Embed Size (px)
Citation preview

Rawlinson et al. Vol. 17, No. 3 /March 2000/J. Opt. Soc. Am. A 477
Confocal laser scanning ophthalmoscopeand spherical harmonics used
as a possible aid to detect glaucoma
Andrew A. Rawlinson, Viviene Cucevic, and Keith A. Nugent
School of Physics, University of Melbourne, Parkville, Victoria 3052, Australia
Anne M. V. Brooks
The Royal Victorian Eye and Ear Hospital, East Melbourne, Victoria 3002, Australia
Anthony G. Klein
School of Physics, University of Melbourne, Parkville, Victoria 3052, Australia
Received February 4, 1999; revised manuscript received July 28, 1999; accepted October 1, 1999
We present a procedure whereby the confocal laser scanning ophthalmoscope can be used to extract informa-tion about the three-dimensional structure of the central excavated area or the cup of the optic nerve head ofthe eye. The data are analyzed in terms of spherical harmonics. It is hypothesized that the shape of the cupof the optic nerve head for a normal eye can be parameterized by a specific set of spherical harmonic coeffi-cients and is different from the set of coefficients describing a glaucomatous eye. The sets of coefficients areanalyzed by using multivariate statistics and can in turn be used to classify new observations. Preliminaryresults indicate that there are significant differences in the coefficients and that the procedure might havepotential as a diagnostic aid for the detection or the screening of glaucoma. © 2000 Optical Society of America[S0740-3232(00)01402-2]
OCIS codes: 170.0170, 170.1610, 170.4460.
1. INTRODUCTIONGlaucoma is an optic neuropathy that can cause varyingdegrees of visual loss in the individual. Glaucoma is fre-quently associated with a rise in the intraocular pressure,which is a function of the production of aqueous humour,which circulates through the anterior chamber of the eyeand drains out through a drainage mechanism. Resis-tance to the outflow of the aqueous fluid maintains a cer-tain level of intraocular pressure that is necessary to theproper functioning of the eye. An increase in this resis-tance will lead to a rise in the intraocular pressure (IOP),which in turn can affect the function of the optic nerve atits exit from the eye—the optic nerve head (ONH)—causing destruction and atrophy of nerve tissue.
It is this atrophy that causes the visual loss in glau-coma. It is characterized by a change in the normal ex-cavation or the cup of the ONH. This process may occurin some patients in the absence of a rise in the IOP, per-haps because of some other abnormality that makes thepatient particularly liable to the effect of IOP. Even inthe normal eye, IOP is much higher than normal tissuepressure elsewhere.
Because of this, IOP alone is a poor screening measurefor the detection of glaucoma.
It is possible that loss of nerve fibers occurs before ac-tual visual loss can be demonstrated1; this may be accom-panied by a change in the cupping of the optic disk. Atest that detects early changes in the optic disk that are
0740-3232/2000/030477-07$15.00 ©
due to glaucoma would enable early diagnosis and the im-mediate institution of treatment, giving a much more sat-isfactory outcome.
Many patients with glaucoma may be unaware of thesubtle onset of the disease, which initially may onlymildly affect vision, and if pressure is elevated, this isusually asymptomatic. However, the cupping of the opticdisk often does change early, and this may enable anearly diagnosis that is not dependent on pressure.
Parameterizing the shape of an object requires infor-mation about its three-dimensional (3-D) structure. Theadvent of the confocal laser scanning ophthalmoscope(CLSO) allows one to take a series of images of the ONH,each of a different focal depth, and then combine them toform a 3-D image of the shape of the ONH as a contour orsurface graphic.
The shape of an object can be expressed mathemati-cally as a linear combination of a suitable set of orthogo-nal functions. Given that the shape of the ONH isroughly hemispherical, we have chosen to use the spheri-cal harmonics Ylm(u, f). Such a procedure has recentlybeen put forward by Cucevic et al.2 It is envisaged that aclear distinction in the shape of the ONH for normal andglaucomatous eyes will show up as different values for thespherical harmonic coefficients in each class of eyes.
