Embed Size (px)
Citation preview

J. clin. Path., 1977, 30, 184-190
Congenital dyserythropoietic anaemia: response tosplenectomy and quantitation of ineffectiveerythropoiesisDIANA SAMSON', D. HALLIDAY2, AND I. CHANARIN1
From the Department ofHaematology' and Division of Clinical Investigation2, Northwick Park Hospitaland Clinical Research Centre, Watford Road, Harrow, Middlesex
SUMMARY The clinical and haematological features of an unusual case of congenital dyserythro-poietic anaemia are described. There was a pronounced haemolytic component to the anaemia,with a mean cell life of five days, and a remarkable response to splenectomy. Measurement of theincorporation of 15N glycine into the haem of circulating red cells and into bilirubin showed thathaem turnover due to ineffective erythropoiesis was increased 45 times compared with a controlgroup (11 63 mg/kg/day, NR = 0-26 ± 0 10) and represented 51 % of total erythroid haem turnover.
Heimpel and Wendt (1968) defined three types ofcongenital dyserythropoietic anaemia: type 1,megaloblastic erythropoiesis with internuclear chro-matin bridges (Wendt and Heimpel, 1967; Heimpelet al., 1971); type II, hereditary erythroblasticmultinuclearity with a positive acidified serum test(HEMPAS) (Crookston, et al., 1969; Verwilghenet al., 1973); and type III, erythroblastic multi-nuclearity and gigantoblasts (Wolff and Von Hofe,1951; Bergstrom and Jacobsson, 1962; Goudsmitet al., 1972). Other congenital dyserythropoietic syn-dromes have been described by Valentine et al. (1973)and Weatherall et al. (1973).The present report describes the clinical and
haematological features of a patient with severecongenital dyserythropoietic anaemia (CDA) whichdoes not fall into any of the above categories, andin whom there was a remarkable response to splen-ectomy. In order to quantitate the degree of ineffec-tive erythropoiesis the incorporation of 15N glycineinto the haem of circulating red cells and intobile pigment was measured.
Case report
NE, the youngest of four children, was born after a
Requests for reprints: Dr. I. Chanarin, Department ofHaematology, Northwick Park Hospital and ClinicalResearch Centre, Watford Road, Harrow, Middlesex,HAl 3UJReceived for publication 21 June 1976
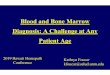
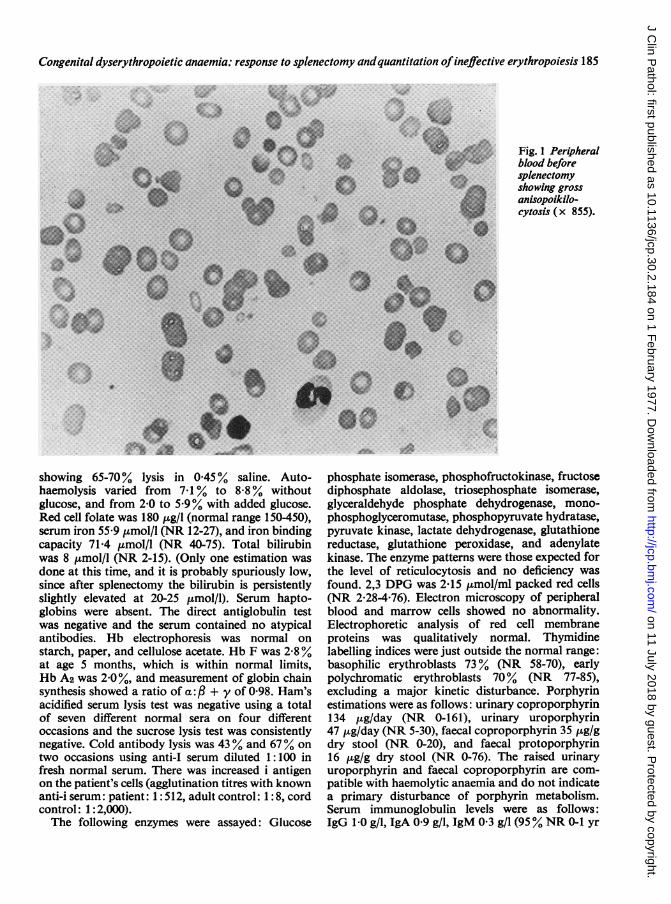
normal pregnancy and delivery. Anaemia andhepatosplenomegaly were first noted at 8 weeks.Both liver and spleen were palpable 3 cm below thecostal margin. There was no lymphadenopathy andhe was not clinically jaundiced. There was norelevant family history. Initial investigations wereas follows: Hb 3 9 g/dl, MCV 76 fl, total WBC18,900/,ul, neutrophils 11,900/,ul, lymphocytes 7,300/pl, monocytes 200/,ul, eosinophils 400/pl, occasionalmyelocytes