Embed Size (px)
Citation preview

This article was downloaded by: [Swinburne University of Technology]On: 03 September 2014, At: 02:32Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
ErgonomicsPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/terg20
Continuous assessment of work activities and posturein long-term care nursesJoanne N. Hodder a , Michael W.R. Holmes a & Peter J. Keir aa McMaster Occupational Biomechanics Laboratory, Department of Kinesiology , McMasterUniversity , Hamilton, ON L8S 4K1, CanadaPublished online: 24 Aug 2010.
To cite this article: Joanne N. Hodder , Michael W.R. Holmes & Peter J. Keir (2010) Continuous assessment of work activitiesand posture in long-term care nurses, Ergonomics, 53:9, 1097-1107, DOI: 10.1080/00140139.2010.502252
To link to this article: http://dx.doi.org/10.1080/00140139.2010.502252
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Continuous assessment of work activities and posture in long-term care nurses
Joanne N. Hodder, Michael W.R. Holmes and Peter J. Keir*
McMaster Occupational Biomechanics Laboratory, Department of Kinesiology, McMaster University,Hamilton, ON L8S 4K1, Canada
(Received 21 July 2009; final version received 20 May 2010)
The high prevalence of low back injuries in nursing has prompted the use of mechanical lift assists while overallassessment of activities and postures remains limited. The purpose of this study was to chronicle trunk posture andwork tasks of long-term healthcare professionals. An inclinometer monitored trunk posture for 27 workers, 20 ofwhom were also observed continuously throughout their shift. Patient lifts and transfers accounted for less than 4% ofthe shift while patient care, unloaded standing and walking and miscellaneous tasks accounted for 85%. Manual liftsand transfers occurred twice as often as mechanically assisted lifts but took only half the time. The workers had amedian trunk flexion angle of 9.28, spent 25% of their time flexed beyond 308 and had peak flexion angles greater than758 in many tasks. Analysis of posture throughout the entire working shift indicates that, in addition to lifts andtransfers, emphasis needs to be placed on patient care and miscellaneous activities when assessing injury risk for nurses.
Statement of Relevance: Patient handling has been the focus in the effort to reduce back pain and injury in nursing.In addition to the use of mechanical lifts, there is a need to examine other aspects of nursing, including patientcare and other ancillary tasks, which comprise the majority of the work shift and, while often unloaded, exhibitextreme postures that may also lead to injury.
Keywords: low back; nursing; patient handling; posture
1. Introduction
Over the past 30 years, low back disorders in thenursing profession have matched or exceeded those inheavy industry (Jensen 1987, Nelson and Baptiste2006). In 2001, the rate of lost time injuries was 7.3 per100 full-time equivalents in nursing home environ-ments, double that seen in construction (3.6/100) andmanufacturing (3.9/100) industries (United StatesBureau of Labor and Statistics 2001). Although theaetiology of low back disorders in nurses is multi-factorial, including physical, psychosocial and indivi-dual factors (Sherehiy et al. 2004), patient handling hasbeen identified as a major contributor, accounting for73–89% of all low back injuries in this sector (Jensen1987, Owen 1989). Physical risk factors specific topatient handling include the mass of the patient(Engkvist et al. 1998, Sherehiy et al. 2004), asymmetryof the load (Engkvist et al. 1998), lift rate/repetition(Engkvist et al. 1998, Yip 2004) and the postureassumed while supporting the patient (Engkvist et al.1998, Sherehiy et al. 2004, Yip 2004).
Interventions to reduce loads and injuries asso-ciated with patient handling have included back injuryeducation and awareness (Venning 1988, Hodder et al.2010), manual transfer technique training (Johnsson
et al. 2002, Hodder et al. 2010), lift teams (Charneyet al. 1991), transfer belts and mechanical floor lifts(Owen and Garg 1991, Zhuang et al. 1999, Evanoffet al. 2003, Li et al. 2004) and ceiling lifts (Zhuanget al. 1999, Keir and MacDonell 2004, Li et al. 2004).Mechanical lifts and lift assists have been found to besuccessful in reducing injuries in both long-term andacute care facilities (Evanoff et al. 2003). Yassi et al.(2001) reported a reduction from 8.2 to 6.1 injuries per100,000 working hours in the first year of sit-to-standand floor lift implementation while Li et al. (2004)found an even greater reduction in musculoskeletalinjury rates from 10.3 to 3.8 injuries per 100 full-timeemployees after implementation of the same lifts in asingle facility. A similar injury rate reduction wasfound by eliminating lifting via floor lift assists from15.4 to 9.3 injuries per 200,000 employee hours(Fujishiro et al. 2005). Zhuang et al. (1999) reportedlumbar compression forces of 2698 to 2951 N usingceiling lifts, which is vastly lower than forces found formanual transfers using a basket sling, which exceededthe National Institute for Occupational Safety andHealth action limit of 3400 N (Waters et al. 1993).After training, ceiling lifts have been reported to be thepreferred method for lifting patients (Engst et al. 2005,
*Corresponding author. Email: [email protected]
Ergonomics
Vol. 53, No. 9, September 2010, 1097–1107
ISSN 0014-0139 print/ISSN 1366-5847 online
� 2010 Taylor & Francis
DOI: 10.1080/00140139.2010.502252
http://www.informaworld.com
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

Santaguida et al. 2005) but not for adjustments in bed(Engst et al. 2005). Mechanical lift use is stronglyassociated with reduced injury rates due to lower forcesacting on (and within) the body as well as improvedbody postures when using these devices. Despite thesebenefits, some barriers still exist with mechanical liftuse. Li et al. (2004) noted that compliance formechanical lift usage gradually decreased over a6-month trial period. Resistance to using mechanicallifts has been reported for a variety of reasons,including taking too much time, feeling that patientswere not comfortable with the lifts, lacking experiencein usage or a lack of device availability at the time ofneed (Owen and Garg 1991, Owen 2000). Mechanicaldevices have been found to take up to 17 times longerthan traditional manual transfer techniques (Owen andGarg 1991). Not including sling placement, ceiling lifttransfers have been reported to take 3.5 to 5.3 timeslonger than manual transfers for experienced andnovice handlers, respectively, while floor lift transferstook 4.0 to 8.3 times longer depending on experience(Keir and MacDonell 2004).
