Embed Size (px)
DESCRIPTION
Congenital Cytomegalovirus Lalith Wijedoru - PowerPoint PPT Presentation
Citation preview

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Congenital CytomegalovirusLalith WijedoruLalith Wijedoru is a medical graduate of University College London Medical School. He completed Senior House Officer training in paediatrics at Sheffield Children’s Hospital before starting Specialist Registrar posts in Leeds and subsequently Alder Hey Children’s Hospital, Liverpool. He holds a MSc in Tropical Paediatrics from the Liverpool School of Tropical Medicine (LSTM), and a junior clinical lectureship at LSTM.
His academic interests relate to the febrile child in resource limited settings in Asia. His particular focus relates to the diagnostic difficulty in distinguishing viral, bacterial and parasitic infections in children, including neonates.
Edited by Prof Tom Solomon, Dr Agam Jung and Dr Sam Nightingale
This session looks at cytomegalovirus (CMV) which is the most common congenital viral infection worldwide. Neonatal clinical
signs, diagnostics, treatment and neurological sequelae in children will be discussed. Public health measures including
screening and immunisation will also be considered

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Learning Objectives
By the end of this session you will be able to:
• Recognise the clinical signs of acute CMV infection in the newborn
• Define both antenatal and postnatal diagnostic methods for congenital CMV
• Describe the treatment options for acute CMV infection in newborns
• List the neurological sequelae of neonatal CMV infection in children
• Discuss the potential public health measures which could reduce CMV-associated neuro-disability in children

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Introduction
Congenital infections remain an important source of neurological disability for thousands of children worldwide. Cytomegalovirus (CMV) is the commonest congenital infection in the developed world. 1-4% of women have a primary infection during pregnancy. Most of them are asymptomatic.
The majority of congenitally-infected infants appear normal at birth, but long-term neurological sequelae of psychomotor retardation and/or hearing loss occur in about 10-15%. Clinical signs of acute CMV infection in infants include growth retardation, microcephaly, thrombocytopenia, and jaundice.
Microbiology including serology, biochemical markers and radiology can be used in both the antenatal and postnatal diagnosis of CMV. The efficacy and duration of treatment is controversial, with ganciclovir and valganciclovir demonstrating encouraging trial results.
Prevention strategies of maternal CMV infection including immunisation and screening. These remain the subject of debate given the current evidence of both vaccine efficacy and anti-viral treatment.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Congenital Infections and Neurology I
Infections associated with pregnancy may be with or without foetal consequence. Serious adverse effects include:
• Foetal death• Stillbirth• Intrauterine growth retardation• Congenital malformations

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Congenital Infections and Neurology II• Symptomatic at birth: Those who are symptomatic at birth generally
have significant long-term neurological sequelae.
• Asymptomatic at birth: Those are asymptomatic at birth may never manifest evidence of neurological damage, or this may become clinically evident later in life.
• TORCH(ES) agents: Specific congenitally-acquired infections are often referred to as the TORCH(ES) agents…
Toxoplasmosis Rubella Cytomegalovirus Herpes (including varicella zoster and herpes simplex) HIV Syphilis
UK public health campaigns for the majority of these infectious agents are fairly robust. However, the herpes viruses (including CMV) are considered to be neglected in this context.
• Prevalence: In northern Europe, the overall rate of congential CMV infection is estimated at 1% of all live births. It is estimated that between 4000 and 6000 children born each year in the United States will develop permanent neurological deficits as a result of CMV.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
MicrobiologyCytomegaloviruses (CMV) belong to the β-herpesviruses sub-family of herpes viruses. These viruses are highly species-specific and infect many animals. Infection is common in human populations, but rarely symptomatic in hosts with normal immune function.
In contrast, it can cause multi-organ disease in immuno-compromised patients of all ages. Foetuses and neonates with their relative poor immune function are particularly at risk. Like with other herpes viruses, primary infection with CMV leads to persistent infection.
CMV can be transmitted from mother to child transplacentally, during birth, and in the postpartum period.
• Early transplacental transmission during the first trimester is associated with the greatest neurological damage to the foetus.
• The majority of transmission occurs in the third trimester and during delivery.
• Intrapartum transmission of CMV occurs in around 50% of infants born to mothers shedding CMV from the cervix or vagina.
• Up to 70% of sero-positive women shed CMV in breast milk