and metamyelocytes, nucleated red cells180/100 WBC, reticulocytes 7 0%, and platelets160,000/,ul. The peripheral blood (Fig. 1) showedmarked anisocytosis and poikilocytosis, spherocytes,schistocytes, polychromasia, Howell-Jolly bodies,and basophil stippling. The marrow (Fig. 2) washypercellular with marked erythroid hyperplasia,normoblastic erythropoiesis, and gross dyshaemo-poiesis. A few binucleate erythroblasts were presentat all stages ofdevelopment but were not a prominentfeature, and cells containing more than two nucleiwere rare. There were also numerous smear cells andreticulum cells, some showing erythrophagocytosis.Iron stores were normal and there were no ringsideroblasts. The following further investigationswere carried out, mainly during the first 6 months oflife. The estimated mean cell life of the patient'sown cells, using 51Cr labelling and the elutioncorrections of Garby and Mollison (1971), was fivedays while that of compatible donor cells was 80days. Surface counting was not carried out, so thatno data are available on splenic sequestration.Osmotic fragility was increased, the patient's cells
184
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
Congenital dyserythropoietic anaemia: response to splenectomy andquantitation ofineffective erythropoiesis 185
. ....71
*64' X
.../. JL; .
tip~~~~~~~~~~~~~~~~~~i
showing 65 70 /% lysis in 0-45% saline. Auto-haemolysis varied from 7 1 % to 8-8% withoutglucose, and from 2-0 to 5-9% with added glucose.Red cell folate was 180 Mg/i (normal range 150-450),serum iron 55-9 pmol/l (NR 12-27), and iron bindingcapacity 71-4 vLmol/l (NR 40-75). Total bilirubinwas 8 umol/l (NR 2-15). (Only one estimation wasdone at this time, and it is probably spuriously low,since after splenectomy the bilirubin is persistentlyslightly elevated at 20-25 Mmol/l). Serum hapto-globins were absent. The direct antiglobulin testwas negative and the serum contained no atypicalantibodies. Hb electrophoresis was normal onstarch, paper, and cellulose acetate. Hb F was 2-8 %at age 5 months, which is within normal limits,Hb A2 was 2-0%, and measurement of globin chainsynthesis showed a ratio of a: P8 + y of 0-98. Ham'sacidified serum lysis test was negative using a totalof seven different normal sera on four differentoccasions and the sucrose lysis test was consistentlynegative. Cold antibody lysis was 43% and 67% ontwo occasions using anti-I serum diluted 1: 100 infresh normal serum. There was increased i antigenon the patient's cells (agglutination titres with knownanti-i serum: patient: 1:512, adult control: 1:8, cordcontrol: 1: 2,000).The following enzymes were assayed: Glucose
v.W.R5 --- Fig. 1 Peripheralblood beforesplenectomyshowing grossanisopoikilo-cytosis (x 855).
