Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1968, 31, 99-105
Contribution to the study of late cervicalsyringomyelic syndromes after dorsal or lumbar
traumatic paraplegiaA. B. ROSSIER, A. WERNER, E. WILDI, AND J. BERNEY
From the Geneva University Cantonal Hospital,Switzerland
Works dealing with a cervical syringomyelicsyndrome of late appearance and at a distance fromthe initial traumatic cord lesion are few in number(Cossa, 1943; Freeman, 1959; Finkle, 1960; Jung,1960; Schott, Trillet, Vauterin, and Koshbin, 1962;Martin and Maury, 1964; Riffat and Domenach,1964; Bischof and Nittner, 1965; Barnett, Botterell,Jousse, and Wynn-Jones, 1966). The incidence ofsuch complications being rare, between 1 and 1-5%(Martin and Maury, 1964; Barnett et al., 1966),we believe it interesting to report a similar case inorder to describe in detail the nosological aspectsof this affection. Of the 132 traumatic cord lesionsthat we have examined so far, we have not foundanother case.
CASE HISTORY
On 22 April 1965, the patient, a 15-year-old boy, fellfrom a height of 20 m. He sustained a compressionfracture of D6, D7, and D8 vertebrae with immediateparaplegia at D6 which remained complete. There wasno loss of consciousness. Treatment was conservative.Twelve months after the beginning of the paraplegia,
the following was observed: the triceps reflex in the leftarm had disappeared; there had been a rise in the levelof the thermo-analgesia on the left side which hadpassed from D6 to D2, while a lack of feeling wasevident in the left upper extremity; this was also of thesyringomyelic type without motor deficit. The patientthen revealed that for about two weeks he had had inthe swimming-pool no appreciation of warmth in hisleft hand.
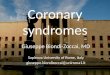
Air myelography (31 May 1966) (Dr. J. Berney) bythe suboccipital and lumbar routes showed considerablewidening of the cervical cord from C3 to C7, revealingin addition a fracture of the spinous process of C7that was confirmed later by histological examination(Figs. la and b).A laminectomy of C2 to C7 (10 May 1966) (Professor
A. Werner) revealed diminution of the thickness of thelaminae of C3, C4, and C5 and a distended dural sacwithout pulsation. The swollen spinal cord showed
flattening of the roots along its sides; a cord torsionbrought the emergence of the left posterior roots almostto the median line. The lateral columns showed a bluishcolour in places and covered a cavity which extendedfrom C3 to C7. Puncture caused shrinking of the cordand yielded 2-3 ml of clear yellowish liquid which didnot coagulate. An incision over the dorsal medianseptum, at the height of C5, made possible a penetrationinto the cavity. A little fragment of gutta percha wasinserted in the incision to prevent it from closing(Dr. J. Berney).
Tables 1 and 2 and Figs. 2-6 illustrate the evolutionof reflexes and of the sensory and muscle deficit beforeand after the operation.
DISCUSSION
SYMPTOMATOLOGY One of the first signs whichoften precede the appearance of the syringomyelicsyndrome is pain-abdominal, thoracic, cervical, orat the level of the arms (Schott et al., 1962; Barnettet al., 1966).
In our case, we noted that one month beforebeing aware of the thermanaesthesia in his lefthand, our patient had complained of dorsal painswhich were initially attributed to the muscularefforts of the motor re-education; they disappearedwith massage in a few days but were followed twomonths later by neck pains. Moreover, palpationof the spinous process of C7 and DI was painful.It is interesting to note that these pains disappearedafter air myelography.
This painful symptomatology is accompanied byan ascending loss of sensation for temperature andpain which little by little reaches the cervicalsegments, sometimes even involving the trigeminalnucleus (Martin and Maury, 1964; Barnett et al.,1966). Accompanying or following the thermo-analgesia, by order of frequence and decreasinglesional importance, it seems that muscle power isfirst affected and then light touch and deep sensa-tion. As a rule, at the level of the involved upper
99

A. B. Rossier, A. Werner, E. Wildi, andJ. Berney
limbs, there is total or partial loss of reflexes.Although rarer, one may find signs of damage tothe autonomic nervous system, such as ClaudeBernard Homer's syndrome and uneven sweating;our patient was free of this as well as of anyarthropathy (Martin and Maury, 1964; Bamett et al.,1966).During the aggravation of the sensory deficit, it
was first the sensitivity to temperature and painthat was the more affected and the more rapidly,whereas touch sensation deteriorated more slowlyand less seriously; after the opreration, the reverseappeared, tactile sensation improving first and morerapidly.
