Embed Size (px)
Citation preview

Confidential: For Review OnlySpreading and scaling up innovation and improvement
Journal: BMJ
Manuscript ID BMJ-2019-049038.R1
Article Type: Analysis
BMJ Journal: BMJ
Date Submitted by the Author: 12-Apr-2019
Complete List of Authors: Greenhalgh, Trisha; University of Oxford, Nuffield Department of Primary Care Health SciencesPapoutsi, Chrysanthi; University of Oxford, Nuffield Department of Primary Care Health Sciences
Keywords: spread, scale-up, implementation science, complexity science, social science
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review Only
1
Revised paper resubmitted to BMJ April 2019
Spreading and scaling up innovation and improvement
A challenging task, potentially achievable through different logics: mechanistic (implementation science), ecological (complexity science) and social (social science)
Trisha Greenhalgh (Professor)Chrysanthi Papoutsi (Postdoctoral Researcher)
Professor of Primary Care Health SciencesUniversity of Oxford [email protected]
Word count for main text: 201456
We have read and understood the BMJ Group policy on declaration of interests and declare the following interests: none.
PPI statement:Patients and the public were not involved directly in this review article. The methodology included a specific search for studies in which patients and the public were involved in spread and scale-up projects.
Copyright:The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to i) publish, reproduce, distribute, display and store the Contribution, ii) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution, iii) create any other derivative work(s) based on the Contribution, iv) to exploit all subsidiary rights in the Contribution, v) the inclusion of electronic links from the Contribution to third party material where-ever it may be located; and, vi) licence any third party to do any or all of the above.
Contributorship: This was a commissioned article. TG did the initial search and wrote the first draft of the paper. CP undertook an additional search, and added comments, additional text and additional references to the paper. Both authors approved the final draft. TG is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding:TG is funded by the National Institute for Health Research Biomedical Research Centre, Oxford; grant BRC-1215-20008 to the Oxford University Hospitals NHS Foundation Trust and the University of Oxford. Funders had no say in the planning, execution or writing up of the paper.
Page 1 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
2
Introduction
The GP in the surgery, the nurse-manager on the ward and the policymaker in the boardroom would be forgiven for losing track of all the new technologies, care pathways and service models that could potentially improve the quality, safety or efficiency of care. Yet we know that innovations rarely achieve widespread uptake even when there is robust evidence of their benefits (and especially when such evidence is absent or contested).1 The NHS Long Term Plan points out that that every approach prioritised in the plan is already happening somewhere in the NHS but has not yet been widely adopted.2
There are common-sense reasons why spreading an innovation across an entire health system is hard. Achieving any change takes work, and it usually also involves – in various combinations – spending money, diverting staff from their day-to-day work, shifting deeply-held cultural or professional norms and taking risks. Simplistic metaphors (“blueprint”, “pipeline”, “multiplier”) aside, there is no simple or replicable way of implementing change at scale in a complex system. A technology or pathway that works smoothly in setting A will operate awkwardly (or not at all) in setting B.
Given these realities, what insights does the rapidly-growing research literature on spread and scale-up offer the busy clinician, manager, commissioner or policymaker? How – if at all – does this literature speak to the patient?
We begin with some definitions. In this paper, we examine how three different approaches can contribute to extending our understanding of spread and scale-up in healthcare improvement. “Spread” generally means replicating an initiative somewhere else and “scale-up” means addressing the infrastructural issues (across an organisation, locality or health system) that arise during full-scale implementation,,3 though these terms do not have a universally agreed definitionin practice the one blurs into the other.
Our 2004 systematic literature review on diffusion, spread and sustainability of innovation in the healthcare sector provided a conceptual framework linking the innovation, individual adopters, the influence of other people (e.g. opinion leaders), organisational (inner context) factors, environmental (outer context) factors, and the implementation process.3 In 2009, Damschroder and her team incorporated this and other work into a Consolidated Framework for Implementation Research (CFIR).4 At the time these widely-cited frameworks were developed, the primary research literature on spread and scale-up was sparse.
In the last few years, the empirical knowledge base on these topics has expanded considerably. A keyword and snowball search identified a number of recent systematic
reviews, narrative reviews, realist reviews and theoretical syntheses on spread or scale-up (summarised in Appendix). Each had a different focus – for example improvement science in
high-income4-6 and low and middle-income countries,3 7 8 innovation in primary care9 or public health,10 complex interventions,11 leadership for innovation,12 the social practice of innovation13 and technology adoption.14 All emphasise the need to attend to the complex relationship between intervention, people, organisation and the wider context, but they
used different conceptual frameworks and theoretical lenses.BOX 1
Page 2 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
3
TABLE 1
In this rapid review, whose methods are described in Box 1, we found that scholars of spread and scale-up had used many different theoretical lenses. We have chosen to highlight three – implementation science, complexity science and social science – each of which is Below, we consider three different lenses on spread and scale-up – implementation science, complexity science and social science – which are based on a different logics of change (respectively, mechanical, ecological and social). Their characteristics are summarised in Table 1. As the examples in Boxes 1-32-4 illustrate, many successful spread and scale-up programmes draw predominantly on one of these lenses but include elements of the other two.
