Embed Size (px)
Citation preview

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 1/21
www.medscape.com
Abstract and IntroductionAbstract
Parkinsonian diseases comprise a heterogeneous group of neurodegenerative disorders, which show significant clinical andpathological overlap. Accurate diagnosis still largely relies on clinical acumen; pathological diagnosis remains the goldstandard. There is an urgent need for biomarkers to diagnose parkinsonian disorders, particularly in the early stages whendiagnosis is most difficult. In this review, several of the most promising cerebrospinal fluid candidate markers will bediscussed. Their strengths and limitations will be considered together with future developments in the field.
Introduction
Idiopathic Parkinson's disease (iPD) is a progressive neurological disorder initially described as a clinical entity by JamesParkinson and then embellished by Charcot and other nineteenthcentury physicians, including Trousseau, Gowers and Erb.It is a clinical construct, based upon the presence of bradykinesia accompanied by at least one other characteristic feature,such as resting tremor, rigidity and impaired postural reflexes.[1] The signs and symptoms are usually asymmetrical at onsetand, typically, there is a good response to levodopa treatment.
'Parkinsonplus' or 'atypical parkinsonism' are terms that refer to a heterogeneous group of neurodegenerative disorders thatmay masquerade particularly in the early stages of the disease as Parkinson's disease (PD).[2] The 'plus' or 'atypical'descriptor indicates the presence of additional characteristics not usual in patients with iPD, such as early autonomicdisturbance and pyramidal signs exhibited by patients with multiple system atrophy (MSA), supranuclear gaze palsy andfrontal/dysexecutive syndrome by those with progressive supranuclear palsy (PSP), dystonia and myoclonus in corticobasaldegeneration (CBD) and early postural instability and falls by all of them. Another disease that could be classified as anatypical parkinsonian disorder is dementia with Lewy bodies (DLB), where dementia onset is before or within a year of onsetof extrapyramidal features. The earlier onset of dementia differentiates DLB from Parkinson's disease dementia (PDD).
Atypical parkinsonian disorders account for less than 10% of all parkinsonism and rarely respond with sustained improvementto levodopa. They usually follow a much more aggressive disease course than iPD and are characterised by atrophy toseveral different cortical and subcortical networks. Furthermore, atypical parkinsonism has been described in otherconditions, such as Alzheimer's disease (AD) and frontotemporal dementia (FTD).
Pathology
Protein misfolding and aggregation is seen with many neurodegenerative diseases. Based on pathological findings,parkinsonian syndromes are classified into αsynucleinopathies (PD, DLB and MSA) and primary tauopathies (PSP andCBD). For pathological lesions used in postmortem diagnosis of parkinsonism, see figure 1.
Cerebrospinal Fluid Biomarkers in ParkinsonianConditions: An Update and Future DirectionsNadia Magdalinou, Andrew J Lees, Henrik ZetterbergJ Neurol Neurosurg Psychiatry. 2014;85(10):10651075.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 2/21
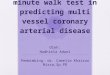
Figure 1.
In Parkinson's disease (PD), there is loss of pigmented neurons from the substantia nigra and remaining neurons may bevery sparse (A). Lewy bodies can be observed in residual neurons (A, inset) and are highlighted, together with Lewy neuritis,using αsynuclein immunohistochemistry (B). Lewy bodies and Lewy neurites may be present in significant numbers in theneocortex (C, frontal cortex). In multiple system atrophy (MSA), αsynuclein is primarily deposited in the form of glialcytoplasmic inclusions in oligodendrocytes (D, putamen) and may also form inclusions in neuronal cytoplasm and nuclei(arrow) (E, pontine nuclei). In progressive supranuclear palsy tau forms, aggregates in neurons and glia, giving rise to tufted

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 3/21
astrocytes (F, caudate) and neurofibrillary tangles (G, pontine nuclei). A characteristic feature of corticobasal degeneration(CBD) is the astrocytic plaque, formed from aggregated tau in the distal processes of astrocytes (H, parietal cortex). In CBD,tau also accumulates in neurons in the form of neurofibrillary tangles (H, inset a) and in oligodendrocytes as coiled bodies (H,inset b). (A) Haematoxylin and eosin; (B–D) αsynuclein immunohistochemistry; (F–H) tau immunohistochemistry. Bar in (A)represents 100 μm in (C); 50 μm in (A, D–G); 25 μm in inset A, B and H. Pathological images kindly provided by Dr JaniceHolton, Queen Square Brain Bank for Neurological Disorders, London.
