-
Conduct Disorder and Cognitive Functioning:Testing Three Causal
Hypotheses
Irvin Sam SehonfeldCity College of New York and the College of
Phystctans and Surgeons,
Columbia Universtty
David ShafEFerCollege of Phystdans and Surgeons, Columbta
Universtty, and New y ork
State Psychtatrtc Instttute
Patricia O'ConnorRussell Sage College
Stephanie PortnoyNew York State Psychtatnc Instttute
SCHONFELD, iRVIN S A M , SHAFFER, D A V I D , O'CONNOR,
PATRICIA, and PORTNOY, STEPHANIE ConductDisorder and Cogntttve
Functtontng Testing Three Causal Hypotheses CHILD
DEVELOPMENT,1988,59,993-1007 The sample consisted of hlack
adolescents who were memhers of the Columhia-Presbytenan chapter of
the Collahorabve Pennatal Project from hirth to age 7 At age 17,
suhjectsand tfieir parents were administered a hattery of
instruments that included standardized psychiatncdiagnosbc
interviews as pait ol a call-hack study Results from least-squares
and logisbc regressionanalyses were compabhle with the hypothesis
that deficiencies m cognitive funcboning are causallyrelated to
adolescent conduct disoider as defined hv DSM III The results
suggested that therelabon of cognibve funcboning to psychiatnc
status appears to he specific to conduct disorders Theresults were
lncompabble widi a "third" vanahle hypothesis (third factors
included neurologicalstatus and environmental disadvantage) and the
hypothesis that conduct prohlems lead to deficits incogmbve
funcbomng Tlie 3 most (and equally) important factors m accounting
for age-17 conductdisorder were cognibve funcboning, parent
psychopathology, and early aggression A closer look atthe data
tentabvely suggested that a hroad deficiency in acculturabonal
leaming, rather than nar-rowly focused social cognibve differences
or nabve endowment, consbtutes a kev element in thelink hetween
cogmbve funcboning and conduct disorder Test hias was ruled out as
a possihleexplanabon for die results
A Widely observed finding m epidemi- borough (Berger, Yule,
& Rutter, 1975) In anologic surveys and in studies of referred
sam- epidemiologic survey of black youngsters re-ples has been the
associabon between con- sidmg m households in the Woodlawn sec-duct
disturbance and deficits in cognibve bon of Chicago, Kellam,
Branch, Agrawal,funcboning On the Isle of Wight, Rutter, and
Ensminger (1975) found that aggressionTizard, and Whibnore (1970)
found that, measured m the first grade was negabvely as-among 10-
and 11-year-olds, children with sociated with concurrent and
third-grade IQconduct disorders tended to have lower IQ In a total
populabon survey of an upstate Newscores tfian neurobc and
nondeviant conbol York county, Huesmann, Eron, Lefkowitz,youngsters
These findings were replicated m and Walder (1984) showed that a
well-con-an epidemiologic survey of an inner London ceived measure
of aggression at age 8 was
The sbidy was supported hy center grant MH 306906 and research
training grant 5 T32 MH13043-13 from the Nabonal Insbtute of Mental
Health as well as hy the City Co lege and the C ^University
Compubng Centers We tiiank Pabicia Cohen, Bruce Link, Jill
Goldstein and threeanonymous reviewers for theu cnbcal comments on
an earlier version °f *e . ^ ^ ' ^ / ' * ' " ; ^ ^versions of this
article were presented at the 1984 meebngs of die Society for
EP'^emiolo^^Research and the Society for Life History Research m
Psychopathologv Correspondence shouW besent to Irvin Sehonfeld,
Deparbnent of Social and Psychological Foundabons, City College of
NewYork, 138A St and Convent Avenue, New York, NY 10031
[Cfc^ De^Jopment, 1988, 5^ 993-l«r7 C 1988 by Ae Soc^ty for
Beseaid, m ^ ^
All rights reserved 00(»-39a0«8/5804-0019$0100]
-
994 Child Development
significantly related to a contemporaneousmeasure of IQ Robins
(1966), in a long-termfollow-up of a chnic-referred sample of
whiteSt Louis youngsters, found that educabonallevel was inversely
related to the rate atwhich individuals were diagnosed for
socio-pathic personality 30 years later Famngton(Famngton, 1978,
West & Famngton, 1973)found that IQ was inversely related to
officialand self-reported delinquency among Englishworlang-class
boys Lewis, Shanok, and Pin-cus (1981) found that, among
incarcerated de-linquents, those classified as very violenttended
to perform less well on a psychoedu-cabonal battery that included
IQ and readingand madiemabcs achievement tests than lessviolent
p)eers
The relabon between IQ and delin-quency may be spunous since IQ
test per-formance IS related to race and social class,and race and
social class are related to delin-quency In response to such an
argument,Hirschi and Hmdelang (1977) adduced evi-dence firom an
array of research reports show-ing that IQ IS related to both
officially re-ported and self-reported delinquency tvtthinrace
and/or class That the relabon holds fordelinquency rates based on
self-reportsweakens the argument for spunousness ow-ing to biases
in detecbon (Hirschi & Hin-delang, 1977, West & Famngton,
1973)
At least three hypotheses explain the as-sociabon between
anbsocial behavior or con-duct disorder, on one hand, and deficits
incognibve funcboning on the other One hy-p)Othesis IS diat conduct
problems lead toinadequate school leaming and attendantdeficits m
cognibve funcboning Given thewell-documented influence of educabon
oncognibve development (Luna, 1976, Sharp,Cole, & Lave, 1979),
the obstmcbng of class-room procedures by students exhibibng
anb-social behaviors may have a retarding effecton cognibve
development m those same stu-dents A second hypothesis is that
cognibvedeficits lead to antisocial behavior, either di-rectly or
through some mediabng condibonRutter and Gdler (1983) argued that
one van-able linking low IQ to conduct disorder ordelinquency may
be the individual's re-sponse to educabonal failure Low IQ
mightalso be associated with inadequate socialsfaUs or coping
behaviors, which m tum leadto fiiistrabng expenences in mteracbng
withodiers and, consequently, to aggression Adurd hypothesis is
that cogmbve deficits andanbsocia] behavior are spunously
associatedbecause some explanatory antecedent factor
(or fectors) is causally related to both (see Sus-ser, 1973)
The first hypothesis (conduct difficulbes- • cognibve deficits)
is inconsistent with anumber of findings Since the average
correla-bon between IQ test scores obtained at ages 5and 17 is
about 7 (e g, Bloom, 1964), it islikely that depressed IQ test
performance ob-served m adolescence is linked to depressedcognibve
funcboning earlier in the life span,temporally preceding
delinquency if notmore mfanble expressions of anbsocial be-havior
This IS not to say that a somewhat sta-ble enbty like IQ is
impervious to other in-fluences, the results of three
epidemiologicsurveys, however, are inconsistent with ^ efirst
hypothesis Kellam et al (1975) found anassociabon between low IQ
and aggressivebehavior in first grade, early enough in theschool
careers of children to cast doubt on theconduct-problems-as-cause
hypothesis Rich-man, Stevenson, and Graham (1982) foundthat low IQ
was related to conduct problemsas early as ages 3 and 4, well
before entry intoschool In addibon, Richman et al (1982)were unable
to find changes m intellectualfuncboning to be associated with
changes inconduct problems in their 5-year follow-up of3- and