Implementation science: spread and scale-up as complex interventionImplementation science, defined as “the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice” (page 2),4 developed from the evidence-based medicine movement in Europe and north America. It is perhaps best known for the sequential, structured (and, some would argue, technocratic andsomewhat top-down) methodology for spreading focused improvement techniques.4 5
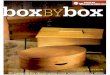
In this approach, illustrated in Figure 1, the first phase (after initial set-up and orientation) is the development of a clearly-defined intervention whose components are optimised to reflect the evidence base (especially on individual behaviour change). There is then a small-scale trial of this intervention in one or a few selected settings, followed by a systematic effort to replicate in other settings, partly by identifying and addressing barriers (which get in the way of the implementation effort) and facilitators (which potentially support it).
Patient input may be harnessed very productively in this effort – though careful attention needs to be paid to power dynamics, the kinds of data that are collected, and how and by whom those data are analysed.6
Whilst theis sequence depicted in Figure 1 is widely promoted, one systematic review showed that nearly half of all successful scale-up initiatives had not followed it.5
FIGURE 1
Implementation science approaches tend to draw heavily on quality improvement methodology. Barker et al describe this implementation science methodology as an “engine”. In their words:
“At the heart of the quality improvement (QI) method is rapid-cycle testing using the Shewhart Plan-Do-Study-Act (PDSA) cycle, which ensures that ideas for change are tested and adapted for local context. The notion of using PDSA to ‘ramp up’ the
Page 3 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
4
implementation process into broader and more diverse environments… provides the essential requirement for an adaptive design that can accommodate different contexts that are encountered as the intervention is scaled up.” (page 4)3
Implementation science-basedIn recent years, implementation science has matured as a field approaches to spread have much in common with in a way that has paralleled developments in the Medical Research Council’s guidance for developing and testing complex interventions.7 Both have shifted in recent years from a highly structured and narrowly experimental approach (which emphasised standardisation and replicability) to a more adaptive approach which recognises the need to think flexibly, understand and respond to local context, use qualitative methods to explore processes and mechanisms, and tinker with the intervention to achieve best fit with different settings.8
An example of spread using an implementation science logic is shown in Box 21.
BOX 21
Complexity science: spread and scale-up as adaptive changeA complex system is a set of things, people and processes that evolve dynamically and can be defined in terms of their relationships and interactions.8 9 They are characterised by uncertainty, unpredictability and emergence. They adapt through self-organisation (e.g. continuous adaptations initiated by front-line staff to allow them to complete tasks given local contingencies and availability of resources), attention to interdependencies (how the parts of the system fit together) and sensemaking (the process by which people, individually and collectively, assign meaning to experience and link it to action).9
To better understand the ecological (emergent, interdependent, adaptive) logic of complex systems, we must use multiple empirical methods, particularly ethnographic observation, applied in real-world rather than experimental settings and followed over time. Narrative (the richly-described case study, ideally incorporating both quantitative data on key metrics and qualitative data that explain why things unfolded as they did) can be a powerful synthesising tool.
To study the ecological (that is, emergent, interdependent, adaptive) properties of complex systems, researchers use multiple methods, particularly ethnographic observation, in real-world settings. Such studies are usually written up as richly-described case studies incorporating both quantitative and qualitative data and including a narrative of how and why things changed over time.
Complexity can be hard to square with spread strategies that seek to replicate a “blueprint” innovation in a standardised way across widely differing settings. Whilst the plan-do-study-act “engine” depicted in Figure 1 may work for small-scale improvement initiatives, spreading and scaling up major innovations across a health system requires attention to the
Page 4 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
5
underlying logic of complex systems, which is ecological rather than mechanical.9-12 Lanham et al, for example, recommend the following principles:9
- acknowledge unpredictability: designers of technologies or programmes should contemplate multiple plausible futures; implementation teams should tailor designs to local context and view surprises as opportunities;
- recognise self-organisation: designers should expect their designs to be modified, perhaps extensively, as they are taken up in different settings; implementation teams should actively capture data and feed it into the adaptation process;
- facilitate interdependencies: designers should develop methods to assess the nature and strength of interdependencies; implementation teams should attend to these interrelationships, reinforcing existing ones where appropriate and facilitating new ones;
- encourage sensemaking: designers should build focused experimentation into their designs; implementation teams should encourage participants to ask questions, admit ignorance, explore paradoxes, exchange different viewpoints and reflect collectively.
To this list, we would add: - develop adaptive capability in staff: individuals should be trained not merely to
complete tasks as directed but to tinker with technologies and processes and make judgements when faced with incomplete or ambiguous data;
- attend to human relationships, since embedding innovation requires people to work together to solve emergent problems using give-and-take and “muddling through”; and
- harness conflict productively: there is rarely a single, right way of addressing a complex problem, so view conflicting perspectives as the raw ingredients for multifaceted solutions.
