Embed Size (px)
DESCRIPTION
National Iodine Deficiency Disorder Control Programme. Moderator: Prof. P.R.Deshmoukh Presenter: Rohan R Patil. Defination. - PowerPoint PPT Presentation
Citation preview

National Iodine Deficiency Disorder Control Programme
Moderator: Prof. P.R.DeshmoukhPresenter: Rohan R Patil

Defination
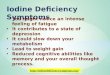
• Iodine deficiency disorders (IDD) refer to all of the consequences of iodine deficiency in a population that can be prevented by ensuring that the population has an adequate intake of iodine.
- World Health Organization

Spectrum of Iodine Deficiency Disorders
Foetus AbortionStill-birthCongenital anomaliesNeonatal cretinismMental deficiencyDiplegia SquintMyxedamotous cretinismDwarfismHypothyroidismPsychomotor Defects
Neonate Neonatal hypothyroidismChild and Adolescent Retarded mental and physical
developmentAdult Goitre and its complication
Impaired mental functionIodine induced hypothyroidism
All Ages Physical Sluggishness

Iceberg of IDD

Iodine Deficiency = Goiter = Visible Swelling
No Pain, Cosmetic problem
Cretinism: A rare event= LOW PRIORITY
Brain Damage
Lack of Energy - hypothyroidism
Learning Disability, ↑Deaths
Child Development & Child Survival
Human Resource Development
= HIGH PRIORITY
The hourglass of IDD
Historic view1962-1983
Current view1984 onwards

Defination of Iodine Deficiency Disorder as Public Health problem
None Mild moderate Severe
Total Goitre Rate
0.0-4.9% 5-19.9% 20.0-29.9% > =30%
Epidemiological criteria for assessing the severity of IDD based on the prevalence of goitre in school-aged children

Defination of Iodine Deficiency Disorder as Public Health problem
Median UI Iodine Intake Iodine Status
<20 Insufficient Severe Iodine Deficiency
20-49 Insufficient Moderate Iodine Deficiency
50-99 Insufficient Mild Iodine Deficiency
100-199 Adequate Adequate Iodine Nutrition
200-299 Above requirements
Likely to provide adequate intake for pregnant/ lactating women
>300 Excessive Risk of hypothyroidism/ Autoimmune thyroid dsease
Epidemiological criteria for assessing iodine nutrition based on median iodine concentrations of school age children ( 6 years)

Defination of Iodine Deficiency Disorder as Public Health problem
Median UI(Ug/dL) Iodine Intake<150 Insufficient150-249 Adequate250-499 Above requirements>500 Excessive
Epidemiological criteria for assessing iodine nutrition based on median or range in urinary iodine concentrations of PREGNANT WOMEN
Total goitre prevalence > 5%MUI (In more than 50% of population)
<100 ug/L
MUI ( In more than 20% of the population)
<50 ug/L
IDD could be defined as a public health problem if

Cause of Iodine Deficiency:
CAUSE
Effect on People
Effect on Animals
Low Availability of Iodine
Soil Erosion
Who’ s Affected
Humans
Livestock
Plants
Water, Soil
How Affected
Health and Socio-economic Impact
Clinical and reproductive Disorders, Decreased Productivity
Iodine poor feeds and fodder, Goitrogens
Environmental Iodine deficiency
Iodine Deficiency: How’s Affected

Magnitude of the problem among Indian states: (NIN study in
2003)
Region
% prevalence of goitre
% P of other signs of IDD
Salt Iodine (>15PPM)By spot Test
Northern
13.4 0.67 63.3%
Eastern
27.5 0.61 44.8%
North Eastern
6.1 0.03 77.9%
Central
10.7 0.62 29.7%
Southern
10.2 0.76 17.9%

Magnitude of problem across Maharashtra:
S.N.
District No. of goiter (1000 population)
1 Ahmednagar 11.06
2 Nanded 1.42
3 Nagpur 11.72
4 Wardha 10.3
5 Nashik 15.00
6 Hingoli 12.08
7 Aurangabad 14.04