In most observations found in the literature, aswell as in our case, between the initial cord leveland the zone affected by the syringomyelic syndrome,there was no cutaneous area in which the differentsensory modalities were all spared. However, inthe few cases in which this was found (Schott et al.,1962), only the repetition of a complete neurologicalexamination in the course of months would havebeen able to confirm or invalidate the persistenceof its neurological integrity. During our firstexamination of 13 May 1966, it was difficult toascertain if there were such a cutaneous normal
FIG. I a.FIG. l b.
area because of the proximity of the segments inquestion. Although on the left the thermaesthesiahad risen to D1, the segments D2 and D3 seemedto have maintained their sensitivity to touch,temperature, and pain. This was no longer thecase in subsequent examinations. The progressionof a pathological process within the cord cannotdevelop everywhere in a uniform manner (Holmes,1915); thus, it must be possible to find in an inter-mediate area, according to the moment whenexamination takes place, the presence of somesensory modalities.The information yielded by myelography seems
to be of variable value; of the seven myelographiesof Barnett et al. (1966), four showed widening ofthe cervical cord. However, one should bear inmind the fact that not all authors have made thisexamination systematically. Moreover, the myelo-graphic techniques vary, making comparison oftheir results difficult. Nevertheless, it is especiallyair myelography, as was employed in our case,which should enable an early diagnosis to be made.
PATHOGENESIS The paucity of cases and especiallythe rarity of operative reports and necropsies makeall explanation of the aetiology of this syringo-
Air myelography showing widening of the cervical cordfrom C3 to C7.Fracture ofspinous process of C7.
100

Study of late cervical syringomyelic syndromes after dorsal or lumbar traumatic paraplegia
TABLE ICLINICAL DETAILS OF PATIENT1
Left side
1965 1966 1965
Reflexes 28.9 13.5 2.6 4.6 8.6 5.7 30.8 23.12 28.9
1966
13.5 2.6 4.6 8.6 5.7 30.8 23.12
Biceps C4-C5-C6Triceps C6-C7-C8Pronators C6-C7-C8Brachioradialis C5-C6Tromner C8-DlHoffman-Knips C8-DISup. abdominal D6-D7Middle abdominal D8-D9Inferior abdominalDIO-Dl l-D12
Cremasteric LI -L2Patellar L2-L3-L4Achilles L5-S1-S2Plantar L5-SI-S2Anal S2-S3-S4Bulbo-cavernosus
glans/catheter S2-S3-S4Anal tone
+ + + + +--+- +
+ X- +. + + ++++T +
+ + + + + + ++
+ +1 -t + + + +-
+ ++
±1 +
Bab.2
+ +
+4+4Bab.2
+
+
+
-3 -3 -
+ +- +_
+ +- +_
+
+ + +
++ +4 + ++4 +4 + 1 +Bab. Bab.2 Bab.2
-4- +
++ ++
+4+4Bab.2
-3 - _ _
+ -
+ -
+
++ -44+4 +-4Bab. Bab.2
+
+ +±
I = polycinetic 2 = withdrawal 3 = diffusion to pectoralis major 4 = clonus
'Patient's name: de T. N. Date of birth: 14.5.1950. Diagnosis: spastic compl. traumatic myelopathy Th.6-Th.7 (22.4.1965). Appearance ofneurological disturbances in the left upper extremity: end of April 1966. Laminectomy: 10.6.1966.
myelic syndrome hypothetical. However, the opera-
tive status of our patient and the correspondenceof the symptoms with those of the cases mentionedin the literature lead one to believe that it is a
similar if not an identical pathological process.A true syringomyelia does not seem probable.
Its order of frequency, according to Mcllroy andRichardson (quoted by Barnett et al., 1966), is0-01 % of the population of a large general hospital.The incidence of 13% mentioned by Martin andMaury (1964) and by Barnett et al. (1966), as wellas our figure of 08%, permit one practically toexclude this diagnosis. With the exception of therenal malformation of the case of Jung (1960), theabsence of associated malformations, in particularof the spine and central nervous system, speaks inthe same sense.None of the authors cited has noticed any lesion
of the cervical spine accompanying the initial dorsalor lumbar injury; it seems improbable that thefracture of the spinous process of C7 in our patientplayed a role in the formation of the cervical cavity.The evolution of the neurological deficit, ascendingsimultaneously from two different levels, cervicaland dorsal, is also against such a hypothesis.A syringomyelic syndrome can be explained only
on the basis of an intramedullary lesion. Arachnoid-itis per se cannot be considered-none was foundwhen our patient was operated upon. However,it is known that it can become complicated by intra-medullary cavitations.