While the majority of research has examined liftingand transferring techniques, patient handling may notbe the only contributor to low back loading and risk ofinjury for nurses. A recent evaluation of humanresources data suggested that, while the 40% ofinjuries that were due to lifting/transferring patientsand may be prevented with mechanical lift assist use,60% of injuries were due to other tasks, such asrepositioning or turning patients or pulling patients upin bed (Pompeii et al. 2009). Nurses spend approxi-mately 60% of their day performing housekeeping,administrative and patient care activities outside ofthose considered patient handling (Engels et al. 1994b).According to Fuortes et al. (1994), nursing aides arethree times more likely to incur a back injury incomparison to registered nurses as they were found tohave greater lift frequencies and more time spent onpatient care activities. The nature and duration ofduties performed is also dependent on the type offacility. For example, long-term care units have higherlift frequency and injury rates than nurses in acutecare, surgical or other hospital wards (Evanoff et al.2003). Jang et al. (2007) monitored nurses in generalinpatient and heart and lung post operative wards andfound that patient care tasks, such as bathing anddressing patients, had the greatest peak flexion anglesin the 1.5 h period tested. Evaluation of tasks over afull shift have been limited to recall logs completed atthe end of the work day for extended home care nurses(Knibbe and Friele 1999).
Although many efforts have been made toanalyse low back loading in nurses, the focus hasbeen predominantly on patient handling tasks
(Winkelmolen et al. 1994, Keir and MacDonell2004, Jang et al. 2007, Skotte and Fallentin 2008).These efforts have either used limited durationobservations in the workplace (Jang et al. 2007) orhave been laboratory-based studies that focusedsolely on patient handling techniques (Winkelmolenet al. 1994, Keir and MacDonell 2004, Skotte andFallentin 2008). Although these studies are able toprovide mean and peak loading during variouspatient handling tasks, they are not able to accuratelydescribe how nurses are being continuously loadedover an entire shift. Continuous assessment ofposture and tasks is a required input for cumulativeloading, which estimates how forces on the bodyaccumulate with repeated load exposure over a fixedperiod of time or, in many cases, over an entire shift(Waters et al. 2006a,b). A combination ofinclinometry and observation has been shown toprovide complementary data for continuousassessment of workers in industry (Trask et al. 2007,Teschke et al. 2009).
There is a need for comprehensive posture data fornurses, nurse aides and/or personal support workers(PSW in Ontario, Canada) while they perform the fullcomplement of tasks required during an entire shift.The purpose of this study was to observe anddocument all PSW activities, including patienthandling tasks and lifting tasks, while continuouslymonitoring trunk posture throughout an entire shift.This study, and its companion study (Holmes et al.2010) evaluating peak and cumulative spine loads, waspart of a large scale examination of the effects of aninitiative to fund the influx of a large number of ceilinglifts in long-term care facilities in Ontario.
2. Methods
2.1. Participants
A total of 27 female PSWs (162.0 + 6.8 cm;69.0 + 11.9 kg; 46.7 + 8.6 years) with 19.5 + 9.3years of experience had their trunk kinematicsmonitored during one work shift. Twenty of thePSWs (161.4 + 7.2 cm, 70.7 + 11.8 kg, 47.2 + 9.4years) were also observed throughout their shift (seesection 2.4 for further details of the observationmethods) and averaged 13.3 + 8.6 years ofexperience. PSWs volunteered from seven long-termcare facilities in Southern Ontario, Canada. The long-term care facilities were varied in size and equipment(Table 1). This study was approved by the HumanResearch Ethics boards at McMaster University, theUniversity of Toronto, and the Institute for Workand Health, Toronto, Ontario. All participantsprovided written informed consent prior to datacollection.
1098 J.N. Hodder et al.
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

2.2. Experimental protocol
Data were collected over an 8-h work shift for eachnurse, which started at either 06.00 or 07.00 hours,depending on the facility. At the beginning of the shift,each PSW had a pager-sized inclinometer/dataloggeraffixed to their sternum via a custom-made harness forcontinuous posture monitoring. In addition to theinclinometer, 20 of the 27 nurses were also observedfor the duration of the shift and all tasks performedwere recorded. Thus, data for the seven nurses whowere not observed are limited to inclinometer (posture)data. The inclinometer device and observational soft-ware were launched simultaneously to synchronise thepostures and observations in time.
