Embed Size (px)
Citation preview
The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
2007;89:2788-2802. J Bone Joint Surg Am.J. Saleh William M. Mihalko, Yaw Boachie-Adjei, Jeffrey T. Spang, John P. Fulkerson, Elizabeth A. Arendt and Khaled
Patellofemoral ArthritisControversies and Techniques in the Surgical Management of
This information is current as of July 22, 2010
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery

Selected
Instructional
Course Lectures
The American Academy of Orthopaedic Surgeons
PAUL J. DUWELIUSEDITOR, VOL. 57
COMMITTEE
PAUL J. DUWELIUSCHAIRMAN
FREDERICK M. AZAR
KENNETH A. EGOL
J. LAWRENCE MARSH
MARY I. O’CONNOR
EX-OFFICIO
DEMPSEY S. SPRINGFIELDDEPUTY EDITOR OF THE JOURNAL OF BONE AND JOINT SURGERY
FOR INSTRUCTIONAL COURSE LECTURES
JAMES D. HECKMANEDITOR-IN-CHIEF,
THE JOURNAL OF BONE AND JOINT SURGERY
Printed with permission of the American Academy ofOrthopaedic Surgeons. This article, as well as other lecturespresented at the Academy’s Annual Meeting, will be availablein March 2008 in Instructional Course Lectures, Volume 57.The complete volume can be ordered online at www.aaos.org,or by calling 800-626-6726 (8 A.M.-5 P.M., Central time).
2787

Controversies and Techniques in the SurgicalManagement of Patellofemoral Arthritis
By William M. Mihalko, MD, PhD, Yaw Boachie-Adjei, MD, Jeffrey T. Spang, MD, John P. Fulkerson, MD,Elizabeth A. Arendt, MD, and Khaled J. Saleh, MD, MSc(Epid), FRCSC
An Instructional Course Lecture, American Academy of Orthopaedic Surgeons
The patellofemoral joint is a complexarticulation that remains a relativelyuncommon topic in the orthopaedicliterature. Most studies have been ofcadavers, and there have been very fewin vivo or clinical measurements1. Therelative lack of interest in the patello-femoral joint is surprising given the factthat patellofemoral symptoms arerelatively common and can be ex-tremely debilitating.
Abnormal mechanics of the pa-tellofemoral articulation lead to abnor-mal pressures on the articular surface,pain, cartilage breakdown, and severefunctional limitations secondary to an-terior knee pain2. An understanding ofbasic concepts regarding patellofemoraljoint kinematics, forces, and contactpatterns will enhance the surgeon’sunderstanding of the progression ofpatellofemoral arthritis. Furthermore,this understanding should ultimatelyallow the surgeon to choose the appro-priate option for each stage of patello-femoral disease.
Anatomic ConsiderationsThe patellofemoral joint comprises thepatella, the femoral condyles, and thetrochlear groove. The patella is a sesa-moid bone that acts to redirect theforces of the quadriceps to the distalpart of the femur, functioning as alever arm to increase the efficiency ofthe extensor mechanism. The femoralcondyles have a dual articulation withthe medial and lateral facets of thepatella3. Additionally, almost 75% ofpeople have a third articulating facet onthe medial ridge of the patella thatarticulates with the medial femoralcondyle after 120� of flexion4. Theridge of the lateral condyle is moreprominent than the medial ridge onlateral radiographs of the knee. Adeficient lateral condyle may be ap-preciated on lateral radiographs andmay contribute to patellar instability.Between the condyles is the centralsulcus, or trochlear groove. The quad-riceps and the patellar tendon have abalanced, blended insertion and ori-
gin on the patella and generatethe majority of forces acting on thepatella.
The flexion-extension pathwayof the patellofemoral joint is a complexand dynamic cycle. In full extension,the patella does not come into contactwith the trochlear groove. As kneeflexion is initiated, the inferior polecomes into contact with the trochlea.As knee flexion continues from 0� to90�, the area of patellofemoral contactmoves proximally on the patella, fromthe inferior pole toward the centralportion, and finally toward thesuperior pole. At 90� of flexion, onlythe superior region of the patella is incontact with the distal aspect of thetrochlear groove5. After 120� of flex-ion, only the most medial and lateralaspects of the patella come into con-tact with the femoral condyles. Thearticular cartilage of the patella is thethickest of any in the body, an adapta-tion to the great pressures throughoutthe patellofemoral joint during knee
Disclosure: In support of their research for or preparation of this work, one or more of the authors received, in any one year, outside funding or grantsin excess of $10,000 from Stryker Orthopaedics. One or more of the authors or a member of his or her immediate family received, in any one year,payments or other benefits in excess of $10,000 or a commitment or agreement to provide such benefits from commercial entities (StrykerOrthopaedics and Smith and Nephew). Also, commercial entities (Stryker Orthopaedics and Smith and Nephew) paid or directed in any one year, oragreed to pay or direct, benefits in excess of $10,000 to a research fund, foundation, division, center, clinical practice, or other charitable ornonprofit organization with which one or more of the authors, or a member of his or her immediate family, is affiliated or associated.
J Bone Joint Surg Am. 2007;89:2788-802
2788
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

flexion6. The majority of patellar mo-tion occurs in the sagittal plane withknee flexion.
Joint ForcesIn early flexion, there is a small com-pressive force vector on the patello-femoral joint. As flexion increases, sodo the compressive forces across thejoint. The three major forces acting onthe patella include (1) the pull of thequadriceps, (2) the tension in the pa-tellar tendon, and (3) the joint reactiveforce of the patellofemoral joint. Theseforces must act through one point in thesagittal plane to be in equilibrium.Unlike a simple lever arm, the patellacreates a changing fulcrum position forthe quadriceps force. The patellar ten-don force is therefore always less thanthe quadriceps force and is more pro-nounced in deep flexion. As detailedabove, in early flexion this point is in theinferior pole of the patella and in deeperflexion this point moves to the superiorpole. Estimates of the forces through thepatella range from 1.5 times bodyweight at 30� of flexion to six timesbody weight at 90� of flexion. Someauthors6,7 have suggested that contactbetween the quadriceps tendon and thedistal part of the femur helps to dissi-pate contact forces after 90� of kneeflexion.
Patellofemoral Contact PatternsAs the contact point of the patellamigrates from the inferior pole in earlyflexion to the superior pole in deepflexion, the contact surface area in-creases. There is a steady increase incontact surface area from initial contactin early flexion to about 60�. There aremixed reports regarding the area ofpatellofemoral contact from 60� to 90�6.After 90� of flexion, the reportedamounts of contact area have varied,depending on individual anatomy, theamount of force applied by the quadri-ceps tendon, and the thickness of thearticular cartilage. It should also benoted that the quadriceps tendon playsa large role in the transfer of load. Past90� of flexion, the tendon transfers loadto the trochlear groove of the femur,providing more contact as well8.
History and Physical Examinationof Patients with an ArthriticPatellofemoral JointExamination of a patient with anteriorknee pain begins, like any other medicalworkup, with a thorough and detailedhistory. Gathering information such asthe duration of discomfort, the locationand quality of pain, provocative orpalliative factors, and functional limi-tation is a key portion of the patientevaluation. The summation of thesefacts will give the orthopaedic surgeonimportant clues regarding the etiologyand diagnosis of the knee pain. Pa-tients with patellofemoral arthritis oftenpresent with anterior knee pain, whichmay radiate medially and/or posteri-orly. The pain is often worse withprolonged flexion or when the patient isgoing downstairs. Knee catching, lock-ing, or giving-way are less specificsymptoms that may or may not repre-sent pathological involvement of thepatellofemoral joint. The subsequentphysical examination will allow the ex-aminer to more accurately differentiatebetween patellofemoral disorders andother derangements of the knee.
Physical examination of the knee,and particularly the patellofemoraljoint, requires both static and dynamicassessment. It has been described as athree-part examination, consistingof standing, sitting, and supineassessments7,9.
The initial examination beginswith the patient standing. Assessment ofthe stance position and visual gaitanalysis are important. The axial align-ment of the lower extremities should benoted, as abnormalities of the pelvis,femur, or tibia can result in patellofe-moral disorders. At the knee, genuvarum and valgum alter the mechanicsof the patellofemoral articulation.Measurement of the Q angle provides akey piece of information in an evalua-tion of a patient with knee pain, espe-cially when the patellofemoralarticulation is the suspected culprit.Briefly, the Q angle is the angle betweentwo lines, one drawn from the middle ofthe tibial tubercle to the patella and theother drawn from the patella to theanterior superior iliac spine. The nor-
mal Q angle ranges from 10� to 20�9, buta number of variations have been de-scribed. Freeman10 described a normalQ angle of 10� to 20� in females and 8�to 10� in males. Aglietti et al.11 describeda normal Q angle of 17� in females and14� in males. Hughston12 believed that aQ angle of >10� in either gender wasabnormal and should be corrected.Despite these variations, large devia-tions from these ranges are definitelyconsidered relevant. An increased Qangle may lead to an increased valgusforce on the patella. This may causelateral patellar subluxation or tilt andincreased compression of the lateralpatellar facet. Pelvic geometry is also animportant element in the examination,as a widened pelvis may increase the Qangle. The pelvic geometry in womendiffers slightly from that in men, aswomen tend to have a wider, gynecoidpelvis. Femoral anteversion may alsocause increased knee valgus. This isindirectly indicated by the presence ofan inward pointing, or ‘‘squinting,’’patella. To ensure accurate examinationof the patella, it is imperative that thepatient’s feet be pointing forward andaligned. After observation of the axialalignment, gait is assessed. An antalgic,or painful, gait may cause a shortenedstance phase of the affected lower limb.This confirms the side of the knee dis-order. Limb-length inequality as wellas varus or valgus thrust should also benoted if present. Lastly, the patient maybe asked to squat and hold that positionfor a few seconds. This is the half-squattest, and if it recreates anterior kneepain it strongly suggests a patellofe-moral etiology.
The second part of the assessmentis performed with the patient seatedwith the legs over the side of theexamination table. The lower limbsshould be visually inspected first. Thighmuscle girth should be evaluated forbilateral symmetry. Atrophy of the vas-tus medialis muscles, evidenced byflattening, contributes to patellofemoralsymptoms. The anatomic position ofthe patella should be carefully observedas it may give clues to the cause of pain.Patella alta, or superior displacement ofthe patella, is common in patients with
2789
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