These principles underpin the concept of the learning health system, defined as one “in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience” (page 17).13 A learning health system is characterised by participatory culture, distributed leadership, engaged patients, shared and evidence-based decision-making, transparent assessment of outcomes, and use of information and technology for continuous learning. Innovation, improvement, spread and scale-up will all occur more readily in such a system.13
The principles of complexity science can be applied more or less radically to spread and scale-up efforts. Øvretveit, writing in the context of international health, has proposed participatory adaptation (i.e. the use of decentralised planning, pragmatic modification and improvement facilitators to adapt the operational details of an intervention to local circumstances) as a way of achieving standardisation, replication and accountability while also respecting emergence and adaptation at the local level.10 The more radical methodology of facilitated evolution draws on the concept of resilience (defined as a system’s capability to withstand and recover from internal tensions and external shocks). Local sites are supported to develop the capacity to find, adapt and develop practices and models of care which address the challenges they face, with no external expectation placed
Page 5 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
6
on which solutions are to be adopted. In one example, the goal of preventing HIV/AIDS in a low-income African community was achieved via a community development initiative which provided women with independent income.10 There are numerous specific models of spread and scale-up that embrace (implicitly or explicitly) ecological logic and the learning health system take a systems perspective; some are listed in Table 2. Another model of spread and scale-up that takes a systems perspective is the learning health system, whose defining characteristics are shown in Figure 2.13 Innovation, improvement, spread and scale-up will all occur more readily in such a system. Øvretveit’s 3S scale-up infrastructure (a combination of strategic leadership, innovation culture, high-quality data capture systems and adaptive facilitation)11 and breakthrough collaboratives (which provide the infrastructure and impetus for inter-organisational exchange of resources, stories and ideas oriented to achieving an improvement goal),11 can both be thought of as components of a learning health system. These should not be viewed as mechanical tools to be applied deterministically to “solve” complexity (though formulaic versions of the breakthrough collaborative model exist). Rather, they are broad approaches that might be used creatively and reflexively to manage complexity.
FIGURE 214
To better understand the ecological (emergent, interdependent, adaptive) logic of complex systems, we must use multiple empirical methods, particularly ethnographic observation, applied in real-world rather than experimental settings and followed over time. Narrative (the richly-described case study, ideally incorporating both quantitative data on key metrics and qualitative data that explain why things unfolded as they did) can be a powerful synthesising tool.
An example of a complexity science approach to scale-up and spread is shown in Box 32.
TABLE 2
BOX 3
Social science: spread and scale-up as social actionSocial science approaches seek to identify and explain social mechanisms – such as what people believe and feel; why people act as they do; how they interpret material artefacts and other people’s actions; and how they draw on programme resources to achieve their goals (or why they refuse or are unable to do so).
As the previous section emphasised, staff in organisations implement change creatively and adaptively rather than mechanically. They experiment with innovations, develop feelings (positive or negative) about them, worry about them, adapt them to particular tasks, ‘work around’ them, and try to redesign them.1 Efforts to standardise the replication of an intervention across multiple settings, therefore, rarely go to plan.
Page 6 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
7
“[T]he theory explaining why a program worked (or did not work) may not be discovered by inspecting the program’s protocols or reading the formal, protocol-driven study reports. Programs almost never proceed as planned. Instead, they, and the assumptions that guide them and shape their actions, usually change over time as the programs progress. For instance, program leaders must respond to human agency and institutional contexts that affect the feasibility of their plans, and they need to figure out ways of doing things that they may not have thought of at the start.” (page 170)14
The term “theory” (strictly, “programme theory”) in the above quote means an explanation that answers the question “what did people do in this particular case and why did that have the effect it did?”. A programme theory is expressed at a very low level of generality (i.e. it may apply only to the case being analysed and closely comparable settings) – for example “the nurses did not engage because of a staffing crisis”. Social scientists also develop more general (“substantive”) theories to explain why spread and scale-up did or did not happen – for example, theories of behaviour change (individual level), absorptive capacity (organisational level), or inter-organisational influence (supra-organisational level). Usually, a social science explanation of a spread or scale-up effort requires both substantive theory(ies) and a more specific programme theory.14-16
Shaw et al synthesised various substantive theories (summarised in the appendix) which have been used to analyse the spread and scale-up effort as social practice.16 These theories, which include normalisation process theory, actor-network theory and structuration theory, help researchers and change agents to tap into (with a view to influencing) the organisational and societal influences which shape and constrain individuals’ actions. What do patients expect? What do different professional groups define as the gold standard of excellence? What do different professionals on the team expect of one another? What is believed to be legally sanctioned (whether or not those beliefs are correct)?
Many social scientists view the organisation as a ‘meso’ level world that mediates between the individual (micro) and societal (macro). Individuals’ actions in organisations are seen as shaped not only by practical and material realities but also by what are known as scripts or routines – that is, expected or required patterns of behaviour defined by formal roles, regulations and standard operating procedures as well as by informal customs, practices and traditions.17 Organisational routines, in turn, are strongly influenced by external social forces including professional norms, public expectations, laws and policies, and commercial and other vested interests.
Organisational change can thus be viewed as inherently transgressive, because doing things differently violates the norms, expectations and rules that are inscribed in organisational routines. Yet because routines are carried out by creative, thinking individuals rather than automatons, they contain within them the scope for adaptation and change.17 Leaders – both clinical and managerial (and perhaps most importantly, hybrid leaders who bridge both these roles) – play a crucial role in creating the preconditions in which staff will feel confident to innovate and improve (for example by setting a climate of risk-taking and collaborative learning rather than one of playing safe and covering one’s back).3 18
Page 7 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
8
An example of how social science has informed a study of spread and scale-up is shown in Box 43.