4-year-olds Rutter, Graham, Ghad-wick, and Yule (1976) and Rutter,
Tizard,Yule, Graham, and Whitmore (1976) alsofound that changes m
psychiatnc status werenot associated with changes m IQ m their
4-year follow-up of the 10- and 11-year-oldsseen on the Isle of
Wight The results of thesestudies indicate that remission m
problemstatus was not associated with change in intel-lectual
status, although it might take longerthan 4 or 5 years for changes
in intellectualstatus to appear
The second hypothesis (cognibve deficits—»• conduct difficulbes)
has modest and indi-rect support in the results of Rutter et
al(1970) Their findings apply to the deficien-cies in the cognibve
skills pertaining to read-ing, but not IQ Families of
conduct-disorderchildren with reading retardabon had signifi-cantly
lower rates of parental discord thanfemilies of conduct-disorder
children withoutreading retardabon, consistent with the viewthat
there are at least two routes to conduct-disorder outcome response
to educabonalfeilure and response to parental discord Re-sponse to
educabonal feilure may have led toconduct disorder m the
reading-retarded sub-group since those children did not differ
fromcontrols m rate of parental discord By con-trast, die femdies
of anbsocial chddren who
-
were not reading retarded tended to show sig-nificantly higher
rates of parental discord thancontrol youngsters
Other indirect support for the second hy-pothesis comes from
Ayllon and Roberts(1974), who found that reducbon in
classroomanbsocial behavior resulted from behaviormodificabon
efforts aimed specifically at im-proving academic performance The
conbn-gencies employed were indifferent to theanbsocial acbvibes in
which the childrenwere engaged Limitabons of this study werethat
subjects came from predominantly uppier-middle-class homes, and
academic perioT-mance was, at a minimum, on grade level
If conduct problems lead to cognibvedeficits or, altemabvely, if
cognibve deficitslead to conduct problems, the outcomeswould take
some bme to develop The schoolcan be expected to consbtute the
chief con-text m which these outcomes emerge becauseit IS the site
m which (a) social mteracbonwith peers is accelerated and (b)
cognibve-academic funcboning takes a prominent placem the child's
life The third hypothesis (thirdvanable —• cognibve deficits, third
vanable —>conduct difficulbes) has noteworthy supportin the
Richman et al (1982) results, whichshow that IQ and conduct
problems are asso-ciated as early as age 3, and in the Kellam etal
(1975) results, which show that anbsocialbehavior is associated
with low IQ as early asgrade 1 Gonduct problems and
cognibvedeficits are linked too early in life for one tocause the
other over the long course school-ing In addibon, Huesmann et al
(1984) andOlweus (1979) found that aggressive behaviorm males has
much the same stability as IQ ItIS therefore possible that, among
males, theongins of conduct problems and deficienciesin cognibve
funcboning anse from commonfectors Candidate fectors include
impairedsocializing skills in ptarents owing, jjerhaps, toparent
psychopathology and early tempera-mental differences in the child
(Rutter et al,1970) In the Huesmann et al (1984), Kellamet al
(1975), and Richman et al (1982) sam-ples, males exhibited more
disturbance thanfemales Such findings are compabble withboth
socializabon and temperament explana-bons Gounterevidence adduced
by Rutter etal (1970) suggests that temperamental fectorsmay not
explain tiie associabon between poorcognibve funcboning (as
manifest m readingretardabon) and conduct disorder becauseanbsocial
behavior appears to be associatedwith reading retardabon that is
either social orbiological m ongm
Sehonfeld et al. 995
In the present invesbgabon, we studiedthe relabon between
cognibve funcboning, asmanifest in IQ and achievement test
perfor-mance, and DSM III (Dtagnosttc and Stattstt-cal Manual of
Mental Dtsorders, Thtrd Edi-tion) categones of conduct disturbance
Thisstudy consbtutes an extension of researchconducted pnor to the
development of theDSM III nomenclature, and our purpose wasto test
the validity of the nval hypotheses thatpotenbally explain the
associabon betweencognibve funcboning and conduct distur-bance
The sample studied consisted of blackmales who parbcipated m a
follow-up studyof the psychiatnc and medical sequelae,
madolescence, of neurological soil signs diag-nosed at age 7
(Shaffer et al, 1985) Blackmale subjects were followed for pracbcal
rea-sons at the medical center at which the studvwas conducted,
they had the highest preva-lence rate of soft signs at the age of 7
Thisselecbon decision, however, limits the gener-alizability of the
findings to other racial andethnic groups, as well as to females
Never-theless, the nature of the sample studied andthe
methodological strengths of the invesbga-bon make it possible to
compare the threehypotheses menboned First, the sample
wasunreferred and unselected for conduct disor-ders, and the
subjects were representabve ofyoungsters from black northem
Manhattanhomes Second, data captunng the environ-mental
disadvantages of the subjects werecollected Third, the neurologic
status of allsubjects was assessed Finally, IQ was mea-sured at
both ages 7 and 17 with the appropn-ate Wechsler scales The
linkages betweenpsychopathology and performance on sub-tests
reflecbng relabvely high and low levelsof acculturabonal leaming (e
g, lnformabonand Block Design, respecbvely) could thus beassessed
(see Gattell, 1963)
Method
Sample —Subjects were members of theGolumbia-Presbytenan Medical
Center chap-ter of the nabonwide GoUaborabve PennatalProject (GPP)
At this site, between 1957 and1963, approximately one in five
mothers con-secubvely presenbng for prenatal care wereaccepted into
the study Only planned adop-bon donors and mothers who failed to
presentfor prenatal care were excluded The researchteam followed
the children unbl their eighthyear Gall-back subjects followed by a
differ-ent team at age 17 consbtuted two groupsOne included
nonretarded black, English-
-
996 Child Development
si>eaking males who met the following cnte-na (a) membership
m the 1962-1963 birthcohort, (b) a posibve diagnosis for any one of
anumber of neurological sofl signs dunng theage-7 medical
examinabon, and (c) no evi-dence of other neurological problems
Thesecond group consisted of nonretarded malesmatched to members of
the first group on dateof birth, race, and language Members of
thesecond group, however, were required to ex-hibit no evidence of
soft or hard neurologicalsigns
At the bme of the follow-up, 63 maleswho received index rabngs
for soft signs atage 7 were matched with 63 sign-free individ-uals
A total of 61 sign-posibve males wereassessed at age 17 Three of
the 61 were laterexcluded because either a major
neurologicaldisorder or a be, missed in an earlier reviewof the
medical records, was documented in alater record check Thus the
sign-posibvesample was reduced to 58 Of the 63 m thesecond sample,
57 were reexammed at age17
Procedures —At the bme of the age-17follow-up, psychiatnc,
neurological, and cog-nibve exammabons were conducted on thesame
day for almost all of the subjects by in-dej)endent examiners with
no knowledge ofthe subjects' status on the archival measuresA
descnpbon of the psychiatnc assessmentprocedures can be found m
