Embed Size (px)
Citation preview

The University of Sydney Page 1
Convert Data Cemeteries into Sources of Knowledge
Presented byProfessor Heiko SpallekFaculty of Medicine and Health
Slideshttp://bit.ly/Spallek-HISA-2019

The University of Sydney Page 2The University of Sydney
My journey
Berlin1993: DMD, PhD
Philadelphia1996: Dental Informatics2000: MBA (Computer
Information Science)
Pittsburgh2000: NIH-funded research2010: Associate Dean
Sydney2016: Deputy Dean2018: Head of School and Dean

The University of Sydney Page 3
Agenda
– The “blue-sky” BIG Picture– Data as an Asset– Data Science for Oral Health– Barriers– Learning Health System– The University of Sydney
– Faculty of Medicine and Health’s Response

The University of Sydney
The Big Picture

The University of Sydney Page 5
"convergence of genomics, biosensors, the electronic patient record and smartphone apps,
all superimposed on a digital infrastructure, with artificial intelligence to make sense of the overwhelming amount of data created”
A unique juncture: Preparing the healthcare workforce
E. J. Topol, ‘High-performance medicine: the convergence of human and artificial intelligence’, Nature Medicine, 2019, doi.org/10.1038/s41591-018-0300-7

The University of Sydney Page 6
Decision Making: Human vs AI
Adapted from: Beam AL, Kohane IS: Big Data and Machine Learning in Health Care. JAMA. 2018 Apr 3;319(13):1317-1318.

The University of Sydney Page 7
Algorithms will transform the thinking underlying medicine!
Source: Obermeyer, Z., & Lee, T. H. (2017). Lost in Thought — The Limits of the Human Mind and the Future of Medicine. New England Journal of Medicine, 377(13), 1209–1211. http://doi.org/10.1056/NEJMp1705348
§ Mismatch between the human mind’s abilities and medicine’s complexity
§ Machine learning in medicine will be a team sport, like medicine itself
§ Education: § train doctors in the data science,
statistics, behavioral science to develop, evaluate, apply algorithms in clinical practice
§ premedical requirements are outdated
The University of Sydney
Data as an Asset
The University of Sydney Page 9
Data = Asset
- upward trend in data generation- < 5% of useful data is analyzed to generate information & derive
knowledge
“Data is a strategic asset with great potential and should be treated and managed as such.”
Data Availability and Use: Productivity Commission Inquiry Report, No. 82, 31 March 2017, http://www.pc.gov.au/inquiries/completed/data-access/report/data-access.pdf

The University of Sydney Page 10
What can we discover from data?
1854: “Broad Street Cholera Outbreak”
JON SNOW

The University of Sydney Page 11
Unmet information– timely access to information on various subjects– better visual representations of dental problems– access to patient-specific evidence-based information– accurate, complete and consistent documentation of patient
records

The University of Sydney
Information about the state of:
§ internal systems, e.g. imaging, lab-test results§ living conditions, e.g. housing, environment§ care received, e.g. medications, treatments§ behaviors, e.g. sleep, exercise
“The potential of this information is so enormous it is almost scary.”
Atul Gawande: The Heroism of Incremental Care, The New Yorker, 2017, http://www.newyorker.com/magazine/2017/01/23/the-heroism-of-incremental-care
Information that matter to health and well-being

The University of Sydney
Data availabilityFAIR: Findability, Accessibility, Interoperability, ReusabilitySource: Wilkinson, M. D. et al. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 3:160018 doi: 10.1038/sdata.2016.18 (2016)
• Electronic Health Records, including electronic medical and dental records, genetic data, proteomics data, microbiome data, bio-specimen data, etc.
• Registry data across multiple disciplines
• Patient-generated heath data (PGHD), e.g. home monitoring, seamless integration of PGHD into EHR
• Precision medicine • Diagnostics
Potential data sources for HIT ecosystem• Socio-economic data (e.g. Census) • Urban planning data • Traffic data • Sensor data • Health Insurances (claims) • Public Health data (surveys) • Environmental data (workplace, bio
surveillance, air quality data, UV radiation, Radon, water fluoridation)
• Education data, including health behaviour interventions in schools and communities
• Dietary data, food consumption, supplements
The University of Sydney Page 14
No Interoperable HIT Ecosystem
A smartphone can MANY things.
EHR can FEW things (= mostly a billing diary)- Lack of interoperable systems- Lack of flexibility, e.g. mobile access in disaster situation.- Tapping on a plastic-covered keyboard with gloved hands
“Building a value-enabling Health IT ecosystem—largely not knowledge barriers, but execution barriers”
Adler-Milstein et al: Crossing the health IT chasm: considerations and policy recommendations to overcome current challenges and enable value-based care, JAMIA doi: 10.1093/jamia/ocx017
"ensuring that electronic repositories become valuable resources rather than expensive investments that are quickly ignored”
Van Knippenberg, D et al: Information, Attention, & Decision Making. Academy of Management Journal, (2015) 58(3), 649–657

The University of Sydney Page 15
There is a human attached to every tooth
Link dental data to general health data!

