Embed Size (px)
Citation preview

Copyright 1998 byThe Cerontological Society of America
The CerontologistVol. 38, No. 1,101-112
Within the field of aging, the conceptualization and measurement of functioning has beendominated by the disability model. In this paper, one limitation of that model is described bycalling attention to a distinction between three "tenses" of functioning. Inadequate attention
has been paid to the distinction between the capacity to function in the abstract (hypotheticaltense) and actual performance in daily life (enacted tense). Failure to attend to this distinction
has obscured considerable discordance between what people say they are able to do instandard functional disability assessments, and what they actually do at home. To illustrate
this point, data from the MacArthur Studies of Successful Aging comparing the hypotheticalto the enacted tenses are presented. These data show a consistent pattern of discordance
between these two tenses.Key Words: Functional status, Theory, Successful aging
Conjugating the "Tenses" of Function:Discordance Among Hypothetical,Experimental, and Enacted Functionin Older Adults
Thomas A. Glass, PhD1
Substantial discordance can be observed be-tween the level of functioning older persons are ca-pable of (based on self-reports), and how activelyand independently they function in the "real"world. Recognition of this discordance has givenrise to the distinction between pathology, impair-ment, disability, and handicap featured in the WorldHealth Organization's taxonomy of functioning, theInternational Classification of Impairments, Disabil-ity, and Handicap (ICIDH) (World Health Organ-ization, 1980). This article argues that the WHO dis-tinction has not gone far enough in sensitizinggerontologists to the complexity of late life func-tioning. This has resulted in a gap in conceptualiza-tion and research due to the failure to differentiateamong three "tenses" of functioning (hypothetical,experimental, and enacted). This article presents amodel to elucidate the distinctions among thesetenses in an effort to fill this gap. Empirical evidenceof the existence of this phenomenon will also beprovided through a report on a data set which asksquestions of high-functioning elderly persons fromthe perspective of more than one tense.
The Dominance of the Disability ModelFor the past several decades, the predominant
The author would like to thank Drs. Rosalie A. Kane, Lisa F. Berkman,and Carlos Mendes de Leon for invaluable comments on an earlier draft.This work was supported by the Brookdale Foundation through the Brook-dale Fellowship Program. Send all correspondence to Dr. Thomas Class,Harvard School of Public Health, Department of Health and SocialBehavior, 677 Huntington Ave., Boston, MA 02115. E-mail: [email protected]
conceptual scheme for thinking about functioninghas been the disability model (Branch, Katz, Kniep-mann, & Papsidero, 1984; Clark, Stump, & Wolinsky,1997; Hubert, Bloch, & Fries, 1993; Jette, 1987; Jette,1994; Jette & Branch, 1985; Katz, Downs, Cash, &Grotz, 1970; Katz, Ford, Moskowitz, Jackson, & Jaffe,1963; Lawrence & Jette, 1996; Nagi, 1965; Pinsky,Branch, Jette, Haynes, Feinleib, Cornoni-Huntley, &Bailey, 1985; Verbrugge & Jette, 1994; Verbrugge,Lepkowski, & Konkol, 1991). An indication of the im-portance of this model is the fact that the term dis-ability has become nearly synonymous with the con-cept of functioning or functional status (McDowell& Newell, 1987). The disability model grew out of thework of Nagi in sociology (Nagi, 1965; Nagi, 1976;Nagi, 1991) and Katz and others in medicine (Katz etal., 1970; Katz et al., 1963) as an attempt to movebeyond the narrow focus on the presence or absenceof disease. Katz developed the activities of daily liv-ing (ADL) index to measure both the effectiveness oftreatments and the underlying mortality risk in frailelderly populations. That the ADL index would be-come synonymous with functioning was foretold inthe subtitle of Katz's first article, "The index of ADL:A standardized measure of biological and psychoso-cial function" (Katz et al., 1963). Today more thanfifty ADL scales have been developed and most, in-cluding the Katz and the Barthel Indices, werespecifically intended to measure functioning amonginstitutionalized patients (Mahoney & Barthel, 1965).
The disability model, as exemplified by the ICIDH,is pictured as a linear pathway leading from diseaseto handicap (in Nagi's framework) (see Appendix,
Vol. 38, No. 1,1998 101
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

DISEASE:
Instrinsicpathology ordisorder.
IMPAIRMENT:
Any loss orabnormality ofpsychological,physiological oranatomicalstructure orfunction.
— * DISABILITY:
Any restriction orlack of ability toperform anactivity in themanner or in therange considerednormal for ahuman being.
HANDICAP:
A disadvantageresulting from animpairment or adisability that limitsor prevents thefulfilment of anomal role(depending on age,sex, and social, andcultural factors) forindividuals.
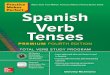
Figure 1. World Health Organization Typology of Health and Functioning: International Classification of Impairment, Disability, andHandicap (ICIDH).
Note 1). The emphasis is on the probabilistic ratherthan deterministic nature of those transitions (Fig-ure 1). The model begins with disease (pathology),which predisposes to impairment (loss of structureor function), which predisposes to disability (re-striction or lack of ability), and finally to handicap(disadvantage). Research which is informed by thedisability model shares the idea that functioningshould be understood in terms of functional capa-bilities in relation to the constraints placed on theindividual by the outside world. In both its conceptsand its measures, this model reflects an emphasison functional ability as a hypothetical construct,rather than actual performance in daily life. As anexample, in a recent test of the disability modelusing data from the Longitudinal Study of Aging,Lawrence and Jette (1996) excluded subjects whoreported that they did not engage in ADL activitiesbecause "it was not possible to determine if theywere abled or disable." This tendency to emphasizefunctional capability and to ignore functional per-formance reflects the history of the disability modelas grounded in studies of functional status amongolder patients in hospitals and nursing homes, farremoved from the real-world constraints which bothenable and dampen functional performance out-side of the institutional setting.
While the disability model continues to predomi-nate the research and policy arenas, several impor-tant criticisms of this model have emerged. Amongthese concerns is that it remains focused on a nar-row band of functioning, too closely linked to phys-ical function and the presence of disease. Numerousresearchers have sought to broaden the definitionof functioning beyond the limited scope of self-care(ADLs). First among the revisions was instrumentalactivities of daily living (IADL), developed in the1970s, which were designed to better capture do-mains of functioning among persons living in thecommunity through the addition of domestic main-tenance tasks (Lawton & Brody, 1969; Lawton, Moss,Fulcomer, & Kleban, 1982).
Motivated primarily by concerns over measure-ment problems, another group of researchers haveargued for performance-based measures of func-tioning (Curalnik, Branch, Cummings, & Curb, 1989;
Reuben, Valle, Hays, & Siu, 1995; Tinetti, 1986). Thesemeasures have sought to minimize the difficultiesarising from the use of self-reports, and are anattempt to move beyond the assessment of the hy-pothetical tense to which most standard self-reported ADL scales are limited. Yet, while the shiftto performance-based assessments has been an im-portant extension into the experimental tense, thishas not lead to a generalized interest in perfor-mance outside the laboratory.
Still others have called for a broadening of ourconcepts of function toward social functioning(Bortz, 1989; Jette & Branch, 1981). Verbrugge andJette (1994) have recently called for the inclusion ofhigher-level activities including social and leisureactivity, trips, child care, and recreation. Other inves-tigators have begun to examine productive activityas one dimension of higher-level functioning (Butler& Gleason, 1985; Class, Seeman, Herzog, Kahn, &Berkman, 1995; Herzog & House, 1991; Kahn, 1986;Myers, Manton, & Bacellar, 1986).
