Embed Size (px)
Citation preview
CONTINUED EXPLORATION OF EVIDENCE-‐BASED TREATMENTS FOR PTSD
COGNITIVE PROCESSING THERAPY
ASHLEE WHITEHEAD, LPC, CADC CERTIFIED CPT PROVIDER PTSD CLINICAL TEAM
PORTLAND VA MEDICAL CENTER���
Contemporary Mental Health Treatment For Returning Veterans Portland State University
CONTINUED EXPLORATION OF COGNITIVE PROCESSING THERAPY 25 % of OIF/OEF veteran VA Health Care users have been diagnosed with PTSD – 120,000 (FY 2009)
Research consistently reveals that MH providers deliver Evidence Based Psychotherapies (EBPs) for PTSD at low rates…
WHY?
Some obstacles to implementing EBPs for PTSD Maintenance view of PTSD Worry about retraumatization with exposure Therapist self-‐efXicacy Client participation and interest
SOLUTION?
Implementation of VHA MH Strategic Plan (2006) National Initiatives for Disseminating PTSD Treatment: Prolonged Exposure & Cognitive Processing Therapy
All veterans with PTSD have access to CPT or PE
EBP Coordinator “champion” at every VA
“Buy-‐in” from MH leadership
Impact of EBP Implementation Initiative 2,700 VA MH providers trained (May 2010) 96% of VAs providing CPT or PE; 72% providing both Average decline of 30% (20 pts) on PTSD Checklist (n=474)
Therapist conXidence levels increase pre to post training
Case studies and Xirst hand clinical experience demonstrate signiXicant positive clinical impact on veterans who receive EBPs
INCREASING POSITIVE OUTCOMES W/EBPS
Therapist Self-‐EfXicacy! PTSD Psychoeducation: Desire to approach outweighs desire to avoid.
Client needs to believe that improvement is possible and he has the ability to tolerate therapy (skills).
Strategic Goal Setting: Develop a personalized plan based on what the client needs to maximize their chance of success in treatment.
Assess barriers (SI, Substance Use, TBI, Support System, Psychosocial stressors).
Consider residential, individual vs. group
CPT – a quick review Cognitive Processing Therapy is a 12-‐session treatment based on a social cognitive theory of PTSD that focused on the meaning individuals make in response to the traumatic event and how people cope as they try to regain a sense of mastery or control over their lives (Resick & Schnicke, 1993).
Over 20 years of clinical practice, initially focused on trauma of rape. In 2006 was expanded to Xit veteran/military population (Resick, Monson, Schnurr).
COGNITIVE PROCESSING THERAPY (CPT) FOR PTSD CPT RATIONALE
PTSD symptoms are attributed to a "stalling out" in the natural process of recovery
What interferes with natural recovery from PTSD? Avoidance Behaviors
reinforce Distorted beliefs about the trauma and become
Generalized to current life situations
Cognitive-‐focused techniques are used to help Clients move past stuck points and progress toward recovery.
COGNITIVE PROCESSING THERAPY (CPT) FOR PTSD STRUCTURE OF CPT SESSIONS
• 12 x 50-‐minute structured sessions
• Participants complete out-‐of-‐session practice assignments
• Sessions typically conducted weekly or bi-‐weekly
• Includes a brief written trauma account along with ongoing practice of cognitive techniques
• 12 x 90-‐120 minute structured sessions
• Participants complete out-‐of-‐session practice assignments
• Typically conducted by 2 clinicians
• 8-‐10 Veterans per group • Includes a brief written trauma account component, along with ongoing practice of cognitive techniques
Individual CPT Group CPT
COGNITIVE PROCESSING THERAPY (CPT) FOR PTSD THE ESSENTIAL INGREDIANTS
The Impact of the Event
Identifying Stuck Points
Identifying and resolving assimilated beliefs
Challenging and balancing overaccomodated beliefs.
Use of Socratic Questioning
Processing natural emotions related to the trauma
COGNITIVE PROCESSING THERAPY (CPT) FOR PTSD 5 major dimensions that may be disrupted by traumatic events: 1) Safety 2) Trust 3) Power and Control 4) Esteem 5) Intimacy
11
SESSION 1. PTSD SYMPTOMS AND RATIONALE
Types of emotions Goal for natural emotions Goal for manufactured emotions
Choosing index traumatic event Practice Assignment: Impact Statement
12
SESSION 2. IMPACT STATEMENT Goal: Client examines the impact of the traumatic event on their lives.