αSynuclein (αSyn) has been found to be the major constituent of the intracellular aggregates in Lewy bodies and Lewyneurites (pathological hallmark of PD and DLB) and in the glial cytoplasmic inclusions in MSA.[3,4] The presence ofabnormally aggregated tau proteins in the form of neurofibrillary tangles, for example, are diagnostic of PSP.[5] Taupositiveintracellular inclusions are the neuropathological findings in CBD.[6] Even though there are also neurofibrillary tangles in AD,Aβ plaques are closely tied to the primary disease process and thus AD is considered to be a secondary tauopathy. FTD canalso have underlying tau pathology.
There is often some overlap between syncleinopathies and tauopathies (for a review, see ref. 7). Cooccurrence of tau and αSyn pathology has been found in neurons and oligodendrocytes in AD, PD and DLB.[8] αSyn has complex and dynamicinteractions with tau. Each of these two proteins has the tendency to seed the aggregation of the other.[9] αSyn inducesaggregation and polymerisation of tau, which promotes formation of intracellular amyloidtau inclusions.[10] Similarinteractions have been described between αSyn and Aβ pathology.[11]
Genetics
Recent advances in genetics have shed light on the underlying pathophysiology because mutations in the gene for eachmisfolded protein can give rise to an inherited form of a relevant neurodegenerative condition. For example, rare hereditaryforms of PD can be caused by mutations affecting the gene coding for αSyn (SNCA); PARK1 (missense) and PARK4(duplication, triplication).[12] Furthermore, in both PD and to a lesser extent in MSA, population studies demonstrated anassociation between disease risk and distinct singlenucleotide polymorphisms in SNCA. DJ1(PARK7) mutations can lead torare forms of autosomalrecessive PD, pointing towards mitochondrial damage/oxidative stress pathways drivenpathogenesis.[13] Even though PD is not a 'tauopathy', population studies also showed variants in tau (MAPT) gene,particularly the H1 haplotype, as another risk factor for PD (for a review, see ref. 14). Several tauopathies are associated withvariants in MAPT, including CBD, FTD linked to chromosome 17 (FTDP17T) and PSP.[15] The fact that the MAPT/tauhaplotype also shows an association with PD strongly suggests that the pathogenic cascades in the tauopathies may berelated to those in the synucleinopathies.[16]
Diagnostic Challenges
Accurate diagnosis of parkinsonian disorders still relies heavily on clinical acumen, although imaging and ancillaryinvestigations may be helpful in some situations. In one postmortem series, 24% of patients clinically diagnosed withidiopathic PD by a consultant neurologist during life were found to have an alternative diagnosis.[1]
Cerebrospinal Fluid Biomarkers
A biomarker is "a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,pathogenic processes or pharmacologic response to a therapeutic intervention".[17] An 'ideal' biomarker should be sensitive,reproducible, closely associated with the disease process, noninvasive and inexpensive.
Cerebrospinal fluid (CSF) has more physical contact with the brain than any other fluid and as such represents a potentiallyreliable biomarker source. Unlike plasma, CSF is not separated from the brain by the tightly regulated blood–brain barrier.Proteins/peptides that may be directly reflective of brain specific activities or disease pathology would most likely diffuse intothe CSF. Furthermore, CSF can be tested serially, which makes possible the study of protein changes reflecting the evolvingpathology throughout the clinical course of the disease. This is preferable to pathological studies, which only reveal theterminal changes of a disease process that has developed over decades.
Historical Background
CSF has been widely investigated in parkinsonian disorders and is considered to offer the most promising insights into thedisease process. Historically, because of dopaminergic abnormalities in parkinsonism, the first compounds to be tested aspotential markers were dopamine and other monoamines and their metabolites. In the 1960s and 1970s, reduced CSFmonoamine concentrations (homovanillic acid and 5hydroxyindoleacetic acid) were found in patients with parkinsonism and

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 4/21
dementia.[18] A study conducted at the National Hospital, Queen Square, London, assessed the effect of levodopa treatmentin CSF homovanillic acid concentration of PD patients. Before levodopa treatment, homovanillic acid concentration was low inall patients, while after treatment it rose to a level that correlated significantly with the levodopa dose.[19]
As these metabolic results were prone to be influenced by a multitude of other factors,[7] the quest went further to investigatea priori defined compounds, such as αSyn and tau. These were tested in patients and in healthy controls, looking fordifferences, patterns and associations. Even though several promising candidates exist, there is still no reliable biomarker.