a patellofemoral disorder, particularlyinstability. The clinical finding of‘‘grasshopper eyes,’’ in which the patel-lae are displaced proximally and areexternally rotated has been described10.Patella alta is radiographically con-firmed with use of the Insall-Salvatiratio. Rotational malalignment is as-sessed by observing the relationship ofthe superior patellar pole to the inferiorpatellar pole. Most commonly, the in-ferior pole is lateral to the superior pole,and deviations from this are importantas they may suggest patellar maltrack-ing. Skin depressions medial and lateralto the inferior pole of the patella arenormal. Their absence can signify aknee effusion, suggesting an intra-articular disorder as opposed to apatellofemoral disorder. Palpation ofthe knee is performed next. The im-portant structures to evaluate includethe patellar margins, the femoral epi-condyles, the tibiofemoral joint line, theGerdy tubercle, and the fibular head.Tenderness in any one or a combinationof these areas may suggest a patholog-ical entity outside of the patellofemoralarticulation.
The third portion of the exami-nation requires the patient to lie supine.This position allows a number of tests tobe performed to evaluate the forcesacting on the patella. The patient is firstasked to flex and extend the knee.Activation of the quadriceps complexpermits visual recording of patellartracking. Normally, in terminal exten-sion, the patella lies laterally within thefemoral sulcus. As the knee is flexed past30�, the patella engages the middle ofthe femoral sulcus13. Lateral subluxationof the patella in terminal extension isknown as the ‘‘J sign.’’ As the knee issubsequently flexed and extended, thepatella may appear to jump in and outof the femoral sulcus. Another test is theactive quadriceps pull test14, in whichthe knee is extended and the patient isasked to contract the quadriceps mus-cles. Normally, the patella tracks supe-riorly in a straight line; lateral deviationof the patella is considered abnormal.To perform the patellofemoral grindtest13, the examiner depresses the patellain the femoral sulcus and then asks the
patient to contract the quadriceps. Painelicited from this test may representarticular injury. To elicit the patellarapprehension sign of Fairbank15, an-other indication of patellar instability,the patient is asked to flex the knee to20� and the examiner then applies alaterally directed force on the patella. Atthis time, the patient may fear patellardislocation and instinctively contractthe quadriceps and extend the knee toguard against it. The passive patellaglide test is performed by flexing theknee 20� to 30�. The examiner thenvisually divides the patella into threevertical segments, manually displacesthe patella medially or laterally, andmeasures the degree of displacement. Ifthe patella displaces more than threesegments laterally, the medial retinacu-lum is probably incompetent. If thepatella displaces less than one segmentmedially, the lateral retinaculum istight. Both of these instances predisposethe patient to lateral patellar subluxa-tion and resultant pain. For the passivepatellar tilt test, the examiner extendsthe patient’s knee and then lifts thelateral edge of the patella away from thelateral femoral condyle. Normally, thepatella will lift off slightly from thelateral femoral condyle, representing apositive tilt angle. An inability to lift thepatella represents a neutral or negativetilt angle and is consistent with a tightlateral retinaculum.
The physical examination of apatient with anterior knee pain is com-prehensive and, when done correctly,can give valuable clues regarding thepresence or absence of a patellofemoraldisorder. The clues can then be used todetermine whether further evaluation isneeded.
Nonoperative Management ofPatellofemoral ArthritisPhysical therapy that includes quadri-ceps strengthening has been the cor-nerstone of nonoperative management.The goal of any strengthening programis to improve the function of the limbwhile not overloading the damagedpatellofemoral articulation. Recentlyimproved understanding of more gen-eralized therapy approaches has shifted
focus away from just the patellofemoraljoint to overall body balance andstability.
Stretching is a simple modalitythat may be beneficial in the manage-ment of patellofemoral arthritis. Thegoal of stretching is to restore passivesoft-tissue balance of the patella. In mostcases, the lateral tissues of the anterioraspect of the knee have become ex-cessively tight. A directed patella-mobilization program focusing on re-leasing the lateral tissues surroundingthe patella may help to decrease excessivepressure on the lateral facet. Althoughattempts at relaxation of the lateral tis-sues may ultimately prove unsuccessful,the low morbidity associated with pa-tellar mobilization and capsular stretch-ing makes its inclusion in nonoperativeregimens simple.
Strengthening of the vastus me-dialis obliquus is a classic physicaltherapy modality for treatment of lat-eral patellar maltracking. Dysplasiaof the vastus medialis obliquus has beenreported in patients with problemsdue to excessive lateral patellar tracking.Most physical therapy regimensinvolve an attempt to selectivelystrengthen the vastus medialis obliquusto increase medially directed forcesacross the patella. Despite the associa-tion between dysplasia of the vastusmedialis obliquus and patellar mal-tracking, the utility and success of se-lective strengthening of the vastusmedialis obliquus have not been over-whelmingly supported by the currentliterature.
Physical therapy ideals haveshifted away from a focus on localmuscle control and joint function to afocus on limb control and body posi-tioning. In that respect, so-called corestrengthening is an excellent approachto the treatment of a patient withpatellofemoral arthritis. Core strength-ening focuses on abdominal musclecontrol, trunk balance, and limb con-trol. Exercises designed to improve limbbalance focus on the hip and the knee tomaximize the efficiency of the limb. Inthis way, alignment and balance areimproved, which hopefully leads todecreased pressures on the patello-
2790
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

