Embed Size (px)
Citation preview

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 1/100
Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 943
_____________________________ _____________________________
Controlling Iodine
Deficiency Disorders
Studies for Program Management in Sub-Saharan Africa
BY
STEFAN PETERSON
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2000

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 2/100
Dissertation for the Degree of Doctor of Medical Science in Pediatrics presented atUppsala University in 2000.
ABSTRACT
Peterson, S. 2000. Controlling Iodine Deficiency Disorders - Studies for Program Management in Sub-Saharan Africa. Acta Universitatis Upsaliensis,Comprehensive Summaries of Uppsala Dissertations from the Faculty of
Medicine 943. 100 pp. Uppsala. ISBN. 91-554-4774-0.
Studies were performed to improve iodine deficiency control programs. Goitrerates and cassava processing practices were compared in three Central AfricanRepublic (CAR) populations. Short-cuts in cassava processing were associatedwith elevated urinary thiocyanate and increased goitre rates, suggesting agoitrogenic effect in one population. While improved cassava processing may bebeneficial, the priority is to correct the iodine deficiency.
The use of the urinary iodine/tiocyanate ratio as indicator of goitrogeniceffects was explored using data from Tanzania and CAR. As the ratio can be
calculated in four mathematically different ways and has physiologicalshortcomings, its use is discouraged.Biannual iodised oil capsule (IOC) distribution in a Tanzanian population
of 7 million during nine years was studied. Mean distribution coverage was 64%,mean delay of subsequent distribution 1.25 years, and only 43% of targetedperson-time was covered. The cost of capsules constituted more than 90% of total program costs. It is cost-effective to invest more funds in communication,support of peripheral staff and supervision.
In a highland Tanzanian village, salt iodine content was highly variablecompared to national standards. While school-children had adequate urinaryiodine, women at delivery and newborns showed signs of inadequate iodinestatus. Salt iodine concentrations should be monitored during production anddistribution down to household level, and iodine status assessed in all vulnerablegroups before adjusting recommended salt iodization levels at production.
WHO’s 1994 change in palpation goitre definition considerably loweredspecificity and increased measured goitre rates by 25% in Tanzanian school-children compared to the previous system. Ultrasound estimation of thyroidvolume under rugged field conditions requires considerable human and materialresources yet had a precision only slightly better than palpation. In resourcepoor settings appropriately trained palpators using the 1960 WHO definition of goitre remain optimal for estimating thyroid size until precision and cost of
ultrasound has improved.Monitoring of process indicators needs to be an ongoing priority activity,separate from periodic evaluations of impact.
Key words: Iodine deficiency, iodized oil, cassava, thiocyanate, iodized salt, cost-effectiveness, epidemiology, monitoring.
Stefan Peterson, Dept of Women’s and Children’s Health, Section for International
Maternal and Child Health, Uppsala University, SE-751 85 Uppsala, Sweden, and
the Dept of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden
© Stefan Peterson 2000ISSN 0282-7476ISBN 91-554-4774-0Printed in Sweden by University Printers, Uppsala 2000

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 3/100
“Iodine deficiency is so easy to preventthat it is a crime to let a single child be born mentally
handicapped for that reason.”
Labouisse, UNICEF
“We were striving for the best, but it turned out as usual.”
Victor Chernomyrdin, Former Prime Minister of Russia
This study is dedicated to the millions of people still affected byIDD and the people working to reduce these disorders

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 4/100
Stefan Peterson
PAPERS INCLUDED IN THE THESIS
This thesis is based on the following papers, which will be referred to by theirRoman numerals:
I. Peterson S, Légué F, Tylleskär T, Kpizingui E, Rosling H. Improved cassava-processing can help reduce iodine deficiency disorders in the Central AfricanRepublic. Nutrition Research 1995;15(6):803-812.
II. Peterson S, Rosling H, Tylleskär T, Gebre-Medhin M, Taube A. EndemicGoitre in Guinea [Limitations of urinary iodine / thiocyanate ratios asindicator of antithyroid effect in population studies]. Lancet 1995; 345
(February 25):513-514.
III. Peterson S, Assey V, Forsberg B, Greiner T, Kavishe F, Mduma B, Rosling H,Sanga A, Gebre-Medhin M. Coverage and cost of iodised oil capsuledistribution in Tanzania. Health Policy and Planning, 1999; 14: 390-399,
IV. Sundqvist J, Wijetunga M, Assey V, Gebre-Medhin M, Peterson S. Saltiodation and risk of neonatal brain damage. Lancet 1998; 352 (July 4):34-35.
V. Peterson S, Sanga A, Eklöf H, Bunga B, Taube A, Gebre-Medhin M,
Rosling H. Thyroid Size Classification by Palpation and Ultrasound inField Surveys. Lancet 2000; 355 (January 8): 106-110. Addendum in
Lancet 2000; 355, (June 3):1995-1997
Offprints were made with permission from the journals.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 5/100
Controlling IDD – Studies for Program Management
CONTENTS
ABBREVIATIONS...... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... ... .... .... .... .... .... .... ... .... .... .... .... .... .6
INTRODUCTION......................................................................................................................7
IODINE PHYSIOLOGY ................................................................................................................7IODINE DEFICIENCY DISORDERS ...............................................................................................9
Goitrogens .........................................................................................................................11
IODINE STATUS INDICATORS ...................................................................................................15Thyroid size.......................................................................................................................15
Urinary iodine ...................................................................................................................18
Hormones ....... .... .... .... ........... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ........... .... .... ....... 20
IODINE SUPPLEMENTATION.....................................................................................................22 Iodized oil ....... .... .... .... ........... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ........... .... .... .... ... 23
Iodized salt .... .... .... .... .... .... .... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ........... .... .... .... ... 26 Iodization of water, sugar, and other vehicles .... .... .... ........... .... .... .... .... ........... .... .... .... ....... 31
Excess iodine intake .... ........... .... .... .... ........... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ... 33
CONTROLLING IODINE DEFICIENCY DISORDERS.......................................................................34 Management structure and strategy .............. .... .... .... .... ........... .... .... .... ........... .... .... .... .... ... 34
Assessing IDD.... .... .... .... .... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ... 36
Communication..................................................................................................................37
Plan of action & Achievement of political will.... .... .... .... .... .... .... .... .... ........... .... .... .... .... ....... 38
Implementation..... .... .... .... .... .... .... .... .... .... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ....... 38
Monitoring and Evaluation......... .... ........... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ....... 38
IDD IN SUB-S AHARAN A FRICA .................................................................................................39Central African Republic.....................................................................................................39
Mainland Tanzania .... .... .... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ... 40 AIM OF THE STUDIES.. .... .... .... .... .... .... .... .... .... .... .... .... .... .... ... .... .... .... .... .... ... .... .... .... .... .... ... 44
MATERIALS, METHODS, RESULTS, AND COMMENTS ........ ........ ........ ........ ........ ........ ....45
A SSESSING IODINE DEFICIENCY AND GOITROGENIC EFFECTS (PAPER I,II).................................45DISTRIBUTING IODINE (PAPER III)............................................................................................51E VALUATING PROGRAM IMPACT (PAPER IV,V) ..........................................................................57
GENERAL DISCUSSION .......................................................................................................65
ELIMINATION, NOT ERADICATION ............................................................................................65MONITORING DOES NOT EQUAL E VALUATION ..........................................................................68
Defining the implementation process.. .... .... .... .... .... .... .... ........... .... .... .... ........... .... .... .... .... ... 69
Monitoring.... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ... 71
Evaluation .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... ........... .... .... .... .... ........... .... .... .... ... 71
Modifying the “Social Wheel” .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... .... ........... .... .... .... .... ... 73
REASSESSING THE SITUATION.................................................................................................76The strategy.......................................................................................................................76
The impact on IDD.............................................................................................................77
The management structure.................................................................................................78
CONCLUSIONS......................................................................................................................81
ACKNOWLEDGEMENTS ....... .... .... .... .... .... .... ... .... .... .... .... .... ... .... .... .... .... .... .... ... .... .... .... .... ... 84
REFERENCES ........................................................................................................................86

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 6/100
Stefan Peterson
6
ABBREVIATIONS
CAR Central African RepublicICCIDD International Council for the Control of Iodine
Deficiency DisordersID Iodine deficiencyIDD Iodine deficiency disordersIIH Iodine induced hyperthyroidismI/SCN Iodine / Thiocyanate ratioIOC Iodized oil capsuleI-salt Iodized saltMIS Management information systemNCCIDD National Council for the Control of Iodine Deficiency
DisordersNFCC National Food Control CommissionPHC Primary Health CarePPM Parts per million, corresponds to a concentration of 1
mg per kgSCN Thiocyanate
T3 TriiodothyronineT4 ThyroxineTBG Thyroxine-binding globulinTFNC Tanzania Food and Nutrition CentreTg ThyroglobulinTRH Thyrotropin-releasing hormoneTSH Thyroid stimulating hormoneUNICEF United Nations Children’s FundUSD United States dollar
WHO World Health Organization
Iodine terminology:Iodize To add iodine, iodide or iodate to e.g. saltIodine The elemental atom form of iodineIodide Ion form of iodine, added as potassium iodide (KI)
Iodate Oxidized ion form of iodine, added as potassiumiodate (KIO3)

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 7/100
Controlling IDD – Studies for Program Management
7
INTRODUCTION
Iodine Deficiency Disorders (IDD) are a range of health problemsand goiter is the visible "marker condition" for more severedisorders. IDD control program activity has increased since theWorld Health Assembly’s endorsement of the objective of eliminating IDD by the year 2000 (WHO 1992) and the WorldDevelopment Report’s conclusion that iodine supplementation isone of the interventions "...that would have the highest cost-effectiveness of any health intervention available in the worldtoday" (World Bank 1993). Iodine supplementation programs
have started in 90 out of 94 IDD affected developing countries(UNICEF 1995). Several interventions with proven high efficacyare being used. Iodized salt is the main method to combat IDDfor long-term control and iodized oil capsules (IOC) acomplementary method in areas where iodization of salt fordifferent reasons cannot be implemented or fails to succeed.
Intensive implementation activities have revealed thelimited knowledge of how to translate efficacious interventionsinto effective programs with relevant mechanisms for programmonitoring, quality assurance, and impact evaluation. This
thesis reports studies of the iodine supplementation program inTanzania −one of the most developed control programs in Africa− and the early stage of the program in the Central AfricanRepublic with goitrogens as a policy issue. Collaboratinginstitutions are the Tanzania Food and Nutrition Center (TFNC)and the Ministère de Santé Publique, Service de Lutte contre lesGrandes Éndemies, Central African Republic.
Iodine PhysiologyIodine is essential for normal growth, development, andfunctioning of the body. Since only minute amounts are requiredeach day, it is known as a micronutrient. Iodine is required forsynthesis of the thyroid hormones, thyroxine (T4) andtriiodothyronine (T3), which are necessary for the regulation of body metabolism (Hetzel 1989).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 8/100
Stefan Peterson
8
The recommended daily iodine intake is 50 g for infants(<12 months), 90 g for children up to the age of 6 years, 120 gfor children 7-12 years old, 150 g for adolescents and adults, and
200 g for pregnant and lactating women (WHO 1996). The adulthuman body contains 20-50 mg of iodine, of which 70-80% arestored in the thyroid gland, a remarkable concentration (Hetzel1989).
In stable iodine intake situations, the amount of iodineexcreted in the urine correlates well with the iodine intake andserves as an estimate of iodine intake. Less than 10% of humaniodine losses are excreted in the faeces (Choufoer et al. 1963),sweat (Mao et al. 1990), and milk (Vermiglio et al. 1992).
The stomach and the upper small intestine rapidly absorbiodine as either one of two chemical forms: iodide or iodate.Iodate is reduced to iodide, which is transported in the blood tothe thyroid gland, where an active transport mechanism pumps itinto the thyroid cell. About 60 g of iodine needs to be trappedper day to maintain an adequate thyroxin level; the efficiency of the trapping mechanism is regulated with the help of TSHdepending on the availability of iodine and the gland’s activity. Inthe gland, iodide is oxidized to iodine, which is bound to tyrosineto form mono- and diiodotyrosine. These are coupled to form
trioodothyronine (T3) and thyroxin (T4) in the thyroid epithelialcells. Thyroxin is then stored in colloid follicles bound tothyroglobulin. When needed, the thyroid stimulating hormone(TSH) will stimulate the proteolysis of thyroglobulin in thethyroid cells to release thyroxin into the blood stream (Hetzel1989; Passmore & Eastwood 1986).
A feedback system regulates iodine metabolism by using thehypothalamic hormone and the thyrotropin-releasing hormone(TRH), which modulates the secretion of TSH from the
hypothalamus. The level of thyroxine (T4) in the blood regulatesmetabolism. Decreasing T4 levels lead to increasing TSH levels,which serve to increase thyroid iodine uptake as well as theproduction and release of more T4 and triiodothyronine (T3) intothe bloodstream. At high TSH levels the thyroid willpreferentially produce the biologically more active T3.Conversely, as thyroid hormone levels rise, TSH secretion falls.Sustained high TSH levels stimulate an increase in the size andnumber of follicular cells, an increase in vascularization, and

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 9/100
Controlling IDD – Studies for Program Management
9
consequently thyroid hypertrophy which leads to better iodinecapture. At some stage of hypertrophy the thyroid is regarded a“goitre”. In addition, persistent stimulation may also cause the
formation of thyroid nodules (Hetzel 1989).Thyroid hormones regulate the metabolism of target organs
by entering the cells of the peripheral tissues and bindngi to thenuclear chromatin via a thyroid hormone receptor protein, whichin turn affects transcription (Baniahmad et al. 1992). T3 is muchmore potent than T4. Thyroxin is therefore generally transformedto T3 prior to biological action with the help of the seleniumcontaining enzyme 5’deiodinase (Kohrle 1999). This couldexplain links between iodine and selenium deficiency
(Anonymous 1993; Thilly et al. 1991; Untoro et al. 1999). A recentpaper suggests that concurrent iron deficiency anaemia impairsthe therapeutic response to iodine supplementation, possiblymediated via decreased T4 to T3 conversion or through decreasedthyroxiperidase activity impairing iodide organification(Zimmerman et al. 2000).
Iodine Deficiency Disorders
Iodine was originally present in all soils. However, rainfall,glaciation, exposure to wind and floods has leached the soils of iodine, especially in mountainous areas and in flood plains. Although some iodine is returned to the soil by rain, this isinsufficient and soils remain iodine deficient (Hetzel & Pandav1996). Foods and animals grown on such soils will be iodine-deficient. The only rich source of iodine is seafood. If seafood iseaten one to two times per week it provides sufficient iodineintake (Passmore & Eastwood 1986). Iodine-containing animal
feeds and antiseptics commonly used in the dairy industry resultin iodine rich milk which is an important source of iodine inmany countries (Phillips 1997). However, food alone is generallynot sufficient to give an adequate iodine intake.
The body’s first reaction to low iodine intake is to increasethe uptake efficiency up to four times the normal rate in order tomaintain the output of thyroxine. This is evidenced by areduction in urinary iodine concentrations. If this adaptation is

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 10/100
Stefan Peterson
10
insufficient, then serum TSH will rise and T4 will fall. Thepreferential production of the more potent T3 over T4 increasesthe efficiency of the use of the available iodine. Only when these
compensatory mechanisms are exhausted will hypothyroidismoccur as thyroxine levels fall below acceptable levels (Hetzel1989).
The term iodine deficiency disorders (IDD) covers a widespectrum of clinical conditions (Hetzel 1983). Some disorders arethe result of compensation mechanisms, such as thyroidenlargement, goiter. Early abortions, stillbirths, increasedperinatal and infant mortality, and mental and growthretardation are some of the other manifestations of iodine
deficiency (Lamberg 1991). Some disorders are associated withpermanent brain damage that occurs during the first twotrimesters of pregnancy (Cao et al. 1994a; Hetzel & Mano 1989;Pharoah & Connolly 1987). The resulting clinical condition,cretinism, is irreversible and it is the most severe and dramaticmanifestation of IDD. However, IDD also include a range of moresubtle brain damages (Stanbury 1994). Iodine supplementationhas been shown to increase iodine deficient children’sintelligence quotient considerably, indicating the suppressiveeffect of continued iodine deficiency (Bleichrodt & Born 1994).
Global estimates of the number of subjects affected by some of the IDD conditions are given in Table 1, (UNICEF 1994b; WHO1999).
Table 1. Global burden of Iodine Deficiency Disorders.
Total population at risk 2.200 million
Subjects with goiter 740 millionSubjects with lowered mental ability 300 millionCretinism 5.7 million
The effects of iodine deficiency on the foetus and neonatealso include increased perinatal and infant mortality (Cobra et al.1997; DeLong et al. 1997; Hetzel 1989; Pharoah et al. 1976). A sign of iodine deficiency in this period is neonatalhypothyroidism. The incidence rate in iodine deficient areas may

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 11/100
Controlling IDD – Studies for Program Management
11
reach up to 1/10, compared to 1/4000 in non-iodine deficientareas (Ermans et al. 1980a; Kochupillai 1992; Kochupillai &Pandav 1987). Even transient hypothyroidism in the neonatal
period has been shown to lead to permanent detrimental effectson a child’s intelligence (Calaciura et al. 1995).
During a child’s school-age years, iodine deficiency is animpediment to proper brain functioning, estimated to be 13.5intelligence quotient points (Bleichrodt & Born 1994). However,the most obvious sign of IDD in this period is thyroidenlargement, goiter. Goiter prevalence rates of 85% and higherhave been found in severely iodine deficient areas (Clugston et al.1987; Eltom et al. 1984). As a sign of hypothyroidism, TSH levels
are elevated in large portions of the school aged group (Moreno-Reyes et al. 1993). In adults widespread goiter, hypothyroidism,and reproductive failures contribute to significant humansuffering and economic underdevelopment (Hetzel 1989; Hetzel &Pandav 1996).
All the effects of iodine deficiency, encompassed by theconcept of IDD, are preventable by increasing the intake of iodine(Burgi et al. 1990). This not only reduces human suffering, but italso brings considerable benefits in terms of improved humanand economic development (Li & Wang 1987) and reductions inmedical care costs (Gutekunst 1993).
GoitrogensWhile Iodine Deficiency Disorders (IDD) are primarily caused byinsufficient dietary intake of iodine, other substances referred toas goitrogens have been suggested to interfere with the properfunctioning of thyroid hormone synthesis and utilization. Manysubstances have been proposed as potential goitrogens of publichealth importance but it has been difficult to confirm or reject
these hypotheses or to estimate the importance of a goitrogeniceffect in any one population.The pseudo-halide ion thiocyanate (SCNΓ) interferes with
the thyroid gland’s uptake and metabolism of iodine throughcompetitive inhibition (Gaitan 1990; Thilly 1992). SCN is formedin the body from glycosides in cabbage, or when cyanide fromtobacco smoking or from cyanogenic substances in insufficientlyprocessed cassava is detoxified to SCN during metabolism

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 12/100
Stefan Peterson
12
(Bourdoux et al. 1978; Chanoine et al. 1991; Hegedüs et al. 1985).Cassava, a staple for 500 million people, contains naturallyoccurring cyanogenic glycosides. To avoid cyanide exposure from
consumption of roots from bitter cassava varieties, effectiveprocessing methods were developed thousands of years ago(Rosling 1988). In Africa, the main steps in the most commonprocessing methods are soaking the root in water (O'Brien et al.1992), fermenting the grated pulp of the root in sacks, orprolonged drying of the root in the sun (Hahn 1989; Mlingi et al.1992). Cell disintegration during processing brings anendogenous enzyme in contact with cyanogenic glycosides thatbreak down into cyanohydrins which rapidly yield volatile
hydrogen cyanide at pH levels above 6 (Cooke & Maduagwu1978). However, insufficiently processed bitter roots may containconsiderable amounts of cyanogenic glycosides and cyanohydrinsthat after ingestion may break down and result in significantcyanide exposure (Casadei et al. 1990; Mlingi et al. 1992; O'Brien et al. 1992; Tylleskär 1994; Tylleskär et al. 1992). In the humanbody most of the cyanide will be enzymatically converted tothiocyanate, which at physiological levels is slowly excreted inthe urine. The implication of thiocyanate in IDD has led to callsto reduce cassava consumption (Biassoni et al. 1991; Biassoni et
al. 1990a; Biassoni et al. 1990b; Biassoni et al. 1998). Yet, otherobservations suggest that with adequate iodine intake overthypothyroidism or goiter will not develop in the presence of highthiocyanate loads (Cliff et al. 1986b; Delange et al. 1994).
The urinary I/SCN ratio (calculated as µg/mg) of a populationsample has been recommended as an indicator of the combinedeffect on the thyroid of low iodine intake and high thiocyanateexposure. Endemic goiter has been found to occur in cassava-eating populations in Zaire when the mean ratio is less than 3,
and cretinism has been found to occur when the mean ratio isless than 2 (Hennart et al. 1982). However, this ratio has notbeen validated with stronger study designs, nor have theprogrammatic implications for IDD control programs of elevatedthiocyanate loads been drawn beyond the drastic proposal toreplace cassava as a staple crop.
Another foodstuff for which goitrogenic effects have beenpostulated is millet (Anonymous 1983; Elnour et al. 1998;Moreno-Reyes et al. 1993). The goitrogenic effects of millet

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 13/100
Controlling IDD – Studies for Program Management
13
cannot be overcome by increased intake of iodine (Gaitan & Dunn1992). High mineral content and bacterial contamination of water may also be goitrogenic. Prolonged boiling inactivates this
effect (El Mahdi et al. 1986; Gaitan 1990). An association has alsobeen found between malnutrition and development of goitrewhich may indicate an enhancement of the effect of goitrogens(Gaitan 1990).
Analysing urinary thiocyanateTo assess the possible goitrogenic effects of thiocyanate (SCN)casual urine samples collected for iodine concentration analysisare typically analyzed also for their thiocyanate concentrations.
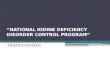
For this procedure a conservant (10% thymol in isopropanol) isadded and refrigeration is recommended. Larger urine volumesare also necessary, as another 0.5 ml are needed for the analysis(Lundquist et al. 1979). Thiocyanate values in Swedish non-cassava eating non-smokers is around 40 mol/l (0.23 mg/dl)(Lundquist et al. 1979) and SCN values of 52 mol/l (0.3 mg/dl)were found in a Brussels population (Lagasse et al. 1982). Unitconversions scales with indicators of levels of abnormality aregiven in Figure 1.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 14/100
Stefan Peterson
14
Figure 1. Unit conversion scales for Iodine (I) and Thiocyanate (SCN)concentrations in urine with indications of different levels of abnormality.
0 0
100
,2
200
300
,4
400,6
500
600
,8
700
800
1
900
1,2
1000
S C N µ m o l / l
0
1,4
I µ m o l / l
0
1
2
4
2
6
3
8
10
4
12
14
5
16
18
High
Normal
Veryhigh
S C N m g / d l
20
I µ g / d
l
Adequate
Mild deficiency
Severedeficiency
Moderatedeficiency