Methods
We reviewed the potential use of CSF proteins as biomarkers in parkinsonism, focusing on αSyn, neuronal injury markersand Aβ42. In addition, we briefly reviewed the latest novel markers and the 'omics' approach. We performed aPubMed/Medline search and limited searches to studies reported in English and published after 2006, including antemortem,human, lumbar CSF; all studies included at least one parkinsonian cohort compared with healthy or neurological controls. Wecombined searches with 'Parkinson's disease', 'progressive supranuclear palsy', 'multiple system atrophy', 'corticobasalsyndrome' (CBS), 'corticobasal degeneration', 'Parkinson's disease dementia', 'dementia with Lewy bodies', 'Lewy bodydementia', 'parkinsonism', 'synucleinopathies', 'tauopathies', 'neurodegenerative diseases' with 'CSF biomarkers' and specificbiomarkers ('αSyn', 'tau', 'phosphorylated tau', 'Aβ42', 'neurofilaments', 'neuronal injury markers', 'inflammatory', 'metabolic'and 'oxidative stress markers'). Further references were found manually from identified publications. For a review of theearlier literature, not captured using the time limit of our search criteria, see Eller and Williams.[20]
CSF Biomarker Candidates in ParkinsonismAβ42
Aβ42 is a 42 aminoacid long, aggregationprone protein, derived from the proteolytic processing of amyloid precursor proteinand is a major component of neuritic plaques in AD. Cognitive impairment and dementia are much more common inparkinsonism than in the general population and have a detrimental effect on quality of life and life expectancy. The linkbetween Aβ42 and PD and dementia has been studied extensively (see ).
Table 1. CSF Aβ42 in parkinsonian disorders
Researchgroups
Participants Main findings
Kang et al 21 PD n=39 (drugnaïve patients), HC n=63 Decrease in PD vs HC
Compta et al 31Baseline: PD n=27 (nondemented)
18 month followup: PD n=16 (nondemented), PD n=11(dementia converters)
Decrease in dementia converters
Bech et al 32PD n=22, PDD n=3, DLB n=11, MSA n=10, PSP n=20, CBDn=3
Decrease in DLB vs other diseasegroups
Hall et al 26PD n=90, PDD n=33, DLB n=70, PSP n=45, CBD n=12, MSAn=48, AD n=48, controls n=107
Decrease in AD>DLB+PDD
Schoonenboomet al 33
DLB n=52, PSP n=20, CBD n=16, AD n=512, FTD n=144, VaDn=34, CJD n=6, controls n=275
Decrease in AD>VaD>DLB>CBD
Parnetti et al 27 PD n=38, DLB n=32, AD n=48, FTD n=31, controls n=32
Decrease in AD, FTD+DLBvs PD and controls
No difference between PDand controls
Andersson et al34 DLB n=47, PDD n=17, AD n=150 Decrease in DLB vs PDD
Shi et al 22
Discovery cohort: PD n=126, MSA n=32, AD n=50, controlsn=137 Slight decrease in PD and MSA vs

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 5/21
Validation cohort: PD n=83controls
Montine et al 28 PD n=41, PDD n=11, AD n=49, HC n=150 Decrease in PDD vs HC
Süssmuth et al29
PSPRS n=20, PSPP n=7, MSAP n=11, MSAC n=14, PDn=23, controls n=20
No difference inparkinsonian syndromes
Lower in PSPRS vs PSPP
Alves et al 23 PD n=109, AD n=20, HC n=36 Decrease in PD vs HC
Ohrfelt et al 30 PD n=15, DLB n=15, AD n=66, controls n=55Decrease in AD+DLB vs controlsand PD
Compta et al 24 PD n=20, PDD n=20, HC n=15 Decrease in PDD>PD vs HC
Parnetti et al 25 PD n=20, PDD n=8, DLB n=19, AD n=23, HC n=20 Decrease in DLB>PDD>PD
AD, Alzheimer's disease; CBD, corticobasal degeneration; CJD, Creutzfeldt–Jakob disease; CSF, cerebrospinal fluid; DLB,dementia with Lewy bodies; FTD, frontotemporal dementia; HC, healthy controls; MSA, multiple system atrophy; MSAC,multiple system atrophy cerebellar type; MSAP, multiple system atrophy parkinsonian type; PD, Parkinson's disease; PDD,Parkinson's disease dementia; PSP, progressive supranuclear palsy; PSPP, progressive supranuclear palsy–parkinsonism;PSPRS, progressive supranuclear palsy–Richardson's syndrome; VaD, vascular dementia.