A second area of criticism of the disability modelhas been that the emphasis on capabilities and diffi-culties has the unintended effect of removing the in-dividual from the social and physical context in whichfunctioning actually takes place. In this way, the mea-surement of functional status has resulted in a de-contextualized view of functioning in older adults. Asa result, there has been a tendency to de-emphasizecompensatory strategies, work-arounds, and the vari-ous coping strategies employed by persons in theirhome settings. Feinstein, Josephy, and Well (1996) re-viewed forty three indices of functional disabilityconcluding that " . . . the most striking omission in in-dexes of disability is the absence of attention to thecollaborative role of the patient.... With uncommonexception, the roles of personal effort and externalsupport are constantly overlooked ..." (p. 414).
Conjugating the Tenses of Function:Enacted Function Explained
According to Webster's dictionary, to conjugate averb is to "recite or display all or some subsets ofthe inflected forms of a verb in a fixed order." Theconjugation of a verb describes the different forms
102 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

of action as they relate to the temporal context ofuse. In linguistics, distinctions are drawn betweenpast, present, and future forms of verbs. For thepurpose of this article, a different type of conjuga-tion is proposed in order to elucidate the meaningof functioning for the field of aging. For the pur-poses of this discussion, the idea of conjugation isnot used in its temporal meaning (past, present, andfuture). Rather, the idea of conjugation refers todifferent aspects of what might be termed "actionpotential." The three tenses described below mayeach exist in past, present, and future forms.
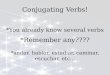
Figure 2 provides a typology of how the conceptof functioning might be conjugated in this manner.Traditional measures of functional status, as a con-sequence in part of the disability model, are primar-ily examples of the hypothetical tense. Subjects areasked a range of questions about whether they areable to perform tasks, how difficult those tasksmight be, and whether they require help from peo-ple or from assistive technologies. In each case, theresulting answer is the product of the respondent'sabstract calculus based, presumably, on that sub-ject's ability to average across situations and con-texts. This calculation is most often unmeasuredand unobserved.
The second tense might be called the experimen-tal tense in that instead of asking hypothetical ques-tions about presumed ability, respondents areasked to demonstrate functional capability in a clin-ical (or experimental) setting. In the experimentaltense, respondents are asked to simulate activitiesthat are thought to be representative of true func-
tioning. As has been observed, this approach hasthe advantage of offering direct observation of thesubject's ability and avoids some of the problems ofself-reports. However, while this tense may ade-quately describe what a person is able to do underthe inspection of the clinical examiner, it tells us lit-tle about the reality of that respondent's function-ing at home. The experimental tense refers, then, tothe demonstrated performance of what is hypothet-ically possible, albeit subject to the conditions andlimitations of the experimental setting.
A third tense, referred to here as the enactedtense, refers neither to hypothetical ability nor towhat the individual is able to perform under specialand circumscribed conditions. Instead, enacted func-tion refers to the functional performance realizedby an individual within the home context. Enactedfunction, whether physical, cognitive, emotional orsocial, refers to the end result of the confluence ofsituational and ecological factors which shape themoment to moment performance of functional tasksin the real world. As such, enacted function is a lowerlevel of abstraction. It requires no abstract calculusof what is possible, but requires instead the accuraterecollection of what has been or is now.
The central argument of this article is that withinthe field of aging, the study of functioning has fo-cused almost exclusively on just one tense. Wehave conceptualized functioning in terms of the in-dividual's capacity in the abstract, rather than whatthat individual is doing now or has actually done inthe past. Researchers have constructed tests whichassess the capability or difficulty of certain actions,
Hypothetical
'Can do...
IDefinition: capacity
Context: none
Measures:Self-report (orproxy)"Are you able to.. .""Any difficulty....""Do you requireassistance...""How difficult is itto.. . ."Q.O.L. items
Experimental Enacted
'Could do... 'Do do...
I IDefinition: capability
Context: labratory
Definition: performanceContext: home
I IMeasures:
Performance-basedtesting (orobservation)Timed performanceQualitativeassessmentTask completionStandardized testscores
Measures:Self-report, proxy, orobservationFrequency/durationof activity/role/taskProductive outputCalories expendedPhysiologicalmarkersOccupational status
Figure 2. Conceptual scheme for conjugating the tenses of functioning.
Vol. 38, No. 1,1998 103
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

but exclude the question of whether those actionsare actually performed. In short, a conceptual frame-work has emerged within gerontology based on thehypothetical rather than the enacted tense of func-tion. Further, the predominant measurement toolsin common use in the field reflect and are driven bythis framework.
The usefulness of this approach to conceptualiz-ing function is not to argue that any one perspec-tive is inherently superior to the others. In fact, thevery quality that makes one tense better suited toone application may be its weakness in another. Forexample, Guralnik and colleagues (1989) correctlyassert that one advantage of performance-basedmeasures (experimental tense) over ADL scales (hy-pothetical tense) is that the former are less influ-enced by "cognition, culture, language, and educa-tion." However, in another research context, thesesame factors may be of primary interest. If an inves-tigator wishes to research how factors such as lan-guage, culture, education, cognition, social support,or other host characteristics impact levels of func-tional performance, measures based on either thehypothetical or the experimental tense may be insuf-ficient. All three tenses may represent different andindependent ways in which individuals think aboutfunctioning. If that is true, gerontologists need todevelop parallel and complementary measurementtools to accommodate those perspectives.
To a large extent, these alternatives already exist.Any standard textbook on questionnaire design willinclude a discussion of how question constructionimpacts the resulting data that is generated (thiswas pointed out by an anonymous reviewer of anearlier draft of this paper). Research on functioning,as well as public policy, however, continues to relyalmost exclusively on the hypothetical tense. Onlyrecently have attempts to further elucidate the ex-perimental tense become widespread. Rarely hasthis led to extensive investigation of the enactedtense. The purpose of this article, moreover, is todraw out the importance of the distinction amongthe three, and to make a case for the importance ofthe enacted tense.
Emphasis on the hypothetical tense has producedconsiderable progress in the field. The ADL disabil-ity scales were designed to capture gross depar-tures from optimal functioning for purposes of pre-dicting those at increased risk for nursing homeadmission or death (Applegate, Blass, & Williams,1990). Most of these scales, including Katz, theBarthel index, and the original PULSES scales weredeveloped for use among hospitalized patients(Wagner, 1987). In the hospital setting, the hypo-thetical nature of these instruments is clearly moreappropriate; although as several commentators havenoted, the emphasis ought to shift to actual perfor-mance of functional tasks as the patient moves fromthe hospital to home (Fuhrer, 1987). As a predictor,rather than as an outcome, the disability indices arewell suited to this task.
Traditional disability scales also have advantagesfor public policy because they allow for the identifi-
cation of environmental barriers and impedimentsmore easily. As a basis for deciding who is eligiblefor health or social services, it may be best to ex-clude the contingencies of the home environment,or at least to minimize their influence as a way ofensuring equity in resource allocation. In this sense,asking subjects if they are able to perform a task inthe hypothetical allows us to separate, or to holdconstant, the complexity which arises from the in-troduction of the social, physical, and cultural con-texts that shape and modify actual performance.
A Graphical Representation of Two Tenses
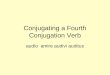
To further illustrate the importance of this distinc-tion, Figure 3 depicts a simple 2-by-2 table whichcontrasts the hypothetical tense (functional capac-ity), as measured by most commonly used ADLscales, with the enacted tense. Enacted functionrefers to the extent and quality of functional perfor-mance realized by an individual within a particularsocio-physical context. Individuals who fall on thediagonal (Types I and IV) may be said to be concor-dant between the hypothetical and enacted tensesof functioning. For these individuals, ADL scaleswould be valid and reliable measures of both func-tional capability and actual performance. The termactual performance here refers to functional perfor-mance within a naturalistic social setting, as con-trasted to performance achieved in a clinical settingor under experimental conditions.