Shaffer et al(1985) The neurological examinabon is de-scnbed m
Stokman et al (1986) Gonnors's(1969) Teachers Quesbonnaire, an
inventoryto assess the extent of deviant classroom be-haviors (e g,
stealing, lnattenbon), was com-pleted by each of the subject's most
recentmathemabcs, English, and social studiesteachers close to the
bme of the psychiatncexaminabon
Cognitive examination—The cognibvebattery consisted of the
Wechsler Adult Intel-ligence Scale (WAIS) and tiie Peabody
Indi-vidual Achievement Tests (PLAT) for readingcomprehension,
mathemabcs, and spellingBased on the work of Bannatyne (1971),
scaleswere constructed from WAIS subtests to re-flect success m
acquinng knowledge (lnfor-mabon -I- Vocabulary -i- Anthmebc) and
spa-tial ability (Block Design + Object Assembly+ Picture
Gomplebon) The scales were con-structed m order to locate tiie core
of the IQ-related differences occumng with conductdisorder While
these scales have been usedextensively with the WISC and tiie
WISG-R(Kaufinan, 1982), Bannatyne (personal com-munication, 1^4)
indicated that they applyequally to the WAIS According to Hom
(1979), the acquired knowledge and spatialabdity scales reflect,
resjjecbvely, accultura-bonal (crystallized) and nabve (fluid)
aspectsof intelligence In order to assess the applica-bility of the
scales in the present sample, anumber of reliability coefficients
were com-puted The lntemal consistency reliabilibesfor the acquired
knowledge (alpha = 82) andspabal abilibes (alpha = 76) scales
weresabsfactory Although the scales were signifi-candy correlated
with each other (r = 54, p <001), the coefficient of tiie
reliability of thedifferences (Cohen & Cohen, 1983) is
consis-tent with the view that the scales measureddifferent
constructs (r[A_B)[A-B] = 54) Aminimally acceptable value for such
a coeffi-cient has been thought to be 50 (Dohren-wend, Shrout, Egn,
& Mendelsohn, 1980)
Psychtatnc diagnoses —As part of thepsychiatnc evaluabon of the
adolescent, thesubject and his parent (usually the
mother)separately received semi structured inter-views that were
constructed frcn exisbng ln-stmments (Shaffer et al 1985) The
interviewof the adolescent included porbons of theSchedule for
Affecbve Disorders and Schizo-phrenia (Spitzer & Endicott,
1977) to assessaffecbve and anxiety symptoms, elements ofan
interview wntten by Rutter and Graham(1968) to assess anbsocial
behaviors, and anumber of new items designed to elicit symp-toms
needed to assign DSM III diagnosesThe parent interview was adapted
frxim an in-strument developed by Rutter and Brown(1966) to gather
sociodemographic data onfemily members and psychiatnc data on
theadolescent The General Well-Being Scale(GWB, Dupuy, 1974) was
also incorporatedinto this interview The GWB assesses psy-chiatnc
funcboning in the caretaker, includ-ing visits to mental health
clinicians and de-pressive symptoms
At the conclusion of each parent and ado-lescent interview, the
interviewer assignedtiie adolescent a Global Assessment Scale(GAS)
rabng (Endicott, Spitzer, Fleiss, & Co-hen, 1976) The GAS is a
conbnuous mea-sure, ranging from 0 to 100, of psychiatncfuncboning
m the adolescent Higher scoresreflect sabsfectory social funcboning
and lowlevels of symptoms, and lower scores, un-paired funcboning
and high levels of symp-toms If a subject received a rabng of 70
orlower on either interview, or if a subject re-ceived a rabng of
75 or lower when only oneinterview was conducted, a case
conferenceon the subject's psychiatnc status was held Ina separate
study of a subsample of nine sub-jects involving four to seven
raters blind to
-
Sehonfeld et al. 997
each other's rabngs, we obtained 79% agree-ment m assigning
subjects GAS scores aboveand below the caseness marker of 70
(Shafferet al , 1986)
At the case conference, two psychiatnstsand one psychologist
reviewed all relevantparent and adolescent interview data
andteacher reports but no other contemporaneousrecords, case
conferees did not know the sub-jects' status on the archival
measures NewGAS scores and as many Axis 1 DSM-111diagnoses (the
clinical syndromes) as applica-ble were assigned by tiie conferees
No ex-clusionary rules were invoked, therefore, sub-jects could
receive more than one diagnosisAny adolescent who received a mean
GASrabng of 70 or less from the conferees wasassi^ed at least one
diagnosis Subjectswhose high interview-based GAS values ex-cluded
them from the conference received nodiagnosis These individuals
were assigned afinal GAS rabng that was the mean of the rat-ings
assigned by the two interviewers
ArchtiMl data —An earlier generabon ofresearehers had collected
data on all subjectsin childhood (see Nichols & Ghen, 1981,
fora complete descnpbon of the early data)Retneved psychological
data included theStanford-Binet and WISG IQ scores obtaineddunng
the age^ and age-7 psychologicalexaminabons, respecbvely Only seven
sub-tests of the WISC (Verbal lnformabon. Com-prehension,
Vocabulary, Digit Span, Perfor-mance Picture Arrangement, Block
Design,Coding) were administered at age 7, age-7 IQwas prorated
(see Nichols & Chen, 1981)Psychologists rated a number of
subject be-haviors, using forced-choice rabng scales,dunng the
age-7 psychological examinabonThe age-17 team, who did not know the
sub-jects' status on otiier vanables, selected threeage-7 behavior
rabngs m construcbng an apnon scale to reflect age-7 aggressive
behav-ior (alpha = 78, see Shaffer, O'Connor,Shafer, & Pmpis,
1983) The tiiree behaviorsm tiie scale were negabvism (0—responds
todirecbons, 1—resbve m response to direc-bons, 2—extremely
negabve), dominabngaggressiveness (0—unasserbve to
normallyasserbve, 1—forceful, 2—dominabng aggres-sive behavior),
and hosblity (0—appropnateto negabve affect, 1—uncooperabve or
angry,2—overt physical or verbal attacks)
Health lnformabon retneved from theearly necords included data
from the age-7neurologic^ examination (Nichols & Chen,1981),
Six groups of neurological soft signswere diagnosed awkwardness or
poor coordi-nabon in Bnger-nose touching, finger pursuit.
and fine motor acbvity (the most frequentlydiagnosed
neurological signs), dysdiadocho-kmesis (difficulbes m performing
rapid al-temabng movements of the hands or feet),mirror movements
(inability to inhibit move-ments in the hand opposite the hand
perform-ing a simple task), bemor, dysgraphesthesia(incorrect
ldenbficabon of a predisplayedsymbol baced on the palm when
blind-folded), and astereognosis (incorrect ldenbfi-cabon of
three-dimensional objects on theoutstretched hand when blindfolded)
Test-retest agreement on a CPP subsample wasfound to be 85% for the
signs involving poorcoordinabon (Nichols & Chen, 1981)
Shafferet al (1985) provided addibonal, indirect evi-dence that the
age-7 signs were reliably mea-sured Other types of archival data
retnevedinclude (a) two single-item responses, oneobtained at about
the bme of the subject'sbirth and another at the bme of the age-7
ex-aminabon, conceming the presence of "men-tal illness" m the
family, and (b) an ordinalmeasure of age-7 family income
ResultsClasstficatton of dtsorders—Table 1
enumerates all diagnoses given the age-17call-back sample For
the purpose of data re-ducbon, two psychiatnsts and one
psycholo-gist sorted the diagnoses into five superordi-nate
categones affecbve disorders, conductdisorders, anxiety-withdrawal
