Embed Size (px)
Citation preview

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board 1203 Front Street | Raleigh NC 27609
wwwncmedboardorg | infoncmedboardorg 8002539653
Controlled Substances Prescribing
What Every Provider Needs to Know
Brooke A Chidgey MD Clinical Assistant Professor of Anesthesiology University of North Carolina School of Medicine
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Learning Objectives
bull Promote best practices for managing chronic pain and prescribing controlled substances through the CDC Guideline
bull Identify strategies for recognizing signs of misuse and abuse of prescription opioids
bull Describe strategies for communicating with patients about avoiding or reducing prescription opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CURRENT STATE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
00
50
100
150
200
250
300
350
400
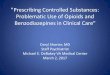
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Death
s p
er
1000
00 p
op
ula
tio
n
Year
Motor Vehicle Traffic (Unintentional)
Drug Poisoning (All Intents)
Firearm (All Intents)
α
1989 ndash Pain added as 5th Vital Sign
Per 10000 age-adjusted to the 2000 US Standard Population α - Transition from ICD-8 to ICD-9 β ndash Transition from ICD-9 to ICD-10
National Vital Statistics System httpwondercdcgov multiple cause dataset Source Death files 1968-2014 CDC WONDER Analysis by Injury Epidemiology and Surveillance Unit
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Learning Objectives
bull Promote best practices for managing chronic pain and prescribing controlled substances through the CDC Guideline
bull Identify strategies for recognizing signs of misuse and abuse of prescription opioids
bull Describe strategies for communicating with patients about avoiding or reducing prescription opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CURRENT STATE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
00
50
100
150
200
250
300
350
400
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Death
s p
er
1000
00 p
op
ula
tio
n
Year
Motor Vehicle Traffic (Unintentional)
Drug Poisoning (All Intents)
Firearm (All Intents)
α
1989 ndash Pain added as 5th Vital Sign
Per 10000 age-adjusted to the 2000 US Standard Population α - Transition from ICD-8 to ICD-9 β ndash Transition from ICD-9 to ICD-10
National Vital Statistics System httpwondercdcgov multiple cause dataset Source Death files 1968-2014 CDC WONDER Analysis by Injury Epidemiology and Surveillance Unit
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CURRENT STATE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
00
50
100
150
200
250
300
350
400
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Death
s p
er
1000
00 p
op
ula
tio
n
Year
Motor Vehicle Traffic (Unintentional)
Drug Poisoning (All Intents)
Firearm (All Intents)
α
1989 ndash Pain added as 5th Vital Sign
Per 10000 age-adjusted to the 2000 US Standard Population α - Transition from ICD-8 to ICD-9 β ndash Transition from ICD-9 to ICD-10
National Vital Statistics System httpwondercdcgov multiple cause dataset Source Death files 1968-2014 CDC WONDER Analysis by Injury Epidemiology and Surveillance Unit
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
00
50
100
150
200
250
300
350
400
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Death
s p
er
1000
00 p
op
ula
tio
n
Year
Motor Vehicle Traffic (Unintentional)
Drug Poisoning (All Intents)
Firearm (All Intents)
α
1989 ndash Pain added as 5th Vital Sign
Per 10000 age-adjusted to the 2000 US Standard Population α - Transition from ICD-8 to ICD-9 β ndash Transition from ICD-9 to ICD-10
National Vital Statistics System httpwondercdcgov multiple cause dataset Source Death files 1968-2014 CDC WONDER Analysis by Injury Epidemiology and Surveillance Unit
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
00
50
100
150
200
250
300
350
400
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Death
s p
er
1000
00 p
op
ula
tio
n
Year
Motor Vehicle Traffic (Unintentional)
Drug Poisoning (All Intents)
Firearm (All Intents)
α
1989 ndash Pain added as 5th Vital Sign
Per 10000 age-adjusted to the 2000 US Standard Population α - Transition from ICD-8 to ICD-9 β ndash Transition from ICD-9 to ICD-10
National Vital Statistics System httpwondercdcgov multiple cause dataset Source Death files 1968-2014 CDC WONDER Analysis by Injury Epidemiology and Surveillance Unit
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina
North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Rx and Drug Overdose Prevention Partners
Research and Evaluation
Prevention Policy Harm Reduction
Prescription Drug Monitoring
Program
Carolinas Poison Center
Enforcement and Regulation
Pain Patient Support
Data and Surveillance
Drug Take Back
Communication Advocacy
Funding
Pharmaceuticals
Community Coalitions
Local Public Health Substance Use
Disorder Treatment Recovery Services
DPH DMHDDSAS DMA DPS ORH
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMBrsquos Response
bull Implementing new programs and initiatives
bull Developing resource pages
bull Increasing communication with doctors and PAs through presentations forum articles website notices and social media
bull Participating in workgroups advisory boards
bull Developing and promoting training on opioids
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
PROGRAMS AND INITIATIVES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Programs and Initiatives
bull Controlled Substances CME Requirement
bull NC Controlled Substances Reporting System (CSRS) oRegistration
oUtilization
bull Adoption of CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CONTROLLED SUBSTANCE SPECIFIC CME REQUIREMENT
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
NCMBrsquos primary goal is to ensure that licensees who prescribe controlled substances ndash