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 15/100
Controlling IDD – Studies for Program Management
15
Iodine Status Indicators
Thyroid size
The size of the thyroid gland in a school-aged child reflects theseverity of iodine deficiency the child has experienced in theprevious years. The goiter rate in school-aged children hastherefore been the most frequently used indicator to assess thedegree of iodine-deficiency in a population (Delange et al. 1997;WHO 1994a). School-aged children also reflect a new cohort’sexposure to iodine deficiency in the last few years. Schoolchildrenaged 6-12 are often used to approximate the goiter rate in theirentire age group. While a school-based survey excludes childrensuffering from many of the severe complications of IDD such ascretinism and deafness, the goiter rate is deemed representativeas long as school attendance in the community is more than 50%(WHO 1994a).
When using the goitre rate to decide whether a population isto be considered iodine deficient or not the decision depends on:(1) the cut-off size at which the thyroid is considered to be a
goiter,(2) the precision of thyroid size estimates around that cut-off, and
(3) the prevalence of goiter in school-aged children at whichiodine deficiency disorders (IDD) are considered a publichealth problem.
Over the years several definitions of goiter have been used andthe acceptable prevalence has changed. In 1960, WHO defined agoiter as “a thyroid gland whose lateral lobes have a volumegreater than the terminal phalanxes of the thumbs of the personexamined” (Delange et al. 1986; DeMaeyer et al. 1979; Perez et al.1960). This allowed for a thyroid to be palpable, yet not to be
considered a goiter. It was not clear whether it was the combinedthyroid volume of both thyroid lobes that had to be larger thanthe combined volume of both thumbs, or whether it was sufficientthat one thyroid lobe was larger than that side’s thumb. Iodinedeficiency was defined as a public health problem when morethan 10% of school children had goiter (Delange et al. 1986;Hetzel 1988; Perez et al. 1960; Querido et al. 1974).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 16/100
Stefan Peterson
16
In 1994 WHO simplified goiter grading by reducing thenumber of goiter grades from four to two. However, the definitionof goiter was simultaneously changed to “an enlarged thyroid
that is palpable but not visible”. Although it may not have been aconscious decision the 1994 definition effectively caused allpalpable thyroids to be regarded as goiters, see Table 2. Inaddition, the goiter rate at which IDD is considered a publichealth problem was lowered from 10% to 5% (WHO 1994a).
Table 2. Simplified classification of goiter according to WHO 1994a.
Grade 0: No palpable or visible goitre.
Grade 1: A mass in the neck that is consistent with an enlargedthyroid that is palpable but not visible when the neck isin the normal position. It moves upward in the neck asthe subject swallows. Nodular alteration(s) can occureven when the thyroid is not visibly enlarged.
Grade 2: A swelling in the neck that is visible when the neck is in a
normal position and is consistent with an enlarged
thyroid when the neck is palpated
The two WHO classification systems and the effect of therevised definition of goiter are illustrated in Table 3. It is obviousthat the new goiter criterion entails a lowering of the threshold atwhich an individual thyroid is considered a goiter. Furthermore,at the population level the lowering of the acceptable goiter rateto 5% will label new populations as “iodine deficient.” No
comparative study on the effect of these changes nor on theprecision obtained in goiter surveys using WHO’s 1960 and 1994criteria for goiter diagnosis was found in the literature.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 17/100
Controlling IDD – Studies for Program Management
17
Table 3. WHO thyroid size classification systems of 1960 with 1986amendments (Delange et al. 1986; Perez et al. 1960) and the 1994 system(WHO 1994a). Shaded areas indicate the thyroid sizes diagnosed as “goiter”
with each system.
Goiter gradesCriteria for thyroid size estimation
WHO1960 WHO1994
Not palpable 0 0
Palpable lobes ≤ terminal phalanxes of subject’s thumbs
0 1
Palpable lobes > terminal phalanxes of subject’s thumbs
1A 1
Visible with neck extended 1B 1 Visible with head in normal position 2 2 Visible at a distance 3 2
The severity of iodine deficiency is judged by the Total GoiterRate, which is calculated as the number of children with goitersdivided by the total number of children examined. Table 4 givesthe benchmarks for grading iodine deficiency. Although goiter
rates can also be calculated for Visible Goiter (VGR: children withgrade 2 / No of children examined) or, in the old classification, forgoiter visible with the neck extended (VGR1B: 1B+2+3 / No of children examined) (Mutamba 1993), these indices have foundless widespread use in IDD program management.
Table 4. Epidemiological criteria for assessing the severity of iodine deficiencydisorders (IDD) based on the prevalence of goiter in school-age childrenaccording to WHO’s 1994 criteria (WHO 1994a).
Mild IDD ModerateIDD
Severe IDD
Total Goitre Rate(TGR)
5.0 - 19.9% 20.0 – 29.9% ∃30.0%

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 18/100
Stefan Peterson
18
The intra-observer (MacLennan et al. 1969) and inter-observer (Tonglet et al. 1994) variation of goiter classification bypalpation has been studied and found to be substantial. Some
interpretations of this has led to calls to discard palpation infavor of the more costly ultrasound estimation of thyroid volume(Gutekunst et al. 1986; Vitti et al. 1994; WHO 1994a; WHO &ICCIDD 1997). Others have argued that the variations observedreflect random misclassification and have little or no effect at thepopulation level, thus allowing continued reliance on palpation,(Anonymous 1994). The justification given by WHO for thechange from palpation to ultrasound is a personalcommunication by Dr R Gutekunst (WHO 1994a). However, the
presented supporting data do not allow determination of theconcordance between ultrasound and palpation, nor are theybased on the subsequently recommended thyroid volume cut-off values (WHO & ICCIDD 1997).
Studies on the precision of ultrasound estimation of thyroidvolume are generally conducted on only a few subjects, andreport intra and inter-measurer errors of 2-13% from not clearlydeducible statistical procedures (Foo et al. 1999; Özgen et al.1999; Vitti et al. 1994). The measurement errors reported fromultrasound estimation of thyroid volume are considerably lower
than errors for determining the volume of other organs such asthe kidney, where the standard deviation of the differencebetween repeated measurements divided by the mean volumeranges from 14-17% (Emamian et al. 1995). This suggests thatdifferent statistical techniques may have been used in thecalculation of the errors.
Urinary iodine
Most of the iodine absorbed is excreted in the urine makingurinary iodine content a good marker of current iodine status. Although 24-hour urine collection accurately determines theamount of iodine excreted, measuring urinary iodineconcentrations in casual morning urine samples yields anadequate assessment of whether a population is iodine deficientif at least 40-50 individuals are sampled (Dunn & van der Haar1990). In a school where 300 children may be examined forgoiter, a systematic sub-sample can be sampled for urine; that is,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 19/100
Controlling IDD – Studies for Program Management
19
every 6th child provides a urine sample. To more accuratelymeasure a population’s iodine status in an area a total sample of 200-300 samples is desirable. Collection of casual urine samples
is widely practiced because the sampling is acceptable to theresearch subjects, the volume required for most analysis methodsis small (1 ml), the iodine content remains stable, and thesamples do not require refrigeration (Benmiloud et al. 1994;Dunn & van der Haar 1990; WHO 1994a). An obvious weaknessof using casual urine samples is the error introduced fromvariations in urinary volumes between individual subjects andbetween different populations.
Using a ratio of urinary iodine and creatinine to compensate
for the lack of 24 hour urine collection has been foundunnecessary and potentially misleading, especially forindividuals who consume very little protein (Dunn et al. 1993;Dunn & van der Haar 1990; Furnée et al. 1994; WHO 1994a).
Historically iodine concentrations are given as µg/literinstead of µmol/liter (100 µg/l = 0.79 µmol/l), see Figure 1. Theanalytic procedure that examines iodine concentrations wasestablished by Sandell and Koltoff in 1937 (Sandell & Kolthoff 1937). The main methods used are still based on the reduction of ceric ammonium sulphate using arsenic containing acids andtimed readings in a colorimeter (Dunn et al. 1993; May et al.1997). Simpler manual methods for urinary iodine analysis arerelatively inexpensive at USD 0.50 - 1.00 per sample (WHO1994a). However, great care must be taken to avoidcontamination with iodine, which is found in household itemssuch as hair shampoo. The method requires special rooms,glassware, reagents, and quality control procedures in referencelaboratories (Dunn et al. 1993). While there have been attemptsto develop analytical methods based on other reactions (Rendl et
al. 1998), these have so far not been validated in the iodinedeficiency concentration range. Because a rapid field test is notyet available, transportation of samples to the laboratory andwaiting for the results is necessary.
The severity of iodine deficiency is determined using medianurinary iodine concentration values, see Table 5. Recently asuggestion has been made to define the severity of IDD usingalso the proportion of iodine concentrations below certain cut-off values, and not just from the median value (Karmarkar &

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 20/100
Stefan Peterson
20
Pandav 1999). This would allow for the identification of situations where a subgroup of the population remains iodinedeficient even though the median iodine concentration is
sufficient. “Elimination” of iodine deficiency is defined asachieving a median urinary iodine concentration above 100 g/lwith no more than 20% of the specimens registering below 50 g/l. Assuming a design effect of 3 due to cluster sampling, asample size of 750 is required to achieve a confidence interval of ∀5% at a prevalence rate of 20% (WHO 1994a).
Table 5. Epidemiological criteria for assessing the severity of iodine deficiencydisorders (IDD) based on median urinary iodine levels (WHO 1994a).
Median value ( g/l) Severity of IDD< 2020 – 4950 – 99∃ 100
SevereModerateMildNo deficiency
Hormones
Thyroid stimulating hormone
Increasing TSH levels is a compensation mechanism for iodinedeficiency. At population level the TSH levels thus indicateiodine deficiency and hypothyroidism. However, use of TSHlevels as an indicator beyond the neonatal period has beendiscouraged because of inconsistent relationships betweenpopulation TSH levels and iodine status (WHO 1994b).
THS levels in the foetus and the newborn are of specialconcern since elevated TSH levels signal insufficient levels of thethyroid hormone. This could cause abnormal brain development
(WHO 1994b). In gestational week 11 TSH is first detected infetal blood. TSH rises sharply at birth up to its maximum at 24hours after birth and then it falls gradually back over the first 3-4days as the infant’s T4 levels rise (Thorpe-Beeston et al. 1991).Therefore, it is recommended to sample neonates either from cordblood at birth or only after 72 hours, and then by heel prick(WHO 1994b). TSH levels in neonates can be used to identifycongenital hypothyroidism in relatively iodine sufficientenvironments. Screening all newborns for TSH will identify the

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 21/100
Controlling IDD – Studies for Program Management
21
approximately 1 per 4000 neonates (0.275%) that suffer from thiscondition in populations with adequate iodine intake. Thisprocedure is usually done by blotting whole blood on filter paper,
drying it, and sending the sample to a reference laboratory.Children with high TSH levels are then subjected to furthertesting to confirm their deficiency and if necessary thyroidhormone medicationis prescribed (Burrow 1980; Dunn & van derHaar 1990). In countries with universal screening such as Italyan incidence exceeding 1:2000 has been suggested as anindication of mild iodine deficiency (Sorcini et al. 1995).
Measurement of the distribution of TSH levels in a sample of newborns can give a picture of the iodine status in the population
(Kochupillai & Pandav 1987; Wächter et al. 1985; WHO 1994a).Table 6 gives the benchmarks for judging the severity of the IDDpublic health problem based on neonatal hypothyroidism.
Table 6. Epidemiological criteria for assessing the severity of iodine deficiencydisorders (IDD) based on prevalence of neonatal hypothyroidism (WHO 1994a).
MildIDD
ModerateIDD
SevereIDD
TSH > 5mU/lwhole blood inneonates
3.0-19.9% 20.0-39.9% ∃40%
ThyroxineThyroxine (T4) is the primary output of the thyroid gland.Thyroxin is de-iodinated in the peripheral cells to T3 which isthought to be the active hormone (Hetzel 1988). In severe iodinedeficiency the T4 levels may decrease, but de-iodination underthe influence of increased levels of TSH maintains adequate
levels of T3 (Kochupillai et al. 1973). The total T4 level dependson the amount of carrier proteins in the blood. It is thereforepreferred to measure the levels of thyroxin that is unbound in theserum, so called free T4. T4 can be used to characterize a findingof an abnormal TSH value in a patient (Todd 1998). However, theuse of T4 is not considered as a suitable indicator for populationlevel assessments of iodine deficiency (Benmiloud et al. 1994;WHO 1994a).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 22/100
Stefan Peterson
22
ThyroglobulinThyroglobulin (Tg) is the storage form of iodine and it is a thyroidhormone precursor. Tg is a glycoprotein found in the follicular
colloid of the thyroid gland. Normally small amounts of thyroglobulin leave the follicular cell. Tg is released into theblood when there is an increased turnover of thyroid cells such asin goiter (Todd 1998). Tg is more sensitive than TSH as ameasure of iodine status, because Tg changes earlier duringiodine deficiency and normalizes sooner during iodinesupplementation. Together with thyroid volume Tg has beenrecommended as a marker of iodine status that is more sensitivethan TSH or T4 (Benmiloud et al. 1994; Eltom et al. 2000a; Eltom
et al. 2000b).Iodine supplementation
Although iodine deficiency started appearing as a theory onthe cause of goiter as early as the 19th century, many othercausative theories persisted into the 20th century. In France,Courtois isolated iodine in 1813 and in 1820 Coindet suggestedthat iodine could treat goiter. Early attempts to use iodine in thisway often produced hyperthyroid effects; its use was therefore not
widely adopted. In 1825, Bossingault found that salt used inGuaca, Colombia contained iodine. In 1833, he suggested thatiodized salt could prevent goiter. Controlled experiments inFrance produced Iodine Induced Hyperthyroidism (IIH) whichagain prevented widespread iodine supplementation (Hetzel1989). In 1915, the use of sodium iodide tablets in Swiss schoolchildren was successful; this led to the introduction of iodized saltin Switzerland in 1922 (Hetzel & Pandav 1996). Marine andKimball carried out large scale controlled supplementation trials
in the United States from 1916 to 1920 that more conclusivelydemonstrated both the curative and preventive aspects of iodinesupplementation. This led up to the community scale use of iodized salt in Michigan in 1924 (Hetzel 1989; Marine & Kimball1922). In Sweden a pioneering national survey of goiter andcretinism preceded the adoption of salt iodization on a nationalscale (Höjer 1931). Other pioneer efforts demonstrated thatcretinism is caused by iodine deficiency and thatsupplementation with iodized oil can prevent new cases

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 23/100
Controlling IDD – Studies for Program Management
23
(McCullagh 1963; Pharoah et al. 1971; Pharoah & Connolly 1987;Pharoah et al. 1976).
In several countries tremendous social and economic gains
have resulted from the control of IDD. In China iodinesupplementation led to increased educational achievement,productivity, and quality of life (Li & Wang 1987). A meta-analysis of iodine supplementation trials in areas of mild tomoderate deficiency concluded that iodine supplementationraised the intelligence quotient by 13.5 points (Bleichrodt & Born1994). A 100-year follow up in Switzerland of an initial surveydemonstrated the disappearance of cretinism and endemic goiter,as well as reductions in isolated deafness, mental deficiency, and
short stature, making iodine supplementation a highly cost-effective intervention for the country (Burgi et al. 1990).Similarly, the World Bank concluded that iodinesupplementation is one of the interventions "that would have thehighest cost-effectiveness of any health intervention available inthe world today" (World Bank 1993). The World Health Assemblyendorsed the objective of eliminating IDD by the year 2000(WHO 1992).
There is overwhelming evidence and resolve to prevent IDDby increasing iodine intake in populations at large. Attempting toreduce IDD through changes in diet is often not practical sincemost foodstuffs, with the exception of seafood, are poor sources of iodine (Passmore & Eastwood 1986). However, use of iodine-containing animal feeds and disinfectants in the dairy industryhave made milk products an important source of iodine in someplaces (Phillips 1997). The approach generally used to increasethe iodine intake countries is either through medicinalsupplements or through fortification of widely used foodstuffssuch as salt.
Iodized oil
Iodized oil was first used as a contrast medium in radiology andlater found, in Papua New Guinea, to be an effective control of IDD when injected (McCullagh 1963). Subsequently, it wasshown that iodized oil can also be given orally (Eltom 1984).Many countries have since used large amounts of iodized oil incontrol programs. Outside of China the supply is dominated by

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 24/100
Stefan Peterson
24
Laboratoire Guerbet, Paris, France. Their Lipiodol Ultra-Fluid isa x-ray contrast medium conventionally used in radiology; e.g., forlymphography. It is a clear yellow poppyseed-oil based substance
containing 480 mg iodine/ml. It is available in 10 ml ampoules forintra-muscular injection as well as in 200 mg capsules and asOriodol in oral pump-dispensers.
Iodized oil capsules cost about 14 US cents per 200 mg of iodine and the pump-dispensed Oriodol about 4 cents per 200 mg(Hetzel & Pandav 1996). This price is rather substantialcompared to e.g. Vitamin A capsules at 2-3 cents each.Subsequently developed cheaper iodised oils have not found theirway into the market (Inglenbleek et al. 1997), nor has, to my
knowledge, any other producer bid against Guerbet in atendering process. The Chinese formulation is based on walnutor soybean oil. This formulation has not been formally evaluatedfor e.g. efficacy, safety and cost against other supplements suchas Lipiodol.
Intra-muscular administrationIn the highland villages of Papua New Guinea, it wasdemonstrated that a single injection of 2400 mg of iodized oil canmaintain normal thyroid function for 3 to 5 years (Buttfield &
Hetzel 1967; McCullagh 1963). The long lasting effect isexplained by the slow release of the large iodine load from themuscle and its storage in fat tissue. Subsequently, the dose waslowered to 1 ml (480 mg) giving an equally long protective period(Dunn & van der Haar 1990) and large scale injection programshave been implemented in countries such as Papua New Guinea,Nepal, and Democratic Republic of Congo (Zaire). In addition,these injections were reported to be safe for pregnant women(Delange 1996; Pharoah & Connolly 1991). However, the high
cost, logistical difficulties, and risks of transmission of diseasessuch as HIV and hepatitis have switched attention to oraladministration of iodized oil.
Oral administrationTaking iodised oil orally eliminates many of the disadvantages of injections. There is no risk of transmitting infectious agents viasyringes, it requires less skilled staff, and it takes less time.However, since there is no intra-muscular store of iodized oil,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 25/100
Controlling IDD – Studies for Program Management
25
most is excreted within the first few days and the duration of theeffect is shorter. An initial study recommended 400 mg every twoyears (Eltom et al. 1985). In 1987, a review recommended 1 ml
(480 mg) for one year’s duration (Dunn 1987b) and in 1990 thiswas extended to 1-2 years (Dunn & van der Haar 1990).Subsequent prophylactic studies have recommended 240 mg of iodine for a 6-month coverage or 480 mg for 12 months(Benmiloud et al. 1994); a study in Zaire found that 47 mg and118 mg was sufficient for up to one year (Tonglet et al. 1992). A study in the Sudan found that 200 mg was sufficient to controliodine deficiency in goitrous adults for a 12 month period(Elnagar et al. 1995). Presumably these discrepancies could be
explained by different underlying severity of the iodinedeficiency, different sampling or evaluation methodologies,influences on iodine absorption/utilization by goitrogens,helminths (Furnée 1994), or iron status (Zimmerman et al. 2000).It seems clear, however, that the physiologically effectiveduration of supplementation lasts closer to one year than to twoyears. This conclusion is an important programmaticdisadvantage.
The drawbacks of iodized oil supplementation include theneed to make direct contact with every targeted person at theappropriate distribution interval. Intermittent bolus doses areless physiologically effective than a constant dietary supply of iodine, and that, although less than for injections, widespreaddistribution poses significant logistical challenges. On thepositive side, oral iodized, oil can be accurately targeted topopulation groups and individuals. A campaign can also beinitiated quickly in a severely iodine deficient area while othercontrol methods are being prepared. Oral iodized oil will thus betargeted for areas with severe to moderate IDD where adequate
coverage with iodized salt is unlikely to be achieved in the nearfuture. Depending on the feasibility of introducing iodized salt inan area, oral iodized oil may have to be considered as a mediumterm control measure when iodine deficiency is severe enough towarrant an intervention (Dunn 1996b).
The target groups for supplementation are, in order of importance: 1) women of childbearing age; 2) children 0-5 years;3) older children; 4) adult men 15-45 years of age (Dunn 1987b).In people older than 45 years of age, iodized oil is not encouraged

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 26/100
Stefan Peterson
26
due to increased risks of hyperthyroidism. The same applies topersons with nodular goiter; however, a reduced dose of iodizedoil could be considered. A recent review concluded that in areas
where iodine deficiency is moderate or severe, iodized oil shouldalso be given during pregnancy (Delange 1996).The cost of providing iodized oil varies according to the
distribution dose, interval, and delivery strategy adopted. Thetotal annual cost of an oil supplementation program has beenestimated at USD 0.50 per person and per year (Jamison et al.1993). However, in spite of the control efforts undertaken usingoral iodized oil in several countries, the literature contains noaccount of the real distribution costs, nor of the actual
distribution coverage achieved, and timeliness of repeatdistributions.
Iodized salt
The first large-scale iodine supplementation programs in theUnited States and Switzerland used iodized salt. Subsequentlyother countries in Europe started similar programs. Salt hasmany advantages. It may be the only foodstuff imported bysubsistence agriculture communities. It is consumed in similar
amounts by all - even the socioeconomic level of a household hasvery little influence on its consumption of salt. Furthermore,iodization does not alter the taste or color. In most settings, thismakes salt an “ideal” vehicle to deliver a micronutrient likeiodine to all individuals in relatively similar daily doses, withouteven having to contact them individually. An added advantage isthat livestock consume salt, benefiting themselves and theconsumers of animal products (Mannar 1996).
Iodizing the saltThe first countries to embark on salt fortification used potassiumiodide (KI). This has been the approach replicated by mostcountries in temperate climates. However, in tropical humidconditions the evaporation of iodide is substantial. In suchsettings potassium iodate, KIO3, provides a less soluble, morestable alternative. Iodate also performs better in salt withimpurities. Strictly speaking this is “iodated” salt but it is oftenreferred to as “iodized” as well (Dunn & van der Haar 1990;Hetzel 1989).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 27/100
Controlling IDD – Studies for Program Management
27
In many settings salt production is fairly centralized to a fewcenters using techniques such as mining, evaporation of saltwater or underground brine. This makes it potentially feasible to
introduce and control the use of large-scale iodization technologyfor dry mixing, drip feeding, or spraying the salt with iodine.Thorough mixing of salt is necessary using drum mixers or screwconveyors. The iodization machines most used in sub-Saharan Africa are made in the Indian subcontinent and generally quitesimple and rugged. The cost of salt iodization is usually aroundUSD 0.02-0.10 per person per year. However, expressed as apercentage of the retail price of salt, it amounts to about 5% of the total cost of the product (range 2-32%) (Mannar 1996; World
Bank 1993).Iodization levels in salt depend on the average daily saltconsumption, the severity of iodine deficiency, and expectediodine evaporation losses during transport, storage, and cooking.Humans usually consume between 5 to 20 grams of salt dailyand need a daily iodine intake of 100-200 micrograms. In awarm, moist climate where salt is packaged in large sacks, therecommended iodization levels for the factory were therefore setat 50-100 mg of iodine per kilo of salt, often expressed as part permillion (ppm), see Table 7 (WHO 1994a).
Table 7. Salt iodization levels in parts per million recommended at differentstages of the distribution chain by WHO in 1994.
Factory outsidethe country
Factory insidethe country
Retail level Household
Dailysaltconsumption
Bulk Smallpack
Bulk Smallpack
Bulk Smallpack
5 gr. 100 80 90 70 80 60 50
10 gr. 50 40 45 35 40 30 25
Iodine induced hyperthyroidism (IIH) was observed inZimbabwe (Todd et al. 1995) where salt was distributed in smallplastic consumer packs minimizing iodine losses. IIH was alsoreported from Zaire (Bourdoux et al. 1996). This resulted in therecommendation that iodization at the production level should bereduced to 20-40 ppm (Clugston et al. 1996; WHO 1996).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 28/100
Stefan Peterson
28
Legislation, quality control, and monitoringSalt iodization raises the cost of large-scale salt production byabout 5%. This may create a situation where both iodized and
non-iodized salt can be sold at different prices, alternatively non-iodized salt could falsely be sold as iodized with a larger profitmargin. This necessitates legislation requiring universal saltiodization. Moreover, enforcement measures need to be in place toprevent cost competition or fraudulent declarations concerningiodization of salt. In addition it is recommended to increase thepopular demand for iodized salt (Dunn & van der Haar 1990).
Quality control of the salt iodization production process isnecessary to ensure adherence to the recommended iodization
levels. Although government quality control inspections are anessential part of the quality control system, the mainresponsibility for quality control is left to the producers. Samplingprocedures for such quality control have been suggested based onthe relatively accurate standard titration method of assessing saltiodine content with intermittent tests using rapid test-kits(Sullivan et al. 1995; WHO 1994a).
In addition, the salt iodine levels need to be monitored alongthe distribution chain: at point of importation (where applicable),in wholesale warehouses, in retail stores, and in households. One
objective of such monitoring is to identify, impound, and discardnon-iodized salt. Such activities require a titration assessment of iodine content. Other objectives of iodine content monitoring is toverify assumptions regarding iodine losses due to the effectivenessof packaging materials, storage methods, and retail conditions anddevelop ways to prevent such losses as well as to study householdsalt storage. In addition, if rapid test kits are used, peripheralmonitoring can serve as a way to educate the pubic about saltiodization. These kits use the starch-iodine color reaction to detect
the presence of either iodide or iodatein a relatively crude way.Where more accurate determination of iodine content is needed,e.g. to quantify losses or as a basis for taking legal action, titrationshould be used (Dustin & Ecoffey 1978; Sullivan et al. 1995; WHO1994a).
Quality control and monitoring responsibilities need to beclearly defined. Monitoring criteria for judging the adequacy of theprocess have been proposed, Table 8. Sampling procedures have