The University of Sydney Page 16
Electronic Medical Record (EMR) Electronic Dental Record (EDR)
Integration for • safe and efficient patient care, e.g. allergies, medication• health profession education based on interprofessional education
principles• biomedical research that acknowledges that the mouth is part of the
body
If you want to bring healthy lives and healthy mouths together, you also need to bring EMRs and EDRs together!
Sample research questions:- Is maintaining a full dentition important for older patient?- Does pre-chemo dental therapy help? - What role does the dentition play in dialysis outcomes? - Does a healthy dentition improve overall health?

The University of Sydney Page 17
What EHRs Do Wrong
§ Alerts and reminders (alert fatigue)§ Data entry (tedious, redundant)§ Incompleteness§ Data overload (note bloat)§ Poor navigability
Electronic Health Records (EHR)
What EHRs Do Right
§ Billing§ Legibility§ Availability§ Result reporting§ Order entry§ Alerts and reminders
Dental Records:WORN—write once read never

The University of Sydney Page 18
100 DMD + 30 DH students; 100,000 patient visits/a dental school– Initial acquisition:
– between US$ 524,523 and US$ 2,503,971
– Ongoing operations/a:– between US$ 631,816 and US$ 848,105
Watch video: https://vimeo.com/fdim/spallek-cost-of-health-it

The University of Sydney Page 19

The University of Sydney Page 20
Challenges of Using EHR Data for Research
– Clinical notes (free text) are not readily queryable1
– Data quality issues1
o Incomplete, missing (e.g. ethnicity)o Inaccurate (e.g. self reported data)o Inconsistent (coding issues)
– Ethical issues (e.g. patient privacy)
– Data may be idiosyncratic and may not be generalizable1
1) Mei Song, Kaihong Liu, Rebecca Abromitis, Titus L. Schleyer, Reusing electronic patient data for dental clinical research: A review of current status. 2) J Dent. 2013 Dec; 41(12): 1148–1163.

The University of Sydney Page 21
Zozus MN, Hammond EH, Green BB, Kahn MG, Richesson R, Rusincovitch SA, Simon GE, Smerek MM. Assessing Data Quality for Healthcare Systems Data Used in Clinical Research (Version 1.0). NIH Health Care Systems Research
Collaboratory. 07/28/2014. https://sites.duke.edu/rethinkingclinicaltrials/assessing-data-quality/
What is Data Quality?
“Fitness for use”

The University of Sydney Page 22
4 Levels of the Power of Data
Four perspectives
• Patient: Provision of tools/ data to engage patients and make them part of the decision making process about their care
• Clinicians: Provision of all relevant data to allow clinicians to make the right decisions about patient care and reflect on their practice
• Services: to use data to support system efficiency and resource allocation as well as improve safety and quality
• Policy Makers: Access to data to make decisions regarding value of care and safety and quality, e.g. “oversight” of data such as trends that emerge when connecting various data sources

The University of Sydney
Data Science for Oral Health
The University of Sydney Page 24
Internet of Dental Things (IoDT)
Kolibree: http://www.kolibree.com/en/
Screen Shot 2015-02-21 at 6.47.53 PM

