-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
1/32
Global Initiative for ChronicObstructive
Lung
Disease
Global Initiative for Chronic
Obstructive
Lung
Disease
POCKET GUIDE TO
COPD DIAGNOSIS, MANAGEMENT,
AND PREVENTION
A Guide or Health Care ProessionalsUPDATED 2013
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
2/32
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
3/32
Global Initiative for ChronicObstructive
LungDisease
Pocket Guide to COPD Diagnosis, Management,
And Prevention, 2013GOLD Board o DirectorsMarc Decramer, MD,
Chair Jean Bourbeau, MD
Katholieke Universiteit Leuven McGill University Health
CentreLeuven, Belgium Montreal, Quebec, Canada
Jorgen Vestbo, MD, Vice Chair Bartolome R. Celli, MDOdense
University Hospital Brigham and Womens HospitalOdense C, Denmark
(and) Boston, Massachusetts USAUniversity o ManchesterManchester,
UK M.Victorina Lpez Varela, MD
Universidad de la RepblicDavid S.C. Hui, MD Montevideo,
UruguayThe Chinese University o Hong Kong
Hong Kong, ROC Roberto Rodriguez Roisin, MDHospital Clnic,
University o Barcelona
Masaharu Nishimura, MD Barcelona, SpainHokkaido University
School o MedicineSapporo, Japan Claus Vogelmeier, MD University o
Gieen and MarburgRobert A. Stockley Marburg, GermanyUniversity
Hospitals BirminghamBirmingham, UK
GOLD Science CommitteeJrgen Vestbo, MD, Denmark, UK, Chair
Fernando Martinez, MD, USAAlvar Agusti, MD, Spain Masaharu
Nishimura, MD,JapanAntonio Anzueto, MD, USA Nicolas Roche, MD,
FrancePeter J. Barnes, MD, UK Roberto Rodriguez Roisin, MD,
SpainMarc Decramer, MD, Belgium Donald Sin, MD, CanadaLeonardo M.
Fabbri, MD, Italy Robert A. Stockley, MD, UKPaul Jones, MD, UK
Claus Vogelmeier, MD, GermanyGOLD Science DirectorSuzanne Hurd,
PhD, USA
GOLD National LeadersRepresentatives rom many countries serve as
a network or the dissemination andimplementation o programs or
diagnosis, management, and prevention o COPD. TheGOLD Board o
Directors is grateul to the many GOLD National Leaders who
participated indiscussions o concepts that appear in GOLD
reports.
2013 Global Initiative or Chronic Obstructive Lung Disease,
Inc.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
4/32
TABLE OF CONTENTS
3 INTRODUCTION
4 KEY POINTS
5 WHAT IS CHRONIC OBSTRUCTIVEPULMONARY DISEASE (COPD)?
6 WHAT CAUSES COPD?
7 DIAGNOSIS OF COPD7 Table 1: Key Indicators or Considering
a
Diagnosis o COPD8 Table 2: COPD and its Dierential Diagnoses
9 ASSESSMENT OF COPD9 Table 3: Classication o Severity o
Airfow
Limitation in COPD
10 Table 4: Combined Assessment o COPD
11 THERAPEUTIC OPTIONS14 Table 5: Formulations and Typical Doses
o
COPD Medications
17 MANAGEMENT OF STABLE COPD17 Table 6: Non-Pharmacologic
Management o COPD19 Table 7: Pharmacologic Therapy or Stable
COPD
20 MANAGEMENT OF EXACERBATIONS21 Table 8: Indications or
Hospital Assessment
or Admission
22 COPD AND COMORBIDITIES
23 APPENDIX I: SPIROMETRY FOR DIAGNOSIS OF AIRLOW LIMITATION
IN COPD24 Figure 1A: Normal Spirogram24 Figure 1B: Spirogram
Typical o Patients with
Mild to Moderate COPD
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
5/32
3
INTRODUCTIONChronic Obstructive Pulmonary Disease (COPD) is a
major cause o morbidity
and mortality throughout the world. Much has been learned about
COPDsince the Global Initiative or Chronic Obstructive Lung Disease
issued its rstreport, Global Strategy or the Diagnosis, Management,
and Prevention oCOPD, in 2001. Treatment o COPD is now aimed at
immediately relievingand reducing the impact o symptoms, as well as
reducing the risk o utureadverse health events such as
exacerbations. These dual goals emphasizethe need or clinicians to
maintain a ocus on both the short-term and long-term impact o COPD
on their patients. A ramework or COPD managementthat matches
individualized assessment o the disease to these treatment
objectives will better meet each patients needs.
Several educational tools and publications oriented around this
approach toCOPD are available at http://www.goldcopd.org and can be
adapted tolocal health care systems and resources:
Global Strategy or the Diagnosis, Management, and Preventiono
COPD. Scientic inormation and recommendations or COPDprograms.
(Updated 2013)
Executive Summary, Global Strategy or the Diagnosis,
Management,and Prevention o COPD. American Journal o Respiratory
and CriticalCare Medicine(in press).
Pocket Guide to COPD Diagnosis, Management, and
Prevention.Summary o patient care inormation or primary health
careproessionals. (Updated 2013)
What You and Your Family Can Do About COPD. Inormation bookletor
patients and their amilies.
