Embed Size (px)
Citation preview
6/01/2011
1
VIRAL INFECTIONSVIRAL INFECTIONS
Dr Tom Connell
Infectious Disease Physician
PLANPLANQuizClassification of viruses
Cases and descriptions
Viruses and pregnancyViruses and pregnancy
Prevention
Common and not so common viruses in
children
‘Virus’ is a latin word used by doctors to mean “your guess is as good as mine”
QUIZQUIZ
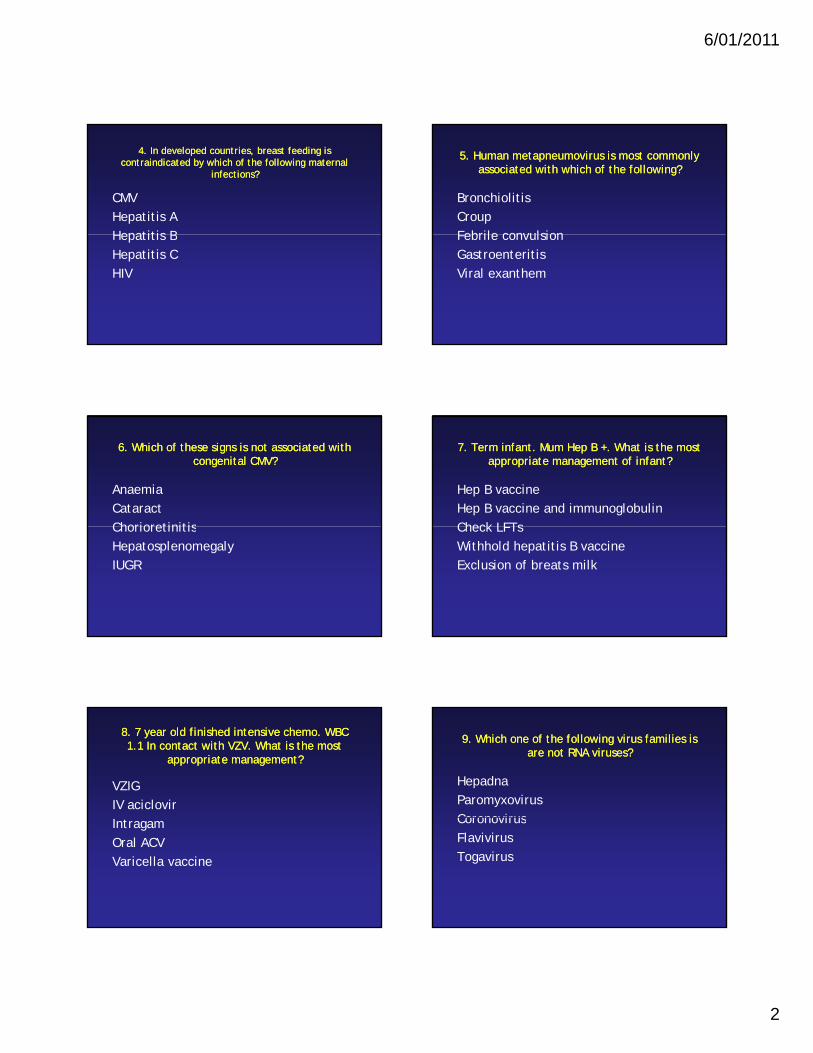
1. Which of the following viruses has not been 1. Which of the following viruses has not been associated with malignancy?associated with malignancy?
CMVEBVHHV 8HHV-8HIVHPV
2. 2. 2 yr old. Lesions on 2 yr old. Lesions on hands and feethands and feet
Fever 38 CFever 38 C
Coxackie A16EBVHSV-1HHV-6Parvovirus B19
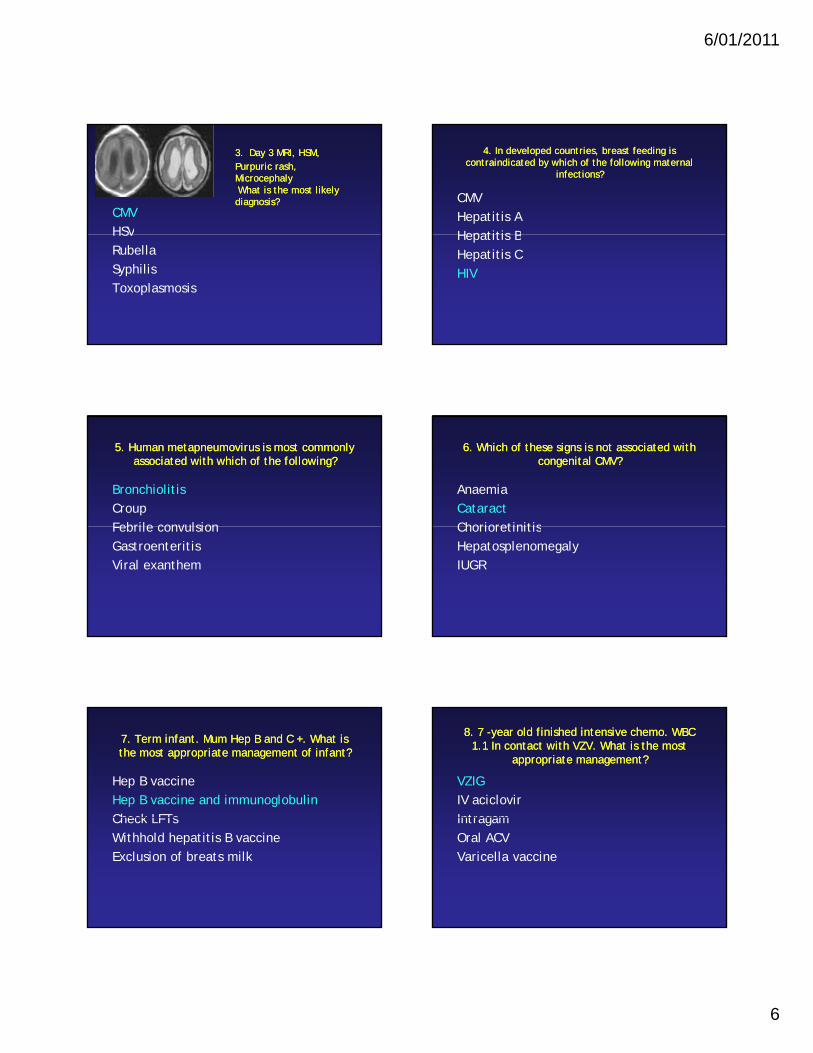
3. Day 3 MRI, HSM, Purpuric rash3. Day 3 MRI, HSM, Purpuric rashMicrocephalyMicrocephalyWhat is the most likely What is the most likely diagnosis?diagnosis?
CMVHSVHSVRubellaSyphilisToxoplasmosis
6/01/2011
2
4. In developed countries, breast feeding is 4. In developed countries, breast feeding is contraindicated by which of the following maternal contraindicated by which of the following maternal
infections?infections?
CMVHepatitis AHepatitis BHepatitis BHepatitis CHIV
5. Human metapneumovirus is most commonly 5. Human metapneumovirus is most commonly associated with which of the following?associated with which of the following?
BronchiolitisCroupFebrile convulsionFebrile convulsionGastroenteritisViral exanthem
6. Which of these signs is not associated with 6. Which of these signs is not associated with congenital CMV?congenital CMV?
AnaemiaCataractChorioretinitisChorioretinitisHepatosplenomegalyIUGR
7. Term infant. Mum Hep B +. What is the most 7. Term infant. Mum Hep B +. What is the most appropriate management of infant?appropriate management of infant?
Hep B vaccineHep B vaccine and immunoglobulinCheck LFTs Check LFTs Withhold hepatitis B vaccineExclusion of breats milk
8. 7 year old finished intensive chemo. WBC 8. 7 year old finished intensive chemo. WBC 1.1 In contact with VZV. What is the most 1.1 In contact with VZV. What is the most
appropriate management?appropriate management?
VZIGIV aciclovirIntragamOral ACVVaricella vaccine
9. Which one of the following virus families is 9. Which one of the following virus families is are not RNA viruses?are not RNA viruses?
HepadnaParomyxovirusCoronovirusCoronovirusFlavivirusTogavirus
6/01/2011
3
10. Which of the following statements 10. Which of the following statements concerning Parvovirus B 19 is concerning Parvovirus B 19 is NOTNOT true?true?
DNA virusIncubation period 4-16 daysAlso called fifth diseaseAlso called fifth diseaseMainly affects young childrenThe majority of infections are
asymptomatic
11. Which of the following conditions has not 11. Which of the following conditions has not been associated with parvoviral infection?been associated with parvoviral infection?
GlomerulonephritisParotitisChronic fatigue syndromeChronic fatigue syndromeMeningitisPurpuric rash
12. Which one of the following statements 12. Which one of the following statements concerning parvovirus in pregnancy is true?concerning parvovirus in pregnancy is true?
Risk highest in the first trimesterIntruterine death is commonLong term effects are commong1:1000 during pregnancyIgG+/Igm- maternal serology indicates
immunity
13. Which one of the following 13. Which one of the following statements is true in relation to HHVstatements is true in relation to HHV--6? 6?
Causes fifth diseaseMost children acquire infection by age 2
yearsyearsAlso called exanthem subitumSeroprevalence is lowHigh mortality
14. Which one of the following conditions is 14. Which one of the following conditions is NOTNOT associated with congenital rubella?associated with congenital rubella?