Estimated % of household consuming adequately iodized salt:
Country % of householdBhutan 95China 93
Vietnam 77Bangladesh 70Indonesia 65
Nepal 63India 50
Myanmar 48

Use of iodized salt in households:
NFHS II NFHS III
>15 ppm 49.3 51.1
<15 ppm 28 25
0 ppm 22.7 23.9

Use of iodized salt in households: (NFHS III)
• r
Urban Rural Total
13
2924
16
3025
72
41
51
Not iodized Inadequately iodized Adequately iodized

PIONEER STUDY CONDUCTED IN KANGRA DISTRICT OF HIMACHAL PRADESH (1956-68)
• Location: Kangra Valley, Himachal Pradesh. Divided into 3 zones –A , B , C
• Type of study: Community based
• Study Period: 1956 – 1968
• Outcome variable: Goiter prevalence among school age children

STUDY DESIGN
• Baseline survey in 1956
• Salt distributed to three zones– Zone A : Salt + Potassium iodide– Zone B : Plain salt– Zone C : Salt + Potassium iodate
• 15 gms of salt/person/day– So as to ensure 200 µg of
iodine/person/day

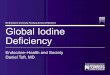
Prevalence of Goitre in Zone A (KI Salt) Prevalence of Goitre in Zone B (Plain salt till 1962, then KI salt)
Prevalence of Goitre in Zone A (KIO3 Salt)

Kangra Valley Study
• Conclusion: Iodine supplementation in the form
of adequately iodized salt on a regular and continuous basis reduces goiter prevalence
• Recommendation: To establish National Goiter Control
Programme.

National Goiter Control Programme
Launched at the end of second five year plan (1962)
Aims:• Initial survey to identify endemic areas• Production & Supply of iodized salt to endemic
areas• Impact assessment surveys after five year

NGCP activities (1962-1983)
• Goiter is a painless disorder which less liable to cause mortality.
• NGCP received low priority from the view point of government as a national public health programme and also from the populationSalt Iodization plants established in public sector
Rajasthan 5Gujrat:3West Bengal :4
Estimated need/year 1 million tonsProduction capacity/Year 0.38 million tonsActual Production/year 0.15 million tons

Universal Salt Iodization: (1983)
• GOI policy decision to iodize all salt meant for human consumption – Universal Salt Iodization (USI)
• Private sector was permitted and encouraged to produce iodized salt
• “Elimination of goiter” was included in Prime Minister’s 20-point National Development Program

National Salt Iodization
• Decision Phase: Enable a decision supported by mobilization of
industry, setting of standards and regulation
• Implementation Phase: Ensure infrastructure for iodization and
packaging of all human and livestock salt. Support with quality assurance and communications.
• Consolidation Phase: Once the goal of USI achieved, it needs to be
sustained through ongoing external evolution monitoring and periodic evolution.

Changing Status of legislation (1968-2005):
• 1968: Iodized salt brought under PFA Act• 1983: Policy decision taken for Universal Salt
Iodization• 1983: Iodized Salt brought under revised PFA
Act• 1997: Sale & storage of non-iodized salt
banned• 2000(May): GOI decided to lift ban on sale of
non-iodized salt.• 2000 (Sept): Ban on sale of non- iodized salt
was lifted.