particularly opioids ndash do so in a manner that is safe appropriate and consistent with current
standards of care
Requiring CME in controlled substances prescribing and related topics is one way of
supporting this
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
bull Effective July 1 2017
bull Complete specific CME
oControlled substances prescribing practices
oRecognizing signs of misuse and abuse
oControlled substance prescribing for chronic pain management
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NORTH CAROLINA CONTROLLED SUBSTANCE REPORTING SYSTEM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull Prescription drug monitoring program
bull Information on controlled substance prescriptions written and dispensed in NC o Aid in patient safety
o Identify patients at risk
o Improve opioid prescribing practices
bull Utilization now considered a best practice when prescribing for pain patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Query
A
A
B
C
D
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS
bull New patient or first encounter prescribing controlled substances for patient
bull Intermittently thereafter based on risk
bull Can register a ldquodelegaterdquo to perform queries for you
bull Use best judgment
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC CSRS Data Points
In the 4th quarter of 2016 bull 18 million opioid prescriptions written by
39682 prescribers in NC bull 508279 queries completed in advance
representing a 28 utilization rate bull 23556 prescribers in NC and 1521
delegates registered with CSRS
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NC Controlled Substances Reporting System (CSRS)
bull 2016 NC law mandating registration
bull Physicians and PAs who have valid DEA registration
bull Law goes into effect when DHHS and CSRS update the system to meet specific requirements
bull NCMB encouraging voluntary registration
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
NCMB POSITION STATEMENT ADOPTION OF THE CDC GUIDELINE
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Provide safe effective outpatient pain treatment
bull Not intended for patients who are in active cancer treatment palliative care or end-of-life care
bull Recommendations in the Guideline may not meet the needs of all patients ndash use your professional judgment when providing care
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
bull Determining when to initiate or continue opioids for chronic pain
bull Opioid selection dosage duration follow-up and discontinuation
bull Assessing risk and addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section I Determining when to initiate or continue opioids for chronic pain
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 1
bull Nonpharmacologic and nonopioid therapies are preferred for chronic pain
bull Benefits of opioid use must outweigh risks
bull Should benefit in both pain and function
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Function
ldquoPain average interference with Enjoyment of life
and interference with General activityrdquo Assessment Scale
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 2
bull Before starting opioid therapy establish realistic treatment goals
bull Consider how therapy will be discontinued if benefits are no longer outweighing risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 3
bull Before prescribing opioids discuss the known risks of this therapeutic option
bull Discuss the responsibility of the patients and providers to reduce these risks
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Discussion Topics
bull Severe adverse effects and common side effects
bull Risks with other drugs
bull Risks when driving
bull Risks of opiate use disorder
bull Appropriate storage and risk to others
bull Precautions being taken to reduce risk (UDS naloxone pill count PDMP etc)
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
A Different Discussion
bull Lack of evidence of long-term benefit of opioids for chronic pain
bull Poor efficacy in neuropathic pain
bull Can worsen other pain conditions
bull Opiate-induced hyperalgesia
bull Difficulty controlling post-procedural pain in future
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section II Opioid selection dosage duration follow-up and discontinuation
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 4
bull Use immediate-release medications when initiating opioid therapy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 5
bull Prescribe lowest effective dosage
bull Carefully reassess individual benefit and risks when increasing to ge 50 MMEday
bull Avoid increasing to ge 90 MMEday OR carefully justify decision
bull Consult with pain specialist
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 6
bull When prescribing opiates for acute pain prescribe minimum quantity needed for severe pain
bull 3 days will often be sufficient rarely more than 7 days worth is needed
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 7
bull Evaluate benefits and harms within 1 to 4 weeks of starting opioid
bull Evaluate at least every 3 months thereafter
bull Taper opioids as necessary
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Concerning Behaviors
bull Requesting early refills
bull Missing pills (stolen lost ruined)
bull Inappropriate urine drug screens
bull Obtaining opioids from others
bull Using multiple pharmacies
bull Dishonesty during encounter
bull Appearing sedated
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Tapering
bull Reduce dosage by 10-50 weekly
bull Rapid taper over 2-3 weeks for ldquosevere adverse event such as overdoserdquo
bull May need to pause and restart
bull Taper considered successful if patient making progress
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
CDC Guideline
Section III Assessing risk and
addressing harms of opioid use
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 8
