Embed Size (px)
Citation preview

Australian and New Zealand Journal of Ophthalmology 1986; 14: 79-84
CONGENITAL CATARACT SURGERY: A RETINAL SURGEON’S VIEWPOINT
DAVID McLEOD FRCS Surgrcal Vitreoretinal Unit. Moorfields €ye Hospital. London
Abstract Rhegmatogenous retinal detachments presenting man years after surgery for congenital cataracts frequently present formidable problems in management. d e techniques and results of treatment are being presented and the implications for modern-day congenital cataract surgery are discussed.
Key words: ???
Just as the range of surgical options in the management of senile cataract has greatly expanded in recent years, so also has the number of available techniques for the treatment of congenital cataract. Prior to the 1960s, congenital cataracts were managed either by multiple needlings or by extracapsular techniques like linear extraction. The reintroduction of “simple lens aspiration”’ (supplemented as necessary by capsulotomy) was a considerable advance, and this is still regarded as the treatment of choice for congenital cataracts by some anterior segment For a brief period in the 1970s, vitreoretinal surgeons became involved in congenital cataract management because of their familiarity with suction-cutting in~trumentation,~ and in some centres “lensectomy” has tended to replace “simple lens aspiration” for congenital cataracts.
The purpose of congenital cataract surgery, of course, is to create a clear optical pathway for vision and also to allow as accurate a refractive correction as possible. The indications for, and timing of, surgery depend on such factors as stimulus-deprivation amblyopia and problems of
optical correction after surgery, as discussed el~ewhere.~ Surgery should preferably result in as few complications as possible in the short and long term, complications such as corneal decom- pensation, glaucoma, persistent or recurrent capsular opacity, cystoid macular oedema and retinal detachment. This paper concerns only retinal detachment after congenital cataract surgery; although it is based on our experiences of lensectomy and also management of patients with retinal detachment after congenital cataract surgery, it is a somewhat theoretical discussion.
RETINAL DETACHMENT AFTER CONGENITAL CATARACT SURGERY Retinal detachment is a well-recognized compli- cation of congenital cataract surgery. Occasionally detachments occur within a relatively short time of surgery (within months) presumably related to vitreous traction exerted during the procedure. However, most detachments occur many years after surgery with an average delay of 20 to 30 years. Because of this delay, the overall frequency of this compli- cation has not been satisfactorily determined; an
~~ ~
Reprint requests: Dr David McLeod, Surgical Vitreoretinal Unit, Moorfields Eye Hospital, London ECIV 2PD, United Kingdom.
CONGENITAL CATARACT SURGERY: A RETINAL SURGEON’S VIEWPOINT 79

estimate of approximately 10% was made by Shapland,6 but this figure was not based on legitimate figures.
We have recently analysed the characteristics and results of surgery in 39 eyes with “congenital aphakic detachments” treated between January 1977 and August 1982.7 The detachments occurred almost exclusively in eyes operated prior to the introduction of simple lens aspiration with an average delay period between cataract surgery and retinal detachment of 28 years. Other characteristics of these detachments were as follows. 1. There was frequently a delay between the onset of symptoms and diagnosis of detachment because of difficulties in ophthalmoscopic visualization of the retina. B-scan ultrasound was often useful in confirming the diagnosis in difficult cases, and also illustrated other features of the detachment. 2. The detachments were rhegmatogenous in origin, with a variety of types of retinal break including flap tears at the posterior border of the vitreous base, and tears related to lattice degener- ation, paravascular or pigmented vitreoretinal adhesions and cystic tufts (operculated tears). 3. The detachments were always associated with posterior vitreous detachment as determined preoperatively by biomicroscopy or ultrasound, or intraoperatively during vitrectomy. 4. The eyes were generally axially myopic as judged by ultrasound or by refractive criteria (aphakic correction less than + 10 dioptres). 5. The management of the detachment was frequently problematical owing to difficulties in ophthalmoscopic visualization of breaks by virtue of lens remnants, corneal decompensation, nystagmus and so on. In two-thirds of the eyes, recourse to vitrectomy techniques was made, primarily to achieve good visualization of breaks, but also to permit internal drainage of subretinal fluid, tamponade of breaks and other micro- surgical manoeuvres. 6. The surgical results for this group of detachments, although reasonably good, were less satisfactory than those obtained in other types of retinal deta~hment.~
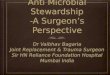
Figure I: Diagram of posterior vitreous detachment in an aphakic eye with posterior capsu- lotomy; dynamic traction operates at the posterior
border of the vitreous base.