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 29/100
Controlling IDD – Studies for Program Management
29
been suggested by Sullivan et al (1995).
Table 8. Criteria for assessing adequacy of salt iodization programs, their
quality control and monitoring (WHO 1994a)
Process Indicator Criterion of adequacy A.Factory or importer level
1. Percent of food grade saltclaimed to be iodized
2. Percent of food-grade salteffectively iodized
3. Adequacy of internal
monitoring process*4. Adequacy of externalmonitoring process
100%
>90%
>90%
10-12 monthly checks perproducer/importer per year
B.Consumer and District Level1. Percent of monitoring sites
with adequately iodized salti) households (or schools)ii) district headquarters(including major markets)
2. Adequacy of monitoringprocess**
Adequate in 90% of samples
90% or more
* Corrective action systematically taken within 3 hours in 90% of cases usingLot Quality Assurance Methodology** Monitoring undertaken in 90% of districts in each province at both householdand district levels
LimitationsWhile salt iodization appears to be the main candidate for iodine
fortification there are several potential challenges related togetting the iodine onto salt, making iodine stay on salt, ensuringthe use of iodized salt, and knowing whether these things occur.
At the iodization stage, challenges include installingiodization machinery, finding a reliable supply mechanism forpotassium iodate, and ensuring that production machinery isused and maintained in an effective and consistent manner. Thisrequires a significant initial investment in equipment andtraining as well as a commitment to continuos external
monitoring and quality control. A special difficulty arises insituations where salt originates from many small-scale

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 30/100
Stefan Peterson
30
producers. Indonesia is one example and Tanzania with itsestimated 197 salt producers another (DailyNews 1994). It iseven more difficult to monitor quality in the salt produced by an
estimated 7,500 women who extract salt from salty soils usingevaporation processes in certain rural areas of Tanzania.(ICCIDD 1997b; Momburi 1993). Although small-scale producersonly produce about 10% of the total world production (UNICEF1994a), artisanal salt production is of large importance ingeographic areas of severe iodine deficiency. As any one produceris too small to sustain an iodation machine organizing saltiodation viably is difficult. UNICEF has suggested alternativestrategies to deal with this situation: organizing small producers
into cooperatives that share an iodization machine; sending amobile salt iodization machine periodically; providing eachproducer with small scale iodization equipment; and establishingcommercial iodization refineries that purchase and iodise the saltfrom the small producers (UNICEF 1994a). The relative cost of iodizing salt in these ways is likely to be higher than in a largescale operation since more transport and handling of the salt isrequired. Monitoring salt iodization among small-scale producersis also a logistic challenge.
In countries where the prevailing salt type is crude or coarse
salt that has not been crushed and homogenised the large, oftenimpure, salt crystals pose technical challenges to iodization.Iodizing wet salt from salt pans adds further technicalcomplexity.
The difficulties caused by iodine evaporation requireadequate wholesale packaging, storage, retail packaging anddisplay mechanisms. Large packaging used for bulk storage andtransportation should be lined with polyethylene and consumerpackaging should preferably be in sealed plastic bags (Mannar &
Dunn 1995). However, often any type of second hand bag is usedto pack salt. The salt may not be dry, which allows the iodine tomigrate to the bottom of 50 and 100 kg sacks causing iodinelevels to be unevenly distributed. Storage may expose the bags tohumidity or heat which accelerates iodine loss (Chauhan et al.1992). At the retail level, it is customary in many places to poursalt out in small heaps left uncovered in the sun causing losses of iodine up to 42% (Kapil et al. 1996). Finally, household storage of the iodized salt may be inadequate and practices such as

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 31/100
Controlling IDD – Studies for Program Management
31
washing the salt can further decrease the iodine content beforecooking, which results in as much as a 30% iodine loss (WHO1994a).
Public acceptance and demand for iodized salt is considered anecessary prerequisite of a successful iodization program. Thiscan only be achieved through a massive education effortinvolving decision makers, salt producers, salt retailers, healthworkers, citizen groups, and the general public (Dunn 1996a;Dunn & van der Haar 1990). In Germany and other Europeancountries, consumer groups often oppose iodine fortificationprograms advocating the consumer’s right to choose betweeniodized and non-iodized products. Similar arguments have been
raised in India. In other countries, lack of demand for iodized saltmay maintain a market for non-iodized salt, or make thepopulation prefer the cheaper non-iodized salt where both typesare available.
Several examples from South Asia and Latin Americademonstrate the need for effective monitoring and enforcementmechanisms to achieve and sustain good coverage withadequately iodized salt; (Murdoch et al. 1999; Hetzel 1989;Passmore & Eastwood 1986). Often salt legislation is notenforced. Monitoring and enforcement mechanisms need to be inplace at each stage of production and distribution. This willinvolve several Government agencies and necessitates the settingup of monitoring mechanisms, titration laboratories, and a steadysupply of rapid test kits (Dunn 1996a; Sullivan et al. 1995; WHO1994a).
The combined effect of these difficulties often leads to delays,sometimes for decades, in achieving an effective salt iodizationprogram. Spain is such an example of the long delay inimplementing a salt iodization program (Fernandez 1990). Even
in the best case it will take a number of years to establish aprogram. However, even after a successful program has beenestablished there may still be populations without effectiveaccess or utilisation of iodised salt, e.g. because of non-iodatingsmall salt producers or local production of salt from salt lakes or“foothill salt” (Momburi 1993). Therefore countries may need toconsider complementary supplementation methods where saltiodization is not likely to succeed (Solomons 1998).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 32/100
Stefan Peterson
32
Iodization of water, sugar, and other vehicles
Iodized water
Since water has to be consumed daily, it is another vehicle foriodine supplementation. In 1923, the city of Rochester, in New York state, was the first municipality to add iodine to its drinkingwater. Since then, cities in Thailand, Malaysia, and Sicily haveadded iodine to their central drinking water. These experienceswere largely successful in correcting iodine deficiency and alsoserved to disinfect the water supply provided chemical iodine isused, not iodide or iodate. In Northern Thailand drops of iodinesolution are added to school water supplies with good results butrequiring constant supervision. However, in many settingsdrinking water comes from many sources making effectiveiodization difficult to achieve (Dunn 1987a; Dunn 1996b).
In semi-arid settings people often drink from one or fromvery few water sources. A system using slow release iodine insilicone matrices has been developed and used in Mali and in theCentral African Republic (Fisch et al. 1993; Pichard et al. 1992; Yazipo et al. 1995a; Yazipo et al. 1995b). This method of iodization in hand-pump wells increases water iodine, urinaryiodine, and reduces goiter rates. A study from the Sudan
confirmed these findings but demonstrated limitations in theeffectiveness of the system in traditional wells (Elnagar et al.1997). The matrices cost around USD 100 each. They need to bechanged every year and the per capita cost will depend on howmany people draw their drinking water from the same well.Small villages are more expensive to supplement per capita.
In a semi-arid area of Xinjiang, China, iodine absorbed bythe crops from iodized irrigation water found its way through thefood chain and into people. This method not only normalizediodine deficiency but also reduced infant mortality at anestimated cost of USD 0.05 per capita per year (Cao et al. 1994b;DeLong et al. 1997; DeLong 1998).
Iodized Sugar and BreadIn the Sudan, sugar is a food that is consumed by a large numberof people and it is subsidized and rationed. A pilot trial to fortifysugar with iodine was successful in increasing urinary iodineconcentrations, in reducing goiter rates, and in improving

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 33/100
Controlling IDD – Studies for Program Management
33
thyroid hormone status. Sugar, therefore, is another way tointroduce iodine into a population (Eltom et al. 1995).
Iodized bread has been used successfully in Holland, Russia,
Australia, and Tasmania but the variations in breadconsumption and the unavailability of bread in remote ruralareas limit the practicality of this method (Clements et al. 1970;Gandz 1974; Gerasimov et al. 1995). Iodized tea has beensuggested as a means of food fortification in Tibet.
Direct supplementationDirect supplementation can also be done using iodide tablets orsolutions. Some of the early supplementation research was done
using sodium iodide tablets (Gibson & Backman 1924 cited inSjöberg & Sundlöf 1971). This supplementation method was usedin the Soviet Union and sodium iodide tablets continue to beused in Germany. Iodine solutions such as Lugol’s (6 mg iodineper drop) have been used successfully in controlling iodinedeficiency in Bolivia. Direct supplementation, which requiresdaily, weekly, or perhaps monthly doses, has limited overalleffectiveness since its effectiveness depends on individual andsystemic responsibility and motivation (Dunn 1996b; Todd &Dunn 1998).
Excess iodine intake
Food, medication, and supplements are sources of iodine. Ingeneral, consumption of iodine that exceeds the recommendeddosage by as much as ten times is well tolerated by most people.However, some people respond adversely to levels close to therecommended intake (Todd 1998). A dramatic increase in theplasma iodide load causes the thyroid gland to block iodine
organification. This transient phenomenon is known as theWolff-Chaikoff effect (Wolff et al. 1949). Other manifestations of excess iodine include thyroiditis, goiter, hypothyroidism, hyper-thyroidism, and sensitivity reactions.
The phenomenon of most relevance for iodinesupplementation programs is iodine-induced-hyperthyroidism(IIH). Symptoms are the usual of thyrotoxicosis: anxiety,palpitations, weight loss, muscle weakness, fatigue, diarrhea,sweating, and hot sensations. More serious cardiac effects suchas: atrial fibrillation, angina, and heart failure may also occur. In
most cases IIH is caused by toxic nodular goiter (Todd 1998).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 34/100
Stefan Peterson
34
Following the introduction of iodine supplementation into apreviously iodine-deficient population susceptible individualsmay develop IIH. In most cases this occurs in women over the age
of 40 with nodular goitre (Todd 1998). The most well-knownexample of this followed the introduction of iodized bread intoTasmania in the 1960’s (Connolly 1971). Recently, in Zimbabwe(Todd et al. 1995) and Zaire (Bourdoux et al. 1996) iodization of salt resulted in cases of IIH. While the condition in any onepatient can be serious and requires immediate medical care, IIHis a temporary and rare phenomenon that can be successfullytreated if detected. Typically, IIH occurs during the first few yearsof an iodization program as a result of the many large goiters
caused by the previous iodine deficiency, thus making it an iodinedeficiency disorder. For a population the benefits of iodinesupplementation on balance far outweigh the risks of increasedhyperthyroidism (WHO 1997). While IIH cannot be fully avoidedit can be minimized by regulating the iodine supply (Todd 1998).Because of this, recommended salt iodization levels were loweredin 1996 to 20-40 ppm (WHO 1996).
Controlling Iodine Deficiency Disorders
Management structure and strategy
Recognizing that it was technically feasible as well as affordableto control IDD, yet effective control programs were not in place, agroup of concerned professionals, mostly IDD researchers with astrong representation of endocrinologists, took the initiative tocreate the International Council for Control of Iodine DeficiencyDisorders (ICCIDD). ICCIDD was officially inaugurated inKathmandu, Nepal in 1986. It has an international executivecommittee, six regional IDD coordinators and working groups aswell as a multidisciplinary network of members. Based on the1986 World Health Assembly resolution to prevent and controlIDD, the ICCIDD has worked closely with multilateral, bilateral,national, and non-governmental organizations to lay out andimplement a global strategy for IDD control. This strategy hasbeen endorsed by the UN System’s coordination subcommittee onnutrition (Hetzel 1987a; Hetzel 1988; Hetzel 1996; WHO 1986).
Success in controlling IDD is a complex process involving

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 35/100
Controlling IDD – Studies for Program Management
35
political, social, and economic dimensions. This process has beenstudied in different countries and a model summarizing requiredprogram steps and objectives was proposed and updated to its
present form based on experiences in South East Asia (Hetzel1987a). It was adopted immediately as the guiding model by theInternational Council for Control of Iodine Deficiency Disorders(ICCIDD), and it has remained fairly constant with only minorchanges being made. It comprises the following steps which areto be completed in a cyclical fashion by a multi-sectoral NationalIDD Control Commission (Hetzel 1988):
1. Assessment (collect data, assess situation)2. Communication (disseminate findings)
3. Planning (develop or update plan of action)4. Political decision (achieve political support)5. Implementation6. Monitoring and evaluation
The latest published version is presented in Figure 2.
Figure 2. The ”Social Wheel” of IDD control (Hetzel 1996)
Intersectoral
Commission
Firstly Assess
Situation
Population at risk
Prevalence of IDD
Disseminate
Findings
Develop or
Update
Plan of Action
Health
Professionals
and Public
Achieve
Political
Will
Implementation
of Programme
Evaluate
Program
Prevalence of IDD
Urinary iodine
Blood sport TSH
Community
Groundswell
Resource
Allocation
Program
Education
Training

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 36/100
Stefan Peterson
36
In the following sections selected technical aspects of theIDD “Social Wheel” control cycle as recommended by ICCIDD,WHO and UNICEF are reviewed (WHO 1994a).
Assessing IDD
Many indicators exist for individual iodine deficiency disorders.The selection of indicators for assessment depends onacceptability, technical feasibility, cost, and the indicator’smeasurement performance. It is generally recommended tocombine at least two indicators, such as thyroid size and urinaryiodine concentration. Commonly used indicators are presented inTable 9 together with criteria for judging the severity of thepublic health problem (WHO 1994a).
Table 9. Summary of IDD prevalence indicators and criteria for classification of severity of public health problem (WHO 1994a).
Severity of public health problem(prevalence)Indicator Target
Population Mild Moderate Severe
Goiter grade > 0
Thyroid volume >97thCentile by ultrasound b
Median urinary iodinelevel ( g/L)
TSH >5mU/L wholeblood
Median Tg(ng/ml serum)c
SACa
SAC
SAC
Neonates
C/A d
5.0-19.9%
5.0-19.9%
50-99
3.0-19.9%
10.0-19.9
20.0-29.9%
20.0-29.9%
20-49
20.0-39.9%
20.0-39.9
>30.0%
> 30.0%
< 20
> 40.0%
> 40
a SAC = school-age childrenb Reference values in (WHO & ICCIDD 1997)c Different assays may have different normal rangesd C/A = children and adults

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 37/100
Controlling IDD – Studies for Program Management
37
The target groups for assessment also merit discussion.While many of the effects of iodine deficiency manifestthemselves in neonates and during early childhood, this age-
group is not very accessible. Adult women, especially pregnantwomen, need adequate iodine status to prevent IDD fromdeveloping in their foetus. However, this group may not be veryappropriate for some indicators since goiters in women do notnecessarily reflect recent iodine status. The most commonlystudied group is children in schools. This highly accessible andco-operative group is also vulnerable and their thyroid size willreflect the iodine status in the last few years (Aghini-Lombardi etal. 1997). Inference is then made from this group to the others,
such as neonates and pregnant women. However, in situationswhere school attendance is low the children at school mayprovide a biased estimate as their peers at home may be worseoff (WHO 1994a). The construction of sampling frames for schoolselection must take into account student geographic origin andstratify for presumed different degrees of iodine deficiency.
Communication
The effects of IDD should be communicated to the public and
politicians. Topics to communicate include the effects on growthand development, the effects on the brain, the effects on schoolperformance, the effects on productivity, and the effects onquality of life. Widespread understanding of the scope and causeof IDD should result in support and demand for interventions.
Press coverage is assured during launching ceremonies of legislation, iodation plants and major meetings (Daily News1994; Kwena 2000). In addition, flyers and posters communicatethe impact of IDD and encourage the consumption of iodized salt.
“Question and answer” booklets have also been produced in somecountries. A few countries have made use of “IDD days” to raiseawareness. ICCIDD now stresses the need to improvecommunication at all levels and has produced a communicationguide which will be translated into several languages (ICCIDD1999a; Ling & Reader-Wilstein ).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 38/100
Stefan Peterson
38
Plan of action & Achievement of political will
The ICCIDD regional groups serve to promote national programs
by coordinating events, providing technical advice, fundraising,and progress monitoring. With their support ICCIDDrecommended managerial structures have been re-created inmany countries. Thus multisectoral National ControlCommissions for IDD implement the strategy and its componentsin individual countries.
Using an intersectoral commission a plan of action is drawn.This involves a situation analysis of the salt sector and saltconsumption as a basis for introducing salt iodization.
Recommended groupings such as a salt producers’ association arethen formed. In addition, salt producers’ co-operatives are formedto organize small salt producers.
In situations where iodized salt is deemed to be long incoming, other control methods, primarily iodized oil, can be usedas temporary control efforts while striving to achieve universalsalt iodization.
The international effort to raise awareness and achievepolitical will has been very successful, as confirmed by theenactment of salt iodization legislation in a growing number of
countries. Much operational and financial support for this processhas been rendered by UNICEF in light of the goal to eliminateIDD by the year 2000 (Grant 1994). Great strides have beenmade towards this target but the challenge of achieving fullelimination remains.
Implementation
With UNICEF and other donor assistance, salt iodizationmachinery has been imported and installed in salt producingcountries, potassium iodate has been procured, and personnelhas been trained. Where control methods other than salt havebeen used, countries have generally been supported by outsidedonors.
Monitoring and Evaluation
The initial strategy spelled out monitoring and evaluation as thefinal step of the “social wheel” (Hetzel 1988). The subsequent

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 39/100
Controlling IDD – Studies for Program Management
39
publication of the model talks of evaluation alone and listsindicators such as prevalence of IDD, urinary iodine, andbloodspot TSH, see Figure 2 (Hetzel 1996). Subsequent technical
documents also suggest methods and indicators for processmonitoring of the intervention, i.e. salt iodization (Sullivan et al.1995; WHO 1994a).
IDD in Sub-Saharan Africa
Iodine deficiency and IDD are widespread in Africa. A third of thetotal population is considered at risk of IDD and 86 million, 16%
of the population, is thought to have goiters. Severe IDD affectslarge parts of Central, Eastern, and Southern Africa(WHO/UNICEF/ICCIDD 1993). Further details are given belowfor two severely endemic countries, the Central African Republicand mainland Tanzania.
Central African Republic
The Central African Republic is a landlocked country across theUbangi river from the Ubangi area in the Democratic Republic of
Congo (former Zaire). IDD in the Ubangi area was extensivelystudied by Ermans et al who found severe iodine deficiency and ahigh prevalence of IDD. Based on findings of increased urinarythiocyanate levels they concluded that cassava was anaggravating factor for IDD (Ermans et al. 1980b; Thilly 1992). Inthe Central African Republic IDD was found to be highlyprevalent both in smaller area surveys (Biassoni et al. 1990b;Mongonou 1982) and in a national survey (Lantum 1991). Allparts of the country are highly endemic with total goiter rates
between 40 and 90%. Approximately two thirds of the populationis affected by IDD (WHO/UNICEF/ICCIDD 1993).Most of the salt in the country is imported. Salt from
Cameroon penetrates the western parts of the country. It isincreasingly iodised following the monopolistic producerSELCAM’s successful iodation efforts (Lantum 1992). Other saltsources are located in South Africa, Namibia, and the Sudan inthe East. Traditional salts, such as “natron” from Lake Chad andthe production of salt by burning grass into ashes, are also

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 40/100
Stefan Peterson
40
available (ICCIDD 1997a; Thilly 1992). Successful trials havebeen conducted with iodized water in the more arid parts of thecountry (Yazipo et al. 1995a; Yazipo et al. 1995b). The national
primary health care commission oversees IDD control efforts,which includes monitoring salt imports and monitoring wateriodization (Lantum 1992).
Cassava is the main staple crop (Fresco 1986). Thethiocyanate load from cassava consumption has been implicatedas an aggravator of goiter in CAR (Biassoni et al. 1990a), andreduced consumption suggested as a means to alleviate theproblem (Biassoni et al. 1991). Another condition attributed todietary cyanide-exposure from cassava, is the paralytic disease
konzo, which has also been reported in CAR (Peterson 1994;Tylleskär et al. 1994).
Mainland Tanzania
Mainland Tanzania has a large landmass with coastline,highlands, mountains, and floodplains. Studies in thesouthwestern part of the Tanzanian highlands havedemonstrated high goiter rates, cretinism, and highly prevalenthypothyroidism in schoolchildren as well as neonates, which
were amenable to correction using injections of iodized oil(Wächter et al. 1986; Wächter et al. 1985). Nation-wide systematicsurveys of iodine deficiency disorders were gradually conductedin numerous small-scale school goiter-surveys during 1980through 1990. Total goiter rates between 1 and 88% were foundwith an estimated 40% of the population affected(WHO/UNICEF/ICCIDD 1993). The summary map of goiter ratesby district shows severe IDD in most highland and floodplainregions in Tanzania (NCCIDD-TFNC 1990). Based on the goiterrates established in the school surveys, van der Haar, Kavisheand Gebre-Medhin estimate that 8 million people have goiter,160,000 cretinism, 450,000 more mildly affected withcretinoidism, and that 30% of total perinatal mortality is causedby iodine deficiency (van der Haar et al. 1988).
The Tanzania Food and Nutrition Center (TFNC) developeda strategy for National IDD control in 1985. The plan called forthe use of iodized oil as an interim control method in severelyaffected areas to prevent further brain damage there, while