Help identify stuck points in statement Ask about other areas that were not touched upon Highlight connection between thoughts and feelings
Introduce ABC Sheets Practice Assignment: ABC Sheets, Stuck Point Log
STUCK POINTS IN 5 DIMENSIONS SAFETY I cannot protect myself/others. The world is completely dangerous. TRUST Other people should not trust me. The government cannot be trusted. POWER/CONTROL I must control everything that happens to me. People in authority always abuse their power. ESTEEM I deserve to have bad things happen to me People are by nature evil and only out for themselves. INTIMACY I am unlovable because of the trauma. If I let other people get close to me, I'll get hurt again.
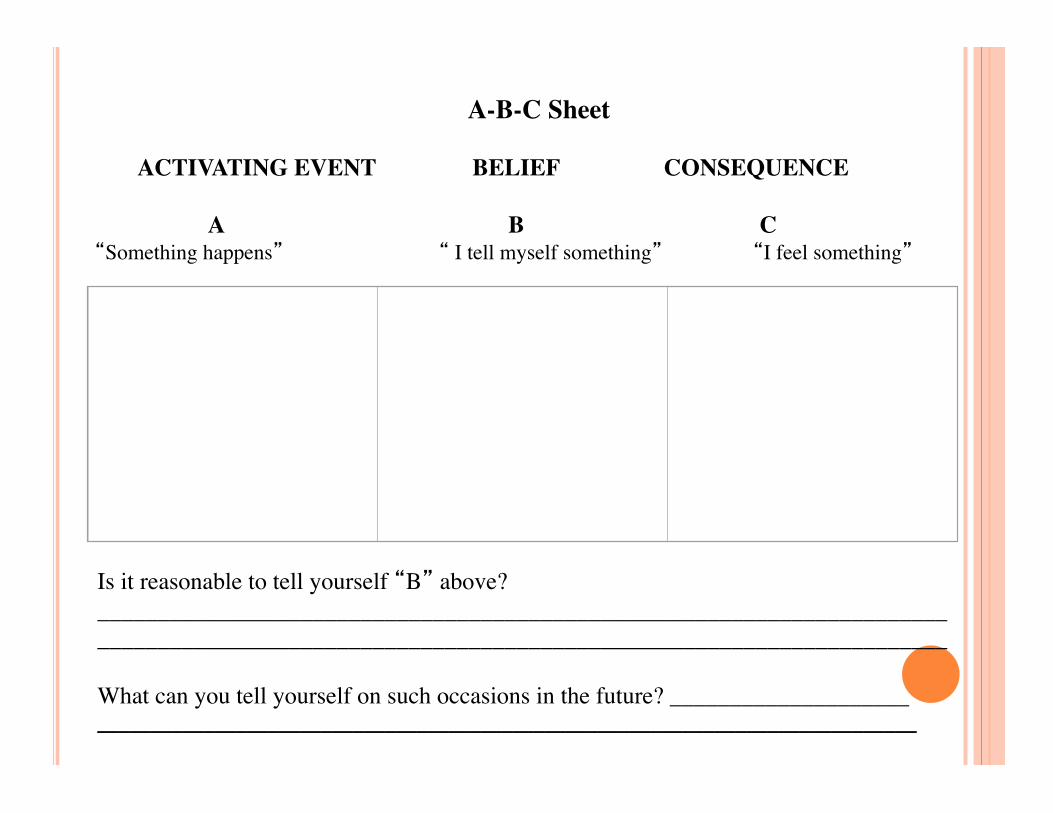
A-B-C Sheet���
ACTIVATING EVENT BELIEF CONSEQUENCE
A B C ��� “Something happens” “ I tell myself something” “I feel something”
Is it reasonable to tell yourself “B” above? _______________________________________________________________________ _______________________________________________________________________ What can you tell yourself on such occasions in the future? ____________________ _____________________________________________________________________________
15
SESSION 3. EVENTS, THOUGHTS & EMOTIONS
Goal: Client learns to recognize relationship between event/thought/emotion and to work through stuck points
Review A-‐B-‐C sheets. Using Socratic questions, help Client generate alternative thoughts and consequent feelings.
Gently begin to challenge undoing or self-‐blame statements.