Types II and III, on the other hand, represent asubstantial measurement challenge that has seldombeen explicitly addressed in aging research. Type IIindividuals enact high levels of functional perfor-mance despite significant difficulty, disability, or di-minished capacity. The reasons for this discordanceare many, and are not well understood. These indi-viduals might be thought of as "over-achievers" inthe sense that within the context of their home envi-ronment, they are functioning at a higher level thanthat which they are presumed to be capable. Type IIIindividuals, on the other hand, actually function at
Functional performance at home(Enacted "tense")
Low High
Type I
Lowfunctioning
Type III
Under-achievers
Type II
Over-achievers
Type IV
Highfunctioning
Low
Functional capacity(Hypothetical "tense")
High
Figure 3. Cross-classification of "hypothetical" and "enacted'tenses of functioning.
104 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

lower levels than would be predicted by ADL scales.Despite the absence of limiting factors such as dis-ease, impairments, or disability, these individuals donot actually perform the tasks about which they arebeing asked. These "under-achievers" may lead sed-entary, immobile lives, and potentially are quite de-pendent on others. Again, the reasons for this dis-cordance are numerous.
Evidence from Previous ResearchWhile a general awareness of this issue can be
seen throughout the literature on functioning, veryfew investigators have studied the problem directly.This author's own interest in this phenomenon wascatalyzed during qualitative interviews with survivingmembers of the New Haven EPESE cohort. Amongthem was a gentleman in his late 80s who reported ahigh level of ADL impairment, yet spent most of hisdays sailing his boat up and down the Connecticutriver. When asked about how he maintained theboat, he demonstrated how he would use duct-tapeto affix a paint brush to his cane to apply a new coatof paint to his boat every Spring. Equally commonwas the story of a woman in her 70s who reportedthat she was able to do everything for herself, whilemaintaining that all she really did was watch televi-sion all day while her 60 year old son with conges-tive heart failure "waited on her hand-and-foot."During these interviews, it became increasinglyclear that it is an error to assume that functional ca-pacity and performance are the same.
Several commentators have noted the lack ofstudies which investigate the reliability and validityof functional disability measures in general (Mc-Dowell & Newell, 1987). Beyond these general criti-cisms, a number of researchers have noted a differ-ence between functional capacity and performance(Hickey, 1980; Jette, 1994; Kelly-Hayes, Jette, Wolf,D'Agostino, & Odell, 1992; Patrick, Darby, Green,Horton, Locker, & Wiggins, 1981; Verbrugge & Jette,1994; Ziebland, Fitzpatrick, & jenkinson, 1993). Forexample, some evidence suggests that those who re-port impaired capacity in one or more domains aresimultaneously quite active and high-functioning inother domains which are assumed to require highdegrees of capacity. In a study of religious participa-tion among members of the New Haven EPESE co-hort, Idler (1987) concludes that " . . . functional dis-ability does not entirely determine behavior: 98 ofthe sample's 358 severely disabled women (who re-ported that they needed assistance in crossing aroom, feeding themselves, bathing, etc.) also reporta frequency of attendance at services of once aweek or more often." Miner, Logan, & Spitz (1993)also found that functional disability is unrelated tofrequency of attending senior centers. Findings fromthe Health Insurance Study (HIS) have shown thatsome subjects who report limitations in physicalactivity report no corresponding limitations in roleactivities (Stewart, Ware, & Brook, 1981). In eachcase, these findings were seen as anomalies, andwere not interpreted as signs of the weakness of amore general model of functioning.
In their influential study of the correlation amongself-reported, interviewer-administered, and perfor-mance-based testing of functional abilities, Reubenet al. (1995) found the relationships to be "inconsis-tent and weak, suggesting that these instrumentsare not measuring the same construct." It is pos-sible that differences between self-reports, inter-views, and performance testing reflect more thanmeasurement error. They may also reflect differ-ences in the meanings of different questions askedin various ways. Several investigators have shownthat subjects will tend to interpret questions aboutfunctioning in ways that are often different thanwhat researchers intend (Keller, Kovar, Jobe, &Branch, 1993), and that the same subjects within thesame disease group, who are given different disabil-ity questionnaires, will evidence substantially differ-ent levels of disability (Ziebland et al., 1993). Thesediscrepancies may also reflect the inherent unrelia-bility of asking questions in the hypothetical tense(Anderson, Bush, & Berry, 1989). They also reflect, inpart, differences in the "tacit models" (Ziebland etal., 1993) which underlie the construction of disabil-ity instruments.
The few studies that have examined multipletenses suggest that reduced function in the enactedtense may be more prevalent than is observed inthe hypothetical tense (Type III discordance). In arecent study, Kelly-Hayes et al. (1992) used Nagi'sdistinction between functional limitation (capacity)and disability (closest to enacted) to look at datafrom the Framingham study. Their findings suggestsubstantial discrepancies between the two and, inmost cases in which differences were observed, re-spondents reported a disability (enacted tense) andnot a functional limitation (hypothetical tense). Inaddition, they found that psychosocial factors weremore strongly associated with disabilities than theywere with limitations. This last finding is importantbecause it suggests that the impact of psychosocialfactors may be greater in determining the enactedrather than hypothetical tense of function. This ob-servation is supported by Mendes de Leon et al.(1996) who studied both the experimental tense(physical performance) and the hypothetical tense(ADL questions) over time and found the relation-ship to be mediated by self-efficacy.
In another study, Patrick et al. (1981) looked atdata from two community surveys of a London bor-ough and found considerable differences across thetwo waves based on what they termed "capacitywording" versus "performance wording" of theirdisability questions. In the study that used the per-formance wording (enacted tense), investigatorsfound as much as a two-fold increase in the preva-lence of disability, leading the authors to suggestthat studies based on capacity wording may sub-stantially under-estimate the true prevalence of dis-ability in populations. A similar conclusion wasreached by Anderson et al. (1989) who found that"capacity wording" of questions produced an under-reporting of dysfunction of at least 10%. Based onthe studies by Patrick, Kelly-Hayes, Anderson, and
Vol. 38, No. 1,1998 105
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

others, it is likely that discrepancies between thetwo tenses of function may be substantial, and thatreliance exclusively on instruments which assessonly the hypothetical tense may lead to biased esti-mates of disability rates as well as an underestima-tion of the importance of psychosocial factors inlate-life functioning.
Three Examples of Discordance: Data Fromthe MacArthur Studies of Successful Aging
We now turn to an empirical example that illus-trates the importance of what has been argued so far.In order to estimate the magnitude of discordancebetween reported capacity and actual functional per-formance, we would ideally choose data that weredrawn from a randomly chosen and community-based study of the elderly. We would hope to haveindicators of functional capacity and enacted func-tioning that would be sensitive to higher-level activ-ities as well as gross impairments and disability inthe physical domains. And, we would hope for mea-sures of both capacity and actual performance thatwere directly observed or performance based (onboth counts) rather than self-reports alone. Datathat meet all of these criteria are currently unavail-able. However, for the purpose of illustration, datafrom the MacArthur Studies of Successful Aginghave several important advantages. First, althoughnot intentional, the MacArthur battery asked twosets of questions about several domains of functionin both the hypothetical and enacted tenses. First,traditional functional disability questions wereasked about the extent to which the respondentfeels that they are able to accomplish a task. Then,much later in the interview, under items which arepart of a battery of productive activity questions,subjects were asked whether and how often thosesame tasks were actually performed. These datathen afford the opportunity to explore the extent ofdiscordance between the hypothetical and the en-acted tenses of functioning. It should be stressedthat while these data offer a rich opportunity to esti-mate the magnitude of concordance or discor-dance, the MacArthur study was not designed toinvestigate this question and there are several no-table limitations associated with these data. For ex-ample, both sets of questions are self-reports andare therefore subject to the problems associatedtherewith.
