Embed Size (px)
Citation preview
Continuing Care and 3-Year Outcomes in Adolescents: Moving Toward a
Disease Management Model
Cynthia Campbell, PhD 1
Constance Weisner, DrPH, LCSW 1, 2
Felicia Chi, MPH 1
Stacy Sterling, MSW, MPH 1
AcademyHealthJune 9, 2008
Washington DC
1 Division of Research, Northern California, Kaiser Permanente
2 Department of Psychiatry, University of California San Francisco
Funded by National Institute on Drug Abuse, National Institute on Alcohol and Alcoholism,
Robert Wood Johnson Foundation and the Center for Substance Abuse Treatment

Continuing Care: What is it?Continuing Care: What is it?
Typically presented as aftercare services Additional chemical dependency (CD) treatment after
usual care 6 mos - 1year
Stepped down, lower intensity
Other psychosocial services
Any type of intervention between treatment system and patient (McKay, 2005)
12 step programs Adolescents are less likely to attend
Associated with better SU outcomes (McKay, 2005)
LiteratureLiterature Recovery Management Checkups
Dennis, Scott et al. Quarterly assessments over two years after intake
Those with problems referred to linkage managers Used MI approach to address SU and other problems
Aim is for ongoing monitoring and linking them back to SU treatment More likely to return to treatment; longer retention; improved outcomes
Assertive Continuing Care Dennis, S. Godley, M. Godley Specific to adolescents Assertive case management for 90 days post discharge Community outreach, home based Associated with improved participation in continuing care, and outcomes
Telephone interventions McKay et al Evidence of association with improved outcomes, although might be more
appropriate for less severe patients (McKay et al., 2001)

Treatment Outcomes Treatment Outcomes Stronger in Short TermStronger in Short Term
Substance use is a chronic problem but treatment is episodic
Typically less than 90 days
Effects of index treatment decrease over time
Treatment careers of multiple uncoordinated episodes (Hser et al., 1997)
Low engagement with continuing care among adolescent patients
How to think of ongoing services for adolescents?

Disease Management ApproachDisease Management Approach
Conceptual approach grounded in the chronic disease management framework
Individual with a serious chronic problem (e.g., diabetes) is treated in specialty care, and when stabilized returns to PC for management and monitoring referred back to specialty care for services as needed in the
course of their health care
Similarly, SU is a chronic condition requiring ongoing care or management delivered in more than one setting (McLellan, 2000; McLellan, 2002; Hser et al, 2007)
A person may do well after treatment, but then relapse
What might an integrated care modelWhat might an integrated care modelfor substance use problems look like? for substance use problems look like?
Lessons from disease managementLessons from disease management
Specialty Care(CD and Psychiatry)
Primary Care
Screen and treat in PC if moderate problem
Continue monitoring
Specialty care if needed
Back to PC for monitoring
Continuing care
Von Korff M, Gruman J, Schaefer J, Curry SJ, Wagner EH. Collaborative management of chronic illness. Ann Intern Med. 1997;127:1097-102. Bodenheimer T, Wagner EH, Grumback K. Improving primary care for patients with chronic illness. JAMA 2002; 288:1775-9.

The Case for Primary CareThe Case for Primary Care
Post-CD treatment primary care management
There is little coordination with CD treatment by PC after treatment
Specialty treatment does not last someone’s whole life, but they will have ongoing medical care
Another opportunity to engage
Population also has a high level of medical conditions, even in adolescents
Need to have these addressed as well
Institute of Medicine, “Improving the Quality of Health Care for Mental and Substance-Use Conditions,” 2006

What are adolescents like by the time they get to treatment?

Setting: Northern California Kaiser Setting: Northern California Kaiser Permanente (KP)Permanente (KP)
Private, group-model managed care health plan
Serves 3.5 million members in 15 counties (about 40% of population in the region)
~400,000 members aged 12-18
16 hospitals, 23 outpatient clinics
~500 pediatricians
Integrated health care system (medical, psychiatry, chemical dependency services)

Study Design and Data SourcesStudy Design and Data Sources
Baseline interviews with adolescents (and a parent) at intake to CD treatment at 4 Kaiser sites (Oakland, Sacramento, Vallejo, Vacaville)
Follow-up interviews with adolescents and parents at 6 months and 1,3, and 5 years (Response rates = 92%, 92%, 86% and 85%, respectively)
Clinical ICD-9 diagnoses from automated records
Health plan administrative utilization and cost databases

Treatment ProgramsTreatment Programs Each offers 1-year program Same modalities of other CD programs in the country Intensive, structured outpatient treatment
Abstinence based Breathalyzer and urine screens
Services include group therapy, education, relapse prevention, family therapy. Individual counseling with a CD clinician available as needed Require participation of a parent or guardian Attendance at 12-step programs expected and monitored
3 Phases Eight weeks more intensive treatment 4 months of relapse prevention/continuing recovery 6 months of after care to maintain abstinence
Few stay that long, true across the literature