Practice Assignment: Written Account/ABC sheets
SOCRATIC QUESTIONS
Clari?ication “What do you mean when you say…?” Probing Assumptions “How did you come to this
conclusion?” Probing Reasons and Evidence “Would these reasons
stand up in a reputable newspaper/ court of law as evidence?”
Questioning Viewpoints and Perspectives “What alternative ways of looking at this are there?”
Analyzing Implications and Consequences “Then what would happen? What would it mean if you gave up that belief?”
Questions About the Question “What is the point of asking that question?”
17
SESSION 4. FIRST ACCOUNT Goal: Client uses the account to process natural emotions and also continue identifying and working through stuck points
Client reads account aloud to therapist. After Client reads account, Client and therapist discuss reactions to writing it/reading it.
First work on emotions. Sit with them, name them.
Then therapist gently challenges self-‐blame and hindsight bias.
Practice Assignment: Rewrite Account
18
SESSION 5. SECOND ACCOUNT Goal: Client uses the 2nd account to process natural emotions and also continue identifying and working through stuck points
Client reads second account of incident. Client and therapist continue to process any remaining self-‐blame or undoing.
Therapist introduces Challenging Questions Worksheet.
Practice Assignment: CQWs
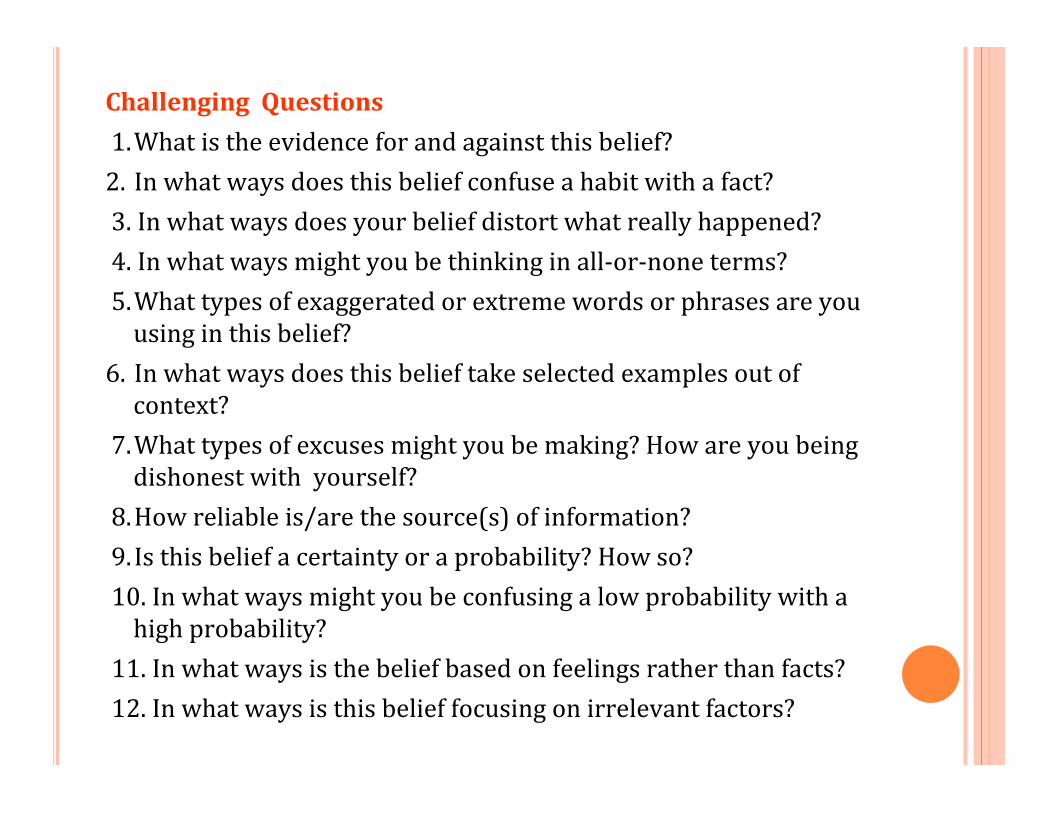
Challenging Questions 1. What is the evidence for and against this belief? 2. In what ways does this belief confuse a habit with a fact? 3. In what ways does your belief distort what really happened? 4. In what ways might you be thinking in all-‐or-‐none terms? 5. What types of exaggerated or extreme words or phrases are you using in this belief?