Multivariate statistical techniques are employed to findsuch differences between the normal and glaucomatousgroups and also to classify new data. Early indications
2000 Optical Society of America

478 J. Opt. Soc. Am. A/Vol. 17, No. 3 /March 2000 Rawlinson et al.
suggest that this objective procedure could be used as anaid in the detection of glaucoma.
Certain conditions should be observed regarding thequality of the data to ensure that there is sufficient infor-mation about the topography of the ONH. When usingthe CLSO, one finds that blood vessels in some eyes canobstruct the ‘‘view’’ of the ONH, although it is appreciatedthat the condition of blood vessels in itself can give someinformation about glaucoma. This leads to a loss of acomplete view of the ONH and in turn a misleading set ofdata for the shape of the ONH for that eye. Also, exces-sive noise in the data or appreciable tilting of the retinalplane can distort the true values of the spherical har-monic coefficients. Ideally one should only use imageswhere these effects are minimal.
Others3–5 have carried out multivariate analyses by us-ing different sets of variables, such as cup–disk ratios,rim areas, and the axial length of the eye. One analysis6
used these variables in addition to responses to questionssuch as ‘‘Is there a family history of glaucoma?’’ which aregraded as 0 for ‘‘not present,’’ 1 for ‘‘suspicion,’’ 2 for ‘‘pres-ence,’’ as variables on which to base a multivariate analy-sis. We base our multivariate analysis entirely on a setof spherical harmonic coefficients.
The outline of the paper is as follows. Section 2 intro-duces the spherical harmonics and how they can be usedin describing the shape of the ONH. Section 3 gives abrief outline of how one computes the various sphericalharmonic coefficients for a particular shape; statisticalanalysis of the data is presented in Section 4, followed bya discussion in Section 5 and the conclusion in Section 6.
2. ORTHOGONAL POLYNOMIALSA closed surface in spherical polar coordinates can bespecified by a radial coordinate r(u, f) representing thedistance from the origin to the point of interest on the sur-face for given angular variables u and f. This surfacecan be expressed as a sum of spherical harmonicsYlm(u, f) (Ref. 7):
r~u, f! 5 (l50
`
(m52l
l
ClmYlm* ~u, f!, (1)
where, for m > 0,
Ylm~u, f! 51
2 ll! F2l 1 1
4p
~l 2 m !!
~l 1 m !!G1/2
exp~imf!
3 ~2 sin u!mdl 1 m
d~cos u!l 1 m ~cos2 u 2 1 !l (2)
and, for m , 0,
Yl,2m~u, f! 5 ~21 !mYlm* ~u, f!, (3)
where we have used the normalization condition
E0
p
du sin uE0
2p
dfYlm~u, f!Yl8m8* ~u, f! 5 d ll8dmm8 . (4)
The coefficients Clm parameterize the surface in termsof spherical harmonics and are given by
Clm 5 E0
2p
dfE0
p
du~sin u!r~u, f!Ylm~u, f!. (5)
This represents the contribution of the specific Ylm(u, f)to the surface.
If the closed surface exhibits a reflection symmetry inthe (x, y) plane, i.e.,
r~p 2 u, f! 5 r~u, f!, (6)
one can break up the u integration into two parts:
E0
p
du~sin u!f~u, f! 5 E0
p/2
du~sin u!f~u, f!
1 Ep/2
p
du~sin u!f~u, f!. (7)
Letting u8 5 p 2 u, we can rewrite the second term as
Ep/2
p
du~sin u!f~u, f! 5 E0
p/2
du8sin~p 2 u8!f~p 2 u8, f!,
(8)
where
f ~p 2 u8,f! 5 r~p 2 u8, f!Ylm~p 2 u8, f! , (9)
and we note that
Ylm~p 2 u, f! 5 ~21 !l1mYlm~u, f!. (10)
Hence Eq. (5) becomes
Clm 5 @1 1 ~21 !l1m#
3 E0
2p
dfE0
p/2
du~sin u!r~u, f!Ylm~u, f!,
(11)
and we immediately see that, as a consequence of the re-flection symmetry,
Clm 5 0 if l 1 m is odd. (12)
Also, r(u, f) is real, i.e.,
r~u, f! 5 @r~u, f!#* , (13)
and using Eq. (3), we then have
Cl,2m 5 ~21 !mClm* . (14)
Equations (12) and (14) are the important results of theproperties for the coefficients Clm . As a result, it is suf-ficient to evaluate Clm for m > 0.