2.3. Posture
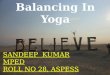
Trunk posture was collected using an inclinometer/datalogger system (Virtual Corset, Microstrain Inc.,Williston, VT, USA) affixed to a harness over thesternum (Figure 1). The inertial inclinometer devicecollected flexion–extension and left–right lateral bendangles of the trunk and sampled at a rate of 7.6 Hz.Prior to placement, the inclinometer was calibratedaccording to manufacturer instructions. The devicewas placed approximately 2.5 cm below the clavicles inthe middle of the sternum. This placement minimisedinterference with the device and nursing activities.After placement, the participant stood upright for 5 s,flexed forward, extended backward, performed left andright bends and returned to an upright standingposture for another 5 s. The average of the twoupright standing postures defined the neutral posturefor that participant. This neutral posture was used aszero for flexion–extension and lateral bend.
2.4. Observations
Three observers were used in this study; all weretrained to use the observational software and hadprevious experience in patient handling. Events were
recorded using a pocket PC (HP iPAQ, HX 2400;Hewlett-Packard Company, Palo Alto, CA, USA) withobservational software (Observer XT, Noldus, VA,USA). The software allowed events to be pre-programmed on to the hand-held device. Theseevents were displayed as a block on the screen of thepocket PC so the observer could tap the screen with astylus to indicate what task was being performed. Twotypes of events, ‘point’ and ‘state’, were programmed.Point events acted as simple time-stamped labels whilestate events indicated the start time of an event thatinitiated a timer, which ended at the screen tap of anew event or the ‘end’ button. Point events weregenerally used to provide context to the upcomingstate events. Thus, point events indicated the type oflift (or lift assist) and included ‘ceiling’, ‘floor’, ‘sit-to-stand’ and ‘manual’ lifts (one and two persontransfers) while state events indicated what specific
Table 1. Facility demographics including size, equipment and personnel information.
FacilityNo. of
approved bedsNo. of residentsin past month
PSWs inpast month
Floor lifts in workingorder (during study)
Ceiling lifts in workingorder (during study)
1 93 93 62 4 212 120 120 118 4 03 60 60 47 2 174 77 77 52 4 05 350 350 316 14 466 60 60 58 9 77 45 45 45 5 1
PSW ¼ personal support worker.
Figure 1. Positioning of the inclinometer in the harnesson the sternum.
Ergonomics 1099
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

task was occurring. For example, when observing aceiling lift transfer to the bed, the observer would tap‘ceiling’ (point event), which would create a label forthe device being used and then ‘to bed’ (state event) toindicate the nature of the transfer and initiate timing ofthe event. The state event of lifting would then beended with tapping ‘end’ or with tapping another stateevent such as ‘walking’. Comments could also beentered, such as the estimated weight of the patient orother notes as deemed necessary. The preset stateevents are grouped in Table 2.
2.5. Data analysis
The number of occurrences and total duration foreach task were calculated for each of the 20 observedPSWs. Continuous sagittal (flexion–extension) andlateral (right–left bend) trunk angles were analysedusing the amplitude probability distribution function(APDF; Jonsson 1978), which represents cumulativeproportion. This analysis was performed for each taskfor the 20 observed PSWs and the entire shift for thefull participant pool (n ¼ 27). The 1st, 10th, 50th(median), 90th and 99th percentiles were determinedfrom the APDF for angle, angular velocity andangular acceleration (velocity and acceleration werecalculated using the finite difference technique). The1st and 99th percentile values represented the peaksfor each measure to exclude extraneous spikes, whichmay occur through contact with the inclinometer. Dueto the bidirectional nature of the angles, the 1stpercentile represented peak extension and left lateralbend while the 99th percentile represented peakflexion and right lateral bend. For the whole shiftdata, independent t-tests were used to compareobserved vs. unobserved PSWs, 06.00 hours vs.07.00 hours shift start times and between each hourof the shift for all measures.
3. Results
The length of data collection for the 20 PSWs rangedfrom 4 h and 22 min to 8 h and 8 min. For theunobserved PSWs, the length of data collection rangedfrom 7 h and 2 min to 8 h and 9 min.
3.1. Event frequency
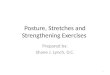
A total of 4694 task events were observed from 20workers, representing a mean of 235 + 17 events pershift. The most frequent task was pushing a patient in awheelchair, with a total of 564 events. There were 761patient care activities, which included bathing, dressingand feeding the patient. A total of 513 miscellaneoustasks were performed. These tasks included makingbeds, sitting, work breaks and other tasks such asengaging the brakes on a wheelchair. The total numberof manual lifts (253) almost doubled the total numberof mechanically assisted lifts (140) as seen in Figures 2and 3. More tasks were performed early in the shift,especially manual transfers and lifts (Figure 3). Thenumber of manual transfers decreased slightlythroughout the day from 47 to 32 while the number ofnurses observed decreased from 20 to 6. The number ofmechanical lifts and transfers appears to increase inhour 7 (Figure 3).
3.2. Event duration
For the 20 observed PSWs, the total time spentperforming each task (expressed in percent duration) isfound in Figure 2. Standing, which included walkingand other unloaded movements, comprised37.6 + 16.7% of the shift. Patient care activities were26.1 + 6.8% and miscellaneous activities represented21.1 + 5.7% of the shift duration. Performing manuallifts accounted for 1.4 + 0.5% of the total shiftduration, while mechanical lifts accounted for only2.5% of shift duration (Figure 2).