This Pocket Guide has been developed rom the Global Strategy or
theDiagnosis, Management, and Prevention o COPD(Updated 2013).
Technicaldiscussions o COPD and COPD management, evidence levels,
and speciccitations rom the scientic literature are included in
that source document.
Acknowledgements: Unconditional educational grants have been
providedby Almirall, AstraZeneca, Boehringer-Ingelheim, Chiesi,
Forest Laboratories,GlaxoSmithKline, Groupo Ferrer, Merck Sharp
& Dohme, Mylan, NoninMedical, Novartis, Pearl Therapeutics,
Pzer, Quintiles, and Takeda. The
participants o the GOLD committees, however, are solely
responsible or thestatements and conclusions in the
publications.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
6/32
4
KEY POINTS
Chronic Obstructive Pulmonary Disease (COPD), a common
preventableand treatable disease, is characterized by persistent
airfow limitationthat is usually progressive and associated with an
enhanced chronicinfammatory response in the airways and the lung to
noxious particlesor gases. Exacerbations and comorbidities
contribute to the overallseverity in individual patients.
Worldwide, the most commonly encountered risk actor or COPD
istobacco smoking. In many countries, outdoor, occupational, and
indoor
air pollution the latter resulting rom the burning o biomass
uels arealso major COPD risk actors.
A clinical diagnosis o COPD should be considered in any patient
whohas dyspnea, chronic cough or sputum production, and a history
oexposure to risk actors or the disease. Spirometry is required to
makethe diagnosis in this clinical context.
Assessment o COPD is based on the patients symptoms, risk
oexacerbations, the severity o the spirometric abnormality, and
theidentication o comorbidities.
Appropriate pharmacologic therapy can reduce COPD
symptoms,reduce the requency and severity o exacerbations, and
improve healthstatus and exercise tolerance.
All COPD patients with breathlessness when walking at their own
pace
on level ground appear to benet rom rehabilitation and
maintenanceophysical activity.
An exacerbation o COPD is an acute event characterized by
aworsening o the patients respiratory symptoms that is beyond
normalday-to-day variations and leads to a change in
medication.
COPD oten coexists with other diseases (comorbidities) that may
havea signicant impact on prognosis.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
7/32
5
WHAT IS CHRONIC
OBSTRUCTIVEPULMONARY DISEASE (COPD)?
Chronic Obstructive Pulmonary Disease (COPD), a common
preventable andtreatable disease, is characterized by persistent
airfow limitation that is usually
progressive and associated with an enhanced chronic infammatory
responsein the airways and the lung to noxious particles or gases.
Exacerbations andcomorbidities contribute to the overall severity
in individual patients.
This denition does not use the terms chronic bronchitis and
emphysema*and excludes asthma (reversible airfow limitation).
Symptoms o COPD include:
Dyspnea
Chronic cough
Chronic sputum production
Episodes o acute worsening o these symptoms (exacerbations) oten
occur.
Spirometry is required to make a clinical diagnosis o COPD; the
presence oa post-bronchodilator FEV1/FVC < 0.70 conrms the
presence o persistent
airfow limitation and thus o COPD.
*Chronic bronchitis, dened as the presence o cough and sputum
production or at least 3months in each o 2 consecutive years, is
not necessarily associated with airfow limitation.Emphysema, dened
as destruction o the alveoli, is a pathological term that is
sometimes(incorrectly) used clinically and describes only one o
several structural abnormalities presentin patients with COPD but
can also be ound in subjects with normal lung unction.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
8/32
6
WHAT CAUSES COPD?Worldwide, the most commonly encountered risk
actor or COPD istobacco smoking. Outdoor, occupational, and indoor
air pollution thelatter resulting rom the burning o biomass uels
are other major COPDrisk actors. Nonsmokers may also develop
COPD.
The genetic risk actor that is best documented is a severe
hereditarydeciency o alpha-1 antitrypsin. It provides a model or
how other geneticrisk actors are thought to contribute to COPD.
COPD risk is related to the total burden o inhaled particles a
personencounters over their lietime:
Tobacco smoke, including cigarette, pipe, cigar, and othertypes
o tobacco smoking popular in many countries, as well
asenvironmental tobacco smoke (ETS)
Indoor air pollution rom biomass uel used or cooking and
heating
in poorly vented dwellings, a risk actor that particularly
aectswomen in developing countries
Occupational dusts and chemicals (vapors, irritants, and
umes)when the exposures are suciently intense or prolonged
Outdoor air pollution also contributes to the lungs total burden
oinhaled particles, although it appears to have a relatively
smalleect in causing COPD
In addition, any actor that aects lung growth during gestation
andchildhood (low birth weight, respiratory inections, etc.) has
the potential toincrease an individuals risk o developing COPD.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
9/32
7
DIAGNOSIS OF COPDA clinical diagnosis o COPD should be
considered in any patient who hasdyspnea, chronic cough or sputum
production, and a history o exposure torisk actors or the disease
(Table 1).