BOX 4
ConclusionThis article has presented three different ‘logics’ through which spread and scale-up can be approached: mechanistic (implementation science), ecological (complexity science) and social (social science). Whilst we have separated these for analytic purposes, there are significant synergies and overlaps between them. Empirical studies of spread and scale-up can and perhaps should combine more than one perspective. As a rule of thumb, the larger, more ambitious and more politically contested the spread challenge, the more ecological and social practice perspectives will need to supplement (or replace) ‘mechanical’ efforts to replicate an intervention. For further reading on the interface between implementation science, complexity science and social practice, we recommend Braithwaite et al’s recent theoretical synthesis.19
Page 8 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
9
Box 1: Search methods and summary of dataset
Through a keyword and snowball search, we identified a number of recent systematic reviews, narrative reviews, realist reviews and theoretical syntheses on spread or scale-up (summarised in Appendix). Each had a different focus – for example improvement science in high-income9 11 20 and low and middle-income countries,3 10 12 innovation in primary care21 or public health,5 complex interventions,15 leadership for innovation,18 the social practice of innovation16 and technology adoption.22 6
All these reviews emphasised the need to attend to the complex relationship between intervention, people, organisation and the wider context, but they used different conceptual frameworks and theoretical lenses
Prompted by a reviewer of an earlier draft of this paper, we searched the literature specifically for reviews that had explicitly considered how patients might be involved in spread and scale-up efforts. We found no such reviews so removed the ‘review’ filter from our search and selected one relevant high-quality primary study.6
Page 9 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
10
Box 21: An implementation science approach to spread and scale-upMcKay et al followed the full sequence of efficacy, effectiveness and implementation trials to develop, test and scale up a physical activity and healthy eating intervention in elementary schools in British Colombia, Canada.23 In the first phase, the multifaceted intervention (consisting of resources, training for teachers, school facilitators and a regional support team) was developed through participatory research with schools, communities and other stakeholders, taking account of contextual realities and behaviour change and social-ecological theories.
Efficacy was evaluated in a cluster randomised controlled trial in 10 schools which measured four outcomes: school-based opportunities for physical activity; actual physical activity levels; students’ chronic disease risk factors (e.g. obesity) and academic performance; students’ self-reported consumption of vegetables and fruit. Process evaluation captured contextual and operational issues that led to refinement of the intervention, which was then evaluated for effectiveness under real-world conditions in a larger cluster randomised controlled trial.
In the implementation and scale-up phase, a further 348 schools were supported to adopt and embed the intervention (with attention to fidelity of key components) and evaluate its impact locally. At the time of publication, 225 trained regional trainers had delivered over 4000 workshops to train over 80 000 teachers, reaching approximately 500 000 students. The programme, which took six years to develop and pilot, was sustained over ten years.
This is a rare example of a predominantly ‘top down’ (structured and programmatic) spread and scale-up strategy that achieved widespread coverage and measurable improvements in some but not all outcome measures. However, its success is also likely to be attributable to the use of participatory research and socio-ecological theories and to a positive policy context, strong professional buy-in, generous resourcing and long timescale.
Page 10 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
11
Box 32: A complexity science approach to spread and scale-upEaton et al used a combination of systematic review and national stakeholder interviews to build up an international case study of challenges to the spread of evidence-based mental health programmes in low and middle-income countries.12 Whilst every country had its own unique problems, some interrelated challenges recurred: limited financial resources and government commitment; over-centralisation of services in large psychiatric hospitals along with a weak, underfunded primary care sector; scarcity of trained mental health personnel; and low public health expertise among mental health leaders.
In the context of such widespread problems, the term “scale-up” was extended to refer to a number of linked goals: increase coverage (the number of people receiving mental health services); increase the range and appropriateness of services offered; increase the extent to which these services were evidence-based (using service models that had been tested in comparable settings); and strengthen the mental health care system through policy formulation, implementation planning and financing. Also key to the spread and scale-up effort were mobilising political will and reducing the stigma of mental health conditions among both lay people and health professionals. Seen from a complexity lens, all these goals are interdependent and mutually reinforcing.
Numerous approaches were taken in different countries at national level (e.g. attempts to influence the prioritisation, planning and resource allocation for mental health services; challenging the tertiary care focus; developing and disseminating evidence-based guidelines; developing human resource policies and programmes) and local level (support for service restructuring; training programmes for primary care staff in common mental disorders; engagement and education of patients, families and communities; and strengthening systems for evaluation and monitoring). Many settings were found to have weak data systems. By improving the quality of routinely collected data, developing reliable metrics of success that fed into system planning in a timely way, and developing links with academic researchers, the potential for system learning was greatly improved, though the spread and scale-up effort was more successful in some settings than others.
In contrast with the example in Box 1, a highly programmatic top-down approach emphasising fidelity of an intervention would not have worked in this case. An adaptive approach, combining national policy efforts with ‘bottom-up’ strengthening of local services, was needed to take account of the precarious political and economic context in many low- and middle-income countries and the multiple interdependencies in the system.
Page 11 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
12
Box 34: A social science approach to spread and scale-upA good example of how researchers used social theory to explain both spread and non-spread of innovations is Dixon-Woods et al’s studies of national efforts to reduce catheter-associated infections in intensive care units in the USA14 (highly successful) and UK (less successful).24
The US investigators had initially concluded (using an implementation science lens) that a technical checklist, introduced in over 100 intensive care units, had dramatically reduced central venous catheter infection rates by making the care process more systematic, rational, consistent and evidence-based. Dixon-Woods and her colleagues undertook post-hoc interviews, re-analysed the data, and came up with a new theory of spread that was predominantly social rather than technical.