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Epidemiology I
CMV is found worldwide. In developed countries, the sero-prevalence of CMV is 40% to 60% in individuals of middle to upper socio-economic status, and <80% among those of lower socio-economic status.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Epidemiology II
Congenital infectionCongenital infection can occur as the result of a primary CMV infection, re-infection with a new strain of CMV, or reactivation of latent infection.
Maternal immunity to CMVMaternal immunity to CMV provides some protection against vertical transmission.
Infection in immediate pre-conception periodIf a primary CMV infection occurs in the immediate pre-conception period, the risk of transmission is around 9%.
Infection in 1st, 2nd, 3rd trimesterPrimary maternal CMV infection occurring in the first, second, and third trimester results in congenital infection in approximately 25%, 50% and 75% of foetuses respectively.
Infection after recurrent maternal infectionIn contrast, the risk of CMV transmission to the foetus after a recurrent maternal infection is only 0.15 to 2%.
However, despite the risk reduction preconception immunity affords, >60% of infants with congenital CMV are born to mothers with pre-pregnancy CMV immunity.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Epidemiology III - Maternal SeroprevalenceIncidence of congenital CMV infection increases with maternal seroprevalence. The incidence of congenital human CMV infection and maternal seroprevalance rates from published studies carried out in North America, Europe, South America and Africa were plotted as shown opposite.
Note that as the rate of maternal seroprevalence increases, so does the incidence of congenital CMV infection. This suggests a threshold level of immunity that would eliminate transmission within human populations may not be attainable [1].
Adapted from – Britt, W. 2008. “Manifestations of Human Cytomegalovirus Infection Proposed Mechanisms of Acute and Chronic Disease” in Current Topics in Microbiology and Human Immunology eds. Shenk, T E & Stinski, M F. Springer-Verlag, Berlin, 2008.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Features I
CMV primarily affects the cerebral ventricles, the ependymal cells, the organ of Corti, and the neurons of the eighth (vestibulocochlear) cranial nerve.
90% of congenitally-infected infants are reported to be asymptomatic at birth.
The remaining symptomatic 10% may demonstrate signs such as microcephaly, growth restriction and thrombocytopenia. Jaundice, petechiae, and hepatosplenomegaly are the most common findings.
Other clinical manifestations include…• Poly or oligohydramnios• Prematurity• Hypotonia• Poor feeding• Seizures• Cerebral ventriculomegaly• Intracranial periventricular
calcifications• “Blueberry muffin” spots• Sensorineural deafness
(10%)• Mental retardation (10-20%)
Other less frequent findings include…• Hydrocephalus• Pneumonitis• Haemolytic anaemia

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Features II
About 10% of infants with symptomatic congenital CMV infection die during early infancy because of multi-organ disease with severe hepatic dysfunction, bleeding diatheses, and secondary bacterial infections. However, infants asymptomatic at birth may also develop sensorineural hearing loss (7–15%), chorioretinitis and CNS malformations.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Features III - Clinical StudiesThe frequency of various clinical and laboratory findings in 106 neonates with symptomatic congenital CMV infection is illustrated in the table on the next slide.
• 68% of infants had at least one clinical finding suggestive of neurological impairment
• Petechiae, jaundice, and hepatosplenomegaly were the most frequently noted abnormalities, present in approximately 75% of symptomatic neonates
• Physiological unconjugated jaundice is generally very common in well neonates, thus identifying a raised conjugated bilirubin fraction in an otherwise asymptomatic infant is important
• Over half were microcephalic and small for gestational age, and about a third born prematurely
• About two-thirds of symptomatic infants had clinical neurological abnormalities such as microcephaly, lethargy/hypotonia, poor suck, or seizures
• Of the neonates who had ophthalmological assessments, chorioretinitis or optic atrophy was noted in 20%
• Of the babies who had audiological assessments, 50% were found to have an abnormal hearing screen