Spirometry is required to make a clinical diagnosis o COPD; the
presence oa postbronchodilator FEV
1/FVC < 0.70 conrms the presence o persistent
airfow limitation and thus o COPD. All health care workers who
care orCOPD patients should have access to spirometry. Appendix I:
Spirometry
or Diagnosis o Airow Limitation in COPD summarizes the lung
unctionmeasurements that are key to making a spirometry diagnosis
and detailssome o the actors needed to achieve accurate test
results.
Table 1. Key Indicators or Considering a Diagnosis o COPD
Consider COPD, and perorm spirometry, i any o these indicators
arepresent in an individual over age 40. These indicators are not
diagnostic
themselves, but the presence o multiple key indicators increases
theprobability o a diagnosis o COPD. Spirometry is required to
establish adiagnosis o COPD.
Dyspnea that is: Progressive (worsens over
time).Characteristically worse with exercise.Persistent.
Chronic cough: May be intermittent and may be unproductive.
Chronic sputum production:
Any pattern o chronic sputum production mayindicate COPD.
History o exposure to risk actors:Tobacco smoke (including
popular local preparations).Smoke rom home cooking and heating
uels.Occupational dusts and chemicals.
Family history o COPD
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
10/32
8
Dierential Diagnosis: A major dierential diagnosis is asthma. In
somepatients with chronic asthma, a clear distinction rom COPD is
not possibleusing current imaging and physiological testing
techniques. In these patients,
current management is similar to that o asthma. Other potential
diagnosesare usually easier to distinguish rom COPD (Table 2).
Table 2. COPD and its Dierential Diagnoses
Diagnosis Suggestive Features
COPD Onset in mid-life.
Symptoms slowly progressive.History of tobacco smoking or
exposure to other types of smoke.
Asthma Onset early in life (often childhood).Symptoms vary
widely from day to day.Symptoms worse at night/early
morning.Allergy, rhinitis, and/or eczema also present.Family
history of asthma.
Congestive HeartFailure
Chest X-ray shows dilated heart, pulmonary edema.Pulmonary
function tests indicate volume restriction,
not airflow limitation.
Bronchiectasis Large volumes of purulent sputum.Commonly
associated with bacterial infection.Chest X-ray/CT shows bronchial
dilation, bronchial wall thickening.
Tuberculosis Onset all ages.Chest X-ray shows lung
infiltrate.Microbiological confirmation.High local prevalence of
tuberculosis.
Obliterative
Bronchiolitis
Onset at younger age, nonsmokers.May have history of rheumatoid
arthritis or acute fume exposure.Seen after lung or bone marrow
transplantation.CT on expiration shows hypodense areas.
Diuse Panbronchiolitis Predominantly seen in patients of Asian
descent.Most patients are male and nonsmokers.Almost all have
chronic sinusitis.Chest X-ray and HRCT show diffuse small
centrilobular nodular
opacities and hyperinflation.
These eatures tend to be characteristic o the respective
diseases, but are notmandatory. For example, a person who has never
smoked may develop COPD
(especially in the developing world where other risk actors may
be more importantthan cigarette smoking); asthma may develop in
adult and even in elderly patients.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
11/32
9
ASSESSMENT OF COPDThe goals o COPD assessment are to determine
the severity o the disease, itsimpact on patients health status,
and the risk o uture events (exacerbations,hospital admissions,
death) in order to guide therapy. Assess the ollowingaspects o the
disease separately:
Symptoms Degree o airfow limitation (using spirometry) Risk o
exacerbations Comorbidities
Assess Symptoms: Validated questionnaires such as the COPD
Assessment Test(CAT), the Modied British Medical Research Council
(mMRC) breathlessnessscale, or the Clinical COPD Questionnaire
(CCQ) should be used to assesssymptoms.
Assess Degree o Airow Limitation Using Spirometry: Table 3
provides theclassication o airfow limitation severity in COPD.
Assess Risk o Exacerbations: An exacerbation o COPD is dened as
an acuteevent characterized by a worsening o the patients
respiratory symptoms thatis beyond normal day-to-day variations and
leads to a change in medication.The best predictor o having requent
exacerbations (2 or more per year) is a
history o previous treated events; the risk o exacerbations also
increases asairfow limitation worsens.
Assess Comorbidities: Cardiovascular diseases, osteoporosis,
depression and
Table 3. Classifcation o Severity o Airow Limitation in
COPD(Based on Post-Bronchodilator FEV
1)
In patients with FEV1/FVC < 0.70:
GOLD 1: Mild FEV1
80% predicted
GOLD 2: Moderate 50% FEV1
< 80% predicted
GOLD 3: Severe 30% FEV1 < 50% predicted
GOLD 4: Very Severe FEV1
< 30% predicted
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
12/32
10
anxiety, skeletal muscle dysunction, metabolic syndrome, and
lung canceramong other diseases occur requently in COPD patients.
These comorbidconditions may infuence mortality and
hospitalizations, and should be looked
or routinely and treated appropriately.Combined Assessement o
COPD: Table 4 provides a rubric or combiningthese assessments to
improve management o COPD.
