Embed Size (px)
Citation preview

222 Geriatric Nursing Volume 24 Number 4
Conducting InterpretingandInterface Pressure Evaluationsof Clinical Support Surfaces
Frederick Shelton, MS, and Judy Wright Lott, DSN, RNC, NNP

July—August 2003 223
Clinical support surfaces, such as patient bed mattresses,bed cushions, operating room table surfaces, andwheelchair pads, are important adjuncts for patient com-fort and safety. These surfaces also can be a significant ex-pense, depending on the surface selected. Interfacepressure measurements frequently are used to evaluatesuch clinical support surfaces. Accurate interpretation ofinterface pressure images requires knowledge about howthe measurements are obtained and how they are inter-preted; otherwise, it is difficult to differentiate true find-ings from a marketing interpretation. Even whenpublished, interface pressure analyses often are not stan-dardized and not well controlled.
The practitioner’s ability to interpret these sources ofdata and make the best decision for his or her patient is con-founded because there are many ways to create invalid datathrough various testing methods. It is possible to misleadreaders by manipulating the way the images are displayed.
The purpose of this article is to describe analysis andevaluation of clinical support surfaces using interfacepressure measurements. The article specifically addressesthe value and the shortcomings of interface pressure mon-itoring. Accurate interpretation of the data can be the sin-gle most critical yet most misunderstood component ofsupport surface comparisons.
On any day, 10% of all acute care patients in the UnitedStates1 and 12% in Europe2 suffer from pressure ulcers(decubitus ulcers or bed sores). Pressure ulcers are verycostly for caregivers and very painful for patients.Pressure sores occur when the tissues are compressed anddistorted, causing impaired local blood circulation, insuf-
ficient nutrients and oxygen delivery, and decreased re-moval of waste products.3
Efforts to reduce the prevalence of pressure ulcers havefocused mainly on preventing hospital-acquired pressureulcers. The primary preventive approach has been to im-prove clinical support surfaces (beds, tables, stretchers,chairs, etc.) that minimize external forces (eg, pressureand shear) on a patient’s body. The ability to determine theefficacy of clinical support surfaces is key to the compari-son of several surfaces.4,5
Interface pressure, the loading between a patient’s skinand the support surface, can determine relative differencesin support surface performance.6 Several researchers haveraised numerous concerns about the use of different meth-ods of interface pressure.7,8 Several types of systems mea-sure interface pressure, each with its particularperformance characteristics. Several common critical vari-ables of interface pressure systems include overall size,creep, drift, flexibility, resolution, accuracy, and repeata-bility; each of these variables affects the reliability of col-lected data. When interpreting interface pressure testing,the first thing to be reviewed must be the interface pres-sure system characteristics and methods used.
Reliability variables include creep, drift, accuracy, re-peatability, and resolution. Creepis the system’s tendencyfor the measurement to shift higher or lower when exposedto a constant pressure over time. Creep depends entirelyon the physics of how the system measures the pressure(capacitive, resistive, piezoelectric, or pneumatic) and theactual construction of the pad. Drift is a system’s tendencyto “float” higher or lower over numerous measurements.This factor is related to the data collection electronics, notthe surface pad itself; it is manifested by the movement ofthe zero itself. Accuracyis the system’s ability to report“actual” pressures. Repeatabilityis a system’s ability toreport a consistent measurement pressure every time it isused under the same conditions. Finally,resolutionis howfine the pressure measurements are (ie, how small a pres-sure peak the system can detect accurately).
Accuracy and repeatability testing should not be conductedon a flat rigid surface but on a range of conformal surfacessimilar to the surfaces it is intended to evaluate. Typically, ac-curacy and repeatability suffer from using extremely rigid orconformal surfaces more than using “middle” surfaces.
The type of data used to evaluate a specific surface’sperformance is as important as the reliability of the data.The most commonly reported data are single value maxi-mum pressures recorded at several critical areas of thebody. These maximum pressures are useful data, but theydo not give any indication of the number of peak pres-sures, the overall size of the pressure peaks, the mean pres-sure on the entire body, or even maximum peak pressuresin locations of the body not considered critical. These fac-tors are equally important for determining the most usefulsurface for patient use. One of the authors9 previouslypublished an article reporting a method for creating a pres-
Interface pressure measurement is a commonmethod to compare various mattresses, operatingroom beds, or other clinical support surfaces usedfor patients. The colorful graphs create a good visualdisplay of information. Unfortunately, no standardmethod exists for performing the measurements ordisplaying the information. Because the graph issuch a good visual representation of the data, manyclinicians rely on the look of the graph. However, al-tering its appearance by simple manipulations of thedisplay characteristics is very easy. This manipulationcan lead to inaccurate conclusions about the prod-uct and consequent purchase of products that areinappropriate, less effective, or more expensive thanothers. This article provides basic information aboutinterface pressure measurement and interpretationso that clinicians can make informed decisions aboutvarious clinical surfaces. (Geriatr Nurs 2003;24:222-7)

224 Geriatric Nursing Volume 24 Number 4
sure index for ranking overall interface pressure for multi-ple body sizes, head-of-bed elevations, and over the entirebody. This index provides a more comprehensive and thor-ough method of analyses because it doesn’t rely on singlemeasurements of 1 body type.
