Embed Size (px)
Citation preview
Confused about what to do with ear pus?
-Let’s discuss the evidence and our otitis externa study.
Introduction
Objectives Authors
Dr Caitlin Chidlow
Dr John van Bockxmeer, FACRRM/DEM, DMO Hedland Health Campus
No conflicts of interest to disclose, no funding for project
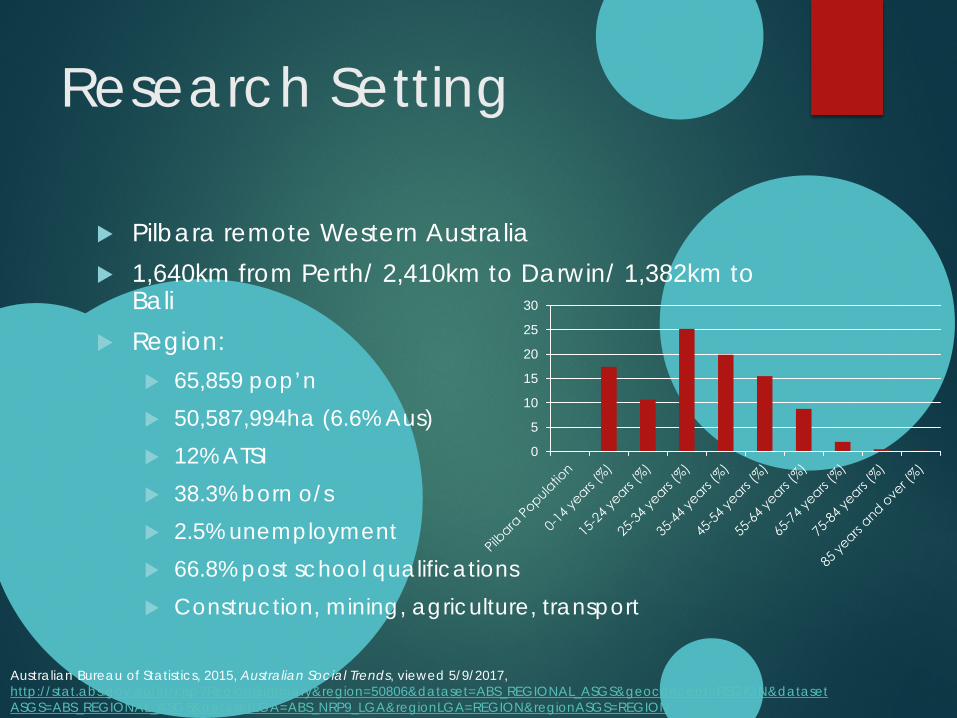
Research Setting
Pilbara remote Western Australia 1,640km from Perth/ 2,410km to Darwin/ 1,382km to
Bali Region:
65,859 pop’n 50,587,994ha (6.6% Aus) 12% ATSI 38.3% born o/s 2.5% unemployment 66.8% post school qualifications Construction, mining, agriculture, transport
0
5
10
15
20
25
30
Australian Bureau of Statistics, 2015, Australian Social Trends, viewed 5/9/2017, http://stat.abs.gov.au/itt/r.jsp?RegionSummary®ion=50806&dataset=ABS_REGIONAL_ASGS&geoconcept=REGION&datasetASGS=ABS_REGIONAL_ASGS&datasetLGA=ABS_NRP9_LGA®ionLGA=REGION®ionASGS=REGION
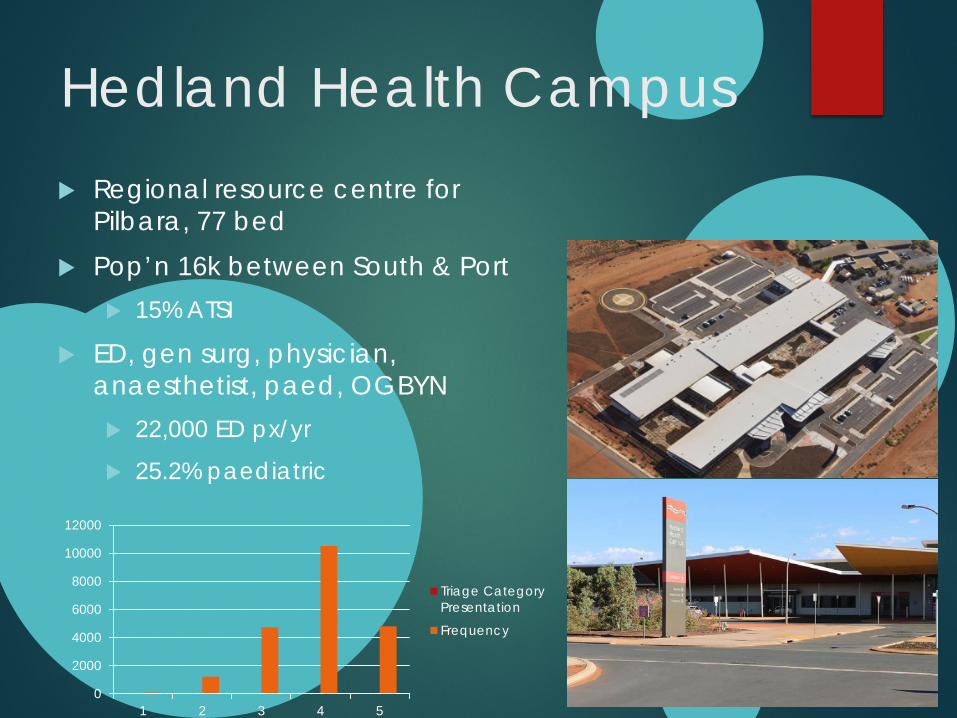
Hedland Health Campus Regional resource centre for
Pilbara, 77 bed Pop’n 16k between South & Port
15% ATSI
ED, gen surg, physician, anaesthetist, paed, OGBYN 22,000 ED px/yr
25.2% paediatric
0
2000
4000
6000
8000
10000
12000
1 2 3 4 5
Triage CategoryPresentation
Frequency
Otitis Externa
What is it? Inflammatory condition of external ear Characterised by pain. Patients may also have
itch, discharge, a feeling of fullness or hearing loss Acute diffuse otitis externa generally presents as a
superficial bacterial infection of the canal May also be fungal
Risk Factors
Also known as “Swimmer’s Ear” due to association with water activities
Common in warmer climates Increased in areas with higher humidity and more
water exposure from swimming Compromised skin barrier and changes to pH also
increases risk
Significance and Diagnostic Issues
Swabs may take several days to show result, longer if taken outside of hospital with micro facilities
Around 1% of presentations to ED each year Mobile population, many FIFO workers, people
visiting from remote communities, tourists passing through
Lots of differing guidelines
Research
Stimulus for research, cases & disease burden ‘What to do with ear pus??’