femoral articulation and improvedfunction. One key benefit of usingcore-strengthening principles duringrehabilitation is the avoidance of ex-cessive repetitive strengthening exer-cises about the knee, which mayexacerbate symptoms.
The patellar McConnell tapetechnique can be useful when excessivelateral patellar translation and tilt arepart of the clinical presentation. Thistechnique depends on having sufficientmobility remaining in the patellofe-moral articulation to medialize the pa-tella passively. A standard tapingregimen requires understanding of thetaping system, and the skin must be ableto withstand multiple applications ofadhesive tape.
Several braces have been designedto alleviate anterior knee pain emanat-ing from the patellofemoral joint. Mostbraces are used in an attempt to drivethe patella medially during the kneeflexion cycle and offload the lateralfacet. The success of these braces isvariable and depends on the willingnessof patients to reliably apply the braceeach day. Some patients may also ex-perience lessening of symptoms as aresult of the heat retained by manyneoprene knee braces. There are limitedclinical data on patellofemoral bracing,but the easy application of such bracesmakes their use in a nonoperative ap-proach reasonable.
The rigors of land-based therapymay aggravate the problems at thepatellofemoral articulation, thereby re-ducing any potential benefits. In suchcases, water exercises may prove helpful.Obese patients may benefit the mostfrom water therapy programs, as jointforces are reduced during these exerciseprograms. Principles similar to thoseused during land-based therapy shouldbe emphasized, including global corestrengthening focusing on abdominal,hip, and knee balance.
When patellofemoral pain haselements of complex regional pain syn-drome (hypersensitivity, burning pain,and pain at rest), aggressive pain man-agement is recommended. Pertinentmodalities include desensitizationtherapy, gabapentin (Neurontin) or
pregabapentin (Lyrica), local applica-tion of a lidocaine patch, and formalconsultation with a pain managementspecialist.
Surgical ProceduresRole of Arthroscopy andSoft-Tissue RealignmentArthroscopic Debridement
When a patient presents with mechan-ical symptoms and a loose body issuspected or confirmed on imagingstudies, an arthroscopic debridementmay be warranted. A chondroplastymay also temporarily relieve discomfortand disability when patellofemoral ar-thritis is present and associated withswelling, crepitus, and synovitis. Re-moval of loose cartilage from the patellaor femur may limit mechanical irritantsas well. The surgeon must realize thatthese measures may have only tempo-rary effects on symptoms and if under-lying mechanical factors havecontributed to the progression of thedisease they will continue to contributeto the clinical progression of symptomsas well.
Arthroscopic Lateral Retinacular Release
This procedure is frequently utilizedand is most effective for treatment ofisolated lateral patellar tilt. When clin-ical and radiographic examinationsconfirm excessive lateral tilt, lateralfacet arthritis may ensue (Fig. 1). Re-lease of the lateral retinacular structuresmay decrease pressure on the lateralfacet and decrease pain. The tight lateralretinaculum should be confirmed onphysical examination and by radio-graphs in a patient for whom conser-vative measures have failed. Theprocedure may be useful in patientswith lateral facet arthrosis with lateraltilt but no subluxation.
When this procedure is per-formed, care should be taken not torelease the tendinous portion of thevastus lateralis muscle from the super-olateral aspect of the patella. This maycause quadriceps weakness and dy-namic imbalance. Release of the lateralstructures may also improve tracking,but when performed in the face ofmalalignment the results are less reliable
unless concurrent tightening of themedial retinacular structures is per-formed. Medial imbrication proceduresare traditionally utilized for treatmentof patellar maltracking, and they maynot be appropriate in the face of ar-thritis of the patellofemoral joint. In thearthritic situation, a medial imbricationmay increase forces on the medial facetof the patella and on the medial condyleand lead to overload of the medialaspect of the joint. Lateral release hasnot been shown to provide long-termbenefit for patients with patellofemoralarthritis.
Lateral Patellar Facetectomy
In patients with long-standing patello-femoral disease, excessive lateral tilt and/or translation may lead to the formationof a large lateral osteophyte visible on theMerchant radiograph (Fig. 2). Someauthors, including Yercan et al.16, sup-port excision of the lateral facet over-growth and retensioning of the lateraltissues. Lateral patellar facetectomy mayprovide pain relief and decrease thelateral overload in the patellofemoralcompartment, but it may decrease bonestock necessary for future replacement.
Proximal Soft-Tissue Realignment
Proximal soft-tissue realignment pro-cedures have also been advocated as away to unload the lateral facet andimprove patellar tracking. One of us(J.P.F.) reported limited success withthis procedure (a 62% failure rate whensigns of degenerative joint disease werepresent) and believes that other align-ment procedures offer more reliableresults in patients with patellofemoralarthritis17.
These procedures are focused onarthritis affecting the lateral facet andhave limited utility for patients withmore generalized arthritis. In particular,disease of the trochlea or medial facetmay lead to an increase in pain follow-ing lateral release procedures. For pa-tients with continued symptomsemanating from the lateral aspect of thejoint, more aggressive alignment pro-cedures may be required. Soft-tissuerealignment procedures alone are alsoindicated for skeletally immature pa-
2791
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

tients with a history of recurrent dislo-cations. The mature patient with a highcongruence angle and minimal arthro-sis may benefit from proximal soft-tissue realignment if therapeutic mea-sures have failed. A Q angle of <10� hasalso been associated with betteroutcomes18.
This technique involves a midlineincision from just above the superiorpole of the patella to the medial aspectof the tibial tubercle. A release of thelateral patellofemoral ligament and aretinacular release are performed, leav-ing the synovial tissue intact to isolatethe joint. The lower fibers of the vastuslateralis are released as well, and therelease is carried down to the level of thetubercle. Medially, the vastus medialis iselevated from the underlying capsuleabout 10 cm from its insertion. It is thenadvanced to the lateral free edge of thevastus lateralis, creating a sleeve aroundthe patella. A compression dressing isapplied, and knee motion is begun atseven to ten days after the surgery. Insallet al. reported a 91% rate of satisfactoryresults at four years after use of this
procedure19. Other techniques involv-ing a lateral release with a medial im-brication have also been described20.They involve a similar lateral retinacularrelease with imbrication of the medial
retinacular tissue from the medial aspectof the quadriceps tendon to the proximalaspect of the tibial tubercle. Scuderi et al.reported an 81% rate of good or excel-lent results after 3.5 years of follow-up20.
Distal RealignmentOsteotomy for Realignment
and/or Resurfacing
Tibial tubercle transfer is recommendedfor treatment of patellofemoral arthritisin patients in whom unloading of dis-crete areas of patellar and femoral dis-ease can lead to clinical success.Requisite for this procedure is healthycartilage onto which patellar loadingand tracking can be transferred. Tibialtubercle transfer, when combined withcartilage resurfacing, holds greatpromise and may reduce the need forearly patellofemoral arthroplasty.Through physical and radiographic ex-aminations, the surgeon must firstdetermine which part of the patello-femoral joint is involved in the diseaseprocess and thus needs to be unloaded.Radiographs made with the knee in45� of flexion combined with preciselateral radiographs, magnetic resonanceimaging scans, and arthroscopy allhelp the surgeon to make this determi-nation, and he or she should make surethat all of the imaging studies correlate
Fig. 1
Radiograph showing arthritis of the lateral facet accompanied by excessive
lateral patellar tilt.
Fig. 2
A large lateral osteophyte is visible on this Merchant radiograph. This is often
a finding in end-stage patellofemoral disease, and it is caused by excessive
lateral tilt and/or translation of the patella.
2792
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