The University of Sydney Page 25Kolibree: http://www.kolibree.com/en/
Onvi: first smart video toothbrush
http://www.bizjournals.com/chicago/news/2016/12/06/chicago-startup-onvi-smart-video-toothbrush.html#i1
Internet of Dental Things (IoDT)
The University of Sydney Page 26
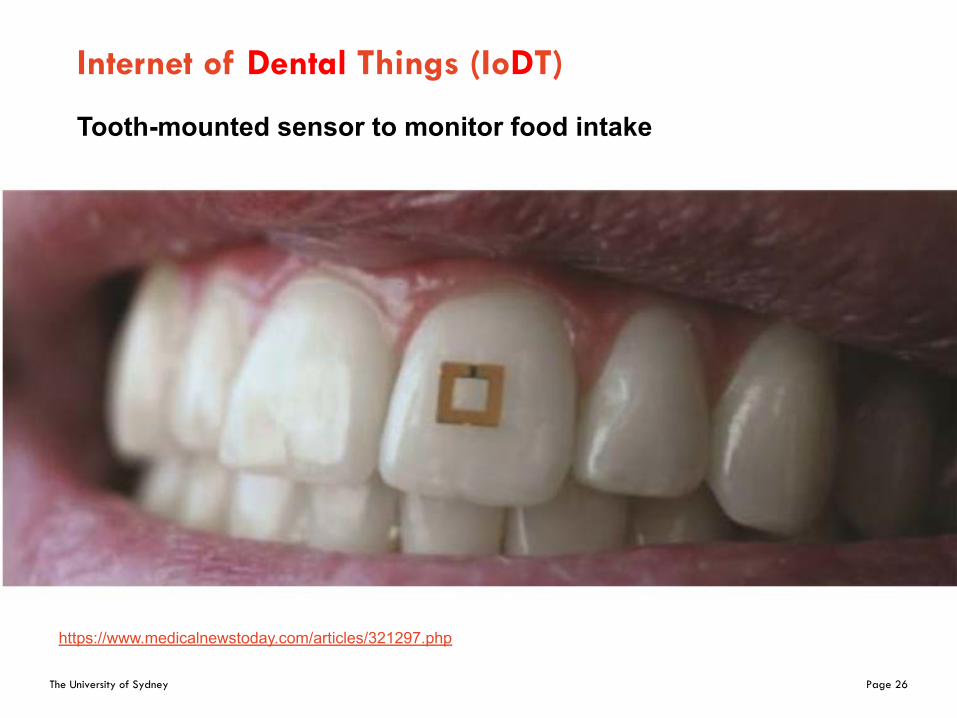
Internet of Dental Things (IoDT)
Kolibree: http://www.kolibree.com/en/
Tooth-mounted sensor to monitor food intake
https://www.medicalnewstoday.com/articles/321297.php

The University of Sydney Page 27Kolibree: http://www.kolibree.com/en/
Graphene-based wireless bacteria detection on tooth enamel
https://www.nature.com/articles/ncomms1767
Internet of Dental Things (IoDT)

The University of Sydney Page 28
Analyzing qualitative data
– Qualitative data = hows & whys
– Transform qualitative quantitative: shallow shadow of original form, e.g., toothache
– Humans explain context when communicating
– Computers get context during design from engineers
The University of Sydney Page 29
Big Mouth Data Repository

The University of Sydney Page 30
A Multi-Institutional Dental Data Repository

The University of Sydney Page 31
2012 2013 2014 2015 2016 2017 2018 20191.1 M
31

The University of Sydney Page 32
2012 2013 2014 2015 2016 2017 2018 20191.1 M 1.59 M
32

The University of Sydney Page 33
2012 2013 2014 2015 2016 2017 2018 20191.1M 1.59M 2.02M
33

The University of Sydney Page 34
2012 2013 2014 2015 2016 2017 2018 20191.1M 1.59M 2.02M 2.4M
34

The University of Sydney Page 35
2012 2013 2014 2015 2016 2017 2018 2019
8 sites ~ 3 Million patients
1.1M 1.59M 2.02M 2.4M 3M
35

The University of Sydney Page 37

The University of Sydney Page 38

The University of Sydney Page 39

The University of Sydney Page 40
Clinical Decision Support forSmoking Cessation Intervention

The University of Sydney Page 41
A Clinic-Randomized Trial of a Clinical Decision Support System to Improve Dental Provider Delivery of Brief Tobacco Interventions and Quitline Referrals
– Principal Investigator: – Brad Rindal, DDS– Heiko Spallek, DMD, PhD, MSBA
– Funding Source: National Institute of Dental and Craniofacial Research (NIDCR) - U01DE026135
– Award Period: 8/2/2016 – 7/31/2020
– Requested Award Amount: $2,488,348 (DC)– https://projectreporter.nih.gov/project_info_description.cfm?aid=915
6468

The University of Sydney Page 42
The Problem
– Tobacco use: a significant ongoing public health problem
– Dental care settings: underused for cessation assistance
– Providers ask about tobacco use but don’t assist the patient in tobacco cessation
– Evidence that Screening for drug useBrief Intervention, and Referral to Treatment (SBIRT)
provide a promising, practical solution

The University of Sydney Page 43
Methods
Illustration by Heiko Spallek

The University of Sydney Page 44
Results
Patient response to question, “At your most recent visit, did your dentist or hygienist . . .”
Smokers seen in usual care
clinics (8)(n=285)
Smokers seen in intervention
clinics (7)(n=263)
P-value
. . . ask about your interest in quittingsmoking?
. . . talk about specific strategies forquitting smoking
. . refer you to a tobacco quit line
70.9 % (200/282)
25.5 % (72/282)
17.4 % (49/282)
89.1% (228/256)
48.4 %(124/256)
38.9 %(100/257)
.0001
.003
.007
Am J Prev Med 2013;44(3):260 –264