The hypothesis of cavitation secondary to cervicalhtematomyelia occurring at the time of the initialaccident must apparently be rejected. Traumatichematomyelia is generally accompanied by im-mediate neurological symptoms and, in the course
of the last few years, most histological examinationsof spinal cord injuries have shown that it is more
rare than was supposed. When the hemorrhagewithin the cord is sufficiently severe, it can lead tothe formation of round or oval cavities in the poster-ior columns with clinical features similar to thoseof true syringomyelia (Minor, 1904). According toWolman (1965), these cavities could spread tonumerous segments, even affecting the wholecervical cord and the upper dorsal cord. Such an
aetiology cannot have existed in our case becauseof the absence of initial clinical signs at the cervicallevel; furthermore, in nervous parenchyme,organization of extravasated blood, pure or asso-
ciated with necrosed tissue, is not, to our knowledge,accompanied by an oedematous reaction. When itresults in the formation of cavities, the contents are
not under increased pressure.Among the remote effects of a cord trauma, there
is the aggravation of a neurological deficit ap-
parently stabilized. Marburg (1936) has stressedthe possibility of late hemorrhage and of secondaryvascular changes, the 'traumatic vasopathies',likely to cause progressive cord lesions. Thesepatches of softening can result in the formation ofcavities, as can a patch of heematomyelia. They occur
2
Right side
101

102
Light touch
D2
A. B. Rossier, A. Werner, E. Wildi, andJ. Berney
Pbin (pin-prick) Thermaesthesia Light touch Pain (pin-prick) Thermaoesthesia
Vibration sense 1 no chanqe at the upper left extremityJoint position sense as compared with the right side
FIG. 2. Patient: de T.N. & 1950. Date of examination: FIG. 3. Patient: de T.N. S 1950. Date of examination:
13 May, 1966. Examiner: R/He. 24 MaY, 1966. Examiner: RIHe.
Light touch Pain (pin-prick) Thermaesthesia Light touch Pain (pin-prick) Thermaesthesia
Laminectomy 10 June 1966
FIG. 4. Patient: de T.N. d 1950. Date of examination. FIG. 5. Patient: de T.N. s 1950. Date of examination:
2 June, 1966. Examiner: RIHe. 21 June, 1966. Examiner: He.
Light touch Pain (pin-prick) Thermaesthesia
Key to figs. 2-bAn.Slight hypo.Hypo-
- Marked hypo.
FIG. 6. Patient: de T.N. d 1950. Date of examination:23 December, 1966. Examiner: R.

Study of late cervical syringomyelic syndromes after dorsal or lumbar traumatic paraplegia
most commonly in the posterior horns and columnsbut may also be found near the central canal, atthe level of the anterior horns. They are accom-panied by a syringomyelic symptomatology. In ourcase, should a process ending in a myelomalaciahave developed, one could explain the enlargementof the spinal cord only by the formation of a cavitywith an increase of its internal pressure. This intra-cavital hypertension could result from changes inthe colloido-osmotic (oncotic) pressure by amechanism comparable to the one proposed byZehnder (1937) to explain some late clinical symp-toms of chronic subdural hematoma.With war-wounded patients Holmes (1915)
found paramedian cavities above and/or below theinitial lesion, at the level of the posterior columnsand usually unilateral. According to this author,neither the grey matter, with the exception of oneof his cases, nor the ependymal canal, was affected.These cavities remained generally connected to the
initial cord lesion by a small track of oedematoustissue or by a fissure, and must have containedliquid under pressure since they compressed theadjacent structures. Holmes (1915) thought thatthey developed from the accumulation of a tran-sudate and of products of tissue degeneration whichcould be seen in serial sections.
After cord trauma, Minor (1904) noted changesin the vascular walls in the form of a hyalinedegeneration with fatty degeneration of theendothelium. He also noted oedema of the vascularwalls sufficient to obliterate the lumen or evento cause thrombosis of the vessel. If to the primarycondition of tissue necrobiosis there be addedsecondary disturbances due to local circulatoryinsufficiency, it would seem that a sufficient numberof circumstances would be gathered to causesecondary cavitations. In some cases the reversibilityof the initial neurological symptoms is traditionallyattributed to regression of post-traumatic cord
TABLE IIMUSCLE TEST CARRIED OUT IN 19661
Right
3.6 8.6 21.6 7.7 30.8 23.12 3.6 8.6 21.6 7.7
Shoulder-blade Serratus
Trapezius sup.Trapezius inf.Trapezius middleRhomboides
Shoulder Deltoides ant.Latissimus dorsiTeres majorDeltoides middleDeltoides post.Pectoralis majorExt. rotat.Int. rotat.