phosphate isomerase, phosphofructokinase, fructosediphosphate aldolase, triosephosphate isomerase,glyceraldehyde phosphate dehydrogenase, mono-phosphoglyceromutase, phosphopyruvate hydratase,pyruvate kinase, lactate dehydrogenase, glutathionereductase, glutathione peroxidase, and adenylatekinase. The enzyme patterns were those expected forthe level of reticulocytosis and no deficiency wasfound. 2,3 DPG was 2-15 Mmol/ml packed red cells(NR 2-28-4-76). Electron microscopy of peripheralblood and marrow cells showed no abnormality.Electrophoretic analysis of red cell membraneproteins was qualitatively normal. Thymidinelabelling indices were just outside the normal range:basophilic erythroblasts 73% (NR 58-70), earlypolychromatic erythroblasts 70% (NR 77-85),excluding a major kinetic disturbance. Porphyrinestimations were as follows: urinary coproporphyrin134 gLg/day (NR 0-161), urinary uroporphyrin47 urg/day (NR 5-30), faecal coproporphyrin 35 jug/gdry stool (NR 0-20), and faecal protoporphyrin16 pg/g dry stool (NR 0-76). The raised urinaryuroporphyrin and faecal coproporphyrin are com-patible with haemolytic anaemia and do not indicatea primary disturbance of porphyrin metabolism.Serum immunoglobulin levels were as follows:IgG 1-0 g/l, IgA 0-9 g/l, IgM 0-3 g/l (95% NR 0-1 yr
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
Diana Samson, D. Halliday, and L Chanarin
Fig. 2 Twobinucleateerythroblasts fronzthe marrow(x 1000). (insetx 7000)
in this laboratory: IgG 3-0-13'6 g/l, IgA 0-3-1V3 g/l,IgM 0-3-2-3 g/l). Urea and electrolytes, urinaryamino acids, chest x-ray, skeletal survey, and intra-venous pyelogram were all normal. Chromosomalanalysis of blood/marrow cells was not performed.The patient was transfused soon after admission
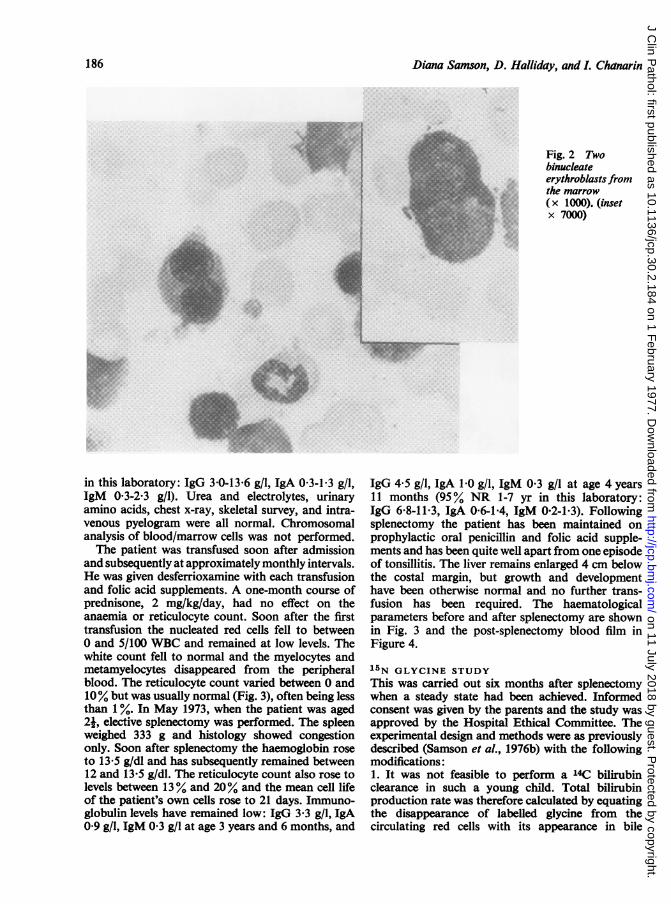
and subsequently at approximately monthly intervals.He was given desferrioxamine with each transfusionand folic acid supplements. A one-month course ofprednisone, 2 mg/kg/day, had no effect on theanaemia or reticulocyte count. Soon after the firsttransfusion the nucleated red cells fell to between0 and 5/100 WBC and remained at low levels. Thewhite count fell to normal and the myelocytes andmetamyelocytes disappeared from the peripheralblood. The reticulocyte count varied between 0 and10% but was usually normal (Fig. 3), often being lessthan 1 %. In May 1973, when the patient was aged24, elective splenectomy was performed. The spleenweighed 333 g and histology showed congestiononly. Soon after splenectomy the haemoglobin roseto 13-5 g/dl and has subsequently remained between12 and 13-5 g/dl. The reticulocyte count also rose tolevels between 13% and 20% and the mean cell lifeof the patient's own cells rose to 21 days. Immuno-globulin levels have remained low: IgG 3-3 g/l, IgA0-9 g/l, IgM 0 3 g/l at age 3 years and 6 months, and
IgG 4 5 g/l, IgA 1.0 g/l, IgM 0 3 g/l at age 4 years11 months (95% NR 1-7 yr in this laboratory:IgG 6-8-11-3, IgA 0-6-1P4, IgM 0-2-1-3). Followingsplenectomy the patient has been maintained onprophylactic oral penicillin and folic acid supple-ments and has been quite well apart from one episodeof tonsillitis. The liver remains enlarged 4 cm belowthe costal margin, but growth and developmenthave been otherwise normal and no further trans-fusion has been required. The haematologicalparameters before and after splenectomy are shownin Fig. 3 and the post-splenectomy blood film inFigure 4.