ChorioretinitisIUGRDeafnessDeafnessPDAThrombocytopenia
15. In a measles outbreak/contact, which of 15. In a measles outbreak/contact, which of the following measures is most appropriate?the following measures is most appropriate?
Infants age 9-12 months should be give one MMR vaccine that will cover for the 12 month immunisation
Measles immunoglobulin should be Measles immunoglobulin should be administered to all contacts
Exclude from school for 7 daysMMR vaccine should be given to susceptible if
within 72 hours
6/01/2011
4
16. Which of the following statements is 16. Which of the following statements is true concerning swine flu influenza?true concerning swine flu influenza?
High mortality in general populationVaccine associated with high risk of GBSInfluenza B virusInfluenza B virusOseltamavir is contraindicated in
pregnancyIncubation period 3-5 days
17. Which of the following statements is NOT 17. Which of the following statements is NOT true in relation to HIV infection?true in relation to HIV infection?
Untreated the chance of MTCT is 30%CMV is not an AIDS defining illnessInfected infants < 12 months should be Infected infants 12 months should be
treated based on VL and CD4 countHIV-infected mothers should not
breastfeedWith treatment in pregnancy rates of
transmission < 1%
18. 3 year old John was found by his mum with a syringe in his 18. 3 year old John was found by his mum with a syringe in his hand. He was crying and it appeared that there was a small hand. He was crying and it appeared that there was a small puncture wound to his hand. Which of the following is true puncture wound to his hand. Which of the following is true
concerning his risk of viral infection with Hep B, Hep C and HIV if concerning his risk of viral infection with Hep B, Hep C and HIV if there had been a significant exposure?there had been a significant exposure?
HIV 10%, Hep B 3%, Hep C, 30%, HIV 0.3%, Hep B 30%, Hep C 3%, p , pHIV 30%, Hep B 3%, Hep C 0.3%HIV 0.1%. Hep B 1%, Hep C 10%
19. Which of the following medications is most 19. Which of the following medications is most likely to be used to treat Hepatitis B infection?likely to be used to treat Hepatitis B infection?
AcyclovirGanciclovirLamivudineLamivudineInterferon gammaVidarabine
20. Which of these situations concerning 20. Which of these situations concerning maternal HSV is associated with the greatest maternal HSV is associated with the greatest
risk to the baby?risk to the baby?
Mother has recurrent genital HSV-infection
Mother acquires infection with HSV-2 Mother acquires infection with HSV 2 having had HSV-1 (non-primary)
Mother has primary HSV-1 early in pregnancy
Mother has primary HSV-1 at 34 weeks
21. Which is 21. Which is notnot a category of antia category of anti--retroviral retroviral medications?medications?
Nucleoside reverse transcriptase inhibitors
Non-nucleoside reverse transcriptase Non nucleoside reverse transcriptase inhibitors
Fusion inhibitorsCCR4 antagonists
6/01/2011
5
22. WHO recommends treating which of the 22. WHO recommends treating which of the following with HIV?following with HIV?
All infants less than 1 yr of ageOnly infants with CD4% <25Only infants with VL>100 000Only infants with VL>100,000No infants as they are at less risk
23. Which strain was responsible for the 23. Which strain was responsible for the swine flu pandemic?swine flu pandemic?
H3N2H5N1H1NIH1NIH2N3
24. Estimated number of confirmed 24. Estimated number of confirmed cases of swine flu in Australia in 2009?cases of swine flu in Australia in 2009?
404004000400040000
25. Estimated number of deaths due to swine 25. Estimated number of deaths due to swine flu in Australia in 2009flu in Australia in 2009
202002000200020000
1. Which of the following viruses has not been 1. Which of the following viruses has not been associated with malignancy?associated with malignancy?
CMVEBVHHV 8HHV-8HIVHPV
2 yr old. Lesions on hands 2 yr old. Lesions on hands and feetand feet
Fever 38 CFever 38 C
Coxackie A16EBVHSV-1HHV-6Parvovirus B19
6/01/2011
6
3.3. Day 3 MRI, HSM, Day 3 MRI, HSM, Purpuric rash, Purpuric rash, MicrocephalyMicrocephalyWhat is the most likely What is the most likely diagnosis?diagnosis?
CMVHSVHSVRubellaSyphilisToxoplasmosis
4. In developed countries, breast feeding is 4. In developed countries, breast feeding is contraindicated by which of the following maternal contraindicated by which of the following maternal
infections?infections?
CMVHepatitis AHepatitis BHepatitis BHepatitis CHIV
5. Human metapneumovirus is most commonly 5. Human metapneumovirus is most commonly associated with which of the following?associated with which of the following?
BronchiolitisCroupFebrile convulsionFebrile convulsionGastroenteritisViral exanthem
6. Which of these signs is not associated with 6. Which of these signs is not associated with congenital CMV?congenital CMV?
AnaemiaCataractChorioretinitisChorioretinitisHepatosplenomegalyIUGR
7. Term infant. Mum Hep B and C +. What is 7. Term infant. Mum Hep B and C +. What is the most appropriate management of infant? the most appropriate management of infant?
Hep B vaccineHep B vaccine and immunoglobulinCheck LFTs Check LFTs Withhold hepatitis B vaccineExclusion of breats milk
8. 7 8. 7 --year old finished intensive chemo. WBC year old finished intensive chemo. WBC 1.1 In contact with VZV. What is the most 1.1 In contact with VZV. What is the most
appropriate management?appropriate management?
VZIGIV aciclovirIntragamIntragamOral ACVVaricella vaccine
6/01/2011
7
9. Which one of the following virus families is 9. Which one of the following virus families is not an RNA virus?not an RNA virus?
HepadnaParomyxovirusCoronovirusCoronovirusFlavivirusTogavirus
10. Which of the following statements 10. Which of the following statements concerning Parvovirus B 19 is concerning Parvovirus B 19 is NOTNOT true?true?
DNA virusIncubation period 4-16 daysAlso called fifth diseaseAlso called fifth diseaseMainly affects young childrenThe majority of infections are
asymptomatic
11. Which of the following conditions has been 11. Which of the following conditions has been not been associated with parvoviral infection?not been associated with parvoviral infection?
GlomerulonephritisParotitisChronic fatigue syndromeChronic fatigue syndromeMeningitisPurpuric rash
12. Which one of the following statements 12. Which one of the following statements concerning parvovirus in pregnancy is trueconcerning parvovirus in pregnancy is true
Risk highest in the first trimesterIntrauterine death is commonLong term effects are commong1:1000 during pregnancyIgG+/IgM- maternal serology indicates
immunity
13. Which one of the following 13. Which one of the following statements is true in relation to HHVstatements is true in relation to HHV--6?6?
Causes fifth diseaseMost children acquire infection by age 2
yearsyearsAlso called exanthem subitumSeroprevalence is lowHigh mortality
14. Which one of the following conditions is 14. Which one of the following conditions is NOTNOT associated with congenital rubella? associated with congenital rubella?
ChorioretinitisIUGRDeafnessDeafnessPDAThrombocytopenia
6/01/2011
8
15. In a measles outbreak/contact, which of 15. In a measles outbreak/contact, which of the following measures is most appropriate?the following measures is most appropriate?
Infants age 9-12 months should be give one MMR vaccine that will cover for the 12 month immunisation
Measles immunoglobulin should be administered to all Measles immunoglobulin should be administered to all contacts
Exclude from school for 7 daysMMR vaccine should be given to susceptible if within
72 hours
16. Which of the following statements is 16. Which of the following statements is true concerning swine flu influenza?true concerning swine flu influenza?
High mortality in general populationVaccine associated with high risk of GBSInfluenza B virusInfluenza B virusOseltamavir is contraindicated in
pregnancyIncubation period 3-5 days
17. Which of the following statements is 17. Which of the following statements is NOTNOTtrue in relation to HIV infection?true in relation to HIV infection?
Untreated the chance of MTCT is 30%CMV is not an AIDS defining illnessInfected infants < 12 months should be Infected infants 12 months should be
treated based on VL and CD4 countHIV-infected mothers should not
breastfeedWith treatment in pregnancy rates of
transmission < 1%
18. 3 year old John was found by his mum with a syringe in his 18. 3 year old John was found by his mum with a syringe in his hand. He was crying and it appeared that there was a small hand. He was crying and it appeared that there was a small puncture wound to his hand. Which of the following is true puncture wound to his hand. Which of the following is true
concerning his risk of viral infection with Hep B, Hep C and HIV if concerning his risk of viral infection with Hep B, Hep C and HIV if there had been a significant exposure?there had been a significant exposure?
HIV 10%, Hep B 3%, Hep C, 30%, HIV 0.3%, Hep B 30%, Hep C 3%, p , pHIV 30%, Hep B 3%, Hep C 0.3%HIV 0.1%. Hep B 1%, Hep C 10%
19. Which of the following medications is most 19. Which of the following medications is most likely top be used to treat Hepatitis B likely top be used to treat Hepatitis B
infection?infection?
AcyclovirGanciclovirLamivudineLamivudineInterferon gammaVidarabine
20. Which of these situations concerning 20. Which of these situations concerning maternal HSV is associated with the greatest maternal HSV is associated with the greatest
risk to the baby?risk to the baby?