7. There was a very high frequency (70%) of bilateral retinal detachment in patients who had previously undergone bilateral congenital cataract surgery.
In summary, retinal detachment after congenital cataract surgery has similar features to other aphakic detachments, being especially seen in axially myopic eyes but, in these patients, having an excessively long delay period between cataract surgery and detachment. Anterior vitreoretinal traction (fibrosis in the retrolental gel or vitreous incarceration), does not appear to have a direct role in the development of retinal breaks. The key event stimulating retinal detachment is complete posterior vitreous detachment (Figure l), and it is perhaps appropriate to review the mechanisms of posterior vitreous detachment relevant to congenital cataract patients.
Firstly vitreous detachment is generally a consequence of exaggerated syneresis of the vitreous gel which is an age-related phenomenon, in this case further accelerated by: (a) aphakia, possibly related to excessive loss of hyaluronic acid from the gel in the aphakic state;’ (b) axia, myopia, the eventual incidence which in congenital cataract patients is unknown, but there is no reason to believe that it is less frequent
80 AUSTRALIAN AND NEW ZEALAND JOURNAL OF OPHTHALMOLOGY

resulting in aphakic breaks, U-tears and giant retinal breaks; and (b) in relation to developmental vitreoretinal adhesions, such as lattice degeneration and cystic retinal tufts.
In summary, the relationship between retinal detachment and congenital cataract surgery is an indirect one via vitreous syneresis, posterior vitreous detachment, dynamic traction and vitreoretinal adhesions.
MODERN METHODS OF CONGENITAL CATARACT SURGERY It has long been recognized that intracapsular cataract extraction is inappropriate for congenital cataracts because of the problems of scleral collapse (inevitable with an “open-sky” approach to a young eye) and the strength of the adhesion between the vitreous and the posterior
Figure 2: Diagram of posterior vitreous detachment in an aphakic eye with incarceration of vitreous in a corneal incision; dynamic and static
traction on the vitreous base.
lens capsule in young individuals. Furthermore, needling and like procedures have now largely been abandoned in favour of the modern techniques: described below.
Closed Extracapsular Techniques These comprise removal of the anterior lens capsule and the lens substance, with preservation of the posterior lens capsule; they leave the vitreous inviolate (Figure 3).
than in the general population, and it may be more frequent; and (c) invasion of the gel by haemorrhage or inflammatory cells at the time of congenital cataract surgery.
Excessive syneresis in congenital aphakia is reflected in the frequent association with asteroid hyalitis. This specific form of gel degeneration is also seen in other conditions with exaggerated gel syneresis (for example, diabetes mellitus). The ensuing vitreous detachment is rhegmatogenous, that is, resulting from rupture of the premacular vitreous cortex and exchange of fluid from a lacuna into the retrohyaloid space.g
Secondly vitreous incarceration into surgical entry sites in the cornea in some eyes may have had some bearing on the induction of posterior vitreous detachment. Such incarceration may also be significant in its association with traction on the vitreous base region, which may well predispose this area to retinal break formation following vitreous detachment (Figure 2).
The excessive mobility of the detached gel mass induced by saccadic rotations (dynamic vitreoretinal traction) results in tearing of the retina at the posterior border of sites of persistent vitreoretinal adhesion: (a) at the posterior border of the vitreous base,
CONGENITAL CATARACT SURGERY: A RETINAL SURGEON’S VIEWPOINT
Figure 3: Diagram of attached vitreous in an aphakic eye after a limbal lensectomy (posterior
capsule intact).
81

Figure 4: Diagram of attached vitreous in an aphakic eye after limbal lensectomy and shallow
anterior vitrectomy.
Simple lens aspiration is effective in most cases, but is associated with difficulties in removing a thick anterior lens capsule or firm lens
In limbal lensectomy a vitreous suction-cutter is used instead of a simple aspiration device to remove a tough anterior capsule or hard lens material.
Unfortunately, capsular thickening from fibrosis occurs some time after lens removal in up to 90% of cases, necessitating capsulotomy.