Elbow TricepsBicepsBrachioradialis
Forearm SupinatorsPronators
Wrist Flexor carpi radialisFlexor carpi ulnarisExtensor carpi radialis longusExtensor carpi radialis brevisExtensor carpi ulnaris
Fingers LumbricalesFlexor digitorum superficialisFlexor digitorum profundusExtensor digitorum communisInterossei palm.
Thumb
Interossei dors.Abductor quinciOpponens quinciFlexor pollicis brevisFlexor pollicis longusExtensor pollicis brevisExtensor pollicis longusAbductor pollicis brevisAbductor pollicis longusAdductor pollicisOpponens pollicis
5 5? 5 5 5 5 5? 4+ 4+ 55 5? 5 5 5 5 5? 5 5 55 5? 5 5 4+ 5? 4 4+ 5
5 5 4+ 4+ 4 4+ 55 55 5 5 5 4+ 5 4+ 4 4+ 4+
5 5 4 4 3 2+ 3 35 45 5 4+ 5 4+ 4+ 4 3 3 3+5 5 4+ 5 4+ 5 4 3+ 4 3+5 4+ 5 5 5 4+ 4 4 4+ 4+5 5 5 5 5 5 4+ 4 4 4+5 5 5 5+ 5 5 4+ 4 4 4+5 4 4+ 5 5 4+ 4 4+ 5-
4 5 5 5 4 5 4 5-
5 4+5 5 5 5 4 4+ 4 4+
4 4 4+ 4 4+5 5 5 4+ 4+ 4 4+ 4+ 5
5 5 4+ 4 4 4 45- 5 4- 3+ 4
5 4+ 4+ 45 5 4+ 4+5 4+ 5 5- 5 5 4 3-4 4 3+ 3+ 4+5 4+ 5 4- 5 4+ 4 3t+ 4 3+ 4 4+5 5 5 5 5 5 4 4+ 4 4+ 5
5 5 5 5 5 4+ 4 4 3+ 3+ 45 5 5 5 5 4 4 4 3- 3+ 4
3+5 5 5 5 5 4+ 4 4 3 3+ 45 5 5 5 5 4+ 4+ 4+ 4 3+ 4+5 5 5 5 4+ 4 4 4 4 3 45 4+ 5 5 5 4+ 4 4+ 4 4 45 5 5 5 5 4+ 4 4+ 4 4 4+5 5 5 5 5 4+ 4++ 4+ 4 4 4+5 5 5 5 5 4+ 4+ 4+ 4 4 4+5 5 5 5 5 4+ 4 4+ 4 4 4+5 5 5 5 5 4+ 4 4 4 4 45 5 5 5 5 4+ 4 4+ 4 3 45 4+ 5 5 5 3+ 3+ 4 4 4 4+
'Testing according to the nomenclature of the British Medical Research Council in 1943.
Left
30.8 23.12
103

A. B. Rossier, A. Werner, E. Wildi, andJ. Berney
oedema; however, there are oedemas which areaccompanied by destruction of the myelin sheathsand axis cylinders. This process is then identifiedwith myelomalacia (Marburg, 1936) and corres-ponds to what Jellinger (1966) has called 'atypischeOedemnekrosen', the characteristic of which is notorganization but liquefaction. Marburg (1936) hasexplained the late appearance of the syringomyelicsyndrome by the fact that necrobiosis developsslowly. Cavitation could evolve silently until itsvolume has become sufficient to cause compressionof the adjacent structures.
Zuilch (1962) has explained the 'pencil-like'necrosis on the basis of a circulatory insufficiencyat the level of the arteriae coronae. This ischaemicnecrosis would occur more easily in watershedareas between two different vascular territories asat the level ofD4-D5. Likewise, an insufficient irriga-tion of the watershed area depending on the posteriorspinal arterial system and the branches of the anteriorspinal artery could explain necrosis at the level ofthe posterior horns or of the posterior grey com-missure, the grey matter being affected first becauseof its greater need of oxygen. It is possible that avascular pathology may be not only arterial butalso venous in origin, local circulatory disturbancesgiving rise to stasis and hence necrosis (Jellinger,1966). In both cases resorption of the necrotictissue could result in secondary formation ofcavities.Whether it is a question of the aggravation of the
neurological symptoms or of their post-operativeimprovement, their simultaneous evolution from twodifferent levels, cervical and dorsal, over severalsegments, would suggest the possibility of ananatomo-pathological continuity between them.Rather than postulate a pathogenesis sui generis,one could postulate that the pathological processhas its origin at the level of or above the initialcord lesion; it would reveal itself only after veryvariable lapses of time, from four months to16 years (Martin and Maury, 1964; Barnett et al.,1966).