Aging researchers have begun to study produc-tive activities — or those activities which generategoods and services of economic value — as a markerof "successful" aging (Cutler & Danigelis, 1993;Class et al., 1995; Herzog, Antonucci, Jackson, Kahn,& Morgan, 1987). For the purpose of this study,questions about productive activity are good indica-tors of enacted functioning because they ask thefrequency and duration of routine activities as theywere actually performed. Productive activity is alsoan ideal indicator of global enacted functioning be-cause it represents high-level functioning which re-quires performance in the social, physical, and cog-nitive domains.
Methods
SubjectsThe data used in these analyses are from the
MacArthur Research Network on Successful AgingField Study, a longitudinal study of high func-tioning men and women aged 70-79. Details of thestudy design are available elsewhere (Berkman,Seeman, Blazer, Kahn, Mohs, Finch, Schneider, Cot-man, McClearn, Nesselroade, Featherman, Gar-mezy, McKhann, Brim, Pragar, & Rowe, 1993). Sub-jects were drawn from three sites of the EstablishedPopulations for the Epidemiologic Studies of the El-derly (EPESE): Durham, NC; East Boston, MA; andNew Haven, CT. Men and women aged 70-79 wereselected on the basis of physical and cognitive func-tion at the time of their 1988 EPESE interview. Age-eligible men and women (N = 4,030) were screenedon the basis of six criteria to identify a relatively"high functioning" cohort, representing approxi-mately the top third of their age peers in terms ofphysical and cognitive function. Of the 1,313 sub-jects who met all criteria, 1,192 (90.8%) agreed toparticipate and provided informed consent. Base-line data collection was completed between May1988 and December 1989 and included a ninetyminute, face-to-face interview covering detailed as-sessments of physical and cognitive performance aswell as information regarding health status. A threeyear follow-up interview was conducted in 1991.However, this study uses only data from the base-line interview.
For comparison purposes, a smaller subsample ofsubjects was interviewed at baseline (n = 163) whowere chosen to represent the middle and low ter-tiles of functioning using the same criteria. Thisgroup was chosen to permit comparisons with thehigh functioning subjects in order to determinethose physical and psychosocial factors that dis-criminate "successful" from "usual" patterns ofaging. The medium and low functioning groupswere not re-interviewed at follow-up.
MeasuresFeatures of the data collection and sampling stra-
tegies for the EPESE studies have been well de-scribed regarding sociodemographic characteristics(Cornoni-Huntley, Ostfeld, Taylor, Wallace, Blazer,Berkman, Evans, Kohout, Lemke, Scherr, & Korper,1993). Variables used in these analyses include age,sex, race, and marital status. Age was recorded as ofthe date of the subject's 1988 MacArthur interview,and is dichotomized in these analyses (0 = 70-74,1 = 75-79). Marital status is also dichotomized (1 ifmarried at baseline, 0 if not).
Our objective in this study was to cross-classifyindicators of functioning across two distinct tenses.To accomplish this goal within the limitations of theMacArthur data, three comparisons were madeusing data from questions both about hypotheticaland enacted tenses. Functional disability scales in-cluded in the MacArthur battery include a 7-item
106 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

measure of limitations in activities of daily living asdeveloped by Katz et al. (1970), a measure of grossmobility based on the work of Nagi (1976), anda self-reported measure of physical performance(Rosow & Breslau, 1966), all of which use wordingthat reflects the hypothetical tense. Among high-functioning respondents, there was no variance onthe Katz ADL index, and only limited variance onthe Nagi and Rosow-Breslau scales (see Appendix,Note 2).
First, we focused on two items from the Rosow-Breslau index which include: 1) "Are you able to doheavy housework like washing windows, walls, orfloors without help?" [coded yes, no, or refused];and 2) "Are you able to walk 1/2 mile without help?"[coded yes, no, and refused]. For the third compari-son, summary indices of potential versus enactedtenses were used, including self-reported limita-tions in ability to function in either the Nagi and theRosow-Breslau scales and a summary index of pro-ductive activities (enacted tense).
To measure enacted function, or the level offunctional performance as realized by each subjectin their home, 18 items from the productive activi-ties battery developed by the MacArthur SuccessfulAging network in conjunction with colleagues fromthe Americans Changing Lives study (Herzog, Kahn,Morgan, Jackson, & Antonucci, 1989). For our firsttwo comparisons, individual items from the produc-tive activity battery which paralleled items from theRosow-Breslau scale were used, including questionswhich asked "Do you currently do any heavy house-work?" and "Do you walk at least 1/2 city block perday?" [both items coded yes, no, refuses, don'tknow]. For the third comparison, a summary indexof productive activities developed in an earlierstudy was used (Glass et al., 1995). This scale com-bines information on five dimensions of productiveactivity chosen to represent the activities commonlyengaged in by older people which produce eco-nomic goods or services including: 1) housework, 2)yard work, 3) child care, 4) paid work, and 5) volun-teer work. In the present study, the summary indexwas divided into tertiles for the high-functioninggroup, as well as the medium- to low-fuctioningcomparison group.
pothetical and enacted function are presented inTables 2, 3, and 4. In Table 2, the ability to performheavy housework is cross-tabulated with the actualperformance of heavy housework. Note that thedata are presented for the high-functioning group(HF) and the medium- to low-functioning group(MLF) separately. Only 6% of the HF group say theyare not able to do heavy housework. Of that group,
Table 1. Comparison of "Successful" and "Usual" Agerson Demographic Features: Means, Frequencies and Percentages
with Statistical Tests of Difference"
Variable
SexMenWomen
Race (non-white)MenWomen
Marital Status(% married)
MenWomen
AgeMen.Women
Education (highestcompleted)
MenWomen
Income (categorical)MenWomen
Cognitive Status(Pfeiffer)
MenWomen
Index of ProductiveActivity
Highfunctioning(N = 1191)
531 (45%)661 (55%)
228 (19%)92(17.3%)
136 (20.6%)
564 (47.4%)367 (69.2%)197 (29.9%)
74.374.174.4
10.610.710.6
13.713.414.0
8.28.28.1
6.7
Mid-lowfunctioning
(n = 162)
73 (45%)89 (55%)
55 (34%)21 (29%)34 (38%)
62 (38.3%)46 (63.0%)16(18.0%)
75.075.075.1
9.810.88.9
15.715.116.2
7.37.47.3
4.8
Test"
n.a.n.a.
19.05.52
14.0
4.771.165.43
3.292.462.21
-0.990.10
^.93
0.780.480.68
-6.67^.23-5.17
Sig.
.000
.019
.001
.029
.283
.020
.001
.014
.028
.321
.921
.000
.439
.633
.498
.000
.000
.000
"Means presented for continuous variables, frequencies, andpercents for categorical variables.
T-tests are shown for continuous variables and chi-squaretests for categorical variables.
Results
Table 1 shows the socioeconomic and selectedfunctional characteristics of the two in total as wellas by gender. In comparing the high-functioningsample (labeled successful agers in the MacArthurstudy) to the medium- to low-functioning group(usual agers), the high-functioning group, as ex-pected, is younger, less likely to be of minority de-scent and less cognitively impaired. With the ex-ception of a difference in education among women,the two groups are not notably different in educa-tion or income. Among the high-functioning group,women were more likely to be married. In bothgroups, just over half (55%) of the sample is female.
The results of the three comparisons between hy-
Table 2. Discordance Between Hypotheticaland Enacted Functioning: Heavy Housework (1988)*
Do you do any heavy housework?
No Yes Totals
Type I Type 11
Are you able to doheavy housework?
No
Yes
highs 40% highs 60% 73 (6%)lows 56% lows 38% 84(52%)
Type Type IV
highs 07% highs 93% 1110(94%)lows 23% lows 77% 78(48%)
"MacArthur Studies of Successful Aging, 1988 (Highs = 1,183,Medium-Lows = 162).