For example, they showed that (perhaps because it was led by respected opinion leaders from a university), the US programme came to be seen as something a ‘good’ intensive care unit should be signing up to. Relationships between participating units strengthened as a result of participation, resulting in extensive inter-organisational networking and lateral support. As the initiative evolved, it took on the characteristics of a grass-roots social movement in which responsible clinicians and managers identified strongly with the programme and wanted to be involved.
A later ethnographic study by the same team, Explaining Matching Michigan,24 used a different programme theory to explain why the same intervention largely failed to spread in UK intensive care units, despite a near-identical phased model of implementation. For example, in the UK the intervention was seen as government-driven and top-down rather than professionally-led and collaborative; the initiative was introduced in parallel with other major infection control policies so had a less distinct identity; there was limited lateral support between participating units; and in low-performing units there appeared to be a history of under-resourced improvement initiatives that had resulted in change fatigue.
This case took a social science approach in the sense that a detailed programme theory was developed to explain both high and low success in different contexts, though the original design had been a conventional (largely behavioural) implementation science intervention.
Page 12 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
13
Figure 1: Rapid-cycle test of change model of spread used in implementation science
Based Drawing partly onon insights and a previous diagram in a review by Barker3
P D
SA
P DSA
P DSA
Ideas, explanations,hunches, theories
z
very small-scale testof change using plan-do-study-act cycle
P DSAP
DSAP
DSAP
DSA
P SA P SAP
DSAP
DSAP
DSA
P DSAP
DSAP
DSAP
DSAP
DSAP
DSA
P DSA
follow-up testsand iterativerefinement
small-scale tests ofchange in multiple sites
widespreadimplementation
with local tailoring
changes that result inimprovement at scalez
specific improvementintervention
P DSA
P D
SA
Page 13 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
14
Figure 2: The learning health system
A learning health system is defined by the US Institute of Medicine as one “in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience” (page 17).24 Its key features are shown below.
Component Characteristic
Culture Participatory, team-based, transparent, improving
Leadership Distributed, networked and dynamic
Patients, service users and the public
Fully and actively engaged
Care decisions Informed, facilitated, shared, coordinated and based on best evidence, every time
Outcomes and costs
Transparent and constantly assessed
Knowledge An ongoing, seamless product of services and research
Health information A reliable, secure and usable resource
Digital technology Used for continuous improvement and learning, with data stewarded and used for the common good
Trust fabric Strong, protected and actively nurtured
Page 14 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
15
Table 1: Different approaches to spread and scale-up in innovation and improvement
Implementation science
Complexity science Social science
Main focus Evidence-based interventions in practice
The evolving and emergent properties of systems
Individuals, groups and organisations
Contribution Provides a concrete, planned approach to the delivery and study of spread and scale up
Ecological view that emphasises the system’s inherent unpredictability and need for adaptive change at multiple, interacting levels
Foregrounds patterns of social behaviour and interaction, professional beliefs and values, and organisational routines and structures
Key mechanisms of spread and scale-up
Uncertainty reduction, emphasis on fidelity and contextual influences
Emergent properties of an interacting system – hence, self-organisation, management of interdependencies and sense-making
Social, professional and organisational influences that shape (and are shaped by) individual and collective action
Preferred methods for achieving spread and scale-up
Structured, programmatic approach to develop and replicate a complex intervention across multiple settings
Gain a rich understanding of the case in its historical, socio-political and organisational context. Use multiple methods flexibly and adaptively. Expect surprises and handle them creatively. Develop individuals and organisations to be creative and resilient.
Develop and apply theories of how individuals’ behaviour and actions are influenced by interpersonal, material, organisational, professional and other factors
Preferred methods for researching spread and scale-up
Metrics for measuring improvement (quantitatively) and systematic approach to exploring processes and mechanisms (qualitatively)
Case study approach using multiple qualitative and quantitative methods. Narrative used as a synthesising tool that can capture complex chains of causation
Ethnography, interview-based methods and case narratives.
Page 15 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
16
Table 2: Specific models for applying complexity science to spread and scale-up
Name of model (Author, year)
Key components Comment
Participatory adaptation (Øvretveit, 2010)10
In the context of international health, use of decentralised planning, pragmatic modification and improvement facilitators to adapt the operational details of an intervention to local circumstances.
Proposed as a flexible way of achieving standardisation, replication and accountability while also respecting emergence and adaptation at the local level
Facilitated evolution (Øvretveit, 2010)10
Local sites are supported to develop the capacity to find, adapt and develop practices and models of care which address the challenges they face, with no external expectation placed on how problems are framed or which solutions are to be adopted. Draws on the concept of resilience (defined as a system’s capability to withstand and recover from internal tensions and external shocks).
More radical approach than participatory adaptation. In one example, the goal of preventing HIV/AIDS in a low-income African community was achieved via a community development initiative which provided women with independent income.
3S scale-up infrastructure (Øvretveit,2011) 11
A combination of strategic leadership, innovation culture, high-quality data capture systems and adaptive facilitation.
Breakthrough collaboratives (Øvretveit,2011) 11
Provision of resources, infrastructure and impetus for inter-organisational exchange of resources, stories and ideas oriented to achieving an improvement goal – typically via periodic collaborative workshops.
These should not be viewed as mechanical tools to be applied deterministically to “solve” complexity (though formulaic versions of the breakthrough collaborative model exist). Rather, they are broad approaches that might be used creatively and reflexively to manage complexity.