3.3. Trunk kinematics
The median posture (SD) for all 27 PSWs over anentire shift was 9.2 + 6.08 flexion and 1.4 + 3.98 rightbend (Figure 4). The range of motion (ROM), definedas the difference between the 1st and 99th percentiles,was 106.2 + 25.88 in the sagittal plane, with anaverage peak flexion of 82.3 + 20.38 and average peakextension of 22.2 + 12.08 (Figure 4). The lateral ROMwas 60.6 + 9.08 (26.5 + 5.88 left bend to 34.3 + 8.08right bend; Figure 4).
Table 2. State (timed) events documented in study grouped by common features.
Transfers Patient care Move patient Patient adjustment Standing/Walking Miscellaneous activities
To bed Bathing Push patient Sling under Standing Make bedTo chair Dressing Walk patient Remove sling Push lift SittingTo toilet Feeding Sit at edge Push cart Break
Up in bed Other
1100 J.N. Hodder et al.
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

While the observed PSWs had slightly lowermedian trunk angles (8.1 + 5.48 flexion, 0.6 + 3.88right lateral bend) than the unobserved nurses(12.6 + 6.68 flexion, 3.7 + 3.38 right bend), therewere no statistical differences in the trunk posturesbetween the observed and unobserved nurses. The firsthour of the shift had significantly greater median trunkflexion than all other hours of the shift (p ¼ 0.03). Inthe first hour, workers had a median trunk flexionangle of 16.6 + 8.38, while the other hours rangedfrom 12.1 + 1.58 to 5.7 + 0.38 (Figure 5). There wasno significance difference in this measure between theworkers starting at 06.00 hours (n ¼ 11, range: 6.9–19.18) vs. those starting at 07.00 hours (n ¼ 16, 4.9–15.28).
With regard to specific tasks, the one-personmanual transfer had the greatest peak flexion with anangle of 84.1 + 15.48, while the two-person manualtransfer only elicited 67.7 + 32.18 of trunk flexion(Table 3). Mechanical devices had similar motions tothe manual transfers, with the ceiling, floor and sit-to-stand lifts exhibiting 74.6 + 33.08, 73.2 + 35.18 and58.6 + 30.38 of forward flexion, respectively. The
patient care activities of dressing and bathing alsohad large peak forward flexion angles of 78.3 + 29.58and 83.6 + 24.98 (Table 3).
In terms of lateral bend, one- and two-personmanual lifts were frequently performed with mediandisplacements to the right of 5.0 + 7.58 and5.1 + 6.98, respectively. Overall, activities classified aspatient care had the largest peak lateral bending,exceeding 308 to the right (R) and 248 to the left(L)(Table 3). In particular, bathing the patient elicitedlateral bend from 35.08 (R) to 27.98 + 8.78 (L), patientdressing was 30.78 (R) to 24.78 (L), while feedingrequired 30.18 (R) to 26.58 (L) (Table 3).
The peak angular velocities (99th percentile) for theentire shift were 70.3 + 14.5 8/s for flexion and66.3 + 13.5 8/s for extension, while peak left and rightbend were virtually identical at 73.8 + 15.9 8/s and73.9 + 15.2 8/s, respectively. Angular trunk velocitieswere highest in the ‘miscellaneous’ category. Inparticular, making the bed elicited maximum trunkflexion velocity of 127.9 + 65.28/s and maximumextension velocity of 117.0 + 36.2 8/s. The highestmaximum lateral bend velocities were also seen making
Figure 2. Mean task frequency (light bars) and cumulative task duration as a percentage of shift duration (black bars)with standard deviation. Note that the standard deviation for ‘standing/walking’ frequency is 43.2 (n ¼ 20). STS ¼ sit to stand.
Ergonomics 1101
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

beds, with 118.6 + 37.7 8/s to the right and112.7 + 26.5 8/s to the left.
4. Discussion
The current approach of combining continuousobservation and trunk posture collection allowed aunique and detailed examination of job content andposture of PSWs in long-term care facilities. PSWsspent 50% of the day with the trunk flexed beyond9.28, with 25% of their time flexed beyond 308.Continuous observation of a subset of 20 PSWsallowed posture to be linked to specific tasks inaddition to determining the number and duration oftasks, providing new insights beyond previous use ofwork logs and short duration observations (Knibbeand Friele 1999, Jang et al. 2007). In the presentsample, manual lifts (and transfers) were performedalmost twice as often as all mechanically assisted liftscombined (ceiling, floor and sit to stand) yet requiredhalf the time. While the impetus for this study was toexamine mechanical lifts, especially ceiling lifts, thedetailed description of tasks and postures assumedthroughout a typical workday provide new insights tothe activities and their associated postures in long-termcare facilities.