disorders, sub-stance abuse, and psychobc disorder Thegroupings are
consistent with child psychiatrynosology (Rutter, Shaffer, &
Sbirge, 1975)Agreement on assignment to the categonesexceeded 90% A
total of 64 adolescents wereldenbfied as having no disorder, and 30
werefound to have a conduct disorder, eithersingly (18) or in
combinabon with some otherdisorder (12)
Scale constructton —Data from the par-ent interview were used to
construct two apnon scales reflecbng types of adversity tiiatcan
affect the adolescent's psychiatnc stabisparent psychopatiiology
and envu-onmentaldisadvantage The parent psychopathologyscale
compnsed five vanables motiier's dys-phonc mood, motiier or fatiier
having visiteda psychiabist/psychologist cnminality meitiier parent
and parental discord (based oninterview items on parental
quan-eling) Theenvu-onmental disadvantage scale compnsedseven
vanables low family income, mothernot being mamed to the biological
fether,lower levels of educabon m tiie motiier orfetiier, four or
more sibhngs, welfere depen-dency and dissabsfacbon witii housing
Thus
-
998 Child DevelopmentTABLE 1
DISTRIBUTION AND GROUPING OF AGE 17 DSM III DIAGNOSES
Frequency
Conduct312 00, Conduct disorder, undersocialized, aggressive
2312 21, Conduct disorder, socialized, nonaggressive 14312 23,
Conduct disorder, socialized, aggressive 6313 81, Opposibonal
disorder 5314 01, Attenbon-deficit disorder, with hyperactivity
3314 80, Attenbon-deficit disorder, residual 1
Affecbve295 70, Schizoa£Fecbve disorder 1296 20, Major
depression, single episode, unspecified 2296 22, Major depression,
single episode, without melancholia 2296 32, Major depression,
recurrent, with melancholia 1296 36, Major depression, recurrent, m
remission 2296 56, Bipolar disorder depressed, m remission 1296 82,
Atypical depression 3300 40, Dysthymic disorder 5309 00, Adjustment
disorder with depressed mood 3
Anxiety-withdrawal300 00, Atypical anxiety disorder 1301 29,
Schizotypal personality disorder 1309 21, Separabon anxiety
disorder 1313 00, Overanxious disorder 9313 21, Avoidant disorder
of adolescence 3
Suhstance ahuse305 01, Alcohol ahuse, continuous use 1305 21,
Cannahis ahuse, conbnuous use 5305 91, Other, mixed suhstance
ahuse, conbnuous use 1
Psychobc disorder295 32, Schizophrenia, paranoid type, chronic
1
Total 74
NOTE —This table presents a complete hst of all diagnoses given
A subject may receive more than one diagnosis
the environmental disadvantage scale encom- unrefeted to the
age-17 environmental disad-passes the tradibonal socioeconomic
lndi- vantage scale, t( 100) = 1 60, (fc) age-7 femilycators as
well as other tyx)es of adversity income was significantiy
correlated to age-17
Items for each scale were range standard- TTf*?"^'**^, ''f'^f^^^
f̂'P = - 4 7 - P <.zed before being aggregated In mnge stan- ^[^
^ut um-elated to age-17 parent psycho-dardizmg tiie items, a score
of zero was given PatholoKV ^^P " "o, î » ;to tiie opbmal response
category (e g , college jf^ stabtltty of IQ test performance
—degree m tiie matemal educabon Item) and a Cogmbve fUncbonmg as
measured by tiiescore of one was given to tiie most adverse age-17
WAIS IQ was found to be moderatelyresponse (e g, elementary school
educabon) conelated with age-7 WISC (r = 66, p <Intennediate
response altemabves were as- QQI) and age-4 Stanford-Binet IQ (r =
50, psigned proporbonally intennediate values be- < QOI) Age-7
and age-4 IQ were also moder-tween zero and one Thus in both scales
^^ely correlated (r = 61, p < 001)higher scores reflected
increasing levels ofadversity The alpha coefficients for the par-
Conduct disorder and cogmtive func-ent psychopathology and
environmental dis- tioning —Table 2 presents the mean scores
ofadvantage scales were 56 and 62, respec- conduct-disorder and
disorder-free adoles-bvely A substudy of the scales' convergent
cents, with and without soft signs, on the cog-and dliscruninant
validity suggested the scales nibve tests administered at age 17
For eachwere adequate (a) t tests revealed that the measure of
cognibve funcboning a two-wayarchival record of the presence versus
ab- (conduct disorder present/absent x soft signssence of family
mental illness was signifi- present/absent) analysis of vanance was
per-cantly related to the age-17 parent psycho- formed The analyses
revealed conduct-patiiology scale, f (100) = 3 16, p < 01, and
disorder main effects for full-scale IQ, F(l,87)
-
Sehonfeld et al. 999TABLE 2
AGE 17 TEST PERFORMANCE OF CONDUCT-DISORDER SUBJECTS WITH AND
WITHOUT EARLY SOFT SIGNS
CROUP
Signs absentNo disorder
MSD
Conduct disorderMSD
Signs presentNo disorder
MSD
Conduct disorderMSD
FIQ
9609 8
9058 5
905117
838110
WAIS
VIQ
9 6 09 6
89 78 0
91512 2
852115
PIQ
96412 1
92 812 3
90512 1
840116
ReadingComp
9 1 613 8
87 112 1
88712 1
82 313 1
PEABODY
Math
95 310 8
87 0115
90313 3
82 3117
Spell
89 613 4
89 812 8
8 6 014 2
78 914 7
ACQUIRED
KNOWLEDGESCALE
23 151
19 04 4
2 2 273
18 053
SPATIALSCALE
27 670
2596 9
24 372
22161
= 6 69, p < 05, verbal IQ, F(l,87) = 6 96, p< 01, PIAT
Matii, F(l,87) = 9 31, p < 001,and the acquired knowledge scale,
F(l,87) =10 12, p < 01 Marginal (p < 10) effects werefound
for performance IQ, F(l,87) = 3 56,and PIAT Reading, F(l,87) = 3 52
The anal-yses revealed soft-signs mam effects for full-scale IQ,
F(l,87) = 6 74, p < 05, perfor-mance IQ, F(l,87) = 7 60, p <
01, PIATSpelling, F(l,87) = 5 45, p < 05, and the spa-bal scale,
F(l,87) = 5 50, p < 05 Marginaleffects were found for verbal IQ,
F(l,87) =357, and PIAT Matii, F(l,87) = 3 29 Nosignificant
mteracbons were obtained
Table 3 presents the mean scores of theconduct-disorder and
disorder-free adoles-cents on cognibve tests administered at ages
4and 7 For each measure of cognibve func-boning, a two-way (conduct
disorder present/absent x soft signs present/absent) analysis
ofvanance was performed Because too few age-7 subtests were
available to construct ac-quired knowledge and spabal scales,
perfor-mance on lnformabon and Block Design(subtests related to
those constmcts) was ex-amined The analyses revealed
conduct-disorder main effects for full-scale WISC IQ,F(l,89) = 4
62, p < 05, verbal IQ, F(l,90) =
TABLE 3
AGE 4 AND 7 TEST PERFORMANCE OF CONDUCT-DISORDER SUBJECTS WITH
AND WITHOUTEARLY SOFT SIGNS
GROUP
AGE 4STANFORD-
BINET FIQ
AGE 7 WISC
VIQ PIQ
WISC
lnfor-mabon
SUBTESTS
BlockDesign
Signs ahsentNo disorder
AfSD
Conduct disorderMSD
Signs presentNo disorder
MSD
Conduct disorderMSD
99013 2
94810 7
94414 6
87 817 8
98489
94210 3
92 312 7
84617 5
9 6 0114
92 287
90612 8
80914 5
10138 6
97 213 2
95 714 5
9 1 6214
9 82 9
8814
873 1
6 8
35
10 72 0
10 82 8
8 92 8
86O KOO
-
1000 Child DevelopmentTABLE 4
CORRELATIONS BETWEEN VARIABLES EMPLOYED IN THE PATH ANALYSES
CASSignsPPEADisadvFull-scale WAIS IQFull-scale WISC IQConduct/no
disorder
GAS
- 20*- 25*- 29**- 26*
33***30**
- 93***
Signs
- 06- 04
01- 39***- 39***
17
PP
- 0944***071223*
EA
- 21*- 12- 16
25*
Disadv
- 28**- 14
18
WAIS
68***- 29**
WISC
- 26*
NOTE —Bivanate correlations were computed with n s that ranged
from 88 to 94 Signs = no of early signs, PPparent psychopathology
EA = presence/absence of earlv aggression Disadv = environmental
disadvantage
* p < 05"p< 01*•* p < 001
6 29, p < 05, and Infonnabon, F(l,90) = 5 25,p < 05 A
marginal effect was found for theage^ Stanford-Binet, F(l,83) = 2