Mother has recurrent genital HSV-infection
Mother acquires infection with HSV-2 Mother acquires infection with HSV 2 having had HSV-1 (non-primary)
Mother has primary HSV-1 early in pregnancy
Mother has primary HSV-1 at 34 weeks
6/01/2011
9
21. Which is 21. Which is notnot a category of antia category of anti--retroviral retroviral medications?medications?
Nucleoside reverse transcriptase inhibitors
Non-nucleoside reverse transcriptase Non nucleoside reverse transcriptase inhibitors
Fusion inhibitorsCXCR4 antagonists
22. WHO recommends treating which of the 22. WHO recommends treating which of the following with HIV?following with HIV?
All infants less than 1 yr of ageOnly infants with CD4% <25Only infants with VL>100 000Only infants with VL>100,000No infants as they are at less risk
23. Which strain was responsible for the 23. Which strain was responsible for the swine flu pandemic?swine flu pandemic?
H3N2H5N1H1NIH1NIH2N3
24. Estimated number of confirmed 24. Estimated number of confirmed cases of swine flu in Australia in 2009?cases of swine flu in Australia in 2009?
404004000400040000
25. Estimated number of deaths due to swine 25. Estimated number of deaths due to swine flu in Australia in 2009flu in Australia in 2009
202002000200020000
Classification of virusesClassification of viruses
6/01/2011
10
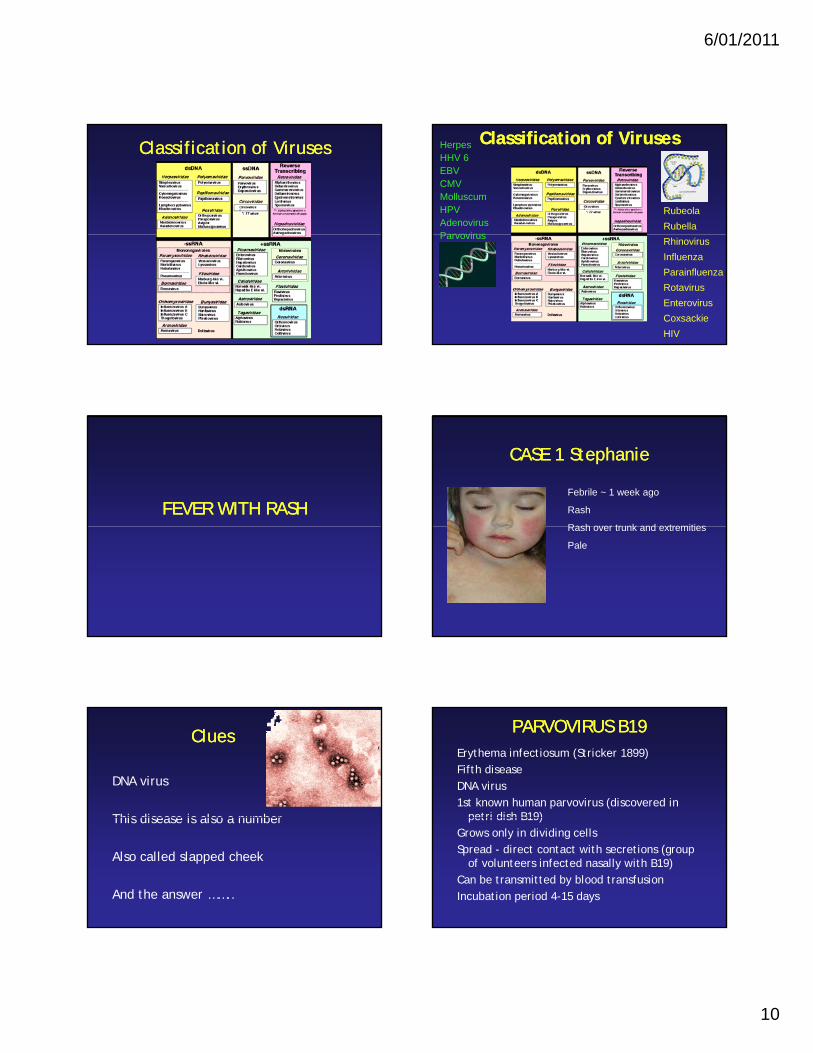
Classification of VirusesClassification of Viruses Classification of VirusesClassification of VirusesHerpesHHV 6EBVCMVMolluscumHPVAdenovirusParvovirus
RubeolaRubella
Parvovirus RhinovirusInfluenzaParainfluenzaRotavirusEnterovirusCoxsackieHIV
FEVER WITH RASHFEVER WITH RASH
CASE 1 StephanieCASE 1 Stephanie
Febrile ~ 1 week ago
Rash
Rash over trunk and extremitiesRash over trunk and extremities
Pale
CluesClues
DNA virus
This disease is also a numberThis disease is also a number
Also called slapped cheek
And the answer ……..
PARVOVIRUS B19PARVOVIRUS B19Erythema infectiosum (Stricker 1899)Fifth diseaseDNA virus1st known human parvovirus (discovered in
petri dish B19)petri dish B19)Grows only in dividing cellsSpread - direct contact with secretions (group
of volunteers infected nasally with B19)Can be transmitted by blood transfusionIncubation period 4-15 days
6/01/2011
11
PARVOVIRUS B19PARVOVIRUS B19Epidemic pattern similar to RubellaMost prevalent in winter and springVirus shedding between D 5 and D 12Attack rate highest in children 5 to 14 yrsS iti (I G)Seropositive (IgG)
2 to 21% of children < 11yrs40 to 60% adults
Pathophysiology and pathology– Direct effects (lysis)– Indirect (immune)
PARVOVIRUS B19PARVOVIRUS B19
IgM
Non specific fever
Virus excretion
Erythema infectiousum
0 7 14 21 28
Viraemia
Reticulocytes
B19 inhibits the formation of blast forming erythroid colonies
PARVOVIRUS B19 CLINICALPARVOVIRUS B19 CLINICAL
Spectrum20% asymptomaticUsual erythema infectiosumUsual erythema infectiosumUnusual clinical manifestations
Erythema InfectiosumErythema Infectiosum
Prodromal phase 2-3 days (viraemia)Symptom free for 7 daysD18- “slapped cheek”Facial exanthem worsens on going from
d outdoors to warm roomD 19-23 maculopapular rash on trunkHeadache in 20%Arthralgia (80% adults, <10% children)Knees, ankles, PIPJ, bilateralNo isolation
PARVOVIRUS RARE CLINICALPARVOVIRUS RARE CLINICALArthritis (association between B19
and RA)Neurological
– Encephalitis (B19 DNA CSF)– Meningitis– GB syndrome– Facial palsy– CT syndrome
Myocarditis (5 children and 4
• Other– GN– Kawasaki– Behcet– PAN– Wegener’s– HepatitisMyocarditis (5 children and 4
adults)Cutaneous
– EM– HSP– Petechiae
Haematological– TTP– Pancytopenia– Haemophagocytic– DB anaemia
– Hepatitis– SLE– Raynaud– Parotitis– Hepatitis– Pseudoappendicitis– CFS– Chronic haemolytic
anaemia
Stephanie comes back…..Stephanie comes back…..
Rash has gone…
But she is very pale…
WHY??