Symptoms:Less Symptoms (mMRC 0-1 or CAT < 10): patient is (A)
or (C)More Symptoms (mMRC 2 or CAT 10): patient is (B) or (D)
Airow Limitation:
Low Risk (GOLD 1 or 2): patient is (A) or (B)High Risk (GOLD 3
or 4): patient is (C) or (D)
Exacerbations:Low Risk ( 1 per year): patient is (A) or (B)High
Risk ( 2 per year): patient is (C) or (D)
Table 4. Combined Assessment o COPDWhen assessing risk, choose
thehighest riskaccording to GOLD grade or exacerbation history.
(One or more hospitalizations or COPD exacerbations should be
considered high risk.)
Patient CharacteristicSpirometric
ClassificationExacerbations per
yearmMRC CAT
ALow Risk
Less SymptomsGOLD 1-2 1 0-1 < 10
BLow Risk
More Symptoms
GOLD 1-2 1 2 10
CHigh Risk
Less SymptomsGOLD 3-4 2 0-1 < 10
DHigh Risk
More SymptomsGOLD 3-4 2 2 10
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
13/32
11
THERAPEUTIC OPTIONS
Smoking cessationhas the greatest capacity to infuence the
natural history oCOPD. Health care providers should encourage all
patients who smoke to quit.
Counseling delivered by physicians and other healthproessionals
signicantly increases quit rates over sel-initiatedstrategies. Even
a brie (3-minute) period o counseling tourge a smoker to quit
results in smoking quit rates o 5-10%.
Nicotine replacement therapy (nicotine gum, inhaler, nasal
spray, transdermal patch, sublingual tablet, or lozenge) aswell
as pharmacotherapy with varenicline, bupropion, ornortriptyline
reliably increases long-term smoking abstinencerates and these
treatments are signicantly more eectivethan placebo.
Smoking Prevention:Encourage comprehensive tobacco-control
policies and
programs with clear, consistent, and repeated nonsmoking
messages. Workwith government ocials to pass legislation to
establish smoke-ree schools,public acilities, and work environments
and encourage patients to keep smoke-ree homes.
Occupational Exposure:Emphasize primary prevention, which is
best achievedby elimination or reduction o exposures to various
substances in the workplace.Secondary prevention, achieved through
surveillance and early detection, isalso important.
Indoor and Outdoor Air Pollution: Implement measures to reduce
or avoidindoor air pollution rom burning biomass uel or cooking and
heating inpoorly ventilated dwellings. Advise patients to monitor
public announcementso air quality and, depending on the severity o
their disease, avoid vigorousexercise outdoors or stay indoors
during pollution episodes.
Physical Activity:All COPD patients benet rom regular physical
activity and
should repeatedly be encouraged to remain active.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
14/32
12
PHARMACOLOGIC THERAPIES FOR STABLE COPD
Pharmacologic therapy is used to reduce symptoms, reduce the
requency andseverity o exacerbations, and improve health status and
exercise tolerance.Each treatment regimen needs to be
patient-specic as the relationship betweenthe severity o symptoms
and the severity o airfow limitation is infuenced byother actors,
such as the requency and severity o exacerbations, the presenceo
respiratory ailure, comorbidities (cardiovascular disease,
osteoporosis,etc.), and general health status. The classes o
medications commonly used intreating COPD are shown in Table 5. The
choice within each class depends onthe availability o medication
and the patients response.
Bronchodilators:These medications are central to symptom
management inCOPD.
Inhaled therapy is preerred. The choice between beta
2-agonists, anticholinergics, theophylline,
or combination therapy depends on the availability o
medicationsand each patients individual response in terms o symptom
relie
and side eects. Bronchodilators are prescribed on an as-needed
or on a regular
basis to prevent or reduce symptoms. Long-acting inhaled
bronchodilators are convenient and more
eective at producing maintained symptom relie than
short-actingbronchodilators.
Long-acting inhaled bronchodilators reduce exacerbations
andrelated hospitalizations and improve symptoms and health
status,
and tiotropium improves the eectiveness o pulmonary
rehabilitation. Combining bronchodilators o dierent pharmacological
classes
may improve ecacy and decrease the risk o side eects comparedto
increasing the dose o a single bronchodilator.
Inhaled Corticosteroids:In COPD patients with FEV1
< 60% predicted, regulartreatment with inhaled
corticosteroids improves symptoms, lung unction, andquality o lie,
and reduces the requency o exacerbations. Inhaled
corticosteroid
therapy is associated with an increased risk o pneumonia.
Withdrawalrom treatment with inhaled corticosteroids may lead to
exacerbations insome patients. Long-term monotherapy with inhaled
corticosteroids is notrecommended.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
15/32
13
Combination Inhaled Corticosteroid/Bronchodilator Therapy: An
inhaledcorticosteroid combined with a long-acting beta
2-agonist is more eective
than either individual component in improving lung unction and
health statusand reducing exacerbations in patients with moderate
to very severe COPD.Combination therapy is associated with an
increased risk o pneumonia.Addition o a long-acting beta
2-agonist/inhaled glucocorticosteroid to tiotropium
appears to provide additional benets.
Oral Corticosteroids: Long-term treatment with oral
corticosteroids is notrecommended.
Phosphodiesterase-4 inhibitors:In GOLD 3 and GOLD 4 patients
with a historyo exacerbations and chronic bronchitis, the
phosphodiesterase-4 inhibitorrofumilast reduces exacerbations
treated with oral corticosteroids. These eectsare also seen when
rofumilast is added to long-acting bronchodilators; thereare no
comparison studies with inhaled corticosteroids.