Lifts and transfers, whether mechanically assistedor not, accounted for a small proportion of all tasks(59%) and required an even smaller percentage oftime (54%). Patient-based activities, includingadjusting patients in bed, care activities (bathing anddressing) and transporting the patient in a wheelchairoccurred 4.8 times as often as transfers (94 vs. 19 timesper shift) and used 10-fold the time (39.3% overall;Figure 2). The impact of this finding is seen whencombined with the high lumbar spine compression andshear loads known to occur with patient adjustmentand handling (Gagnon et al. 1987). Similar to Engelset al. (1994b), the PSWs in this study spent about 60%of the shift performing activities other than patienthandling, including standing, patient care and othermiscellaneous duties (Figure 2). The standing categoryincluded walking, pushing empty floor lifts and linencarts, gathering housekeeping supplies and othergeneric unloaded movements comprised almost 38%of the shift duration. The PSWs in the current studyspent 21.1% of the shift on miscellaneous tasks such asmaking beds, gathering patient care supplies andengaging wheelchair brakes. In nursing homes in theNetherlands, Engels et al. (1994b) found slightly moretime was spent on similar tasks (33.4%). This categorywas highly variable in both time and frequency, which
Figure 3. Frequency of lifts and transfers by hour and type for observed participants. The number of nurses observed in eachhour is indicated for each hour. STS ¼ sit to stand.
1102 J.N. Hodder et al.
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

Figure 4. Distribution of sagittal and lateral angular displacement for the entire shift. Mean amplitude probabilitydistribution function for flexion–extension (Flex-ext) and lateral bend (Lat bend) were reconstructed based on percentilesindicated by data points from each subject (1st, 5th, 10th, 50th, 90th, 95th, 99th). Flexion and right bend are positive, error barsrepresent standard deviation for each percentile (n ¼ 27).
Figure 5. Distribution of flexion–extension angles for each hour of the shift. Mean amplitude probability distributionfunction was reconstructed based on percentiles indicated by data points from each subject (1st, 5th, 10th, 50th, 90th, 95th, 99th).Flexion is positive, (n ¼ 27). The first hour of work has increased trunk flexion.
Ergonomics 1103
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

suggests differences between facilities in terms ofduties, level of patient disability and perhaps subtledifferences in how the observers recorded events in thiscategory (Figure 4). These accessory tasks have beenassociated with up to 60% of the injuries in hospitalworkers (Pompeii et al. 2009).
The posture recording system provided uniqueinsight into the postures associated with each task bydetermining median and peak trunk angles for eachtask. Peak angles are insightful with regard to risk ofacute injury and are especially useful when loading isconsidered (Holmes et al. 2010). It has also beensuggested that posture may be a better predictor ofspinal forces than loads acting at the hands(Hoozemans et al. 2008). In terms of angular deviationand high loads, the single-person manual lift had oneof the highest peak flexion angles (84.1 + 15.48) andwas never within 108 of neutral; additionally, rightbend exceeded 318. Ceiling and floor lifts had lowerpeak flexion angles (just under 758; Table 3) but,interestingly, ceiling lift use had one of the highest (andmost variable) peak right bend angles (30.8 + 19.98).It should be noted that the larger lateral bend with theceiling lift should be considered as ‘unloaded’ with
regard to patient weight. Perhaps the most curiousfinding was that the largest deviations from verticalwere found during break times and exceeded 908 offlexion, approached 308 of extension and also had 358of bend to each side. Although these activities couldinclude stretches and other unloaded actions, thesepostures suggest that further attention may bewarranted for actions during breaks and othermiscellaneous activities.
Patient care activities, especially bathing anddressing patients, required large flexion angles (over788) and large lateral deviations, especially to the right,which exceeded 308. Poor postures in these tasks havebeen shown in many studies (Engels et al. 1994a,Zhuang et al. 1999, Jang et al. 2007). Jang et al. (2007)monitored nurses and nursing aides using the lumbarmotion monitor over a 1.5 h collection period andfound peak flexion and lateral bend angles of 98.08 and43.18 (respectively) for bathing patients, both slightlylarger than the current study (83.68 flexion and 35.08lateral bend). Compared to the current study, Janget al. (2007) found 118 greater flexion and 48 greaterlateral bend than the values for making beds in thecurrent study (95.28 vs. 83.98 and 36.98 vs. 32.58).
Table 3. Peak angular displacements and standard deviations.