Vol. 38, No. 1,1998 107
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Table 3. Discordance Between Hypotheticaland Enacted Functioning: Walking City Blocks (1988)'
Do you walk at least 1/2of a city block per day?
No Yes Totals
Type I Type II
No highs 35% highs 65% 37 (3%)Are you able to walk lows 60% lows 40% 52(33%)1/2 mile without help?
Type III Type IV
Yes highs 15% highs 85% 1104(97%)lows 24% lows 51% 104(67%)
Approximately one-third of the sample of bothhigh- and low-functioning groups report hypotheti-cal and enacted tenses which are consistent withone another. Again, however, our focus is on theoff-diagonal cells of the Table. Among those HFwho report 1-2 functional limitations, nearly onethird (27%) performed in the highest tertile of pro-ductive activity. Similarly, among those with no limi-tations, 30% are in the lowest tertile of productivity.Among medium- to low-functioning respondents,31% are in the highest tertile of productivity despitereporting three or more functional limitations. Fi-nally, 28% of those with no limitations are amongthe least productive subjects.
Table 4. Discordance Between Hypotheticaland Enacted Function: Disability and Productive Activity
Tertile of Productive Activity?
Low Medium High Totals
3+ highs n.a. highs n.a. highs n.a. n.a.lows 32% lows 37% lows 31% 78(48%)
Anyfunctional 1-2 highs 41% highs 32% highs 27% 304(26%)limitations lows 41% lows 27% lows 32% 44(27%)
0 highs 30% highs 33% highs 36% 888 (75%)lows 28% lows 30% lows 43% 40(25%)
Note. Percentages do not add to 100 due to rounding.
however, 60% report later in the questionnaire thatthey do perform heavy housework. Among the MLFgroup, just over half say they are not able to doheavy housework, while 38% of that group reportsthat they do heavy housework. Conversely, amongthose who said that they were able to do heavyhousework, 7% of the HF group and 23% of the MLFgroup reported that they, in fact, did not do anyheavy housework.
Table 3 presents results of a similar analysis forwalking. In this case, the wording of the two ques-tions was not exactly the same. Here we contrastthose who said they were or were not able to walkone-half mile without help, with those who walk atleast one-half city block per day. Among the HFgroup, only 3% said they were not able to walk one-half mile without help. Among that group of 37 re-spondents, 65% said they walk one-half city blockper day. Among the MLF group, 40% of those whosaid they are not able to walk one-half mile, re-ported that they did walk at least one-half city blockeach day. Among those who said they are able towalk one-half mile, nearly one-quarter walk lessthan one-half city block per day.
Finally, Table 4 presents a similar analysis whichlooks at any self-reported impairment in the hypo-thetical tense with a summary index of enactedfunction. We contrast those who report 0 versus 1-2versus 3 or more functional limitations (Nagi orRosow-Breslau), with the index of productive activi-ties broken into tertiles. In first looking at the diago-nal cells of the Table, a consistent pattern is visible.
Discussion
The purpose of presenting these data has been tocall attention to the possibility of substantial dis-cordance between answers to questions about func-tional capacity and actual performance in the homecontext. A thorough and comprehensive examina-tion of this discordance is beyond the scope of thesedata and this study. These data are clearly not with-out limits. However, although others have pointedout the importance of question design in studies offunctional status (Anderson, Bush, & Berry, 1989;Hickey, 1980; Kovar, 1991; Robine, Michel, & Branch,1992), few investigators have taken seriously the ideathat functional performance may be as important asfunctional capacity. In the absence of better data,these analyses suggest a relatively consistent picture.Across multiple comparisons, the degree of discor-dance between hypothetical and enacted tenses offunction appears to be between the range of 25%and 35%. That is, many older persons appear to beboth overachieving and underachieving in theirfunctional performance relative to self-reports offunctional capacity as measured by standard in-dices. This discordance appears to be relativelysymmetrical in that the magnitude of overachievingroughly matches the magnitude of underachieving.This suggests that failure to include separate assess-ments of performance may lead to considerablemisclassification and measurement error.
Why Does This Matter?
Is the distinction between hypothetical, experi-mental, and enacted tenses simply a linguistic trick,or are the implications of this argument important?Is there anything here beyond simple measurementerror? In the remainder of this discussion, eight rea-sons for the significance and importance of thisphenomenon are presented.
Missing Information. — Social and behavioral sci-entists have increasingly moved toward a broaderand richer conception of aging. The new themeshave been heterogeneity, fluidity, adaptation, modi-fiability, and "successful aging" (Berkman, 1988;Maddox, 1987; Rowe & Kahn, 1987). From large-scaleepidemiological data sets, much has been learned
108 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

about the plasticity of human aging. Old notions ofaging as an inevitable process of decline and lossof capacity are being replaced. Many of these ideasconfirm and reiterate the conventional wisdom thatas we age, the mind matters. Regrettably, the devel-opment of new multidimensional instruments forthe assessment of global functioning in all its facetshas lagged behind. Instead, aging researchers haverelied on measures designed in the 1960s largely forclinical purposes, which are based almost exclu-sively on the hypothetical tense. Designed to cap-ture the physiological substrata underlying func-tional status, these instruments have been lesssuccessful at capturing how elderly people are actu-ally functioning in their daily lives. As a result, a rig-orous assessment and subsequent investigation ofthe contribution of psychosocial factors to function-ing has been lacking. A new sensitivity to the impor-tance of multiple tenses of functioning is needed aswell as new and innovative tools for disaggregatingthose tenses.
Will the Real Disability Please Stand Up? - It iswidely recognized that the definition and measure-ment of disability has a profound impact on therates of disability observed in a given population.For example, Jette (1994) shows that wording basedon "difficulty" as opposed to the need for "humanassistance" resulted in disability estimates that were1.2 to 5 times greater. Given the importance ofwording, it may be especially important to measureactual performance of self-care tasks independentlyof difficulties and help, both human and non-human.And while some studies clearly focus appropriatelyon the identification of impairments at the hypo-thetical tense, it may be equally important to beginto recognize that what really matters most, both inrelation to quality of life, and as a true marker of un-derlying risk of poor outcome, is not what peoplecan do, but what they do do.
Evaluation of Interventions: A Better Mousetrap.— The main goal of health interventions is the opti-mization or restoration of the actual, functional per-formance of life activities. As Kane and Kane (1987)observe, "If long-term care is directed at improvingor maintaining functioning, then its success can bemeasured by functional outcomes" (p. 107). Yet, ourevaluation tools often pertain only to whether helpis needed, not whether it is received; whether diffi-culties are encountered, not whether they are over-come; and whether performance is possible, notwhether it is achieved. By definition, outcome mea-sures which tap into performance will be more ap-propriate and definitive than those that ask onlyabout the hypothetical ability to function. The re-verse is also true. As observed by Anderson et al.(1989), "Treatment programs should not take credit(and resources) for restoring function that does notexist." (p. 15). Interventions which do not translatereductions in capacity into corresponding incre-ments in performance are clearly less effective thanthose that do.
In addition, interventions targeted at the enactedtense may require different strategies and ap-proaches. As the work of Mendes de Leon and othershave shown (Mendes de Leon, Fillenbaum, Williams,Brock, Beckett, & Berkman, 1995), attention to issuessuch as self-efficacy may be necessary in order totranslate the benefits of increased capacity into theultimate goal of increased function as realized in theresidential context.