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 41/100
Controlling IDD – Studies for Program Management
41
working towards a universal salt iodization program. Injection of iodized oil was initially tried in two districts but abandoned dueto cost and shortage of trained staff. Instead, iodized oil capsules
(IOC) were distributed beginning in 1986. Using an initialcriterion of district Visible Goiter Rate >10%, a total of 20districts were targeted for IOC distribution. Later the criterionwas revised to Visible Goiter and grade 1B >10% and 5 moredistricts were added. Supported by the Swedish InternationalDevelopment Authority, the objective was to distribute two IOC(400mg) every two years to the general public 2-45 years of age,excluding persons with multi-nodular goiter, and one IOC(200mg of iodine) to children aged 12-23 months of age. (ICCIDD
1997b; Sanga 1994).The efforts to iodize salt in Tanzania began in 1973.However, technical, administrative, and coordination problemsamong the actors stifled the effort (Sanga 1994). The saltiodization effort should have been re-launched with Dutchsupport together with the start of the IOC distribution. However,due to several sources of delays it was only in 1991 that UNICEFimported three iodization machines from India and installedthem in three major salt works. These first machines werefollowed by 42 more machines until 1995 (UNICEF 1996). Manyof these were smaller rotary drum type mixers provided to 200 orso small-scale salt producers located mainly on the southerncoast. These producers were encouraged to form co-operativesand channel all their salt through a centrally located iodizationmachine. The installed iodization capacity at 150,000 tons peryear was theoretically sufficient to satisfy the national needassuming constant salt production throughout the year.Constraints on the program include seasonal salt production andonly about 140 salt producers being officially registered.
Government has been unwilling to centralize salt production to afew larger producers, presumably for reasons of maintaining jobopportunities (Sanga 1994; UNICEF 1996).
In the central parts of the country production of “foothill salt”from salty soils is widespread. Some 7,500 women are believed tobe involved. By certain estimates this production is quitesubstantial amounting up to 40,000 metric tons, although it hasyet to be substantiated how widespread exclusive use of the saltis (ICCIDD 1997b; Momburi 1993).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 42/100
Stefan Peterson
42
A 1995 law requires all salt for human consumption to beiodized whether produced in the country or imported (some10,000 metric tons per year) (ICCIDD 1997b). Domestic salt
production takes place mainly on the coast and in the extremewest of the country with complex distribution patterns requiringan estimated 4-6 weeks to reach the consumer (TISCO 1992).Consuming an average of 8 grams of salt per day, Tanzanianconsumers appear to have strong preferences because of the“taste” and the price for coarse, crudely refined, large-crystal saltdistributed in 50 kg reused sacks of different material. Thecoarse salt is often moist and does not hold iodine very well.Furthermore, it is retailed loose in markets, freely exposed to the
sun, providing opportunities for rapid iodine loss. Refined tablesalt in small 0.5 kg plastic bags is widely available, however, atapproximately double the price of the coarse salt. It is mainlyused to sprinkle on special foods such as roasted meat. Takingthese production, distribution, and retail patterns into account,salt iodization levels were set at 75-100 ppm at the factory so asto achieve household levels of 37 ppm or more (Sanga 1994).
A National Control Commission for IDD (NCCIDD) wasorganized for all stakeholders. TFNC, under the Ministry of Health, is the secretariat. An association for salt producers has
been formed to encourage dialogue, distribution of the UNICEFsupplied iodization machines, distribution of potassium iodate,and initially providing appropriate packing materials. Supportwas also provided for monitoring. The monitoring responsibilityis divided among the different actors. These are the Ministry of Water, Energy and Minerals (MOWEM) for the production sites,the National Food Control Commission (NFCC) with their districthealth assistants for the distribution chain, and TFNC for thehousehold consumption level (ICCIDD 1997b; Sanga 1994).
Larger production sites were given a salt titration laboratory. Tofacilitate production site monitoring, a number of vehicles weresupplied to the zonal mining officers in MOWEM. For moreaccurate quality control and enforcement during the distributionchain, NFCC set up network of regional salt titrationlaboratories. Peripheral Health Assistants’ and TFNC’smonitoring has largely used rapid field test kits. Altogether theexternal support for the iodization program amounted to 80% of the budget during the first few years (Sanga 1994).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 43/100
Controlling IDD – Studies for Program Management
43
I. Peterson S, Légué F, Tylleskär T, Kpizingui E, Rosling H. Improved cassava-processing can help reduce iodine deficiency disorders in the Central AfricanRepublic. Nutrition Research 1995; 15(6):803-812.
II. Peterson S, Rosling H, Tylleskär T, Gebre-Medhin M, Taube A. Endemic Goitre inGuinea [Limitations of urinary iodine / thiocyanate ratios as indicator of antithyroid effect in population studies]. Lancet 1995; 345(February 25):513-514.
III. Peterson S, Assey V, Forsberg B, Greiner T, Kavishe FP, Mduma B, Rosling H,Sanga B, Gebre-Medhin M. Coverage and cost of iodized oil capsule distribution inTanzania. Health Policy and Planning 1998; 14(4):390-399.
IV. Sundqvist J, Wijetunga M, Assey V, Gebre-Medhin M, Peterson S. Salt iodation andrisk of neonatal brain damage. Lancet 1998; 352(July 4):34-35.
V. Peterson S, Sanga A, Eklöf H, Bunga B, Taube A, Gebre-Medhin M, Rosling H.Classification of Thyroid Size by Palpation and Ultrasonography in Field Surveys.
Lancet 2000; 355 (January 8):106-110. Addendum in Lancet 2000; 355, (June 3):1995-1997
Figure 3. Location and titles of studies in Africa

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 44/100
Stefan Peterson
44
AIM OF THE STUDIES
The overall aim of the studies presented in this thesis is toimprove the methodologies to assess the severity of iodinedeficiency, to monitor the implementation of iodinesupplementation programs, and to evaluate program impact. Thespecific objectives of the five studies are as follows:
- to elucidate whether the thiocyanate load from cassavasignificantly aggravates the effects of iodine deficiency in threecassava consuming communities of the Central AfricanRepublic and draw conclusions for IDD control policy (paper I);
- to analyze the mathematical and physiological properties of the iodine/thiocyanate ratio as an epidemiological indicator forthe postulated goitrogenic effects at urinary I/SCN ratios <3 g/mg using data from Tanzania and the Central AfricanRepublic (paper II);
- to estimate the population time supplemented by Iodized Oil
Capsule (IOC) distribution over a nine year period in aTanzanian population of 7 million and to estimate the cost andeffectiveness of the three distribution strategies used (paperIII);
- to study the relationship among the three main iodinedeficiency indicators in three vulnerable groups and to relatethis to the iodine content in table salt in a Tanzaniancommunity (paper IV);
- to determine the effects on goiter rate of the WHO 1994change in palpation criteria for goiter and to compare therelative precision between the old and new palpation systemsand ultrasound determined goiter in a school survey in ruralTanzania (paper V).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 45/100
Controlling IDD – Studies for Program Management
45
MATERIALS, METHODS,
RESULTS, AND COMMENTSThis thesis consists of several studies, Figure 3. A range of quantitative and qualitative research methods have been used,Table 10. The sections below present the five individual studiesgrouped into three areas related to their relevance in differentstages of the IDD control program cycle. Study I and II relate tothe assessment stage, study III to the implementation stage, andstudy IV and V to the evaluation stage. For each of the threeareas material and methods are presented, results summarisedand briefly commented on.
Table 10. Summary of research methods used in this thesis.
Method Paper I Paper II Paper III Paper IV Paper V
Epidemiology& Biostatistics
Biochemicalanalysis
Qualitativemethods
Cost analysis
Modeling of secondary data
Assessing Iodine Deficiency and GoitrogenicEffects (paper I,II)
Having arrived in the Central African Republic to study healtheffects of cassava (Tylleskär et al. 1994), I was struck by finding agoiter in every other child I examined. Since the country isextremely dependent on cassava the potential goitrogenic effectscould be considerable as an explanatory factor. Theepidemiological indicator urinary I/SCN ratio had been proposedto assess the presence of the potential goitrogenic effects
(Delange et al. 1980). A considerable scientific debate has

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 46/100
Stefan Peterson
46
addressed the issue (Bourdoux et al. 1978; Bourdoux et al. 1980;Cliff et al. 1986a; Delange & Ahluwalia 1983; Delange & Ermans1971; Delange et al. 1982; Gaitan 1990). However, the question of
the goitrogenic effect’s practical importance for iodine deficiencycontrlp efforts at population level and the utility of the I/SCNratio for assessment of potential goitrogenic effects was unclear.
Materials and Methods
In study one, cassava processing practices were elucidated in tworural and one urban setting using focus group discussions andparticipant observation (Khan & Manderson 1992; Scrimshaw &
Gleason 1992). A 24 hour dietary recall was made in 20 randomlyselected households to establish the importance of cassava in thediet (Cameron & Van Staveren 1988). Casual urine samples werecollected for analysis of iodine and thiocyanate in adults in theinterviewed households as well as among school children in thelocal school in each community. Samples were immediatelyfrozen until they were analyzed in Sweden for iodine by amodified Sandell−Kolthoff method (Sandell & Kolthoff 1937) andfor thiocyanate (Lundquist et al. 1979), respectively. All goitergradings were performed independently in triplicate according to
Perez et al. (1960). In case of differences, consensus on grade wasreached after discussion. The iodine/thiocyanate-ratio (I/SCN)(Delange et al. 1980) was calculated as the mean, median, andmode of the individual samples' ratios obtained through thedivision of each iodine-concentration (Φg/dl) by the samespecimen's thiocyanate-concentration (mg/dl).
In study two, a literature review was carried out for use of the I/SCN ratio. The Central African Republic study andadditional data from Tanzania were re-analyzed according to the
various practices identified in the literature.Results
All three Central African communities studied were iodinedeficient, as judged by urinary iodine concentrations. All threestudy sites depended on bitter cassava as the main staple. Bittercassava was the dominant staple consumed in all households.However, processing practices differed between the communities,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 47/100
Controlling IDD – Studies for Program Management
47
with a recent introduction of a shortcut processing method in awestern village, see Figure 4. In semi-urban Bangui cassava wasbought already processed from the village.
Traditional
Shortcut(Western village)
1st night 2nd 3rd 4th 5th 6th
Soaking
Sun-drying Pounding
Basket fermentation
Crushing with machete
Mashing
TraditionalTraditional(Central village)
Legend
Figure 4. Cassava processing practices in the two rural areas of CAR.
This change in processing practices resulted in tripled urinarythiocyanate levels compared to the low levels where traditionalprocessing or traded cassava products were consumed. Associatedwith this was a near doubling of the goiter rate indicating apossible goitrogenic effect, see Table 11.
Table 11 Cassava processing, urinary iodine and thiocyanate and goiter rates in thestudied populations______________________________________________________________________________
Western Village Central Village Bangui
Cassava processing shortcut traditional tradedproducts
School Population School Population School
I g / dlmean ± SEM 6.98±0.73 10.80±2.21 6.17±0.81 5.76±0.45 6.30±4.21median 5.78 4.57 4.19 4.45 1.65n 48 84 47 103 61
SCN mol / lmean ± SEM 239±19 231±17 48±8 81±9 65 ±6median 232 186 31 57 57n 48 84 47 103 61
Crude TGR(%) 51 50 28 28 22
95% Conf.Int. 43-59 38-62 20-36 18-38 16-28n 152 72 101 95 184

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 48/100
Stefan Peterson
48
0
5
1 0
1 5
2 0
2 5
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8 5 4 6 0
Urinary I/ SCN ratio (µg/ mg)
Ce n t r al Sc h oo l
> 6 0
m ode 1 5 - 1 7 . 9
me dian 2 2 .7
me an 3 1 . 0
0
5
1 0
1 5
2 0
2 5
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8 5 4 6 0
Urinary I/ SCN ratio (µg/ m g)
W e st e rn Sch oo lmode 0 - 2 .9
me an 7 . 4
m edian 5 . 6
Figure 5. Distributions of urinary Iodine/Thiocyanate ratios in two groups of Central African schoolchildren.
The mean I/SCN ratio failed to indicate the possible
goitrogenic effect in the western area using the postulated cut-off < 3 g /mg, see Figure 5.
.
n
n

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 49/100
Controlling IDD – Studies for Program Management
49
The literature review in paper II revealed that the ratio is poorlydefined. It has been calculated in several different ways yielding
widely different results, namely as averages of individual ratios:
mean I/SCN (Hennart et al. 1982) and median I/SCN
Mathematically expressed as:
I1 In( _________ + ... +________ ) SCN1 SCNn I1 In
mean_________________________
OR median (________
..._________
)n SCN1 SCNn
and as ratios of group averages:
mean I/mean SCN (Delange 1980) and median I/median SCN (Konde et al. 1994)
Mathematically expressed as:
∑ ( I1-n )( _____________ )
n median ( I1-n )_____________________ OR ___________________________
∑ ( SCN1- n) median ( SCN1-n )( ______________ )
n
Using material from the western part of the Central African
Republic and from Tanzania the four different options werecalculated, Table 12. These different approaches yield differentresults varying by a factor of 2 to 4. This is partly explained bythe effects of skewed distributions. Furthermore, it can bemathematically shown that the ratio obtained from the groupmeans gives larger weight to the individual ratios with high SCNvalues, causing this mean to be lower than the mean obtainedusing individual ratios.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 50/100
Stefan Peterson
50
Table 12. Comparisons of urinary I/SCN ratios calculated in different ways fordata from the Central African Republic (CAR) and Tanzania.
CAR Tanzania
n=132 n=217 Averages of individual I/SCN ratios
Mean g/mg (±SEM) 10.1 (±1.7) 35.0 (±10.0)Median g/mg 5.2 9.4
Ratios of group I/SCN averagesMean g/mg 6.9 7.5Median g/mg 4.2 8.7
Crude Goiter Rate 47% 59%
I ( g/dl)mean (±SEM) 9.4 (±1.4) 5.6 (±0.4)median 4.8 3.6
SCN (mg/dl)mean (±SEM) 1.4 (±0.08) 0.74 (±0.08)median 1.1 0.41
There are also physiological limitations in the use of theratio. Above the kidney threshold for thiocyanate re-absorptionaround 1.5 mg/dl, the urinary thiocyanate concentrations are notlinearly related to the serum concentrations that could exert thepossible antithyroid effect (Bourdoux 1995; Rosling 1994). Theratio will also be affected by the 10-12 fold seasonal variation of thiocyanate concentrations (Casadei et al. 1990).
Comments
We found that parts of the Central African Republic are severelyto moderately affected by IDD and that goitrogens frominsufficient cassava-processing covaries with increasedprevalence of goitre (Peterson 1994). This covariation hassubsequently been confirmed by others (Biassoni et al. 1998).However, the main cause of the observed goiters is iodinedeficiency. Distributing iodine should be the main priority as itcan overcome the possible thiocyanate effects (Delange et al.
1994; Gaitan & Dunn 1992). Promotion of effective cassavaprocessing can complement iodine distribution, but it should not

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 51/100
Controlling IDD – Studies for Program Management
51
delay the initiation of the iodine supplementation. Effectiveprocessing of cassava is associated with much lower urinarythiocyanate levels. This has subsequently also been
demonstrated in West Africa (Bilabina et al. 1995). There is no justification to discourage the consumption of cassava from anIDD point of view and continued studies of goitrogens during theassessment stage of an IDD program can detract from thenumber one priority − to distribute iodine.
The iodine/thiocyanate ratio has mathematical andphysiological shortcomings. Its further use should bediscouraged. It is recommended to judge absolute iodine andthiocyanate levels independently instead of combining them into
a ratio, which obscures the absolute levels (Figure 1).
Distributing Iodine (paper III)
Iodine can be distributed in many ways. Many countries haveincluded IOC in their iodine supplementation programs butTanzania has to our knowledge had the most extensiveexperience. While many studies have examined IOC efficacyusing different doses and time intervals, the literature does notcontain any information on large-scale supplementationprograms’ coverage and cost. We set out to determine theproportion of targeted person-time effectively covered according toprogram objectives, as well as the cost and effectiveness of different strategies to distribute iodised oil capsules to targetedpopulations.
Materials and Methods
In study three, we examined 57 distribution rounds of iodized oilcapsules from 1986 to 1994 in 27 Tanzanian districts with a totalpopulation of 7 million. We reviewed IOC distribution reportsand administrative records, interviewed past and presentprogram managers, and conducted supervision visits to selecteddistricts. The primary and secondary data was analyzed using acomputer spreadsheet model for the proportion of targetedpopulation-time covered as outlined in Figure 6.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 52/100
Stefan Peterson
52
2 years delay of repeat
Time
firstdistribution
repeatdistribution
uncovered
covered covered covered T a r g e t
p o p u l a t i o n
N u m b e r
o f
p e r s o n
s
Figure 6. Person-time covered in the distribution of Iodized Oil Capsules -schematic representation
From the start of district IOC distribution, the objective wasto cover everyone between 1 and 45 years of age every two years.Census data for each district was updated to the year of theanalysis, adjusted for the proportion of the population in the
target age-group, and used as denominator to calculate thecoverage in any one distribution round (Mbalilaki 1988). Themean of individual districts’ distribution coverages wascalculated for first and repeat distribution rounds as well as forall combined. Based on the objective to repeat distribution aftertwo years the total population-time covered was calculated(hatched areas in Figure 6). This covered population-time wasdivided by the total population-time targeted (total area undercurve in Figure 6) to yield the population time covered according
to program objectives.For the 20 distribution rounds in 1992-93 a detailed reviewwas done of the distribution strategies planned and finallyemployed. Costs were determined from a health care providerpoint of view including opportunity costs of labor and vehicles butexcluding overhead cost to the donor as well as direct and indirectcosts to the beneficiaries. Cost per dose was determined bydividing the total drug cost and the distribution cost by thenumber of doses reported ingested. Comparisons were madebetween the three distribution strategies used.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 53/100
Controlling IDD – Studies for Program Management
53
Results
Reported district distribution coverage ranged from 20% to 96% of the targeted population, with an overall mean coverage of 64%.Coverage declined over subsequent distribution rounds. Multiplelinear regression analysis suggested that coverage wassignificantly and inversely related to distribution round ( p <0.05), and positively related (not significantly) to initial visiblegoiter rate severity ( p =0.2).
Repeat distribution was not timely, occurring with a meandelay beyond target of 1.25 years. Taking also this into account,
43% of targeted person-time was covered according to programobjectives of distributing at two-year intervals. Of the person-years not covered, 42% were due to less than total coverage and58% due to delayed repeat distribution beyond the planned two-year interval.
In a sub-study of the 20 distribution rounds between 1991and 1993, we found that three different distribution strategieshad been used to organize mass distribution campaigns in oneparticular day in each village. Some districts received centralfunding for fuel and health worker per-diems in addition toreceiving the IOC. They set up a “district team” which toured thedistrict using district vehicles to organize and distribute iodinesupplements in all villages. Other districts received only the IOCand were told to integrate the distribution into Primary HealthCare (PHC). Eight out of the nine districts attempting thisdistribution strategy did not accomplish the task before thecapsules were about to expire. To ensure rapid distributionbefore expiration date, some of these districts set up a “nationaldistrict team” to facilitate iodine distribution. Staff from the
national program initiated and supported the distribution. Theseteams, using government cars, were supported with money forfuel and per-diem pay.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 54/100
Stefan Peterson
54
Table 13. Mean coverage and cost per ingested dose (2 IOC) in 1992 USD.
Distribution strategy District team PHC National+ Total
District team
No. of distribution roundsplanned 11 9 4 20
carried out and analyzed 10 1 4 15
Mean coverage 61% 56% 68% 62%
Cost of 2 IOC 0.30 0.30 0.30 0.30
Mean cost of unaccounted for IOC / dose reported ingested* 0.16 0.22 0.20 0.18
Mean management & distribution cost / dose reported ingested 0.05 0.03 0.07 0.06
Mean total cost / dose reported ingested 0.51 0.55 0.56 0.53(for 2 year duration)
The “district team” approach was the most cost effective at 51cents per dose, corresponding to an annual cost of 26 cents, seeTable 13. The analysis was driven by the lower proportion of IOCunaccounted for under this approach. This finding was fairlyinsensitive to different assumptions on the proportion of unaccounted-for IOC actually wasted. The cost analysis explainsthis by revealing that the cost of the oil capsules constitute morethan 90% of program cost at current coverage levels, Table 14.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 55/100
Controlling IDD – Studies for Program Management
55
Table 14. Cost profiles for iodized oil capsule distribution in a district using"district team" distribution and for the Expanded Program on Immunization.
Programs Iodized oil capsule Expanded Program ondistribution Immunization
IOC/vaccine 92% 10%Transport 3% 13%Social Mobilization 5%Labour 2% 42%Equipment NA 13%Building and other costs NA 5%Mgmt, training and supervision 3% 12%TOTAL 100% 100%Coverage 63% 80%
Source: Mbozi district distribution report and Bateson (1992).NA: Not applicable and therefore not costed.
Comments
The tendency for distribution coverages to decline oversubsequent distribution rounds has been observed previously
with Vitamin A distribution campaigns (West & Sommer 1987). Itis attributed to “program fatigue” among health workers (Greiner1991) and the emergence of rumors that the IOC was a secretlypromoting “family planning” or other schemes to control thepopulation (Magambo et al. 1990). Although the difference wasnot significant, the tendency towards higher population coveragein places with more visible goiter suggests that populationmotivation is higher in such places and that IOC, and possiblyother direct-contact supplementation methods, will work bestwhere the population is highly motivated. The need forinformation and communication activities to increase thepopulation’s awareness and motivation in this regard is crucial.
Control of iodine deficiency with IOC requires directinteraction with each recipient at regular but long intervals asthere is no “herd immunity”, such as in immunization where an80% coverage may stop transmission. In contrast, 100% of thepopulation needs to be covered regularly and timely to eliminateIDD. This was not achieved. Distribution coverage wasincomplete and delays to repeat distribution common and
substantial. In fact, there are bigger potential gains from

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 56/100
Stefan Peterson
56
reducing distribution delays than from increasing distributioncoverage. This highlights the need for proper and carefulplanning of iodine distribution in order to avoid administrative
delays and to ensure that iodine distribution occurs during anappropriate agricultural season. This has implications for thedistribution chain: the donor, the national program, the district,and the local leadership.
More intensive supervision of IOC distribution in moreexpensive distribution-campaigns is cost-effective compared tounsupervised primary health care distribution, see Table 13. The“district team” approach adds outside funds for distributionexpenses to the district and brings coverage rates up, cuts losses
of IOC, and lowers the annual cost of supplementation to USD0.26. The cost analysis explains this finding since more than 90%of the total cost is for the drug. This points out the high cost of theIOC itself at 15 US cents per capsule (1992). By comparison, a Vitamin A capsule costs only 2.8 US cents and the capsulesconstituted 40% of the total average cost for a large scaledistribution program in the Philippines (Loevinsohn et al. 1997).Providing expensive IOC to an underfunded and over-stretcheddistribution system by “integrating into Primary Health Care”may therefore have been based more on ideology than evidence.
At present drug prices there is scope for increased cost-effectiveness of IOC delivery through investments in distribution,supervision and community mobilisation rather than justdelivering an expensive drug to expire on a pharmacy shelf. Thislesson should apply also to other high item-cost healthinterventions with intermittent distribution.
Onchocerciasis control programs that annually distributeivermectin have proven to be successful when communities directthe treatments themselves. Community directed treatment is
organized in endemic areas by explaining program objectives andstrategies to the affected population. The population decides onhow to organize the distribution and, most importantly, selects itsown community-based distributors who are trained on basicprinciples of the treatment and then organize with theircommunities to treat everyone during a convenient time of theyear. Using village population lists, coverages of 82% rising overthe years to 92% have been achieved in Ecuador villages of about5,000 persons (Guderian et al. 1997). In Uganda an analysis of

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 57/100
Controlling IDD – Studies for Program Management
57
the sustainability of the distribution indicated that a significantpredictor of sustainable distribution over several years waswhether the community had chosen the distributor itself
(Katabarwa & Mutabazi 1998). Community ownership, directand visible effects of the treatment, regular availability of drugs,and community confidence in the initiative are all listed asreasons for the strategy’s success (Tarimo 2000). Lessons to learnfor iodized oil capsule distribution include the need to informcommunities and let them direct the activity in order to achievesustainability. However, this success comes at a cost, the percapita distribution cost alone was estimated at USD 0.29 toachieve an 85% coverage in a Ugandan population of 46,000
(Kipp et al. 1998).
Evaluating Program Impact (paper IV,V)
Iodizing salt is the long-term strategy chosen by most countries.WHO and ICCIDD recommended iodization at 100 parts permillion for bulk production in warm, moist climates (WHO1994a). Tanzania adopted this recommendation. Following thereports of iodine induced hyperthyroidism among older subjectswith large goiters WHO lowered the recommendation to 20-40ppm and suggested confirmatory surveys of urinary iodine toensure a median of 100-200 g/l (WHO 1996). Such surveys arecustomarily done in school-children, yet even more vulnerabletarget groups are the pregnant woman, the foetus and thenewborn. However, no biological indicators are usually assessedin these groups of prime beneficiaries due to logistical difficulties(WHO 1997). Yet knowing their status and relation to school-children’s indicators is critical before taking a decision to change
salt iodine content. We studied the relation of iodine deficiencyindicators in different vulnerable groups in a Tanzaniancommunity with full coverage of salt presumably iodized at 100ppm at its site of production.
A convenient marker of the last years’ iodine status in acommunity is the distribution of thyroid sizes in schoolchildren(Aghini-Lombardi et al. 1997). This indicator is then used as amarker for the likely presence of other, more serious disorders