Closed Vitreo-lensectomy In these techniques, not only is the anterior capsule and lens substance removed, but also the posterior lens capsule and a variable amount of vitreous (Figure 4).
With limbal vitreo-lensectomy, a vitreous suction cutter may be used as an extension of either simple lens aspiration or limbal lensectomy to remove the posterior capsule and anterior vitreous where, for example, a dense posterior subcapsular plaque cannot be adequately cleared from the pupillary axis or if the posterior capsule ruptures during aspiration, with herniation of gel into the anterior chamber. Some surgeons now routinely remove the posterior capsule and anterior vitreous in preference to capsu- lotomy,lO,ll so as to ensure clarity of the media
and as accurate a contact lens prescription as possible, thus mitigating against amblyopia.
The pars plana route (Pars plana lensectomy) is perhaps the most conducive to complete lens removal and offers easy access to the whole of the vitreous cavity; use of a corneal contact lens facilitates posterior vitrectomy and removal of any lens material dislodged posteriorly.
VITREORETINAL IMPLICATIONS OF CONGENITAL CATARACT SURGERY All modern-day methods of congenital cataract surgery offer the prospect of good ophthal- moscopic visualization of any retinal breaks causing retinal detachment (with the proviso that a small capsulotomy in a thickened posterior capsule may still cause some difficulties). What is essentially in question, however, is the effect of cataract extraction technique in influencing the initiation of later retinal detachment.
It can be safely assumed that those techniques which leave the posterior lens capsule and vitreous intact will not result in early retinal detachment. Subsequent capsulotomy is also likely to be trouble-free from the vitreoretinal viewpoint, although gel incarceration into the cornea has been reported. However, there is a risk of early detachment in both limbal vitreo-
Figure 5: Diagram of detached rim of cortical gel after pars plana lensectomy and posterior “core”vitrectomy; dynamic and static traction on
the vitreous base near surgical entry site.
82 AUSTRALIAN AND NEW ZEALAND JOURNAL OF OPHTHALMOLOGY

lensectomy and pars plana vitreo-lensectomy procedures. In both techniques, the use of high suction forces and/or an inefficient vitreous cutter may result in excessive traction on the vitreous base and retinal tear formation at surgery. Thus, limbal vitreo-lensectomy cannot be assumed to be an inherently safe technique; indeed, there is probably more destructive power by way of vitreoretinal traction in improper vitrectomy than anything our forbears could achieve using, for example, two discission needles.
Pars plana vitreo-lensectomy also carries with it the risk of entry-site complications, especially in small eyes where the pars plana has not fully developed. Not only is there a danger of disin- sertion of the oral retina at the time of instrument insertion (which must be checked for carefully at the end of the procedure by indirect ophthalmoscopy and scleral indentation), but, since any pars plana entry site constitutes a posterior segment penetrating injury and is inevitably associated with incarceration of basal vitreous into the wound, there is also a danger of tear formation postoperatively at the posterior border of the vitreous base in the vicinity of the entry site. In view of this risk, however small in most cases, we routinely carry out cryotherapy to the immediately post-oral retina over 30 O on each side of any pars plana entry site. It goes without saying that anyone proposing to operate through the pars plana must be prepared to examine the retinal periphery at the end of surgery and to perform any procedure necessary if retinal complications are identified.