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Features IV – Clinical Studies
Adapted from Boppana SB et al. Newborn findings and outcome in children with symptomatic congenital CMV infection. Pediatr Res 1992.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Findings and Deficits IThe risk for neurological sequelae is increased when CMV infection occurs in the first trimester. The majority of infants with symptomatic congenital CMV infection at birth have evidence of central nervous system (CNS) impairment. The outcome and neurological deficits in 38 symptomatic congenital CMV infants are outlined in the table opposite.
Table adapted from Kylat RI, Edmond NK, Ford-Jones EL. Clinical findings and adverse outcomes in neonates with symptomatic congenital cytomegalovirus infection. Eur J Pediatr (2006) 16 5773-778.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Clinical Findings and Deficits II
Ocular manifestations secondary to congenital CMV include:- chorioretinitis - corneal
opacities- anterior polar cataracts - optic nerve
hypoplasia- optic nerve coloboma - (and even)
anophthalmia
Late onset neurologic symptoms include:- learning disability - cerebral palsy- sensorineural hearing loss (SNHL)
It is important to note that there is an unrecognised burden of CMV-associated neuro-disability in the paediatric population. The clinical findings and deficits listed in the table may be described as an 'unclassified' neurological syndrome in children with psychomotor retardation, with diagnoses often made retrospectively.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Sensorineural Hearing Loss
Of infants with asymptomatic congenital CMV infection at birth, 10% to 15% will go on to develop symptoms, typically manifested as sensorineural hearing loss (SNHL).
Congenital CMV infection is the most common non-genetic cause of SNHL in children. In the DECIBEL study, 23% of children with profound SNHL had congenital CMV infection. Permanent hearing loss occurs in approximately 14% of children with congenital CMV infection.
SNHL from congenital CMV can present later in childhood. However, symptomatic infection at birth appears to be much more likely to be associated with delayed SNHL than asymptomatic infection. Rates of delayed-onset hearing loss in symptomatic newborns are in the vicinity of 30- 35%.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Estimates of Long-term Sequelae in Infants with Congential CMV
In a given cohort of 1000 infants with congenital CMV, 170-190 will have permanent sequelae, of whom one out of three is from the symptomatic group and two out of three are from the asymptomatic group [2].
Adapted from Sung H & M R Schleiss. 2010. Update on the current status of human cytomegalovirus vaccines. Expert Review Vaccines 9 (11), 1303-1314
17-20% of all infants with congenital CMV will have
permanent sequelae.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Diagnosis I - Prenatal Diagnosis
Although the culture and polymerase chain reaction (PCR) of amniotic fluid for the detection of CMV or CMV DNA allows for prenatal identification of the majority of infected infants, the specificity of the PCR assay is only between 50 and 80%. The sensitivity of amniotic fluid culture or PCR is lower when the procedure is carried out before 21 weeks of gestation. However, the presence of CMV or CMV DNA in amniotic fluid and foetal blood samples does not appear to correlate with symptomatic congenital infection or an adverse long-term outcome in infected children.
Maternal sero-conversion is another strategy used to demonstrate acute maternal CMV infection. However, there is a high rate of false positives and false negatives. Current serological diagnostic methods utilising CMV-specific IgM require more specific evaluation.
Studies using ultrasonography, amniocentesis and fetal blood sampling have demonstrated that it is possible to make a prenatal diagnosis of congenital CMV infection. The variable prognosis of CMV infection limits the value of prenatal diagnosis.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Diagnosis II - Primary Maternal CMV Infection
Adapted from Nyholm J L & Schleiss M R. 2010. Prevention of maternal cytomegalovirus infection current status and future prospects. International Journal of Women’s Health 2010 225-35