70, p = 10The analyses revealed soft-signs main effectsfor
fiill-scale WISC IQ, F(l,89) = 8 10, p <01, verbal IQ, F(l,90) =
9 60, p < 01, andBlock Design, F( 1,90) = 1136, p < 001
Mar-ginal effects (p < 10) were found for the Stan-ford-Bmet,
F(l,83) = 3 09, and perfonnanceIQ, F(l,89) = 3 06 No significant
mteracbonswere obtained
Path analyses —In order to invesbgatefurther the relabon between
conduct disorderand its possible antecedents,
path-analybcprocedures were mboduced The correlabonmatnx used in
construcbng the path models ispresented m Table 4 A number of
assump-bons about the causal ordenng of the van-ables needed to be
made before conducbngthe j)ath analyses It was assumed that
theconstructs underlying full-scale WAIS IQ, en-vironmental
disadvantage, parent psychopia-thology, age-7 aggression, and soft
signs tookcausal precedence over age-17 psychiatncstatus This
assumpbon was partiy suppnirtedby the conbnuity of WAIS IQ,
environmentaldisadvantage, and parental mental healthwith related
archival measures, and thefinding that excessive aggressive
behaviorwas rare at age 7 (only seven subjects dis-played
measurable aggressive behavior dur-ing tesbng) Since soft signs
were measured atage 7 and are m some sense refiecbve of cen-tral
nervous system funcboning, they werethought to be causally pnor to
the onset of theconduct disorder The models made no as-sumpbons
about the causal order of soft signs,environmental disadvantage,
parent psycho-pathology, and early aggression Since one ofthe goals
of this invesbgabon was to assesstiie c(»nmon-antecedents
hypotiiesis, these
four vanables were considered to be causallypnor to both
full-scale WAIS IQ and CAS
In conducbng the path analysis, the sam-ple was limited only to
those subjects with aconduct-disorder diagnosis (n = 30) or
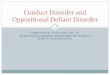
nodiagnosis (n = 64) In the full ptath model,depicted m Figure 1,
CAS was regressed(least squares) on five factors, including num-ber
of early soft signs, full-scale WAIS IQ,early aggression
(absent/present), the envi-ronmental disadvantage scale (converted
tostandard scores), and the parent psychopa-thology scale
(converted to standard scores),and IQ was regressed on the other
four fac-tors CAS consbtuted a global index of sever-ity of the
conduct disorder
Early
Envitoi>-••nUlDisadv
tarantPaycho-
pathDlogy
Ib ofearly
Soft SignsI M"
^lll-acaletiUS
10
-7 »(- 17)
(- 37)
-1 82
1- 12)
*p < 05"D< 01
•**£ < 001
FlC 1 —Full path model showing die effect ofeach exogenous
vanable on CAS and full-scaleWAISIQ
-
In order to maximize power, means weresubsbtuted for missing
values for the few sub-jects for whom scorable values were
absent(no more than four subjects lacked values onany one
predictor) Tests for systemabc differ-ences revealed no bias in the
occurrence ofmissing values (Cohen & Cohen, 1983) Itwas
tiiought that, if third vanables explain thezero-order relabon
between cognibve func-boning and conduct disturbance, the pathfirom
IQ to CAS would be nonsignificantwhen IQ and the other four
{X)tenbal causalfitctors were entered m the same regressionequabon
As can be seen in Figure 1, the pathfirom IQ to CAS was
significant, conbollingfor the other factors
Beginning with the full model, causallinks of negligible size
were eliminated Avanable was retained when two cntena weremet
within a regression fiamework (a) itspath coefficient attained the
10 significancelevel when entered in the model last, and(b) the
vanable accounted for at least 2% ofthe vanance in CAS or WAIS IQ
when en-tered m the model last Three predictors ofCAS—early
aggression, WAIS IQ, and parentpsychopathology—met these cntena
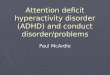
The tnmmed f>ath model is depicted inFigure 2 In this model,
causal paths from en-vironmental disadvantage and soft signs toCAS
were eliminated To facilitate under-standing of the model, both
unstandardizedand standardized (in parentheses) path coeffi-cients
were included in the diagram The un-
Qwicon-•anulDtaadv
tt> ofEarly
SDft Signa
Ea
fm
-lyMionl/*b
MnPay(
pattK
2 28*
mt* » ->logy
—]
( 20)
1
Full-ac4la
10 •-
-14 47*
1- 27)
-4 18**
{- 29)
-7 19(- 17)
40***
( 32)
(- 37)
• E 1 05**£ < 01•"e < 001
FIG 2 —Tnnuned patii model showing the ef-fiscts on GAS and WAIS
IQ of the exogenous vari-ables meeting causal cntena. Paths from
environ-mental disadvantage and early signs to CAS werednqq;>ed
The paA from early aggression and WAISIQ attained a p value of
10
Sehonfeld et al. 1001
standardized coefficients may be interpretedto indicate tiie
following relabons to CAS (a)adjusbng for the effects of the otiier
vanables,the presence of early aggression was associ-ated with a 14
47-point average decrease inGAS at age 17, (b) an adjusted increase
of 1SD in the parent psychopathology scale wasassociated with a 4
18-point average decreasein CAS, (c) an adjusted 1-point increase
in IQwas associated with a 40-point average in-crease in CAS Thus
an adjusted 15-point(1 SD) increase in IQ was associated with
a6-point average increase in CAS Similarly, a15-point decrease m IQ
was associated with a6-point decline in CAS
The unstandardized coefficients may beinterpreted to indicate
the following relabonsto WAIS IQ (a) adjusbng for tiie effects of
tiieother &ctors, each addibonal soft sign was as-sociated with
a 4 60-point average decrease inWAIS IQ, (b) an adjusted increase
of 1 SD inenvironmental disadvantage was associatedwith a 4
47-point average decrease in WAISIQ, (c) an adjusted increase of 1
SD in parentpsychopathology was associated with a 2 28-point
average increase in WAIS IQ, (d) thepresence of aggression at age 7
was associatedwith a 7 19-point average adjusted decrease inWAIS
IQ
The standardized path coefficients pro-vide an index of the
relabve effects of eachexogenous vanable on CAS or IQ The
threevanables (WAIS IQ, parent psychopathology,and early
aggression) exerted approximatelyequal effects on CAS The effects
of environ-mental disadvantage and early signs on IQwere more
sizable than the effects of earlvaggression and parent
psvchopathology Dis-advantage and early signs exerted about
equaleffects on WAIS IQ
Another path analysis (see Fig 3) of thefactors affecbng WAIS IQ
was conducted Incontrast to the previous analysis, age-7 WISCIQ was
introduced as a conbol vanable Thepreviously descnbed inclusion
rules gov-erned this analysis When WISC IQ was in-boduced, the
paths fix)m early aggression andparent psychopathology became
nonsignifi-cant owing to vanance shared with WISC IQ,however, the
paths from environmental disad-vantage and number of signs to WAIS
IQ con-bnued to meet causal cntena The two van-ables exerted about
equal direct effects onWAIS IQ Number of signs also exerted
indi-rect effects on WAIS IQ tiirough WISC IQAlthough we did not
construct an age-7 mea-sure of environmental disadvantage, we
ex-pected early disadvantage to have an adverseeffect on cognibve
funcboning The Spear-
-
1002 Child Development
EarlyAggraaaion
trm/Hs (- 27)
Envirrjo-•anUlDisadv
-2
(-
15*
19)
MrantE^yctD-
pathology
No ofEarly
Soft Signs
Pull-acaieMUS
FUil-acaUWISC
10
£ l**p <
***£ <01001
FIG 3 —Path model in which age-7 WISC IQwas entered as a control
vanable Wlien WISC IQwas entered, the padis from early aggression
andparent psychopadiology to WAIS IQ no longer metcausal
cntena.