Methylxanthines. Methylxanthines are less eective and less well
tolerated thaninhaled long-acting bronchodilators and are not
recommended i those drugs
are available and aordable. There is evidence or a modest
bronchodilatoreect and some symptomatic benet o these medications
compared withplacebo in stable COPD. Addition o theophylline to
salmeterol produces agreater increase in FEV
1and relie o breathlessness than salmeterol alone.
Low-dose theophylline reduces exacerbations but does not improve
post-bronchodilator lung unction.
Other Pharmacologic Treatments
Vaccines: Infuenza vaccines can reduce serious illness and death
in COPDpatients. Vaccines containing killed or live, inactivated
viruses are recommended,and should be given once each year.
Pneumococcal polysaccharide vaccine isrecommended or COPD patients
65 years and older, and has been shown toreduce community-acquired
pneumonia in those under age 65 with FEV
1
< 40% predicted.
Alpha-1 Antitrypsin Augmentation Therapy: Not recommended or
patientswith COPD that is unrelated to alpha-1 antitrypsin
deciency.
Antibiotics:Not recommended except or treatment o inectious
exacerbationsand other bacterial inections.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
16/32
14
Table 5. Formulations and Typical Doses o COPD Medications*
DrugInhaler
(mcg)
Solution forNebulizer(mg/ml)
OralVials forInjection
(mg)
Durationof Action(hours)
Beta2-agonists
Short-actingFenoterol 100-200 (MDI) 1 0.05% (Syrup)
4-6Levalbuterol 45-90 (MDI) 0.21, 0.42 6-8
Salbutamol (albuterol) 100, 200(MDI & DPI)
5 5 mg (Pill),0.024%(Syrup)
0.1, 0.5 4-6
Terbutaline 400, 500 (DPI) 2.5, 5 mg (Pill) 4-6
Long-actingFormoterol 4.5-12 (MDI & DPI) 0.01 12
Arformoterol 0.0075 12Indacaterol 75-300 (DPI) 24Salmeterol
25-50 (MDI & DPI) 12Tulobuterol 2 mg (transdermal) 24
AnticholinergicsShort-acting
Ipratropium bromide 20, 40 (MDI) 0.25-0.5 6-8Oxitropium bromide
100 (MDI) 1.5 7-9 Long-actingAclidinium bromide 322 (DPI) 12
Glycopyrronium bromide 44 (DPI) 24Tiotropium 18 (DPI), 5 (SMI)
24Combination short-acting beta
2-agonists plus anticholinergic in one inhaler
Fenoterol/Ipratropium 200/80 (MDI) 1.25/0.5
6-8Salbutamol/Ipratropium 75/15 (MDI) 0.75/0.5 12
6-8Methylxanthines
Aminophylline 200-600 mg (Pill) 240Variable,up to 24
Theophylline (SR) 100-600 mg (Pill) Variable,up to 24Inhaled
corticosteroids
Beclomethasone 50-400 (MDI & DPI) 0.2-0.4Budesonide 100,
200, 400 (DPI) 0.20. 0.25, 0.5Fluticasone 50-500 (MDI &
DPI)Combination long-acting beta
2-agonists plus corticosteroids in one inhaler
Formoterol/Budesonide 4.5/160 (MDI)9/320
(DPI)Formoterol/mometasone 10/200, 10/400 (MDI)
Salmeterol/Fluticasone 50/100, 250, 500 (DPI)25/50, 125, 250
(MDI)Systemic corticosteroidsPrednisone 5-60 mg
(Pill)Methyl-prednisolone 4, 8, 16 mg (Pill)Phosphodiesterase-4
inhibitorsRoflumilast 500 mcg (Pill) 24
MDI=metered dose inhaler; DPI=dry powder inhaler; SMI=sot mist
inhaler*Not all ormulations are available in all countries; in some
countries, other ormulations may be available.Formoterol nebulized
solution is based on the unit dose vial containing 20 mcg in a
volume o 2.0 ml
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
17/32
15
Mucolytic Agents: Patients with viscous sputum may benet rom
mucolytics(e.g. carbocysteine), but overall benets are very
small.
Antitussives:Use is not recommended.
Vasodilators: Nitric oxide is contraindicated in stable COPD.
The use oendothelium-modulating agents or the treatment o pulmonary
hypertensionassociated with COPD is not recommended.
OTHER TREATMENTS
Rehabilitation:Patients at all stages o disease benet rom
exercise trainingprograms with improvements in exercise tolerance
and symptoms o dyspneaand atigue. Benets can be sustained even ater
a single pulmonaryrehabilitation program. The minimum length o an
eective rehabilitationprogram is 6 weeks; the longer the program
continues, the more eective theresults. Benet does wane ater a
rehabilitation program ends, but i exercisetraining is maintained
at home the patients health status remains above pre-rehabilitation
levels.