Objectives: Demographic data & representation
Overview of current practices and alignment with guidelines
Microbiology
Investigate seasonal trends
Research Method
15 month retrospective audit extract by Dx All patients px to HHC ED 1/12/15 through 1/4/17
Routine clinical care and data
Extracted from webPAS/ultra
Excel analysis
Ethics approval WACHS & WAAHEC
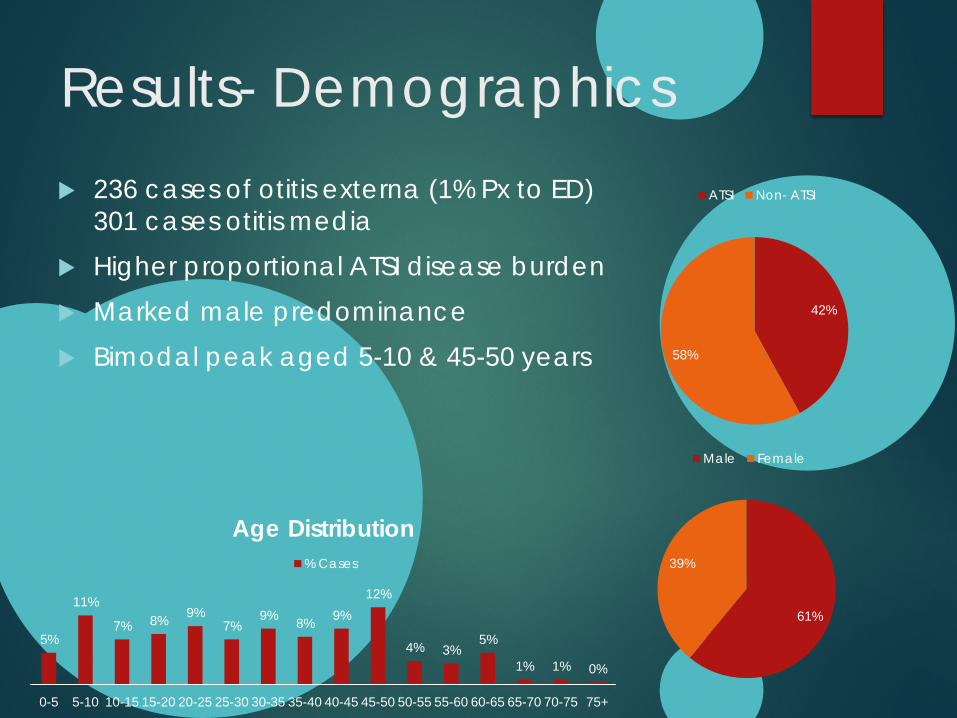
Results- Demographics 236 cases of otitis externa (1% Px to ED)
301 cases otitis media Higher proportional ATSI disease burden Marked male predominance Bimodal peak aged 5-10 & 45-50 years
42%
58%
ATSI Non- ATSI
61%
39%
Male Female
5%
11%