We also note that since Y00(u, f) 5 1/2Ap, we canwrite
C00 5 2Ap^r&, (15)
where ^r& is the average value of the radial coordinateover the integration range. C00 represents the purehemispherical contribution to the shape, and the higher-order spherical harmonic coefficients contribute to the de-parture of the shape from the basic hemisphere.

Rawlinson et al. Vol. 17, No. 3 /March 2000/J. Opt. Soc. Am. A 479
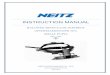
3. NUMERICAL ANALYSISImage data was gathered by using the Zeiss CLSO, theoutput of which produces an extended focus image and adepth image, as shown in Fig. 1. The Zeiss CLSO uses a633-nm He–Ne laser beam to scan the retina. The beamis characterized by a spot size of 10 mm, a power of 150mW, and a scan time of 0.32 s. The output data consist of672 3 576 pixels in eight planes separated by 100 mmeach. Its operation is based on the confocal principle,8,9
whereby the scattered return light from the focal spot ispassed through a pinhole at the conjugate focus of the in-strument. This isolates the light that comes from a par-ticular plane and largely rejects the light that originateseither in front of or behind the plane being measured atthat time. Eight different positions of the confocal pin-hole give an image slice in each of the eight planes men-tioned; the output data are, therefore, a 3-D block of datarepresenting a 3-D image of the area of the optic disk un-der observation.
The software with the Zeiss CLSO then allows one toextract information relating to the topography of the op-tic. The details of the programming of the software werenot available, but the principle is to identify the brightestpoint in a scan in depth as corresponding to a point on thesurface of the optic disk. Thus a quantitative two-dimensional image of the topography of the optic disk isreturned, and these were the data used in this study.
The accuracy and the reproducibility of the Zeiss CLSOhave been reported previously.2,10 Unlike the HeidelbergRetina Tomograph,11 it is not dependent on an observerboth to manually trace the contour of the disk margin andto choose the reference topography from which others arecalculated.
The depth image can be viewed as a surface graphic de-picting the shape of the ONH, which roughly looks like aflat region with a cuplike or hemispherelike shape in thecenter. The surface z(x, y) gives the depth z of the cup atthe coordinate (x, y). As there is generally noise in thedata, the data are smoothed by using the boxcar method,
where the value of the cell is replaced by the average overa 3 3 3 or 5 3 5 celled array centered on that cell.
To perform a spherical harmonic decomposition, we re-quire a closed surface, so a mirror reflection is performedin the (x, y) plane of the cup-shaped object to get a closedsurface. Thus a reflection symmetry is imposed on thesystem. This is the closed surface that we choose to rep-resent as a linear combination of spherical harmonicsYlm(u, f).7
The z(x, y) data consist of z values (depth) on an (x, y)grid of 640 3 549 points. A decision has to be made as towhere to place the origin of the coordinate system, as thiswill affect the Clm . Ideally, the origin of the (x, y) planeshould be directly above or below the deepest point of thecup. The origin of the z axis depends on where one placesthe (x, y) plane in such a way that the cup can be re-flected in this plane, giving a closed surface. The flat re-gion of the image should ideally be parallel to the (x, y)plane, yet some images exhibit noticeable tilting with re-spect to the (x, y) plane, with the result that the origin ofthe z axis has to be moved deeper into the cup. This inturn reduces the size of the shape to be analyzed and af-fects the values of the Clm .
Having chosen the origin of the coordinate system, weselect a 401 3 401 grid of points and center it at the ori-gin. The data are then converted from Cartesian to polarcoordinates, and the resulting cup is reflected in the (x, y)plane to give a closed surface.