The University of Sydney Page 45
Conclusions
– A computer-assisted tool is effective at increasing the frequency of tobacco cessation treatment based on the SBIRT in a dental setting
– This results are consistent with results of studies in medical settings
– This study focused on provider behavior, not quit rates.
Limitations

The University of Sydney
mHealth for Optimizing Acute Post-Operative Dental Pain Management

The University of Sydney
Using new health information technology
Grant title:Optimizing Acute Post-Operative Dental Pain Management
Principal Investigator: Elsbeth Kalenderian, DDS, PhD
Funding Source: Agency for Healthcare Research and Quality (AHRQ), 1U18HS026135-01
Award Period: 08/01/2018 – 06/30/2021
Requested Award Amount: $ 1,186,383 (DC)
https://projectreporter.nih.gov/project_info_description.cfm?aid=9568143

The University of Sydney
The problem: “Pain as the fifth vital sign”Dentists § responsible for 12% of all immediate-release opioid Rxs (1.2 billion
pills) in the US§ 85% to 99% of oral surgeons prescribe opioids following third-molar
extractions§ more than 60% of adolescent dental patients fill new opioid Rxs
within 7 days of tooth extractions
Insufficient pain assessment: primary reasons for under-treatment
Managing acute post-operative pain remains sub-optimal for most US adults undergoing outpatient surgery
Patient-reported outcomes (PROs) allow clinicians to directly assess patient’s symptoms, symptom burden, functional status, health behaviors, health-related quality of life, and care experiences

The University of Sydney
Expanding the role of health IT in dentistry

The University of Sydney Page 50
De-Implementing Opioid Use and Implementing Optimal Pain Management Following Dental Extractions
– Principal Investigator: – Brad Rindal, DDS
– Heiko Spallek (consultant)
– Funding Source: National Institute of Dental and Craniofacial Research (NIDCR) - U01DE027441
– Award Period: 09/01/2017 – 08/31/2021
– Requested Award Amount: $2,901,907 (DC)– https://projectreporter.nih.gov/project_info_description.cfm?aid=943
8338

The University of Sydney Page 51
Vision?
“The Collaboration for Health IT (Collaboration) is working to bring about significant and positive change in Electronic Health Records
(EHR) software in order to advance patient care, research and education in the dental profession.”
https://collaboration4hit.org/

The University of Sydney Page 52
Dentistry = Drilling + Filling + Billing (and not Killing)?
How do we
• escape the cycle of repair and replacement?• integrate with the broader health system?• show evidence of improved oral health outcomes?• shift from a procedure-based to a diagnosis-based profession?• minimize the variation in the delivery of care?• provide patient-centered rather than oral health-centered care? • shape education based on the changing health profile of the
community?• help dental practitioners to adapt to a delivery system integration that
includes medical, allied health, mental care?• integrate the work of mid-career level providers?
The University of Sydney
How will success look like?
Dental professionals improve oral and general health supported by
§ data-driven analysis of oral health status via standardized caries risk management strategies
§ use of standardized diagnostic terminology to reap benefits of proper coding (SNODDS)
§ prevention is prioritized over treatment§ strictly utilizes evidence-based treatment approaches§ embed oral health as part of primary health§ treat the patient, not just the teeth
“What would an EHR system look like that dentists suddenly can’t live without?”
Paraphrased from: I.B.M.’s Watson’s health team, Eric Brownhttp://www.nytimes.com/2015/03/22/opinion/sunday/why-health-care-tech-is-still-so-bad.html?_r=0

The University of Sydney
What are the barriers?

The University of Sydney Page 55
Recalcitrant Profession
“The dental education paradigm continues to focus on restorative care and a practice environment that is detached and isolated from the
other health professions.” Polverini, P. J., & Krebsbach, P. H. (2017). Research and Discovery Science and the Future of Dental Education and
Practice, (September), 97–107. http://doi.org/10.21815/JDE.017.040
Impressions are remarkably perseverant!Elizabeth Kolbert: Why Facts Don’t Change Our Minds
http://www.newyorker.com/magazine/2017/02/27/why-facts-dont-change-our-minds
When the axe came into the woods, many of the trees said:
“At least the handle is one of us.”
The University of Sydney Page 56
AI and Behaviour Change
Artificial Intelligence in Health Care. Will the Value Match the Hype? by Emanuel and WachterJAMA. May 20, 2019. doi:10.1001/jama.2019.4914 https://jamanetwork.com/journals/jama/fullarticle/2734581
– Convert AI-derived predictions into effective action
– Behaviour Changeo Clinicianso Patients
– Data, analytics and AI are about identification.
– Behaviour change of clinicians and patients are triggered by structures, culture and incentives.