7% 8% 9% 7%
9% 8% 9% 12%
4% 3% 5%
1% 1% 0%
0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70 70-75 75+
Age Distribution % Cases
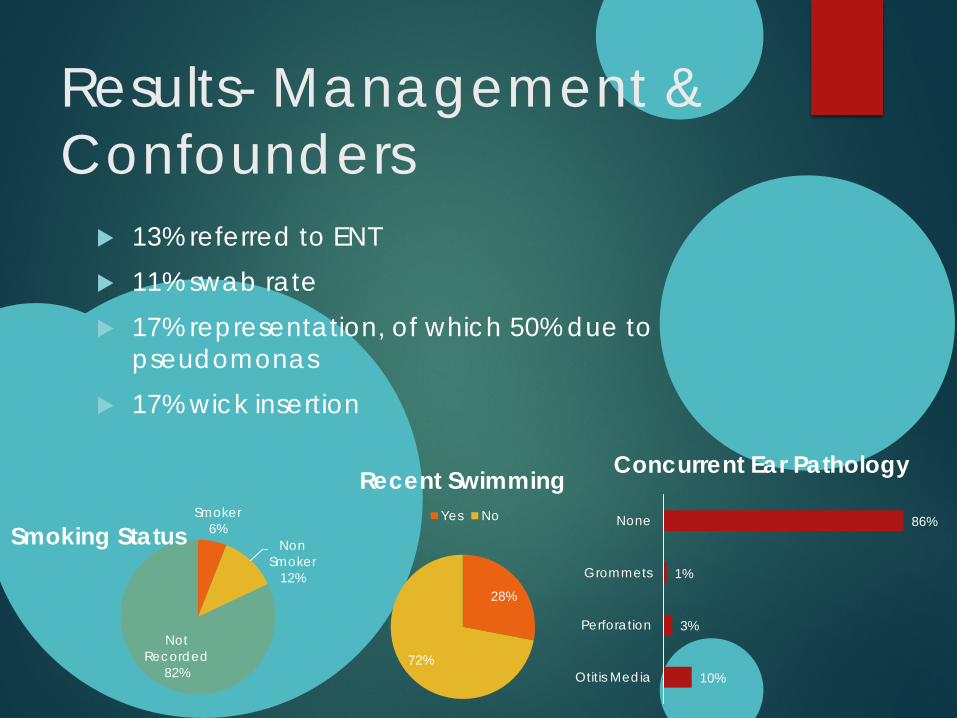
Results- Management & Confounders
13% referred to ENT 11% swab rate 17% representation, of which 50% due to
pseudomonas 17% wick insertion
28%
72%
Recent Swimming Yes NoSmoker
6% Non
Smoker 12%
Not Recorded
82%
Smoking Status
10%
3%
1%
86%
Otitis Media
Perforation
Grommets
None
Concurrent Ear Pathology
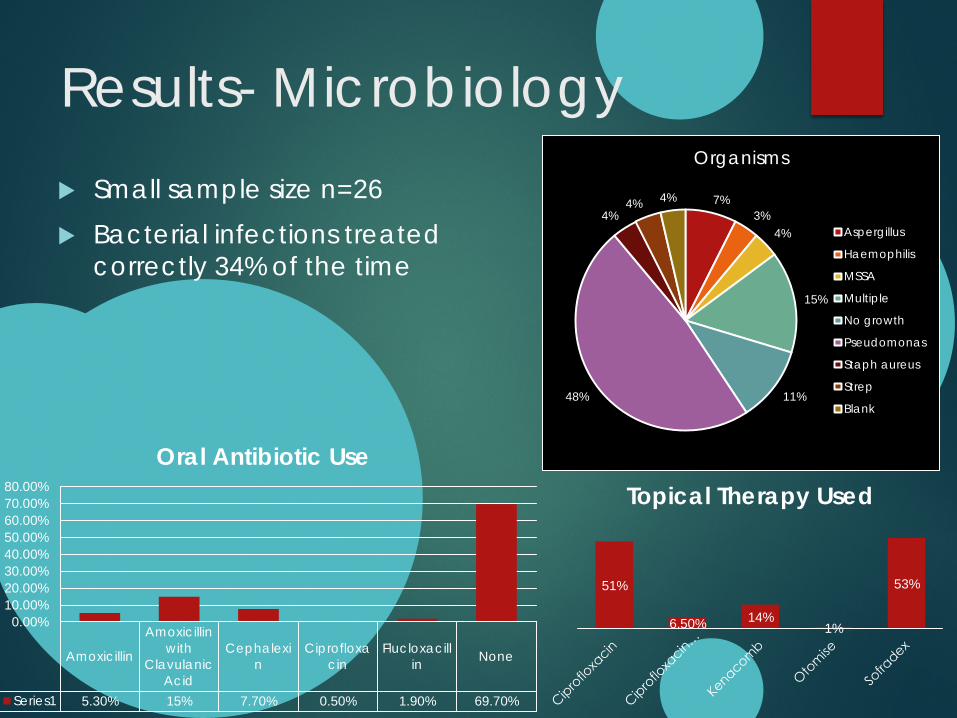
Results- Microbiology Small sample size n=26 Bacterial infections treated
correctly 34% of the time
7% 3%
4%
15%