15N GLYCINE STUDYThis was carried out six months after splenectomywhen a steady state had been achieved. Informedconsent was given by the parents and the study wasapproved by the Hospital Ethical Committee. Theexperimental design and methods were as previouslydescribed (Samson et al., 1976b) with the followingmodifications:1. It was not feasible to perform a 14C biirubinclearance in such a young child. Total bilirubinproduction rate was therefore calculated by equatingthe disappearance of labelled glycine from thecirculating red cells with its appearance in bile
186
II
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
Congenital dyserythropoietic anaemia: response to splenectomy andquantitation ofineffective erythropoiesis 187
Splenectomy
14 FI
HbgIdl 12 Hb10
30Retics % 20 Retics
10_
Platelets 1, 000x101 600 Platelets
300
Tf%*21 100 _ <.io aLwhite cellcountx10op
Fig. 3 Haemato-- logicalparameters
before and aftersplenectomy.
~~//
Jul Aug Sep Oct Nov Dec Jan Jan Jan
1974 1975 1976
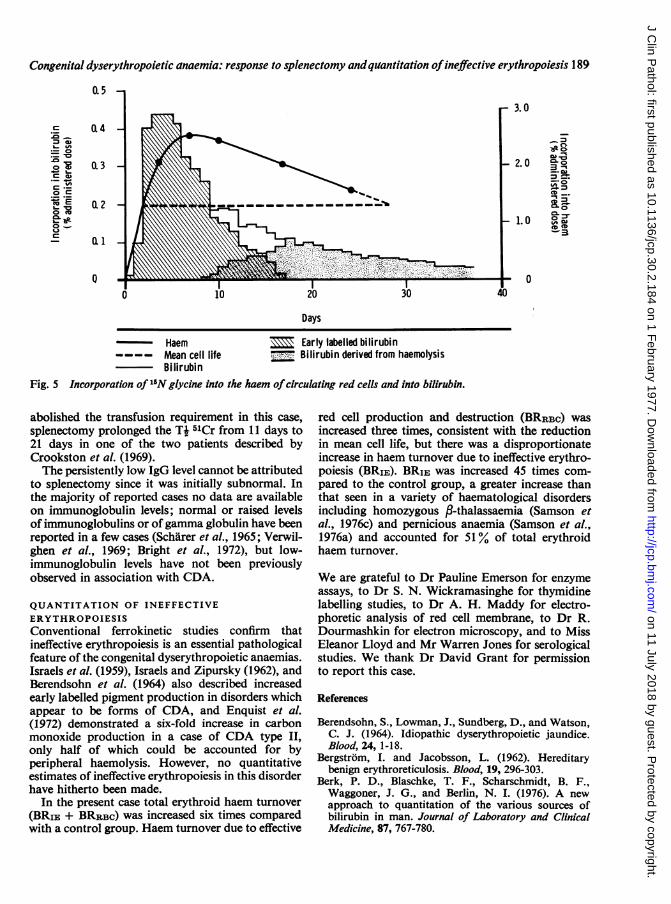
CALCULATION OF % INCORPORATION INTOEARLY LABELLED BILIRUBINThe % 15N glycine lost from peripheral blood haemdaily between day 7 and day 17 was derived from thegraph (Fig. 5). This would give rise to an equal %15N glycine incorporation into bilirubin on that daywhich was therefore subtracted from the total% 15N glycine incorporation into bilirubin to givethe % 15N glycine incorporated into early labelledbilirubin (Table). From the graph the apparentmean cell life of the cells labelled with 15N is shownto be 27 days, compared with a mean cell life of 21days determined by 51Cr survival, indicating re-utilisation of 15N glycine for haem synthesis whichwould be associated with further excretion of labelledbilirubin. For this reason the early labelled bilirubinrelating to the synthesis of the initial cohort of redcells is considered to end at day 10. The total %incorporation of 15N glycine into the early labelledbilirubin days 0-10 (GELP) was 2-83 %.