It is most unlikely that any surgical technique for the removal of cataract can be regarded as being free of the risk of retinal detachment when one considers the patient’s whole lifetime. The absence to date of retinal detachment following simple lens aspiration probably reflects the very delayed onset of posterior vitreous detachment following this procedure (which was popularized only 20 years ago,” rather than indicating the inherent safety of the technique. Bearing in mind particularly the increasing popularity of vitreo- lensectomy (because it ensures a clear visual axis and facilitates accurate refraction), what are the
relative merits of various cataract-surgical techniques in determining the development of delayed retinal detachment (via posterior vitreous detachment)? Current experience suggests that, in the long term, most operated eyes will develop vitreous detachment “posterior capsule-intact” procedures having the longest delay, “lensectomy plus posterior vitrectomy” procedures having the shortest delay (sometimes only a matter of months), and “lensectomy plus anterior vitrectomy” and “aspiration plus capsu- lotomy” procedures an intermediate delay, all other factors (such as myopia and longevity) being equal. Is there, however, a critical mass of vitreous gel which maximizes the risk of retinal tear formation (via dynamic traction) after posterior vitreous detachment? If so, how much gel should be removed at the time of vitreo- lensectomy - a shallow anterior vitrectomy Gust enough to prevent fibrous-membrane formation in the iris plane) or as much gel as possible? G i ~ a r d ’ ~ . ’ ~ has implied that it is feasible to remove all the vitreous gel (other than the basal gel) at pars plana vitreo-lensectomy, and it might be predicted that the long-term risk of retinal detachment in such circumstances would be minimized. In our experience, however, only a “complete core vitrectomy” can be achieved in an eye with an attached vitreous, and even a very thin rim of mobile detached cortical gel (Figure 5 ) may produce a retinal break. Nevertheless, the more complete type of vitrectomy achievable through the pars plicata may eventually prove advantageous over anterior vitrectomy in reducing dynamic traction after vitreous detachment. There is also reason to suppose, however, that the basal gel incarcerations inevitably present after pars plana vitreo- lensectomy may, in fact, predispose the eye to retinal break formation after posterior vitreous detachment - possibly including giant break formation at the posterior border of the vitreous base. Prophylactic 360 O post-oral cryopexy should therefore be considered in such cases.
PROPHYLAXIS Monitored transcleral cryopexy at the presumed location of the posterior border of the vitreous
CONGENITAL CATARACT SURGERY: A RETINAL SURGEON’S VIEWPOINT 83

base immediately postorally (through 360 "), together with treatment of any identified abnormal vitreoretinal adhesions (lattice degeneration and cystic tufts), should be considered for: (i) fellow-eyes in patients suffering retinal detachment following bilateral congenital cataract surgery; (ii) axially myopic eyes after congenital cataract surgery; and (iii) those eyes in which vitreo-lensectomy is performed via the pars plana.
Such treatment is probably unnecessary if posterior vitreous detachment has already occurred without vitreoretinal complications.
ACKNOWLEDGEMENTS I am grateful to Miss Heather Lucas for secretarial assistance, and to Mr Terry Tarrant for the illustrations.
References 1. Scheie HG. Aspiration of congenital or soft cataracts:
a new technique. Am J Ophthalmol 1960; 5 0 1048-1056.
2. Rice NSC. Lens aspiration: a decade in retrospect. Trans Ophthalmol SOC UK 1977; 97: 48-51.
3. Rice NSC. (1982) Surgery of congenital cataracts: the choice of operative technique. In: Francois, Maumanee, Esente, eds. Cataract surgery and visual rehabilitation. The Hague: Junk, 1982: 141-143.
4. Peyman GA, Raichand M, Goldberg b. Surgery of congenital and juvenile cataracts: a pars piicata approach with the vitrophage. Br J Ophthalmol 1978; 62: 780-783.
5. Beller R, Hoyt CS, Marg E, Odom JV. Good visual function after neonatal surgery for congenital monocular cataracts. Am J Ophthalmol 1981; 91: 559-565.
6. Shapland CD. Retinal detachment in aphakia. Trans Ophthalmol SOC UK 1934; 54: 176-196.
7. Jagger JD, Cooling RJ, Fison LG, Leaver PK, McLeod D. Management of retinal detachment following congenital cataract surgery. Trans Ophthamol SOC UK (in press).
8. Osterlin SE. Biochemical changes in the vitreous of the aphakic eye. In Mod Probl Ophthalmol 1974; 12.
9. Eisner B. Biomicroscopy of the peripheral fundus. Berlin- Heidelberg-New York: Springer, 1973.
10. Taylor D. Choice of surgical technique in the management of congenital cataract. Trans Ophthalmol SOC UK 1981;
11. Parks MM. Posterior lens capsulotomy during primary cataract surgery in children. Ophthalmology 1983; 90: 344-345.
12. Girard LG. Pars plana lensectomy by ultrasonic fragmentation. In: Francois, Maumanee, Esente, eds. Cataract surgery and visual rehabilitation. The Hague: Junk, 1982: 171-177.
13. Girard LG. A versatile and simple technique for lens removal. Surv Ophthalmol 1982; 27: 96-101.
101: 114-117.
84 AUSTRALIAN AND NEW ZEALAND JOURNAL OF OPHTHALMOLOGY