bull Evaluate risk factors for opioid-related harms
bull Implement strategies to mitigate risk
bull Naloxone for higher risk patients
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
At Risk Populations
bull Sleep apnea
bull Renal or hepatic insufficiency
bull ge 65 years old
bull Mental health conditions
bull Substance use disorder
bull Prior nonfatal overdose
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 9
bull Review prescription drug monitoring program for dosages and dangerous combinations
bull Review before initiation of opioid and at least every 3 months
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 10
bull When prescribing opiates for chronic pain perform urine drug testing before starting opiate therapy
bull Consider repeating at least annually
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Urine Drug Screening
bull Looking for
o Illicit drugs
o Prescribed drugs
o Drugs taken but not prescribed
bull Need context for interpretation
o When was last dose
o How does patient take medication
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Results
bull What are you testing for
bull Drug metabolites
o Hydrocodone Hydromorphone
o Oxycodone Oxymorphone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Patient Dismissal
bull Do not dismiss patient from practice based on urine drug test result
bull Could be considered abandonment
bull Could leave patient at risk
bull A missed opportunity
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 11
bull Avoid prescribing opioid pain medication and benzodiazepines concurrently whenever possible
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Recommendation 12
bull Clinicians should offer or arrange evidenced-based therapy for patients with opioid use disorder
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
TurnTheTide
ldquoWe have to stop treating addiction as a moral failing and start seeing it for what it is a chronic disease that must be treated with urgency and
compassionrdquo
ndash Dr Vivek H Murthy United States Surgeon General
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Key Points
bull Evaluate YOUR patient
bull Assess individual risks and benefits
bull Avoid opiates if you can
bull Start low and go slow
bull Reassess throughout (days ndash 3 months)
bull 50 MME and 90 MME are NOT strict limits
bull Use opportunities to get patients help
bull Document document document
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
IMPLEMENTING THE GUIDELINE CASES
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
57yo M presents as a new patient to your clinic He states he has been using opiates for the last
10 years to control his pain His most recent regimen has been Oxycodone ER 60mg twice
daily He is looking to establish care with you to take over his prescription He also takes
pregabalin 100mg twice daily for neuropathy
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Patient has had numerous back surgeries over the years He has tried and failed the following therapies
bull Physical therapy TENS unit home exercises
bull Gabapentin duloxetine topical lidocaine
bull NSAIDs contraindicated due to gastric ulcers
bull Epidural steroid injections
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Other Information
bull No alcohol smoking or drug history
bull Works daily at his farm tending to crops and animals
bull Denies side effects to medication regimen except constipation which is controlled through diet
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr H
bull Patient has remaining pills in bottle with him
bull NC CSRS reveals history of one provider prescribing current regimen for last 4 years
bull No other controlled substances besides pregabalin
bull POC UDS +oxycodone
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
What Would You Do
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Ms M
43yo F presents as a new patient with severe back pain ever since she had her child 4 years
ago She has been taking oxycodone 15mg every 4 hours for pain because nothing else
works She is now out of her medication and needs a refill
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Further Questioning
Previous imaging studies with mild disc degeneration Cannot tolerate PT or exercise due to pain Is not willing to try gabapentin or other adjunctive therapies because she ldquoknows what worksrdquo
Patient unable to leave urine specimen
NC CSRS reveals numerous small prescriptions from multiple providers
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Next Step
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Mr E
51yo M longtime patient on hydrocodoneAPAP 10325mg q6hr prn pain Patient calls for early
refill because going on a trip
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
2 Months Later
Patient returns but is short on pills because he left some at home in his pill organizer
Urine drug screen performed revealed no substances Patient reported last use was this AM
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Now What
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Resources
o wwwncmedboardorgprescribingcme
o wwwncmedboardorgsafeopioids
o Dowell D Haegerich T Chou R et al CDC Guidelines For Prescribing Opioids for Chronic Pain MMWR Recomm Rep 201665(No 1) 1-49
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Controlled Substances CME Requirement
Who must comply with new requirement
bull All physicians and PAs who prescribe controlled substances
bull Residents who hold a full medical license
bull Maintenance of Certification participants who prescribe controlled substances
For other questions on the controlled substances CME visit wwwncmedboardorgprescribingcme
North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg

North Carolina Medical Board wwwncmedboardorg | infoncmedboardorg
Questions
bull Website wwwncmedboardorg
bull Call 18002539653
bull Email infoncmedboardorg