LOCALIZATION OF THE PATHOGENIC PROCESS Atoperation our patient showed unilateral cysticformation at the site of the left lateral columns.The neurological evolution suggested an expandingand non-destructive process. In the left upper limba rapid involvement of thermal sensation was foundat first, followed more slowly by a less severeimpairment of tactile appreciation. After thelaminectomy recovery was in the reverse order.As for the motor effects, it was noted that at thebeginning paresis affected hand muscles more thanthose of the rest of the arm. Finally, there was an
almost complete absence of impairment of thegnostic sense. All of these elements suggest cavitationin the grey or white matter at the base of the leftposterior horn, near the rubrospinal tract and thelateral corticospinal tract. Only these two localiza-tions could explain the loss of sensation for tempera-ture and pain on the same side as the anatomicallesion observed at operation. The unilateral deficitspoke against a lesion in the region of the centralcanal. These two localizations could also explainthe repercussion of the compression on the fibresof the lateral corticospinal tract, the innermostfibres of which are related to the upper limbs, andon the motor cells of the anterior horns where cellscorresponding to the muscles of the hand occupythe most dorsolateral portion (Crosby, Humphrey,and Lauer,1962). The almost complete absence ofgnostic involvement could be explained by theanatomical localization of the lesion which exertedits compressive effects on the nearest tissues-thatis, the lateral pyramidal tract and/or the grey mattercells. The latter because of their looser consistencyare more sensitive than the white matter to anexpanding process.
CONCLUSIONS
Present knowledge does not permit definite con-clusions as to the precise pathogenesis of these latesyringomyelic syndromes. However, it permitssome hypotheses based on clinical facts and onoperative records and necropsies. At the initialstage, two main aetiological factors can be takeninto account, haematomyelia, which is infrequent, andmyelomalacia through local circulatory disorders.At the final stage, one or several intramedullarycavitations form, at first in the posterior columnsand horns. The common clinical result of this is asyringomyelic syndrome. However, in our case,one may imagine that an oedema of undeterminedcause-insidious and slow to progress-was theorigin of the imbalance of the interstitial tissuepressure and it is not necessary to involve a malacicprocess. The slowness of tissue necrobiosis on theone hand, and, on the other, the necessity of havinga cyst of sufficient volume to exert compression onthe adjacent structures can explain the late appear-ance of the new neurological symptoms. At thebeginning it is not a very destructive process.The considerable post-operative regression of theneurological deficit in our case and in the patientsof Freeman (1959) and Finkle (1960) proves this.Left to itself, the evolution of symptoms can reach aplateau or even show spontaneous regression.Sometimes, however, it can be dramatic and leadto tetraparesis (cf. case no. 2 of Barnett et al., 1966).
104

Study of late cervical syringomyelic syndromes after dorsal or lumbar traumatic paraplegia
We therefore think that such a syndrome requiressurgical intervention when the myelography revealswidening of the spinal cord. This statement seemsto be justified by the success of surgery in ourpatient and in the cases of Freeman (1959) andFinkle (1960). The 12-month post-operative follow-up of our patient does not yet allow us to concludethat definite improvement has taken place but ithas to be remembered that each of the imposedcases of Freeman (1959) and Finkle (1960) had afollow-up of two years' duration.As the syringomyelic syndrome often manifests
itself initially in the upper limbs, the suddenappearance of unexplained pain suggesting a lesionat the thoracic or cervical level should indicaterepetition of the neurological examination in thecourse of the following weeks or months.
SUMMARY
On the basis of the detailed pre- and post-operativeclinical evolution of one of their patients, theauthors discuss within the framework of the casespublished up to the present time, the symptoma-tology, pathogenesis, prognosis, and therapy of latecervical syringomyelic syndromes, the anatomicallesion of which appears to be situated at a distancefrom the initial dorsal or lumbar traumatic cordlesion. An hypothesis on the anatomical localizationof the pathological cavitation is advanced.