In most studies, Aβ42 is significantly reduced in PD compared with controls and is associated with worse cognitiveperformance.[21–25] However, other investigations showed no difference between PD and controls.[26–30]
Compta et al [31] collected CSF from 27 nondemented PD patients and followed them over time. Patients who converted todementia within 18 months had a significantly lower baseline CSF Aβ42 than the patients who remained nondemented.
DLB patients have the lowest CSF levels of Aβ42 among the parkinsonian cohorts.[25,32–34] One study found that almost halfof DLB patients had a CSF biomarker profile consistent with AD,[33] which agrees with the knowledge of Aβ pathology in thisdisease.[35–37]
There is evidence that low Aβ42, a marker of Aβ plaque pathology, may predict cognitive decline in patients with PD,[38] butother longitudinal studies with larger cohorts are necessary to clarify this further.
αSyn
αSyn is a 140 aminoacid long protein that localises to presynaptic terminals and is widespread in the brain, comprising 1%of cytosolic protein. In presynaptic terminals, αSyn is present in close proximity to the synaptic vesicles. The precise functionof αSyn is obscure, but it is speculated that its main role is in the control of neurotransmitter release.[39] Although mostlyconsidered an intracellular protein, αSyn is capable of transfer between cells leading to a speculation of a prionlikemechanism operating in PD pathology spread.[40]
αSyn can be modified by truncation, acetylation, phosphorylation, oxidation, nitrosylation, glycation or glycosylation.[41] Lewybodies are formed mostly of posttranslationally modified αSyn. αSyn deposition is key in the pathogenesis ofsynucleinopathies. In vitro, similar to AD, αSyn fibrillation involves αSyn oligomerisation followed by oligomer conversioninto mature amyloid cultures, which are toxic to cultured neuronal cells.[42]
Total αSyn (tαSyn)
Inconsistent results were initially reported in parkinsonian conditions with studies demonstrating considerable overlap of tαSyn in several neurodegenerative conditions.[30,43–45] A consensus is now emerging, and the vast majority of recent studies(predominantly using ELISA techniques) have shown a reduction of tαSyn levels in PD compared with controls.[21,22,26,46–55] In addition, there is decreased tαSyn in other synucleinopathies, such as MSA and DLB,[26,47,49,50,51,54] without gooddiscriminatory value between the groups (see ).
Table 2. CSF αsynuclein in parkinsonian disorders
ResearchParticipants Analyte Method Main findings

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 6/21
groups
Van Dijk etal 46
PD n=53, HC n=50
tαSyn
tαSyn/tproteinratio
TRFRETDecrease in both tαSyn+tαSyn/tprotein ratio levels in PD vsHC
Kang et al201321
PD n=39 (drugnaïve patients),HC n=63
tαSyn ELISA Decrease in PD vs HC
Wennströmet al 47
PD n=38, PDD n=22, DLB n=33,AD n=46, HC n=52
tαSyn ELISADecrease in PDD > PD > DLB vsAD+HC
Mollenhaueret al 48
PD n=78 (de novo, drugnaïvepatients), HC n=48
tαSyn ELISA (3rd generation)Decrease in de novo PD patientsvs HC
Hall et al 26PD n=90, PDD n=33, DLB n=70,PSP n=45, CBD n=12, MSAn=48, AD n=48, controls n=107
tαSynBeadbased multianalyte assay(Luminex)
Modest decrease in AD >DLB+PDD > PD+MSA vscontrols, AD and PSP
Aerts et al43
PD n=58, MSA n=47, DLB n=3,VaD n=22, PSP n=10, CBD n=2
tαSyn ELISA No difference between groups
Tateno et al49
PD n=11, DLB n=6, MSA n=11,AD n=9, controls n=11
tαSyn ELISA
Decrease in PD, DLB,MSA vs AD+ controls
No difference among PD,DLB, MSA
Wang et al50
Discovery cohort:
PD n=83, MSA n=14, PSD n=30,AD n=25, HC n=51
Validation cohort:
PD n=109, MSA n=20, PSPn=22, AD n=50, HC n=71