The University of Sydney Page 57
“If we’re not careful with how we use data from the medical system, we’ll take the enormous power of algorithms, and we’ll use them to automate and scale up
our ignorance and our greed.”
Ziad Obermeyer, Associate Professor of Health Policy and Management at UC Berkeley

The University of Sydney Page 58
Issues when using observational data
§ “There is an implicit assumption that once we collect enough data, bias will no longer be a problem”
§ Algorithms will reproduce human judgement, bias, errors and incentives ($)
Olhede SC, Wolfe PJ. The growing ubiquity of algorithms in society: implications, impacts and innovations.Philos Trans A Math Phys Eng Sci. 2018;376(2128):20170364.
Ziad Obermeyer, Brian Powers, Christine Vogeli, SendhilMullainathan: Dissecting racial bias in an algorithm used to manage the health of populations. Science 25 Oct 2019:Vol. 366, Issue 6464, pp. 447-453
https://www.wired.com/story/how-algorithm-favored-whites-over-blacks-health-care/

The University of Sydney Page 59
Data Stewardship

The University of Sydney Page 60
Re-identification
We randomly sampled 5,000 numbers from our crowdsourcedMetaPhone dataset and queried the Yelp, Google Places, and Facebook directories. With little marginal effort and just those three sources—all free and public—we matched 1,356 (27.1%) of the numbers. Specifically, there were 378 hits (7.6%) on Yelp, 684 (13.7%) on Google Places, and 618 (12.3%) on Facebook.
http://www.theatlantic.com/technology/archive/2013/12/stanford-researchers-it-is-trivially-easy-to-match-metadata-to-real-people/282642/
The University of Sydney Page 61
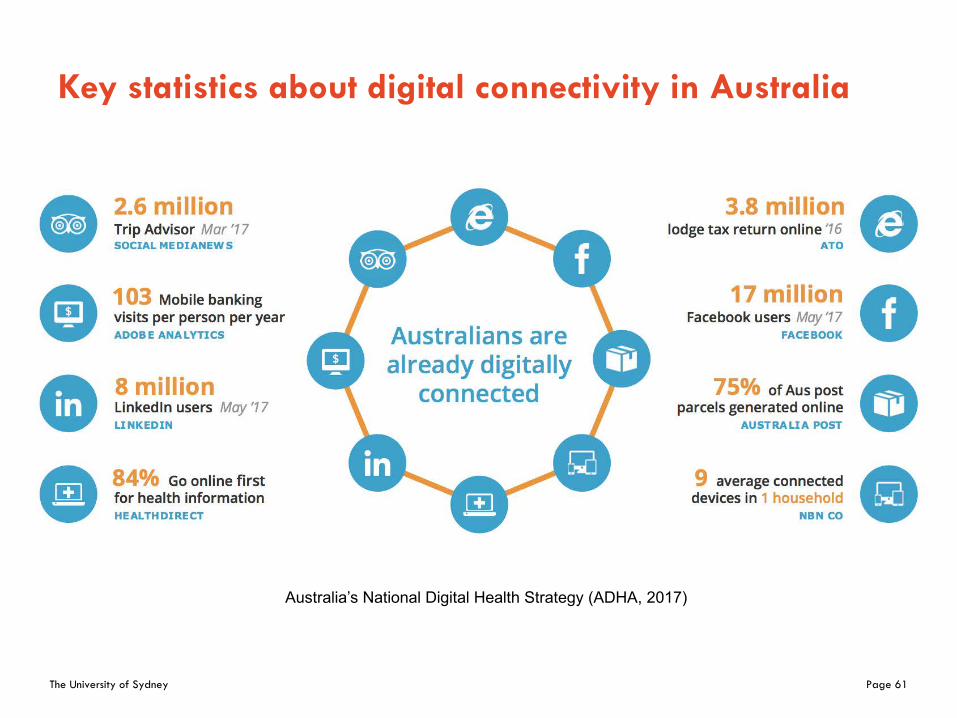
Key statistics about digital connectivity in Australia
Australia’s National Digital Health Strategy (ADHA, 2017)

The University of Sydney Page 62
Australians give away a lot of personal information
Data Availability and Use: Productivity Commission Inquiry Report, No. 82, 31 March 2017http://www.pc.gov.au/inquiries/completed/data-access/report/data-access.pdf