Health care practitioners must evaluate the data of var-ious different support surfaces in making a decision aboutwhich surface reduces pressure on the skin overall. How apractitioner compares the data from different support sur-faces is critical to the validity of the conclusions that canbe drawn from those data. Many researchers believe thatinterface pressure data should be used only for relativejudgments between surfaces tested under the same condi-tions.10,11 However, the interpretation of the data, evencollected on the same system in the same fashion, can bevery misleading, depending on how it is displayed. Thisarticle describes the measurement of interface pressure forclinical support surfaces and data interpretation obtainedfrom those measurements to ensure that different supportsurfaces can be evaluated appropriately.
METHODS
Measurement Device
A full body interface pressure system was chosen tomeasure pressure for each support surface. The system hasa semiconductive film system that measures the reductionof resistance for each sensor element as a result of loadingthe element in the normal direction. The full body systemhas more than 1000 sensing elements across the entirebody. The system has some time-dependent creep associ-ated with its measurements, most of which occurs in thefirst 30 seconds after loading. Therefore, all data collec-tion was done at 60 seconds after loading to allow the sys-tem time to stabilize for improved repeatability. Creepoccurs when an object of constant weight is placed on thesystem and the system measurement of this pressure con-tinues to “creep” up.12
SubjectsInterface pressure measurements are highly sensitive
to subject variability and the method of subject place-ment. No 2 humans, even of the same weight and stature,are anatomically identical. Therefore, when taking inter-face pressure data, numerous subjects of varied bodysizes should be used. Previous work has detailed the per-centile body types of typical US populations, includingelderly populations.9 Subjects from all parts of the spec-trum need to be tested so the results represent the bulk ofthe US population.
Statistical data from the Vital Statistics Series were usedto determine height and weight of the desired range of per-sons in the US. A fifth percentile female was determined asthe smallest body type at 4 feet, 10 inches (1.5 m) and 104pounds (47.2 kg). A ninety-fifth percentile male was deter-mined as the largest body type at 6 feet, 0 inches (1.8 m)
and 213 pounds (96.6 kg). Finally, a fiftieth percentile per-son was determined using the median height and weightand a female body type, which represents the middle bodytype of the overall range at 5 feet, 2 inches (1.6 m) and135 pounds (61.2 kg).13
Head-of-Bed ElevationsInterface pressure measurements were taken at 3 eleva-
tions of the head section of the bed: 0, 30, and 45 degrees.The 0-degree head-of-bed elevation was chosen because itreflects the supine position most commonly used in thehospital for critically injured or ill patients. The 30-degreehead-of-bed elevation was chosen because it represents atypical elevation at which caregivers place patients duringtheir recovery to promote clearing of the lungs and healing.Finally, the 45-degree head-of-bed elevation was chosenbecause it is the highest elevation patients typically used inrecovery activities, such as eating, watching television, in-teracting with visitors. The beds were raised to this positionusing standard operating mode, which also articulates theknee section of the bed as the head is elevated.
SurfacesFor the purposes of illustrating how the data can be dis-
played, changed, and interpreted, a rigid and a soft surfacewas used.
RESULTS
Full Body Interface Pressure Maps
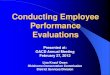
When interface pressure analysis is done, full bodymapping should be conducted rather than local measure-ments or mapping. Figure 1 shows how the redistribution
Figure 1. The towel roll completely eliminates the pressure on theheel itself. The pressures are redistributed to the area directlyproximal where the artery that feeds the foot is located, which canactually decrease blood-flow to the heels and can actually in-crease risk of breakdown.

July—August 2003 225
of loads can be missed if only local measurements aremade rather than using a broader map. Vascular testing14
showed that placing a towel roll under the heels is moredetrimental than merely resting them on the rigid inner-spring surface. However, if data are reported only for thepressures directly under the heels, the towel roll has sig-nificantly lower pressures than resting on the surface.14
What those data do not show is the redistribution of pres-sure onto the Achilles tendon, which is the vascular sourcefor the entire foot. Likewise, the same misconception canbe seen in Figure 2, where a lumbar support was used toredistribute loads that normally would be in the sacral re-gion to the lower back.