11% 48%
4% 4% 4%
Organisms
Aspergillus
Haemophilis
MSSA
Multiple
No growth
Pseudomonas
Staph aureus
Strep
Blank
51%
6.50% 14% 1%
53%
Topical Therapy Used
Amoxicillin
Amoxicillinwith
ClavulanicAcid
Cephalexin
Ciprofloxacin
Flucloxacillin None
Series1 5.30% 15% 7.70% 0.50% 1.90% 69.70%
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%
Oral Antibiotic Use
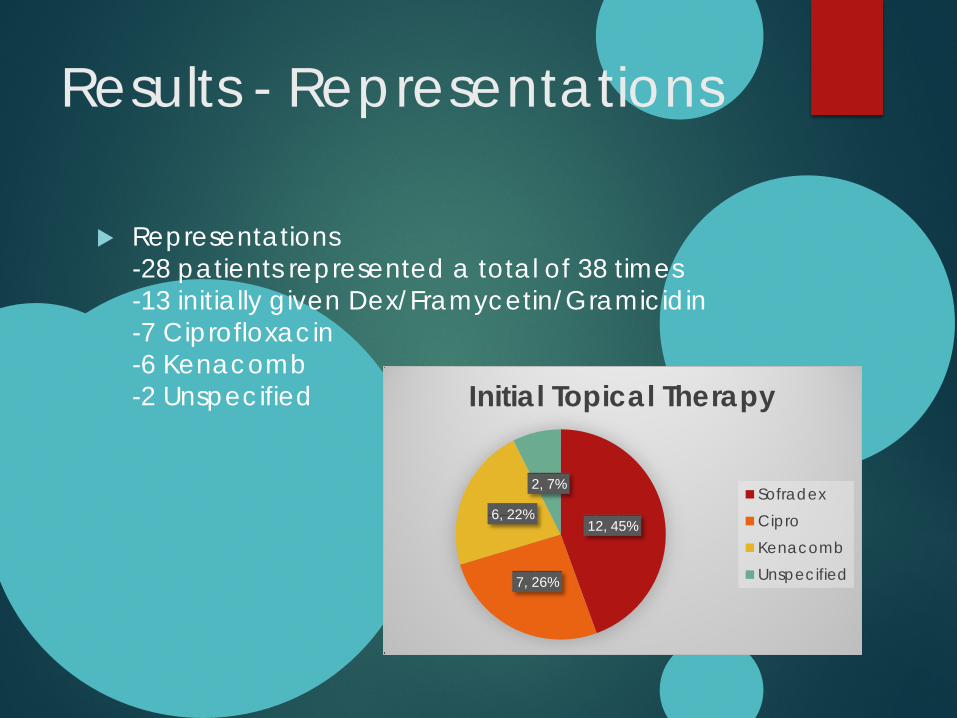
Results - Representations
Representations -28 patients represented a total of 38 times -13 initially given Dex/Framycetin/Gramicidin -7 Ciprofloxacin -6 Kenacomb -2 Unspecified
12, 45%
7, 26%
6, 22%
2, 7%
Initial Topical Therapy