Experience-based co-design (Bate and Robert, 2006)25
In collaborative workshops, and also in preparatory and follow-up work, patients work together with staff to identify emotional ‘touch points’ in the patient journey and redesign the service in a way that centres on improving the patient experience.
Not explicitly complexity-focused but follows many of the principles of effective change in complex systems – notably self-organisation, collective sensemaking and harnessing conflict productively.
Page 16 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
17
Figure 2: The learning health system
A learning health system is defined by the US Institute of Medicine as one “in which science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the delivery process and new knowledge captured as an integral by-product of the delivery experience” (page 17).24 Its key features are shown below.Component Characteristic
Culture Participatory, team-based, transparent, improving Leadership Distributed, networked and dynamicPatients, service users and the public
Fully and actively engaged
Care decisions Informed, facilitated, shared, coordinated and based on best evidence, every time
Outcomes and costs
Transparent and constantly assessed
Knowledge An ongoing, seamless product of services and researchHealth information A reliable, secure and usable resourceDigital technology Used for continuous improvement and learning, with data stewarded
and used for the common goodTrust fabric Strong, protected and actively nurtured
Page 17 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
18
Page 18 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
19
Key messages- Spread (replicating an intervention) and scale-up (building an infrastructure to support
full-scale implementation) are difficult;- Implementation science traditionally takes a structured and phased approach to
developing, replicating and evaluating an intervention in multiple sites;- Complexity science encourages a flexible and adaptive approach to change in a dynamic,
self-organising system;- Social science approaches consider why people act in the way they do, especially the
organisational and wider social forces that shape and constrain people’s actions;- These approaches are closely linked; all can provide insights into the challenges of
spread and scale-up.
References
1. Greenhalgh T, Robert G, Macfarlane F, et al. Diffusion of innovations in service organizations: systematic review and recommendations. The Milbank quarterly 2004;82(4):581-629. doi: 10.1111/j.0887-378X.2004.00325.x [published Online First: 2004/12/15]
2. NHS England. NHS Long Term Plan. London: NHS England 2019.3. Barker PM, Reid A, Schall MW. A framework for scaling up health interventions: lessons
from large-scale improvement initiatives in Africa. Implementation Science 2015;11(1):12.
4. Nilsen P. Making sense of implementation theories, models and frameworks. Implementation Science 2015;10(1):53.
5. Indig D, Lee K, Grunseit A, et al. Pathways for scaling up public health interventions. BMC public health 2018;18(1):68.
6. Renedo A, Marston CA, Spyridonidis D, et al. Patient and Public Involvement in Healthcare Quality Improvement: How organizations can help patients and professionals to collaborate. Public Management Review 2015;17(1):17-34.
7. Craig P, Dieppe P, Macintyre S, et al. Developing and evaluating complex interventions: the new Medical Research Council guidance. British Medical Journal 2008;337(7676):a1655. doi: 10.1136/bmj.a1655
8. Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift: BioMed Central, 2018.
9. Lanham HJ, Leykum LK, Taylor BS, et al. How complexity science can inform scale-up and spread in health care: understanding the role of self-organization in variation across local contexts. Social Science & Medicine 2013;93:194-202.
10. Øvretveit J. Widespread focused improvement: lessons from international health for spreading specific improvements to health services in high-income countries. International Journal for Quality in Health Care 2011;23(3):239-46.
11. Øvretveit J, Garofalo L, Mittman B. Scaling up improvements more quickly and effectively. International Journal for Quality in Health Care 2017;29(8):1014-19.
Page 19 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
20
12. Eaton J, McCay L, Semrau M, et al. Scale up of services for mental health in low-income and middle-income countries. The Lancet 2011;378(9802):1592-603.
13. Institute of Medicine Round Table on Value and Science-Driven Healthcare. The learning health system and its innovation collaboratives. Accessed on 23.1.19 at http://www.nationalacademies.org/hmd/Activities/Quality/~/media/Files/Activity%20Files/Quality/VSRT/Core%20Documents/ForEDistrib.pdf. Washington, DC: National Academy of Medicine (formerly Institute of Medicine) 2011.
14. Dixon-Woods M, Bosk CL, Aveling EL, et al. Explaining Michigan: developing an ex post theory of a quality improvement program. The Milbank quarterly 2011;89(2):167-205.
15. Willis CD, Riley BL, Stockton L, et al. Scaling up complex interventions: insights from a realist synthesis. Health research policy and systems 2016;14(1):88.
16. Shaw J, Shaw S, Wherton J, et al. Studying scale-up and spread as social practice: theoretical introduction and empirical case study. Journal of medical Internet research 2017;19(7)
17. Greenhalgh T. Role of routines in collaborative work in healthcare organisations. BMJ 2008;337:a2448. doi: 10.1136/bmj.a2448 [published Online First: 2008/11/19]
18. Currie G, Spyridonides D. Sharing leadership for diffusion of innovation in professionalized settings. Human Relations 2019;in press
19. Braithwaite J, Churruca K, Long JC, et al. When complexity science meets implementation science: a theoretical and empirical analysis of systems change. BMC medicine 2018;16(1):63.
20. Leeman J, Birken SA, Powell BJ, et al. Beyond “implementation strategies”: classifying the full range of strategies used in implementation science and practice. Implementation Science 2017;12(1):125.