Peak displacement (8)
Flexion Extension Right bend Left bend
1 Person manual 84.1 + 15.4 10.4 + 14.0 31.4 + 11.1 720.7 + 11.02 Person manual 67.7 + 32.1 5.6 + 8.4 27.0 + 16.5 720.9 + 7.3Ceiling lift 74.6 + 33.0 74.6 + 3.3 30.8 + 19.9 723.9 + 7.5Floor lift 73.2 + 35.1 9.1 + 8.6 23.7 + 16.4 721.1 + 7.5STS lift 58.6 + 30.3 6.9 + 4.7 26.1 + 16.0 716.0 + 2.8Patient care 77.2 + 30.7 0 + 5.9 31.9 + 15.3 726.4 + 8.5Bathe patient 83.6 + 24.9 70.4 + 6.6 35.0 + 13.8 727.9 + 8.7Dress patient 78.3 + 29.5 0.9 + 8.7 30.7 + 13.7 724.7 + 9.7Feed patient 69.6 + 37.8 70.4 + 2.2 30.1 + 18.3 726.5 + 6.9
Patient adjustment 66.0 + 28.4 4.8 + 9.4 26.0 + 12.1 717.9 + 8.1Sling under 65.7 + 26.9 3.6 + 6.4 27.5 + 11.7 715.7 + 8.2Remove sling 64.7 + 32.2 5.7 + 10.7 24.1 + 15.7 720.6 + 5.6Sit in bed 67.7 + 26.0 6.2 + 11.1 24.8 + 8.7 719.5 + 10.5Up in bed 68.8 + 27.3 71.2 + 4.1 25.1 + 15.9 721.1 + 2.0
Move patient 60.7 + 29.6 2.9 + 9.2 26.1 + 15.2 719.2 + 10.4Push patient 64.5 + 30.4 3.2 + 7.8 26.5 + 14.6 721.2 + 9.6Move patient 57.9 + 28.9 3.1 + 13.1 25.8 + 17.3 718.7 + 13.6Walk patient 59.8 + 29.6 2.3 + 6.6 25.8 + 13.8 717.9 + 8.1
Miscellaneous 77.6 + 26.9 77.4 + 9.6 29.2 + 14.5 727.0 + 6.6Make Bed 83.9 + 32.3 0.4 + 5.1 32.5 + 14.1 728.2 + 1.8Other 70.7 + 28.2 2.5 + 7.6 24.2 + 16.2 722.3 + 8.7Sitting 64.1 + 24.5 75.3 + 11.0 24.0 + 16.6 723.0 + 10.5Break 91.6 + 22.4 727.2 + 14.8 36.3 + 11 l 734.3 + 5.4
Standing/Walking 65.0 + 28.7 3.6 + 8.7 25.1 + 13.3 720.5 + 9.6Push linen cart 61.4 + 30.0 4.5 + 6.7 23.7 + 13.8 718.8 + 8.5Push empty lift 60.8 + 27.0 5.6 + 9.3 22.7 + 11.1 718.5 + 10.3Standing 72.7 + 29.2 0.6 + 10.1 29.1 + 14.8 724.2 + 12.6
STS ¼ sit to stand.
Note: Italicised and indented numbers represent subcomponents of each category. Positive values represent trunk flexion and right bend whilenegative numbers represent extension and left bend (n ¼ 20).
1104 J.N. Hodder et al.
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

Zhuang et al. (1999) measured posture from video andfound mean angles similar to the median angles of thecurrent study. The slight differences between studiesare likely a combination of the measurement devicesand specifics of the activities.
Manual lifts and transfers were used proportio-nately more often in the first 2 h of the shift (Figure 2),while in the first hour of the shift, the median trunkflexion angle was also greatest. The start of themorning shift, especially the 06.00 hours shift, isassociated with helping patients out of bed and feedingthem in a short time period; thus, larger trunk flexionwas likely in conjunction with higher loads. Thecombination of increased flexion and performingmanual lifts and transfers in the morning may be aconcern, given that the lumbar spine is stiffestimmediately after rising in the morning (Adams et al.1987). Thus, perhaps inadvertently, workers appear tobe increasing the risk of low back injury. However, itappears that assistive devices were used more often atthe end of the shift as the total number of mechanicallyassisted lifts remained relatively constant in spite of areduced number of nurses observed (Figure 3). Thismay have been due to perceived need of assistance orthere being more time to use the devices.
All facilities in this study had no lift policies and allfacilities had mechanical lifts of some variety available(Table 1). While not evaluated in the current study, thedistribution of the assists within each facility may haveplayed a role in their use as manual lifts (and transfers)occurred almost twice as often as all mechanicallyassisted lifts combined (ceiling, floor and sit to stand).Manual lifts and transfers, although greater in number,required half the time of assisted lifts. This supportsanecdotal comments about the lift assists taking ‘toomuch time’ or there not being enough lifts available,leading nurses to choose to manually transfer patientsin spite of recognising the potential consequences(Owen 2000). In the current study, ceiling lift use wasoften limited to bed and chair transfers due to retro-fitinstallations that did not include access to the toilet orbath (although this information was not specificallycollected). While ceiling lift use was sometimes limitedby installation constraints, their use was associatedwith the least amount of overall flexion (median angleof 23.78 + 10.08) of all lifts observed, which wassubstantially less than the one-person manual lift(41.28 + 9.78) and floor lifts (34.78 + 12.18). Whiletwo person manual transfers had lower flexion(27.38 + 17.38) than floor lifts, the spine loads wouldbe greater, given that the handler must support aproportion of the patient’s weight, thus increasing therisk of injury. The current results support the use ofmechanical lifts for improving trunk posture andreducing risk of injury.
While peak velocities in specific tasks were higherover the entire shift, the current study found peakvelocities (99th percentile) for flexion and lateral bendto be 70.38/s and 73.98/s, respectively. Marras et al.(1993) suggested that lumbar spine angular velocityand acceleration were important risk factors for lowback injury. The peak velocities from the current study(above) exceeded the values of 558/s (sagittal plane)and 468/s (lateral plane) previously reported for high-risk workers (Marras et al. 1993). The highest sagittalvelocities were found in the miscellaneous tasks, whichmay or may not be associated with spinal loading;thus, may require further assessment. Additionalcomments recorded noted that the large displacementsand velocities documented under miscellaneous tasksoccurred when the care giver was leaning forward toengage or disengage the brakes on the wheelchair.
Cumulative load exposure has been associated withrisk of back injury development (Waters et al.2006a,b). Previous limitations to this type ofassessment have been the methods in which posturedata were collected and/or extrapolated for an entireshift. However, the size, capacity and unobtrusivenessof the inclinometer used in the current study make it auseful measurement tool for long collection periods. Incombination with documentation of when the patienthandler is unloaded or loaded along with estimates ofmass, the methods used in the current study lend wellto cumulative load assessment. An assessment of thecumulative load exposure to the PSWs is presented inanother separate communication (Holmes et al.submitted).