A grid of usteps 3 fsteps points is set up for u P @0, p/2#and f P @0, 2p#, respectively. For a given u and f, theremay be more than one surface point, in which case an av-erage of all the possible r(u, f) is taken—this is primarilycaused by blood vessels and noise in the data. Also, theremight be an occasion where a surface data point at spe-cific angles is absent, in which case an interpolation be-tween nearby angles is carried.
The spherical harmonic coefficients Clm are now evalu-ated by using Simpson’s rule for numerical integration.For numerical purposes one imposes an upper limit forthe l sum in Eq. (1):
Fig. 1. Extended focus (left) and depth (right) images of a glaucomatous eye, obtained from the CLSO.

480 J. Opt. Soc. Am. A/Vol. 17, No. 3 /March 2000 Rawlinson et al.
r~u, f, lmax! 5 (l50
lmax
(m52l
l
ClmYlm* ~u, f!
5 (l50
lmax H (m51
l
2 Re@Clm* Ylm~u, f!#
1 Cl0Yl0~u, f!J . (16)
How well the reconstructed surface compares with thedata can be assessed by computing the variance for vari-ous values of lmax 5 0, 4, 10 to see how the addition ofhigher-order spherical harmonics improves the fit to thesmoothed raw data:
s 2~lmax! 5
(i50
usteps
(j50
fsteps
@rdata~u i , f j! 2 r~u i , f j , lmax!#2
ustepsfsteps,
(17)
where we have chosen usteps 5 200 and fsteps 5 400.This means that for a given lmax the departure of the fit-ted surface from the actual surface, on the average, is ap-proximately Dr(lmax) ; As 2(lmax) units at each point onthe surface. Many images yield a value of C00 in therange of 200–400. Using Eq. (15), we find that this cor-responds to ^r& ranging from approximately 60 to 120, sothat s 2(10) 5 100 corresponds to Dr(10) ; 10, implyingan error in the fit on the order of 10%. One finds, in gen-eral, for l Þ 0 that the magnitudes of the Clm are lessthan approximately 25% of C00 and decrease as l in-creases. For the particular eye in Fig. 1, we find thats 2(lmax) 5 248.6, 14.3, 4.8 for lmax 5 0, 4, 10, respectively,so we see that the addition of higher-order spherical har-monics improves the fit to the data. A contour plot of thesurface rdata(u,f) obtained from the data of the depth im-age of Fig. 1 is displayed in Fig. 2, and a contour plot ofthe reconstructed surface based on spherical harmonics,r(u,f,10), is shown in Fig. 3.
Fig. 2. Contour plot of the depth image in Fig. 1.
For many patients both left and right eyes are scanned.We have adopted the left eye as the standard eye andthus convert all right eyes into left eyes. To obtain a lefteye from a right eye, one makes a reflection in the y –zplane:
rL~u, f! 5 H rR~u, p 2 f! for 0 < f , p
rR~u, 3p 2 f! for p < f , 2p, (18)
where the superscripts R and L denote the coefficients forthe right and left eyes, respectively. The coefficients arethen related by
ClmL 5 Clm
R* . (19)
4. MULTIVARIATE ANALYSISWe have chosen to analyze the spherical harmonic coeffi-cients Clm by using multivariate analysis techniques12
with the Minitab 10.5 Xtra13 statistics package, which al-lows one to separate distinct groups of eyes—normal andglaucomatous—by finding differential features. This in-formation is encapsulated in the linear discriminant func-tion (LDF) for each group. The use of the LDF reducesthe dataset of a multivariate population to that of aunivariate population. Once the LDF’s are derived, onecan proceed to classify new observations into one of thetwo groups of eyes.
Given the following properties of the spherical har-monic coefficients—Cl0 are real, Clm are complex forl Þ 0 and m Þ 0, Clm 5 0 if l 1 m is odd, and only Clmsuch that m > 0 are needed (see Section 2)—we shalltreat the real and imaginary parts as distinct variables,or predictors, when carrying out the multivariate analy-sis.