tαSyn
pαSyn
pαSyn:tαSynratio
Beadbased multianalyte assay(Luminex)
tαSyn decrease inPD+MSA vs controls
Increase αSyn ratio inMSA vs PSP
Increase αSyn ratio in PDvs controls and PSP
Park et al 58PD (drugnaïve) n=23, controlsn=18
tαSyn
oαSyn
Dual ELISA method forsimultaneousmeasurement of tandoαSyn
tαSyn: no difference
oαSyn: increase in PD
Mollenhaueret al 54
Training cohort: PD n=51, DLBn=55, MSA n=29, AD n=62,controls n=76
Validation cohort: PD n=273,DLB n=66, PSP n=8, MSA n=15,NPH n=22, controls n=23
tαSynELISA (1st and 2ndgeneration)
Decrease in PD, DLB,MSA vs AD, NPH, PSPand controls
High degree ofconcordance in tαSynlevels between PD+MSA
Parnetti etal 27
PD n=38, DLB n=32, AD n=48,FTD n=31, controls n=32
tαSyn
tαSyn/ttau
ELISA
tαSyn decrease in alldiseased groups(especially DLB/FTD)
Ratio: decrease in PD vsall other diseased groups

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 7/21
ratio
Shi et al 22
Discovery cohort: PD n=126,MSA n=32
AD n=50, controls n=137
Validation cohort :PD n=83
tαSynBeadbased multianalyte assay(Luminex)
Decrease in PD vs controls andAD
Tokuda et al57
First cohort (all analytes):
PD n=32, controls n=28
Second cohort (oasyn):
PD n=25, AD n=35, PSP n=18,controls n=43
tαSyn
oαSyn
oαSyn:tαSynratio
ELISA
tαSyn: trend towardsdecrease in PD
oαSyn+ratio increase inPD
Hong et al52 PD n=117, AD n=50, HC n=132 tαSyn
Beadbased multianalyte assay(Luminex)
Decrease in PD vs AD andcontrols (after omitting sampleswith high haemoglobinconcentration)
NoguchiShinoharaet al 44
DLB n=16, AD n=21 tαSyn ELISA No difference
Spies et al45
DLB n=40, AD n=131, VaDn=28, FTD n=39
tαSyn ELISA No difference
Ohrfelt et al30
PD n=15, DLB n=15, AD n=66,controls n=55
tαSyn ELISADecrease in AD, no difference inparkinsonian groups
Mollenhaueret al 53
PD n=8, DLB n=38, AD n=13,CJD n=8, controls n=13
tαSynELISA (1st and 2ndgeneration)
Marginal decrease in LBD andPD vs all other groups
Tokuda et al55 PD n=38, controls n=38 tαSyn ELISA Decrease in PD vs controls
AD, Alzheimer's disease; CBD, corticobasal degeneration; CJD, Creutzfeldt–Jakob disease; CSF, cerebrospinal fluid; DLB,dementia with Lewy bodies; FTD, frontotemporal dementia; HC, healthy controls; MSA, multiple system atrophy; NPH, normalpressure hydrocephalus; PD, Parkinson's disease; PDD, Parkinson's disease dementia; PSP, progressive supranuclearpalsy; TRFRET, timeresolved Förster's resonance energy transfer; VaD, vascular dementia.
Mollenhauer et al assessed levels of tαSyn in patients with synucleinopathies, patients with tauopathies and in neurologicalcontrols without neurodegenerative disease, first in a training set and then in a validation set. In the training set, acombination of tαSyn, ttau and age differentiated synucleinopathies from neurological controls and AD with an area underthe curve (AUC) of 0.908. Only tαSyn levels and not ttau or Aβ42 discriminated PD and MSA from controls with a positivepredictive value of 91%.[54]
Parnetti et al investigated whether the combination of ttau, ptau and tαSyn can improve differentiation of PD from DLB,AD, FTD and controls. They found an inverse correlation between tαSyn and total tau in all subjects and a lack of specificityof CSF tαSyn determination alone as a marker of synucleinopathy (sensitivity 94%, specificity 25%). However, ttau/tαSynand ptau/tαSyn ratios were identified as possible biomarkers for PD (sensitivity 89%, specificity 61%).[27]
Shi et al [22] also showed that a combination of tαSyn and ptau/ttau could discriminate PD from MSA with a sensitivity of90% and a specificity of 71%, when blood contaminated samples were excluded. tαSyn was decreased in PD andespecially in MSA compared with controls.