21. Charif AB, Zomahoun HTV, LeBlanc A, et al. Effective strategies for scaling up evidence-based practices in primary care: a systematic review. Implementation Science 2017;12(1):139.
22. Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. Journal of medical Internet research 2017;19(11):e367. doi: 10.2196/jmir.8775 [published Online First: 2017/11/03]
23. McKay HA, Macdonald HM, Nettlefold L, et al. Action Schools! BC implementation: from efficacy to effectiveness to scale-up. Br J Sports Med 2015;49(4):210-18.
24. Dixon-Woods M, Leslie M, Tarrant C, et al. Explaining Matching Michigan: an ethnographic study of a patient safety program. Implementation science 2013;8(1):70.
25. Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. BMJ Quality & Safety 2006;15(5):307-10.
Page 20 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
Appendix: Reviews and theoretical syntheses of spread and scale-up in healthcareFor the purposes of the table below, ‘systematic review’ means a paper describing an explicit search strategy and formal analytic approach to data extraction and combining primary literature. ‘Narrative review’ means a review that had a specific goal or research question but no explicit search strategy. ‘Theoretical synthesis’ means a section of an empirical paper which synthesised the theoretical literature on a particular approach to scale-up or spread that was not covered in other reviews. ‘Realist synthesis’ means a review that used realist methods to identify context-mechanism-outcome configurations. One primary study (Renedo 2015), with a narrative review as part of the same paper, was included as this was the only paper to address the inclusion of patients and lay people in the spread and scale-up effort.
Author, Year (country of lead author)
Goal of review Study design (theoretical lens)
Inclusion criteria for primary studies
Main findings
IMPLEMENTATION SCIENCE APPROACHESBarker 20151 (USA)
Synthesise published sequential scaling-up frameworks into a new framework
Systematic review with empirical testing in two large projects in Africa (complex intervention lens)
Papers in English from peer-reviewed and grey sources on models, frameworks or theories for scale-up
Core components for scale-up: the sequence of activities required for scaling up; mechanisms to achieve uptake; and underlying factors and support systems. Authors advise a 4-phase process: [a] set-up (prepare the ground and test the intervention to be scaled up); [b] develop the scalable unit (an early testing phase); [c] test the intervention in a variety of settings representing a range of contexts; [d] replicate at full scale.
Renedo 20152 (UK)
Review the literature on patient and lay involvement in implementation science
Narrative review followed by a primary (longitudinal case) study in London, UK
Active efforts to involve patients and the public in improvement initiatives
Patient input to local spread and scale-up was helped by: [a] organisational emphasis on non-hierarchical, multidisciplinary collaboration; [b] recognition and respect from staff; [c] commitment to rapid action, including quick translation of research into practice; and [d] the process of constant data collection and reflection facilitated by improvement methods.
Charif 20173 (Canada)
Synthesise empirical studies of scaling up evidence-based practice in primary care
Systematic review (knowledge translation / behaviour change lens)
Strategies to scale up evidence-based practice in primary care. Controlled trials, before-and-after studies and interrupted time series designs
14 studies, mostly before-and-after designs in specific clinical area e.g. newborn care, tuberculosis, with over-representation of low and middle-income countries. EPOC Effective Public Health Practice Project tool identified flaws in designs. Most common scale-up strategy was clinician education for behaviour change. Impacts of interventions were variable but most demonstrated some success.
Leeman 20174 (USA)
Develop a classification system for implementation strategies
Narrative review (interactive systems framework lens)
Strategies to scale up evidence-based interventions
Scale-up strategies are a sub-set of implementation strategies. They may be targeted at individuals (e.g. motivation and capacity to understand and use evidence), the inner organisational setting (leadership engagement, resources, infrastructure) or the outer setting (public policy; human and material resources; cross-setting learning and collaboration).
Indig 20185 (Australia)
Evaluate public health interventions in high income countries that were scaled up or implemented at scale, using an evidence-based model of spread
Systematic review of primary studies, along with review of relevant conceptual frameworks
Primary studies with: 1) a public health intervention; 2) a chronic disease prevention focus; and 3) delivered at scale (state, national or international)
Successful spread was measured as ‘institutionalised’ (had become business as usual in a host organisation), ‘commercialised’ (delivered by or in partnership with private provider) or ‘adapted’ (customised to a particular setting or group). Unifying framework assumed a 4-stage pathway – development, efficacy testing, real world trial and dissemination – as the benchmark. Of 40 programmes, just over half had followed all 4 stages; the others had omitted one or more of the other stages (but succeeded nevertheless).
COMPLEXITY SCIENCE APPROACHESEaton 20116 (Nigeria)
Synthesise evidence on scaling up mental health interventions in low and middle income countries
Systematic review and survey of key national stakeholders
Empirical studies of scale-up of mental health interventions in countries meeting World Bank definition of LMIC
Scale-up requires a system-wide approach that includes political will, reorganisation of services, development and application of evaluation metrics and mobilisaiton of resources (see Box 3 for further detail).
Øvretveit 20117 (Sweden)
Synthesise theoretical models for spread and scale-up of
Narrative review
Empirical studies and theoretical papers addressing
3 ways innovations spread in international health: [a] Hierarchical control (top-down, implementation science-based, tends to be structured and technocratic); [b] Participatory adaptation (decentralised, democratic but
Page 21 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
interventions in international health
intentional spread strategies
retains belief in accountability and rational planning); [c] Facilitated evolution (support sites to build their capacity and identify fit for purpose solutions for their priorities).