The Underestimation of Life-Context — In addi-tion to the survey data shown here, this research isbased on in-depth interviews conducted by the au-thor in an effort to determine the meanings of vari-ous types of questions about functioning and theirrelation to quality of life in late life. As a conse-quence of this qualitative work, it became increas-ingly clear that functional performance is substan-tially shaped by the social and cultural context ofthe home-world and that functioning cannot be un-derstood in the absence of that context (Class, 1991;Keith, 1985,1988). However, because aging researchhas relied so heavily on large-scale survey studiesthat include little information about that social con-text data, it is perhaps not surprising that the fieldhas tended to underestimate its importance (Kasl,1995). By integrating qualitative data collected innaturalistic settings with large scale survey data, alevel of richness and insight can be achieved whichis lacking when either type of data is examinedalone. In many interviews, subjects answered ques-tions about the hypothetical tense, then gave muchdifferent answers when asked to describe what theyactually did. There exists a need for more qualitativestudies of functioning in the real world which ex-plore explicitly the different tenses of function andhow discrepancies are understood as meaningful byolder persons.
Compensatory Strategies. — Aging specialists havelong recognized that older persons cope differ-ently, and vary in their use of compensatory strate-gies and technologies in dealing with the challengesof late life. The concept of compensation is particu-larly important for identifying factors which helpdisabled persons overcome those challenges andavoid the handicaps that can result. Forms of com-pensation might include substitution of goals, slowertimetables, help from equipment or from others,environmental modification, avoidance of hazard,or even greater effort. The concept of compensa-tion is appealing if for no other reason than it caststhe disabled person in a heroic light. However, tothe extent that enacted function is not measured in-dependently of the hypothetical tense, it becomesnearly impossible to fully explore the impact of thesecompensatory strategies. It may be argued that thediscordance observed in these data represents littlemore than the effects of these various strategies(i.e., help from people or specialized equipment).Certainly the need to perform productive activitiesdepends on more than the ability to do so, but alsoon the need to produce as dictated by one's socioe-
Vol. 38, No. 1,1998 109
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

conomic resources. It is possible that the failure tomeasure the two tenses separately has led to a sys-tematic myopia, whereby the real importance andsignificance of those types of help may be substan-tially underestimated.
Determinants of Under and Over Achievement. —It is not a novel observation that some elders seemto overcome seemingly extraordinary challenges,while others appear to be devastated by only minordisabilities (Hickey, 1980). This observation should beobvious and compelling to clinicians, as it is to any-one who has known a "super" grandparent. How-ever, the disability model, which ends with handicap,leaves off prior to the endpoint of actual perfor-mance within broad fuctional domains. As such, wecurrently lack the tools, both methodologically andconceptually, to study those factors most closely as-sociated with these two discordant types. What arethe factors that are associated with overcoming im-pairments among those living in the community?What are the factors which are associated with lowlevels of enacted function, despite the relative ab-sence of disease or disability? This may be an espe-cially important risk group as is indicated by studiesshowing the deleterious consequences of inactivity(Hartley, 1985; Kannel, Belanger, D'Agostino, & Israel,1986; Kiely, Wolf, Cupples, Beiser, & Kannel, 1994; Lee& Markides, 1990; Leon, 1985; Paffenbarger, Hyde,Wing, & Hsieh, 1986; Simonsick, Lafferty, Phillips,Mendes, Kasl, Seeman, Fillenbaum, Hebert, & Lemke,1993). By developing new tools for the assessment ofenacted function, the capability to address thesequestions will be substantially enhanced.
Differential Discordance Across Age Categories.— There is evidence that the discrepancies betweenhypothetical and enacted tenses may be greater inolder people than in younger people. That is, mea-sures based on the hypothetical tense alone maybe especially poor markers of actual functioning inolder populations, therefore leading to unwarrantedconclusions about the prevalence of dysfunction. Forexample, in a study of stroke recovery Ferrucci andhis colleagues (Ferrucci, Bandinelli, Guralnik, Lam-poni, Berttini, Falchini, & Baroni, 1993) looked at therelation between motor impairment (an index offunctional capability as it relates to the stroke's sever-ity) and functional performance (measured using theBarthel Index of ADL). Their findings, based on aprospective study of 50 first-time stroke survivors,show that motor impairment predicts most of therecovery that is observed among younger people(<65), while older subjects were "more likely to em-ploy compensatory strategies to overcome some ofthe neural impairment that remains after stroke" (p.200). Older persons kept pace with the recovery ofyounger persons in terms of enacted function, de-spite demonstrating significantly less improvementat the motor level. Studies such as this one suggestthat the need to look at enacted and hypotheticalfunction independently may be more acute amongthe oldest old.
A Strategy for Measuring Successful Aging. — Re-search in aging over the last decade has emphasizedpopulation heterogeneity and a widening of thescope of factors thought to determine functioning(Maddox, 1979, 1987). The distinction between "suc-cessful," "normal," and "pathological" patterns ofaging is now widely recognized (Baltes & Baltes, 1990;Berkman, 1988; Roos & Havens, 1981; Rowe & Kahn,1987; Rudinger & Thomae, 1990). Yet, the concept ofsuccessful aging has not been fully translated intooperational measures and testable hypotheses, withsome notable exceptions. The distinction betweenhypothetical and enacted function may be a key tofurther specifying (and measuring) the mechanismsunderlying successful aging. In this study, discrep-ancies were observed between what respondentssay they are able to do, and how they actually per-form. The observation of these discrepancies isespecially important among a cohort of older sub-jects who were selected to be homogeneous andhigh-functioning. Many of the psychosocial factorsthat have been linked with successful aging includ-ing social networks and supports, resiliency, per-sonality characteristics, motivation, and self-efficacymay be more closely associated with enacted func-tion than with its more hypothetical forms. A newmethod of measuring enacted function will createadditional avenues for the empirical study of suc-cessful aging beyond what has yet been achieved.
Conclusions and Implications
This article has proposed a conceptual model todescribe and understand differences between func-tional capacity and actual functional performance inthe home. Although the importance of the wordingof survey questions is commonly recognized, thedevelopment and implementation of new measuresof enacted function have lagged. Cerontological re-search has remained focused on standard measuresof function which are limited to the assessment ofcapability (hypothetical tense). The absence of inde-pendent measurement of the separate tenses offunction may lead to misclassification of risk, mea-surement error, and a gap in research on the im-portance of psychosocial factors and compensatorystrategies. It has been argued that the distinctionamong hypothetical, experimental and enacted func-tion is more than semantic, and more than a techni-cal detail of question design, but addresses theways in which the field of aging has tended to con-ceptualize functioning and how the history of thefield informs our understanding of that conceptual-ization. Several empirical examples were providedfrom the MacArthur Studies of Successful Agingwhich suggest a consistent pattern of substantialdiscordance between the hypothetical and enactedtenses of functioning. The full extent of, and expla-nations for, these discrepancies remain poorly un-derstood and, in large part, masked by the conceptsand measures currently in wide use.
The implications of this argument for researchers,interventionists, and policy makers are potentially
110 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

far-reaching. Research is needed to compare inde-pendent assessments of the three tenses of function.This will require the development of additional mea-surement tools specifically designed to capture en-acted function to complement established methodsfor the assessment of disability (hypothetical tense)and physical performance (experimental tense).Measures of enacted function could be developed inboth self-report and observer-rated formats. In ei-ther case, these new measures must be designed tocapture functional performance in the home setting,and must be sensitive to both the frequency and du-ration of functional performance. These new mea-sures may be quite useful for designers of interven-tions. As an outcome, enacted function can be usedto assess the efficacy of interventions more preciselybecause in tapping actual performance, rather thanjust capability, they capture the complex influencesof the social and physical milieu, all of which are rel-evant to the ultimate efficacy of any intervention. Inthe policy domain, many programs utilize standardADL scales to determine eligibility, despite evidencewhich suggests that "capacity wording" leads to un-derestimation of the true extent of functional diffi-culties (Anderson, Bush, & Berry, 1989; Kelly-Hayes etal., 1992; Patrick et al., 1981). The addition of separatemeasures of enacted function would allow for morevalid and reliable estimation of true disability in pop-ulations, and would lead to the identification ofunder-served groups. Finally, dual assessments ofhypothetical and enacted function will identify theprevalence of discrepant patterns II and III (over-and under-achieving) which constitute, in one case,an important new category of risk and, in the othercase, an important new phenomenon for study. Inshort, much can be learned from those individualsfor whom assessments of how they might functionand how they do function do not coincide.