man correlabon between age-7 family incomeand WISC IQ was 33, p
< 001 The Spear-man correlabon between early income andnumber of
signs was nonsignificant The cor-relabons were then recomputed
using para-metnc stabsbcs The first-order parbal corre-labon
between early income and WISC IQ,controlling for signs, was 27, p
< 01
Other analyses relevant to the path mod-els —We considered the
possibility that weimsspecified our path-analybc models Forexample,
adolescent psychopathology andWAIS IQ may influence each other
bidirec-bonally, or some third factor may cause bothWAIS IQ and CAS
In order to rule out tiiesealtemabves, we examined the WAIS IQand
CAS residuals using USREL procedures(Joreskog & Sorbom, 1981)
In each analysisthe residuals were uncorrelated, a result thatIS
lncompabble with those two possibihbes(Kenny, 1979)
Smce WAIS IQ is more reliable than anyother measure, it is
possible that its reiabon toCAS was enhanced compared to that of
theother pnedictors In response to this possibil-ity we recomputed
the standardized pathcoe£Bcients based on a correlabon matnx
inwhich the bivanate correlabons were cor-rected for attenuabon
(see Kenny, 1979) Thedirections of tiie effects paralleled the
find-ings obtained m tiie earlier analyses
To clanfy tiie relabon between cognibvefuncboning and conduct
problems sbll fur-ther, three addibonal path analyses were
con-ducted In each analysis, we subsbtuted oneof three altemabve
measures of cognibvefuncboning for WAIS IQ the acquiredknowledge
scale, the spabal scale, or age-7Wise IQ When the acquired
knowledgescale was subsbtuted for WAIS IQ, the pathcoefficient from
cognibve funcboning to CASwas significant (p < 01), when the
spabalscale was subsbtuted, the path coefficient wasnonsignificant,
when WISC IQ was sub-sbtuted, the path coefficient was
marginallysignificant (p < 06)
One final test was conducted to rule outthe possibility that
change in IQ from age 7 to17 (either increase or decrease) rather
thantrait IQ affected psychiatnc funcboning Theleast-squares
regression analyses were re-peated with an IQ change score
replacingfiill-scale WAIS IQ The results of tiie analy-sis failed
to reveal anything approaching aneffect for IQ change
Logtsttc regresston analysts —Becausepath analysis calls for the
use of conbnuousdependent vanables, CAS was used as a de-pendent
measure within a sample of youthswith a conduct disorder or no
disorder CAStherefore served as a proxy for conduct disor-der In
order to buttress the results of the pathanalyses, a logisbc
regression analysis wasconducted m which a dichotomous mea-sure—the
presence of conduct disorder ver-sus the absence of any
disorder—was re-gressed on the same five predictors (Cleary
&Angel, 1984) The results of tiie logisbc re-gression indicate
that early aggression, parentpsychopathology, and WAIS IQ were the
bestpredictors (p = 05) of conduct disorder whenentered into the
regression equabon last Theother two factors, environmental
disadvantageand signs, were unrelated to the disorder
Logisbc regression analysis was alsoused to compute the adjusted
odds rabo foreach of the three nsk factors for conduct disor-der,
controlling for the other two factors(Kleinbaum, Kapper, &
Morgenstem, 1982)The adjusted odds rabo for conduct disordergiven a
standard deviabon (15-point) decreasem full-scale IQ was 265 (p
< 01) If tiie ac-quired knowledge scale were subsbtuted
forfull-scale IQ, the adjusted odds rabo givena standard deviabon
(9-point) decrease was3 42 (p < 01) The adjusted odds rabo for
thepresence of early aggression was 2 34 (p <07), and for a
standard deviabon increase inparent psychopatiiology, 189 (p <
05)
-
In another logisbc analysis—the pres-ence of any anxiety
disorder (n = 20) versustiie absence of all disorders (n —
64)—wasregressed on the five predictors The resultsindicated that
WAIS IQ was unrelated to thepresence of anxiety disorders A
parallel anal-ysis indicated that WAIS IQ was unrelated tothe
presence of affecbve disorders (n = 30)Too few cases were available
to examine sub-stance abuse Cauboning that the n's aresmall, these
addibonal analyses suggest thatthe relabon of cognibve funcboning
to psy-chiatnc status IS specific to conduct disorders
Discussion
The results of the path analyses are con-sistent with the view
that three factors con-tnbute to the development of conduct
disor-der at age 17 IQ (whether measured at ages 7or 17), parent
psychopathology, and early ag-gression As reflected in the
standardizedpath coefficients, each factor exerted almostequivalent
effects on psychiatnc funcboningLogisbc regression analyses suggest
that IQ isspecifically related to conduct disorder, al-though tests
involving lai^er sample sizeswould be warranted in order to
cross-validatethis finding Profiles of the mean IQ scores
forconduct-disorder and disorder-free subjectstaken at different
bmes underline the consis-tency of the relabon of conduct disorder
tocognibve funcboning Least-squares and lo-gisbc regression
analyses, as well as tests formean differences, link conduct
disorder todeficits in acquired knowledge but not spabalability,
suggesbng that the ongins of the IQdeficits affecbng psychiatnc
status reside mthe individual's leaming environment Thefindings
involving change IQ and age-7Wise IQ suggest that endunng deficits
incognibve funcboning affect adolescent psy-chiatnc status
The acquired knowledge scale is thoughtto reflect crystallized
intelligence, an intellec-tual abdity believed to be highly
dependenton past leaming and acculturabon By con-trast, the spabal
ability scale is thought toreflect fluid intelligence, an
intellectual abil-ity believed to be h i^ ly related to
biological/hereditary factors (Sehonfeld, 1986)
Conduct-disorder-related differences are more pro-nounced on the
age-7 and -17 verbal IQ scalesthan on contemporary performance IQ
scalesHom (1982) noted that verbal IQ overlapssomewhat with
crystallized ability, and per-formance IQ shares features with
fluid abilityDifferences found on two of the three
age-17achievement tests are consistent with the pat-tem of IQ
findings Thus, the results tend to
Sehonfeld et al. 1003
be consistent with the view that long-termdeficits in cognibve
funcboning, parbcularlydeficits related to acculturational
knowledge,lead to conduct disturbance
The possibility that the findings may bethe result of
methodological factors needs tobe examined One methodological
factor con-cems the relabve reliabihbes of the differentmeasures
The mtemal consistency reliabilityof tiie WAIS IQ for 18- and
19-year-olds m tiiestandardizabon sample was 97 (Wechsler,1955),
considerably greater than the reliabil-lbes of the environmental
disadvantage andparent psychopathology scales Excessive er-ror
vanance in the environmental disadvan-tage and parent
psychopathology scales tendsto bias the effects to be detected, and
differ-ences in reliability favor the detecbon of IQ-related
effects (Kenny, 1979)
In response to the problem of differenbalreliabihbes, the
standardized path coeffi-cients were recomputed using
disattenuatedcorrelabons The paths from parent psychopa-thology,
early aggression, and WAIS IQ toCAS were sbengthened, but their
signs re-mained unchanged In addibon, when the ac-quired knowledge
scale was subsbtuted forfiill-scale IQ, the reliability of the
cognibvefuncboning vanable was weakened, the mag-nitude of the path
coefficient from cognibvefuncboning to CAS, however, was
increased
Although the path analyses suggest thatfull-scale IQ has a
direct effect on adolescentpsychopathology, it may be argued that
par-ent psychopathology, a factor related to ado-lescent conduct
problems, mediates both, andtherefore the relabon between low IQ
andadolescent psychopathology is spunous Anumber of findings argue
against this viewFirst, the signs of the path coefficient
fromparent psychopathology to WAIS IQ in thefirst two path diagrams
indicate that mildlyincreased parent psychopathology levels
areassociated with higher, not lower, levels ofIQ Second, the sign