with the findings on physicalexamination.
To select the correct osteotomy,one must understand that moving thetibial tubercle anteriorly decreases theflexion of the patella within the troch-lear groove and therefore shifts contacton the patella more proximally so thatthis area is loaded earlier in the flexionarc. The most common areas involvedin patients with malalignment are thelateral and distal articular regions21.Anterior and medial transfer of thetibial tubercle would thus be appropri-ate in these patients. It should be real-ized that dysplasia or atrophy of thequadriceps may also be present in pa-tients with malalignment, and thereforea combined proximal realignment maybe necessary22-24.
There are two main indicationsfor tibial tubercle transfer:
1. The need to realign the patellaby establishing proper alignment.(This may also be accomplished withmedial imbrication and lateral release,but that ‘‘pulls’’ the patella posterome-dially and risks adding excessive load onthe medial facet.)
2. When degenerative disease islimited and a realignment osteotomycan unload the affected area. The ben-efits provided by recent advances inallograft and autograft cartilage resur-facing procedures may also be enhancedby simultaneous tibial tubercle transferto unload the affected areas.
Relative and absolute contraindi-cations to tubercle transfer include in-adequate patient health or obesity, poorbone quality, diffuse patellar or troch-lear chondral degeneration, proximalpatellar lesions (crush injuries), reflexsympathetic dystrophy or diffuse pain,poor motivation on the part of thepatient, and an inadequate trial ofnonoperative measures.
Anterior or Elevation Osteotomy of the
Tibial Tubercle
This procedure, known as the Maquetosteotomy, is designed to unload themore distal areas of the patella anddecrease overall forces within the jointitself. It is particularly effective inyounger patients with distal patellar
articular degeneration, but it does notaddress alignment issues in and ofthemselves. In general, soft-tissue re-lease should be attempted prior to os-teotomy. Contraindications includediffuse involvement of the proximalpole regions of the patella.
The technique is performedthrough a medial parapatellar incisionthat is extended past the tubercle. Thejoint, along with the fat pad, is inspectedand is debrided to allow mobilizationof the tendon. A 2.5 by 5-cm section ofiliac crest is then harvested for theprocedure. The osteotomy can be per-formed with use of multiple small drillholes or a thin oscillating saw blade ‡8cm from the superior aspect of thetubercle distally in the coronal plane.Once mobilized, the proximal segmentis displaced anteriorly, allowing plasticdeformation of the bone at the distalattachment. The iliac crest graft is thenfashioned to allow 1.5 to 2 cm ofanteriorization at the tubercle. Morethan 1.5 cm of anteriorization, however,is associated with a higher prevalenceof skin problems postoperatively. If
necessary, a cancellous screw can beutilized for supplemental fixationthrough the tubercle and the graft, intothe metaphyseal aspect of the tibia.Postoperative care involves use ofcrutches and partial weight-bearing andpassive motion. Full weight-bearing isallowed at six weeks, when the osteot-omy site is usually healed. Maquetreported a 95% rate of successful resultsin his series25, but rates as low as 31%have been reported in other series26
(Fig. 3).
Medial Tibial Tubercle Transfer
This operation, known as the Elmslie-Trillat procedure, is a direct medialtransfer procedure. It is effective forcontrolling instability and lateraltracking27-29. The operation is mainlyindicated for patients with an excessiveQ angle, lateral instability, and patellarand/or trochlear cartilage with grade-IIor less severe lesions. The procedureis contraindicated for patients withchondral lesions with a grade of greaterthan II9, a normal Q angle, or an openproximal tibial physis.
Fig. 3
Lateral and Merchant radiographs of a patient who underwent a Maquet osteotomy and had
eighteen years of pain relief. In the four months prior to presentation, the symptoms and pain had
returned.
2793
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S
The technique is performed withuse of a lateral parapatellar incisionextending from the proximal pole to thedistal aspect of the tibial tubercle. Thelateral patellofemoral ligament is thenreleased along with the lateral retinac-ulum, leaving the underlying synoviallayer intact and preserving the lateralgeniculate blood supply to the patella30.The tubercle is then cut in the coronalplane with use of osteotomes and drillholes to aid in the osteotomy. Theperiosteal sleeve is left intact, and thetubercle is medialized and then fixedwith a cancellous lag screw. After thesurgery, the limb is immobilized for sixweeks and partial weight-bearing isallowed. After six weeks, when radio-graphic evidence of healing has beennoted, motion and strengthening exer-cises are begun. The rate of satisfactoryresults in published series31 has been‡80%.
Anteromedial Tibial Tubercle Osteotomy
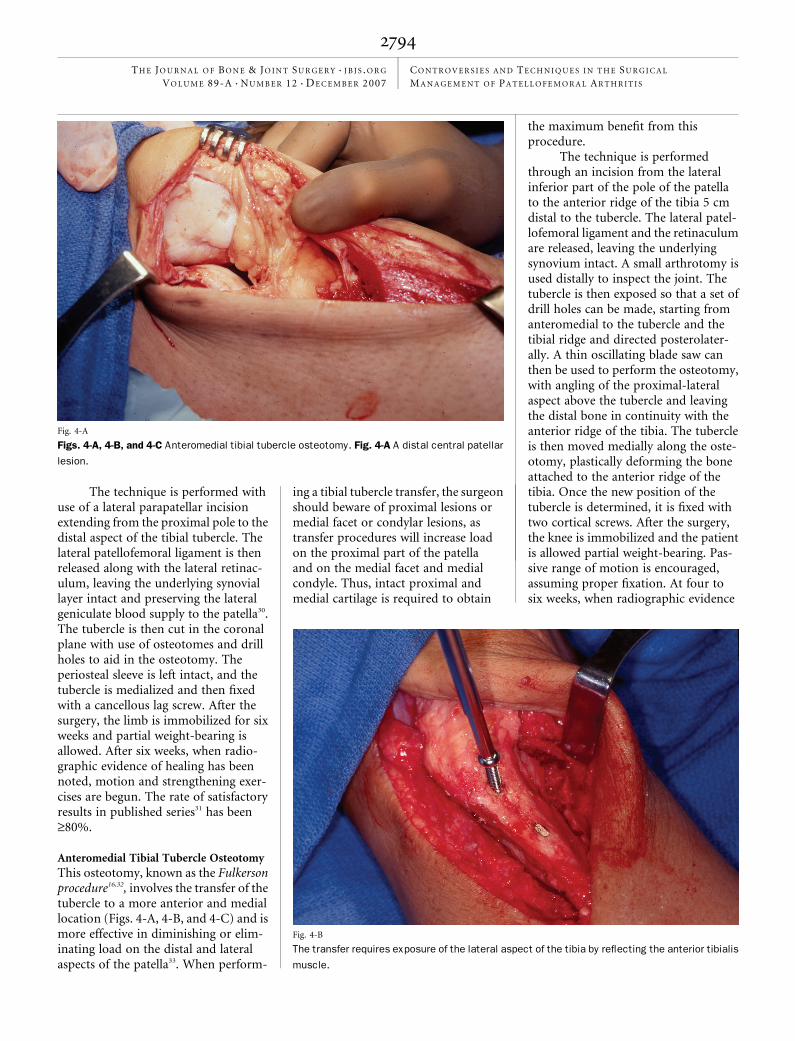
This osteotomy, known as the Fulkersonprocedure16,32, involves the transfer of thetubercle to a more anterior and mediallocation (Figs. 4-A, 4-B, and 4-C) and ismore effective in diminishing or elim-inating load on the distal and lateralaspects of the patella33. When perform-
ing a tibial tubercle transfer, the surgeonshould beware of proximal lesions ormedial facet or condylar lesions, astransfer procedures will increase loadon the proximal part of the patellaand on the medial facet and medialcondyle. Thus, intact proximal andmedial cartilage is required to obtain
the maximum benefit from thisprocedure.
The technique is performedthrough an incision from the lateralinferior part of the pole of the patellato the anterior ridge of the tibia 5 cmdistal to the tubercle. The lateral patel-lofemoral ligament and the retinaculumare released, leaving the underlyingsynovium intact. A small arthrotomy isused distally to inspect the joint. Thetubercle is then exposed so that a set ofdrill holes can be made, starting fromanteromedial to the tubercle and thetibial ridge and directed posterolater-ally. A thin oscillating blade saw canthen be used to perform the osteotomy,with angling of the proximal-lateralaspect above the tubercle and leavingthe distal bone in continuity with theanterior ridge of the tibia. The tubercleis then moved medially along the oste-otomy, plastically deforming the boneattached to the anterior ridge of thetibia. Once the new position of thetubercle is determined, it is fixed withtwo cortical screws. After the surgery,the knee is immobilized and the patientis allowed partial weight-bearing. Pas-sive range of motion is encouraged,assuming proper fixation. At four tosix weeks, when radiographic evidence
Fig. 4-A
Figs. 4-A, 4-B, and 4-C Anteromedial tibial tubercle osteotomy. Fig. 4-A A distal central patellar
lesion.
Fig. 4-B
The transfer requires exposure of the lateral aspect of the tibia by reflecting the anterior tibialis
muscle.
2794
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