An ICMR task force study, 1989
• Location: 14 districts of 9 states• Type of study: Community Based• Type of Population: Rural (all age groups,
both sexes)• Study Design: Multistage random sampling• Sample Size: 4,09,923• Year of data collection: 1984-86

PREVALENCE OF GOITRE & CRETINISM IN STUDY DISTRICTS
DISTRICT PERCENTAGE (%)
GOITRE CRETINISM
Vishakhapatnam 15.8 0.2
Dibrugarh 65.8 2.2
Muzaffarpur 33.7 1.7
Sitamari 31.8 1.1
Surat 22.7 0.4
Mandla 34.4 2.1
Dhule 16.5 0.1
Central Manipur 10.4 3.0
West Manipur 19.8 6.1
Nilgiri 6.9 1.7
Baharaich 20.2 0.2
Basti 20.0 0.4
Gorakhpur 18.6 0.1
Mirzapur 6.2 0.3
TOTAL 21.1 0.7

National Iodine Deficiency Disorders Control Programme (NIDDCP)
Objectives and components • Surveys to assess the magnitude of the Iodine Deficiency
Disorders. • Supply of iodated salt in place of common salt. • Resurvey after every 5 years to asses the extent of Iodine
Deficiency Disorders and the Impact of iodated salt. • Laboratory monitoring of iodated salt and urinary Iodine
excretion. • Health education. & Publicity

National Iodine Deficiency Disorders Control Programme (NIDDCP)
GOAL:
• To reduce the prevalence of iodine deficiency disorders below 10 percent in the entire country by 2012 A.D.

National Iodine Deficiency Disorders Control Programme (NIDDCP)
POLICY• To iodate the entire edible salt in the country
by 1992. The programme commenced in April 1986 in a phased manner
• To enhance the production, demand and supply of iodated salt
• banning the sale of non-iodated salt for direct human consumption in the entire country with effect from 17th May, 2006 under the Prevention of Food Adulteration Act 1954

National Iodine Deficiency Disorders Control Programme (NIDDCP)
• r Nodal Ministry: MOHFW
IDD Cell Central Level: DGHS
STATES/UNITON TERRITORY IDD CELL
State Health Directorate

National Iodine Deficiency Disorders Control Programme (NIDDCP)
Achievements:• The policy regarding production of iodated salt
has been liberalized, permitting production by the private sector.
• The annual production of iodated salt was raised from 5 lakh MT in 1985-86 to 49.83 lakh MT in 2005-06 expected to further rise to 50 lakh MT in the near future.
• The Salt Commissioner, in consultation with the Ministry of Railways:-under priority category ‘B’; a priority second to that of Defence.

National Iodine Deficiency Disorders Control Programme (NIDDCP)
• PFA, 1954: stipulate that the iodine content of salt at the production and consumption levels should be at least 30 and 15 ppm respectively.
• Banning the sale of non iodated salt for direct human consumption in the country with effect from 17th May, 2006
• NIDDCP has been included in the 20 Point Programme of the Prime Minister.

National Iodine Deficiency Disorders Control Programme (NIDDCP)
• To establish an IDD Control Cell in their State Health Directorates. Presently, 31 States/UTs have established such Cells.
• A National Reference Laboratory for the monitoring of IDD has been set up
• Four regional IDD monitoring laboratories has been set up

National Iodine Deficiency Disorders Control Programme (NIDDCP)
• Cash grants are also provided by the Central Government for health education and publicity campaigns to promote the consumption of iodated salt.
• For ensuring quality control of iodated salt at consumption level, testing kits for ‘on the spots’ qualitative testing have been distributed

National Iodine Deficiency Disorders Control Programme (NIDDCP)
FINANCIAL ASSISTANCE PATTERN TO STATES/UT
• Financial assistance is being provided to all the states/UTs’s in form of quarterly advance release of funds from 2002-03 for various components under the programme.
IDD SURVEYS• Financial assistance of Rs. 25000 per district is
being provided to State/UT IDD Control Cells for conducting surveys for assessing the magnitude of goiter and other IDD.