of the path did notchange when disattenuated correlabons
wereemployed Third, the path from parent psy-chopatiiology to WAIS
IQ became nonsignifi-cant when WISC IQ was conboUed
The use of WAIS IQ consbtutes anotiierpotenbal problem because
of the possibilityof bias in tesbng black adolescents Bias
con-nected to tesbng, however, is minimal fortiiree reasons First,
tiie analyses were con-ducted withm, not between, race Second,
theIQ test results are consistent witii othersources of data on
deviant behavior That ado-lescents fiee of disorder perfonned
better
-
1004 Child Development
than adolescents with a conduct disorder isconsistent with a
body of literature involvingvery different samples (Hirschi fit
Hmdelang,1977) Third, the pattem of cross-age IQ cor-relabons IS
highly consistent with research in-volving other samples (Bloom,
1964) On theother hand, because the sample consists ex-clusively
of" black males, the generalizabilityof tiie results to whites and
females is limitedA longitudinal study involving whites andblacks
as well as males and females would beof great utility in
cross-validabng the presentfindings
One limitabon of the present study con-sists of the lack of
evidence on the distnbu-bon of moderate conduct problems m
earlylife The evidence on early aggressive behav-ior comes from the
psychologists' rabngs ofthe subjects' conduct dunng tesbng, hardly
anordinary sample of behavior It was assumedtiiat the subjects who
manifested any aggres-siveness dunng the age-7 psychological
ex-aminabon were likely to be excessively ag-gressive outside the
tesbng situabon sinceone-to-one psychological tesbng usually
in-hibits behavioral excess Support for this ex-pectabon comes
fix>m the finding that five ofthe seven call-back subjects who
had posibverabngs for aggression at age 7 were found tohave a
conduct disorder at age 17 This resultIS consistent with findings
based on othermeasures and other samples (Huesmann etal, 1984,
Olweus, 1979)
The results are not consistent with thehyjxrthesis that conduct
problems lead todefiats in cognibve funcboning The thirdpath
analysis mdicated that early aggressionwas unrelated to age-17 IQ
when age-7 WISCIQ was conbolled, althou^ a stronger testcould have
been conducted if a more differ-entiated measure of eariy
aggression wereavailable The sturdiest predictors of age-17IQ
outside of age-7 IQ were environmentaldisadvantage and soft signs,
results that areconsistent with the view tiiat both biologicaland
environmental handicaps adversely affectcognibve funcboning
Parallel relabons weremirrored m findings linking both age-7
disad-vantage, as captured by family income, andsoft signs to age-7
IQ
The results of the path analyses are in-consistent with the
common-antecedentshpotiiesis Soft signs, a factor that shared
anuxlerate but significant amount of vanancewith IQ, did not
consbtute a third vanablediat explained the IQ-conduct disturbance
as-sociation. The odier diree candidate diird fee-tors, parent
psychopathology, disadvantage,and early a^ression, also did not
explain the
IQ—conduct disturbance associabon It is pos-sible that some
unmeasured vanable consb-tutes the third factor that explains an
associa-bon In the present study, however, the fourpotenbal third
vanables were selected on thebasis of their known links to IQ and
conductproblems
Before going into some detail on the rela-bon of cognibve
funcboning to conduct prob-lems, we bnefly comment on the other
twofactors, early aggression and parent psychopa-thology, found to
affect psychiatnc status Inline with Olweus (1980), the measure of
earlyaggression used here might be interpreted asreflecbng early
temperament One weaknessin Olweus's measure of early
temperament,however, is that it was based on p)arent recallof
behavior occumng about 7 years pnor tointerview On the other hand,
the measurepertained to a broad band of behaviors Onestrength of
the measure of early aggressionemployed here is that it was based
on obser-vabons made dunng the i)enod of interest Atthe same bme,
the observabons pertained to anarrow band of behaviors Even so,
both theOlweus measure and the present one wererelated to later
conduct problems, suggesbngthat temperament might be implicated m
thedevelopment of anbsocial conduct
Consistent with pnor research, parentpsychopathology was found
to contnbute tothe development of conduct disorder in chil-dren
(Olweus, 1980, Rutter et al, 1970) Forwant of power to test each
factor individually,the parent psychopathology scale includeditems
reflecbng disturbance in either parentas well as in the mantal
relabonship as awhole Candidate mechanisms by which par-ents'
psychopathology contnbutes to conductproblems m their offspnng
include deviantsocializabon and impaired child-managementsblls
The quesbon of how the deficits m cogni-bve funcboning lead to
conduct disorder re-mains One explanabon is tiiat
educabonalfailure, a consequence of cognibve deficits,leads to low
self-esteem and antagonism toschool, paving the way for conduct
disorder(Rutter et al, 1970, Rutter & Ciller, 1983)This
hypothesis, however, is not consistentwith the distnbubons of
conduct-disorder anddisorder-fi:ee subjects expressing dislike
forschool in response to an item on the age-17adolescent interview
(57% vs 47%, N S ) Itshould, however, be noted that the results
arebased on responses to a smgle interview itemand thus subject to
instability
To develop an altemabve hypothesis, wedraw upon studies that
attempt to descnbe
-
how aggressive and rejected children processsocial infonnabon
Dodge (Dodge, 1980,Dodge & Frame, 1982) found that
aggressiveboys tend to show bias in processing parbcu-lar types of
social mformabon Compiaredto nonaggressive controls, aggressive
boystended to attnbute hosblity to peers issuingambiguous social
cues—especially cues di-rected toward themselves Vosk, Forehand,and
Figueroa (1983) found that, compared tosocially accepted children,
rejected childrentended to misinterpret affecbve states mothers
It should be noted that charactensbcs ofresearch on social
cogmbon include the re-liance on cross-secbonal designs and the
useof convenience samples Although not thepurpose of the Dodge and
Vosk studies, it isdi£Bcult, using cross-secbonal designs, to
testebologic hypotheses conceming the relabonbetween aggression and
cogmbon (MacMa-hon & Pugh, 1970) Aggressive behavior maycause
attnbubonal biases, or attnbubonal bi-ases may be spunously related
to aggressionbecause third factors, like pervasive develop-mental
difficulbes or deviant parental sociali-zabon pracbces, produce
both The use ofconvenience samples makes it difficult to de-scnbe
tiie charactensbcs of the populabon ofaggressive boys (Kleinbaum et
al , 1982) Withtiiese caveats m mmd, the social cogmbon lit-erature
IS helpful in developing altemabvehypotheses conceming the relabon
betweencognibve funcboning and conduct problems
Damon (1981) summanzed a line ofthought which holds that there
should be nodisbncbon between the processes involved macquinng
social and other types of knowledgebecause "all cogmbon is
lntnnsically social inongin" (p 162) Since IQ consbtutes an
om-nibus measure of cognibve funcboning, lowtest scores are likely
to be related to cognibvedifferences that appear in a vanety of
circum-stances, including situabons that call for theprocessing of
social mformabon Consistentwitii the data presented here, the
sourcesof differences in cognibve funcboning, asreflected in IQ
test performance, include bi-ological and environmental adversibes
It isunlikely that the s^gressive children studiedby Dodge, the
rejected children studied byVosk et al , and the conduct-disorder
childrenStudied here (samples which should be over-lapping) show
only differences in some cir-cumscnbed set of cogmbve behaviors
perb-nent to interprebng social cues It seemsequally, if not more,
plausible that differencesin understanding social cues emerge out
ofthe un&vorable learning contexts that give
Sehonfeld et al. 1005