of healing has occurred, weight-bearingis advanced along with strengtheningtherapy. Reports have described satis-factory results in more than two-thirdsof patients at five years after thesurgery16,32-34.
Anterolateralization of the Tibial Tubercle
This procedure may be a goodtherapeutic option when there isa medial lesion resulting from over-imbrication during a previous medial-ization of the tibial tubercle. This lesionmay or may not be associated withmedial subluxation. Anterolaterali-zation may also be an effective salvageprocedure following failed anterioriza-tion of the tibial tubercle. It can help torealign a medially tracking patella, un-loading a medial lesion that was over-loaded as a result of a previous medialtubercle transfer, and can be selectivelycombined with resurfacing of the pa-tella. Anterolateralization requires anintact lateral facet.
Autologous Cartilage ResurfacingAutologous chondrocyte implantationmay be indicated for the managementof focal chondral defects in the knee of ayoung patient. The procedure may beconsidered when an intact joint spacehas been documented on radiographic
examination and the lesion has well-shouldered margins, and when there isno diffuse involvement of the remainingportion of the patella. It is critical thatthe etiology of the cartilage defect andthe underlying abnormal biomechanicsof the patella be accurately identifiedbefore the decision is made to moveforward with this procedure. Having a
proper diagnosis as well as correctingthe underlying biomechanical abnor-malities are paramount for a successfuloutcome of autologous chondrocyteimplantation. The workup for thesepatients should include a thorough re-view of the history and a careful physicaland radiographic examination of theaxial alignment of the lower extremityas well as the patellofemoral joint. Aroutine series of radiographs, includinganteroposterior standing, 45� postero-anterior flexion weight-bearing (Rosen-berg), lateral, and skyline (Merchant)radiographs as well as a standing full-length lower-extremity axial alignmentradiograph, is made for all patients.When maltracking is suspected onclinical examination, a computed to-mography scan should be performed,with the leg in extension. Computedtomography scans are then obtainedwith and without quadriceps contrac-tion to assess lateral patellar subluxa-tion, the presence of dysplasia of thetrochlea, and patellar height. All of thesefindings are extremely useful in deter-mining the appropriateness of thisprocedure.
Once a patient is considereda candidate for autologous chon-drocyte implantation, arthroscopic ex-
Fig. 4-C
The anteromedial tibial tubercle transfer is stabilized with two cortical lag screws.
Fig. 5-A
Figs. 5-A through 5-E Patellofemoral arthroplasty. Fig. 5-A Radiographs of a sixty-eight-year-old
with isolated patellofemoral arthritis.
2795
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

amination is performed to assessthe geometry of the lesion and anypathological motion of the joint. Acartilage biopsy specimen is also ob-tained from the non-weight-bearingportion of the superior aspect of theintercondylar notch. This specimen isprocessed and utilized for cell culture.Approximately 200 to 300 mg of artic-ular cartilage is sent in a sterile transportmedium to be commercially culturedand cryopreserved2,35.
The transplantation procedure isthen performed as a second procedure.The chondrocytes are injected beneath aperiosteal patch secured with resorbablesutures and fibrin glue35,36.
The rehabilitation after the sur-gery includes non-weight-bearing andthe use of continuous passive motionfor six to eight hours per day for sixweeks. The patient is allowed to pro-gress to full weight-bearing by fourmonths after the surgery, but inline
impact activities (running) are notpermitted for twelve to eighteen monthsand cutting sports are not allowed for atleast eighteen months35,36.
Minas and Bryant35 performed aseven-year, prospective cohort study offorty-five patients who had undergoneautologous chondrocyte implantationfor treatment of full-thickness chondraldefects of both the patella and thetrochlea, or of one surface of the joint.The average age of the patients at thetime of surgery was 36.9 years, and theaverage duration of follow-up was 47.5months. The patients were surveyed,and 71% were satisfied with the out-come, 16% were neutral, and 13% weredissatisfied. Eighty-seven percent of thepatients said that they would have thesurgical procedure again under similarcircumstances. Seventy-one percent ofthe patients rated the result as good toexcellent and only 7%, as poor. TheShort Form-36 (SF-36), the Knee Soci-ety Score, the Western Ontario andMcMaster Universities OsteoarthritisIndex (WOMAC), and the modifiedCincinnati knee score all showed largesignificant improvements (p = 0.0016).Typically, patients started to have painrelief by four to six months after thesurgery, and they were allowed to returnto non-impact sports activities at ninemonths postoperatively. Full-impactactivities were begun by eighteenmonths after the surgery. The graftsfailed in eight patients (18%). Petersonet al.36 reported similar results, up to tenyears after autologous chondrocyte im-plantation, regardless of whether patel-lar maltracking had been addressed atthe time of, or corrected prior to, thetime of the implantation.
PatellectomyPatellectomy has been performed forover a century as one of the surgicaltreatments of severe anterior kneepain26,37. Its popularity has waxed andwaned over time, with mixed resultsand opinions regarding its effectiveness.One of us (J.P.F.) found that patellec-tomy provided adequate pain relief butwith permanent loss of knee extensorpower17. In the end, the results haddeteriorated with time in the majority
Fig. 5-B
Intraoperatively, the patellofemoral arthritis was seen to be
severe and extensive.
Fig. 5-C
With the Avon patellar replacement system (Stryker Orthopaedics,
Mahwah, New Jersey), an anterior femoral cut guided by a cutting block
with 2-mm shim adjustments is utilized to ensure that no notching occurs.
2796
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

of patients. The operation should beviewed as a salvage procedure, and thesurgeon should warn the patient againstunrealistic expectations concerning theoutcome. Historically, the best resultshave been noted in patients with severearthrosis of the patellofemoral joint.The technique basically involves amidline incision with a sharp dissection
of the patella. Care should be taken torepair the retinaculum to prevent anextensor lag after surgery, and trackingof the quadriceps tendon should bechecked to make sure that a proximalrealignment procedure is not necessary.The patient then is allowed early mo-bilization and weight-bearing aftersurgery.
ReplacementPatellofemoral Arthroplasty
There has been a recent resurgence ofinterest in patellofemoral arthroplasty.It has been indicated for end-stagepatellofemoral arthritis, when deterio-ration of the patellofemoral joint isdiffuse (Figs. 5-A through 5-E). Short-term reports have shown a high level ofeffectiveness, particularly when align-ment issues are corrected38-40. Patellofe-moral arthroplasty can work well inpatients of normal stature with isolatedpatellofemoral disease and no second-ary gain issues.
Isolated patellofemoral arthritisoccurs in up to 10% of patients whohave osteoarthritis of the knee. Over theyears, several different patellofemoralimplants have been designed and pre-vious reports of different patellofemoralimplants have shown variable results38.The Lubinus prosthesis was reported tohave a 50% failure rate at eight years in astudy of seventy-six cases39. The mainreasons for failure were malalignment,wear, impingement, and disease pro-gression. The Avon patellofemoral ar-throplasty was a second-generationdesign with features designed to im-prove alignment and wear40.
The first Avon patellofemoralimplants were placed in September1996 and entered into a prospectivereview. Outcomes were assessed withuse of pain scores, Bartlett’s patellascore, and the Oxford knee score. Todate, 307 knees have been treated and159 knees have been reviewed at twoto five years postoperatively. The me-dian pain score improved from 15 of40 points preoperatively to 36 of 40points at five years. The Bartlett patellascore improved from 10 of 30 points to26 of 30 points at five years. The Oxfordknee score improved from 19 of 48points to 39 of 48 points at five years.Malalignment developed in four knees(1.3%), one of which required distalsoft-tissue realignment. There havebeen no cases of deep infection, frac-ture, wear, or loosening. Evidence ofdisease progression developed in eigh-teen knees (6%), fifteen of which un-derwent revision to a total kneereplacement40-42.
Fig. 5-D
Trial components are utilized to outline the intercondylar extension,
which is then prepared with use of osteotomes to remove the
osteochondral bone. The patella is prepared with use of a patellar
clamp and an onlay technique.
Fig. 5-E
The trochlear implant is cemented and fixed with four pegs, as can be seen in these postoperative
radiographs.
2797
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