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Diagnosis III - Microbiological DiagnosisCongenital CMV infection is proven by isolation (culture) of the virus from body fluids during the first 3 weeks of life.
Urine and saliva are useful for this purpose as neonates shed high levels of virus. PCR methods can also be used on urine and saliva samples, although these need further evaluation.
Viraemia is not present in all newborn infants with congenital CMV infection; therefore detection of virus in peripheral blood should not be relied upon to diagnose congenital infection. Detection of IgM antibody to CMV is not as reliable as viral isolation and is not recommended for diagnosis.
The age of the patient at the time of sample collection for detection of CMV is of some importance. Neonates who acquire CMV during birth or from breast milk shed virus after 3 weeks of age. Thus, detection of CMV in urine or saliva after 3 weeks of age is not unequivocal proof of CMV acquisition in utero.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Diagnosis IV - Laboratory DiagnosisThe laboratory abnormalities seen in infants with symptomatic congenital CMV infection include (in decreasing order of frequency):
• Elevated serum aspartate aminotransferase• Conjugated hyperbilirubinemia• Thrombocytopenia – Is noted in the first few days of life in the
majority of CMV-infected infants. This normalizes in most patients by the third week of life.
• Atypical lymphocytosis• Haemolytic anaemia• Elevated cerebrospinal (CSF) fluid protein – CSF protein levels
appear to correlate positively with clinical indicators of CNS damage.
Elevations of serum transaminases and conjugated bilirubin are present in the immediate newborn period and peak during the second week of life. However, hyperbilirubinemia and liver function abnormalities often persist beyond the neonatal period, resolving over a few months.
Invasive procedures such as liver biopsy are therefore not justified on the basis of persistent liver function abnormalities.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Diagnosis V – Sero-Diagnosis
• Sero-conversion from negative to positiveSimilarly, sero-conversion from negative to positive could be considered.
Pregnant women with an infectious mononucleosis-like illness could be detected this way with early testing, but this is unlikely to happen in obstetric practice.
• CMV-specific IgM in cord bloodThe diagnosis could also be established by the presence of CMV-specific IgM in cord blood or in the infant’s blood in the first 3 weeks of life.
This can be detected in only 70% of congenitally-infected infants, as the titres may rise only late in acute infection.
The diagnosis cannot be confirmed using CMV-specific IgG titre from cord blood as this may be a reflection of passive placental transmission.
Sero-diagnosis is also used in both maternal and neonatal CMV. There are certain parameters which would suggest evidence of CMV infection.
• Four-fold rise in anti-CMV IgG titres A four-fold rise in anti-CMV IgG titres would be suggestive, but this requires serial blood testing to demonstrate use

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Neuro-imaging IImaging findings of congenital CMV infection include intracranial calcification, ventriculomegaly, white matter disease, neuronal migrational disorders, lissencephaly and cortical atrophy.
Not all of these findings are seen in every patient, and abnormalities may range from mild to severe. In fact, unenhanced head CT results may be normal in as many as 68% of infants with symptomatic congenital CMV infection that was confirmed at birth. An abnormal CT scan is a sensitive indicator of poor cognitive outcome in symptomatic patients.
Intracranial calcification is the most frequently reported imaging finding of congenital CMV infection, occurring in 34%–70% of patients.Ventriculomegaly is the second most common and is often associated with cerebral volume loss.
White matter abnormalities are common in those with congenital CMV infection, occurring in as many as 22% of patients.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
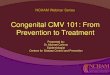
Neuro-imaging II
The 4 sample images demonstrate ventriculomegaly and scattered periventricular calcification. These radiological findings are consistent with intrauterine TORCH infection, such as CMV.
Image by Radswiki.net from Radiopaedia.org