There are a few limitations to the current study.First, the inclinometer is gravity based and wasmounted on the trunk; thus, flexion, extension andlateral bend are measured with regard to vertical andtrunk twist could not be recorded. However, previousexamination of inclinometry found it to be reliable anddetailed when compared to other methods ofmeasuring postures in lengthy assessments, especiallywhen complemented with observations (Trask et al.2007, Teschke et al. 2009). Some may be concernedabout errors in the differentiated velocities andaccelerations from the inclinometer data; however,these data were sampled at 7.6 Hz, well above thesampling rate of 3–5 Hz found to provide a goodrepresentation of posture from 60 Hz video data(Callaghan et al. 2001). Many factors affected thelength of data recording for each worker; thus, recordswere of different durations. Recording was stopped atthe time in the shift when the PSW began documentingpatient status. Thus, if a smaller patient load or moreable bodied/cooperative patients was seen, more timewas left for documentation and a shorter recordingtime resulted. Although the multi-factorial nature of
Ergonomics 1105
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

occupationally related low back injury has manypsychosocial and individual factors (Sherehiy et al.2004, Yip 2004), this paper focused on kinematicmeasurements. This approach is supported by thereview of physical and psychosocial risk factors bySherehiy et al. (2004), who found that working postureitself was significantly associated with the developmentof musculoskeletal disorders in nurses. Finally, thisstudy demonstrates the importance of consideringworkplace factors beyond the known need formechanical assistive devices, such as ceiling lifts, andis not intended to lessen the importance of their use.
5. Conclusions
The long-term care workers in this study spent nearly50% of the day with trunk flexion beyond 108 and 25%of their time flexed beyond 308. In addition, peakflexion angles exceeded 758 in many tasks. Whilepatient handling is associated with injury risk, patientlifts and transfers accounted for only 5% of the shift.While manual lifts and transfers were used nearly twiceas often as all mechanically assisted lifts (ceiling, floorand sit to stand), they required only half the time. Thelarge majority of the shift was spent performingactivities such as patient care, standing/walking tasksand other miscellaneous tasks. While there is a greatneed to assist patient handlers to reduce the stresses ofpatient lifts and transfers, these findings indicate thatother tasks that comprise the majority of the workperformed should not be overlooked for their involve-ment in risk of injury.
Acknowledgements
This study was supported by the Ontario Ministry of Healthand Long Term Care, as well as the National Sciences andEngineering Research Council of Canada (Discovery grant#217382–04). Special thanks to Dr P.W. Johnson for initialassistance with the Virtual Corset.
References
Adams, M.A., Dolan, P., and Hutton, W.C., 1987. Diurnalvariations in the stresses on the lumbar spine. Spine, 12(2), 130–137.
Bureau of Labor Statistics, 2001. Survey of occupationalinjuries and illnesses, 2001. Washington, DC: USDepartment of Labor.
Callaghan, J.P., Salewytsch, A.J., and Andrews, D.M., 2001.An evaluation of predictive methods for estimatingcumulative spinal loading. Ergonomics, 44, 825–837.
Charney, W., Zimmerman, K., and Walara, E., 1991. Thelifting team: A design method to reduce lost time backinjury in nursing. American Association of OccupationalHealth Nurse Journal, 39 (5), 231–234.
Engels, J.A., Landeweerd, J.A., and Kant, Y., 1994a. AnOWAS-based analysis of nurses’ working postures.Ergonomics, 37 (5), 909–919.
Engels, J.A., et al., 1994b. Physical work load and itsassessment among nursing staff in nursing homes.Journal of Occupational Medicine, 36 (3), 338–345.
Engst, C., et al., 2005. Effectiveness of overhead liftingdevices in reducing the risk of injury to care staff inextended care facilities. Ergonomics, 48 (2), 187–199.
Engkvist, I.-L., et al., 1998. The accident process precedingoverexertion back injuries in nursing personnel.Scandinavian Journal of Work, Environment & Health, 24(5), 367–375.
Evanoff, B., et al., 2003. Reduction in injury rates in nursingpersonnel through introduction of mechanical lifts in theworkplace. American Journal of Industrial Medicine, 44(5), 451–457.
Fuortes, L.J., et al., 1994. Epidemiology of back injury inuniversity hospital nurses from a review of workers’compensation records and a case-control study. Journalof Occupational Medicine, 36 (9), 1022–1026.
Fujishiro, K., et al., 2005. The effect of ergonomicinterventions in healthcare facilities on musculoskeletaldisorders. American Journal of Industrial Medicine, 48,338–346.
Gagnon, M., et al., 1987. Lumbo-sacral loads and selectedmuscle activity while turning patients in bed. Ergonomics,30, 1013–1032.
Hodder, J.N., et al., 2010. Effects of training and experienceon biomechanics of patient transfers. InternationalJournal of Industrial Ergonomics, 40 (3), 282–288.
Holmes, M.W., Hodder, J.N., and Keir, P.J., 2010.Continuous assessment of low back loads in long termcare nurses. Ergonomics 53 (9), 1108–1116.
Hoozemans, J.M., et al., 2008. Effect of lifting weight and loadmass on low back loading. Ergonomics, 51 (7), 1053–1063.