The technique involves a medialparapatellar approach to the knee andalignment of the anterior femoral re-section guide (Fig. 5-C). The alignmentof this cutting block is paramount toensure that no femoral notching orundersizing of the trochlear implantoccurs. Most newer designs include anextension of the trochlear implant intothe notch of the femur. This area isresected manually with either a tem-plate (Avon; Stryker Orthopaedics,Mahwah, New Jersey) or, in some sys-tems, with a template and router(Journey; Smith and Nephew, Mem-phis, Tennessee). Peg holes are thendrilled for the template, and the patellais addressed in the usual total-knee-resurfacing fashion. Care should betaken not to allow excessive overstuffingof ‡4 mm since this may affect post-operative motion. Postoperatively, pa-tients are allowed full weight-bearingand motion is initiated immediately.
Results to date suggest that theimproved designs have minimized theprevious problems of malalignment andearly wear42. The functional results arecomparable with those of a total kneereplacement. Complication rates arelow, and there is an excellent postop-erative range of motion. Although dis-ease progression remains a potentialproblem, these prostheses offer a rea-sonable alternative to total knee re-placement in the small group of patientswith isolated patellofemoral disease.
Total Joint Arthroplasty
The use of total knee replacement totreat severe isolated patellofemoral ar-throsis that is recalcitrant to therapeuticmeasures has been well established forolder patients43-46. The procedure is notadvocated for younger patients withisolated patellofemoral arthritis, but itcan be used with reliable results inpatients in their eighth decade of life.Total knee replacement should not beconsidered until nonoperative man-agement has failed. The exact age atwhich total knee arthroplasty becomes aviable option for the treatment ofpatellofemoral arthritis is debatable andcase-dependent, but certainly an ageyounger than fifty-five years should be
considered a relative contraindication46.Careful adherence to proper techniquesand component alignment is well rec-ognized as being crucial to the success ofany total knee arthroplasty, and this isno different for patients with patellofe-moral arthritis. There are areas thatneed more emphasis in these patients toensure a properly aligned knee replace-ment. Particular attention must be di-rected toward the correction of extensormechanism alignment. This is evi-denced by the reported rates of reti-nacular release in these patients, whichare as high as 68%47-49, a threefoldincrease compared with the rates asso-ciated with standard total kneearthroplasty.
Complications involving the ex-tensor mechanism and the patellofe-moral joint remain the primarynoninfectious indications for revisiontotal knee arthroplasty50. Specifically,imbalance of the extensor mechanismand resultant poor patellar tracking arethe most common causes of pain aftertotal knee arthroplasty. Patellofemoralcomplications include patellar sublux-ation or dislocation; wear, loosening, orfailure of the patellar component; andpatellar fracture. Component position-ing, especially rotational alignment ofthe femoral and tibial components, iscritical to patellofemoral stability.Component malrotation is one of themost frequent causes of patellofemoralcomplications51-53.
Any surgical alteration that ab-normally increases the tension in thelateral retinaculum or increases the Qangle and produces a laterally directedmuscle vector will cause lateral mal-tracking of the patella and instability ofthe patellofemoral joint after total kneearthroplasty (Fig. 6). Positioning of thefemoral and tibial components is ofsupreme importance. Valgus angula-tion of the femoral component willincrease the Q angle and produce alaterally directed muscle vector. Thisalignment error is more common inpatients with degenerative arthritis whohave a preoperative valgus deformity of>10� combined with loss of bone stockof the distal part of the lateral femoralcondyle53.
Technically, the distal femoral cutshould be made perpendicular to themechanical axis of the limb (6� of valgusangulation with respect to the anatomicaxis of the femur)54. There are a numberof pitfalls to avoid during componentpositioning. A medially placed pros-thesis will cause increased contactstresses between the lateral flange of thefemoral component and the lateralborder of the patellar component, re-sulting in patellar subluxation (Fig. 7).The femoral component should belateralized as much as possible to reducetension on the lateral retinaculum andreduce shearing stresses placed on thepatella.
Component malrotation is thepredominant cause of patellofemoralcomplications in patients with normalaxial alignment51. The epicondylar axis(a line from the lateral epicondylarprominence to the medial sulcus on themedial epicondyle) is the most reliableguide to ensure correct rotationalalignment of the femoral component.The anterior and posterior femoral cutsshould be made parallel to the epicon-dylar axis. Internal rotation of thefemoral component with respect to thefemur will rotate the trochlear groovemedially, increase tension on the lateralretinaculum, and cause lateral patellarmaltracking. Erring on the side of slightexternal rotation should improve pa-tellar component tracking.
Whiteside’s line (drawn from thedeepest part of the patellar groove an-teriorly to the center of the intercon-dylar notch posteriorly) is anotherreliable guide for rotational alignment55.The anterior and posterior femoral cutsshould be made perpendicular to thisline. The least reliable landmark forrotational alignment of the femoralcomponent is the posterior condylarline. It is internally rotated relative tothe epicondylar axis. If the posteriorcondylar line is used as a reference,posterior deficiency of the lateral fem-oral condyle (and valgus deformity)may cause the femoral component to besubstantially internally rotated. Thiswill cause lateral patellar maltracking.Studies have demonstrated that a fem-oral component set parallel to the pos-
2798
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

terior condylar line is more likely to bemalrotated and more likely to require alateral retinacular release to correct pa-tellar maltracking56,57. Internal rotationof the tibial component will also causepatellar maltracking by forcing the tibiainto external rotation and increasingthe Q angle. The correct placement ofthe tibial component is rotationalalignment of the middle of the compo-nent’s anterior border with the tibialcrest or the medial one-third of thetibial tubercle. The combined amount
of internal rotation of the femoral andtibial components is directly propor-tional to the severity of patellofemoralinstability: 1� to 4� should be usedwhen there is lateral tracking and pa-tellar tilting; 3� to 8�, when there ispatellar subluxation; and 7� to 17�,when there is early patellar dislocation(at less than two years) or late failureof the patellar prosthesis (at two tosix years).
The patellar component shouldbe placed on the medial portion of the
patella, mimicking the normal anatomyof a medially oriented sagittal ridge. Alaterally placed patellar button will in-crease the tension in the lateral reti-naculum and cause lateral patellarmaltracking. A centrally placed patellarcomponent more frequently requires alateral retinacular release to track nor-mally than does a medially placedcomponent57.
During patellar preparation,more bone must be removed from thethicker medial facet, with the patellarcut kept parallel to the plane of themedial and lateral poles of the patella. Acommon mistake involves resection oftoo much of the lateral facet and toolittle of the medial facet with a resultantlateral tilt of the patellar component(Fig. 8).
The current literature seems tofavor patellar resurfacing. Multiplestudies have demonstrated success withpatellar resurfacing, with good relief ofpain and good overall outcomes58-60.However, other studies have shownsuccess without insertion of a patellarcomponent61. Ideally, a patient treatedwithout patellar resurfacing shouldhave no patellar arthritis, and a femoralcomponent that was designed to ac-commodate the native patella should beutilized.
‘‘Overstuffing’’ of the patellofem-oral joint by using a femoral compo-nent that is too large (especially in theanteroposterior dimension) or resect-ing an inadequate amount of the patellaincreases tension on the lateral retinac-ulum62. The mismatch of the implantand the resected bone may also increasethe circumference of the arc that thequadriceps tendon will travel in flexionand this can affect motion as well. Thepatellar resection should equal thethickness of the patellar component,while maintaining at least 12 mm ofbone to minimize the risk of fracture.The goal should be to maintain theoverall thickness of the patellofemoraljoint in the anteroposterior dimension.
Alternative surgical approachessuch as the subvastus, or ‘‘southern,’’approach potentially offer less disrup-tion of the extensor mechanism, fewerrequired lateral releases, less patellar
Fig. 6
A femoral cut made perpendicular to the me-
chanical axiswill place the femoral component in
approximately 6� of valgus angulation with re-
spect to the anatomic axis of the femur. (Med-
ialization of the femoral component may result in
lateral patellar subluxation.) (Reproduced, with
modification, from: Crockarell JR, Guyton JL.
Arthroplasty of ankle and knee. In: Canale ST,
editor. Campbell’s operative orthopaedics. 10th
ed. St. Louis: Mosby-Year Book; 2003:255.
Reprinted with permission.)
2799
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