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Treatment I
In some infants, there was even an improvement in audiometric parameters compared to untreated infants, of whom 41% showed auditory function deterioration.
However, at age 12 months, hearing had deteriorated in 21% of the treated infants. This suggests that 6 weeks of treatment may not be sufficient to prevent hearing loss.
Side-effects of ganciclovir therapy are thrombocytopenia, neutropenia, and gonadal toxicity.
Ganciclovir
Ganciclovir is a synthetic acyclic nucleotide analog of guanine which blocks viral DNA synthesis. It has been used for just under two decades in the treatment of congenital CMV.
There is only one large randomised controlled study of the effect of ganciclovir on hearing loss (Amir et al., 2010). The results showed that 6 weeks of intravenous ganciclovir prevented hearing deterioration at 6 months.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Treatment II
Given the observations of rebound viraemia and incomplete resolution of symptoms, clinical trials have been conducted looking at intravenous ganciclovir followed by long-term oral valganciclovir for the treatment of infants with symptomatic congenital CMV disease.
Passive immunisation with hyper-immune globulin (CMV HIG) has been studied for the in utero treatment and prevention of congenital CMV infection. CMV HIG is a pooled, high-titre immunoglobulin preparation derived from donors with high levels of CMV antibody. This intervention is still in early phase trials.
Valganciclovir
Valganciclovir is another guanine derivative which is a pro-drug of ganciclovir. It has been used as CMV prophylaxis in paediatric transplant recipients.
In some centres in the United States, treatment for symptomatic infants with congenital CMV has been either intravenous ganciclovir or valganciclovir.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Vaccines IA vaccine for congenital cytomegalovirus (CMV) infection is a public health priority. Analysis of cost–effectiveness indicates that a vaccine could have a major impact on the economic burden of paediatric neuro-disability caused by congenital CMV.
Like other herpes viruses, CMV has immune evasion genes which makes it difficult to develop appropriate vaccine targets. The vaccine table summarises CMV vaccines that have undergone clinical trial evaluation since 2005. A breakthrough came with the publication of a Phase II study of a purified, recombinant vaccine based on adjuvant glycoprotein B. This vaccine demonstrated an efficacy of approximately 50% against acquisition of HMV infection in a clinical trial among young women [4].
Novel approaches to CMV vaccines include vectored vaccines, DNA vaccines, bacterial artificial chromosome (BAC)-based vaccines, and genetically engineered, live attenuated vaccines. These vaccines are in various stages of pre-clinical and clinical development [2].

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Vaccines II
Vaccine table
Source Sung H & M R Schleiss. 2010. Update on the current status of human cytomegalovirus vaccines. Expert Review Vaccines 9 (11), 1303–1314.

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Key Points• Cytomegalovirus is a herpesvirus, and the commonest
congenitally-transmitted infection in the developed world
• Most infections are asymptomatic in both mothers and infants, although microcephaly, jaundice, and thrombocytopenia are common acute manifestations in the newborn
• The major long-term neurological sequelae of congenital CMV are sensorineural hearing loss, ophthalmic deficits, and general psychomotor retardation
• Isolation of the virus from bodily fluids is the mainstay of CMV diagnosis. Sero-diagnosis has numerous limitations
• Treatment with intravenous ganciclovir is recommended, with extended oral treatment with valganciclovir undergoing clinical trials
• Vaccines for CMV are currently being developed and tested. Pushes for more robust screening programmes for CMV remain controversial

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
SummaryHaving completed this session you will now be able to:
• Recognise the clinical signs of acute CMV infection in the newborn• Define both antenatal and postnatal diagnostic methods for
congenital CMV• Describe the treatment options for acute CMV infection in newborns• List the neurological sequelae of neonatal CMV infection in children• Discuss the potential public health measures which could reduce
CMV-associated neuro-disability in children
References
1. Britt, W. 'Manifestations of Human Cytomegalovirus Infection: Proposed Mechanisms of Acute and Chronic Disease' in Current Topics in Microbiology and Human Immunology eds. Shenk, T E & Stinski, M F. Springer-Verlag, Berlin, 2008.Kimberlin et al., 2003.
2. Sung & Schleiss, 2010.3. Kimberlin et al., 2003.4. Pass, Zhang, Evans et al., 20095. CDC. View.6. Neuroimaging of Pediatric Central Nervous System Cytomegalovirus
Infection