We would like to express our thanks to Mr. C. Ryser,medical artist to the Faculty of Medicine of the Universityof Geneva, for having so kindly undertaken to preparethe figures and graphs for this work.
REFERENCES
Barnett, H. J. M., Botterell, E. H., Jousse, A. T., and Wynn-Jones, M.(1966). Progressive myelopathy as a sequel to traumaticparaplegia. Brain, 89,159-174.
Bischof, W., and Nittner, K. (1965). Zur Klinik und Pathogenese dervaskular bedingten Myelomalazien. Neurochirurgia, 8,215-231.
Cossa, P. (1943). Syringomyelie secondaire a une blessure de la moelledorsale superieure. Rev. Neurol., 75, 39-40.
Crosby, E. C., Humphrey, T., and Lauer, E. W. (1962). CorrelativeAnatomy of the Nervous System. MacMillan, New York.
Finkle, J. R. (1960). Lesions ascending from spinal cord injuries. InProc. ninth Ann. Clin. Spinal Cord Injury Confr., pp. 45-48.Veterans Administration Hospital, Long Beach, California.
Freeman, L. W. (1959). Ascending spinal paralysis. Case presentation.J. Neurosurg., 16, 120-122.
Holmes, G. (1915). The Goulstonian lectures on spinal injuries of
warfare. I. The pathology of acute spinal injuxies. Brit. med. J.,2, 769-774.
Jellinger, K. (1966). Zur Orthologie und Pathologie der Ruckenmarks-durchblutung. Springer, Vienna.
Jung, E. (1960). Syringomyelie in Kombination mit Entwicklungs-storung der Nieren und mit schwerer Wirbelsaulenverletzung.Med. Klinik.,55. 1678-1679.
Marburg, 0. (1936). Die traumatischen Erkrankungen des Gehirnsund Ruckenmarks. In Handbuch der Neurologie, edited by0. Bumke and 0. Foerster. Vol. 11; Spezielle Neurologie.III. Erkrankung des Ruckenmarks und Gehirns. I. Traumatischeprdsenile und senile Erkrankungen Zirkulationsstorungen.Springer, Berlin.
Martin, C., and Maury, M. (1964). Syndrome syringomy6lique aprisparaplegie traumatique. A propos de six cas de syndromesyringomyelique cervical survenant dans des paraplegiesdorsale ou lombaire. Presse mid., 72, 2839-2842.
Mcllroy, W. J. and Richardson, J. C. Quoted by Barnett et al. (1966).Minor, L. (1904). Traumatische Erkrankungen des Ruckenmarkes.
(Ruckenmarks-Zerquetschung, Hamatomyelie, Nekrose etc.).In Handbuch der pathologischen Anatomie des Nervensystems,Vol. 2, edited by E. Flatau, L. Jacobson, and L. Minor.pp. 1008-1058. Karger, Berlin.
Riffat, G., and Domenach, J. (1964). Syndrome syringomyeliquesuccedant ai un traumatisme medullaire ancien. Lyon Med.,212, 1043.
Schott, B., Trillet, M., Vauterin, C., and Koshbin. (1962). Syndromessyringomyeliques tardifs sus-lesionnels apres traumatismem6dullaire (a propos de trois observations cliniques). Rev.Neurol., 106, 751-755.
Wolman, L. (1965). The disturbance of circulation in traumaticparaplegia in acute and late stages: a pathological study.Paraplegia, 2, 213-226.
Zehnder, M. (1937). Die subduralen Hamatome. Zbl. Neurochir., 2,339-353.
Zulch, K. J. (1962). R6flexions sur la physiopathologie des troublesvasculaires m6dullaires. Rev. Neurol., 106, 632-645.
ADDENDUM
Since this article was submitted for publication,another similar case has come to our attention.The patient was born in 1912. There was a traumaticcomplete cord lesion D8 in June 1956 (fractures D8and D9). In March 1959 a syringomyelic syndromeappeared on the right side. The symptoms pro-gressed very slowly until the patient was first seenin our centre in March 1967 with an upper neuro-logical limit at C3. A neurological condition wasfound similar to that of our first case. Air myelogramshowed a considerable enlargement of the cordextending from C3 to D7. A laminectomy (9 August1967) from C7 to D3 with a median posterior cord in-cision showed a cystic cavity in communication withthe fourth ventricle. Protein content was 1160 mg/l.in the spinal fluid and 286 mg/l. in the hydromyeliccavity. Two months after the operation the patienthad made such a recovery that sensory and motorconditions were almost normal.
105