In most studies, there was no correlation of tαSyn with disease duration or disease severity. Interestingly, genderspecificvariations were reported in levels of tαSyn.[47] Both Mollenhauer et al [48] and Kang et al [21] studied drugnaïve PD patientsand still found reduction in tαSyn, so it was proven that this finding was not related to a dopaminergic medication effect.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 8/21
There are several theories why there is reduced tαSyn in PD, MSA and DLB. High brain levels of pathological tαSyn andlow CSF levels may reflect a reduction of 'free' tαSyn circulating in the CSF. This could be similar to 'pathological proteintrapping' reported for brain Aβ42 in AD CSF.[56]
Oligomeric and Phosphorylated αSyn
Tokuda et al evaluated soluble αSyn oligomers as potential early markers of PD and found that both the level of oligomericαSyn and the oligomer/tαSyn ratio were substantially higher in patients with PD (including those with mild and earlystagedisease) compared with healthy controls and patients with nonneurodegenerative neurological conditions. CSF oligomer/tαSyn ratio had a sensitivity of 89.3% and a specificity of 90.6% for PD.[57] These findings were replicated in two further,independent studies.[58,59] Both oligomeric and phosphorylated oligomeric forms of αSyn were detected in postmortemventricular CSF, which may be useful in distinguishing between PD, DLB and MSA.[60] The results need to be replicated inlarger groups of living patients.
Neuronal Injury MarkersTau
Tau is important for the function of axonal microtubules and, as a result, plays an important role in the structural integrity ofthe neuron and axonal support. When hyperphosphorylated, it has reduced binding affinity for microtubules, causing theirmalfunction. At the same time, it adopts an abnormal conformation leading to aggregation and inclusion formation.[61]
Total and Phosphorylated Tau (ttau and ptau)
In the past, there were inconclusive results when assessing tau levels in CSF of parkinsonian patients (see ). In PD, moststudies found normal values,[23,24,25,26,27,29,30] but lower levels were also reported.[21,22,28] In atypical parkinsonism, high ttau levels were found in DLB[25,27,34] and low ptau/ttau ratio in MSA and PSP compared with PD.[29] However, otherinvestigations found no difference between parkinsonian syndromes.[22,26,30] In particular, no significant change has beenseen in PSP.[26] Age, not diagnosis, is thought to be the strongest factor affecting ttau protein levels.[54]
Table 3. CSF neuronal injury markers: tau, neurofilament light chain (NFL) and glial fibrillary acidic protein (GFAP) inparkinsonian disorders
Researchgroups
Participants Analyte Method Main findings
Kang et al 21PD n=39 (drugnaïve patients), HCn=63
ttau, ptau
Beadbased multianalyte assay(Luminex)
Decrease in ttau+ptau in PDvs controls
Luk et al 64PDD n=11, PSP n=44, CBS n=22,AD n=11, controls n=34
3R/4Risoforms
ImmunoPCR(adapted fromsandwich ELISAs)
Decrease in 4Rtau inPSP and AD vs controls
Lower 4Rtau in AD vsPDD
No difference in 3Rtau
Hall et al201226
PD n=90, PDD n=33, DLB n=70,PSP n=45, CBD n=12, MSA n=48,AD n=48, controls n=107
ttau, ptau
NFL
Beadbased multianalyte assay(Luminex)
Increased tand ptau inAD vs DLB+PDD
NFL differentiates PDfrom atypicalparkinsonism
Bech et al 32PD n=22, PDD n=3, DLB n=11,MSA n=10, PSP n=20, CBD n=3
NFL ELISA
Higher NFL levels inatypical parkinsoniandisorders vs PD

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 9/21
No difference betweenparkinsonian groups
Andersson etal 34