SofradexCiproKenacombUnspecified
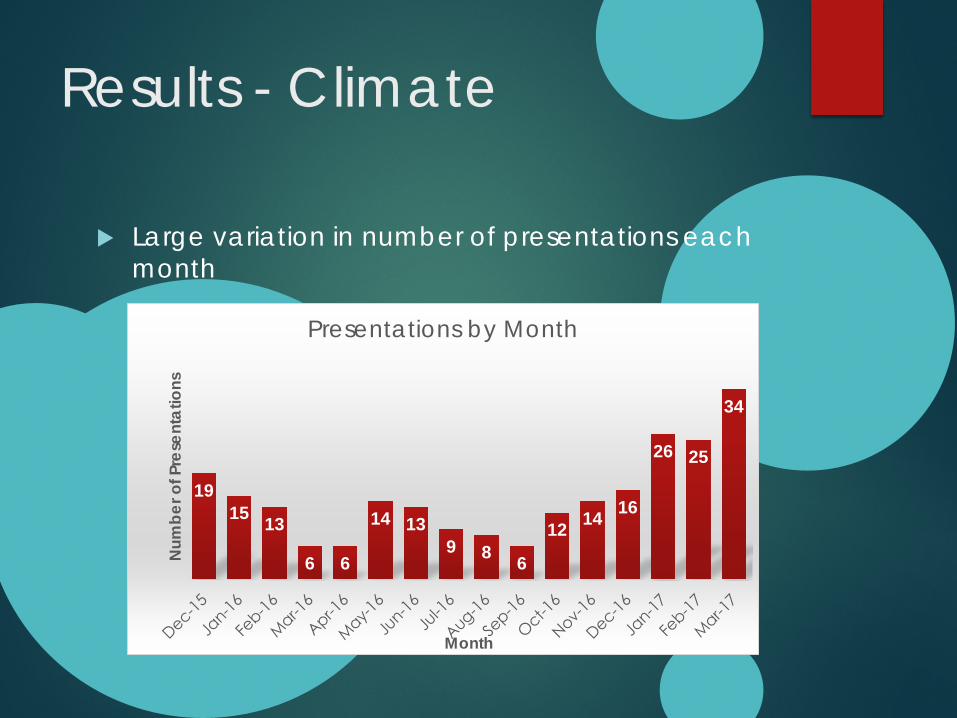
Results - Climate
Large variation in number of presentations each month
19 15 13
6 6
14 13 9 8 6
12 14 16
26 25
34
Num
ber o
f Pre
sent
atio
ns
Month
Presentations by Month
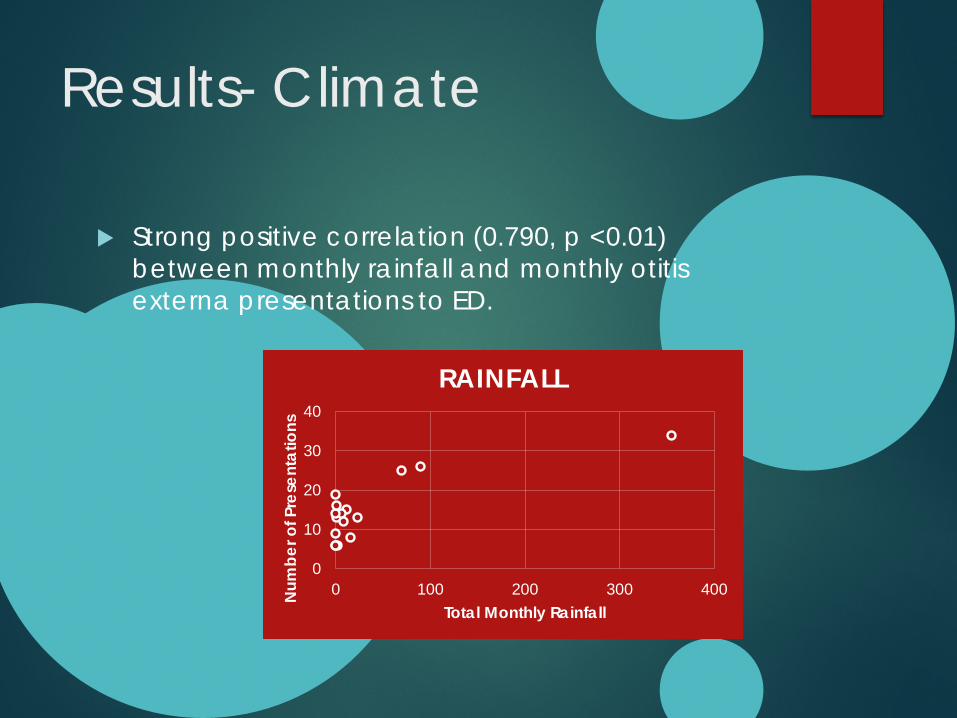
Results- Climate
Strong positive correlation (0.790, p <0.01) between monthly rainfall and monthly otitis externa presentations to ED.
0
10
20
30
40
0 100 200 300 400Num
ber o
f Pre
sent
atio
ns
Total Monthly Rainfall
RAINFALL
Results - Climate
Moderate association (0.54, p <0.05) with higher minimum temperatures and increased otitis externa presentation rates.