FURTHER PARAMETERSBRRBc and BRIE, bilirubin production from red celldestruction and from ineffective erythropoiesis, andthe percentage ineffective erythropoiesis werecalculated as previously described (Samson et al.,
TransfusionsI
C//XI
\jv~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
20 White count
10jj5 L- "
Feb Mar Apr Dec Jan Feb Mar Apr May Jun
1971 1973
pigment. This necessitated prolonging the studyperiod.2. In view of the enormous increase in erythroidhaem turnover, it was not considered necessary toquantitate hepatic haem turnover by measuring theincorporation of 8-aminolaevulinic acid into earlylabelled bilirubin.
CALCULATION OF BILIRUBIN PRODUCTIONRATE (BRP)The incorporation of the administered glycine (80 mgof 98-5 atom % excess 15N) on day x =BRP x 8 x MW glycine x atom % excess bilirubinday x/MW bilirubin x 80 x 98-5 = 0-0128 x BRPx atom % excess 15N bilirubin day x.Assuming that all labelled bilirubin produced afterday 17 is derived from destruction of circulating redcells (see Fig. 5)x=24£ % incorporation glycine into bilirubin =%x=18
incorporation glycine into Hb haem day 17-% incorporation glycine into Hb haem day 24.
x=240-0128 x BRP x L atom %excess 15N bilirubin =
x=182-17-1-57 BRP = 330 mg/day.
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
Diana Samson, D. Halliday, and L Chanarin
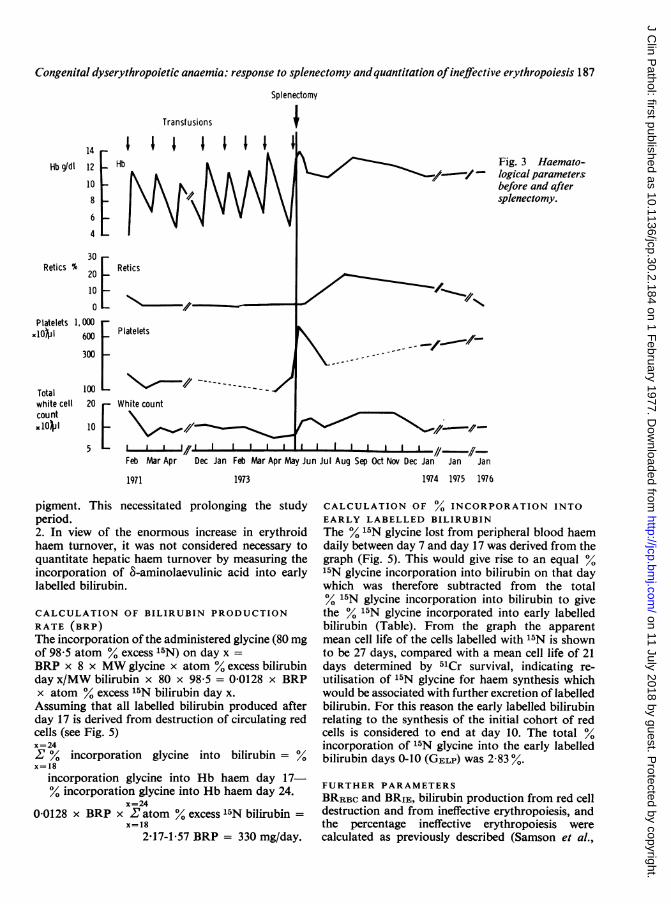
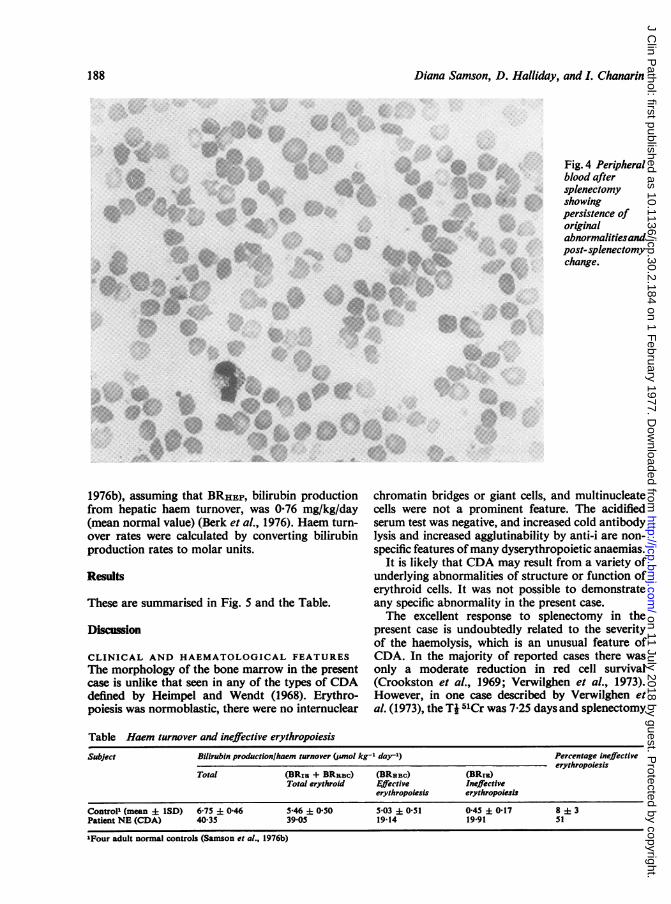
Fig. 4 Peripheralblood aftersplenectomyshowingpersistence oforiginalabnormalitiesandpost-splenectomychange.
1976b), assuming that BRHEp, bilirubin productionfrom hepatic haem turnover, was 0-76 mg/kg/day(mean normal value) (Berk et al., 1976). Haem turn-over rates were calculated by converting bilirubinproduction rates to molar units.