6/01/2011
12
PARVOVIRUS B19PARVOVIRUS B19
IgM
Non specific fever
Virus excretion
Aplastic crisis
Erythema infectiousum
0 7 14 21 28
Viraemia
Reticulocytes
B19 inhibits the formation of blast forming erythroid colonies
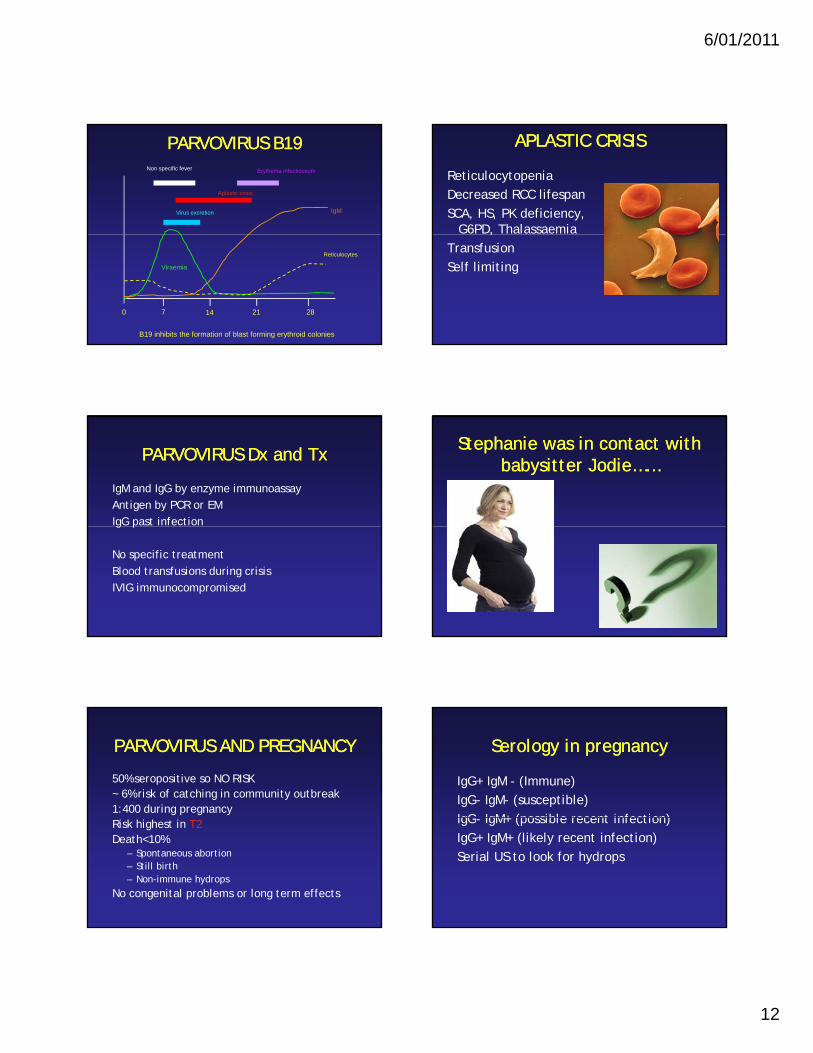
APLASTIC CRISISAPLASTIC CRISIS
ReticulocytopeniaDecreased RCC lifespanSCA, HS, PK deficiency,
G6PD, Thalassaemia,Transfusion Self limiting
PARVOVIRUS Dx and TxPARVOVIRUS Dx and Tx
IgM and IgG by enzyme immunoassayAntigen by PCR or EMIgG past infectiong p
No specific treatmentBlood transfusions during crisisIVIG immunocompromised
Stephanie was in contact with Stephanie was in contact with babysitter Jodie……babysitter Jodie……
PARVOVIRUS AND PREGNANCYPARVOVIRUS AND PREGNANCY
50% seropositive so NO RISK~ 6% risk of catching in community outbreak1:400 during pregnancyRisk highest in T2Death<10%
– Spontaneous abortion– Still birth– Non-immune hydrops
No congenital problems or long term effects
Serology in pregnancySerology in pregnancy
IgG+ IgM - (Immune)IgG- IgM- (susceptible)IgG IgM+ (possible recent infection)IgG- IgM+ (possible recent infection)IgG+ IgM+ (likely recent infection)Serial US to look for hydrops
6/01/2011
13
CASE 2 ELLACASE 2 ELLA12 monthsFever for 2 daysFebrile convulsionFeeding wellDevelops rash D4
HHV 6 Roseola InfantumHHV 6 Roseola Infantum
Herpesvirus1st description 1809 (Willan)Sixth diseaseSeroprevalence 80%Most acquire by 5 yrsVeeder (Exanthem subitum)“descriptive of the most striking clinical symptom, namely, the sudden,
unexpected appearance of a rash on the fourth day”
Roseola InfantumRoseola InfantumRare < 3/12 or > 4 yrsPeak 7-13 months (20% ED visits)90% within first 2 yearsHHV 6, HHV 7 and echovirus 16,
coxsackie, enterovirus
Roseola Infantum ClinicalRoseola Infantum Clinical
Fever for 3 - 5 daysRash for 1-2 days (Blanching)Usually well childUsually well childBeliner - palpebral oedemaWBC usually lowConvulsions (6-30%)
CLINICALCLINICALHHV 6 IMMUNOCOMPROMISEDHHV 6 IMMUNOCOMPROMISED
• IMMUNOCOMPROMISED– BM suppression– Interstitial
pneumonitis
• CNS– Aseptic meningitis– FC
pneumonitis– Renal dysfunction– Skin rash
– Meningitis– ? MS flares
6/01/2011
14
DIAGNOSISDIAGNOSIS
SerologyPCR (Quantitative)
Treatment– Ganciclovir– Foscarnet– Cidofovir
CASE 3 TomCASE 3 Tom
18 months2 days of feverPost auricular
adenopathyRash‘not himself’
CluesClues
RNA virusSpread by respiratory dropletsIncubation period of 14 21 daysIncubation period of 14-21 daysCauses problems in pregnancyOften called German measles
..Also called Bastard scarlatina….?
RUBELLARUBELLA
De Bergen and Orlow (German)1881 distinct disease RubellaGregg (Australian Opthalmologist) 1941gg ( p g )Congenital defects in babiesPandemic 1964Live attenuated Rubella vaccines 1969
RUBELLARUBELLA
TogavirusOnly one antigenic typePeriodic epidemics where vaccination coverage
i lis lowTransmission by NPProlonged contact requiredMaximal shedding 5 days prior to 6 days post
appearance of rashImmunity lifelong - Ab and CMI
RUBELLA CLINICALRUBELLA CLINICAL
Incubation period 14-21 daysMild prodrome in infants and childrenPrecede the rash by 1-5 daysy yRash first on face - hands - feetDisappeared by D325% subclinical infectionLeucopenia/neutropeniaNow more common in adolescents
6/01/2011
15
RUBELLA COMPLICATIONSRUBELLA COMPLICATIONSJoints
– Arthralgia/arthritis– Rare in children– Lasts ~ 9 days– ? Association with RA
Neurological– Encephalitis rare (only 6
Other– Thrombocytopenia– Purpura– Myocarditis– Testicular pain
Haemol tic anaemiap ( y
cases in 30,000 1964)– 2 to 4 days after rash– Numbness and tingling– SSPE like illness rare
– Haemolytic anaemia
RUBELLA DIAGNOSISRUBELLA DIAGNOSIS
Specific rubella IgMCan detect from salivaRise in titre (Study IgG in paired sera)Rise in titre (Study IgG in paired sera)
Jodie was also babysitting Jodie was also babysitting Tom!Tom!
AND SHE IS 12 WEEKS PREGNANT……….
CONGENITAL RUBELLACONGENITAL RUBELLA
In utero infection first 12 weeks
CONGENITAL RUBELLACONGENITAL RUBELLAGeneral
– IUGR (50-85%)– FTT– In utero death 10-30%
Eyes– Cataracts (30%)– Unilateral or bilateral– Retinopathy (35%)
Cardiovascular– PDA (30%)– PPBS (25%)– Pulm Art hypoplasia (25%)– AS (2-5%)– TOF (2-5%)– Myocarditis (10%)
Bone– Glaucoma (5%)
Auditory– Nerve deafness (80-90%)
Neurological– Mental retardation (10-20%)– Meningoencephalitis (10-20%)– Behaviour disorders (10-20%)
Bone– Radiolucencies (20%)
Haematological– Thrombocytopenia– HSM
CONGENITAL RUBELLA CONGENITAL RUBELLA DIAGNOSISDIAGNOSIS
Virus isolation– Nose, throat, urine, buffy coat of blood, CSF– Serology difficult to interpret– Rubella specific IgM– Compare maternal to infant (drop in IgG)– Late diagnosis can be made by avidity assays
Should babies be isolated?– Yes– Carers should be known IgG+– Can shed for up to 1 yr
6/01/2011
16
What do about Jodie?What do about Jodie?
URGENT serologyIgG+ (protected)IgG- (susceptible)Watch for symptomsWatch for symptomsNasal swabSerologyIf seroconversion risk of
infection highRepeat test? Immunoglobulin
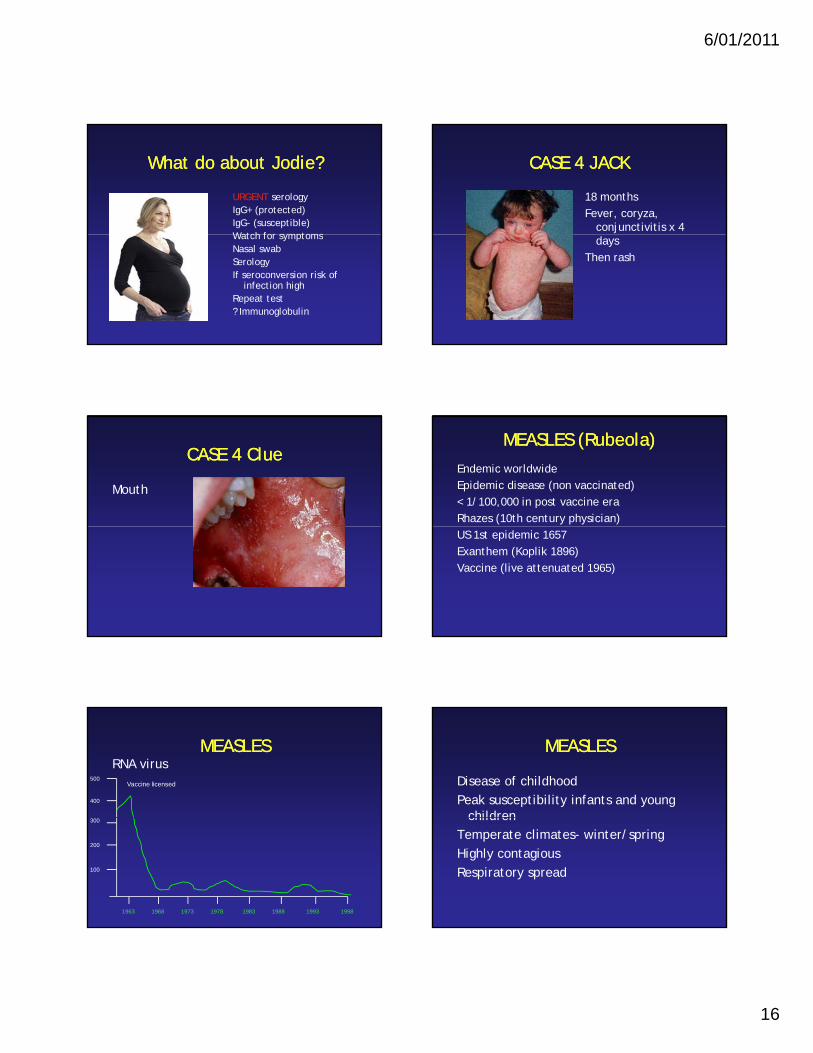
CASE 4 JACKCASE 4 JACK
18 monthsFever, coryza,
conjunctivitis x 4 days
Then rash
CASE 4 ClueCASE 4 Clue
Mouth
MEASLES (Rubeola)MEASLES (Rubeola)Endemic worldwideEpidemic disease (non vaccinated)< 1/100,000 in post vaccine eraRhazes (10th century physician)US 1st epidemic 1657Exanthem (Koplik 1896)Vaccine (live attenuated 1965)
MEASLESMEASLESRNA virus
500
400
Vaccine licensed
1963 1968 1973 1978 1983 1988 1993 1998
300
200
100
MEASLESMEASLES
Disease of childhoodPeak susceptibility infants and young
childrenchildrenTemperate climates- winter/springHighly contagiousRespiratory spread

6/01/2011
17
MEASLES CLINICALMEASLES CLINICAL
Incubation period 10 days
Prodrome lasts 2-3 days
Rash day 14From head to feetImmunity 14 days post
exposure
MEASLES CLINICALMEASLES CLINICAL
Respiratory– Common– Different appearance on
CXR– Secondary bacterial
Neurological– Abnormal EEG common– Encephalitis (1:1000)– Usually during exanthem– 25% sequelae
CSF (↑ ↑ i )y
infection– OM– LTB
Cardiac– Myocarditis– Pericarditis– ECG changes
– CSF (↑wcc, ↑protein)Others
– Black measles (haemorrhagic skin eruption)
– TP– SSPE (Dawson 1933)– 0.6/100,000– Mean incubation 7 years– Increase CSF IgG– 6-9 months until death
MEASLES MANAGEMENTMEASLES MANAGEMENT
No specific treatmentVitamin A (enhance IgG activity and total
lymphocyte numbers)100,000 IU 6/12 to 1 yr00,000 U 6 to y200,000 IU >1 yrIsolation until 5 days after rash (infectious
from prodrome)Vaccine may be used if within 72 hoursMeasles immunoglobulin
WHAT ABOUT THE CRECHE?WHAT ABOUT THE CRECHE?