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 58/100
Stefan Peterson
58
such as cretinism and infant deaths as well as a summaryindicator of the adequacy of the iodine supply (Dulberg 1985). A number of different classification systems exist for grading
thyroid size using palpation or ultrasound. In addition to thereduction in number of goitre grades, the 1994 WHO palpationsystem implies a change in definition of what constitutes a“goiter”. Furthermore, ultrasound estimation of thyroid volumehas been recommended as more precise and objective thanpalpation (WHO 1994a). We studied the implications of thechange in palpation goitre definition and compared theobtainable precision using palpation with that of ultrasonicestimation of thyroid volume in a goiter survey in rural Tanzania.
Material and Methods
Relation of outcome indicators and target groups (paper IV)We studied the iodized salt distribution coverage and iodinestatus in different vulnerable groups in Ilembula village in theseverely iodine deficient Njombe District (Wächter et al. 1986;Wächter et al. 1985), where iodized salt had been available for 1-2 years (Sundqvist & Wijetunga 1996). We surveyed village saltiodine content twice during one month using rapid test kits for
household and school-children’s samples and titration for retailsamples (Sullivan et al. 1995). Thyroid size was graded accordingto Perez et al. (1960) in school-children and women in householdsand delivering at Ilembula Hospital. Two examiners gradedindependently and settled differences in grade through re-examination and discussion. Urinary iodine concentration wasmeasured in schoolchildren and women at delivery. Cord bloodwas collected on filter paper from consecutive deliveries andfrozen at minus 20 until analysed by the Neonatal Delfia
technique at the National Swedish Hypothyroidism laboratory.The iodine deficiency indicators collected in the different groupswere evaluated against WHO severity “benchmarks”, see Table 9(WHO 1994a).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 59/100
Controlling IDD – Studies for Program Management
59
Goiter definition (paper V)In this study three independent, blinded examiners did doubleestimation of thyroid size with the old and new palpation
classification systems in 225 primary school children in ahighland Tanzanian village. Palpation results were compared todouble ultrasound estimation of thyroid volume according toBrunn et al. (1981 and Delange et al. (1997). Kappa values werecalculated as measures of agreement. Logistic regression wasused to study the influence of ultrasonographically determinedthyroid size parameters on whether a palpator considered a childgoitrous or not. Using ultrasound “goiter” by WHO cutoff valuesas gold standard the sensitivity and specificity of the two
palpation systems was calculated (WHO & ICCIDD 1997).
Table 15. Iodine deficiency (ID) indicators and WHO severity grading in differentpopulation groups (WHO 1994a)
School- Household Women at Neonateschildren Women Delivery
n 60 25 111 123
Total Goiter Rate (%) 62 52 55(95% conf int) (49-74) (31-73) (46-64)
ID severity severe severe severe
Urinary iodine ( g/l)Median 140 68
<20 g/l 0 % 10 %<50 g/l 7 % 32 %<100 g/l 28 % 62 %
ID severity none mild
TSH (mU/l whole blood)Median 1.5
>5 mU/l 25 %>7.5 mU/l 15 %>10 mU/l 10 %
ID severity moderate

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 60/100
Stefan Peterson
60
Results
In Ilembula village semiquantitative test-kits indicated that 98%
of household salt-samples contained iodine at 25 ppm.Twentynine retail samples had a median titration iodine contentof 27 ppm (range 11-127), but only 17 % complied with thenational recommendation (>37 ppm). Thus almost all salt fromhouseholds was commercially produced and iodized during thestudy month, although at relatively low levels. Iodine deficiencyindicators and their severity grading are given in Table 15.
Goiter rates indicated “severe“ iodine deficiency in all groupsexamined suggesting delayed goiter regression since median
urinary iodine in the school-children was normal. However,irrespective of whether the delivering women came from the localward, local or neighbouring district cord-blood TSH and urinaryiodine indicated “moderate“ and “mild“ ID, suggesting that theneonates were still at risk of brain damage.
Our comparative study of the two palpation systems and the"gold standard" ultrasound demonstrated that the recent changein goiter definition entailed an increase in estimated goiter ratesby up to 25% in the studied population. This is explained by the
effective lowering of the cut-off between a normal thyroid and a“goiter”, Table 3. This has major implications for follow-upstudies using the new classification system when baselinestudies were done with the old system, such as in Tanzania. Atglobal level the number of IDD affected will increase considerablydue to the combined effects of lowering the cut-off for goiter anddecreasing the acceptable prevalence to 5%. Furthermore, thelowering of the cut-off for goiter decreases specificity to a level of around 30% where it becomes impossible to demonstrate
elimination of IDD with the new classification system due to falsepositives, Figure 7.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 61/100
Controlling IDD – Studies for Program Management
61
WHO 1960 System
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0% 20% 40% 60% 80% 100%
WHO 1994 System
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0% 20% 40% 60% 80% 100%
True Goiter Rate
True Neg
False Neg
False Pos
True Pos
Measured Goiter Rate
True Goiter Rate
Measured Goiter Rate
Figure 7. Graphical illustration of goitre criterion performance using body-surface normated thyroid volume by ultrasound determined goiter as goldstandard in 225 primary school children in highland Tanzania. Palpationusing WHO 1960 criterion: sensitivity 56%, specificity 76%. WHO 1994
criterion: sensitivity 80%, specificity 29%. After Taube 1986.
There is considerable random misclassification of goiter statusupon repeated palpation which, however, results in minimalchanges in estimated goiter rates, see Table 16. The level of reclassification in palpation with a kappa value of 0.57 is veryclose to the result for ultrasound, 0.63 indicating similar precision.Palpation is more influenced by thyroid width than by thyroid
length or depth, while ultrasound estimates all three parametersequally. Ultrasound estimation of thyroid volume is demonstratedto be imprecise due to measurement error and lobe shapedeviation from the ellipsoid form. This results in a wide confidenceinterval where the 95% confidence interval for an estimatedvolume of 10 ml is ±4 ml. Converted to a goiter rate this results inconsiderable random misclassification making ultrasound, likepalpation, unreliable at the individual level but reliable atpopulation level as long as the misclassification is random.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 62/100
Stefan Peterson
62
Table 16. Intra-rater variation. Cross-tabulations of repeated palpation(examiner A) and ultrasound determinations of total goitre rate in 225
primary school children in highland Tanzania. Number of children and (TotalGoiter Rate).
Examination Results
First round GoiterSecond round Goiter No Yes TOTAL R
e c l a s s i f i c a
t i o n P r e v a l e n c e
D i f f e r e n c e
K a p p a *
Palpator A No 90 23 113(WHO'60) Yes 25 87 112 (50%)TOTAL 115 110 225 21% 1% 0.57
(49%)Palpator A No 33 21 54
(WHO'94) Yes 16 155 171 (76%)TOTAL 49 176 225 16% -2% 0.53
(78%)Ultrasound No 41 17 58
Body surface Yes 14 153 167 (74%)
Normated TOTAL 55 170 225 14% -2% 0.63(76%)
* Labelling of agreement according to (Altman 1991): kappa <0.2: poor; 0.21-0.4: fair; 0.41-0.6: moderate; 0.61-0.8: good; 0.81-1: very good
Comments
The study of outcome indicators revealed that while all the saltwas iodized the iodine concentrations varied greatly at retaillevel indicating either poor quality of iodation or that large losses
of iodine had occurred during transport and storage. We foundthat, while an assessment of the easily accessible andcustomarily evaluated school-children showed adequate or evenslightly high urinary iodine, other vulnerable groups laggedbehind. Women at delivery showed signs of inadequate iodinestatus and goiter, although the relation between iodine intakeand thyroid hormone status in pregnancy is not clearcut andpregnancy-induced changes cannot be ruled out (Elnagar et al.1998; Eltom et al. 2000b). However, newborns showed signs of
thyroid stress indicating a high turnover rate of the littleavailable iodine (Delange 1998). Hypothyroidism, even if

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 63/100
Controlling IDD – Studies for Program Management
63
transient, has been linked with negative effects on schoolachievement and cognition (Huda et al. 1999) and our findingssuggest that the important target group of neonates may still be
at risk of brain damage at the iodine levels found in the study.The findings could be explained by insufficient time since theintroduction of iodized salt, or that current salt iodine levels athousehold level, while sufficient for school children, may havebeen inadequate for other vulnerable groups.
In addition our study demonstrated that goiter regressionmay be delayed in all groups compared to thyroid hormone andurinary iodine levels necessitating longer periods before goiterreassessments to allow time for new "iodine replete" cohorts of
school-children to replace the formerly iodine-deficient children(Aghini-Lombardi et al. 1997; Zhao et al. 1999).It remains to be seen whether universal salt iodization is
feasible in countries with widespread small-scale salt productionor whether integration with other control methods, such as IOC,will be necessary to achieve elimination of IDD. However, onceiodized salt is available in sufficient quantities appropriatemonitoring is necessary to adopt international recommendationson salt iodization levels to local circumstances in order to avoidside effects of excess iodine intake. In evaluating the prevalenceof iodine induced hyperthyroidism, it should also be noted thatalready while the iodine deficiency continues the prevalence of IIH is twice that of iodine sufficient communities (Aghini-Lombardi et al. 1999). It is important to monitor salt iodineconcentrations during production and distribution down tohousehold level, as well as to assess iodine status with improvedindicators in all vulnerable groups in the local setting, beforeadapting international recommendations on new iodizationlevels at production. Measures also need to be put in place to
reduce variations in salt iodine content during production. Varying salt iodine content may not only be a risk factor for IIHbut also to reduce the effectiveness of iodized salt in reducingthyroid volume (Zhao et al. 1999).
For goiter surveys in settings where ultrasound surveys arenot feasible, we find that appropriately trained palpators usingthe old WHO classification of goiter remain "good enough" tomonitor elimination of iodine deficiency by the goitre criterion.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 64/100
Stefan Peterson
64
However, an allowance for a 10% acceptable prevalence must bemade. This 10% cut-off should be applicable for palpation surveysonly, to allow for the 10% false positives that result from a
specificity of 90% which seems to be the typically attainableperformance using the Perez criterion reaches (Smyth et al.1999). It is, however, not an argument against the lowering of thecutoff for true prevalence of goiter to 5%. However, it should benoted that applying the new palpation criterion and the lower 5%cutoff doubled the estimated number of goitrous individuals inthe world from 2-300 million to 686 million. The populationconsidered at risk of iodine deficiency simultaneously rose from1,000 to 1,600 million (Clugston & Bailey 1996; Dunn & van der
Haar 1990; Hetzel 1988; WHO/UNICEF/ICCIDD 1993).Subsequent additions have increased the population consideredat risk to 2.2 billion −more than one third of the world’spopulation− and the number of goitrous to 740 million (WHO1999).
The differences between 225 repeat ultrasoundmeasurements in our study were larger than errors reported fromsmall validation exercises elsewhere (Foo et al. 1999;Zimmerman et al. 2000). However, the attainable precision inlarge-scale routine surveys in remote low-income country settings
has not been determined before. Our findings in support of thecontinued utility of palpation are important sinceultrasonography is technically difficult and costly to use in theremote highland regions of low-income countries where IDD islikely to linger.
The findings also demonstrate the importance of clarity of definitions in epidemiology and the need to avoid inadvertentoversights, such as the effective lowering of the goiter definitionin the 1994 ICCIDD/WHO publication which effectively rendered
palpation useless with its low specificity (WHO 1994a). It issuggested that using the research publication process with peer-review to scrutinize major changes may help in this regard.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 65/100
Controlling IDD – Studies for Program Management
65
GENERAL DISCUSSION
Elimination, not Eradication
Joint international and national efforts focusing on saltiodization has made remarkable progress towards reducingiodine deficiency in the last decade. Presently 63 out of 99reporting countries claim that more than 50% of their householdsconsume iodized salt and in 26 countries the reported levelreaches 90% of the households (UNICEF 2000). However, thebattle is not won and the issue of sustainability is critical. A
nutritional deficiency like IDD will never be eradicated in thesame way as smallpox was. Supplementation needs to besustained forever or else iodine deficiency will return (Dunn1998). To control iodine deficiency, each and every member of thedeficient community needs to be reached regularly with theintervention as, unlike immunizable diseases, no “herdimmunity” is provided when the large majority of the targetpopulation is covered. Yet another difference between the majorinfectious and nutritional disorders among poor populations isthat nutritional deficiencies constitute no threat to the affluent
populations of the world, whereas infectious diseases do.During the last decade iodine deficiency control programs
have been initiated in most low-income countries withconsiderable external support. In the case of Tanzania, this hasamounted to 80% of the program budget (Sanga 1994).Sustaining such high levels of support seems unlikely. Theinterdependence between countries is not as important for IDDas with infectious diseases such as smallpox, polio, or measles(Dayrit 1998). Over time the manifestations of IDD may also
disappear making the perceived need for iodine supplementationless obvious (Alnwick 1998).The need to build an iodine deficiency control program that is
sustainable is crucial no matter what iodine distribution systemis set up. This also applies to the communication, monitoring, andenforcement systems. The experience from Tanzania isilluminating in this regard. The responsibility to monitor theprogram is divided between several ministries. Monitoring theproduction sites is the responsibility of the Ministry of Water,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 66/100
Stefan Peterson
66
Energy and Minerals (MOWEM) and their regional miningofficers. However, a 1998 assessment found that they have notbeen supervised since 1995 (Carlsson et al. 1999). Although both
the central Ministry and the zonal officers were supplied withvehicles for site monitoring, these visits were not taking place,except when donor-funded and then at a high cost. A subsequentvisit by TFNC to the southern salt producing region revealed thatno monitoring was taking place at the production sites and thatthe supervision vehicle had been sold (Assey et al. 1998).
Monitoring of the distribution process is the responsibility of the National Food Control Commission, Ministry of Health. Whilethis monitoring initially worked relatively well it is now largely
not performing, or at least not reporting, since outside fundingstopped (Assey et al. 1998). Now only household monitoringcontinues under the direction of the Tanzania Food and NutritionCentre, also largely dependent on external funding.
Sustainability issues apply also to the internal monitoringprocess at the salt factories. While the larger ones were equippedwith titration equipment, site visits have not given evidence of regular use of this equipment or regular use of a quality controllogbook. Use of rapid test kits seem more widespread but is alsoless accurate, providing essentially an indication of whether
iodine is present or not (Carlsson et al. 1999). In summary,internal and external salt production quality control systemsbroke down, the distribution monitoring started well but hasdeclined; although household monitoring has partially continued,the monitoring process does not fulfill the adequacy criteria, seeTable 8.
As for the actual production of iodized salt, the donation andinstallation of the iodization machines was the beginning of newprocedures. Previous to iodization, salt could be packed directly
into sacks on the salt pan and then taken straight for sale orstorage. Iodization increases the number of production stepsthereby increasing the salt price or decreasing the profit margin.In small salt producing co-operatives, the relative costs fortransporting the salt to the iodation plant and producing iodizedsalt is likely to be even greater than in large operations, perhapseven exceeding the profit. Careful analysis of the economicconsequences of salt iodization is crucial for sustainability.
The technical challenges include both installation and

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 67/100
Controlling IDD – Studies for Program Management
67
maintenance of the iodization equipment. In many settingsmachines have never been installed due to expense or technicalunsuitability of the equipment. Where installed, upkeep of
machines has proven difficult to organize. Following machinebreakdowns, new more sustainable ways of iodizing werepioneered using a hand spray pump to put iodine on salt heapswith subsequent manual mixing (Assey et al. 1998). This methodseems to be more sustainable for iodization in low cost settings,but the quality of the iodization has yet to be evaluated.
While the Tanzania salt producers’ association was chargedwith distributing iodization machines, potassium iodate andspecial lined bags, this body has not functioned well. There is
dissatisfaction among producers with the association’sfunctioning as a discussion forum and in giving access toiodization machines and potassium iodate. In fact, the lack of asustainable source and mechanism for re-supply of potassiumiodate is one of the major constraints cited by salt producers. Theoriginally donated stock of labelled, lined polyethylene bags wassoon used up and then largely replaced by second-handunmarked bags (Carlsson et al. 1999). These constraints areshared by salt traders from other countries. A Mombasa workshopfor salt producers from 13 Eastern and Southern Africancountries identified the main barriers to effective salt iodization:the lack of monitoring systems; ineffective enforcement; theexistence of taxes and duties on iodine; legal trade barriersbetween countries; and the large number of small scale saltproducers who lack technical skills and resources (Kwena 2000).
Yet Tanzania has made great advances in controlling iodinedeficiency. The preliminary findings from schools surveys in 16endemic districts indicate sufficient to high urinary iodineconcentrations in all but 2 districts (Kimboka 2000). While the
challenges to uphold and finetune this success are many, thisstudy concurs with a recent evaluation of the IDD program inconcluding that the main priority in the current Tanzanianresource-constrained situation is to put a salt iodizationproduction and monitoring system in place, starting in thefactories. It was suggested that this will require commitment,accountability, and organizational changes in the concernedgovernment agencies and NCCIDD as well as a more proactivesecretariat (Carlsson et al. 1999).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 68/100
Stefan Peterson
68
Monitoring does not equal Evaluation
Monitoring and evaluation are presented together as the last step
of the global IDD control strategy (Hetzel 1987b; Hetzel 1988). Inthe latest published version of the IDD “social wheel,” monitoringdoes not appear, presumably this was inadvertently left out,Figure 2 (Hetzel 1996). Be that as it may, the tendency to see“monitoring and evaluation” as the same is widespread inacademic medicine and public health and to the disadvantage of both concepts. Monitoring and evaluation are different activities(Barutwanayo et al. 1993; Rubin 1995; UNICEF 1990), see Box 1.
Box 1. Definition of terms. Adapted after Barutwanayo et al. 1993; Rubin 1995;UNICEF 1990.
Monitoring a continuous activity to measure the process of carrying out activities for program implementation(also called implementation evaluation or processevaluation)
Evaluation a periodic assessment of a program’s outcomes andimpact (effectiveness evaluation). It may alsoprovide information on effectiveness, efficiency,
and sustainability
Effectiveness a measure of the extent to which originalobjectives have been achieved
Efficiency an economic term measuring the cost at which theobjective was achieved
Efficacy an intervention’s effect under ideal circumstances,
typically determined in controlled clinical trials
It has been suggested that monitoring findings suggestingpossibilities of impact should precede any impact evaluation(Greiner 1997). This seems logical. If you have no monitoring datasuggesting that the intervention has reached its targetedpopulation, why should you spend resources to evaluate impact? An evaluation, when carried out, should first validate themonitoring findings and second reassess the situation both interms of outcomes, such as changes in behaviors and laboratory

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 69/100
Controlling IDD – Studies for Program Management
69
parameters, and in terms of impact, changes in morbidity andmortality (Barutwanayo et al. 1993). Similarly, for obstetricservices it is suggested to monitor availability, utilization, and
quality of the service as process indicators before measuringmaternal mortality (Koblinsky et al. 1994; Maine et al. 1997).Moreover, the monitoring information will help the interpretationof the impact findings, thus opening up the “black box” research of evaluating impact alone in the absence of any explanatoryinformation on the implementation process (Rossi & Freeman1993).
Defining the implementation process
The widespread practice of confusing monitoring with evaluationand to concentrate on measuring impact indicators may reflectthe tendency for nutrition programs to concentrate more on “whatto do” than on “how to do it” (Field 1985). There is a need to focusattention on the implementation process since any intervention isdependent on a favorable programmatic context to translate itsobjectives into community effectiveness. While any oneintervention has a certain efficacy under controlled conditions,the process of implementing it in a program has a number of
steps that are contingent upon each other to produce the desiredoutputs, outcomes, and impacts. For curative care these stepshave been outlined as a formula (Tugwell et al. 1985).Community effectiveness is the multiplicative combination of conditional probabilities of efficacy, diagnostic accuracy, healthprovider compliance, patient compliance, and coverage. Assumingindependence, Tugwell suggests the following calculation:
Community effectiveness = Efficacy x Diagnostic accuracy x
Health provider compliance x Patient compliance x CoverageFor a supplementation or fortification program applied to an
entire population, diagnostic accuracy does not apply. Coveragetranslates into access to the intervention and health workercompliance translates into quality of the intervention whilepatient compliance remains. Thus the components:
Community effectiveness = Efficacy x Access x Quality xCompliance

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 70/100
Stefan Peterson
70
This formula demonstrates that even if the efficacy is 100%given 50% access, 50% acceptable quality and 50% compliance,the resulting effectiveness is only 12.5% in spite of the impressive
efficacy. An intervention with lower efficacy may even result inbetter community effectiveness if it is easier to implement andsustain. While the assumption of independence may not fullyapply, and the reduction in effect may be overstated, thecalculation gives the rationale for focusing on “the how” of anintervention and not just “the what” (Field 1985).
This realization is manifested in the evaluation literature’srecommended practice of describing a program’s “logical model” asa basis for planning and subsequently evaluating an intervention
(Goodman 1998; MMWR 1999; Moyer et al. 1997). A logic modeldescribes the complete sequence of events for bringing aboutchange, often in the form of a flowchart. This chart can also spellout infrastructure requirements and interrelationships. The logicmodel promotes discussion and clarification of the program’sstrategies, thus focusing and improving the program design(MMWR 1999).
Box 2. Definition of terms for monitoring and evaluation. Adapted afterBouchet; DiPrete-Brown et al. 1998; Levinson et al. 1999.
Input Funds, materials, goods, training and actionsnecessary for project activities
Process The way activities must be carried out to achieve theproject outputs
Output Provision of project goods and services to the targetpopulation; the primary project deliverables
Outcome Intermediate change in the condition, behavior orpractice of the target population
Impact Changes in the occurrence of targeted conditions inthe target population
Benefits Effects resulting from the impact, usually incombination with other factors