maltracking, and preservation of themedial vascular supply to the patella63.The technique may be difficult, how-ever, in heavier patients or those withscarring, contractures, or largeosteophytes.
Patellofemoral stability may beassessed with use of either the no-thumbs test or the single-suture tech-nique. The patella should track centrallyin the trochlear groove without lateralsubluxation or lateral tilt through a fullrange of motion. Ideally, these testsshould be performed with the tourni-quet deflated, as binding of the extensormechanism may lead to perceived mal-tracking of the patellar component.With the no-thumbs test, the knee istaken through the full flexion arc with-out closing the medial arthrotomy andwithout applying any medial force with
the thumb to keep the patella located. Ifthere is patellar tilting or slight sublux-ation with the no-thumbs test, thesingle-suture technique can be used,thus avoiding an unnecessary lateralrelease. With the single-suture tech-nique, the medial tension vector of theextensor mechanism is simulated byreapproximating the medial retinacu-lum at the superior pole of the patellawith a single number-0 suture. If thesuture does not break through a fullrange of flexion of the knee, then alateral release is not necessary.
Lateral retinacular release iscommonly used to correct maltrackingof the extensor mechanism47. The tightretinaculum is released approximately 2cm lateral to the lateral patellar border,with the release extending from thevastus lateralis muscle to the proximal
part of the tibia. Care should be taken topreserve the superior lateral geniculateartery. There are numerous possiblecomplications of lateral retinacular re-lease, including substantial vascularcompromise (evident on a technetiumbone scan), osteonecrosis of the patella,patellar fracture, prolonged wound-healing and wound slough, an increasedrisk of infection, increased postopera-tive pain and swelling, and prolongedrehabilitation.
Patellar fracture has even beenshown to be more likely after lateralrelease, whether or not the superiorlateral geniculate artery is preserved.Mesh expansion release of the lateralretinaculum is an alternative to tradi-tional retinacular release, with the po-tential benefit of less disruption to thepatellar blood supply.
The results of total knee arthro-plasty for the treatment of isolatedpatellofemoral arthritis have been verygood and have included reliable painrelief. However, a high rate of residualpostoperative patellar tilt, asymmetri-cally resurfaced patellae, and residualsubluxation has been reported in theliterature46. These findings emphasizethe need to adhere to the technicalprinciples reviewed in this section toproperly handle the inherent complex-ity of these cases. Studies43-46 havedemonstrated good-to-excellent resultsin terms of pain relief, and these resultswere superior to those achieved incomparison groups in which total kneearthroplasties had been performed forother conditions. It should be pointedout that anterior knee pain in patientswith isolated patellofemoral arthritiswas greater than that in patients withtricompartmental arthritis. One mayview total knee replacement for arthro-sis of an isolated patellofemoral articu-lation as excessive; however, total kneearthroplasty currently remains the mostproven and predictable single proce-dure for this specific population ofolder patients with patellofemoraldisease43-46.
Future DirectionsIncreased interest and improvement incomputer-assisted navigation systems
Fig. 8
Lateral patellar subluxation of the patella on the left following total knee arthroplasty. Note the
lateral tilt of the patella on the right, a result of excessive resection of the lateral facet and too
little resection of the medial facet.
Fig. 7
Medialization of the femoral component may result in lateral
patellar subluxation (Reproduced, with modification, from:
Krackow KA. The technique of total knee arthroplasty. St.
Louis: CV Mosby; 1990. p 139. Reprinted with permission.)
2800
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

for total joint arthroplasty have thepotential to improve the accuracy ofcomponent alignment64-67. This mayreduce patellofemoral complica-tions66,67. It is important to note thatthere has not yet been any reportedimprovement in accuracy or variabilitywhen computer navigation, rather thanconventional techniques, has been usedfor the critical step of rotationallyaligning the femoral component in theoperating room67.
OverviewPatellofemoral arthritis is a commoncause of anterior knee pain. When thedisease is in its early stages, a careful andcomplete course of nonoperative treat-ment may provide sufficient pain reliefand functional improvement. If surgeryis required, limited soft-tissue proce-dures such as arthroscopic lateral re-lease and debridement may work well if
the lateral portion of the joint is pri-marily affected. Tibial tubercle transfer,particularly anteromedialization, is apowerful way to correct malalignmentand offload the lateral and distal parts ofthe patella. The indications for tibialtubercle transfer may expand if it provesto be a successful adjunct to cartilageresurfacing procedures.
For more severe disease, patello-femoral arthroplasty has evolved into asafe and reliable alternative. When apatient is older or when the arthritis ismore diffuse, total knee arthroplasty is areliable and reproducible way to im-prove function and decrease pain. Caremust be taken to properly positioncomponents to avoid problems with thepatellar component after the surgery.
William M. Mihalko, MD, PhDYaw Boachie-Adjei, MDKhaled J. Saleh, MD, MSc(Epid), FRCSC
Department of Orthopaedic Surgery(W.M.M. and Y.B.-A.), Department ofMechanical and Aerospace Engineering(W.M.M.), and Division of AdultReconstruction (K.J.S.), University of Virginia,P.O. Box 800159, Charlottesville, VA 22908-0159. E-mail address for W.M. Mihalko:[email protected]. E-mail address forY. Boachie-Adjei: [email protected] address for K.J. Saleh:[email protected]
Jeffrey T. Spang, MDUniversity of Connecticut Health Center, 263Farmington Avenue, Farmington, CT 06030
John P. Fulkerson, MDOrthopaedic Associates, 499 FarmingtonAvenue, Farmington, CT 06032
Elizabeth A. Arendt, MDDepartment of Orthopaedic Surgery,University of Minnesota, 2450 RiversideAvenue South, Suite 200, Minneapolis, MN55454
References
1. Amis AA, Senavongse W, Darcy P.Biomechanics of patellofemoral joint prostheses.Clin Orthop Relat Res. 2005;436:20-9.
2. Saleh KJ, Arendt EA, Eldridge J, Fulkerson JP,Minas T, Mulhall KJ. Operative treatment ofpatellofemoral arthritis. J Bone Joint Surg Am.2005;87:659-71.
3. Kwak SD, Colman WW, Ateshian GA, GrelsamerRP, Henry JH, Mow VC. Anatomy of the humanpatellofemoral joint articular cartilage: surfacecurvature analysis. J Orthop Res. 1997;15:468-72.
4. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. 1.Functional anatomy of the patello-femoral joint.J Bone Joint Surg Br. 1976;58:287-90.
5. Amis AA, Farahmand F. Biomechanics of theknee extensor mechanism. Knee. 1996;3:73-81.
6. Grelsamer RP, Weinstein CH. Appliedbiomechanics of the patella. Clin Orthop Relat Res.2001;389:9-14.
7. Scuderi GR, editor. The patella. New York:Springer; 1995. p 74.
8. Huberti HH, Hayes WC. Patellofemoral contactpressures. The influence of q-angle andtendafemoral contact. J Bone Joint Surg Am.1984;66:715-24.
9. Insall JN, Scott WN. Surgery of the knee. 3rd ed.Philadelphia: Churchill Livingstone; 2001. p 161.
10. Freeman BL III. Recurrent dislocations. In:Crenshaw AH, editor. Campbell’s operativeorthopaedics. 7th ed. St. Louis: CV Mosby; 1987. p2173-218.
11. Aglietti P, Insall JN, Cerulli G. Patellar pain andincongruence. I. Measurements of incongruence.Clin Orthop Relat Res. 1983;176:217-24.
12. Hughston JC. Subluxation of the patella.J Bone Joint Surg Am. 1968;50:1003-26.
13. Scuderi GR. Surgical treatment for patellarinstability. Orthop Clin North Am. 1992;23:619-30.
14. Kolowich PA, Paulos LE, Rosenberg TD,Farnsworth S. Lateral release of the patella:indications and contraindications. Am J SportsMed. 1990;18:359-65.
15. Fairbank HA. Internal derangement of theknee in children. Proc R Soc London. 1937;3:11.
16. Yercan H, Ait Si Selmi T, Neyret P. Thetreatment of patellofemoral osteoarthritis withpartial lateral facetectomy. Clin Orthop Relat Res.2005;436:14-9.
17. Fulkerson JP. Alternatives to patellofemoralarthroplasty. Clin Orthop Relat Res. 2005;436:76-80.
18. Hughston JC, Walsh WM. Proximal and distalreconstruction of the extensor mechanism forpatellar subluxation. Clin Orthop Relat Res.1979;144:36-42.
19. Insall J, Bullough PG, Burstein AH. Proximal‘‘tube’’ realignment of the patella forchondromalacia patallae. Clin Orthop Relat Res.1979;144:63-9.
20. Scuderi G, Cuomo F, Scott WN. Lateral releaseand proximal realignment for patellar subluxationand dislocation. A long-term follow-up. J Bone JointSurg Am. 1988;70:856-61.
21. Fulkerson JP. Anteromedialization of the tibialtuberosity for patellofemoral malalignment. ClinOrthop Relat Res. 1983;177:176-81.
22. Pidoriano AJ, Weinstein RN, Buuck DA,Fulkerson JP. Correlation of patellar articularlesions with results from anteromedial tibial
tubercle transfer. Am J Sports Med. 1997;25:533-7.
23. Fithian DC, Meier SW. The case for advance-ment and repair of the medial patellofemoralligament in patients with recurrent patellarinstability. Oper Tech Sports Med. 1999;7:81-9.
24. Kelly MA, Griffin FM. Proximal realignment ofthe patellofemoral joint. Tech Orthop. 1997;12:178-84.
25. Maquet P. [A biomechanical treatment offemoro-patellar arthrosis: advancement of thepatellar tendon]. Rev Rhum. 1963;30:779. French.
26. Engebretsen L, Svenningsen S, Benum P.Advancement of the tibial tuberosity for patellarpain. A 5-year follow-up. Acta Orthop Scand.1989;60:20-2.
27. Post WR, Fulkerson IP. Distal realignment ofthe patellofemoral joint: indications, effects,results, and recommendations. Orthop Clin NorthAm. 1992;23:631-43.
28. Carney JR, Mologne TS, Muldoon M, Cox JS.Long-term evaluation of the Roux-Elmslie-Trillatprocedure for patellar instability: a 26-year follow-up. Am J Sports Med. 2005;33:1220-3.
29. Shelbourne KD, Porter DA, Rozzi W. Use of amodified Elmslie-Trillat procedure to improveabnormal patellar congruence angle. Am J SportsMed. 1994;22:318-23.
30. Cox JS. An evaluation of the Elmslie-Trillatprocedure for management of patellar dislocationsand subluxations: a preliminary report. Am J SportsMed. 1976;4:72-7.
31. Brown DE, Alexander AH, Lichtman DM. TheElmslie-Trillat procedure: evaluation in patellardislocation and subluxation. Am J Sports Med.1984;12:104-9.
2801
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S