Jang, R., et al., 2007. Biomechanical evaluation of nursingtasks in a hospital setting. Ergonomics, 50 (11), 1835–1855.
Jensen, R.C., 1987. Disabling back injuries among nursingpersonnel: research needs and justification. Research inNursing and Health, 10, 29–38.
Johnsson, C., Carlsson, R., and Lagerstrom, M., 2002.Evaluation of training in patient handling and movingskills among hospital and home care personnel.Ergonomics, 45 (12), 850–865.
Jonsson, B., 1978. Kinesiology. With special reference toelectromyographic kinesiology. Contemporary ClinicalNeurophysiology (EEG Suppl. no. 34), 417–428.
Keir, P.J. and MacDonell, C., 2004. Muscle activity duringpatient transfers: a preliminary study on the influence oflift assists and experience. Ergonomics, 47 (3), 296–306.
Knibbe, J.J. and Friele, R.D., 1999. The use of logs to assessexposure to manual handling of patients, illustrated in anintervention study in home care nursing. InternationalJournal of Industrial Ergonomics, 24 (4), 445–454.
Li, J., Wolf, L., and Evanoff, B., 2004. Use of mechanicalpatient lifts decreased musculoskeletal symptoms andinjuries among health care workers. Injury Prevention, 10,212–216.
Marras, W.S., et al., 1993. The role of dynamic three-dimensional trunk motion in occupationally-related lowback disorders: The effects of workplace factors, trunkposition and trunk motion characteristics on risk injury.Spine, 18 (5), 617–628.
Nelson, A., 2006. Patient handling in health care. In: W.S.Marras and W. Karwowski, eds. The occupationalergonomics handbook: Interventions, controls, andapplications in occupational ergonomics, chapter 46, 2nded., Boca Raton, FL: CRC Press, 46-1–46-13.
1106 J.N. Hodder et al.
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14

Nelson, A. and Baptiste, A.S., 2006. Update on evidence-based practices for safe patient handling and movement.Orthopaedic Nursing, 25 (6), 367–368.
Owen, B.D., 1989. The magnitude of low back problems innursing. Western Journal of Nursing Research, 11 (2),234–242.
Owen, B.D., 2000. Preventing injuries using an ergonomicapproach. Association of Perioperative Registered NursesJournal, 72 (6), 1031–1036.
Owen, B.D. and Garg, A., 1991. Reducing risk for back painin nursing personnel. American Association of Occupa-tional Health Nurse Journal, 39 (1), 24–32.
Pompeii, L.A., et al., 2009. Musculoskeletal injuries resultingfrom patient handling tasks among hospital workers.American Journal of Industrial Medicine, 52 (7), 571–578.
Santaguida, P.L., et al., 2005. Comparison of cumulative lowback loads of caregivers when transferring patients usingoverhead and floor mechanical lifting devices. ClinicalBiomechanics, 20 (9), 906–916.
Sherehiy, B., Karwowski, W., and Marek, T., 2004.Relationship between risk factors and musculoskeletaldisorders in the nursing profession: A systematic review.Occupational Ergonomics, 4, 241–279.
Skotte, J.H. and Fallentin, N., 2008. Low back injury riskduring repositioning of patients in bed: the influence ofhandling technique, patient weight and disability. Ergo-nomics, 51 (7), 1042–1052.
Teschke, K., et al., 2009. Measuring posture for epidemiol-ogy: comparing inclinometry, observations and self-reports. Ergonomics, 52 (9), 1067–1078.
Trask, C., et al., 2007. Measuring low back injury risk factorsin challenging work environments: an evaluation of costand feasibility. American Journal of Industrial Medicine,50 (9), 687–696.
Venning, P.J., 1988. Back injury prevention among nursingpersonnel: the role of education. American Association ofOccupational Health Nurse Journal, 36 (8), 327–332.
Waters, T.R., et al., 1993. Revised NIOSH equation of thedesign and evaluation of manual lifting tasks.Ergonomics, 36, 749–776.
Waters, T., et al., 2006a. Cumulative spinal loading exposuremethods for manual materials handling tasks. Part 1: iscumulative spinal loading associated with lower backdisorders? Theoretical Issues in Ergonomics Science, 7 (2),113–130.
Waters, T., et al., 2006b. Cumulative spinal loading exposuremethods for manual materials handling tasks. Part 2:methodological issues and applicability for use inepidemiological studies. Theoretical Issues in ErgonomicsScience, 7 (2), 131–148.
Winkelmolen, G.H.M., Landeweerd, J.A., and Drost, M.R.,1994. An evaluation of patient lifting techniques.Ergonomics, 37 (5), 921–932.
Yassi, A., et al., 2001. A randomized controlled trial toprevent patient lift and transfer injuries of health careworkers. Spine, 26 (16), 1739–1746.
Yip, V.Y.B., 2004. New low back pain in nurses: workactivities, work stress and sedentary lifestyle. Journal ofAdvanced Nursing, 46 (4), 430–440.
Zhuang, Z., et al., 1999. Biomechanical evaluation ofassistive devices for transferring residents. AppliedErgonomics, 30, 285–294.
Ergonomics 1107
Dow
nloa
ded
by [
Swin
burn
e U
nive
rsity
of
Tec
hnol
ogy]
at 0
2:32
03
Sept
embe
r 20
14