Results
These are summarised in Fig. 5 and the Table.
Discussion
CLINICAL AND HAEMATOLOGICAL FEATURES
The morphology of the bone marrow in the presentcase is unlike that seen in any of the types of CDAdefined by Heimpel and Wendt (1968). Erythro-poiesis was normoblastic, there were no internuclear
chromatin bridges or giant cells, and multinucleatecells were not a prominent feature. The acidifiedserum test was negative, and increased cold antibodylysis and increased agglutinability by anti-i are non-specific features ofmany dyserythropoietic anaemias.
It is likely that CDA may result from a variety ofunderlying abnormalities of structure or function oferythroid cells. It was not possible to demonstrateany specific abnormality in the present case.The excellent response to splenectomy in the
present case is undoubtedly related to the severityof the haemolysis, which is an unusual feature ofCDA. In the majority of reported cases there wasonly a moderate reduction in red cell survival(Crookston et al., 1969; Verwilghen et al., 1973).However, in one case described by Verwilghen etal. (1973), the Ti 51Cr was 7-25 days and splenectomy
Table Haem turnover and ineffective erythropoiesisSubject Bilirubin production/haem turnover (pmol kg-l dayL) Percentage ineffective
erythropoiesisTotal (BRIs + BRRBC) (BRRBC) (BRi,)
Total erythroid Effective Ineffectiveerythropolesis erythropoiesis
Control& (mean + 1SD) 675 + 046 546 + 0-50 503 + 051 045 ± 017 8 + 3Patient NE (CDA) 40135 39105 19-14 19 91 51
'Four adult normal controls (Samson et al., 1976b)
188
.t ....g. t.. .