Lanham 20138 (USA)
Synthesise the literature on complexity approaches to scale-up and spread
Theoretical synthesis, applied to two large US case studies
Publications linking spread, scale-up and complexity
Strategies should: acknowledge unpredictability, recognise self-organisation, facilitate interdependencies and encourage sensemaking (see text for elaboration)
Greenhalgh 20179 (UK)
Develop a framework to explain non-adoption, abandonment and challenges to scale-up, spread and sustainability of technology-based service innovations
Systematic review with empirical testing in six case studies in UK health and social care (complex adaptive system lens)
Frameworks for explaining or evaluating technology-based change in healthcare
Scale-up and spread of technology-based interventions depends on the dynamic interaction of a complex system. Key interacting domains include the illness or condition, the technology, the value proposition, the inner organisational context (including the implementation process), the wider external context, and evolution over time. Complexity in multiple domains reduces the chances of project success. System-level planning should include building adaptive capacity and resilience in people, organisations and technologies.
Øvretveit 201710 (Sweden)
Synthesise system-level approaches to spread and scale-up
Theoretical synthesis, applied to two large US case studies (system science lens)
Not explicitly stated
Lessons for successful scale-up: [a] Prepare and assess context (including readiness for change and financial context); [b] Establish a 3S scale-up system (structure, strategy and system supports including facilitation); [c] Invest in, and draw upon, the 3S system to provide the oversight, facilitation and data to share knowledge and practices between implementing units; [d] Link with applied research.
SOCIAL SCIENCE APPROACHESShaw 201711 (Canada)
Synthesise theories of social practice relating to spread of technology-based innovations in health and social care
Theoretical synthesis with empirical application to a single UK-based case study in social care (social practice lens)
Theoretical lenses which considered spread as social or socio-technical practice
10 named theories: activity theory, socio-technical systems theory, several variants of practice theory, several variants of structuration theory, actor-network theory, technological sensemaking, normalisation process theory. All emphasise the reciprocal relationship between human behaviour/action, organisational and wider contextual influences including professional norms, social expectations, laws, regulations, material and practical constraints and resources.
Willis 201612 (Canada)
Undertake a realist synthesis of studies on scaling up complex interventions
Realist synthesis focusing on context-mechanism-outcome configurations
Case examples of scaling up a complex intervention
Complex interventions are more successful in some contexts than others. 4 mechanisms – awareness, commitment, confidence and trust – contribute to individuals’ engagement with the scaling-up effort. These are differentially triggered in different contexts.
Currie 2019 (UK)13
Synthesise theories of leadership relevant to spread of innovation in healthcare organisations
Theoretical synthesis with application to 12 innovation projects in UK healthcare (leadership lens)
Theories of leadership pertaining to spread of innovations among organisations
Organisational leaders are important for spread – both managerial (for allocating resources and setting climate) and professional (for engaging peers and influencing resource allocation). Hybrid clinician-managers may play a pivotal role, contingent on resources and organisational structure.
1. Barker PM, Reid A, Schall MW. A framework for scaling up health interventions: lessons from large-scale improvement initiatives in Africa. Implementation Science 2015;11(1):12.
2. Renedo A, Marston CA, Spyridonidis D, et al. Patient and Public Involvement in Healthcare Quality Improvement: How organizations can help patients and professionals to collaborate. Public Management Review 2015;17(1):17-34.
3. Charif AB, Zomahoun HTV, LeBlanc A, et al. Effective strategies for scaling up evidence-based practices in primary care: a systematic review. Implementation Science 2017;12(1):139.
Page 22 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
4. Leeman J, Birken SA, Powell BJ, et al. Beyond “implementation strategies”: classifying the full range of strategies used in implementation science and practice. Implementation Science 2017;12(1):125.
5. Indig D, Lee K, Grunseit A, et al. Pathways for scaling up public health interventions. BMC public health 2018;18(1):68.
6. Eaton J, McCay L, Semrau M, et al. Scale up of services for mental health in low-income and middle-income countries. The Lancet 2011;378(9802):1592-603.
7. Øvretveit J. Widespread focused improvement: lessons from international health for spreading specific improvements to health services in high-income countries. International Journal for Quality in Health Care 2011;23(3):239-46.
8. Lanham HJ, Leykum LK, Taylor BS, et al. How complexity science can inform scale-up and spread in health care: understanding the role of self-organization in variation across local contexts. Social Science & Medicine 2013;93:194-202.
9. Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. Journal of medical Internet research 2017;19(11):e367. doi: 10.2196/jmir.8775 [published Online First: 2017/11/03]
10. Øvretveit J, Garofalo L, Mittman B. Scaling up improvements more quickly and effectively. International Journal for Quality in Health Care 2017;29(8):1014-19.
11. Shaw J, Shaw S, Wherton J, et al. Studying scale-up and spread as social practice: theoretical introduction and empirical case study. Journal of medical Internet research 2017;19(7)
12. Willis CD, Riley BL, Stockton L, et al. Scaling up complex interventions: insights from a realist synthesis. Health research policy and systems 2016;14(1):88.
13. Currie G, Spyridonides D. Sharing leadership for diffusion of innovation in professionalized settings. Human Relations 2019;in press
Page 23 of 23
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960