An observation is specified by a set of predictors interms of the spherical harmonic coefficients through thevector C:
C 5 ~C00 , C11r , C11
i , C20 , C31r , C31
i ,...,
Clmaxlmax
r , Clmaxlmax
i !, (20)
Fig. 3. Contour plot of spherical harmonic reconstruction of thedepth image in Fig. 1.

Rawlinson et al. Vol. 17, No. 3 /March 2000/J. Opt. Soc. Am. A 481
where the superscripts r and i refer to the real and imagi-nary parts of the coefficients, respectively. If one chooseslmax 5 4, we have three real (when l 5 0, 2, 4 and m5 0) and six complex (when m Þ 0 and l 1 m is even)coefficients, giving a total of 3 1 2 3 6 5 15 predictors.Similarly, one finds for lmax 5 10 that there are 66 predic-tors.
First, we must use calibration data, consisting of obser-vations that are known to be clinically diagnosed as nor-mal or glaucomatous, to compute the means ^C& j and thecovariance matrices S j of the predictors for each group j( j 5 N or G for normal and glaucomatous, respectively):
S j 5 ^~C 2 ^C& j!8~C 2 ^C& j!& (21)
where the prime, denotes the transpose of a matrix. Thepooled covariance matrix S is now defined by
S 5~nN 2 1 !SN 1 ~nG 2 1 !SG
nN 1 nG 2 2, (22)
where nj is the number of observations for group j.Then, given the ^C& j and S from the calibration data,
one can define the squared distance of a new observationCnew from the centroid of each group ^C& j by
dj2~Cnew! 5 ~Cnew 2 ^C& j!S
21~Cnew 2 ^C& j!8
5 22~^C& jS21Cnew8 2 0.5^C& jS
21^C& j8!
1 CnewS21Cnew8
5 22LDFj~Cnew! 1 CnewS21Cnew8 , (23)
where we have used the fact that the covariance matrix issymmetric, and the LDF’s are defined by
LDFj~Cnew! 5 ^C& jS21Cnew8 2 0.5^C& jS
21^C& j8 . (24)
We can rewrite this as
LDFj~Cnew! 5 KjCnew8 1 Kjconst , (25)
where
Kj 5 ~Kj00 , Kj11r , Kj11
i , Kj20 , Kj31r , Kj31
i ,...,
Kjlmaxlmax
r , Kjlmaxlmax
i ! 5 ^C& jS21,
Kjconst 5 20.5^C& jS
21^C& j8 (26)
are evaluated by using the means of the predictors of eachgroup and the pooled covariance matrix of the calibrationdata.
One can now use Eq. (23) or (24) to classify new obser-vations by evaluating dj
2(Cnew) [or LDFj(Cnew)] for bothgroups j 5 N, G. The group that yields the smaller dj
2
(or the larger LDFj) classifies that observation.
5. RESULTS OF MULTIVARIATE ANALYSISClinical diagnosis of glaucoma was made by two indepen-dent observers as described previously,2 with glaucoma-tous cupping assessed, by using the criteria of Kirsch andAnderson.14 It was decided to consider three groups ofclinically diagnosed eyes as follows:
• Group 1, consisting of 34 normal eyes from 18 malesand 16 females, aged 53 6 15 yr (mean 6 standard devia-
tion) (range 20–79 yr) with normal optic disks, normalfull threshold 24–2 Humphrey computerized visual fields[mean deviation (MD), 20.81 6 1.41; corrected-patternstandard deviation (CPSD), 1.09 6 0.63] and IOP< 21 mm Hg; 31 glaucomatous eyes from 17 males and14 females, aged 68 6 14 yr (range 24–86 yr) with glau-comatous cupping of the optic disk, typical glaucomatousvisual field loss on full threshold 24–2 Humphrey comput-erized visual fields (MD, 213.77 6 9.49; CPSD, 6.056 3.16) and IOP.21 mm Hg. Each eye had s 2(10)& 100. These were the calibration data used to derivethe LDF’s for normal and glaucomatous eyes.