Adolescent CD Patients & Matched ControlsAdolescent CD Patients & Matched Controls
Sample:
419 adolescents (143 girls, 276 boys)
Mean age of initiation (11.5)
Age ranged from 13 to 17 years (mean = 16.15)
Ethnicity: 6% Asian
9% Native American
16% African-American
20% Hispanic
49% White
Matched Controls:
2,084 adolescents from the health plan
No documented alcohol or drug history
Matched on gender, age, length of health plan enrollment, and catchment area
Sterling S, Weisner C. Chemical dependency and psychiatric services for adolescents in private managed care: Implications for outcomes. Alcohol Clin Exp Res. May 2005;25(5):801-9.
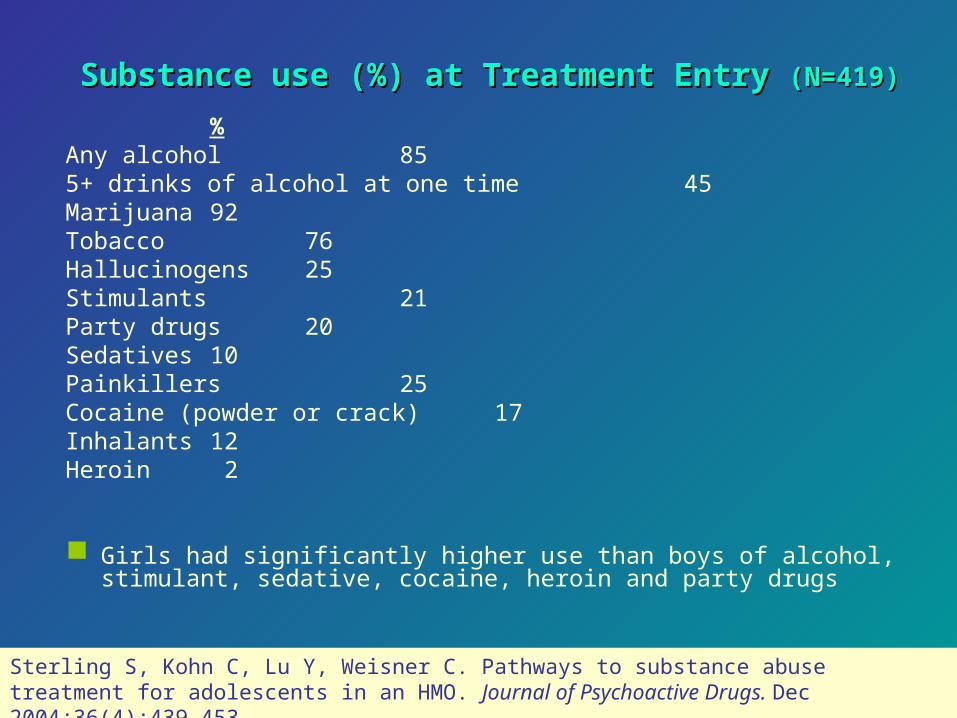
Substance use (%) at Treatment Entry Substance use (%) at Treatment Entry (N=419)(N=419) %
Any alcohol 855+ drinks of alcohol at one time 45Marijuana 92Tobacco 76Hallucinogens 25Stimulants 21Party drugs 20Sedatives 10Painkillers 25Cocaine (powder or crack) 17Inhalants 12Heroin 2
Girls had significantly higher use than boys of alcohol, stimulant, sedative, cocaine, heroin and party drugs
Sterling S, Kohn C, Lu Y, Weisner C. Pathways to substance abuse treatment for adolescents in an HMO. Journal of Psychoactive Drugs. Dec 2004;36(4):439-453.

Medical Conditions among Adolescent Medical Conditions among Adolescent CD Treatment Intakes (%) CD Treatment Intakes (%)
Tx Intakes Controls p-value
Abdominal Pain 10.6 5.7 <.001Respiratory System Cond. 54.5 37.8 <.0001Gastroenteritis 6.5 3.9 <.05Conjunctivitis 6.9 3.2 <.001Muscle Pain 8.4 3.9 <.0001Scoliosis 3.1 1.3 <.01Benign Uterine Cond. 7.7 3.2 <.0001Injury & Poisoning 49.6 36.4 <.0001Urinary Tract Infection 3.4 2.0 <.05STDs 4.8 1.5 <.0001
*One-third of parents reported that their child had chronic health problems (asthmaand allergies most commonly). Past pregnancies: 15% of girls
Mertens JR, Flisher AJ, Fleming MF, Weisner CM. (2007). Medical conditions of adolescents in alcohol and drug treatment: comparison with matched controls. Journal of Adolescent Health Feb;40(2):173-9.