The University of Sydney Page 63
Technology Impact Depicted in Entertainment
1998Gattaca
Genetic profiling
2002 Minority Report
Pre-crime unit
2018 Anon
Lack of anonymity
2018 -Altered Carbon
Consciousness is digitized and stored

The University of Sydney Page 64
Medical Devices Hit By Ransomware
A Bayer MedRad device used to assist in MRI scans infected with the WannaCry ransomware.
JAMA: Cybersecurity—A Serious Patient Care Concernhttp://jamanetwork.com/journals/jama/fullarticle/2654933
The University of Sydney Page 65
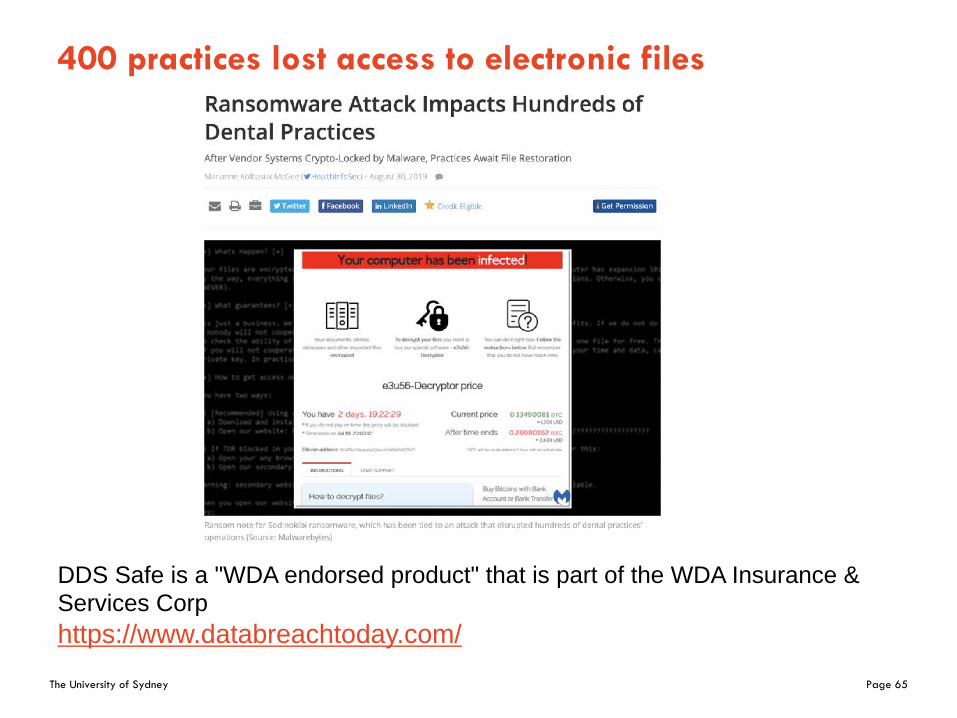
400 practices lost access to electronic files
DDS Safe is a "WDA endorsed product" that is part of the WDA Insurance & Services Corphttps://www.databreachtoday.com/

The University of Sydney Page 66
Consequences of Machine Learning
• convenience and efficiency • phenomenon of deskilling• focus on text at the expense of other elements• reduced interest in and decreased ability to
perform holistic evaluations of patients
Trend:
“purely accuracy-driven performance metrics are pushing toward more opaque models, like artificial neural networks >> tension between
accuracy and interpretability”
Cabitza F, Rasoini R, Gensini GF. Unintended Consequences of Machine Learning in Medicine.AMA. Published online July 20, 2017.
http://jamanetwork.com/journals/jama/fullarticle/2645762

The University of Sydney Page 67
Garbage In - Garbage Out
FT Magazine: http://www.ft.com/intl/cms/s/2/21a6e7d8-b479-11e3-a09a-00144feabdc0.htmlNature: http://www.nature.com/news/when-google-got-flu-wrong-1.12413#/fever
The Conversation: https://theconversation.com/social-media-for-tracking-disease-outbreaks-fad-or-way-of-the-future-66401