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 71/100
Controlling IDD – Studies for Program Management
71
The use of flowcharts or tabulations of steps is also part of theQuality Assurance practice. Quality assurance sets standards andguidelines, communicates them, and then monitors and tries to
improve performance in relation to these standards (DiPrete-Brown et al. 1998). Taking a “systems view” of the programstandards, indicators and thresholds are set for inputs, processes,outputs, outcomes, and impact, see Box 2 and Figure 8.
Monitoring
Monitoring focuses on inputs, processes, and outputs. Using themodel in Figure 8, a system for collecting and compiling dataneeds to be designed as the program’s Management InformationSystem (MIS). By using the MIS to compile required monitoringdata, the information can then be analyzed and used to guideprogram decision-making for improved performance (Bouchet;DiPrete-Brown et al. 1998; Rossi & Freeman 1993). During theanalysis it is important to prioritize and focus interventions onthe main “bottlenecks” identified in the flowchart or systemsmodel (DiPrete-Brown et al. 1998; Maine et al. 1997).
Evaluation
Most interventions aim to influence morbidity and mortality bychanging proximate determinants, e.g. to reduce cretinism andgoitre by getting all households to regularly consume adequatelyiodized salt. The program’s outputs to achieve this is iodized saltproduction and distribution all over the country as well as healtheducation to enlighten consumers on the importance of usingiodized salt. It is then assumed that these outputs will translateinto outcomes in the form of consumers buying and using iodised
salt and getting adequate iodine intake, see Figure 8. Based onthe scientific literature, it is also reasonable to make theassumption that adequate iodine intake will then translate to thedesired impact in terms of actual morbidity/mortality reductions.Therefore, once monitoring has indicated an adequate output, e.g.good coverage with adequately iodized salt, then the evaluationcan be limited to validate the monitoring findings (output) and toevaluate the outcome and impact (Levinson et al. 1999).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 72/100
M O N
I T O R I N G ( e x t e n d s t o o u t c o m e s )
E V A L U A
T I O N ( s t a r t s f r o m o u t p u t s )
____ ___ ___ ___
___ ___ ___ ___ ___ ___ _____ ____________________________________
_____________________________________________________________ ___ _
__ ___ ___ ___ ___ ___ ___ ___ ___
_____________
__________________________________________________________________
__________________________________________________________________
____________________________________________ ___ ___ ___ ___ ___ _
__ ___ ___ ___ ___ __
I N P U T
O U T P
U T
O U T C O M
E
I M P A C T
B E N E F I T S
C o n s t
a n t s u p p l y o f
p o t a s s i u m i o d a t e
R e d u c t i o n i n
i m p a i r m e d b r a i n
d e v e l o p m e n t
H u m a n a n d
E c o n o m i c
D e v e l o p m e n t
F u n c t i o n a l i o d i z a t i o n
m a c h i n e
P o t a s s
i u m i o d a t e
a d d e d
t o a l l s a l t u s i n g
i o d i z a t i o n m a c h i n e f o r
m i x i n g
I o d i z e d s a l t p r o d u c e d
i n s u f f i c
i e n t q u a l i t y ,
q u a n t i t y a n d w i t h
a d e q u a t
e p a c k a g i n g
A d e q u a t e i o d i n e
i n t a k e
( a s s e s s e d a s
u r i n a r y i o d
i n e )
T h y r o i d s i z e
r e d u c t i o n
Q u a l i t y c o n t r o l
l a b o r a t o r y
T i t r a t i o n s a m p l e s
t a k e n d a i l y
I o d i z e d s a l t
d i s t r i b u t e d t o a l l
p a r t s o f
t h e c o u n t r y
H o r m o n a l l
e v e l s
P e r i n a t a l a n d
i n f a n t m o r t a l i t y
r e d u c t i o n
T r a i n
i n g
R a p i d
t e s t k i t s u s e d
h o u r l y
P a c k a
g i n g m a t e r i a l
A l l s a l
t p a c k a g e d i n
l i n e d b
a g s
I o d i z e d s a l t r e t a i l e d
a p p r o p r
i a t e l y
I o d i z e
d o i l c a p s u l e s :
•
A r r i v i n g t i m e l y
•
I n s u f f i c i e n t q u a n t i t y
•
I n g o o d q u a l i t y
I O C d i s t r i b u t i o n w i t h
a d e q u a t e c o m m u n i t y
i n v o l v e m e n t a n d
s u p p o r t o f d i s t r i b u t i o n
I o d i z e d o i l c a p s u l e s
d i s t r i b u
t e d i n r i g h t
d o s e t i m
e l y a t
i n d i c a t e
d i n t e r v a l s
T a r g e t e d
p o p u l a t i o n
s w a l l o w s I O
C
M e s s a
g e s d e l i v e r e d
a d e q u a t e l y
T a r g e t e d
c o m m u n i t i e s
b u y a n d u s e
i o d i z e d s a l t
C o m m
u n i c a t i o n
m a t e r
i a l f o r :
•
I n t e
r p e r s o n a l d e l i v e r y
•
M a s
s m e d i a d e l i v e r y
K n o w l e d g e a b l e :
•
S a l t w
o r k e r s
•
W h o l e s a l e r s
•
R e t a i l e r s
•
C o n s u
m e r s
F i g u r e 8 . A s y s t e m s v i e w o f a n i o d i n e f o r t i f i c a t i o n / s u p p l e m e n t a t i o n p r o g r a m w i t h e x a m
p l e s o f i s s u e s f o r m o n i t o r i n g a n d
e v a l u a t i o n . O u t c o m e s a r e b o t h b i o l o g i c a l a n d b e h a v i o r a l . A d
a p t e d f r o m D i P r e t e - B r o w n
e t a l . 1 9 9 8 ; L e v i n s o n e t a l . 1 9 9 9 a n d
B o u c h
e t .
P R O C E S S

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 73/100
Controlling IDD – Studies for Program Management
73
However, measuring impacts such as mortality and incidence of cretinism is often more difficult and costly, while evaluation of themore proximate determinants at the outcome stage is generally
easier and cheaper to perform. Evaluation of such proximatedeterminants of impact has therefore been suggested asalternative and complementary evaluation measures (Blecher1996; Lorenz et al. 1995; Mosley & Chen 1984; van Norren et al.1989). In the case of iodine deficiency, urinary iodineconcentrations is a convenient outcome indicator. For evaluationsurveys it can be combined with the most easy to measure impactindicator, thyroid size. However, such measurements haveprecision problems whether done by palpation or ultrasound
(paper V) and goiter regression is delayed after correction of iodinedeficiency (paper IV). Other impact indicators, while occasionallynecessary to measure for validation studies, require extensivesurveys in groups that may be hard to reach (paper IV).
Modifying the “Social Wheel”
There is a good case for separating process monitoring fromevaluations of outcome and impact. Measurements of the process,outcome, and impact may all be necessary but their periodicityshould be different and measurement of process and outcome needto precede, if not replace, the more popular impact evaluations(Schrettenbrunner & Harpham 1993). Impact evaluations are alsotime-consuming, logistically challenging, expensive and yieldresults that can only be interpreted together with processindicators (paper IV). Methodological measurement errors mayalso give spurious results (paper II, V).
The need to first monitor the intervention, i.e. saltiodization, is well reflected in ICCIDD’s current Global Action plan
1999-2001 (ICCIDD 1999a) and in forthcoming WHO monitoringdocuments (ICCIDD 1999b). It is therefore suggested to stop using“Monitoring and Evaluation” as one concept in IDD strategies inorder to recognize that process monitoring is a crucial activity in itsown right. Effective monitoring requires appropriateadministrative arrangements and practical procedures. Thestrategy and “social wheel” for IDD control could reflect this byadding a smaller monitoring wheel on to the bigger one at theimplementation stage. As this monitoring wheel is a small wheel

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 74/100
Stefan Peterson
74
turning a big one it has to turn around many times while the bigwheel makes one turn, i.e. monitoring has to be done throughoutthe implementation years while program evaluation could be done
at 3-5 year intervals, see Figure 9. The same addition is needed inUNICEF’s “triple A” program cycle (UNICEF 1998).
Figure 9. Modified ”Social Wheel” of IDD control for the second and subsequentturns. Superimposed is UNICEF’s “Triple A process” and the smaller processmonitoring wheel, which turns faster than the larger program wheel. Additionalevaluation and updating tasks added. Compare Figure 2.
Adding such a “faster-turning” wheel points out theimportance of monitoring as distinct from evaluation. Thisdistinction helps clarify the steps and requirements for successful
implementation. This relates particularly to the necessarydistinction between the importance and sequencing of measuring
RE- AssessSituation
Disseminate
Findings
UPDATE
Plan of Action
MAINTAIN
Political
Will
Implementation
of Programme
EVALUATEProgram
Program functioning
Communication strategy
Outcome & Impact
indicators
Administrative
arrangements and
Partner responsibilities
ASSESSMENT
ANALYSISACTION
Output
Process InputInputs
Process
Outputs
MONITORING

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 75/100
Controlling IDD – Studies for Program Management
75
salt iodine content (output) and measuring urinary iodine(outcome). Using rapid test kits or titration on salt is an everydayevent at production and distribution level the outcome of which
should be monitored at least monthly by the IDD program office.It is part of the monitoring and enforcement process. Salttitration laboratories are required down to factory and regionallevels within countries, which is technically feasible since theyare relatively simple to manage. Instructions for sampling areavailable and should be adapted to the specific situation(Sullivan et al. 1995).
Assessing iodine intake by measuring urinary iodine,however, is an intermittent, much more complex activity, which
serves to confirm findings of adequate salt iodine content andprovide impetus for adjusting salt iodization levels. It thereforehas more a characteristic of a periodic evaluation indicator andrequires careful elaboration of sampling procedures.Furthermore, the laboratory technology for urinary iodine iscomplex. Capacity for determining urinary iodine is thus onlyrequired at national level for larger countries, or can even beshared among groups of countries, since very few countries willneed to run continuos analysis of urinary iodine levels.
The role of the community in iodine control must also bereassessed. Enrolling community based non-governmentalorganizations in monitoring and advocacy for iodized salt is onepromising avenue (Pandav et al. 1995). While public education tocreate awareness and demand for iodized salt is stressed as adeterminant of a successful program (Dunn 1996a), the currentplacement of communication in the “social wheel” as a steppreceding the intervention may need to be revised. The reason isthat communication issues also need to become part of the
program implementation concurrent with salt iodization.Communication also needs to become more relevant to differentcontexts. Attention and research needs to be devoted to defining:the different target audiences and the benefits, costs and otherbarriers that interfere with desired behaviors. These audiencesinclude actors such as the salt workers whom we want to spendthe extra energy and money to iodize all salt appropriately.Messages need to be developed that will promote these behaviorsmost effectively, and the most effective channels of

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 76/100
Stefan Peterson
76
communication need to be identified for each targeted actor(Cabanero-Verzosa 1999). Use of such strategic communicationwas highly effective in increasing consumer knowledge of IDD
and iodized salt in a campaign in Ecuador (Cabanero-Verzosa1999). Other target audiences, requiring different messages andchannels will include politicians, salt producers, salt factoryworkers, and salt retailers. This can be achieved by morecountries using the available ICCIDD communication strategy(Ling & Reader-Wilstein). An example is the recent presscampaign in India to maintain the ban on sale of non-iodised salt(CFAR 2000). Including communication as part of theintervention also implies that its delivery needs to be monitored
and its effect evaluated in the last stage of the program cycle.
Reassessing the Situation
The strategy
A combined focus on process monitoring and impact evaluationwill assist programs to reassess the feasibility of their controlstrategies during the evaluation stage. The blueprinted focus on
universal salt iodization has been largely successful in mostsettings (Kavishe 1996). Focusing attention on iodizing the salthas also been wise. Goitrogens do not merit attention until iodinehas reached the population (paper I,II). The logistics of distributing iodized oil capsules have also precluded theirwidespread use for effective mass supplementation (paper III).Most iodine deficiency control programs have now reachedmaturity and need to reassess the experience of applying thisinitial strategy. As they set out on the next turn of the control
cycle, they may need to be less dogmatic; e.g., they may need torecognize that small scale salt iodation using salt co-operativesand shared iodization machines may not be feasible in allsettings. Especially as structural adjustment towards fewer,large-scale salt producers may not be politically acceptable as itmay create soceio-economic inequalities. Programs need theflexibility to try out new economically and practically viablealternatives for special contexts. One such example is thedevelopment in Tanzania of iodization of salt in heaps directly on

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 77/100
Controlling IDD – Studies for Program Management
77
the salt pan, using portable pesticide sprayers. Studies on theperformance of such methods and other practices in use will benecessary, and form the basis for adapting new international
recommendations for iodization levels (paper IV; PAMM 1998;WHO 1996).
Ensuring sustainable and functional monitoring of saltiodization, distribution, and use is crucial to strengthen andsustain the salt iodization program (Pandav et al. 1995; Wang etal. 1997). Adequately iodized salt will then supply the largemajority of the population with iodine. The second step is then toidentify geographic or socio-economic pockets where iodized saltdoes not work. For example, iodization may not be a viable
alternative when people can access local salt supplies without theuse of a producer, when the market is dominated by many small-scale salt producers, or when there are price differences betweeniodated and non-iodated salt. In such pockets the severity of iodine deficiency needs to be assessed. If severe enough towarrant control efforts, distribution of iodized oil capsules shouldbe considered as an alternative control strategy and monitoringshould be developed. Paper III indicated that IOC distributionwas most effective where IDD was most severe and especiallywhen local health workers were facilitated to interact with thelocal communities. The final step is to devote special attention tofine-tuning the supplementation to optimally cover vulnerablegroups such as neonates, pregnant women as well as groups withspecial dietary practices.
The impact on IDD
Ultimately programs need to demonstrate their impact inreducing IDD. Some of the impacts may be difficult and costly to
measure, such as reduced incidence of cretinism or decreasedperinatal death rates. Other impacts are comparatively easy todemonstrate such as reductions in thyroid size andhypothyroidism. However, it is essential to select optimalmethods for remote and resource poor environments. Thesampling procedures and methods used ultimately depend on thehuman and financial resources available to conduct theevaluation. In countries with per-capita health expendituresaround USD 5 per year these resources are very limited. Research

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 78/100
Stefan Peterson
78
is needed to validate convenient indicators of outcome and impact(e.g., urinary iodine and thyroid size in school children) againstimpact in more vulnerable target groups (e.g., pregnant women
and newborns) that are harder to reach.Further developments in this regard could include assessingprogram impact through studying the distribution of thyroidvolumes in a community. While ultrasound measures thyroidvolume, the present interpretation of ultrasound data introducesthe same dichotomization as “goiter” by making reference to the97th percentile. This has led to considerable debate on whatshould be the cutoff (Delange 1999; Foo et al. 1999; Xu et al.1999; paper V). However, dichotomizing thyroids into “normal”
and “goiter” allows no quantification of thyroid size, nor anystatement on how far from “normal” a volume is. It is also notpossible to merge data across age, body surface area, and sexgroups. Similar to anthropometry it is thus suggested to developthyroid volume z-scores. (Foo & Mafauzy 1999; WHO 1995).
Further study will be required of the practically attainableprecision of ultrasound surveys under field-conditions andavailable budget frames. Standardization of the statisticalmethodology for assessing ultrasound measurement error willhelp in that regard. The present findings suggest that due to the
combined ultrasound measurement error and error resultingfrom the assumption of an ellipsoid thyroid shape, the estimatedvolume will differ considerably from the true volume in any oneindividual. The apparent precision may thus be largely spuriousas long as the ellipsoid approximation method is used (Brunn etal. 1981; paper V) while field adaptations of other, more precisemethods could improve the precision (Hegedüs et al. 1983).
The management structure
Most studies in this thesis have focused on biomedical aspects of methods for monitoring and evaluation. However, as programsreach their evaluation stage, it will also be necessary to evaluatethe functionality of the institutional arrangements with regardsto monitoring and enforcement. This includes the achievementsand constraints of partners on the National Control Commissionfor IDD in fulfilling their envisioned roles. While the NCCIDDwas a great step forward in putting all stakeholders around a

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 79/100
Controlling IDD – Studies for Program Management
79
table in Tanzania, it does not follow that they have the sameobjectives. The difference between the health sector and the saltindustry is not only one of different educational backgrounds, as
often pointed out in the IDD literature, but each has differentincentives and goals. The health sector needs to recognize thatthe salt industry’s primary motive and justification is to make aprofit. Effective monitoring, enforcement, and social marketing of iodized salt will assist the serious partners in that regard, whilepoor enforcement will undercut the collaborating salt industriesas non-iodizing competitors will sell 5-10% cheaper (or with acorrespondingly larger profit) in the “large volume, small profitmargin” salt business. Experience from Tanzania suggests that
the institutional arrangements for monitoring need to berearranged to give a clear and unified responsibility formonitoring of salt iodization to one body. Such unifiedresponsibility for monitoring and management has beenidentified as an essential requirement in scaling up a project to aprogram (Greene & Kevany 1994).
Donors need to see the totality of their support, so as not towaste resources overall by attempting to make marginal savings,e.g. on distribution expenses for expensive medications. Similarlywhen partners agree to co-finance an intervention, provisionsmust be made to ensure that all necessary ingredients areactually supplied in adequate quality, such as in an arrangementwhere the donor buys the drug and the government foots thedistribution bill. Competitive bidding needs to be used forpurchase of inputs and researchers can facilitate this process byevaluating comparative efficacies between interventions, e.g.Chinese and French IOC, rather than merely continuing studythe effect of giving different doses of one manufacturer’s product.
The other, equally important requirement is to set up
procedures that are within the capacity of national agencies’financial resources, especially with regards to recurrent costs(Greene & Kevany 1994). Small scale salt producers in Tanzaniaunable to sustain the cost of iodization machines, thus resortingto spraying and hand-mixing, is one example of inappropriatetechnology. Another is the inability to sustain factory monitoringof salt iodization in Tanzania in light of the excessive costs totransport officials from several ministries with considerable costfor per-diems for the necessary visits.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 80/100
Stefan Peterson
80
Continued modest donor funding also of recurrent costs forIDD control could indeed be justified as very cost-effectiveutilization of donor funds (World Bank 1993) and in line with
what was done for immunization programs. However, if international organizations and donors are careful to supportestablishment of sustainable procedures in each setting and if appropriate advocacy is done, it could become a national priorityto cover the recurrent costs of an IDD control program. At costsaround 5-10 US cents per person per year salt iodization isarguably within reach of national resources, even on a 5 dollarper capita health budget. And provide "... the highest cost-effectiveness of any health intervention available in the world
today" (World Bank 1993).

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 81/100
Controlling IDD – Studies for Program Management
81
CONCLUSIONS
1. We found that studied parts of the Central African Republicare severely to moderately affected by IDD. Goitrogens frominsufficient cassava-processing may have aggravated IDD in onearea. Although promotion of effective cassava processing may bebeneficial, such action should by no means delay theestablishment of effective national iodine supplementation.
2. The urinary I/SCN ratio failed to identify the possiblegoitrogenic effect observed in our Central African study.Furthermore, the ratio was found to be mathematically ill-defined, it has physiological shortcomings, and suffers fromseasonal variation. It is recommended to judge absolute urinaryiodine and thiocyanate levels independently rather than using aratio.
3. In IDD endemic areas not covered by iodized salt, iodized oilcapsule distribution remains an important tool to achieveelimination of IDD, provided that high coverage is achieved.However, the overall coverage achieved in Tanzania was only
43% of the targeted population time. The attempt to integrate theIOC distribution into primary health care resulted in lowercoverage than other strategies in Tanzania. The cost of the IOCconstitutes more than 90% of program costs and significantsavings can be made from reducing capsule waste. Availablefunds will be better used if distribution is focused on severelyaffected communities and a larger proportion of resources isallocated to social mobilization and organisation, labor, training,and supervision. These findings are of general relevance also for
campaign distribution of other medications with long distributionintervals in low-income countries.
4. All the salt was iodized in a highland study community.However, the iodine concentrations varied greatly at retail leveland indicated that factory quality control was insufficient or thatlosses of iodine during distribution had been larger than expected.The easily accessible and customarily evaluated school childrenshowed adequate or even slightly high urinary iodine. However,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 82/100
Stefan Peterson
82
other vulnerable groups such as women at delivery andnewborns showed signs of inadequate iodine status. Goiterregression may be delayed in all groups compared to
normalization of thyroid hormone and urinary iodine levels.Local studies are necessary to adapt internationalrecommendations on salt iodization levels to local circumstances.This will help avoid side effects of excess iodine intake such ashyperthyroidism, yet ensure adequate iodine intake in thepopulation. It is recommended to monitor salt iodineconcentrations at both production and distribution down to thehousehold level, as well as to assess iodine status in allvulnerable groups as a basis for adapting international
recommendations on new iodization levels at production.5. The WHO 1994 goiter classification system with the 5%prevalence cut-off will due to its low specificity makedemonstration of elimination of iodine deficiency by palpationimpossible. This will require programs to invest in costlyultrasound equipment and training. However, ultrasoundestimation also has considerable errors. Appropriately trainedpalpators using the 1960 Perez definition of goiter remainsoptimal for monitoring elimination of iodine deficiency in many
resource-poor settings. We recommend a return to palpation withthe Perez goiter criterion with a 10% acceptable prevalence forfuture goiter surveys in resource-poor countries.
6. Under the stewardship of ICCIDD, WHO and UNICEF iodinedeficiency control programs across the globe have maderemarkable progress over the last decade. They have benefitedfrom large international support and used internationallyrecommended strategies. As these programs now enter their
second cycle of implementation adjustments need to be made toeach national context. Methodologies for assessing severity of iodine deficiency and setting up standardized control strategieshave been successful. However, monitoring methodologies nowneed to be strengthened, especially with regards to sustainingand acting on ongoing process monitoring of the implementation.Starting from the salt production stage, monitoring needs to beinstitutionalized step by step. Appropriate sampling proceduresneed to be worked out. Once one step is successful monitoring of the next step needs to follow until there is indication of sufficient

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 83/100
Controlling IDD – Studies for Program Management
83
implementation to warrant a more refined evaluation. Institutinga quality assurance process with a committed organizationresponsible for maintaining a management information system
and acting on an ongoing monitoring is a top priority. Whereiodized salt fails, iodized oil capsule distribution will needconsiderable strengthening to successfully control IDD throughinvestments in the distribution and monitoring.
For impact evaluation there is need to refine internationalguidelines for aspects such as evidence based methodology forthyroid size estimation, and the relation of iodine statusindicators in different vulnerable groups. In addition toproduction of these much needed practical guidelines and
information materials from international organisations, keymethodological developments also need to undergo the peerreview process and be published in regular scientific journals.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 84/100
Stefan Peterson
84
ACKNOWLEDGEMENTSMany people have helped out during the course of this work. Thank you all. Inparticular I would like to acknowledge:
The many local health workers, village leaders, and community guides thathelped my way around Tanzanian and Central African villages and all thepeople that so readily took part in the studies. Thanks are also due to the pastand present IDD researchers and practitioners across the world, in particularthe people in ICCIDD who have pushed the drive against IDD.
Hans Rosling for inspiration, never-ending enthusiasm, mentoring and yourreadiness to let me run away and do other things beyond research. Agneta andMagnus Rosling for hospitality and generosity in lending Hans to me.
Mehari Gebre-Medhin for good scientific discussions and preparing me so wellfor work in Africa. Mehari and Susanne for the good injera-wat.
Karin Wennqvist for your life-long dedication to building an internationalpublic health center in Uppsala and your ever competent support.
Ted Greiner for sharing your knowledge, experience, material and contacts soliberally and for the many manuscript revisions.
Finn Diderichsen for your generosity, support and many useful discussions.
Thorkild Tylleskär for introducing me to field research in Africa, subsequentcollaboration and friendship.
Adam Taube for not only enlightening my student parties at the studentnation but also subsequently my scientific endeavours.
Wilbald Lorri, Festo Kavishe, Benedicta Mduma and “tovarish” Kimboka fortaking me into TFNC so readily. Vincent Assey, Alfred Sanga and BernardBunga for our many days and evenings together in Dar es Salaam and up-country, the good collaboration and for sharing Tanzania so generously withme. Nicholas Mlingi and everybody else at TFNC for your hospitality, help andfriendliness.
Francois Légue and Eugène Kpizingui for good collaboration and UNICEF andthe Ministry of Health for support in the Central African Republic. Staff of ÖrebroMissionen in Sweden and the Central African Republic for collaboration,support and hospitality., CAR.
Kristine Eklund and Inga Andersson for assistance with computers,paperwork, bookings and a whole lot more. Birgitta Jennische for sending themany IDD articles to me and the Medical Library for so competently