Body TypesClinical support surfaces function differently for per-
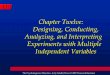
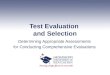
sons of different height and weight. Figure 3 shows how asingle surface can function well for one body type but notfor another. When interpreting interface pressure data, per-formance for the entire population must be considered.This surface functions well for a small, lightweight personbut results in high pressure on the bony prominences, lead-ing to a detrimental condition, for a heavier person. Theopposite can be true as well; a surface may function wellfor a heavier person but be too stiff and rigid for a lighter,smaller person. Even interface pressure maps of persons ofsimilar stature and weight vary dramatically for the samesurface and head-of-bed elevation (Figure 4). This diffi-culty can be exacerbated in obese, pediatric, and neonatalpatients. These patient types often are completely left outwhen a surface’s performance is evaluated.
Display of the DataInterface pressure systems have the ability to change
the color scales and color representation of pressure spots.When comparing exactly the same interface pressure map,the visual representation of the data can be shown many
Figure 3. The same support surface can provide dramatically dif-ferent performance depending on the size and weight of the pa-tient In this example, the surface performs well for the shorter,lighter subject. However, the taller, heavier subject “bottoms out”(which increases pressures in the region).
Figure 4. Two human subjects of similar height, weight, and bodybuild can produce dramatically different interface pressure maps,even on a similar support surface. This is due to the anatomic dif-ferences found in all humans. Therefore, multiple subjects for eachweight range should be used or comparisons should be madeusing only the same subjects.
Figure 2. The same trends as were seen In the heel region can beseen in the lumbar area if a towel roll is used.

226 Geriatric Nursing Volume 24 Number 4
ways (Figure 5). Likewise, the color sequence also canmodify the visual representation of the data (Figure 6).
DISCUSSION
Many system-dependent variables affect interface pres-sure testing. Likewise, numerous interface pressure mea-surement technologies exist, each of which approachesthese variables through different methods. The most im-portant variables are repeatability, resolution, drift, creep,and accuracy in that order and for these reasons: repeata-bility reflects a system’s ability to consistently make reli-able measurements from surface to surface and patient topatient. Resolution of the system determines the numberof simultaneous measurements made; it also controls thesystem’s ability to distinguish peak pressures from smallbony prominences. Drift can affect the measurements asthe same pressures tend to be represented by differentmeasurements over time as the system shifts. Creep is rel-atively easy to overcome as long as the time-dependentproperties are consistent; all measurements need only bemade after the same time of contact with the surface.Finally, accuracy is considered the least important becausewhat the “actual” pressures are is not as important as mea-surement consistency.
Contrary to traditional dogma, 32 mm Hg is not themagic number of pressure required to stop blood flow.Actually, this number varies for each person, each bodylocation, nutrition, disease process, etc. and can be as lowas 12 mm Hg for severely compromised persons.15-17
Therefore, it becomes much more valuable to be able toconsistently compare pressures caused by different sur-
faces on the same subjects rather than knowing the exactpressures on different surfaces.
As a final note, these variables typically measure dif-ferently on conformal surfaces than on rigid surfaces.Systems should be evaluated on the conformal surfaces forwhich they are intended.
The subjects used to evaluate the clinical support sur-faces also can significantly affect the conclusions drawnfrom the data. Extremely conformal surfaces, soft enoughfor a small or lightweight person to sink into, can workvery well for that body type. However, a heavier or tallerperson may have high pressure peaks as a result of totallycompressed surfaces. Likewise, a surface rigid enough fora heavy person may be entirely too rigid for a lightweightperson. Therefore, representatives from all parts of thepopulation that are going to be placed on the clinical sup-port surfaces should be tested. And because each human isdifferent, numerous subjects from each part of the popula-tion should be tested, especially for extremes in popula-tions such as obese persons and children or infants. Also,all positions that are to be used for the surfaces should betested (eg, 0-65 degrees head-of-bed elevation) becausethey can influence the validity of the conclusions.
Finally, what is measured and how it is displayed canaffect the conclusions of the data. If only local measure-ments are made, pressure redistribution easily can bemissed. Since these surfaces cannot affect gravity or pa-tient weight, redistribution is the only method a supportsurface has to lower pressures over critical regions.Likewise, how the data are displayed can either inform ormislead the practitioner. To make sound conclusions, all
Figure 5. The two interface pressure images shown here representthe same dataset (the same individual, same surface, and sameraw data file). The differences seen are solely due to change in thecolor scale used. If the peak pressure represented by the red (topend of the scale) is not clearly presented and held the same for allimages, the interpretation can become very misleading.
Figure 6. The two interface pressure images shown here repre-sent the same dataset (the same individual, same surface, andsame raw data file). The differences are solely due to a change inthe color scale. This can be very useful in calling the reader’s at-tention to a point of interest. However, it can also be very mislead-ing if the reader is not aware of the change.