Oxygen Therapy: The long-term administration o oxygen (> 15
hours perday) to patients with chronic respiratory ailure has been
shown to increasesurvival in patients with severe, resting
hypoxemia. Long-term oxygen therapyis indicated or patients who
have:
PaO2at or below 7.3 kPa (55 mmHg) or SaO
2at or below 88%, with
or without hypercapnia conrmed twice over a three-week period;
or
PaO2between 7.3 kPa (55 mmHg) and 8.0 kPa (60 mmHg), or SaO
2
o 88%, i there is evidence o pulmonary hypertension,
peripheraledema suggesting congestive cardiac ailure, or
polycythemia(hematocrit > 55%).
Ventilatory Support: The combination o non-invasive ventilation
with long-termoxygen therapy may be o some use in a selected subset
o patients, particularlyin those with pronounced daytime
hypercapnia. It may improve survival butdoes not improve quality o
lie. There are clear benets o continuous positiveairway pressure
(CPAP) on both survival and risk o hospital admission.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
18/32
16
Surgical Treatments:The advantage o lung volume reduction
surgery (LVRS)over medical therapy is more signicant among patients
with upper-lobepredominant emphysema and low exercise capacity
prior to treatment,
although LVRS is costly relative to health-care programs not
including surgery.In appropriately selected patients with very
severe COPD, lung transplantationhas been shown to improve quality
o lie and unctional capacity.
Palliative Care, End-o-lie Care, and Hospice Care: The disease
trajectory inCOPD is usually marked by a gradual decline in health
status and increasingsymptoms, punctuated by acute exacerbations
that are associated with anincreased risk o dying. Progressive
respiratory ailure, cardiovascular diseases,malignancies and other
diseases are the primary cause o death in patients withCOPD
hospitalized or an exacerbation. Thus palliative care, end-o-lie
care,and hospice care are important components o the management o
patientswith advanced COPD.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
19/32
17
MANAGEMENT OF STABLE COPDOnce COPD has been diagnosed, eective
management should be basedon an individualized assessment o current
symptoms and uture risks:
Relieve symptoms Improve exercise tolerance Improve health
status
and Prevent disease progression Prevent and treat exacerbations
Reduce mortality
These goals should be reached with minimal side eects rom
treatment,a particular challenge in COPD patients because they
commonly havecomorbidities that also need to be careully identied
and treated.
NON-PHARMACOLOGIC TREATMENT
Non-pharmacologic management o COPD according to the
individualizedassessment o symptoms and exacerbation risk is shown
in Table 6.
REDUCE SYMPTOMS
REDUCE RISK
Table 6. Non-Pharmacologic Management o COPD
Patient Group Essential RecommendedDepending on
Local Guidelines
A
Smokingcessation
(can includepharmacologic
treatment)
Physical activityFlu vaccinationPneumococcalvaccination
B, C, D
Smokingcessation
(can includepharmacologic
treatment)Pulmonary
rehabilitation
Physical activityFlu vaccinationPneumococcalvaccination
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
20/32
18
PHARMACOLOGIC TREATMENT
A proposed model or initial pharmacological management o
COPD
according to the assessment o symptoms and risk (Table 3) is
shown inTable 7.
Bronchodilators Recommendations:
For both beta2-agonists and anticholinergics, long-acting
ormulations are preerred over short-acting ormulations. The
combined use o short- or long-acting beta
2-agonists and
anticholinergics may be considered i symptoms are not
improvedwith single agents.
Based on ecacy and side eects, inhaled bronchodilators
arepreerred over oral bronchodilators.
Based on evidence o relatively low ecacy and greater sideeects,
treatment with theophylline is not recommended unlessother
bronchodilators are not available or unaordable or long-term
treatment.
Corticosteroids and Phosphodiesterase-4 Inhibitors
Recommendations
There is no evidence to recommend a short-term therapeutic
trialwith oral corticosteroids in patients with COPD to identiy
thosewho will respond to inhaled corticosteroids or other
medications.
Long-term treatment with inhaled corticosteroids is
recommendedor patients with severe and very severe airfow
limitation andor patients with requent exacerbations that are not
adequately
controlled by long-acting bronchodilators. Long-term monotherapy
with oral corticosteroids is not recommendedin COPD.
Long-term monotherapy with inhaled corticosteroids is not
recommendedin COPD because it is less eective than the combination
o inhaledcorticosteroids with long-acting beta
2-agonists.
Long-term treatment containing inhaled corticosteroids should
notbe prescribed outside their indications, due to the risk o
pneumoniaand the possibility o a slightly increased risk o ractures
ollowinglong-term exposure.
The phosphodiesterase-4 inhibitor rofumilast may also be used
toreduce exacerbations or patients with chronic bronchitis,
severeand very severe airfow limitation, and requent exacerbations
thatare not adequately controlled by long-acting
bronchodilators.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
21/32
19
*Medicationsineach
boxarementione
din
alphabeticalorderand
thereforenotnecessarilyin
orderofpreferen
ce.