Vaccinate (MMR)– Susceptible contacts if within 72 hours– Contacts 1 dose of MMR– Infants 9-12 months of age (second dose at 12 months)
M l I l b liMeasles Immunoglobulin– IM injection within 7 days of exposure– 0.2ml/kg (max 15 ml)– > 9 months if MMR contraindicated– Non immune pregnant women– Impaired immunity– Infants 6-9 months (followed 5 months later by MMR)
If no vaccine exclude from school for 14 days
AND CAN YOU BELIEVE IT…..AND CAN YOU BELIEVE IT…..
• Jodie picked up her son at the creche were Jack was
• Pregnancy– Premature labour– Still birth– Spontaneous abortion– Check serology– If negative give
immunoglobulin
RASHES WITH VESICLESRASHES WITH VESICLES
6/01/2011
18
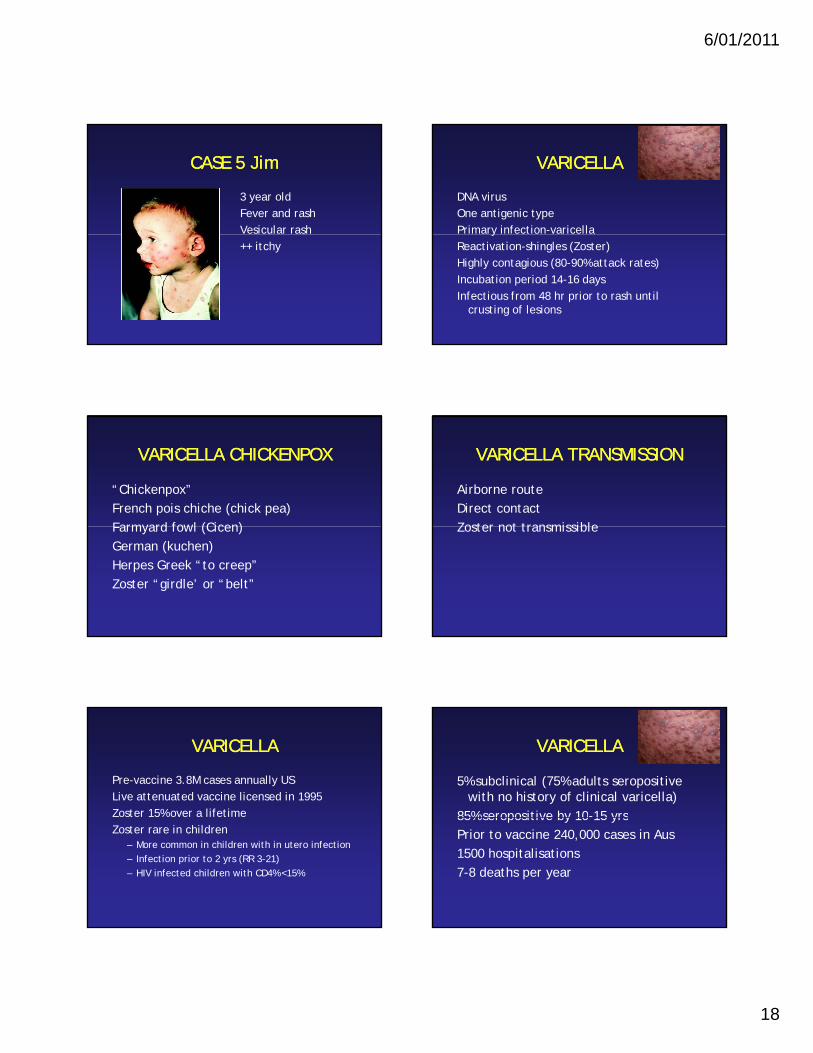
CASE 5 JimCASE 5 Jim
3 year oldFever and rashVesicular rash++ itchy
VARICELLAVARICELLA
DNA virusOne antigenic typePrimary infection-varicellayReactivation-shingles (Zoster)Highly contagious (80-90% attack rates)Incubation period 14-16 daysInfectious from 48 hr prior to rash until
crusting of lesions
VARICELLA CHICKENPOX VARICELLA CHICKENPOX
“Chickenpox”French pois chiche (chick pea)Farmyard fowl (Cicen)Farmyard fowl (Cicen)German (kuchen)Herpes Greek “to creep”Zoster “girdle’ or “belt”
VARICELLA TRANSMISSIONVARICELLA TRANSMISSION
Airborne routeDirect contactZoster not transmissibleZoster not transmissible
VARICELLA VARICELLA
Pre-vaccine 3.8M cases annually USLive attenuated vaccine licensed in 1995Zoster 15% over a lifetimeZoster rare in children
– More common in children with in utero infection– Infection prior to 2 yrs (RR 3-21)– HIV infected children with CD4% <15%
VARICELLAVARICELLA
5% subclinical (75% adults seropositive with no history of clinical varicella)
85% seropositive by 10-15 yrs85% seropositive by 10 15 yrsPrior to vaccine 240,000 cases in Aus1500 hospitalisations7-8 deaths per year
6/01/2011
19
VARICELLA CLINICALVARICELLA CLINICAL
200-500 skin lesionsMouth, conjunctivaLimited prodrome in childrenLimited prodrome in childrenMore likely in adults
VARICELLA COMPLICATIONSVARICELLA COMPLICATIONS
Bacterial superinfection– SA, GAS
CNS– Aseptic meningitis– Cerebellar ataxia– Transverse myelitis– Reye (aspirin use)
Arthritis, myocarditis, GNVaricella pneumonia in IC
ZOSTERZOSTER
Dermatomal distributionPainful in adultsPHNPHNIF/ Culture from skin lesions
TREATMENTTREATMENT
SupportiveAcyclovirIV acyclovirIV acyclovirFamciclovir
VARICELLA EXPOSUREVARICELLA EXPOSURE
Post exposure – Varicella vaccine within 72 hours but up to 5 days
Household contacts– Household contacts of those with impaired
immunity
Healthcare workers– If vaccinated watch for rash for 3 weeks– If unvaccinated or uncertain history (vaccine)– If does not want vaccination (reassign or place on
sick leave from D 10-21)
Zoster ImmunoglobulinZoster ImmunoglobulinPublic Health
– ZIG within 96 hours to pregnant women if susceptible
– ZIG to neonates whose mother develops VZV from 7 days prior to 2 days after deliveryZIG t t i th fi t 30 d if th – ZIG to neonates in the first 30 days if mother no history or negative serology
– Premature infants <28 weeks– IC where vaccine may be contraindicated
Dose– 0- 10 kg 200IU– 11-30 kg 400 IU– > 30 kg 600 IU
6/01/2011
20
VARICELLA VARICELLA IMMUNOCOMPROMISEDIMMUNOCOMPROMISED CMVCMV
DNA virusFirst described in 1881(Ribbert)Initially in salivary glands (Salivary gland Initially in salivary glands (Salivary gland
virus)60-70% seroprevalence
CMVCMV
CMV acquisition– Exposure in the home– SES– Daycare exposure– Prevalence rates of 20-50% in daycare
No seasonal variationMost common cause of congenital
infection
CMV TRANSMISSIONCMV TRANSMISSION
Direct person to person spreadIntimate contact with secretionsExcretion starts 4 6 weeks following Excretion starts 4-6 weeks following
infectionMay persist for years
CMV TRANSPLANTCMV TRANSPLANT
Primary, reinfection, reactivationD+/R-CMV pneumonitis BMT > renal> liver CMV pneumonitis BMT > renal> liver
patientsProphylaxis
CMV CLINICALCMV CLINICAL
>90% asymptomaticFever and malaise up to 4
weeksHeadacheMyalgias
OrganomegalyImmunocompromised
– Fever– Leucopenia
MyalgiasAbdominal painDiarrhoea
RashCMV pneumonia
– IC
– Transaminitis– Pneumonitis– Enterocolitis– Retinitis– Encephalitis– 1-4 months post transplant
6/01/2011
21
CMV POST TRANSPLANTCMV POST TRANSPLANT CMV DIAGNOSISCMV DIAGNOSIS
SerologyCMV IgG persists for lifeCaution in ICIgM interpretation
Biopsy – Tissue culture
PCRIgM interpretationRemove RFCMV IgM 6 weeks and may
persist for monthsAvidity
CMV antigenaemiaRegular monitoring in
IC
CMV TREATMENTCMV TREATMENT
Medications– Ganciclovir– Valganciclovir– Cidofovir
Prevention– CMV - blood– Hyperimmune globulin
Prophylactic anti viralsCidofovir– Foscarnet
IC– Induction (IV) and
maintenanceImmunoglobulinCMV Hyperimmune globulin
– Prophylactic anti-virals– Hygiene– Leucocyte depleted
blood– ? Vaccine– Viral surveillance
CMV pregnancyCMV pregnancy
• What are the options?