• Group 2, consisting of 20 normal eyes from sevenmales and 13 females, aged 47 6 17 yr (range 18–81 yr),24 glaucomatous eyes from nine males and 12 females,aged 73 6 9 yr (range 57–86 yr), and 19 ocular hyperten-sive (OHT) eyes from five males and 11 females, aged 646 11 yr (range 47–81 yr) with normal optic disks, normalfull threshold 24–2 Humphrey computerized visual fieldsand IOP.21 mm Hg. Each eye had s 2(10) & 100. TheLDF’s based on group 1 are used to predict, or classify,the status of these eyes.
• Group 3, consisting of 16 normal eyes from threemales and nine females, aged 65 6 17 yr (range 23–84 yr)and ten glaucomatous eyes from eight males and twofemales, aged 74 6 12 yr (range 58–93 yr), each with100 & s 2(10) & 600. Again, the LDF’s are used to pre-dict, or classify, the status of these eyes.
In deriving the LDF’s, we used only one eye of each pa-tient in group 1, even though the spherical harmonic co-efficients of both eyes of the same patient are, in general,quite varied. For classification purposes, as for groups 2and 3, both eyes of the same patient could be used.
We considered LDF’s of differing values of lmax5 1 ,..., 10 and found that the success rate for classifyingnew observations increases as lmax increases, reaching anoptimal point at approximately lmax 5 4. Increasing lmaxto 10 did not change the success rate appreciably; henceit was decided to use lmax 5 4 so as to minimize the needfor higher-order spherical harmonics, which might be in-fluenced by blood vessels and noisy data rather than bychanges in the shape of the excavated cup of the ONH.Choosing lmax 5 4 gives us a set of 15 predictors on whichto carry out the multivariate analysis. The coefficientsfor the LDF’s are displayed in Table 1 for the case wherelmax 5 4, where the squared distance between the cen-troids of the two groups is 9.29.
The results of the multivariate analysis are displayedin Table 2. For group 1 the cross-checking process inMinitab, where dj
2 is evaluated for each eye in the calibra-tion data and then classified according to which of dN
2 ordG
2 is smaller, considered two of the 31 glaucomatous eyesand two of the 34 normal eyes as misclassifications,meaning that the spherical harmonic coefficients of a mis-classified eye perhaps more closely resembled the class inwhich it has not been classified. This gives a successfulclassification rate of 94%. Not having a 100% successrate indicates an overlapping in the range of values ofsome predictors of each group. In many biological sys-tems there can be a great variation in a set of parametersdescribing the system, so we regard this as an acceptableclassification rate.

482 J. Opt. Soc. Am. A/Vol. 17, No. 3 /March 2000 Rawlinson et al.
Of the eyes in group 2, we see that of the normal andglaucomatous eyes, the LDF’s successfully predicted thestatus of 91% of those eyes. Of the 19 eyes with OHT,with pressure increase only, by clinical definition, 12 wereclassified as normal and seven as glaucomatous. Ofthese seven classified as glaucomatous, three eyes, al-though they could not have been classified as glaucoma-tous at the time, the fellow eye was glaucomatous, andthis test suggested that the eye examined was developingglaucoma; in one eye a disk hemorrhage appeared soon af-ter the scanning laser examination, and this was consis-tent with glaucoma; the remaining three eyes wereequivocal. These findings suggest that some degree of
Table 1. Linear Discriminant Function (LDF)Coefficients for Glaucomatous (G) and
Normal (N) Groups with lmaxÄ4a
LDF Coefficient G N
Kjconst 233.319 218.342
Kj00 0.211 0.172Kj11
r 0.222 0.297Kj11
i 0.089 0.085Kj20 0.231 0.251Kj22
r 0.410 0.120Kj22
i 20.364 20.145Kj31
r 0.193 0.248Kj31
i 0.318 0.282Kj33
r 20.657 20.270Kj33
i 20.123 0.123Kj40 0.443 0.379Kj42
r 20.586 20.587Kj42
i 21.069 20.782Kj44
r 1.111 0.837Kj44
i 0.209 0.254
a The squared distance between the centroids of the two groups is 9.29.