Association between maximum temperature and presentation rate not significant (0.200, p-value 0.457)
Guidelines & Adherence
We reviewed the most recent guidelines and systematic reviews on management of otitis externa including; Cochrane Collaboration 2010 review BMJ Best Practice Guidelines (UK) 2017 SAGE Clinical Practice Guidelines (USA) 2014
(American Academy of Otolaryngology) Australian Doctor 2007 Kids Health WA Guidelines 2013 Royal Children’s Hospital Guidelines 2009 Therapeutic Guidelines Australia 2014 Kimberley Aboriginal Medical Services 2014
Consensus Guidelines
Consensus no role for oral antibiotics in first-line management of uncomplicated AOE in immune competent patients
Avoid ototoxic drops in patients with perforations Simple oral analgesics first line for pain management Fungal infections should be cleaned
Both children’s hospitals recommend keeping ears
dry by avoiding swimming, ear plugs when showering to prevent further infections
Conflicting Guidelines
Antimicrobials SAGE and BMJ recommend quinolones over other drops KAMS recommended Cipro Therapeutic guidelines, RCH and Kids Health WA recommended
Dexamethasone/Framycetin/Gramicidin first-line Cipro HC only available on PBS for selected groups Aural Toilet KAMS recommended betadine irrigation and tissue spears Therapeutic guidelines recommended suction but said to avoid water RCH recommended ear toilet Kids Health WA recommended saline irrigation if no perforation present
Conflicting Guidelines
Fungal Infections Australian guidelines recommended anti-fungal
therapy first line whereas several international guidelines recommended acetic acid first line
Cochrane review showed acetic acid slightly less effective compared with other topical treatments for both bacterial and fungal infections
Topical Analgesics SAGE and Kids Health WA recommended the use of
topical analgesia if no perforation Other guidelines recommended avoiding topical
analgesics as they may limit effectiveness of antimicrobials
Conflicting Guidelines
Swabs Kids Health WA said swabs unhelpful RCH said swab everyone with discharge KAMS recommended taking both bacterial and
fungal swabs for everyone Wicks Nearly all guidelines recommended insertion of
ear wicks if canal obstructed or oedematous 2010 Cochrane review showed poor evidence
regarding benefit of ear wicks
How Do We Compare?
Dexamethasone/Framycetin/Gramicidin used in 45% of patients, Cipro or Cipro HC in 28%, Kenacomb in 12%
Kenacomb used for all fungal infections, no ascetic acid used.
11% of patients swabbed. Ear wicks documented in 16% of presentations.
Conclusions & Recommendations
No clear consensus guidelines Need for more region specific guidelines? Larger study to determine benefits of swabs to
guide therapy?
Further research Why is rainfall associated with more frequent otitis
externa presentations - ? More places to swim after heavy rainfall?
Further data needed to examine relationship between smoking status and otitis externa
Need to examine hearing protection as a cause of otitis externa

Recommendations
No need to swab patients If represent then treat for pseudomonas and take
fungal and bacterial swabs As a first line follow eTG guidelines and use
Dexamethasone/Framycetin/Gramicidin
Only use wicks if canals are really narrow and you are comfortable inserting them
Recommendations
In areas with high minimum temperatures and rainfall educate patients on risks of otitis externa and ear hygiene
Ciprofloxacin drops first line in Aboriginal children
Reinforce the need for OTC analgesia
Reinforce ear hygiene to patients, especially if fungal infections
Questions ?
Acknowledgements
We would like to formally acknowledge the Kariyarra People, traditional owners of the Port Hedland area, Hedland Health Campus Emergency Department, Wirraka Maya Health Service, WA Country Health Service and the WA Aboriginal Health Ethics Committee .
We would like to thank David Bath for his contribution to statistics and Dr Sarah Prunty for her guidance regarding current guidelines.

References
1. Rosenfeld RM, Schwartz SR, Cannon CR, Roland PS, Simon GR, Kumar KA, et al. Clinical Practice Guideline. Otolaryngology–Head and Neck Surgery. 2014;150(2):161-8.
2. Kaushik V, Malik T, Saeed SR. Interventions for acute otitis externa. Cochrane Database of Systematic Reviews. 2010(1).
3. Taplin MA. External Ear Conditions. Australian Doctor. 2007 April:25-32.
4. Cheffins T, Heal C, Rudolphy S, Evans R, Vietch C. Acute Otitis Externa – Management by GPs in North Queensland. Australian Family Physician. 2009 April: 262-266
5. Otitis Externa. Therapeutic Guidelines. 2014 6. Acute Otitis Externa. BMJ Best Practice. 2017 7. Coates H. Ear drops and ototoxicity. Australian Prescriber.
Issues. 2008:1.