CMV PREGNANCYCMV PREGNANCY
Nigro et al 2008
CASE 7 JohnCASE 7 John
7 years old– Sore throat– Fatigue– Fever 2 weeks– Lymphadenopathy– Splenomegaly
– In his throat…
6/01/2011
22
CASE 7 JohnCASE 7 John
• 7 years old– Blood film
EBVEBV
Pfeiffer 1889“ Drusenfeiber” Glandular feverInitially suggestive of leukaemia1930s Paul and Bunnell (high heterophile abs in a 1930s Paul and Bunnell (high heterophile abs in a
medical student with EBV)1958 Dennis Burkitt (Epstein et al noted viral particles
similar to HSV - HHV 4)Serendipity 1968 Lab technician seroconverted with
EBV (6 days after getting symptoms)
EBVEBV
DNA virusEBV 1 and 2Lytic infection in oropharyngeal cellsy p y gInfects B cellsEstablished latency in B cells (1-50 /1,000,000)
EBM TRANSMISSIONEBM TRANSMISSION
Kissing diseaseEBV not transmitted efficientlyIncubation period 30 50 daysIncubation period 30-50 days
EBV CLINICALEBV CLINICAL
Acute Phase– Fever 1-2 weeks– Sore throat– Lymphadenopathy (W 2-4)– Tonsillopharyngitis (W 1)– Splenomegaly (50%)
Hepatomegaly (60%)
HLH– 1939– Fever– Pancytopenia– Splenomegaly– Haemophagocytosis– XLPD
Malignancy– Hepatomegaly (60%)– Rash
Resolution phase– 3-4 wks– Enlarged nodes 3-4 M– Severe fatigue– CFS no clear association
Malignancy– BL- African and PNG– Jaw>abdominal– HD
Complications– Rare– Neurological (1-5%)– ITP (20-50%)– Neutropenia– Cardiac– Respiratory (AO 1-5%)– Neck abscesses
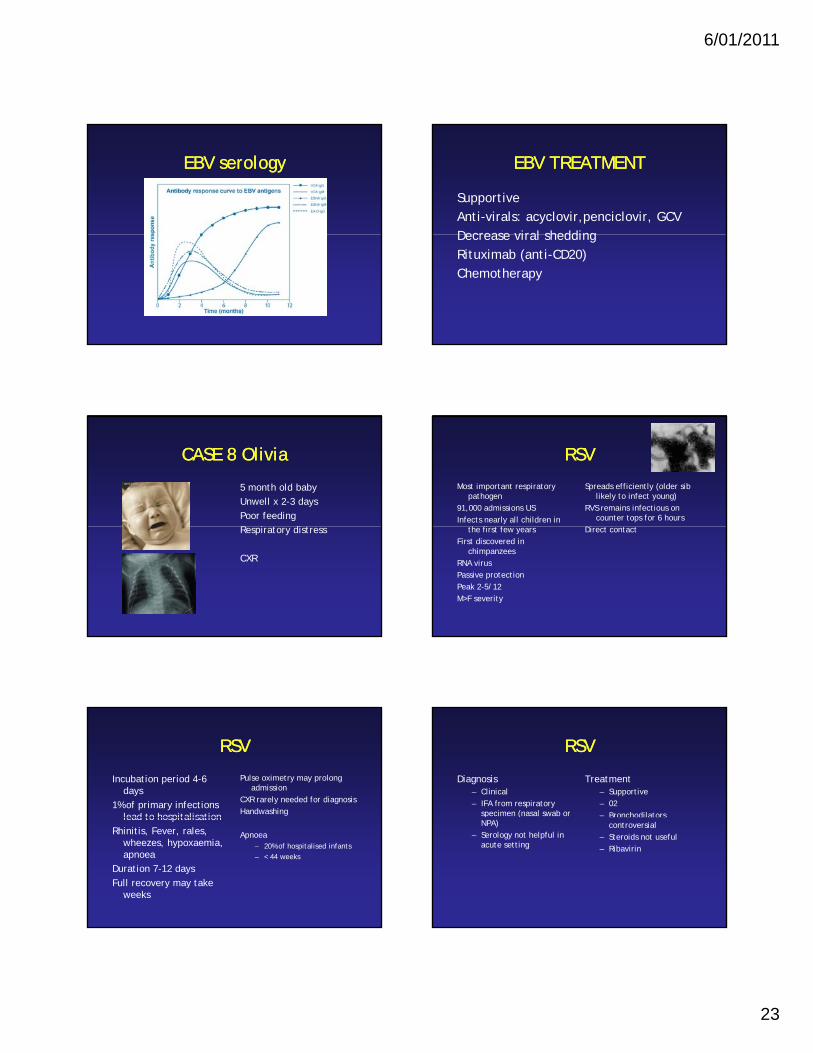
EBV DIAGNOSISEBV DIAGNOSIS
FBE + Film– Lymphocytosis– Atypical Lymphocytes– Low plts
Serology– IgM VCA– IgG VCA– EA antibodies
Heterophile abs– Agglutination of
sheep/horse RBCs– Rapid test (Monospot)– False positive and
negatives
EA antibodies– EBNA later
6/01/2011
23
EBV serologyEBV serology EBV TREATMENTEBV TREATMENT
SupportiveAnti-virals: acyclovir,penciclovir, GCVDecrease viral sheddingDecrease viral sheddingRituximab (anti-CD20)Chemotherapy
CASE 8 OliviaCASE 8 Olivia
5 month old babyUnwell x 2-3 daysPoor feedingR i diRespiratory distress
CXR
RSVRSV
Most important respiratory pathogen
91,000 admissions USInfects nearly all children in
Spreads efficiently (older sib likely to infect young)
RVS remains infectious on counter tops for 6 hours
the first few yearsFirst discovered in
chimpanzeesRNA virusPassive protectionPeak 2-5/12M>F severity
Direct contact
RSVRSV
Incubation period 4-6 days
1% of primary infections lead to hospitalisation
Pulse oximetry may prolong admission
CXR rarely needed for diagnosisHandwashinglead to hospitalisation
Rhinitis, Fever, rales, wheezes, hypoxaemia, apnoea
Duration 7-12 daysFull recovery may take
weeks
Apnoea– 20% of hospitalised infants – < 44 weeks
RSVRSV
Diagnosis– Clinical– IFA from respiratory
specimen (nasal swab or
Treatment– Supportive– 02– Bronchodilators
NPA)– Serology not helpful in
acute setting
Bronchodilators controversial
– Steroids not useful– Ribavirin
6/01/2011
24
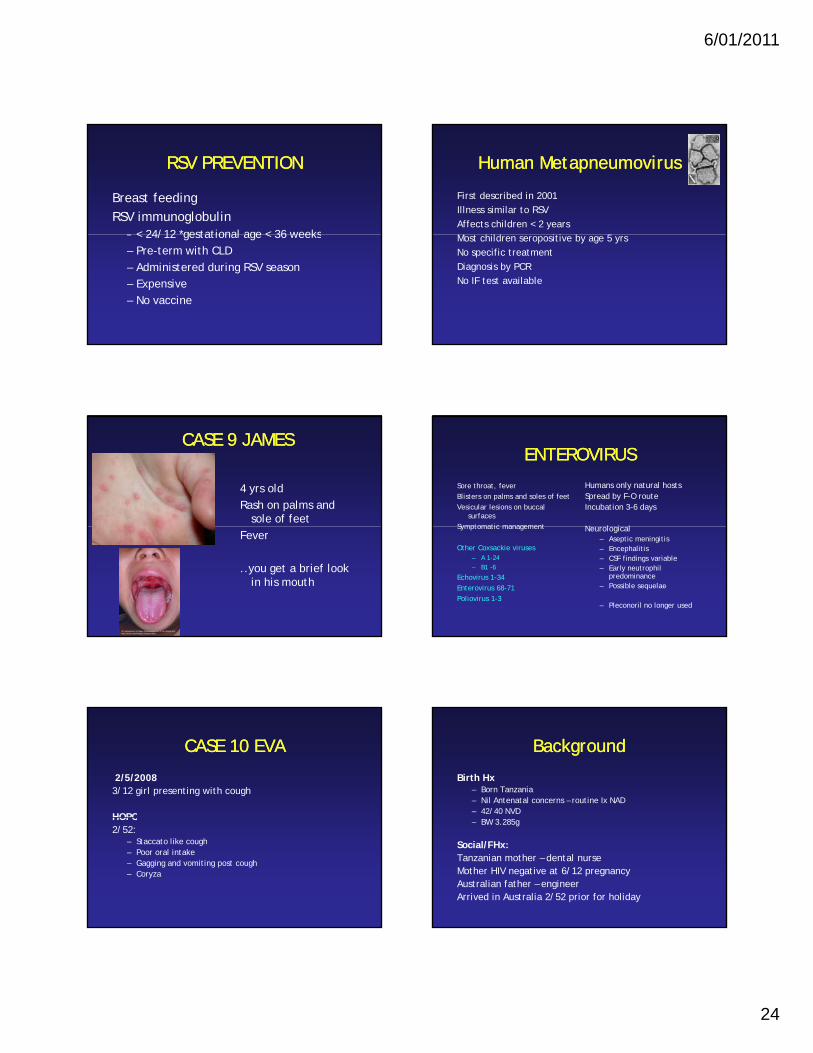
RSV PREVENTIONRSV PREVENTION
Breast feedingRSV immunoglobulin
– < 24/12 *gestational age < 36 weeks– < 24/12 gestational age < 36 weeks– Pre-term with CLD– Administered during RSV season– Expensive– No vaccine
Human MetapneumovirusHuman Metapneumovirus
First described in 2001Illness similar to RSVAffects children < 2 yearsM hild i i b 5 Most children seropositive by age 5 yrsNo specific treatmentDiagnosis by PCRNo IF test available
CASE 9 JAMESCASE 9 JAMES
4 yrs oldRash on palms and
sole of feetFever
..you get a brief look in his mouth