DLB n=47, PDD n=17, AD n=150ttau, ptau
ELISA Increased ttau in DLB vs PDD
Shi et al 22Discovery cohort: PD n=126, MSAn=32, AD n=50, controls n=137
Validation cohort: PD n=83
ttau, ptau
Beadbased multianalyte assay(Luminex)
Decrease in PD vs tocontrols
Decrease in PD+MSAvs AD
Parnetti et al201127
PD n=38, DLB n=32, AD n=48,FTD n=31, controls n=32
ttau, ptau
ELISA
Increase inAD>FTD>DLB vs PDand controls
No difference betweenPD and controls
Kuiperij et al102 NA
33/55
kDa tauforms
Immunoprecipitationassay and westernblotting
Not able to detect tauform ratio
Suggested that 33/55kDa bands seen areheavy and light IgGchains
Borroni et al103
PSP n=18, CBS n=16, FTD n=28,controls n=25
33/55
kDa tauforms
Immunoprecipitationassay and westernblotting
tau form ratio significantlyreduced in PSP vs othergroups
Constantinescuet al 71
PD n=10, MSA n=21, PSP n=14,CBD n=11, HC n=59
(×2 consecutive samples)
NFL
GFAPELISA
NFL: normal levels inPD, elevated in MSA,PSP+CBD
No statisticalsignificance overtime
GFAP: no difference
Montine et al28
PD n=41, PDD n=11, AD n=49,HC n=150
ttau, ptau
Beadbased multianalyte assay(Luminex)
ttau: no differencebetween parkinsoniangroups
ptau: reduced in PD vsHC
Süssmuth et al29
PSPRS n=20, PSPP n=7, MSAP n=11, MSAC n=14, PD n=23,controls n=20
ttau, ptau
GFAP
ELISA
ptau/ttau ratio lower inPSP and MSA vs PD
GFAP: increase inparkinsonian syndromes

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 10/21
(no difference betweendisease groups)
Alves et al 23 PD n=109, AD n=20, HC n=36ttau, ptau
ELISANo difference between PD andcontrols
Ohrfelt et al 30PD n=15, DLB n=15, AD n=66,controls n=55
ttau, ptau
ELISANo difference betweenparkinsonian groups
Compta et al 24 PD n=20, PDD n=20, HC n=15ttau, ptau
ELISAt and p tau: increase in PDDvs PD and controls
Parnetti et al 25PD n=20, PDD n=8, DLB n=19,AD n=23, HC n=20
ttau, ptau
ELISA
ttau: DLB > PDD >controls
ptau: no differencebetween parkinsoniangroups
Borroni et al 65PSP n=21, CBS n=20, FTD n=44,AD n=15, PD n=10, DLB n=15,controls n=27
33/55
kDa tauforms
Semiquantitativeimmunoprecipitationand western blotting
tau forms significantly reducedin PSP vs controls and otherneurodegenerative diseases
Brettschneideret al 70
PD n=22, MSA n=21, PSP n=21,CBD n=6, controls n=45
NFH ELISAIncreased in MSA and PSP vsPD, CBD and controls
AD, Alzheimer's disease; CBD, corticobasal degeneration; CBS, corticobasal syndrome; CSF, cerebrospinal fluid; DLB,dementia with Lewy bodies; FTD, frontotemporal dementia; HC, healthy controls; MSA, multiple system atrophy; MSAC,multiple system atrophy cerebellar type; MSAP, multiple system atrophy parkinsonian type; NF_H, neurofilament heavychain; NFL, neurofilament light chain; PD, Parkinson's disease; PDD, Parkinson's disease dementia; PSP, progressivesupranuclear palsy; PSPP, progressive supranuclear palsy–parkinsonism; PSPRS, progressive supranuclear palsy–Richardson's syndrome.
ttau and ptau may prove useful in differentiating AD from PD and can perhaps improve diagnostic accuracy when used incombination with other markers rather than on their own.
Tau Isoforms
Imbalances in the homeostasis of tau isoforms with three (3Rtau) and four (4Rtau) microtubulebinding repeat domainsare important in neurodegenerative disease pathogenesis. In a normal adult brain, there are comparable levels of 3R and4R[62] but in PSP, CBD and FTDP17 cases, the neurofibrillary tangles and glial inclusions are predominantly 4R, whereasPick bodies in FTD are predominantly 3Rtau[63] and neurofibrillary tangles in AD contain both 3R and 4Rtau isoforms.