**Medicationsin
this
columncanbeusedalone
orincombination
with
otheroptionsintheFirst
andAlternativeC
hoice
columns
Glossary:
SA:short-acting
LA:long-acting
ICS:inhaledcorticosteroid
PDE-4:phosphodiesterase-4
prn:whennecess
ary
Table7:PharmacologicTherapyforStableCOPD*
Patient
Group
RECOMMENDED
FIRSTCHOICE
ALTERNATIVECHOICE
OTHERPOSSIBLE
TREATMENTS**
A
SAanticholinergicprn
or
SAbeta2-agonistprn
LAanticholinergic
or
LAbeta2-agonist
or
SAbeta2-agonistand
SAanticholinergic
Theophylline
B
LAanticholinergic
or
LAbeta2-agonist
LAanticholinergicand
LAbeta2-agonist
SAbeta2-agonistand/
or
SAanticholinergic
Theophylline
C
ICS+
LAbeta2-agonist
or
LAanticholinergic
LAanticholinergicand
LAbeta2-agonist
or
LAanticholinergicand
PDE-4
Inhibitor
or
LAbeta2-agonistand
PDE-4
Inhibitor
SAbeta2-agonistand/
or
SAanticholinergic
Theophylline
D
ICS+
LAbeta2-agonist
and/or
LAanticholinergic
ICS+LA
beta2-agonistand
LA
anticholinergic
or
ICS+LA
beta2-agonistand
PDE-4inhibitor
or
LA
anticholinergicand
LA
beta2-agonist
or
LA
anticholinergicand
PDE-4inhibitor
Carbocysteine
SAbeta2-agonistand/
or
SAanticholinergic
Theophylline
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
22/32
20
MANAGEMENT OF
EXACERBATIONSAn exacerbation o COPD is dened as an acute event
characterized by aworsening o the patients respiratory symptoms
that is beyond normal day-to-day variations and leads to a change
in medication.
The most common causes appear to be respiratory tract inections
(viral orbacterial).
How to Assess the Severity o an Exacerbation
Arterial blood gas measurements (in hospital): PaO2
< 8.0 kPa(60 mmHg) with or without PaCO
2> 6.7 kPa, (50 mmHg) when
breathing room air indicates respiratory ailure. Chest
radiographs are useul in excluding alternative diagnoses. An ECG
may aid in the diagnosis o coexisting cardiac problems.
Other laboratory tests:
Whole blood countcan identiy polycythemia or bleeding. The
presence opurulent sputum during an exacerbation can be
sucient indication or starting empirical antibiotic treatment.
Biochemical tests can help detect electrolyte disturbances,
diabetes,
and poor nutrition.
Spirometric tests are not recommended during an exacerbation
because theycan be dicult to perorm and measurements are not
accurate enough.
Treatment Options
Oxygen:Supplemental oxygen should be titrated to improve the
patientshypoxemia with a target saturation o 88-92%.
Bronchodilators:Short-acting inhaled beta2-agonists with or
without short-acting anticholinergics are the preerred
bronchodilators or treatment o anexacerbation.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
23/32
21
Systemic Corticosteroids: Systemic corticosteroids shorten
recovery time,improve lung unction (FEV
1) and arterial hypoxemia (PaO
2), and reduce
the risks o early relapse, treatment ailure, and length o
hospital stay. A
dose o 30-40 mg prednisolone per day or 10-14 days is
recommended.
Antibiotics:Antibiotics should be given to patients:
With the ollowing three cardinal symptoms: increased
dyspnea,increased sputum volume, increased sputum purulence;
With increased sputum purulence and one other cardinal symptom;
Who require mechanical ventilation
Adjunct Therapies: Depending on the clinical condition o the
patient, anappropriate fuid balance with special attention to the
administration odiuretics, anticoagulants, treatment o
comorbidities, and nutritional aspectsshould be considered. At any
time, health care providers should stronglyenorce stringent
measures against active cigarette smoking.
Patients with characteristics o a severe exacerbation should be
hospitalized(Table 8). Indications or reerral and the management o
exacerbations o
COPD in the hospital depend on local resources and the acilities
o thelocal hospital.
Table 8. Indications or Hospital Assessment or Admission
Marked increase in intensity o symptoms
Severe underlying COPD Onset o new physical signs
Failure o an exacerbation to respond to initial medical
management
Presence o serious comorbidities
Frequent exacerbations
Older age
Insucient home support
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
24/32
22
COPD AND COMORBIDITIESCOPD oten coexists with other diseases
(comorbidities) that may have asignicant impact on prognosis. In
general, the presence o comorbiditiesshould not alter COPD
treatment and comorbidities should be treated as ithe patient did
not have COPD.
Cardiovascular disease (including ischemic heart disease, heart
ailure,atrial brillation, and hypertension) is a major comorbidity
in COPD andprobably both the most requent and most important
disease coexisting withCOPD. Cardioselective beta-blockers are not
contraindicated in COPD.
Osteoporosisand anxiety/depression, major comorbidities in COPD,
areoten under-diagnosed and are associated with poor health status
andprognosis.
Lung canceris requently seen in patients with COPD and has been
ound tobe the most requent cause o death in patients with mild
COPD.
Serious inections, especially respiratory inections, are
requently seen inpatients with COPD.
The presence o metabolic syndrome and maniest diabetes are
morerequent in COPD and the latter is likely to impact on
prognosis.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
25/32
23
APPENDIX I: SPIROMETRY
FOR DIAGNOSIS OF AIRFLOWLIMITATION IN COPDSpirometry is required
to make a clinical diagnosis o COPD and shouldbe available to all
health care proessionals who work with COPD patients.