ENTEROVIRUSENTEROVIRUS
Sore throat, feverBlisters on palms and soles of feetVesicular lesions on buccal
surfacesSymptomatic management
Humans only natural hostsSpread by F-O routeIncubation 3-6 days
N l i lSymptomatic management
Other Coxsackie viruses– A 1-24– B1 -6
Echovirus 1-34Enterovirus 68-71Poliovirus 1-3
Neurological– Aseptic meningitis– Encephalitis– CSF findings variable– Early neutrophil
predominance– Possible sequelae
– Pleconoril no longer used
CASE 10 EVACASE 10 EVA
2/5/20083/12 girl presenting with cough
HOPCHOPC2/52:
– Staccato like cough– Poor oral intake– Gagging and vomiting post cough– Coryza
BackgroundBackground
Birth Hx– Born Tanzania– Nil Antenatal concerns – routine Ix NAD– 42/40 NVD– BW 3.285g
Social/FHx: Tanzanian mother – dental nurseMother HIV negative at 6/12 pregnancyAustralian father – engineer Arrived in Australia 2/52 prior for holiday
6/01/2011
25
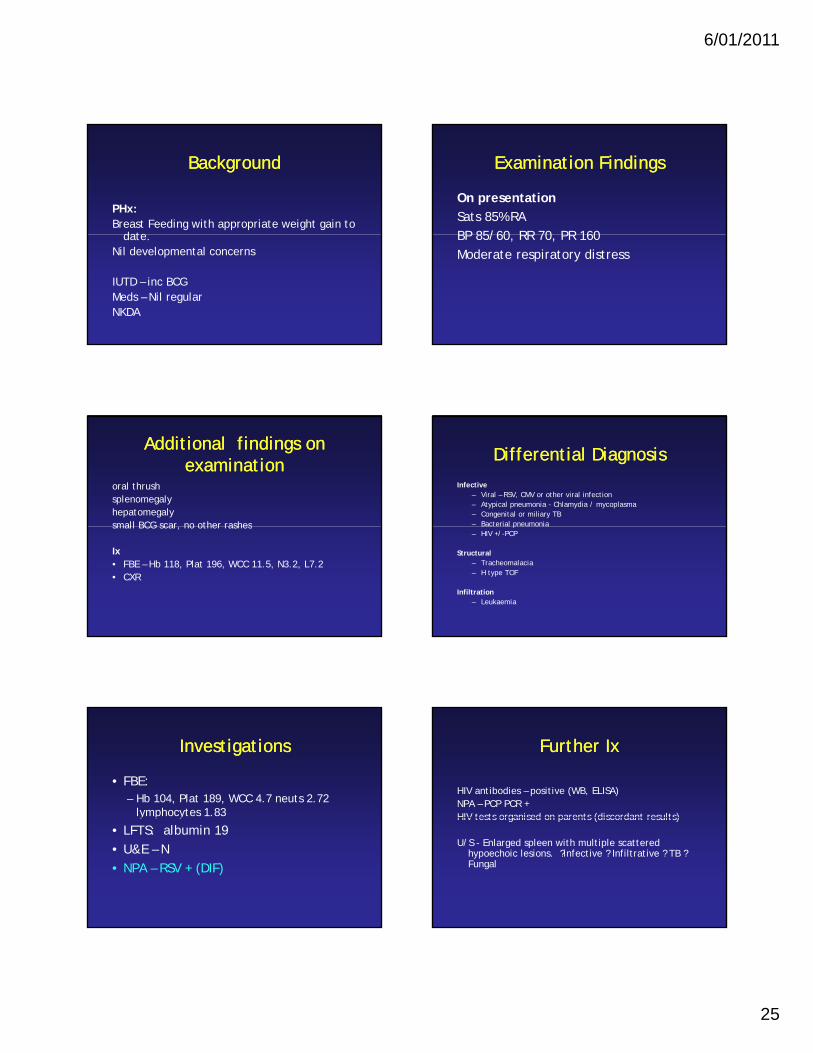
BackgroundBackground
PHx: Breast Feeding with appropriate weight gain to
date date. Nil developmental concerns
IUTD – inc BCGMeds – Nil regularNKDA
Examination FindingsExamination Findings
On presentationSats 85% RABP 85/60 RR 70 PR 160BP 85/60, RR 70, PR 160Moderate respiratory distress
Additional findings on Additional findings on examinationexamination
oral thrushsplenomegalyhepatomegaly small BCG scar no other rashessmall BCG scar, no other rashes
Ix• FBE – Hb 118, Plat 196, WCC 11.5, N3.2, L7.2• CXR
Differential DiagnosisDifferential DiagnosisInfective
– Viral – RSV, CMV or other viral infection– Atypical pneumonia - Chlamydia / mycoplasma– Congenital or miliary TB – Bacterial pneumoniaBacterial pneumonia– HIV +/-PCP
Structural– Tracheomalacia– H type TOF
Infiltration– Leukaemia
InvestigationsInvestigations
• FBE:– Hb 104, Plat 189, WCC 4.7 neuts 2.72
lymphocytes 1.83y p y
• LFTS: albumin 19• U&E – N• NPA – RSV + (DIF)
Further IxFurther Ix
HIV antibodies – positive (WB, ELISA)NPA – PCP PCR +HIV tests organised on parents (discordant results)HIV tests organised on parents (discordant results)
U/S - Enlarged spleen with multiple scattered hypoechoic lesions. ?infective ? Infiltrative ? TB ? Fungal

6/01/2011
26
Further InvestigationsFurther Investigations
HIV HIV RNA PCR - >750,000 copies/mlCD4 13% (absolute 237) (23-60)CD8 47% (14-25)
CMVNPA and urine culture +BAL culture +IgG Neg and IgM +CMV blood quantitative viral load 2x10^3 copies/mL (5/5)
Global view of HIV
Western & Central Europe
<100<100[[<100 –– <200]]
Middle East & North Africa46004600
Eastern Europe & Central Asia
3700 3700 [1700 [1700 –– 6000]6000]
South & South East
North America<<100
[<100 –– <200]East Asia
32003200[2100 [2100 –– 4500]4500]Caribbean
2300
Estimated number of children (<15 years) Estimated number of children (<15 years) newly infected with HIVnewly infected with HIV
46004600[2300 [2300 –– 7500]7500]
Sub-Saharan Africa390 000390 000
[210 000 [210 000 –– 570 000]570 000]
South & South-East Asia18 00018 000
[11 000 [11 000 –– 25 000]25 000]Oceania
<500<500[<500 –– <1000]
Latin America69006900
[4200 [4200 –– 9700]9700]
2300[1400 – 3400]
Total: 430 000 (240 000 – 610 000)An estimated 1200 children infected daily
HIVHIV
• Vertical transmission• 25-30% die by 1 yr• <1% infection rate in
developed countriesdeveloped countries• ART effective if can access• More resources• Diagnosis often too late
HIV virionHIV virion HIV life cycleHIV life cycle
6/01/2011
27
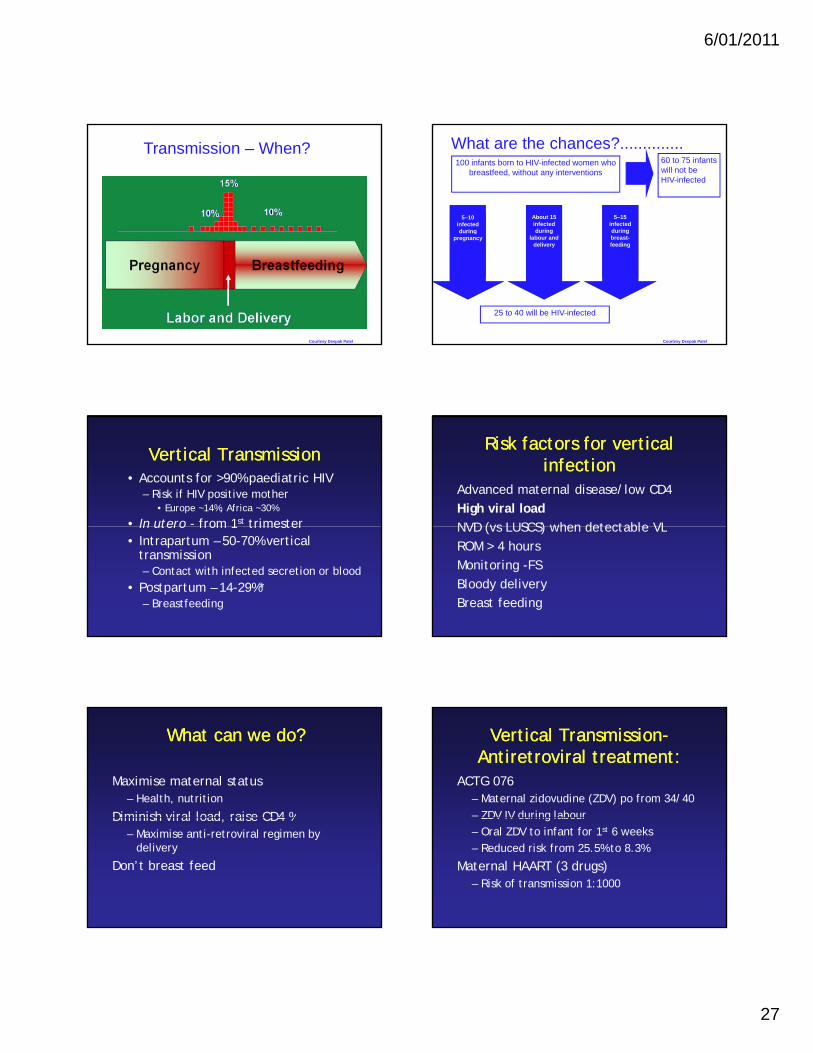
Transmission – When?