The stakeholders in Iodine Deficiency Disorder control Programme (IDDCP):
• Elected representatives• Government ministries • Salt producers, importers and distributors• Concerned civic groups, Professional
organizations• Nutrition, food and medical scientists

National Iodine Deficiency Disorders Control Programme (NIDDCP)
Components• Political Support: Primarily at governmental level, through the
minister of health and the executive group of government.
• Administrative arrangements: A social model for a national IDD control
programme

National Iodine Deficiency Disorders Control Programme (NIDDCP)
• Indicators of IDD assessment:Grade 0
No palpable or visible goitre.
Grade 1
A goitre that is palpable but not visible when the neck is in the normal position,(i.e., the thyroid is not visibly enlarged). Thyroid nodules in a thyroid which is otherwise not enlarged fall into this category
Grade 2
A swelling in the neck that is clearly visible when the neck is in a normal positionand is consistent with an enlarged thyroid when the neck is palpated

National Iodine Deficiency Disorders Control Programme (NIDDCP)
Indicators goalProportion of households consuming adequately iodized salt
>90%
Proportion of population with urinary iodine levels below 100 μg/l
<50%
Proportion of population with urinary iodine levels below 50 μg/l
<20%
Indicators of IDD assessment:

Five year PlansTENTH Five Year Plan (2002-2007):• Effforts to reduce price differentials between
iodised & non-iodised salt• More cost effective targeting of the PDS to
address macro and micronutrient deficiencies NIDDCP FOR THE 11TH PLAN:• To bring down prevalence of IDD below 10%
in the entire country by 2012 AD.• To ensure 100% consumption of adequately
iodated salt (15 PPM) at the household level.

Why consumption of adequately iodized salt was decreased?
•Government of India lifts ban on sale of Non-iodized salt •Increase in Rail Tariff – 1st April 2002•Consequently increase in movement of iodized salt by road (especially from Rajasthan)•Currently, No mechanism in place for monitoring quality of iodized salt transported by road•Disappearance of most common visible effect of iodine deficiency i.e. goiter•Perception in people that : - iodized salt consumption is NOT required anymoreCommunication strategy•DID NOT focus on mental handicap as a consequence of iodine deficiency•WAS NOT commensurate with seriousness of problem both in terms of scale & frequency

Action to be Taken
• Supply– Salt Industry Support Small scale salt producers
• Potassium iodate subsidy Initial assistance for repair and maintenance of salt iodization plants
• Technical & training support

INFORMATION, EDUCATION AND COMMUNICATION (IEC)
• Radio/TV spots have been prepared and their broadcast/telecast is being carried out.
• A 10 minutes video film on IDD has been prepared and is being distributed to the States.
• Pamphlets have been developed for distribution to States & UTs.
• Posters depicting the various facets of IDD manifestation have also been prepared.
• Salt Testing Kits for the qualitative testing of iodated salt to show presence of iodine are being used for creating awareness among people, including those living in remote, rural areas and urban slums.

INFORMATION, EDUCATION AND COMMUNICATION (IEC)
• Discouraging the production of large crystals of Bargara salt for edible use which cannot be iodated uniformly.
• Sensitizing iodated salt manufacturers about their role in quality monitoring.
• IEC activities have also been intensified in coordination with the Song & Drama Division, Directorate of Field Publicity DAVP Doordarshan & AIR with a view to promote the consumption of iodated salt among the masses.

Communication Challenges to overcome
• A) Penetrate the system with key messages
• B) Communication Themes

References:
WHO, Iodine status worldwide WHO Global Database on Iodine Deficiency, WHO:2004.WHO, UNICEF, ICCIDD Assessment of iodine deficiency disorders and monitoring their elimination, A guide for programme managers, WHO:3 ; 2007.Umesh Kapil. Current status of salt iodization and level of iodine nutrient in India African Journal of Pharmacy and Pharmacology Vol. 2 (3). pp. 066-076, May, 2008.Pandav CS , Yadav K,Karmarkar MG. The Success story of Iodine Deficiency in India: Science, Statesman and Society Wisdom in Hindsight; ICCIDD New Delhi, Sept 2010.ICMR task force study preliminary analysis of report 1989.Revised Policy Guidelines On National Iodine Deficiency Disorders Control Programme October 2006