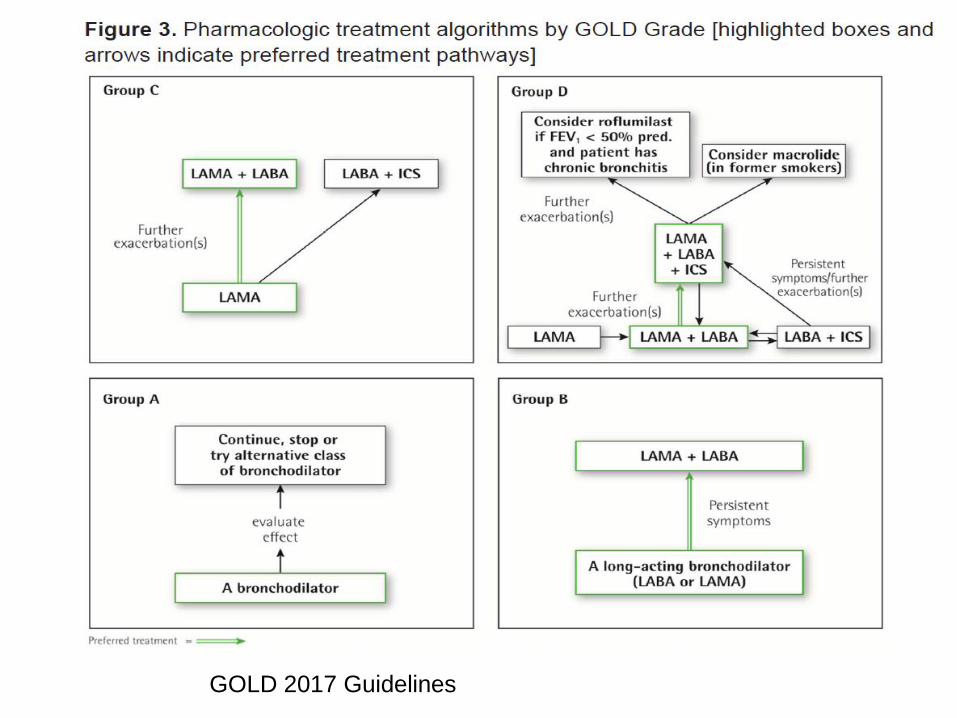
GOLD 2017 Guidelines

Bronchodilators in stable COPD
• Group A
– Regular and PRN use of SABA or SAMA improves FEV1 and symptoms
(Level A)
• Group B, C, and D
– LABA and LAMA significantly improve lung function, dyspnea, health
status, and reduce exacerbations rates (Level A)
– LAMA have a greater effect on exacerbation reduction compared to
LABA (Level A) and decrease hospitalizations (Level B)
– Combination treatment with LABA and LAMA increase FEV1 and
improve symptoms compared to monotherapy (Level A), reduces
exacerbations (level B)
Anti-inflammatory therapy
• Mainly reduce exacerbations
• ICS/LABA is more effective than either monotherapy in improving
lung function and reducing exacerbations (Level A)
• Regular treatment with ICS increases the risk of pneumonia
especially in those with severe disease (Level A)
– Current smokers
– Prior pneumonia
– Body index < 25
• ICS other side effects
– Oral candidiasis
– Horse voice
– Skin bruising

Anti-inflammatory therapy
• Group D
– ICS/LAMA/LABA in select patients improves lung function, symptoms,
and health status (level A)
• reduces exacerbations compared to ICS/LABA
• LAMA monotherapy
• Long term use of oral glucocorticoids has numerous side effects
(level A) with no evidence of benefits (Level C)

Performance Metric: Inhaler Technique

Performance Metric
Inhaler Technique • Key to routine management of any COPD patient
• Inhaler technique must be observed and checked
regularly
• Technique training a continuous process vs one-off
session at initiation of therapy
• Are patients on long-term inhaled therapy proficient
with their inhaler therapies?
Identify patients seen in pulmonary who had inhaler technique
education and documented.

PDE4 Inhibitors Roflumilast
• PDE4 inhibitors in patients with chronic bronchitis, severe to very severe COPD and a
history of exacerbations improves lung function and reduces moderate to severe
exacerbations (Level A)
• PDE4 inhibitors improve lung function and decrease exacerbations in patients on
LABA/ICS (Level B)
• Frequent Side effects:
– Nausea and Diarrhea
– Reduced appetite
– Weight loss (avoid in underweight patients)
– Sleep disturbance and headaches
• Use with caution in patients with depression