Table 2. Summary of Results with the Useof Multivariate Analysis based on LDF’s and
Comparison with Clinical Diagnosis
Subjects
Clinician Diagnosed
OHTNormal Glaucomatous
Group 1: Eyes used to derive the LDF’s (Calibration data)Normal 32 2 (1 early glaucoma) —Glaucomatous 2 29 —Total 34 31
Successful classification rate: (32 1 29)/(34 1 31) [ 94%
Group 2: Prediction based on LDF’s and s 2(10) & 100Normal 18 2 ‘‘12’’Glaucomatous 2 22 ‘‘7’’Total 20 24 19
Successful prediction rate: (18 1 22)/(20 1 24) [ 91%
Group 3: Prediction based on LDF’s and 100 & s 2(10) & 600Normal 13 2 (both early glaucoma) —Glaucomatous 3 8 —Total 16 10
Successful prediction rate: (13 1 8)/(16 1 10) [ 81%
change in the configuration of the optic disk is occurringbefore field loss and before being obvious ophthalmoscopi-cally.
The results of group 3 show that the LDF’s correctlypredicted the status of 81% of those eyes.
6. CONCLUSIONAs extended focus and depth images are collected fromthe Zeiss CLSO, it becomes apparent that a good ex-tended focus image did not necessarily mean that one hasa sufficiently good quality depth image to be included inthe set of images to carry out the multivariate analysis.An image was deemed to be good enough if one was ableto obtain an acceptable spherical harmonic fit to the origi-nal data—the goodness of fit determined by the decreas-ing magnitude of s 2(lmax) as lmax increases. On this ba-sis we accepted approximately 50% of the images fornumerical and statistical analysis. When one convertsthe raw depth images to surface graphics, it becomes ap-parent that noise is a major cause of lack of quality.Given an image with acceptable levels of noise, the pres-ence of blood vessels can obscure part of the ONH, andtilting of the retinal plane can render the image unsuit-able for analysis, as these effects can give misleading val-ues for the spherical harmonic coefficients.
Our approach was to make no assumptions about thedistributions of the predictors and investigate the mostbasic use of the LDF—that of measuring the distance ofan observation from the centroids of each group, wherethe centroid that is closer to the observation classifiesthat eye. That is, we take a hyperplane that perpendicu-larly bisects the line joining the two centroids; thus nor-mal eyes are deemed to be those on one side of the hyper-plane and glaucomatous eyes are deemed to be those onthe other. The LDF’s used the means of the predictors ofeach group and the pooled covariance matrix. Minitabcan evaluate the probabilities as to which group the mis-classified eyes belonged, where Minitab makes the as-sumption that the predictors are normally distributed.
If more reliable data can be obtained, further analysison the nature of the covariance matrices of each groupmight help determine if a hyperplane should be biased incertain directions to improve the success rate of classifi-cation of eyes.
Those images deemed to be of sufficient quality aresubject to multivariate analysis to ascertain whether thespherical harmonic coefficients can be used to distinguishthe two groups of eyes. The LDF’s are computed for eachclass of eyes and then used to classify new observations,correctly predicting the status of '80%–90% of the eyes,the percentage range depending on the quality of imagesin order to extract the spherical harmonic coefficients. Insome patients the distribution of blood vessels at theONH may detract from the efficiency of the method.
These results strongly suggest that the detection ofglaucoma by using a spherical harmonic decompositionhas merit and warrants further investigation.
ACKNOWLEDGMENTSThis research was carried out under Research Projects 87/100/93 and 89/126/94 of the Royal Victorian Eye and Ear

Rawlinson et al. Vol. 17, No. 3 /March 2000/J. Opt. Soc. Am. A 483
Hospital and funded by the Eye Ear Nose and Throat Re-search Institute, the Australian Research Council, andthe Research Committee of the Royal Victorian Eye andEar Hospital. Andrew A. Rawlinson thanks Lloyd Hol-lenberg of the School of Physics and Mark Burgman of theEnvironmental Sciences Group in the School of Botany,University of Melbourne, for discussions relating to thiswork.
Address correspondence to Keith A. Nugent at the lo-cation on the title page or by e-mail, [email protected].