6. In what ways does this belief take selected examples out of context?
7. What types of excuses might you be making? How are you being dishonest with yourself?
8. How reliable is/are the source(s) of information? 9. Is this belief a certainty or a probability? How so? 10. In what ways might you be confusing a low probability with a high probability?
11. In what ways is the belief based on feelings rather than facts? 12. In what ways is this belief focusing on irrelevant factors?
20
SESSION 6. CHALLENGING QUESTIONS Goal: Client learns how to challenge stuck points Client and therapist review Challenging Questions Worksheets to question single statements or beliefs.
Therapist introduces Patterns of Problematic Thinking Sheet to see if there are typical patterns of cognition.
Practice Assignment: CQWs & Problematic Patterns Sheets
Patterns of Problematic Thinking 1. Jumping to conclusions: 2. Exaggerating or minimizing: 3. Disregarding important aspects: 4. Oversimplifying: 5. Over-‐generalizing: 6. Mind reading: 7. Emotional reasoning:
22
SESSION 7. PROBLEMATIC PATTERNS Goal: Client continues to learn skills to help them identify and challenge stuck points and patterns of maladaptive thinking
Client and therapist review Patterns of Problematic Thinking.
Therapist introduces Challenging Beliefs Worksheets.
Therapist introduces the Xirst of 5 modules: Safety. Practice Assignment: CBWs and read Safety module
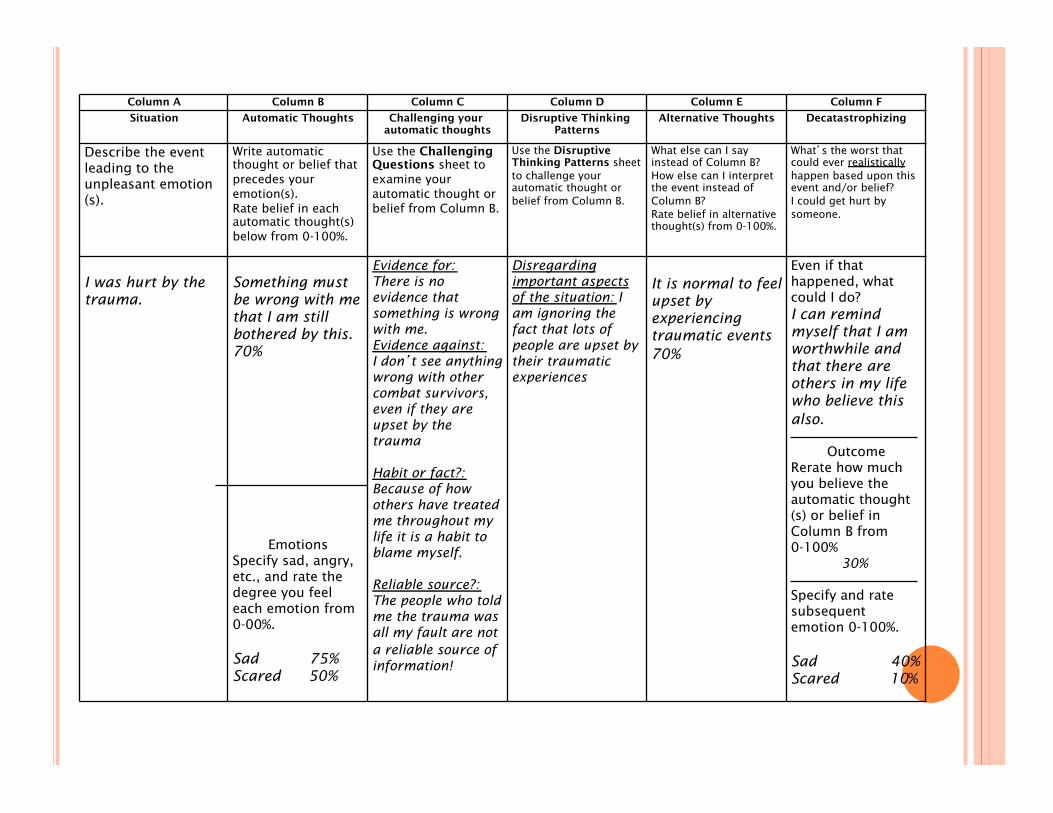
Column A Column B Column C Column D Column E Column F Situation Automatic Thoughts Challenging your
automatic thoughts Disruptive Thinking
Patterns Alternative Thoughts Decatastrophizing
Describe the event leading to the unpleasant emotion(s).