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Further Reading
• Nyholm J L & Schleiss M R. Prevention of maternal cytomegalovirus infection: current status and future prospects. International Journal of Women's Health 2010;2:25-35
• Boppana SB et al. Newborn findings and outcome in children with symptomatic congenital CMV infection. Pediatric Research. 1992;31:158A
• Britt, W. 'Manifestations of Human Cytomegalovirus Infection: Proposed Mechanisms of Acute and Chronic Disease' in Current Topics in Microbiology and Human Immunology eds. Shenk, TE & Stinski, MF. Springer-Verlag, Berlin. 2008
• Amir J, Wolf DG, Levy I. Treatment of symptomatic congenital cytomegalovirus infection with intravenous ganciclovir followed by long-term oral valganciclovir. European Journal of Pediatrics. 2010;169:1061–1067
• Fink KR et al. Neuroimaging of Pediatric Central Nervous System.Cytomegalovirus Infection. 2010. View
• Kimani R W et al. Sensorineural Hearing Loss in a Paediatric Population. Arch Otolaryngol Head Neck Surg. 2010;136(10): 999-1004
• Dollard SC, Schleiss MR, Grosse SD. Public health and laboratory considerations regarding newborn screening for congenital cytomegalovirus. J Inherit Metab Dis 33 2010;(Suppl 2):S249–S254
• Sung H & M R Schleiss. Update on the current status of human cytomegalovirus vaccines. Expert Review Vaccines. 2010;9(11), 1303–1314

CONGENITAL CYTOMEGALOVIRUS
• Learning Objectives• Introduction• Congenital Infections
• Microbiology• Epidemiology• Clinical Features• Clinical Findings and
Deficits• Sensorineural Deafn
ess• Long term Sequelae• Diagnosis• Neuro-Imaging• Treatment• Vaccines• Key Points• Summary• Further reading• Self Assessment
Self Assessment
Question 1
Which one of the following is a common neurological sequelae of neonatal CMV infection?
A. Spastic quadriplegia/hemiplegiaB. Sensorineural hearing lossC. Seizures/epilepsyD. Visual impairment

Liverpool Medical Institution, UK Provisional date: May 2013
NeuroID 2013: Liverpool Neurological Infectious Diseases Course
Ever struggled with a patient with meningitis or encephalitis, and not known quite what to do?Then the Liverpool Neurological infectious Diseases Course is for you!
For Trainees and Consultants in Adult and Paediatric Neurology, Infectious Diseases, Acute Medicine, Emergency Medicine and Medical Microbiology who want to update their knowledge, and improve their skills.
For more information and to REGISTER NOW VISIT: www.liv.ac.uk/neuroidcourse
• Presented by Leaders in the Field • Commonly Encountered Clinical Problems • Practical Management Approaches • Rarities for Reference • Interactive Case Presentations • State of the Art Updates • Pitfalls to Avoid • Controversies in Neurological Infections
To learn more about neurological infectious diseases…
Convenors: Prof Tom Solomon, Dr Enitan Carrol, Dr Rachel Kneen, Dr Nick Beeching, Dr Benedict Michael
Feedback from previous course:“Would unreservedly recommend to others” “An excellent 2 days!! The best course for a long time”



















![Case Report Symptomatic Congenital Cytomegalovirus Infection · 2016. 11. 5. · Ann Clin Cytol Pathol 2(5): 1035 (2016) 2/3. palsy [8], choreoretinitis with visual problems and epilepsy](https://img.pdfslide.us/doc/110x75/6147eb29a830d0442101bf2b/case-report-symptomatic-congenital-cytomegalovirus-infection-2016-11-5-ann.jpg)