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 85/100
Controlling IDD – Studies for Program Management
85
and enthusiastically digging them out.
Everybody past and present at IMCH and the Dept of Nutrition for help,companionship and discussions, scientific and other.
Colleagues at Socialmedicin and the Dept of Public Health Sciences inStockholm for scientific interaction and the many coffee breaks we spentdiscussing statistics, public health and development.
Gösta Tibblin and other former colleagues at the Dept of Family Medicinewhere I worked and was inspired during the preparation of this work.
Hampus Eklöf for leaving your expecting family to suffer the hardships of measuring thyroids in Tanzania. Birger Forsberg for good collaboration andencouragement. Johanna Sundqvist and Mevan Wijetunga for long days and
nights in Ilembula and the even longer analysis and writing phase. Vincent Assey, Lena Carlsson, Claes Guthenberg, Gunilla Sparell, and Ann-SofieEriksson for laboratory analyses.
Kurt Svärdsudd and Bengt Höjer for the stimulating discussions andconstructive advice during my “half-time” seminar.
John Dunn, Francois Delange and Pierre Bordoux for inspiration during thestart of my work. Michael Zimmerman, Pavel Langer, and Mária Tajtáková forstimulating scientific debate.
Linley Chiwona-Karltun for progressing from being a fellow IDD researcher to
becoming part of the family.
My colleagues and friends in Uganda and WHO/IMCI for good collaborationand many new insights.
Friends in MSF Stockholm for being my social life throughout the process.
My parents Gunvor and Assar Peterson for giving me the support andencouragement to become what I am. And for paying all those taxes that paidthe way.
My mother-in-law Anne Marie Swartling for support and practical help to allowme to pursue and finish up this work.
My immediate family: Malin Swartling for critical realism, scientificdiscussions, patience and encouragement. Holger for helping out on thecomputer and being such a fun distraction.
And then, foremost, the ones I should have listed but forgot to…
This work was supported by Sida / SAREC, InDevelop, Uppsala University, andthe Stockholm County Council.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 86/100
Stefan Peterson
86
REFERENCES Aghini-Lombardi F, Antonangeli L,
Martino E, Vitti P, Maccherini D,Leoli F, Rago T, Grasso L, ValerianoR, Balestrieri A & Pinchera A. Thespectrum of thyroid disorders in aniodine-deficient community: thePescopagano survey. J Clin
Endocrinol Metab 1999;84:561-6.
Aghini-Lombardi F, Antonangeli L,Pinchera A, Leoli F, Rago T,Bartolomei AM & Vitti P. Effect of iodized salt on thyroid volume of
children living in an area previouslycharacterized by moderate iodinedeficiency. J Clin Endocrinol Metab1997;82:1136-9.
Alnwick D. Candidate noninfectiousdisease conditions. Global diseaseelimination and eradication as publichealth strategies. Bull World HealthOrgan 1998;76 Suppl 2:55-60.
Altman D. Practical statistics for
medical research. London: Chapman& Hall, 1991.
Anonymous. Millet - a possiblygoitrogenic cereal. Nutr Rev1983;41:113-6.
Anonymous. Interrelationshipsbetween selenium deficiency, iodinedeficiency, and thyroid hormones.Proceedings of a workshop.
Aberdeen, United Kingdom, March25-27, 1991. Am J Clin Nutr
1993;57:235S-318S.
Anonymous. Editorial comment on:Interobserver variation in theassessment of thyroid enlargement: A pitfall in surveys of the prevalence of endemic goitre. Food and Nutrition
Bulletin 1994;15:69-70.
Assey V, Kusindah B, Bunga B &Munga J. Progress report on saltiodation in Kilwa, Lindi andMtwara districts. TFNC Report
No 1842. Dar es Salaam: TanzaniaFood and Nutrition Center, 1998.
Baniahmad A, Tsai S, O'Malley B &Tsai M. Kindred thyroid hormonereceptor is an active andconstitutive silencer and areceptor for thyroid hormone andretinoic acid responses. Proc Natl
Acad Sci 1992;89:10633-7.
Barutwanayo M, Bassalia D,
Birabuza A, Celacollette C, KeitaM, Madji N, Maiga A, Maoude H,Ndihokubwayo H, Niangue J,SidiMohamedO M & Yazipo E.Malaria control in Africa:Guidelines for the evaluation of national programs (Africa ChildSurvival Initiative CombattingChildhood CommunicableDiseases (ACSI-CCCD). Atlanta,Georgia: US Dept of Health andHuman Services, CDC,International Health Program
Office, 1993.
Bateson A. Average cost profileprepared for the 15th EPI Global
Advisory Group meeting.: EPI-GPV, WHO, Geneva, 1992.
Benmiloud M, Chaouki ML,Gutekunst R, Teichert HM, WoodWG & Dunn JT. Oral iodized oilfor correcting iodine deficiency:optimal dosing and outcome
indicator selection. J Clin Endocrinol Metab 1994;79:20-4.
Biassoni P, Ravera G, Bertocchi J,Schenone F & Bourdoux P.Influence of dietary habits onthyroid status of a nomadicpeople, the Bororo shepherds,roaming a central African regionaffected by severe iodinedeficiency.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 87/100
Controlling IDD – Studies for Program Management
87
Eur J Endocrinol 1998;138:681-5.
Biassoni P, Ravera G, Schenone F,
Green J & Bertocchi J. Hormonal andbiochemical patterns in subjects froma new endemic goiter area in theCentral African Republic.Thyriodology 1991;3:63-68.
Biassoni P, Schenone F, Bertocchi J,Green J, Mela G & Balestra V.Ouham-Pendé: a new endemic goiterarea in the Centroafrican Republic(C.A.R.). Preliminary observations onschool children. Thyriodology
1990a;2:35-40.Biassoni P, Schenone F, Ravera G,Balestra V, Green J & Bertocchi J.Ouham-Pendé: a new endemic goiterarea in the Centroafrican Republic(CAR): epidemiological survey on7261 subjects. Thyriodology1990b;2:73-80.
Bilabina I, Fliniaux M, Doh A, DesmetG, Bour H & Brazier M. Evaluationde la teneur en iode et en acidecyanhydrique d'aliments consommésau Togo. Cah Nutr Diét 1995;30:300-5.
Blecher M. Use of indicators in healthcare management. World Health
Forum 1996;17:287.
Bleichrodt N & Born M. A meta-analysis of research on iodine and itsrelationship to cognitive devlopment.In: Iodine deficiency and braindamage. Report of the Franklin
Symposium 1994. J. Stanbury (ed)Philadelphia: CognizantCommunications Corporation, 1994.
Bouchet B. Monitoring the quality of primary health care. Bethesda, MD:Quality Assurance Project.
Bourdoux P. Measurement of thiocyanate in serum or urine yieldsdifferent information. J Anal Toxicol1995;19:127.
Bourdoux P, Delange F, Gerard M,Mafuta M, Hanson A & Ermans AM.
Evidence that cassava ingestionincreases thiocyanate formation: apossible etiological factor inendemic goitre. J Clin Endocrinol
Metab 1978;46:613-621.
Bourdoux P, Delange F, Gerard M,Mafuta M, Hanson A & Ermans
AM. Antithyroid action of cassavain humans. In: Role of cassava inthe etiology of endemic goitre andcretinism. IDRC Monograph136e.Ottawa, Canada: InternationalDevelopment Research Centre,1980.
Bourdoux P, Ermans A, Mukalaywa Mukalay A, Filetti S & VigneriR. Iodine-induced thyrotoxicosisin Kivu, Zaire. Lancet1996;347:552-3.
Brunn J, Block U, Ruf G, Bos I,Kunze W & Scriba P. Volumetrieder Schilddrüsenlappen mittelsreal-time sonographie. Dtsch MedWochenschr 1981;106:1338-1340.
Burgi H, Supersaxo Z & Selz B.Iodine deficiency diseases inSwitzerland one hundred yearsafter Theodor Kocher's survey: ahistorical review with some newgoitre prevalence data. Acta
Endocrinol 1990;123:577-90.
Burrow G (ed) Neonatal ThyroidScreening. New York: Raven,1980.
Buttfield I & Hetzel B. Endemic
goitre in Eastern New Guineawith special reference to the useof iodised oil in prophylaxis andtreatment. Bull World HealthOrgan 1967;36:243-262.
Cabanero-Verzosa C. Strategiccommunication for developmentprojects. Washington DC: WorldBank, 1999.
Calaciura F, Mendorla G,
Distefano M, Castorina A, Fazio T,Motta R, Sava L, Delange F & Vigneri R. Childhood

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 88/100
Stefan Peterson
88
IQ measurement in infants withtransient congenital hypothyroidism.Clin Endocrinol 1995;43:473-477.
Cameron M & Van Staveren W (eds).Manual on methodology for foodconsumption studies. Oxford: OxfordUniversity Press, 1988.
Cao X-Y, Jiang X, Dou Z, Rakeman M,Zhang M, O'Donnell K, Ma T, AmetteK, DeLong N & DeLong G. Timing of vulnerability of the brain to iodinedeficiency in endemic cretinism. N
Engl J Med 1994a;331:1739-44.
Cao X-Y, Jiang X-M, Kareem A, Dou Z-H, Rakeman M, Zhang M-L, Ma T,O´Donell K, DeLong N & DeLong G.Iodination of irrigation water as amethod of supplying iodine to aseverely iodine-deficient populationin Xinjiang, China. Lancet1994b;344:107-110.
Carlsson J, Ismail S, Jitta J & Tekle E.Working with nutriton. A comparative study of the TanzaniaFood and Nutrition Centre and the
National Nutrition Unit of Zimbabwe.Sida Evaluation 99/10. Stockholm:Sida, 1999.
Casadei E, Cliff J & Neves J.Surveillance of urinary thiocyanateconcentration after epidemic spasticparaparesis in Mozambique. Journalof Tropical Medicine and Hygiene1990;93:257-261.
CFAR. Dissemination on universal
salt iodisation. New Dehli: Centre for Advocacy and Research. ICCIDD,2000.
Chanoine JP, Toppet V, Bourdoux P,Spehl M & Delange F. Smokingduring pregnancy: a significant causeof neonatal thyroid enlargement. Br J Obstet Gynaecol 1991;98:65-8.
Chauhan S, Bhatt A, Bhatt M &
Majeethia K. Stability of iodised saltwith respect to iodine content.
Research and Industry 1992;37:38-41.
Choufoer J, van Rhijn M,
Kassenaar A & Querido A.Endemic goiter in western NewGuinea. Iodine metabolism ingoitrous and non goitroussubjects. Clin Endocrinol1963;23:1203-17.
Clements F, Gibson H & Howeler-Coy J. Goiter prophylaxis byaddition of potassium iodate tobread. Experience in Tasmania.
Lancet 1970;:489.
Cliff J, Essers S & Rosling H. Ankle clonus correlating withcyanide intake from cassava inrural children from Mozambique.
J Trop Pediatr 1986a;32:186-189.
Cliff J, Lundquist P, Rosling H,Sörbo B & Wide L. Thyroidfunction in a cassava-eatingpopulation affected by epidemicspastic paraparesis. Acta
Endocrinologica 1986b;113:523-
528.
Clugston G & Bailey K. WHO. In:SOS for a billion. B. Hetzel & C.Pandav (eds). Dehli: OxfordUniversity Press, 1996.
Clugston G, Beaudry M & DelangeF. Iodine-induced thyrotoxicosis.
Lancet 1996;347:1051.
Clugston G, Dulberg E & Pandav
C. Iodine Deficiency Disorders inSouth East Asia. In: ThePrevention and Control of IodineDeficiency Disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier, 1987.
Cobra C, Muhilal, Rusmil K,Rustama D, Djatnika, Suwardi SS,Permaesih D,Muherdiyantiningsih, Martuti S &Semba RD. Infant survival isimproved by oral iodinesupplementation. J Nutr1997;127:574-8.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 89/100
Controlling IDD – Studies for Program Management
89
Connolly R. An increase inthyrotoxicosis in southern Tasmaniaafter an increase indietary iodine.
Med J Aust 1971;1:1268-71.
Cooke RD & Maduagwu EN. Theeffect of simple processing on thecyanide content of cassava chips.
Journal of Food Technology1978;13:299-306.
DailyNews. Status of salt industry inTanzania. In Daily News. Dar esSalaam, 1994. Issue April 29.
Dayrit M. Report of the workgroup on
noninfectious diseases. Globaldisease elimination and eradicationas public health strategies. BullWorld Health Organ 1998;76 Suppl2:80-84.
Delange F. Administration of iodizedoil during pregnancy: a summary of the published evidence. Bull World
Health Organ 1996;74:101-108.
Delange F. Screening for congenitalhypothyroidism used as an indicatorof the degree of iodine deficiency andof its control. Thyroid 1998;8:1185-92.
Delange F. What do we call a goiter? Eur J Endocrinol 1999;140:486-8.
Delange F & Ahluwalia R. Cassavatoxicity and thyroid: research andpublic health issues. IDRCmonograph 207e). Ottawa, Canada:International Development ResearchCentre, 1983.
Delange F, Bastani S, Benmiloud M,DeMayer E, Isayama M, Koutras D,Muzzo S, Niepomniszcze H, Pandav C& Riccabona G. PAHO/WHOtechnical group on endemic goiter,cretinism, and iodine deficency 5thmeeting 1983 Lima, Peru. Definitionof endemic goiter and cretinism,classification of goiter size andseverity of endemias, and surveytechniques. In: Towards the
eradication of endemic goiter,cretinism, and iodine deficiency. J.Dunn (ed) Washington D.C.: PAHO
Scientific publication no 502, 1986.
Delange F, Benker G, Caron P,Eber O, Ott W, Peter F, Podoba J,
Simescu M, Szybinsky Z, Vertongen F, Vitti P, Wiersinga W& Zamrazil V. Thyroid volume andurinary iodine in Europeanschoolchildren: standardization of values for assessment of iodinedeficiency. Eur J Endocrinol1997;136:180-7.
Delange F, Ekpechi L & Rosling H.Cassava cyanogenesis and iodinedeficiency disorders. Paperpresented to the Internationalworkshop on cassava safety,Ibadan, Nigeria, ActaHorticulturae, InternationalSociety for Horticultural Sciences,1994.
Delange F & Ermans A. Role of adietary goitrogen in the etiologyof endemic goiter on Idjwi island.
Am J Clin Nutr 1971;24:1361-1373.
Delange F, Iteke FB & Ermans
AM. Nutritional factors involvedin the goitrogenic action of cassava. IDRC Monograph184e).Ottawa, Canada: InternationalDevelopment Research Centre,1982.
Delange F, Vigneri R, Trimarchi F,Filetti S, Pezzino V, Squatrito S,Bourdoux P & Ermans A. Theiodine/thiocyanate ratio. In: Roleof cassava in the etiology of endemic goitre and cretinism.
A.M. Ermans, N.M. Mbulamoko, F.Delange & R. Ahluwalia (eds).Ottawa, Canada: InternationalDevelopment Research Centre,1980.
DeLong G, Leslie P, Wang S, Jiang X, Zhang M, Rakeman M, Jiang J,Ma T & Cao X. Effect on infantmortality of irrigation water in aseverely iodine deficient area of China. Lancet 1997;350:771-3.
DeLong GR. Dynamics of environmental supplementation of

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 90/100
Stefan Peterson
90
iodine: four years' experience of iodination of irrigation water inHotien, Xinjiang, China. Arch
Environ Health 1998;53:238-9.
DeMaeyer E, Lowenstein F & ThillyC. The control of endemic goitre.Geneva: WHO, 1979.
DiPrete-Brown L, Miller-Franco L,Rafeh N & Hatzell T. Qualityassurance of health care indeveloping countries. Second ed.Bethesda, Maryland: Quality
Assurance Project, 1998.
Dulberg E. A model for predicting thedevelopmental IDDs from goitredata. IDD Newsletter, ICCIDD 1985;1.
Dunn J. Alternatives to salt and oil foriodine supplementation. In: Theprevention and control of iodinedeficiency disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier SciencePublishers, 1987a.
Dunn J. Iodized oil in the treatment
and prophylaxis of IDD. In: Theprevention and control of iodinedeficiency disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier SciencePublishers, 1987b.
Dunn J. Seven deadly sins inconfronting endemic iodinedeficiency, and how to awoid them. J Clin Endocrinol Metab 1996a;81:1332-1335.
Dunn J. The use of iodized oil andother alternatives for the eliminationof iodine deficiency disorders. In:SOS for a billion. B. Hetzel & C.Pandav (eds). Dehli: OxfordUniversity Press, 1996b.
Dunn J. What's happening to ouriodine. . J Clin Endocrinol Metab1998;83:3398-33400.
Dunn J, Crutchfield H &Gutekunst R. Methods formeasuring iodine in urine:ICCIDD/WHO/UNICEF, 1993.
Dunn J & van der Haar F. A practical guide to the correction of iodine deficiency: InternationalCouncil for the Control of IodineDeficiency Disorders (ICCIDD),WHO, UNICEF, 1990.
Dustin J & Ecoffey J. A field testfor detecting iodine-enriched salt.
Bull World Health Organ1978;56:657-658.
El Mahdi E, Eltom M, Karlsson F& Mukhtar E. Water goitrogensand endemic goiter in the Sudan.Trop Geogr Med 1986;38:180-182.
Elnagar B, Eltom A, Wide L,Gebre-Medhin M & Karlsson FA.Iodine status, thyroid functionand pregnancy: study of Swedishand Sudanese women. Eur J Clin
Nutr 1998;52:351-5.
Elnagar B, Eltom M, Karlsson FA,
Bourdoux PP & Gebre-Medhin M.Control of iodine deficiency usingiodination of water in a goitreendemic area. Int J Food Sci Nutr1997;48:119-27.
Elnagar B, Eltom M, Karlsson FA,Ermans AM, Gebre-Medhin M &Bourdoux PP. The effects of different doses of oral iodized oilon goiter size, urinary iodine, andthyroid-related hormones. J Clin
Endocrinol Metab 1995;80:891-7.Elnour A, Lieden S, Bourdoux P,Eltom M, Khalid SA & HambraeusL. Traditional fermentationincreases goitrogenic activity inpearl millet. Ann Nutr Metab1998;42:341-9.
Eltom A, Elnagar B, Elbagir M &Gebre-Medhin M. Thyroglobulinin serum as an indicator of iodinestatus during pregnancy. Scand J

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 91/100
Controlling IDD – Studies for Program Management
91
Clin Lab Invest 2000a;60:1-8.
Eltom A, Eltom M, Elnagar B, ElbagirM & Gebre-Medhin M. Changes in
iodine metabolism during latepregnancy and lactation: alongitudinal study among Sudanesewomen. Eur J Clin Nutr2000b;54:429-433.
Eltom M. Endemic goitre in theSudan. [Doctoral Thesis]. UppsalaUniversity, Sweden, 1984.
Eltom M, Elnagar B, Sulieman EA,Karlsson FA, Van Thi HV, Bourdoux
P & Gebre-Medhin M. The use of sugar as a vehicle for iodinefortification in endemic iodinedeficiency. Int J Food Sci Nutr1995;46:281-9.
Eltom M, Hofvander Y, Torelm I &Fellstrom B. Endemic goitre in theDarfur region (Sudan). Epidemiologyand aetiology. Acta Med Scand1984;215:467-75.
Eltom M, Karlsson FA, Kamal AM,Boström H & Dahlberg P. Theeffectiveness of oral iodized oil in thetreatment and prophylaxis of endemic goiter. J Clin Endocrinol
Metab 1985;61:1112-7.
Emamian S, Nielsen M & Pedersen J.Intraobserver and interobservervariations in sonographicmeasurements of kidney size in adultvolunteers. Acta Radiol 1995;36:399-401.
Ermans A, Bourdoux P, Lagasse R,Delange F & Thilly C. Congenitalhypothyroidism in developingcountries. In: Neonatal ThyroidScreening. G. Burrow (ed) New York:Raven Press, 1980a.
Ermans AM, Mbulamoko NM, DelangeF & Ahluwalia R. Role of cassava inthe etiology of endemic goitre andcretinism. IDRC Monograph136e).
Ottawa, Canada: InternationalDevelopment Research Centre, 1980b.
Fernandez RL. A simple matter of salt: an ethnography of nutritionaldeficiency in Spain. Berkeley:University of California Press,
1990.
Field J. Implementing nutritionprograms: Lessons from anunheeded literature. Ann Rev
Nutr 1985;5:143-72.
Fisch A, Pichard E, Prazuck T,Sebbag R, Torres G, Gernez G &Gentilini M. A new approach tocombating iodine deficiency indeveloping countries: the
controlled release of iodine inwater by a silicone elastomer. Am J Public Health 1993;83:540-545.
Foo LC & Mafauzy M. Does the useof mean or median Z-score of thethyroid volume indices provide amore precise description of theiodine deficiency disorder statusof a population? Eur J Endocrinol1999;141:557-60.
Foo LC, Zulfiqar A, Nafikudin M,Fadzil MT & Asmah AS. Localversus WHO/InternationalCouncil for Control of IodineDeficiency Disorders-recommended thyroid volumereference in the assessment of iodine deficiency disorders. Eur J
Endocrinol 1999;140:491-7.
Fresco L. The agricultural sector inthe Central African Republic. Anassessment of the technical
constraints and potential. WorldBank, Agricultural Sector Report,Washington DC, 1986.
Furnée C. Prevention and controlof iodine deficiency: Studies onthe efficacy of oral iodized oil.[Doctoral thesis]. Wageningen
Agricultural University,Netherlands, 1994.
Furnée C, van der Haar F, West C
& Hautvast J. A critical appraisal

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 92/100
Stefan Peterson
92
of goiter assessment and the ratio of urinary iodine to creatinine forevaluating iodine status. Am J Clin
Nutr 1994;59:1415-1417.
Gaitan E. Goitrogens in food andwater. Ann Rev Nutr 1990;10:21-39.
Gaitan E & Dunn J. Epidemiology of iodine deficiency. Trends End. Metab.1992;13:427.
Gandz AS. [Iodized bread in theprophylaxis of endemic goiter inchildren]. Pediatriia 1974;53:77-8.
Gerasimov G, Nazarov A, Mayorova N,Schischkina A, Arbusova M,Mischenko B & Dedov I. Breadiodization for micronutrientsupplementation in iodine deficientregions of Russia. Thyroid1995;Suppl 1:S-40.
Goodman RM. Principals and tools forevaluating community-basedprevention and health promotionprograms. J Public Health Manag
Pract 1998;4:37-47.
Grant J. Iodine Deficiency Disorderson the run. Paper presented to theRegional meeting on universal saltiodization to eliminate IDD in the
Americas, Quito, Equador, UNICEF,New York, 1994.
Greene J & Kevany J. Projects toprogrammes: An internationalperspective. Food and Nutrition
Bulletin 1994;15:227-232.
Greiner T. Lessons learned and issuesemerging from experience withuniversal distribution of vitamin A capsules in Bangladesh. A report tothe World Bank. ICH, UppsalaUniversity, Sweden, 1991.
Greiner T. Rapid appraisal beforeimpact evaluation studies. World
Health Forum 1997;18:66-67.
Guderian R, Anselmi M, EspinelM, Mancero T, Rivadeneira G,Proano R, Calvopina H, Vierira J& Cooper P. Succesful control of
onchocerciasis with community-based ivermectin distibution inthe Rio Santiago focus in Ecuador.Trop Med Int Health 1997;2:982-8.
Gutekunst R. Iodine Deficiencycost Germany over one billiondollars per year. IDD Newsletter1993: 29-31.
Gutekunst R, Smolarek H,Hasenpusch U, Stubbe P,
Friedrich HJ, Wood WG & ScribaPC. Goitre epidemiology: thyroidvolume, iodine excretion,thyroglobulin and thyrotropin inGermany and Sweden. Acta
Endocrinol (Copenh) 1986;112:494-501.
Hahn SK. An overview of Africantraditional cassava processing andutilization. Outlook on Agriculture1989;18:110-18.
Hegedüs L, Karstrup S, VeiergangD, Jacobsen B, Skovsted L &Feldt-Rasmussen U. Highfrequency of goitre in cigarettesmokers. Clin Endocrinol1985;22:287-92.
Hegedüs L, Perrild H, Poulsen L, Andersen J, Holm B, Schnohr P,Jensen G & Hansen J. Thedetermination of thyroid volumeby ultrasound and its relationship
to body weight, age, and sex innormal subjects. J Clin Endocrinol Metab 1983;56:260-263.
Hennart P, Bourdoux P, Lagasse R,Thilly C, Putzeys P, Courtois P,
Vis H, Yunga Y, Seghers P &Delange F. Epidemiology of goitreand malnutrition and dietarysupplies of iodine, thiocyanate,and proteins in Bas Zaire, Kivu,and Ubangi. In: Nutritional factorsinvolved in the goitrogenic action