WK
AN:-A-f
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
Congenital dyserythropoietic anaemia: response to splenectomy andquantitation ofineffective erythropoiesis 189
0Q5
a
-_
_
= .
02
C
-._0
c ._
0 c
L i?o_L-
Q4
a.3
0.2
01
_0 10 20 30
Days
Haem Early labelled bilirubinMean cell life . Bilirubin derived from haemolysis
BilirubinFig. 5 Incorporation of 15N glycine into the haem ofcirculating red cells and into bilirubin.
abolished the transfusion requirement in this case,splenectomy prolonged the Ti 51Cr from 11 days to21 days in one of the two patients described byCrookston et al. (1969).The persistently low IgG level cannot be attributed
to splenectomy since it was initially subnormal. Inthe majority of reported cases no data are availableon immunoglobulin levels; normal or raised levelsof immunoglobulins or ofgamma globulin have beenreported in a few cases (Scharer et al., 1965; Verwil-ghen et al., 1969; Bright et al., 1972), but low-immunoglobulin levels have not been previouslyobserved in association with CDA.
QUANTITATION OF INEFFECTIVE
ERYTHROPOIESISConventional ferrokinetic studies confirm thatineffective erythropoiesis is an essential pathologicalfeature of the congenital dyserythropoietic anaemias.Israels et al. (1959), Israels and Zipursky (1962), andBerendsohn et al. (1964) also described increasedearly labelled pigment production in disorders whichappear to be forms of CDA, and Enquist et al.(1972) demonstrated a six-fold increase in carbonmonoxide production in a case of CDA type II,only half of which could be accounted for byperipheral haemolysis. However, no quantitativeestimates of ineffective erythropoiesis in this disorderhave hitherto been made.
In the present case total erythroid haem turnover(BRn3 + BRRBc) was increased six times comparedwith a control group. Haem turnover due to effective
red cell production and destruction (BRRBc) wasincreased three times, consistent with the reductionin mean cell life, but there was a disproportionateincrease in haem turnover due to ineffective erythro-poiesis (BRIE). BRIE was increased 45 times com-pared to the control group, a greater increase thanthat seen in a variety of haematological disordersincluding homozygous ,B-thalassaemia (Samson et
al., 1976c) and pernicious anaemia (Samson et al.,1976a) and accounted for 51 % of total erythroidhaem turnover.
We are grateful to Dr Pauline Emerson for enzymeassays, to Dr S. N. Wickramasinghe for thymidinelabelling studies, to Dr A. H. Maddy for electro-phoretic analysis of red cell membrane, to Dr R.Dourmashkin for electron microscopy, and to MissEleanor Lloyd and Mr Warren Jones for serologicalstudies. We thank Dr David Grant for permissionto report this case.
References
Berendsohn, S., Lowman, J., Sundberg, D., and Watson,C. J. (1964). Idiopathic dyserythropoietic jaundice.Blood, 24, 1-18.
Bergstrom, I. and Jacobsson, L. (1962). Hereditarybenign erythroreticulosis. Blood, 19, 296-303.
Berk, P. D., Blaschke, T. F., Scharschmidt, B. F.,Waggoner, J. G., and Berlin, N. I. (1976). A newapproach to quantitation of the various sources ofbilirubin in man. Journal of Laboratory and ClinicalMedicine, 87, 767-780.
3.0
_n
2. 0 3 "
0
~1. 0 ° r
CDC3
0
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from
190
Bright, M., Cobb, J., Evans, B., and Parry, T. E. (1972).Congenital dyserythropoietic anaemia with erythro-blastic multinuclearity. Journal of Clinical Pathology,25, 561-569.
Crookston, J. H., Crookston, M. C., Burnie, K. L.,Francombe, W. H., Dacie, J. V., Davis, J. A., andLewis, S. M. (1969). Hereditary erythroblastic multi-nuclearity associated with a positive acidified-serumtest: a type of congenital dyserythropoietic anaemia.British Journal ofHaematology, 17, 11-26.