The University of Sydney
Vision of a Learning Health System

The University of Sydney Page 69
Impact of Advances in Discovery and Clinical Sciences
– Misalignment of stakeholders à Health sector underperformance
– Ageing demographics: 20% of the global population > 60 years in 2050
– Increasing burden of non-communicable chronic diseases (NCDs): 75% of healthcare expenses
– Acceleration of science and discovery:Unaffordable costs: cell therapy > $1m / patient
– Progress in technology:Interconnectivity breaks the structures of healthcare systems
Health and Healthcare in the Fourth Industrial Revolution: Global Future Council on the Future of Health and Healthcare 2016-2018 https://www.weforum.org/reports/health-and-healthcare-in-the-fourth-industrial-revolution-global-future-
council-on-the-future-of-health-and-healthcare-2016-2018
The University of Sydney Page 70
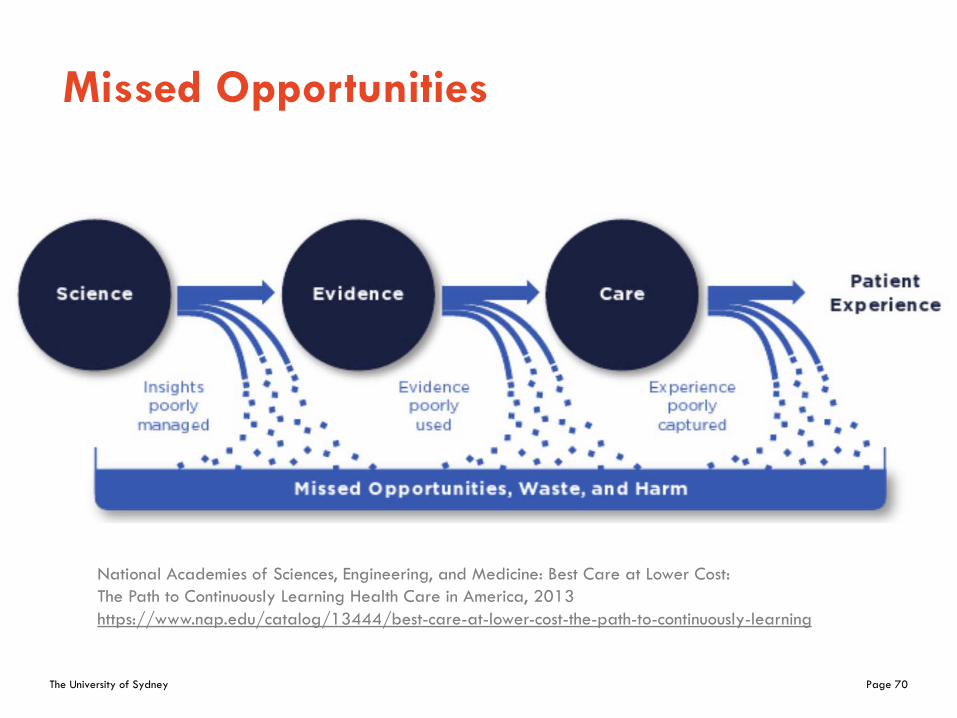
Missed Opportunities
National Academies of Sciences, Engineering, and Medicine: Best Care at Lower Cost: The Path to Continuously Learning Health Care in America, 2013https://www.nap.edu/catalog/13444/best-care-at-lower-cost-the-path-to-continuously-learning

The University of Sydney
A health system that can learn
§ Every patient’s characteristics and experience are available for study
§ Best practice knowledge is immediately available to support decisions
§ Improvement is continuous through ongoing study
§ This happens routinely, economically and almost invisibly
§ All of this is part of the culture
§ Charles P. Friedman, PhD§ Josiah Macy, Jr. Professor of Medical Education§ Chair, Department of Learning Health Sciences§ Professor of Information and Public Health§ University of Michigan

The University of Sydney Page 72
Data FAIRness & Knowledge FAIRness
• Deliberate and evolutionary process of infrastructure co-production in which the full spectrum of stakeholders are directly engaged.
• Purposefully collected data outside of care experience can be important components of the learning process.
Friedman, Rubin, Sullivan: Toward an Information Infrastructure
for Global Health Improvement,IMIA May 2017:
https://imia.schattauer.de/en/contents/archive/issue/special/manuscript/27496.ht
ml

The University of Sydney Page 73
The LHS Must Do This
AssembleRelevant Data
Take Action to Change Practice
InterpretResults
AnalyzeData
Deliver Tailored Message
A Problem of Interest
Decision to Study

The University of Sydney Page 74
Not This
AssembleRelevant Data
Take Action to Change Practice
InterpretResults
AnalyzeData
Deliver Tailored Message
A Problem of Interest
Decision to Study
Journals?