July—August 2003 227
these variables must be considered. Comparisons of sin-gle interface pressure maps, such as those often seen inmarketing advertisements, often are misleading. Thepractitioner evaluating the surface must know that thecolor scale or visual presentation of the data can bechanged easily. This ability to manipulate the color andvisual presentation can seriously hamper the readers’ abil-ity to draw valid conclusions. Table 1 depicts a system forevaluations.
CONCLUSION
The health care provider is ultimately responsible formaking decisions about support surfaces. The caregivermust be knowledgeable about the effects of support sur-faces and evaluate data from different surfaces to choosethe optimal support surface for individual patients. To dothis, the provider must be able to read and interpret the sci-ence that manufacturers use regarding their products.
REFERENCES1. Barczak C, Barnett R, Childs E, Bosley L. Fourth national pressure ulcer preva-
lence survey. Adv Wound Care 1997;10(4):18-26.2. O’Dea K. The prevalence of pressure sores in four European countries. J Wound
Care 1995;4:192-5.3. Maklebust J, Sieggreen M. Etiology and pathophysiology of pressure ulcers. In:
Maklebust J, Sieggreen M, editors. Pressure ulcer guidelines for prevention andnursing management. 2nd ed. Springhouse (PA): Springhouse Publishing; 1996.p. 19-27.
4. Ferrel B, Osterweil D, Christenson P. A randomized trial of low-air-loss bedsfor treatment of pressure ulcers. J Am Med Assoc 1993;269:494-7.
5. Frantz R, Xakellis G. Characteristics of skin blood flow over the Trochanterunder constant, prolonged pressure. Am J Phys Med Rehabil 1989;68:272-6.
6. Burman P. Using pressure measurements to evaluate different technologies.Decubitus 1993;6(3):38-42.
7. Ferguson-Pell M, Bell F, Evans J. Interface pressure sensors: existing devices,their suitability and limitations. In: Kenedi R, Cowden J, editors. Bedsorebiomechanics. Baltimore: University Park Press; 1976. p. 189-97.
8. Ferguson-Pell M, Cardi M. Prototype development and comparative evaluationof wheelchair pressure mapping systems. Assist Technol 1993;5:78-91.
9. Shelton F, Barnett R, Meyer E. Full body interface pressure testing as a methodfor performance evaluation of clinical support surfaces. Appl Ergon1998;29:491-7.
10. Krouskop T. Selecting a support surface. Can ET J 1990;9:5-14.11. McLean J. Pressure reduction or pressure relief: making the right choice. J ET
Nurs 1993;20:211-5.12. Nicol K, Henning E. Time-dependent method for measuring force distribution
using a flexible mat as a capacitor. In Komi P, editor. Biomechanics V.B.Baltimore: University Park Press; 1976. p. 433-40.
13. US Department of Health and Human Services. Vital & Health Statistics series11 survey 1976-1980.
14. Barnett R, Shelton F, Gebhart EJ, Childs EJ. The clinical efficacy of variousheel pressure management methods. Transactions of the 30th AnnualConference of the Wound, Ostomy, and Continence Nurses Society; Salt LakeCity, June 14-18, 1998.
15. Barnett R, Ablarde J. Skin vascular reaction to short durations of normal seat-ing. Arch Phys Med Rehabil 1995;76:533-40.
16. Barnett R, Shelton F. Measurement of support surface eficacy: pressure. AdvWound Care 1997;10(7):21-9.
17. Barnett R, Ablarde J. Skin vascular reaction to standard patient positioning ona hospital mattress. Adv Wound Care 1994;7(1):58-65.
FREDERICK SHELTON, MS, is a senior engineer with Enigma Limited inHillsboro, Ohio. JUDY WRIGHT LOTT, DSN, RNC, NNP, is dean and aprofessor of nursing in the Baylor University Louise Herrington School ofNursing in Dallas,Texas.
© 2003 Mosby, Inc. All rights reserved.0197-4572/2003 $30.00 + 0doi:10.1067/mgn.2003.63
• Evaluate appropriateness of measurement device used according to variables (size, creep, drift, flexibility, resolution,accuracy, and repeatability).
• Examine the accuracy of the statistical tests, including significance and sample size.
• Evaluate appropriateness of measurement techniques, positions, and subjects.
•Evaluate type of surfaces used, including some “control surfaces,” to bracket where the test surfaces are in the over-all range of performance.
• Look for evidence of full body interface pressure mapping, in addition to single body site mapping. Full body aver-ages should be the first evaluation, then local pressure measurements in critical areas.Vascular analysis also mightbe necessary if further evidence is required.
• Analyze graphical scale and color representation of data display. Be sure this displayed scale is related to a knowncontrol surface or condition, etc. Raw pressure in mm Hg is not necessarily good enough or even appropriate.
Interpretation of A Surface Interface Pressure AnalysisTable 1.