Other agents
• Long term Azithromycin (250mg/day or 500mg 3X week) or
erythromycin (500mg BID) reduce exacerbations in former smokers
(Level A)
– Associated with increase bacterial resistance and hearing test
impairment
• RELIANCE trial roflumilast vs Azithromycin
• Regular use of NAC and carbocysteine reduce the risk of
exacerbations in select populations (Level B)
• Simvastatin does not prevent exacerbations (Level A)
• Leukotriene modifiers have not been tested adequately in COPD
• Vasodilators worsen gas exchange with no improvement in health
status and should be used with caution in patients with pulmonary
HTN and COPD

Pulmonary Rehabilitation Programs
• Patients with high symptom burden and risk of
exacerbations
– Group B, C, D
– Participate in rehab program that considers the individual’s
characteristics and comorbidities
– Combination of constant load or interval training with strength
training provides better outcomes than either method alone
• Reduce readmissions and mortality in patients following
a recent exacerbation (less than 4 weeks prior
hospitalization)
• Tiotropium improves the effectiveness of pulmonary
rehab in increasing exercise performance (Level B)

Treatment of Hypoxemia
• In patients with severe resting hypoxemia long-term oxygen therapy
(>15 hours/day) is indicated as it has been shown to reduce
mortality (Evidence A)
– PaO2 ≤ 55mmHg or SaO2 ≤ 88% confirmed twice over a 3 week period
– PaO2 between 55mmHg and 60mmHg, or SaO2 88% if there is evidence of:
• Pulmonary hypertension
• Peripheral edema suggesting congestive heart failure
• Polycythemia (hematocrit >55)
• ? Moderate hypoxemia or desaturations with activity

Oxygen Therapy for COPD Ann Intern Med. 2017;166:JC17
• Randomized unblinded trial
• Long term oxygen was of no benefit:
– Moderate resting hypoxemia SpO2 89%-93%
– Moderate desaturation with activity (SpO2 decreased to 80% to 89% during 6
MWT)
• Outcomes measured
– Death
– First hospitalization
– COPD exacerbations
– Quality of life

Body mass index Obstruction Dyspnea Exercise Index
Best predictor of survival
0 1 2 3
BMI >21 <21
FEV1 >65 50-64 36-49 <35
MMRC
dyspnea
0-1 2 3 4
6MWT
(m)
>350 250-349 150-249 <149
Adapted from Celli B et al. NEJM
2004;350:1005-12.
4-year predicted
survival
0-2 80%
3-4 67%
5-6 57%
7-10 18%

Palliative Care in COPD
• Breathlessness
– Opiates
– Oxygen and fans blowing air onto the face
• Malnutrition
– Nutritional supplementation improves overall health status
• Fatigue
– Self-management education
– Pulmonary Rehab
– Nutrition
– Mind-body interventions



COPD Checklist for Every Clinic Visit
Smoking cessation
Depression
Spirometry needed?
Inhaler Technique
Vaccinations
Pulmonary rehabilitation
Oxygen needed?
PCP, ER, or Hospital for AECOPD in last
year
Co-morbidities (CAD, osteoporosis, lung
cancer)
Surgical Options needed?
Palliative Care needed?


Management of COPD exacerbations: ERS/ATS Guideline
Eur Respir J March 2017;49:1600791
Recommendation Strength
Quality
of
Evidence
1
For ambulatory patients with an exacerbation of COPD, we suggest a short
course (≤14 days) of oral corticosteroids
Conditional
Very low
2 For ambulatory patients with an exacerbation of COPD, we suggest the
administration of antibiotics Conditional Moderate
3
For patients who are hospitalized with a COPD exacerbation, we suggest the
administration of oral corticosteroids rather than intravenous corticosteroids if
GI access and function are intact
Conditional Low
4
For patients who are hospitalized with a COPD exacerbation associated with
acute or acute-on-chronic respiratory failure, we recommend the use of
noninvasive mechanical ventilation
Strong Low
5
For patients with a COPD exacerbation who present to the emergency
department or hospital, we suggest a home-based management program
(hospital-at-home)
Conditional Moderate
6 For patients who are hospitalized with a COPD exacerbation, we suggest the
initiation of pulmonary rehabilitation within 3 weeks after hospital discharge Conditional Very low
7 For patients who are hospitalized with a COPD exacerbation, we suggest not
initiating pulmonary rehabilitation during hospital stay Conditional Very low

NIMV for COPD
• Reduce WOB
• Improve gas exchange
• Reduce hospital morbidity
• Reduce ICU and Hospital LOS
• Improve Survival
• GOLD Recommends Acute Exacerbations with:
– Respiratory acidosis
– Severe Dyspnea with signs of respiratory failure
• Data for home chronic use inconclusive
• COPD and OSA patients CPAP improves survival and avoids hospitalization
Brochard et al NEJM 1995;333:817-22
Antonelli et al NEJM 1998;339:429-35
Kramer et al AJRCCM 1995;151:1799-1806
Confalonieri et al EurRJ 1996;9:422-30
Bott et al Lancet 1993;341:1555-57