The University of Sydney Page 75
How can we accelerate 17 years to 17 months
Screen Shot 2015-02-21 at 6.47.53 PM

The University of Sydney
FMH’s Response

The University of Sydney Page 77
Digital Health & Health Service Informatics
Academic Lead role entails providing leadership to – ensure that digital health education and training is
embedded in FMH programs to position our graduates for future practice
– coordinate and align research activities in digital health space across the Faculty
– collaborate with our partners in other faculties, LHDs, NSW Health, institutes, government, NGOs, ...
– guide the development of potential commercial activities

The University of Sydney Page 78
Advisory Team
– Natasha Nassar, Professor, Chair in Translational Childhood Medicine– Andrew Black, Director, Westmead Living Lab – Tim Shaw, Professor of eHealth, and Director of Research and Workforce
Capacity, Digital Health CRC– Tom Snelling, Professor: Clinical Trials/Vaccines/Infectious Diseases expert– Jonathan Morris AM, Professor of ObGyn & Director Clinical and Population
Perinatal Health Research at the Kolling Institute – Clara Chow, Professor of Medicine and Academic Director Westmead
Applied Research Centre, Cardiologist, Westmead Hospital– Naren Gunja, Associate Professor, CMIO, Western Sydney Health District – Adam Elshaug, Professor of Health Policy, Co-Director Menzies Centre for
Health Policy– Mark Rees, Professor: Dep Exec Dean FMH (Research Partnerships)– Supported by Jacqueline Wells, Project Officer, Digital Health and Informatics
Network (DHIN)

The University of Sydney Page 79
Working Party: Digital Health Education Strategy
Chair A/Prof Melissa Baysari: [email protected]
Goaldevelop a strategy for professional entry-level health education in digital health, eHealth and informatics
Members represent the disciplines of digital health, dentistry, nursing, pharmacy, physiotherapy, occupational therapy, speech pathology, exercise and sport science, rehabilitation counselling and medicine.

The University of Sydney Page 80
Working Party: Science Communication, Public Engagement & Outreach
ChairA/Prof Sonja van Wichelen: [email protected]
Goaldevelop a strategy for how we connect digital health with the humanities, arts and social sciences
Leading the Working Party is Associate Professor Sonja van Wichelen who is Research Director of the Biohumanity Theme, exploring the influence of the biosciences on concepts of human individuality.

The University of Sydney Page 81
Working Party Artificial Intelligence Alliance
ChairDr Andrew Black: [email protected]
Goaldevelop close collaboration between the University of Sydney and the AAAiH
The Australian Alliance for Artificial Intelligence in Healthcare brings together more than 60 national and international partners and engaged stakeholders in academia, government, consumer, clinical and industry organisations to translate frontier artificial intelligence (AI) technologies into real-world health services.
Dr Andrew Black is also the NSW State Hub Lead.

The University of Sydney Page 82
Working Party Digital Health Executive Program
ChairDr Audrey P Wang: [email protected]
Goaldevelop a strategy and program for Executive Training in the Digital Health and Biomedical Informatics space
Executives will need to champion a new era of a digitally smart and agile workforce with sweeping changes to the people and culture healthcare strategy.
The University of Sydney Page 83
Discipline of Biomedical Informatics and Digital Health in the School of Medical Sciences (SoMS)
– biomedical informatics departments = integral part of top-tier academic health science centres
– Research Mission
– trigger innovation from the clinical floor up to the health system level
– Educational Mission– educate all levels of health professionals about data
science and digital health on a par in importance with anatomy and physiology
– Policy Development– at Health System, State and National level striving for
harmonisation, standard adoption and sharing of data

The University of Sydney Page 84
eHealth@Sydney 2020
Tuesday 11th February, 2020 Charles Perkins CentreThe University of Sydney
Keynote speaker: Dr Charles FriedmanDepartment Chair of Learning Health Sciences, University of MichiganEditor-in-Chief: Learning Health Systems Journal dhin.net.au/ehealthsydney-2020/

The University of Sydney Page 85
eHealth@Sydney 2020Plenary speakers – 11 February, 2020• Professor Wendy Chapman, Associate Dean for Digital Health and Informatics,
University of Melbourne• Professor Enrico Coeira, Director of the Centre for Health Informatics, Australian Institute
of Health Innovation, Macquarie University• David Bunker, Executive Director, Queensland Genomics
Monday 10th February, 2020 4.30pm-5.30pmCharles Perkins Centre
Associate Professor Patricia Abbott, Director of the Hillman Scholars in Nursing Innovation Program and Associate Professor at the University of Michigan School of Nursing, will launch the eHealth@Sydney 2020 event program with a talk on progress towards the adoption of Health Information Technologies in health.

The University of Sydney Page 86
Thank you."The most serious misjudgement we made was to think that a gradual, incremental effort would work.”
Heiko Spallek– [email protected]– + 61 439 320 490– https://linktr.ee/heikospallek
William G.Bowen, president of Princeton University (1972-1988)
Slideshttp://bit.ly/Spallek-HISA-2019