What is Spirometry?
Spirometryis a simple test to measure the amount o air aperson
can breathe out, and the amount o time taken to do so.
A spirometer is a device used to measure how eectively, andhow
quickly, the lungs can be emptied.
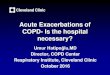
A spirogram is a volume-time curve.
Spirometry measurements used or diagnosis o COPD include(see
Figures 1A and 1B):
FVC (Forced Vital Capacity): maximum volume o air that can
beexhaled during a orced maneuver.
FEV1
(Forced Expired Volume in one second): volume expired in therst
second o maximal expiration ater a maximal inspiration. This
is a measure o how quickly the lungs can be emptied.
FEV1/FVC: FEV
1expressed as a proportion o the FVC, gives a
clinically useul index o airfow limitation.
The ratio FEV1/FVC is between 0.70 and 0.80 in normal adults;
a
value less than 0.70 indicates airfow limitation and thus o
COPD.
FEV1
is infuenced by the age, sex, height, and ethnicity, and is
best considered as a percentage o the predicted normal
value.There is a vast literature on normal values; those
appropriate orlocal populations should be used1,2,3,4.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
26/32
24
Why do Spirometry or COPD?
Spirometry is needed to make a clinical diagnosis o COPD.
Together with the presence o symptoms, spirometry helps
gaugeCOPD severity and can be a guide to specic treatment
steps.
A normal value or spirometry eectively excludes the diagnosis
oclinically relevant COPD.
The lower the percentage predicted FEV1, the worse the
subsequent
prognosis.
Figure 1A: Normal Spirogram
1 2 3 4 5 6
1
2
3
4
Volume,
liters
Time, seconds
5
1
FEV1 = 4L
FVC = 5L
FEV1/FVC = 0.8
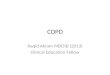
Figure 1B: Spirogram Typical o Patients with Mild to Moderate
COPD*
Vo
lume,
liter
s
Time, seconds
5
4
3
2
1
1 2 3 4 5 6
FEV1 = 1.8L
FVC = 3.2L
FEV1/FVC = 0.56
Obstructive
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
27/32
25
FEV1
declines over time and usually aster in COPD than in
healthysubjects. Spirometry can be used to monitor disease
progression,but to be reliable the intervals between measurements
must be at
least 12 months.
What You Need to Perorm Spirometry
Several types o spirometers are available. Relatively large
bellows orrolling-seal spirometers are usually only available in
pulmonary unctionlaboratories. Calibration should be checked
against a known volume (e.g.,rom a 3-litre syringe) on a regular
basis. There are several smaller hand-held devices, oten with
electronic calibration systems.
A hard copy o the volume-time plot is very useul to
checkoptimalperormance and interpretation, and to exclude
errors.
Most spirometers require electrical power to permit operation o
the motorand/or sensors. Some battery-operated versions are
available that candock with a computer to provide hard copy.
It is essential to learn how your machine is calibrated and when
and howto clean it.
How to Perorm Spirometry
Spirometry is best perormed with the patient seated. Patients
may beanxious about perorming the tests properly, and should be
reassured.Careul explanation o the test, accompanied by a
demonstration, is very
useul. The patient should:
Breathe in ully.
Seal their lips around the mouthpiece.
Force the air out o the chest as hard and ast as they can until
theirlungs are completely empty.
Breathe in again and relax.
Exhalation must continue until no more air can be exhaled, must
be at least6 seconds, and can take up to 15 seconds or more.
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
28/32
26
Like any test, spirometry results will only be o value i the
expirations areperormed satisactorily and consistently. Both FVC
and FEV
1should be the
largest value obtained rom any o 3 technically satisactory
curves and the
FVC and FEV1 values in these three curves should vary by no more
than5% or 150 ml, whichever is greater. The FEV1/FVC is calculated
using the
maximum FEV1
and FVC rom technically acceptable (not necessarily thesame)
curves.
Those with chest pain or requent cough may be unable to perorm
asatisactory test and this should be noted.
Where to nd more detailed inormation on spirometry:
1. GOLD: A spirometry guide or general practitioners and a
teachingslide set is available: http://www.goldcopd.org
2. American Thoracic
Societyhttp://www.thoracic.org/adobe/statements/spirometry1-30.pd
3. Australian/New Zealand Thoracic Society
http://www.nationalasthma.org.au/publications/spiro/index.htm
4. British Thoracic
Societyhttp://www.brit-thoracic.org.uk/copd/consortium.html
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
29/32
27
NOTES
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
30/32
28
NOTES
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
31/32
-
7/29/2019 COPD GOLD_pocket Guide 2013(1)
32/32
The Global Initiative or Chronic Obstructive Lung Diseaseis
supported by unrestricted educational grants rom:
2013 Global Initiative or Chronic Obstructive Lung Disease
Inc
Almirall
AstraZeneca
Boehringer Ingelheim
ChiesiForest Laboratories
GlaxoSmithKline
Grupo Ferrer
Merck Sharp and DohmeMylan
Nonin Medical
Novartis
Pearl Therapeutics
Pzer
Quintiles
Takeda