References
Anderson, J. P., Bush, J. W., & Berry, C. C. (1989). Error causes in function as-sessment for quality of life and health outcome measures: Performanceversus capacity and other sources. Technical report of the Health PolicyProject, University of California at San Diego, San Diego, CA.
Applegate, W. B., Blass, J. P., & Williams, T. F. (1990). Instruments for thefunctional assessment of older patients. New England Journal of Medi-cine, 322,1207-1214.
Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on success-ful aging: The model of selective optimization with compensation. InP. B. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives fromthe behavioral sciences. Cambridge: Cambridge University Press.
Berkman, L. (1988). The changing and heterogeneous nature of aging andlongevity: A social and biomedical perspective. In C. L. Maddox & M. P.Lawton (Eds.), Annual review of gerontology and geriatrics (Vol. 8).New York: Springer Publishing Company.
Berkman, L. F., Seeman, M., Blazer, D., Kahn, R., Mohs, R., Finch, C,Schneider, E, Cotman, C, McClearn, C, Nesselroade, J., Featherman, D.,Carmezy, N., McKhann, C , Brim, C, Pragar, D., & Rowe, J. (1993). High,usual and impaired functioning in community-dwelling older men andwomen: Findings from the MacArthur Foundation research network onsuccessful aging. Journal of Clinical Epidemiology, 46,1129-1140.
Bortz, W. M. (1989). Redefining human aging. Journal of the American Geri-atric Society, 37,1092-1096.
Branch, L. C , Katz, S., Kniepmann, K., & Papsidero, J. A. (1984). A prospec-tive study of functional status among community elders. AmericanJournal of Public Health, 74, 266-268.
Butler, R. N., & Cleason, H. P. (1985). Productive aging: Enhancing vitality inlater life. New York: Springer.
Clark, D. O., Stump, T. E., & Wolinsky, F. D. (1997). A race- and gender-
specific replication of five dimensions of functional limitation and dis-ability. Journal of Aging and Health, 9, 28-42.
Cornoni-Huntley, J., Ostfeld, A, Taylor, J., Wallace, R., Blazer, D., Berkman,L. F., Evans, D., Kohout, F., Lemke, J., Scherr, P., & Korper, S. (1993). Es-tablished populations for the epidemiologic studies of the elderly:Study design and methodology. Aging/Clinical Experimental Research,5, 27-37.
Cutler, S. J., & Danigelis, N. L (1993). Organized contexts of activity. In J. R.Kelly (Ed.), Activity and aging: Staying involved in later life. NewburyPark, CA: Sage Publications.
Feinstein, A. R., Josephy, B. R., & Wells, C. K. (1986). Scientific and clinicalproblems in indexes of functional disability. Annals of Internal Medi-cine, 705,413-420.
Ferrucci, L, Bandinelli, S., Curalnik, J. M., Lamponi, M., Berttini, C, Falchini,M , & Baroni, A. (1993). Recovery of functional status after stroke: Apostrehabilitation follow-up study. Stroke, 24, 200-205.
Fuhrer, M. J. (1987). Overview of outcome analysis in rehabilitation. In M. J.Fuhrer (Ed.), Rehabilitation outcomes: analysis and measurement. Balti-more: Paul H. Brookes Publishing Co.
Class, T. A. (1991). A healthy state of tension: A review essay on three re-cent works in aging. Journal of Cross-cultural Gerontology, 6,119-125.
Glass, T. A., Seeman, T. E., Herzog, A. R., Kahn, R., & Berkman, L. F. (1995).Change in productive activity in late adulthood: MacArthur Studies ofSuccessful Aging. Journal of Gerontology: Social Sciences, 50B, S65-S76.
Curalnik, J. M., Branch, L C , Cummings, S. R., & Curb, J. D. (1989). Physicalperformance measures in aging research. Journal of Gerontology:Medical Sciences, 44, M141-146.
Hartley, L. (1985). The role of exercise in the primary and secondary pre-vention of artherosclerotic coronary artery disease. CardiovascularClinics, 15,1-8.
Herzog, A., Antonucci, T., Jackson, J., Kahn, R., & Morgan, J. (1987). Produc-tive activities and health over the life course. Paper presented at themeeting of the American Association for the Advancement of Science,Chicago, IL.
Herzog, A., & House, J. (1991). Productive activities and aging well. Genera-tions, 15, 49-54.
Herzog, A. R., Kahn, R. L, Morgan, J. N., Jackson, J. S., & Antonucci, T. C.(1989). Age differences in productive activities. Journal of Gerontology:Social Sciences, 44, S129-S138.
Hickey, T. (1980). Health and aging. Monterey, CA: Brooks/Cole Publishing.Hubert, H. B., Bloch, D. A., & Fries, J. F. (1993). Risk factors for physical dis-
ability in an aging cohort: the NHANES I Epidemiologic FollowupStudy. Journal of Rheumatology, 20, 480-488.
Idler, E. L. (1987). Religious involvement and the health of the elderly:Some hypotheses and an initial test. Social Forces, 66, 226-238.
Jette, A. (1987). The Functional Status Index: reliability and validity of a self-report functional disability measure. Journal of Rheumatology, 74,15-21.
Jette, A. (1994). Physical disablement concepts for physical therapy re-search and practice. Physical Therapy, 74, 380-386.
Jette, A. M. (1994). How measurement techniques influence estimates ofdisability in older populations. Social Science & Medicine, 38, 937-942.
Jette, A. M., & Branch, L. G. (1981). The Framingham disability study: II.Physical disability among the elderly. American Journal Public Health,71,1211-1216.
Jette, A. M., & Branch, L G. (1985). Impairment and disability in the aged.Journal of Chronic Diseases, 38,59-65.
Kahn, R. L. (1986). Productive activities and well-being. Paper presented atannual meetings of The Gerontological Society of America, Chicago, IL.
Kane, R. A., & Kane, R. L (1987). Long-term care: Principles, programs andpolicies. New York: Springer.
Kannel, W. B., Belanger, A., D'Agostino, R., & Israel, I. (1986). Physical activ-ity and physical demand on the job and risk of cardiovascular diseaseand death: the Framingham Study. American Heart Journal, 112,820-825.
Kasl, S. V. (1995). Strategies in research on health and aging: Looking be-yond secondary data analysis. Journal of Gerontology: Social Sciences,50B, S191-S193.
Katz, S., Downs, T. D., Cash, H. R., & Grotz, R. C. (1970). Progress in devel-opment of the index of ADL. Gerontologist, 10, 20-30.
Katz, S., Ford, A. B., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963).Studies of illness in the aged. The Index of ADL: A standardized mea-sure of biological and psychosocial function. Journal of the AmericanMedical Association, 185, 914-919.
Keith, J. (1985). Cross-cultural research on aging. In Binstock & Shanas(Eds.), Handbook on aging and the social sciences. New York: VanNostrand and Reinhold.
Keith, J. (1988). Participant observation. In K. W. Schaie, R. T. Campbell, W.Meredith, & S. C. Rawlings (Eds.), Methodological issues in aging re-search. New York: Springer.
Keller, D. M., Kovar, M. G., Jobe, J. B., & Branch, L. G. (1993). Problems elic-iting elders' reports of functional status. Journal of Aging and Health, 5,306-318.