32. Fulkerson JP, Becker GJ. Anteromedial tibialtubercle transfer without bone graft. Am J SportsMed. 1990;18:490-7.
33. Sakai N, Koshino T, Okamoto R. Painreduction after anteromedial displacement of thetibial tuberosity: 5-year follow-up in 21 knees withpatellofemoral arthrosis. Acta Orthop Scand.1996;67:13-5.
34. Morshuis WJ, Pavlov PW, de Rooy KP.Anteromedialization of the tibial tuberosity in thetreatment of patellofemoral pain and malalignment.Clin Orthop Relat Res. 1990;255:242-50.
35. Minas T, Bryant T. The role of autologouschondrocyte implantation in the patellofemoraljoint. Clin Orthop Relat Res. 2005;436:30-9.
36. Peterson L, Brittberg M, Kiviranta I, AkerlundEL, Lindahl A. Autologous chondrocytetransplantation. Biomechanics and long-termdurability. Am J Sports Med. 2002;30:2-12.
37. Ackroyd CE, Polyzoides AJ. Patellectomy forosteoarthritis. A study of eighty-one patientsfollowed from two to twenty-two years. J Bone JointSurg Br. 1978;60:353-7.
38. Argenson JN, Guillaume JM, Aubaniac JM. Isthere a place for patellofemoral arthroplasty? ClinOrthop Relat Res. 1995;321:162-7.
39. Tauro B, Ackroyd CE, Newman JH, Shah NA.The Lubinus patellofemoral arthroplasty. A five- toten-year prospective study. J Bone Joint Surg Br.2001;83:696-701. Erratum in: J Bone Joint SurgBr. 2002;84:308.
40. Ackroyd CE, Newman JH. The Avon patello-femoral arthroplasty—development and earlyresults. J Bone Joint Surg Br. 2001;83 SupplII:146-7.
41. Ackroyd CE, Newman JH. The Avonpatellofemoral arthroplasty: two to five yearresults. J Bone Joint Surg Br. 2003;85 SupplII:162-3.
42. Ackroyd CE, Newman JH, Evans R, Eldridge JD,Joslin CC. The Avon patellofemoral arthroplasty:five-year survivorship and functional results. J BoneJoint Surg Br. 2007;89:310-5.
43. Thompson NW, Ruiz AL, Breslin E, BeverlandDE. Total knee arthroplasty without patellarresurfacing in isolated patellofemoralosteoarthritis. J Arthroplasty. 2001;16:607-12.
44. Laskin RS, van Steijn M. Total kneereplacement for patients with patellofemoralarthritis. Clin Orthop Relat Res. 1999;367:89-95.
45. Parvizi J, Stuart MJ, Pagnano MW, HanssenAD. Total knee arthroplasty in patients withisolated patellofemoral arthritis. Clin Orthop RelatRes. 2001;392:147-52.
46. Mont M, Haas S, Mullick T, Hungerford D.Total knee arthroplasty for patellofemoral arthritis.J Bone Joint Surg Br. 2002;84:1977-81.
47. Laskin RS. Lateral release rates after totalknee arthroplasty. Clin Orthop Relat Res.2001;392:88-93.
48. Lewonowski K, Dorr LD, McPherson EJ, HuberG, Wan Z. Medialization of the patella in total kneearthroplasty. J Arthroplasty. 1997;12:161-7.
49. Malo M, Vince KG. The unstable patella aftertotal knee arthroplasty: etiology, prevention, andmanagement. J Am Acad Orthop Surg. 2003;11:364-71.
50. Lonner JH, Lotke PA. Aseptic complicationsafter total knee arthroplasty. J Am Acad OrthopSurg. 1999;7:311-24.
51. Berger RA, Crossett LS, Jacobs JJ, Rubash HE.Malrotation causing patellofemoral complicationsafter total knee arthroplasty. Clin Orthop RelatRes. 1998;356:144-53.
52. Berger RA, Rubash HE, Seel MJ, ThompsonWH, Crossett LS. Determining the rotationalalignment of the femoral component in total kneearthroplasty using the epicondylar axis. Clin OrthopRelat Res. 1993;286:40-7.
53. Merkow RL, Soudry M, Insall JN. Patellardislocation following total knee replacement. JBone Joint Surg Am. 1985;67:1321-7.
54. Krackow KA. The technique of total kneearthroplasty. St. Louis: CV Mosby; 1990. p 139.
55. Whiteside LA, Arima J. The anteroposterioraxis for femoral rotational alignment in valgus totalknee arthroplasty. Clin Orthop Relat Res.1995;321:168-72.
56. Nagamine R, Whiteside LA, Otani T, White SE,McCarthy DS. Effect of medial displacement of thetibial tubercle on patellar position after rotationalmalposition of the femoral component in total kneearthroplasty. J Arthroplasty. 1996;11:104-10.
57. Anouchi YS, Whiteside LA, Kaiser AD, MillianoMT. The effects of axial rotational alignment of thefemoral component on knee stability and patellartracking in total knee arthroplasty demonstratedon autopsy specimens. Clin Orthop Relat Res.1993;287:170-7.
58. Bourne RB, Burnett RS. The consequences ofnot resurfacing the patella. Clin Orthop Relat Res.2004;428:166-9.
59. Forster MC. Patellar resurfacing in total kneearthroplasty for osteoarthritis: a systematicreview. Knee. 2004;11:427-30.
60. Holt GE, Dennis DA. The role of patellarresurfacing in total knee arthroplasty. Clin OrthopRelat Res. 2003;416:76-83.
61. Feller JA, Bartlett RJ, Lang DM. Patellarresurfacing versus retention in total kneearthroplasty. J Bone Joint Surg Br. 1996;78:226-8.
62. Mihalko W, Fishkin Z, Krackow K.Patellofemoral overstuff and its relationship toflexion after total knee arthroplasty. Clin OrthopRelat Res. 2006;449:283-7.
63. Matsueda M, Gustilo RB. Subvastus andmedial parapatellar approaches in total kneearthroplasty. Clin Orthop Relat Res.2000;371:161-8.
64. Stulberg SD, Loan P, Sarin V. Computer-assisted navigation in total knee replacement:results of an initial experience in thirty-fivepatients. J Bone Joint Surg Am. 2002;84 Suppl2:90-8.
65. Victor J, Hoste D. Image-based computer-assisted total knee arthroplasty leads to lowervariability in coronal alignment. Clin Orthop RelatRes. 2004;428:131-9.
66. Bathis H, Perlick L, Tingart M, Luring C,Zurakowski D, Grifka J. Alignment in total kneearthroplasty. A comparison of computer-assistedsurgery with the conventional technique. J BoneJoint Surg Br. 2004;86:682-7.
67. Haaker RG, Stockheim M, Kamp M, Proff G,Breitenfelder J, Ottersbach A. Computer-assistednavigation increases precision of componentplacement in total knee arthroplasty. Clin OrthopRelat Res. 2005;433:152-9.
2802
TH E JO U R N A L O F BO N E & JO I N T SU R G E R Y d J B J S .O R G
VO L U M E 89-A d NU M B E R 12 d D E C E M B E R 2007
CO N T R O V E R S I E S A N D TE C H N I Q U E S I N T H E S U R G I C A L
MA N A G E M E N T O F PA T E L L O F E M O R A L A R T H R I T I S