Enquist, R. W., Gockerman, J. P., Jenis, E. H., Warkel,R. L., and Dillon, D. E. (1972). Type II congenitaldyserythropoietic anemia. Annals of Internal Medicine77, 371-376.
Garby, L. and Mollison, P. L. (1971). Deduction of meanred-cell life-span from r1Cr survival curves. BritishJournal of Haematology, 20, 527-536.
Goudsmit, R., Beckers, D., de Bruijne, J. I., Engelfriet,C. P., James, J., Morselt, A. F. W., and Reynierse, E.(1972). Congenital dyserythropoietic anaemia, TypeIII. British Journal of Haematology, 23, 97-105.
Heimpel, H., Forteza-Vila, J., Queisser, W., and Spiertz,E. (1971). Electron and light microscopic study of theerythroblasts of patients with congenital dyserythro-poietic anemia. Blood, 37, 299-310.
Heimpel, H. and Wendt, F. (1968). Congenital dyserythro-poietic anaemia with karocrrhexis and multinuclearityof erythroblasts. Helvetica Medica Acta, 34, 103-115.
Israels, L. G., Suderman, H. J., and Ritzmann, S. E.(1959). Hyperbilirubinemia due to an alternate pathof bilirubin production. American Journal of Medicine,27, 693-702.
Israels, L. G. and Zipursky, A. (1962). Primary shunthyperbilirubinaemia. Nature (London), 193, 73-74.
Samson, D., Halliday, D., and Chanarin, I. (1976a).Reversal of ineffective erythropoiesis following treat-ment in pernicious anaemia. British Journal of Haemo-tology, in press.
Diana Samson, D. Halliday, and I. Chanarin
Samson, D., Halliday, D., Nicholson, D. C., andChanarin, I. (1976b). Quantitation of ineffectiveerythropoiesis from the incorporation of [1'N] 8-amino-laevulinic acid and [15N] glycine into early labelledbilirubin. I. Normal subjects. British Journal ofHaematology, 34, 33-44.
Samson, D., Halliday, D., Nicholson, D. C., andChanarin, I. (1976c). Quantitation of ineffectiveerythropoiesis from the incorporation of [15N] 8-amino-laevulinic acid and [15N] glycine into early labelledbilirubin. II. Anaemic patients. British Journal ofHaematology, 34, 45-53.
Scharer, K., Marti, H. R., and Baumann, T. (1965).Konstitutionelle Anamie mit Kernteilungsstorung derErythroblasten. Schweizerische medizinische Wocher-schrift, 95, 1511-1515.
Valentine, W. N., Konrad, P. N., and Paglia, D. E. (1973).Dyserythropoiesis, refractory anaemia, and "pre-leukemia:" metabolic features of the erythrocytes.Blood, 41, 857-875.
Verwilghen, R. L., Lewis, S. M., Dacie, J. V., Crookston,J. H., and Crookston, M. C. (1973). HEMPAS:Congenital dyserythropoietic anaemia (Type II).Quarterly Journal of Medicine, 42, 257-278.
Verwilghen, R., Verhaegen, H., Waumans, P., and Beert,J. (1969). Ineffective erythropoiesis with morphologic-ally abnormal erythroblasts and unconjugated hyper-bilirubinaemia. British Journal of Haematology, 17,27-33.
Weatherall, D. J., Clegg, J. B., Knox-Macaulay, H. H. M.Bunch, C., Hopkins, C. R., and Temperley, I. J. (1973).A genetically determined disorder with features bothof thalassaemia and congenital dyserythropoieticanaemia. British Journal of Haematology, 24, 681-702.
Wolff, J. A. and Von Hofe, F. H. (1951). Familialerythroid multinuclearity. Blood, 6, 1274-1283.
Wendt, F. and Heimpel, H. (1967). Kongenitale dysery-thropoetische Anamie bei einem zweieiigen Zwillings-paar. Medizinische Klinik, 62, 172-177.
on 11 July 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.2.184 on 1 F
ebruary 1977. Dow
nloaded from