Mental Health Conditions of AdolescentsMental Health Conditions of Adolescentsin CD Treatment & Matched Controls (%)in CD Treatment & Matched Controls (%)
Tx Intakes Controls p-value
Depression 36.3 4.2 <.0001
Anxiety Disorder 16.3 2.3 <.0001
Eating Disorders 1.2 0.43 .067
ADHD 17.2 3.0 <.0001
Conduct Disorder 19.3 1.2 <.0001
Conduct Disorder (w/ODD) 27.3 2.3 <.0001
Any Psychiatric DX 55.5 9.0 <.0001

Gender Differences in Mental Health Comorbidities:Gender Differences in Mental Health Comorbidities:Adolescents in CD TreatmentAdolescents in CD Treatment (in %) (in %)
30
17
10
2 2
14
21
14
43
28
05
1015202530354045
GirlsBoys
**<.01
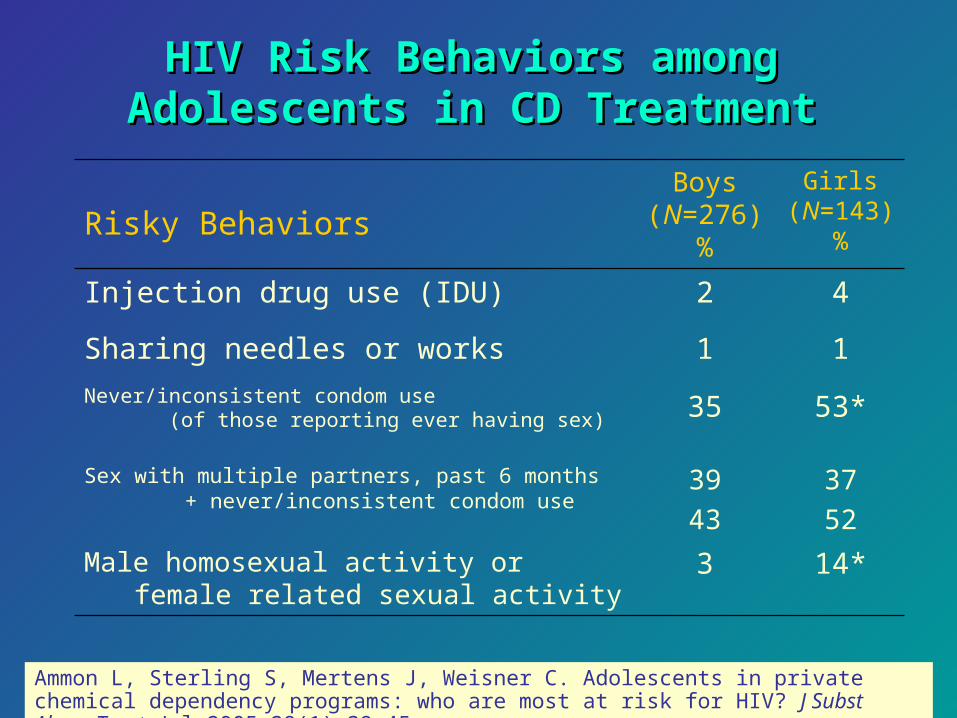
HIV Risk Behaviors amongHIV Risk Behaviors amongAdolescents in CD TreatmentAdolescents in CD Treatment
14*3Male homosexual activity or female related sexual activity
37
52
39
43
Sex with multiple partners, past 6 months + never/inconsistent condom use
53*35Never/inconsistent condom use (of those reporting ever having sex)
11Sharing needles or works
42Injection drug use (IDU)
Girls(N=143)
%
Boys(N=276)
%Risky Behaviors
Ammon L, Sterling S, Mertens J, Weisner C. Adolescents in private chemical dependency programs: who are most at risk for HIV? J Subst Abuse Treat. Jul 2005;29(1):39-45.

AdolescentAdolescent Chemical Dependency Chemical Dependency Patients: HIV Risk BehaviorsPatients: HIV Risk Behaviors
Rate of at least 1 reported HIV risk behavior was 47%
Boys who drank 5 or more drinks in a day at least once during the past 6 months were 4 times more likely than other patients to engage in multiple HIV risk behaviors.
Girls who used narcotic analgesics (painkillers) without prescription at least once during the previous 6 months were 5 times more likely to engage in multiple HIV risk behaviors.
Ammon L, Sterling S, Mertens J, Weisner C. Adolescents in private chemical dependency programs: who are most at risk for HIV? J Subst Abuse Treat. 2005;29(1):39-45.