nse to global deficits in cognibve funcboningThis explanabon is
consistent with thefindings revealing greater
conduct-disorder-related differences on IQ subtests
reflecbngacculturabon (e g, lnformabon, the acquiredknowledge
scale) than on subtests assessing amore nabve spabal ability (e g,
Block Design,the spabal ability scale)
Future research with representabve sam-ples of young people can
examine a vanety ofcognibve factors that potenbally increase thensk
for conduct problems Longitudinal de-signs could include, at two or
more p>oints inbme, omnibus cognibve measures, like theWechsler
scales, as well as more fine-grainedcognibve measures, like Dodge's
and Vosk'sSuch research would be very useful in test-ing ebologic
hypotheses conceming whichspecific cognibve differences contnbute
toconduct problems
References
Ayllon, T , & Roberts, M D (1974) Eliminabngdiscipline
problems by strengthening aca-demic performance Journal of Applied
Behav-toral Analysts, 7, 71-76
Bannatyne, A (1971) Language, reading, andleamtng dtsabtltties
Spnngfield, IL Thomas
Berger, M , Yule, W, & Rutter, M (1975) Attain-ment and
adjustment m two geographicalareas II The prevalence of specific
readingretardabon Bnttsh Journal of Psychiatry, 126,510-519
Bloom, B S (1964) Stabtltty and change tn humancharactensttcs
New York Wiley
Cattell, R B (1963) Theory of fluid and crystal-lized
mtelligence A cntical expenment Jour-nal of Educattonal Psychology,
54, 1-22
Cleary, P D , & Angel, B (1984) The analysis ofrelationships
involving dichotomous depen-dent vanables Journal of Health and
SoctalBehavtor, 25, 334-348
Cohen, J , & Cohen, P (1983) Applted
multipleregressum/correlatton analysts for the behav-toral sciences
(2d ed) HtUsdale, NJ Erlbaum
Connors, C K. (1969) A teacher rating scale for usein drug
studies with children Amertcan Jour-nal of Psychiatry, 126,
884-888
Damon, W (1981) Explonng children's social cog-nition In J H
Flavell & L Ross (Eds ), Soctalcogntttve development Frontters
and posstblefutures (pp 154-175) Cambndge CambndgeUniversity
Press
Dodge, K A (1980) Social cognition and children'saggressive
behavior Chtld Development, 51,162-170
Dodge, K. A, & Frame, C L (1982) Social cogni-bve biases and
deficits in aggressive boysChdd Development, 53, 620-«35
-
1006 Child Development
Dohrenwend, B P , Shrout, P E , Egn, C , & Men-delsohn, M D
(1980) Nonspecific psychologi-cal distress and odier dimensions of
psy-chopathology Archtves of General Psychtatry,2n,
122&-1236
Dupuy, H J (1974) Uttltty of the Nattonal Centerfor Health
Stattsttcs' General Well-BetngSchedule tn the assessment of
self-representa-ttons of subjective well-betng and dtstress Pa-per
presented at tfie National Conference ondie Evaluation of Drug,
Alcohol, and MentalHealdi Programs, Washington, DC
Endicott, J S , Spitzer, R L, Fleiss, J , & Cohen, J(1976)
The Global Assessment Scale Ar-chtves of General Psychtatry. 33,
766-771
Famngton, D P (1978) The family backgrounds ofaggressive youths
In L A Hersov, M Berger,& D Shaffer (Eds ), Aggression and
anttsocialbehaviour tn chtldhood and adolescence (pp73-93) Oxford
Per^mon
Hirschi, T, & Hmdelang, M J (1977) Intelligenceand
delinquency A revisionist review Amen-can Soctological Review, 42,
571-587
Hom, J L (1979) Intelligence and agtng Paperpresented at the
Symposium de la ClmiquePsychiatnque, Ceneva, Switzerland
Hom, J L. (1982) The aging of human abilibes InB Wolman (Ed),
Handbook of developmentalpsychology (pp 847-870) Englewood
Cliffs,NJ Prenbce-Hall
Huesmann, L R, Eron, L D , Lefkowitz, M M , &Walder, L O
(1^4) Stability of aggressionover bme and generabom Developmental
Psy-chology, 20, 1120-1134
Joreskog, K. G, & Sorbom, D (1981) USREL VUser's gutde
Chicago Nabonal EducabonalResources
Kaufrnan, A S (1982) Intelltgent testing wtth theWISC-R New York
Wiley
Kellam, S G, Branch, J D , Agrawal, D C , &Ensminger, M E
(1975) Mental health andgotng to school The Woodlawn Program
ofAssessment, Early Intervention and Evalua-tion Chicago Umversity
of Chicago Press
Kenny, D A. (1979) Correlation and causalityNew York Wiley
Klembaum, D G, Kupper, L L., & Morgenstem,H (1982)
Epidemtologic research Pnnctplesand quantitattve methods Belmont,
CALifistime Learmng
Lewis, D O, Shanok, S S , & Pincus, J N (1981)The
neuropsychiatnc status of violent maledelinquents In D O Lewis
(Ed), Vulner-abilities to delinquency (pp 67-88) NewYoik
Spectrum
Luna, A K (1976) Cognitive development Its cul-tural and social
foundations Cambndge, MAHarvard Umversity Press
MacMahon, B, & Pug^, T F (1970) Eptdemiol-ogy Principles and
methods Boston Litde,Brown
Nichols, P L,&Chen,T C (1981) Minimalbratndysfunctton A
prospecttve study HiUsdale,NJ Erlbaum
Olweus, D (1979) Stability of aggressive reacbonpattems m males
A review PsychologtcalBullettn, 86, 852-875
Olweus, D (1980) Familial and temperamental de-terminants of
aggressive behavior in adoles-cent boys A causal analysis
DevelopmentalPsychology, 16, 644-660
Richman, N , Stevenson, J , & Graham, P J (1982)Pre-school
to school A behavioural studyLondon Academic Press
Robins, L (1966) Devtant children grown up Bal-timore Williams
& Wilkins
Rutter, M , & Brown, G W (1966) The reliabihtyand validity
of measures of family life and rela-bonships m &milies
containing a psvchiatncpabent Soctal Psychtatry, 1, 28-53
Rutter, M , & GiUer, H (1983) Juventle
deltquencyHammondsworth Penguin
Rutter, M , & Graham, P (1968) The reliability andvalidity
of the psychiatnc assessment of thechild I Interview with die child
Bnttsh Jour-nal of Psychtatry, 114, 563-579
Rutter, M , Graham, P, Chadwick, O, & Yule, W(1976)
Adolescent turmoil Fact or ficbon''Journal of Child Psychology and
Psychtatry,17,35-56
Rutter, M , Shafifer, D , & Sturge, C (1975) Multi-axtal
classtficatton scheme for psychtatrtc dts-orders tn chtldhood and
adolesence LondonInsbtute of Psychiatry
Rutter, M , Tizard, J , & Whibnore, K. (1970) Edu-catton,
health and behavtour London Long-man
Rutter, M , Tizaid, J , Yule, W, Graham, P, & Whit-more, K
(1976) Research report IsleofWi^tStudies, 1964-1974 Psychologtcal
Medtctne,6, 313-332
Schonfeld, I S (1986) The Genevan and Cattell-Hom concepbons of
intelligence comi>aredThe early lmplementabon of numencal
solu-bon aids Developmental Psychology, 22, 204-212
Shaffer, D , O'Connor, P A, Shafer, S Q , & Prupis,S (1983)
Neurological "soft signs" Theu- on-gin and significance for
behavior In M Rutter(Ed), Developmental neuropsychiatry (pp144-163)
New York Guilfoid
Shaffer, D , Sehonfeld, I , O'Connor, P A, Stok-man, C,
Traubnan, P, Shafer, S, & Ng, S(1985) Neurological soft signs
Their relabon-ship to psychiatnc disorder and intelligence
inchildhood and adolescence Archtves of Gen-eral Psychiatry, 42,
342-352
Sha£fer, D , StcJanan, C S , O'Connor, P Q, Shafer,S, Bamiack, J
E , Hess, S , Spalten, D , &Sehonfeld, I (1986) Early soft
neurologicalsigns and later psychopathology In L Erlen-meyer-Kunlmg
& N E Miller (Eds ), Ufe-span
-
Schonfeld et al. 1007research on the predictton of
psychopathology(pp 31-48) HiUsdale, NJ Erlbaum
Sharp, D , Cole, M , & Lave, C (1979) Educabonand cogmbve
development The evidencefirom expenmental research Monographs ofthe
Soctety for Research m Child Develop-ment, 46(1-2, Senal Nos 178,
179)
Spitzer, R L , & Endicott, J (1977) Scheduleof Affective
Dtsorders and Schizophrenia(SADS) (3d ed) New York Biometncs
Re-search Division, New York State PsychiatncInsbtute
Stokman, C J , Shafer, S Q, Shaffer, D , Ng, S ,O'Connor, P A ,
fit Wolff, R R (1986) Assess-
ment of "neurological soft signs in adoles-cents Reliability
studies DevelopmentalMedicine and Chtld Neurology, 28, 428-439
Susser, M (1973) Causal thinking tn the healthsctences New York
Oxford University Press
Wechsler, D (1955) Manual for the WechslerAdult Intelltgence
Scale New York Psycho-logical Corp
West, D J, & Famngton, D P (1973) Who be-comes deltnquent^
London Hememann
Vosk, B N , Forehand, R, & Figueroa, R (1983)Pereepbon of
emobons and rejected childrenJournal of Behavioral Assessment,
5,151-156