Courtesy Deepak Patel
100 infants born to HIV-infected women who breastfeed, without any interventions
60 to 75 infants will not be HIV-infected
5–10 infected during
About 15 infected during
5–15 infected during
What are the chances?..............
25 to 40 will be HIV-infected
pregnancy labour and delivery
breast-feeding
Courtesy Deepak Patel
Vertical TransmissionVertical Transmission• Accounts for >90% paediatric HIV
– Risk if HIV positive mother• Europe ~14%, Africa ~30%
• In utero - from 1st trimesterIn utero from 1 trimester• Intrapartum – 50-70% vertical
transmission– Contact with infected secretion or blood
• Postpartum – 14-29%*– Breastfeeding
Risk factors for vertical Risk factors for vertical infectioninfection
Advanced maternal disease/low CD4High viral loadNVD (vs LUSCS) when detectable VLNVD (vs LUSCS) when detectable VLROM > 4 hoursMonitoring -FSBloody deliveryBreast feeding
What can we do? What can we do?
Maximise maternal status– Health, nutrition
Diminish viral load raise CD4 %Diminish viral load, raise CD4 %– Maximise anti-retroviral regimen by
delivery
Don’t breast feed
Vertical TransmissionVertical Transmission--Antiretroviral treatment:Antiretroviral treatment:
ACTG 076– Maternal zidovudine (ZDV) po from 34/40– ZDV IV during labourZDV IV during labour– Oral ZDV to infant for 1st 6 weeks– Reduced risk from 25.5% to 8.3%
Maternal HAART (3 drugs)– Risk of transmission 1:1000
6/01/2011
28
Increasing number of HIV infected women delivering in Victoriadelivering in Victoria
Currently in past two years ~ 60 women
Service development in Melbourne-
Dr Michelle Giles (ID)Dr Olga Vugovic (ID)Dr Tom Connell (PID)Louise BordunDr Penelope Bryant (PID)Prof Richard Doherty (PID)Jane HowardKaren Blyth
Obstetrician
ID Physician GP
Paediatrician
Nurse specialists
PharmacistRWH
MMC
RCH
Prevention of Infection
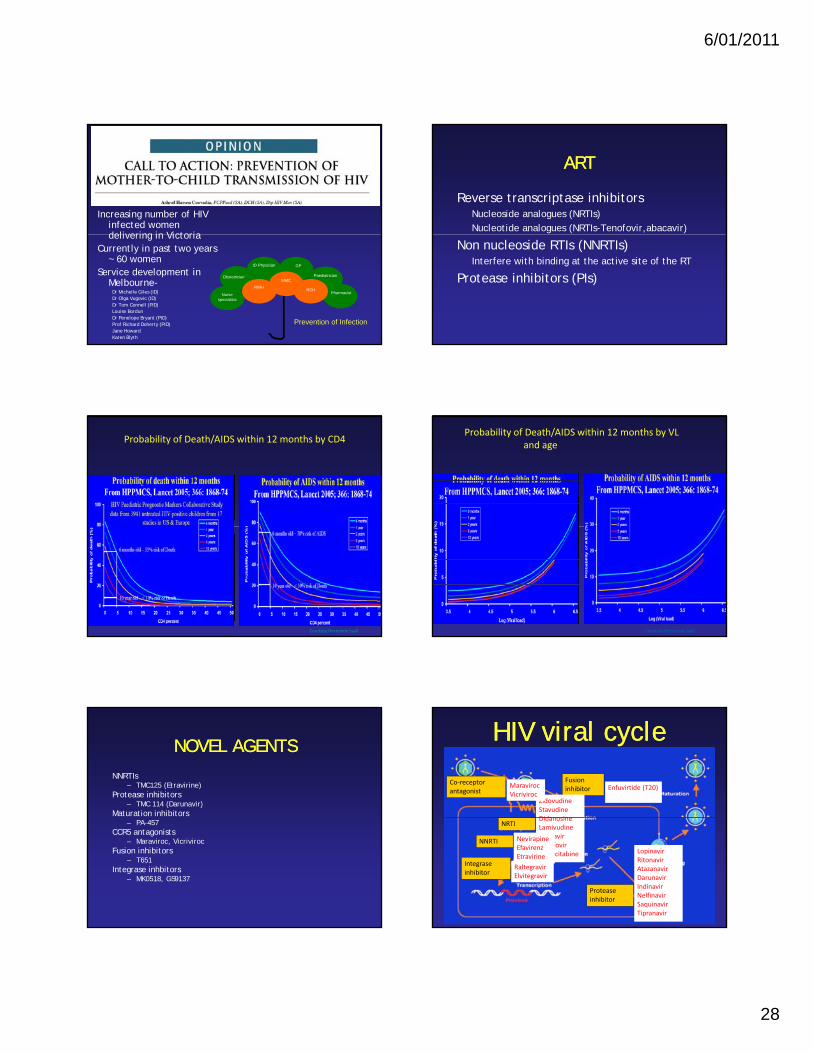
ARTART
Reverse transcriptase inhibitorsNucleoside analogues (NRTIs)Nucleotide analogues (NRTIs-Tenofovir,abacavir)
Non nucleoside RTIs (NNRTIs)Interfere with binding at the active site of the RT
Protease inhibitors (PIs)
Probability of Death/AIDS within 12 months by CD4
Courtesy Hermione Lyall
Probability of Death/AIDS within 12 months by VL and age
Courtesy Hermione Lyall
NOVEL AGENTSNOVEL AGENTSNNRTIs
– TMC125 (Etravirine)Protease inhibitors
– TMC 114 (Darunavir)Maturation inhibitors
– PA-457CCR5 antagonists
– Maraviroc, VicrivirocFusion inhibitors
– T651Integrase inhbitors
– MK0518, GS9137
HIV viral cycleHIV viral cycle
Co‐receptor antagonist
Fusion inhibitor
ZidovudineStavudineDidanosine
Enfuvirtide (T20)MaravirocVicriviroc
NRTI
NNRTI
Integrase inhibitor
Protease inhibitor
DidanosineLamivudineAbacavirTenofovirEmtricitabine
NevirapineEfavirenzEtravirine
LopinavirRitonavirAtazanavirDarunavirIndinavirNelfinavirSaquinavirTipranavir
RaltegravirElvitegravir
6/01/2011
29
ARTART
WHO 2008
Meds do not taste nice!
Vertical TransmissionVertical Transmission--management of newborn:management of newborn:
Diagnostic PCR:– 1st within 48 hrs pick up 38%– 2nd at 2-4 weeks pick up 93%– 3rd at 4 months pick up 99.7%p p
serology at 12-18 months
INFLUENZAINFLUENZA
“last greatest plague of man”Epidemic 412 BC300 000 hospitalisations annually300,000 hospitalisations annually8 influenza pandemics since 15801918 (20 M deaths worldwide)Orthomyxovirus
INFLUENZAINFLUENZA
RNA virusSurface glycoproteins Haemagluttinin
(HA)(HA)Neuraminadase (NA)
INFLUENZAINFLUENZA
Droplet spreadIncubation 1-7 daysViral shedding shorter for Influenza AViral shedding shorter for Influenza AHumoral and cell mediated immunityAnti HA - neutralisationAnti-NA- decrease severitySecretory IgA
6/01/2011
30
INFLUENZA CLINICALINFLUENZA CLINICAL
Clinical– Abrupt onset– Fever 2-3 days– Chills
Complications– Bacterial infections– Myositis– Encephalopathy
– Headache– Myalgia
PneumoniaGIT
– Abdominal pain– Anorexia
– Reye syndrome– Cardiac– Sudden death
TreatmentAmantadine (A)Inhaled zanamivir (A/B)Oseltamavir (A/B)
H1N1 swine flu H1N1 swine flu
• 40000 confirmed cases• Very infectious• High risk in pregnant women• High risk in pregnant women• 200 deaths• Vaccine