Outcome Argument for Continuing Care

One Reason for Continuing Care:One Reason for Continuing Care:Alcohol and Drug Use after TreatmentAlcohol and Drug Use after Treatment
1 year after treatment – doing better, but many not abstinent* 61% abstinent from alcohol 59% abstinent from drugs 47% abstinent from both 36% in remission (non problematic use)
3 years after treatment 38% abstinent from alcohol 57% abstinent from drugs 30% abstinent from both 26% in remission
* 30-day abstinence* Remission: used alcohol but no more than once/week and never more than 2 drinks, OR used marijuana, but only once/month or less, AND b) Used no other drugs (excluding tobacco); AND, c) Had no dependence/abuse symptoms

Initial Exploration of Continuing CareInitial Exploration of Continuing Care
Anchored in PC, with specialty CD and MH services as indicated
Initial specifications tested 1 or more PC visit each year after 1 yr FUSubsequent MH or CD services if needed,
either within or outside KP

Role of PC-based Continuing Care: To Return Role of PC-based Continuing Care: To Return More Severe Teens to Treatment and Improve More Severe Teens to Treatment and Improve
Outcomes Outcomes
Three years after treatment: 1 or more PC visits/year was associated with
abstinence and remission 32% abstinent vs. 18% 28% remitted vs. 14%
For those with any MH symptoms at 1 year, 1 or more MH visits was related abstinence (40% vs. 25%)
Among those not abstinent at 1 year, CD readmission were related to abstinence (40% vs. 33%)
1 or more PC visits was associated with a CD readmission and MH services after index CD treatment
All p <.05

Cost Considerations for Continuing CareCost Considerations for Continuing Care
Medical costs decrease after CD treatment for adults
Medical costs for adolescent CD patients did not decrease in the year after treatment as they do for adults
Parthasarathy S, Weisner CM, Hu T-W, Moore C. Association of outpatient alcohol and drug treatment with health care utilization and cost: revisiting the offset hypothesis. J Stud Alcohol. Jan 2001;62(1):89-97.
Parthasarathy S, Weisner C. (2006). Health care services use by adolescents with intakes into an outpatient alcohol and drug treatment program. The American Journal on Addictions 15(Supp 1):113-21.

Costs at 3 yearsCosts at 3 years
Overall, average costs increased in the year after treatment, then decreased
Costs are higher for the cases compared to the controls, although the difference has narrowed by 3 years
Looking at abstinence at 3 years, both abstainers and non-abstainers had higher average costs than the matched sample (p<.05) Abstainers had higher costs in all departments except ER.
Could be a proxy measure for appropriate use

Disease Management ApproachDisease Management Approach
Specialty Care(CD and Psychiatry)
Primary Care
Screen and treat in PC if moderate problem
Continue monitoring
Specialty care if needed
Back to PC for monitoring
Continuing care
Von Korff M, Gruman J, Schaefer J, Curry SJ, Wagner EH. Collaborative management of chronic illness. Ann Intern Med. 1997;127:1097-102. Bodenheimer T, Wagner EH, Grumback K. Improving primary care for patients with chronic illness. JAMA 2002; 288:1775-9.

What Could This Look Like in PC?What Could This Look Like in PC?
Two approaches
1. Training PC providers to screen for problems, especially in those who have been in treatment or diagnosed
2. “Patient-centered” approach (IOM) Empowers patient Educates patient and family about importance of managing
SU problems similar to medical problems Addresses stigma, communication, how to raise the issue
with providers

SummarySummary Primary care is important after CD treatment as
well - keeping primary care in the loop after treatment
Treatment is not a “magic bullet” and even “aftercare” ends at some point
Important for individuals in becoming accustomed to talking about alcohol and other behavioral problems to physicians as a life pattern
Future Research

COLLABORATORSCOLLABORATORS
Felicia Chi, MPH Sujaya Parthasarathy, PhD Lyndsay Ammon, PhD Cand. Charlie Moore, MD David Pating, MD Steve Allen, PhD Ken Athey, LCSW Michael Leotaud, LCSW Agatha Hinman, CA Georgina Berrios, BA Melanie Jackson-Morris, BA Yun Lu, MPH Cynthia Perry-Baker, BA Gina Smith-Anderson, BA Barbara Pichotto, BA, CADAC
Northern California Kaiser Permanente Adolescent Medicine
and Chemical Dependency Rehabilitation Programs*
*Thanks to clinicians, patients and family members for participating in these studies

Are there opportunities for PC intervention?

Utilization Patterns during 24 Months prior to Treatment Utilization Patterns during 24 Months prior to Treatment IntakeIntake
24 months prior to intake (%)
12 months prior to intake (%)
3 months prior to intake (%)
Primary Care* 89.5 79.2 48.7
Psychiatry 50.1 42.0 30.8
ER 26.3 17.9 11.7
*Includes visits to the following departments: Family Practice, General Medicine, GYN, Medicine, Pediatrics, Physical Medicine and Urgent Care.