REFERENCES1. J. Caprioli, ‘‘Correlations of visual function with nerve and
nerve fibre layer structure in glaucoma,’’ Surv. Ophthalmol.33, 319–330 (1989).
2. V. Cucevic, A. M. V. Brooks, N. T. Strang, A. G. Klein, andK. A. Nugent, ‘‘Use of a laser confocal scanning ophthalmo-scope to detect glaucomatous cupping of the optic disc,’’Aust. N.Z. J. Ophthalmol. 25, 217–220 (1997).
3. S. M. Drance, M. Schulzer, B. Thomas, and G. R. Douglas,‘‘Multivariate analysis in glaucoma. Use of discriminantanalysis in prediction glaucomatous visual field damage,’’Arch. Ophthalmol. (Chicago) 99, 1019–1022 (1981).
4. R. O. W. Burk, J. Konig, K. Rohrschneider, H. Noack, andH. E. Volcker, ‘‘Dreidimensionale papillentopographie mit-tels laser scanning tomographie: klinisches korrelat einercluster-analyse,’’ Klin. Monatsbl. Augenheilkd. 204, 504–512 (1994).
5. P. J. Airaksinen, A. Tuulonen, and H. I. Alanko, ‘‘Predictionof development of glaucoma in ocular hypertensive
patients,’’ in Glaucoma Update IV, G. K. Krieglstein, ed.)(Springer-Verlag, Berlin, 1991), pp. 183–186.
6. S. M. Drance, M. Schulzer, G. R. Douglas, and V. P.Sweeney, ‘‘Use of discriminant analysis. II. Identifica-tion of persons with glaucomatous visual field defects,’’Arch. Ophthalmol. (Chicago) 96, 1571–1573 (1978).
7. J. Mathews and R. L. Walker, Mathematical Methods ofPhysics (Benjamin, New York, 1964).
8. R. Weinreb, A. W. Dreher, and J. F. Bille, ‘‘Quantitative as-sessment of the optic nerve head with the laser tomogra-phic scanner,’’ Int. Ophthalmol. 13, 25–29 (1989).
9. W. H. Woon, F. W. Fitzke, A. C. Bird, and J. Marshall,‘‘Confocal imaging of the fundus using a scanning laser oph-thalmoscope,’’ Br. J. Ophthamol. 76, 470–474 (1992).
10. G. A. Cioffi, A. L. Robin, R. D. Eastman, H. F. Perell, F. A.Sarfarazi, and S. E. Kelman, ‘‘Confocal laser scanning oph-thalmoscope: reproducibility of optic nerve head topo-graphic measurements with the confocal laser scanningophthalmoscope,’’ Ophthalmology 100, 57–62 (1993).
11. F. S. Mickelberg, K. Wijsman, and M. Schulzer, ‘‘Reproduc-ibility of topographic parameters obtained with the Heidel-berg Retina Tomograph,’’ J. Glaucoma 2, 101–103 (1993).
12. R. A. Johnson and D. W. Wichern, Applied MultivariateStatistical Analysis, 2nd ed. (Prentice-Hall, EnglewoodCliffs, N.J., 1988), p. 461; P. A. Lachenbruch, ‘‘Some mis-uses of discriminant analysis,’’ Methods Info. Med. 16, 255(1977); M. M. Tatsouka, ‘‘Multivariate analysis of vari-ance,’’ in Handbook of Multivariate Experimental Psychol-ogy, 2nd ed., J. R. Nesselroade and R. B. Cattell, eds. (Ple-num, New York, 1988), p. 399.
13. B. F. Ryan, B. L. Joiner, and T. A. Ryan, Jr., Minitab Hand-book, 2nd ed. (Duxbury, Boston, 1985); I. Gordon and R.Watson, Basic Statistics with Minitab (U. of MelbournePress, Parkville, Australia, 1994).
14. R. E. Kirsch and D. R. Anderson, ‘‘Clinical recognition ofglaucomatous cupping,’’ Am. J. Ophthalmol. 75, 442–454(1973).