Kelly-Hayes, M., Jette, A. M., Wolf, P. A., D'Agostino, R. B., & Odell, P. M.(1992). Functional limitations and disability among elders in the Fram-ingham Study. American Journal of Public Health, 82, 841-845.
Vol. 38, No. 1,1998 111
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from

Kiely, D., Wolf, P., Cupples, L, Beiser, A., & Kannel, W. (1994). Physical ac-tivity and stroke risk: the Framingham Study. American Journal of Epi-demiology, 140, 608-620.
Kovar, M. C. (1991). Functional ability and the need for care: Issues formeasurement research. Vital & Health Statistics — Series 5, Compara-tive International Vital & Health Statistics Reports, 97-103.
Lawrence, R. H., & Jette, A. M. (1996). Disentangling the disablement pro-cess. Journal of Gerontology: Social Sciences, 51B, S173-S182.
Lawton, M. P., & Brody, E. M. (1969). Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist, 9,179-186.
Lawton, M. P., Moss, M., Fulcomer, M., & Kleban, M. H. (1982). A researchand service oriented multilevel assessment instrument. Journal ofGerontology, 37, 91-99.
Lee, D. J., & Markides, K. S. (1990). Activity and mortality among aged per-sons over an eight year period. Journal of Gerontology: Social Science,45, S39-S42.
Leon, A. S. (1985). Physical activity levels and coronary heart disease analy-sis of epidemiologic and supporting studies. Medical Clinics of NorthAmerica, 69,3-20.
Maddox, C. L. (1979). The sociology of later life. Annual Review Sociology,5,113-135.
Maddox, C. L (1987). Aging differently. The Gerontologist, 27,557-564.Mahoney, F. I., & Barthel, D. W. (1965). Functional evaluation: The Barthel
Index. Maryland State Medical Journal, 14, 61-65.McDowell, I., & Newell, C. (1987). Measuring health: A guide to rating
scales and questionnaires. New York: Oxford University Press.Mendes de Leon, C. F., Fillenbaum, C. C , Williams, C. S., Brock, D. B.,
Beckett, L. A., & Berkman, L. F. (1995). Functional disability among el-derly blacks and whites in two diverse areas: the New Haven andNorth Carolina EPESE. Established populations for the epidemiologicstudies of the elderly. American Journal of Public Health, 85, 994-998.
Mendes de Leon, C. F., Seeman, T. E., Baker, D. I., Richardson, E. D., &Tinetti, M. E. (1996).Self-efficacy, physical decline, and change in func-tioning in community-living elders: a prospective study. Journals ofGerontology: Social Sciences, 51, S183-S190.
Miner, S., Logan, J. R., & Spitze, G. (1993). Predicting the frequency of se-nior center attendance. Gerontologist, 33, 650-657.
Myers, C. C, Manton, K. C , & Bacellar, H. (1986). Sociodemographic as-pects of future unpaid productive roles. In Institute of Medicine/Na-tional Research Council (Eds.), America's aging: Productive roles in anolder society. Washington DC: National Academy Press.
Nagi, S. Z. (1965). Some conceptual issues in disability and rehabilitation.In M. B. Sussman (Ed.), Sociology and rehabilitation. Washington, DC:American Sociological Association.
Nagi, S. Z. (1976). An epidemiology of disability among adults in the UnitedStates. Milbank Memorial Fund Quarterly, 54,439-468.
Nagi, S. Z. (1991). Disability concepts revisited: Implications for prevention.In A. Pope & A. Tarlov (Eds.), Disability in America: Toward a nationalagenda for prevention. Washington, DC: National Academy Press.
Paffenbarger, R. S., Jr., Hyde, R. T., Wing, A. L, & Hsieh, C. C. (1986). Physi-cal activity, all-cause mortality, and longevity of college alumni. NewEngland Journal of Medicine, 6314, 605-613.
Patrick, D. L, Darby, S. C, Green, S., Horton, G., Locker, D., & Wiggins, R.D. (1981). Screening for disability in the inner city. Journal of EpidemiolCommunity Health, 35, 65-70.
Pinsky, J., Branch, L., Jette, A., Haynes, S., Feinleib, M., Cornoni-Huntley, J.,& Bailey, K. (1985). Framingham Disability Study: Relationship of dis-ability to cardiovascular risk factors among persons free of diagnosedcardiovascular disease. American Journal of Epidemiology, 122,644-656.
Reuben, D. B., Valle, L. A., Hays, R. D., & Siu, A. L. (1995). Measuring physi-cal function in community-dwelling older persons: a comparison of
self-administered, interviewer-administered, and performance-basedmeasures. Journal of the American Geriatrics Society, 43,17-23.
Robine, J. M., Michel, J. P., & Branch, L. G. (1992). Measurement and utiliza-tion of healthy life expectancy: Conceptual issues. Bulletin of theWorld Health Organization, 70, 791-800.
Roos, N. P., & Havens, B. (1981). Predictors of successful aging: A twelve-year study of Manitoba elderly. American Journal of Public Health, 81,63-68.
Rosow, I., & Breslau, N. (1966). A Guttman health scale for the aged. Jour-nal of Gerontology, 21, 556-559.
Rowe, J. W., & Kahn, R. L. (1987). Human aging: usual and successful. Sci-ence, 237,143-149.
Rudinger, G., & Thomae, H. (1990). The Bonn Longitudinal Study of Aging:Coping, life adjustment, and life satisfaction. In P. B. Baltes & M. M.Baltes (Eds.), Successful aging: Perspectives from the behavioral sci-ences. Cambridge: Cambridge University Press.
Simonsick, E. M., Lafferty, M. E., Phillips, C. L, Mendes, D., Leon, C. F., Kasl,S. V., Seeman, T. E., Fillenbaum, G., Hebert, P., & Lemke, J. H. (1993).Risk due to inactivity in physically capable older adults. American Jour-nal of Public Health, 83,1443-1450.
Stewart, A. L., Ware, J. E., & Brook, R. H. (1981). Advances in the Measure-ment of functional status: Construction of aggregate indexes. MedicalCare, XIX, 473-488.
Tinetti, M. E. (1986). Performance-oriented assessment of mobility prob-lems in elderly patients. Journal of the American Geriatric Society, 34,119-126.
Verbrugge, L. M., & Jette, A. M. (1994). The disablement process. Social Sci-ence & Medicine, 38,1-14.
Verbrugge, L. M., Lepkowski, J. M., & Konkol, L. L. (1991). Levels of disabil-ity among U.S. adults with arthritis. Journal of Gerontology, 46, S71-83.
Wagner, K. A. (1987). Outcome analysis in comprehensive medical rehabil-itation. In M. J. Fuhrer (Ed.), Rehabilitation outcomes: Analysis andmeasurement. Baltimore: Paul H. Brookes Publishing Co.
World Health Organization. (1980). International classification of impair-ments, disabilities, and handicaps. Geneva: World Health Organization.
Ziebland, S., Fitzpatrick, R., & Jenkinson, C. (1993). Tacit models of disabil-ity underlying health status instruments. Social Science & Medicine,37, 69-75.
Received December 18,1996Accepted June 20,1997
Appendix
Notes
1. There are minor differences in the language used bydifferent authors in the disability tradition. Where Nagiuses the terms "disability" and "handicap" (Nagi, 1965),Verbrugge and Jette use instead the terms "functionallimitations" and "disability" (Verbrugge & Jette, 1994).
2. Subjects were considered to be high-functioning ifthey met several criteria including a) no disability onthe Katz ADL scale, b) not more than one disabilityitem on either the Rosow-Breslau or Nagi scales ofgross mobility and physical performance, and c) ascore of 6 or higher on the 9-item test of cognitive per-formance developed by Pfieffer.
112 The Gerontologist
at INSE
RM
on July 16, 2013http://gerontologist.oxfordjournals.org/
Dow
nloaded from