Write automatic thought or belief that precedes your emotion(s). Rate belief in each automatic thought(s) below from 0-100%.
Use the Challenging Questions sheet to examine your automatic thought or belief from Column B.
Use the Disruptive Thinking Patterns sheet to challenge your automatic thought or belief from Column B.
What else can I say instead of Column B? How else can I interpret the event instead of Column B? Rate belief in alternative thought(s) from 0-100%.
What’s the worst that could ever realistically happen based upon this event and/or belief? I could get hurt by someone.
I was hurt by the trauma.
Something must be wrong with me that I am still bothered by this. 70%
Emotions Specify sad, angry, etc., and rate the degree you feel each emotion from 0-00%. Sad 75% Scared 50%
Evidence for: There is no evidence that something is wrong with me. Evidence against: I don’t see anything wrong with other combat survivors, even if they are upset by the trauma Habit or fact?: Because of how others have treated me throughout my life it is a habit to blame myself. Reliable source?: The people who told me the trauma was all my fault are not a reliable source of information!
Disregarding important aspects of the situation: I am ignoring the fact that lots of people are upset by their traumatic experiences
It is normal to feel upset by experiencing traumatic events 70%
Even if that happened, what could I do? I can remind myself that I am worthwhile and that there are others in my life who believe this also.
Outcome
Rerate how much you believe the automatic thought(s) or belief in Column B from 0-100% 30% Specify and rate subsequent emotion 0-100%. Sad 40% Scared 10%
24
SESSION 8. CBW AND SAFETY Client and therapist review challenging belief worksheets.
Client and therapist discuss safety issues.
Therapist introduces Trust module. Practice Assignment: CBWs and read Trust Module
25
SESSION 9. CBW AND TRUST Client and therapist review practice on trust issues and other completed Challenging Beliefs Worksheets.
Therapist introduces Power/Control module.
Practice Assignment: CBWs and read Power/Control module
26
SESSION 10. CBW AND POWER AND CONTROL
Client and therapist review control/power issues and other Challenging Beliefs Worksheets
Therapist introduces Esteem module. Practice Assignment: CBWs, read Esteem module, practicing giving and receiving compliments/praise, pleasurable activity
27
SESSION 11. CBW AND ESTEEM Client and therapist review esteem issues and other Challenging Beliefs Worksheets.
Client and therapist review other practice.
Therapist introduces Intimacy module. Practice Assignment: CBWs, read Intimacy module, and rewrite impact statement
28
SESSION 12. INTIMACY AND FINAL IMPACT
Client and therapist review Challenging Beliefs Worksheets on intimacy
Client reads new Impact Statement Client and therapist review course of therapy and skills learned
Client and therapist identify future goals and issues which still need attention
FINAL THOUGHTS What is the risk of not doing an Evidence
Based Treatment for PTSD?
Instead of thinking of “My client can’t do CPT because...” Try, “What does my client need to increase their chances of success with CPT?”
HOW TO REFER A CLIENT TO CPT
Cognitive Processing Therapy is available through VA Medical Centers, including through the Portland VAMC PTSD Clinical Team (PCT) for eligible veterans.
Portland VA Medical Center http://www.portland.va.gov/ Eligibility/Enrollment (503) 220-‐8262, ext. 55289 Admission to the PCT requires a consult from the veteran's Mental Health Provider at the Portland VA Medical Center. If the veteran does not have a Mental Health Provider, the Xirst step would be to call the Mental Health Access Clinic at 503-‐220-‐8262 x56409. A screening interview will be required as a condition of admission.
REFERENCES
Karlin, et. al Dissemination of Evidence-‐Based Psychological Treatments for Posttraumatic Stress Disorder in the Veterans Health Administration. Journal of Traumatic Stress V. 23, No. 6, December 2010.
Cognitive Therapy for Posttraumatic Stress Disorder by Shipherd, Street, and Resick in Chapter 5 of Cognitive-‐Behavioral Therapies for Trauma, Second Edition by Victoria M. Follette PhD and Josef I. Ruzek (2007)
Ashlee Whitehead, LPC, CADC Licensed Professional Counselor, PTSD Clinical Team
Military Sexual Trauma (MST) Coordinator Portland VA Medical Center
3710 SW US Veterans Hospital Rd. Portland, OR 97239
Ph: 503.220.8262 Ext. 57429 [email protected]