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 93/100
Controlling IDD – Studies for Program Management
93
of cassava. F. Delange, F. Iteke & A.Ermans (eds). Ottawa: InternationalDevelopment Research Centre, 1982.
Hetzel B. Iodine deficiency disordersand their eradication. Lancet1983;ii:1126-1129.
Hetzel B. An overview of theprevention and control of iodinedeficiency disorders. In: Theprevention and control of iodinedeficiency disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier SciencePublishers, 1987a.
Hetzel B. Toward a global strategy forthe prevention and control of iodinedeficiency disorders. In: Theprevention and control of iodinedeficiency disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier SciencePublishers, 1987b.
Hetzel B. The prevention and controlof iodine deficiency disorders.Geneva: ACC/SCN state of the artseries. Discussion paper no 3., 1988.
Hetzel B. The story of iodinedeficiency. An internationalchallenge in nutrition. Oxford:Oxford University Press, 1989.
Hetzel B. Recent progress in theelimination of iodine deficiencydisorders. In: SOS for a billion. B.Hetzel & C. Pandav (eds). Dehli:Oxford University Press, 1996.
Hetzel B & Mano M. A review of experimental studies of iodinedeficiency during fetal development.
J Nutr 1989;119:145-151.
Hetzel B & Pandav C. SOS for abillion. Dehli: Oxford UniversityPress, 1996.
Höjer JA. Kropfstudien. In: SvenskaLäkaresällskapets Handlingar. Acta
societatis medicorum suecanæ. A.Pettersson (ed) Stockholm: IsaacMarcus Boktryckeri, 1931.
Huda S, Grantham-McGregor S,Rahman K & Tomkins A.Biochemical hypothyroidismsecondary to iodine deficiency isassociated with poor schoolachievement and cognition inBangladeshi children. J Nutr1999;129:980-7.
ICCIDD. IDD Prevalence andControl Program Data. Central
African Republic: ICCIDD, 1997a.
Issue May 1997.www.people.virginia.edu/¨~jtd/iccidd/mi/idd_032
ICCIDD. IDD Prevalence andControl Program Data. Tanzania:ICCIDD, 1997b. Issue May 1997.www.people.virginia.edu/¨~jtd/iccidd/mi/idd_166
ICCIDD. ICCIDD Global ActionPlan 1999-2001: ICCIDD, 1999a.Issuewww.people.virginia.edu/¨~jtd/iccidd/plan.htm
ICCIDD. Indicators for assessingIDD status. In IDD Newsletter,1999b. Issue August.
Inglenbleek Y, Jung L, Férard G,Bordet F, Goncalves A & DechouxL. Iodised rapeseed oil foreradication of severe endemicgoitre. Lancet 1997;350:1542-45.
Jamison D, Mosley W, Measham A & Bobadilla J (eds). Diseasecontrol priorities in developingcountries. New York: OxfordUniversity Press, 1993.
Kapil U, Prakash S, Shah A &Nayar D. Some factors influencingloss of iodine from iodized salt.
IDD Newsletter 1996;12:12.
Karmarkar M & Pandav C.Interpretation of indicators of

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 94/100
Stefan Peterson
94
iodine deficiency disorders: Recentexperiences. The National Medical
Journal of India 1999;12:113-7.
Katabarwa M & Mutabazi D. Theselection and validation of indicatorsfor monitoring progress towards self-sustainment in community-directed,ivermectin-treatment programmesfor onchocericiasis control in Uganda.
Ann Trop Med Parasitol 1998;92:859-868.
Kavishe F. Can Africa meet the goal of eliminating iodine deficencydisorders by the year 2000? Food and
Nutrition Bulletin 1996;17:262-267.Khan M & Manderson L. Focus groupsin tropical diseases research. Health
Policy and Planning 1992;7:56-66.
Kimboka S. Personal Communicationon Tanzania national IDD evaluation1999: TFNC. March, 2000.
Kipp W, Burnham G, Bamuhiiga J,Weis P & Buttner D. Ivermectindistribution using community
volunteers in Kabarole district,Uganda. Health Policy and Planning1998;13:167-73.
Koblinsky M, A T & Daly P.Programming for Safe Motherhood: aguide to actioni. Health Policy and
Planning 1994;9:252-66.
Kochupillai N. Neonatalhypothyroidism in India. Mt Sinai J
Med 1992;59:111-5.
Kochupillai N, Karmarkar M,Weightman D, Hall R, Deo M,McKendrick M, Evered D &Ramalingaswami V. Pitutary-thyroidaxis in Himalayan endemic goitre.
Lancet 1973;:1021-1024.
Kochupillai N & Pandav C. Neonatalchemical hypothyroidism in iodinedeficient enviroments. In: ThePrevention and Control of Iodine
Deficiency Disorders. B. Hetzel, J.Dunn & J. Stanbury (eds).
Amsterdam: Elsevier, 1987.
Kohrle J. The trace elementselenium and the thyroid gland. Biochimie 1999;81:527-33.
Konde M, Ingenbleek Y, Daffe M,Sylla B, Barry O & Diallo S.Goitrous endemic in Guinea.
Lancet 1994;344:1675-1678.
Kwena E. Children who don't getenough iodine are at great risk. InThe East African. Nairobi, 2000.
Issue February 14-20.Lagasse R, P. B, Courtois P,Hennart P, Putzeys P, Thilly C,Mafuta M, Yunga Y, Ermans AM& Delange F. Influence of thedietary balance of iodine/thiocyanate and protein onthyroid function in adults andyoung infants. In: Nutritionalfactors involved in the goitrogenicaction of cassava. F. Delange, F.B.Iteke & A.M. Ermans (eds).
Ottawa, Canada: InternationalDevelopment Research Centre,1982.
Lamberg BA. Endemic goitre--iodine deficiency disorders. Ann
Med 1991;23:367-72.
Lantum D. Lutte contre lestroubles dûs à la carence en iode.Rapport de l'enquête nationale,14-25 mars 1991. Ministère de la
Santé Publique et des AffairesSociales, Bangui, RépubliqueCentrafricaine, 1991.
Lantum D. Francophone Central Africa. In IDD Newsletter, 1992.
Levinson FJ, Rogers BL, HicksKM, Schaetzel T, Troy L & YoungC. Monitoring and evaluation of nutrition programs in developingcountries. Nutr Rev 1999;57:157-64.
Li J & Wang X. Jixian: A success

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 95/100
Controlling IDD – Studies for Program Management
95
story in IDD control. IDD Newsletter1987;3:4-5.
Ling J & Reader-Wilstein C. Ending
iodine deficiency now and forever:ICCIDD.www.people.virginia.edu/¨~jtd/iccidd/ plan.htm
Loevinsohn B, Sutter R & Costales M.Using cost-effectiveness analysis toevaluate targeting strategies: thecase of vitamin A supplementation.
Health Policy and Planning1997;12:29-37.
Lorenz N, Kilima P, Tanner M &Garner P. The right objectives inhealth care planning. World Health
Forum 1995;16:280-2.
Lundquist P, Mårtensson J, Sörbo B &Öhman S. Method for determiningthiocyanate in serum and urine(Addendum in Clin Chem1983;29:403). Clin Chem 1979;25:678-681.
MacLennan R, Gaitán E & ClintonMiller M. Observer variation ingrading and measuring the thyroid inepidemiological surveys. In: EndemicGoiter: PAHO, 1969.
Magambo F, Mlingi N & Bunga B. Aninvestigation into factors leading tosome resistance to a new innovation:The case of iodinated oil capsuledistribution: Rukwa Region,Tanzania. Tanzania Food andNutrition Centre, TFNC report No
1242, 1990.
Maine D, Wardlaw T, Ward V,McCarthy J, Birnbaum A, Akalin M &Brown J. Guidelines for monitoringavailability and use of obstetricservices. New York: UNICEF, WHO,UNFPA, 1997.
Mannar M. The iodization of salt forthe elimination of iodine deficiencydisorders. In: SOS for a billion. B.
Hetzel & C. Pandav (eds). Dehli:
Oxford University Press, 1996.
Mannar M & Dunn J. Saltiodization for the elimination of
iodine deficiency:ICCIDD/MI/UNICEF/WHO, 1995.
Mao I, Ko Y & Chen MTsoiihs. Thestability of iodine in human sweat.
Jpn J Physiol 1990;40:693-700.
Marine D & Kimball O. Theprevention of simple goitre inman. American Journal of MedicalScience 1922;:163-634.
May SL, May WA, Bourdoux PP,Pino S, Sullivan KM & MaberlyGF. Validation of a simple,manual urinary iodine method forestimating the prevalence of iodine-deficiency disorders, andinterlaboratory comparison withother methods. Am J Clin Nutr1997;65:1441-5.
Mbalilaki N. Tanzania Census1988. Dar Es Salaam: Bureau of Statistics, Ministry of Finance,Economic Affairs and Planning,1988.
McCullagh S. The Huon Peninsulaendemic: I. The effectiveness of anintramuscular depot of iodized oilin the control of endemic goitre.
Med J Aust 1963;1:767-9.
Mlingi N, Poulter N & Rosling H. An outbreak of acute intoxicationsfrom consumption of insufficiently
processed cassava in Tanzania. Nutrition Research 1992;12:677-687.
MMWR. Framework for programevaluation in public health.
MMWR Morb Mortal Wkly Rep1999;48:1-40.
Momburi B. Survey for saltproduction "foot hill sources" .The case for Dodoma district. Dares Salaam: Ministry of Water,
Energy and Minerals, 1993.
Mongonou F. Goitre éndemique

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 96/100
Stefan Peterson
96
dans la region de Bouar. [Thése pourle Doctorat en Medicine.]. Universitéde Bangui, RCA, 1982.
Moreno-Reyes R, Boelaert M, elBadawi S, Eltom M & Vanderpas JB.Endemic juvenile hypothyroidism ina severe endemic goitre area of Sudan. Clin Endocrinol (Oxf)1993;38:19-24.
Mosley W & Chen L. An analyticalframework for the study of childhoodsurvival in developing countries.
Population and Development Review1984;10 (Suppl):25-45.
Moyer A, Verhovsek H & Wilson VL.Facilitating the shift to population-based public health programs:innovation through the use of framework and logic model tools. Can
J Public Health 1997;88:95-8.
Murdoch D, Harding E & Dunn J.Persistence of iodine deficiency 25years after initial correction effortsin the Khumbu region of Nepal. N Z
Med J 1999;112:266-8.
Mutamba J. Endemic goitre inZimbabwe. [Master's thesis]. ICH,Uppsala University, Sweden, 1993.
NCCIDD-TFNC. Map of TanzaniaDistrict Goitre Survey (1980-1990).Dar es Salaam: National Council forthe Control of IDD, 1990.
O'Brien G, Mbome L, Taylor A &Poulter N. Variations in cyanogen
content of cassava during villageprocessing in Cameroon. FoodChemistry 1992;44:131-136.
Özgen A, Erol C, Kaya A, Özmen M, Akata D & Akhan O. Interobserverand intraobserver variations insonographic measurement of thyroidvolume in children. Eur J Endocrinol1999;140.
PAMM. Quality assurance,monitoring and enforcement of salt
iodization programs. Report of atraining workshop., Blantyre,Malawi, PAMM, EmoryUniversity, Rollins School of
Public Health, Atlanta, Georgia,1998.
Pandav C, Pandav S, Anand K,Wajih S, Prakash S, Singh J &Karmarkar M. A role fornongovernmental organizations inmonitoring the iodine content of salt in northern India. Bull World
Health Organ 1995;73:71-5.
Passmore R & Eastwood M.
Davidson and Passmore HumanNutrition and Dietetics.Edinburgh: Churchill Livingstone,1986.
Perez C, Scrimshaw S & Muñoz A.Technique of endemic goitresurveys. In: EndemicGoitreGeneva: WHO, 1960.
Peterson S. Cassava, iodinedeficiency disorders and konzo inthe Central African Republic.
MFS Report No 69. InternationalChild Health Unit, UppsalaUniversity, 1994.
Pharoah P, Buttfield I & Hetzel B.Neurological damage to the fetusresulting from severe iodinedeficiency during pregnancy.
Lancet 1971;1:308-310.
Pharoah P & Connolly K. A controlled trial of iodinated oil for
the prevention of endemiccretinism: A long-term follow-up. Int J Epidemiol 1987;16:68-73.
Pharoah PO & Connolly KJ. Effectsof maternal iodinesupplementation duringpregnancy. Arch Dis Child1991;66:145-7.
Pharoah PO, Ellis SM, Ekins RP &Williams ES. Maternal thyroidfunction, iodine deficiency andfetal development. Clin
Endocrinol (Oxf) 1976;5:159-66.

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 97/100
Controlling IDD – Studies for Program Management
97
Phillips D. Iodine, milk, and theelimination of endemic goitre inBritain: the story of an accidentalpublic health triumph. J Epidemiol
Community Health 1997;51:391-393.
Pichard E, Soula G, Fisch A, Rhaly AA, Diarra M, Sebbag R & GentiliniM. Prevention of iodine deficiencydisorders in children in the rural
African zone. Ann Pediatr (Paris)1992;39:71-8.
Querido A, Delange F, Dunn J, Fierro-Benitez R, Ibbertson H, Koutras D &Perinetti H. Definitions of endemic
goiter and cretinism, classification of goiter size and severity of endemiasand survey technique. In: Endemicgoiter and cretinism: Continuingthreats to world health. J. Dunn & G.Medeiros-Neto (eds). PAHO Sci Pub,1974.
Rendl J, Bier D, Groh T & Reiners C.Rapid urinary iodide test. Exp Clin
Endocrinol Diabetes 1998;106 Suppl3:S12-6.
Rosling H. Cassava toxicity and foodsecurity. A review of health effects of cyanide exposure from cassava and of ways to preent these effects. UNICEF& ICH, 1988.
Rosling H. Measuring effects inhumans of dietary cyanide exposurefrom cassava. In: Internationalworkshop on cassava safety. M.Bokanga, A. Essers, N. Poulter, H.Rosling & O. Tewe (eds). Ibadan,
Nigeria: Acta Horticulturae,International Society forHorticultural Sciences, 1994.
Rossi P & Freeman H. Evaluation: asystematic approach. Newbury Park,CA: SAGE Publications, 1993.
Rubin F. A basic guide to evaluationfor development workers. Oxford:Oxfam, 1995.
Sandell E & Kolthoff I. Microdetermination of iodine by acatalythic method. Microchem Acta
1937; 9-25.
Sanga A. Towards the eliminationof iodine deficiency disorders by
the year 2000: A challenge forTanzania. [Master's thesis].London School of Hygiene andTropical Medicine, 1994.
Schrettenbrunner A & Harpham T. A different approach to evaluatingPHC projects in developingcountries: how acceptable is it toaid agencies? Health Policy and
Planning 1993;8:128-35.
Scrimshaw N & Gleason G (eds).Rapid assessment procedures.Qualitative methodologies forplanning and evaluation of healthrelated programmes. Boston:International NutritionFoundation for DevelopingCountries (INFDC), 1992.
Sjöberg K & Sundlöf G.Strumasjukdomen före och efter
jodprofylaxen [Endemic goitrebefore and after iodineprophylaxis]. Läkartidningen1971;68:980-984.
Smyth PP, Darke C, Parkes AB,Smith DF, John R, Hetherton AM& Lazarus JH. Assessment of goiter in an area of endemiciodine deficiency. Thyroid1999;9:895-901.
Solomons NW. There needs to bemore than one way to skin the
iodine deficiency disorders cat:novel insights from the field inZimbabwe [comment]. Am J Clin
Nutr 1998;67:1104-5.
Sorcini M, Oliveri A, Fazzini C,Medda E, Grandolfo M, Aghini-Lombardi F, Balestrazzi P,Giovanelli G & Carta S. Incidenceof congential hypothyroidism(CH): An indicator of iodinedeficient areas in Italy. 1995;.
Stanbury J (ed) The damaged brainof iodine deficiency: cognitive,

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 98/100
Stefan Peterson
98
behavioral, neuromotor, andeducative aspects. New York:Cognizant communication, 1994.
Sullivan K, Houston R, Gorstein J &Cervinskas J (eds). Monitoringuniversal salt iodisation programmes.
Atlanta, Georgia: PAMM, MI,ICCIDD, 1995.
Sundqvist J & Wijetunga M. Intake of Iodised Salt and Iodine Status in aCommunity - a survey carried out inthe village of Ilembula in Iringaprovince, southern Tanzania. 89/1996.Uppsala: ICH, Dept of Pediatrics,
Uppsala University, 1996.Tarimo E. Final report onsustainability of community-directedtreatment of onchocerciasis withivermectin. Ougadogou: AfricanProgramme for Onchocerciasis,
APOC, 2000.
Taube A. Sensitivity, specificity andpredicitive values: a graphicalapproach. Stat Med 1986;5:585-591.
Thilly C. Goitre. In: Médecine ethygiène en Afrique Centrale de 1885à nos jours. P. Janssens, M. Kivits &J. Vuylsteke (eds). Brussels:Fondation Roi Baudouin, 1992.
Thilly C, Contempre B & Vanderpas J.Surcharge en Thiocyanate et Carenceen Sélénium: Des Cofacteurs danslÉtiologie du Goitre et du CrétinismeEndémiques au Nord-Zaire. Bull
Acad R Med Belg 1991;145:440-450.
Thorpe-Beeston J, Nicolaides K,Felton C, Butler J & McGregor A.Maturation of the secretion of thyroidhormone and thyroid stimulatinghormone in the fetus. N Engl J Med1991;324:532-535.
TISCO. Salt production, importation,distribution pattern and marketing inTanzania. Dare es Salaam: NCCIDD,
1992.
Todd C. Hyperthyroidism andother thyroid disorders
WHO/AFRO/NUT/99.1WHO/NHD/99.1): WHO/ICCIDD,1998.
Todd C, Allain T, Gomo Z, HaslerJ, Ndiweni M & Oken E. Increasein thyrotoxicosis associated withiodine supplements in Zimbabwe.
Lancet 1995;346:1563-4.
Todd C & Dunn J. Intermittentoral administration of potassium
iodide solution for the correctionof iodine deficiency. Am J Clin Nutr 1998;67:1279-1283.
Tonglet R, Bourdoux P, DramaixM, Hennart P & Ermans A.Interobserver variation in theassessment of thyroidenlargement: A pitfall in surveysof the prevalence of endemicgoitre. Food and Nutrition Bulletin1994;15:64-70.
Tonglet R, Bourdoux P, Minga T &Ermans AM. Efficacy of low oraldoses of iodized oil in the controlof iodine deficiency in Zaire. N
Engl J Med 1992;326:236-41.
Tugwell P, Bennett K, Sackett D &Haynes R. The measurementiterative loop: a framework for thecritical appraisal of need, benefitsand costs of health interventions.
Journal of Chronic Diseases
1985;38:339-351.Tylleskär T. The causation of Konzo. [Doctoral Thesis]. UppsalaUniversity, Sweden, 1994.
Tylleskär T, Banea M, Bikangi N,Cooke R, Poulter N & Rosling H.Cassava cyanogens and konzo, anupper motoneuron disease foundin Africa. Lancet 1992;339:208-211.
Tylleskär T, Légué FD, Peterson S,Kpizingui E & Stecker P. Konzo in

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 99/100
Controlling IDD – Studies for Program Management
99
the Central African Republic. Neurology 1994;44:959-961.
UNICEF. Chapter 6. Monitoring and
Evaluation. In: UNICEF Policy andProcedure manual. New York:UNICEF, 1990.
UNICEF. Small salt producers anduniversal salt iodation. New York:UNICEF Nutrition Section, 1994a.
UNICEF. State of the world'schildren: Oxford University Press,1994b.
UNICEF. State of the world'schildren: Oxford University Press,1995.
UNICEF. Universal Salt IodationUpdate. Vol 1. New York: , 1996.
UNICEF. State of the world'schildren: Oxford University Press,1998.
UNICEF. State of the world'schildren: Oxford University Press,2000.
Untoro J, Ruz M & Gross R. Lowenvironmental selenium availabilityas an additional determinant forgoiter in East Java, Indonesia? BiolTrace Elem Res 1999;70:127-36.
van der Haar F, Kavishe P & Gebre-Medhin M. The public healthimportance of IDD in Tanzania. Cent
Afr J Med 1988;34:60-5.
van Norren B, Boerma J & SempebwaE. Simplifying the evaluation of primary health care programmes. SocSci Med 1989;28:1091-97.
Vermiglio F, Lo Presti V, FinocchiaroM, Battiato S, Grasso L, Ardita F,Mancuso A & Trimarchi F. Enhancediodine concentrating capacity by themammary gland in iodine deficientlactating women of an endemic goiter
region in Sicily. J Endocrinol Invest1992;15:137-42.
Vitti P, Martino E, Aghini-Lombardi F, Rago T, AntonangeliL, Maccherini D, Nanni P,Loviselli A, Balestrieri A, Araneo
G & Pinchera A. Thyroid volumemeasurement by ultrasound inchildren as a tool for theasessment of mild iodinedeficiency. J Clin Endocrinol
Metab 1994;79:600-3.
Wächter W, Mvungi M, König A,Pickardt C & Scriba P. Prevalenceof goitre and hypothyroidism inSouthern Tanzania: effect of iodised oil on thyroid hormone
deficiency. J EpidemiolCommunity Health 1986;40:86-91.
Wächter W, Mvungi M, Triebel E, Vanthiel D, Marschner I, Wood W,Habermann J, Pickardt C & ScribaP. Iodine deficiency,hypothyroidism and endemicgoitre in Southern Tanzania. J
Epidemiol Community Health1985; 263-270.
Wang J, Harris M, Amos B, Li M,Wang X, Zhang J & Chen J. A tenyear review of the iodinedeficiency disorders program of the People's Republic of China. J
Public Health Policy 1997;18:219-41.
West KJ & Sommer A. Delivery of oral doses of vitamin A to preventvitamin A deficiency andnutritional blindnes. A state-of-the-art review. ACC/SCN State-of-
the-art series. Nutrition policydiscussion paper No 2. UnitedNations ACC/SCN, 1987.
WHO. Resolution 29. The 39thWord Health Assembly. Geneva:WHO, 1986.
WHO. National strategies forovercoming micronutrientmalnutrition (EB. 89.R11), 1992.
WHO. Indicators for assessingiodine deficiency disorders andtheir control through salt

7/26/2019 Controlling Iodine Deficiency Disorder
http://slidepdf.com/reader/full/controlling-iodine-deficiency-disorder 100/100
Stefan Peterson
iodation. WHO/NUT/94.6. Geneva:WHO/UNICEF/ICCIDD, 1994a.
WHO. Iodine and health: eliminating
iodine deficiency disorders safelythrough salt iodization: a statementby the World Health Organization.Geneva: WHO/NUT/94.4, 1994b.
WHO. Physical status: the use andinterpretation of anthropometry.Geneva, 1995.
WHO. Recommended iodine levels insalt and guidelines for monitoringtheir adequacy and effectiveness.
WHO/NUT/96.13.WHO/UNICEF/ICCIDD, 1996.
WHO. Joint WHO/UNICEF/ICCIDDconsultation. Review of findings from7-country study in Africa on leveles of salt iodization in relation to iodinedeficiency disorders, includingiodine-induced hyperthyroidism.WHO/NUT/97.5. Geneva, 1997.
WHO. Progress towards theelimination of Iodine Deficiency
Disorders (IDD). WHO/NHD/99.4.Geneva, 1999.
WHO & ICCIDD. Recommendednormative values for thyroid volumein children aged 6-15 years. BullWorld Health Organ 1997;75:95-97.
WHO/UNICEF/ICCIDD. GlobalPrevalence of Iodine DeficiencyDisorders, MDIS Working paper #1.Geneva: WHO, Micronutrient
inhibitory action of excess iodideon organic iodide synthesis in thenormal thyroid. Endocrinology1949;45:504-13.
World Bank. Investing in health.New York: Oxford UniversityPress, 1993.
Xu F, Sullivan K, Houston R, ZhaoJ, May W & Maberly G. Thyroidvolumes in US and Bangladeshischoolchildren: comparison withEuropean schoolchildren. Eur J
Endocrinol 1999;140:498-504.
Yazipo D, Ngaindiro LF, Barriere-Constantin L, Namboua L, PichardE, Ndoyo J & Bourdoux P.[Effectiveness of a wateriodination system for preventingiodine deficiency diseases inCentral Africa]. Santé 1995a;5:9-17.
Yazipo D, Ngaindiro LF, NambouaL, Ndoyo J, Pichard E, Barriere-Constantin L & Bourdoux P.Combatting iodine deficiency: the
iodization of water in the Central African Republic [letter;comment]. Am J Public Health1995b;85:732.
Zhao J, Xu F, Zhang Q, Shang L, Xu A, Gao Y, Chen Z, Sullivan K &Maberly G. Randomized clinicaltrial comparing different iodineinterventions in school children.
Public Health Nutrition1999;2:173-8.