Luk and colleagues had previously developed antibodies selective for the two isoforms and adapted an immunoPCRprocedure in order to detect the isoforms' miniscule amounts in the CSF. Decrease in 4Rtau isoform was found in PSP andAD compared with CBS, PDD and controls. There was no difference in 3Rtau.[64]
We think that 4Rtau could be used as a marker of disease progression in PSP, but further large samples and longitudinalseries are needed.
Truncated Tau Forms
Borroni and colleagues looked at fulllength (55 kDa) and truncated (33 kDa) tau forms in several neurodegenerativediseases. In ratio with the fulllength tau forms, the truncated tau forms (33 kDa/55 kDa forms) were substantially reduced inPSP compared with healthy controls (sensitivity 96% and specificity 85% PSP compared with PD/DLB; sensitivity 90% andspecificity 76.2% PSP compared with CBD).[65] These fragments are proteolytic products of tau that were detected byimmunoprecipitation techniques, which are more time consuming, less quantitative and more operatordependent than ELISAtechniques.
Findings were reproduced by the same group in another cohort of patients.[66] However, these results were not reproduced

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 11/21
by another group, which did not find a reduced tau ratio in an independent cohort of PSP patients,[67] speculating that the33/55 kDa bands seen are heavy and light IgG chains. Recent findings of other endogenous tau fragments in CSF suggestthat specific assays for these fragments should be developed and evaluated in relation to different tauopathies.[68]
Neurofilament Light Chain Protein (NFL)
Neurofilaments are major structural elements, whose main role is to maintain the axonal calibre and neuronal shape and size.[69] They are, thus, critical for the morphological integrity of neurons and for the conduction of nerve impulses along axons.They are composed of three subunits of different molecular weights: light, medium and heavy chain.
Neurofilament heavy chain (NFH) forms an important component of the cytoskeleton. Higher CSF levels of NFH were foundin PSP and MSA compared with PD, CBD and neurological controls.[70]
Neurofilament light chain forms the backbone of neurofilaments and can selfassemble. Increased levels in CSF reflectaxonal degeneration of large myelinated axons. Recent studies showed consistent results in differentiating PD from atypicalparkinsonian conditions[26,32,71] but not in discriminating between atypical parkinsonian syndromes. Consecutive analyses ofCSF showed no increase in NFL levels with disease progression.[71]
NFL can be useful in the differential diagnosis of PD versus other neurodegenerative conditions as it is very sensitive indetecting more aggressive neuronal death than occurs in PD.
Glial Fibrillary Acidic Protein
Glial fibrillary acidic protein (GFAP) is a protein predominantly expressed in fibrillary astrocytes. Disintegration of astroglialcells postacute brain injury can lead to high CSF GFAP levels. Süssmuth et al [29] showed that there are increased levels inparkinsonian syndromes compared with controls (patients with other neurological disorders), but there was no differencebetween diseased groups. However, another group found similar GFAP levels in parkinsonian syndromes and healthycontrols without significant change over time.[71]
Other Candidate MarkersOxidative Stress Markers
DJ1. DJ1 is a multifunctional protein involved in many processes. It is thought to have a protective role in oxidative stressduring neurodegeneration (). As we have already discussed, it has been linked to autosomalrecessive PD. Results on DJ1as a CSF biomarker have been inconsistent so far. One study showed decreased levels in PD compared with controls with asensitivity of 90% and a specificity of 70%,[52] whereas another showed no difference among parkinsonian syndromes[72] andthe most recent one demonstrated significant increase in MSA compared with PD and controls.[73] The diagnostic accuracyfor discriminating MSA from PD was improved by combining DJ1 levels with ttau and ptau levels.
Table 4. CSF biomarkers for oxidative stress, inflammation and energy failure in parkinsonian disorders
Researchgroups
Participants Analyte Method Main findings
Herbert et al 73PD n=43, MSA n=23,controls n=30
DJ1 ELISA
Increase inMSA>PD
Significantdifference in MSAvs PD, MSA vscontrols and PDvs controls
Constantinescuet al 78
PD n=6, MSA n=13, PSPn=18, CBD n=6, HC n=18
UrateEnzymatic method on amodular system
No difference
Lowest levels inDLB, but nodifference

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 12/21
Wennstrom etal 47
PD n=38, PDD n=22, DLBn=33, AD n=46, HC n=52
Neurosin ELISAbetweensynucleinopathies
When pooled,synucleinopathiesdecrease levelsvs AD+HC
Goldstein et al82
PD n=34, MSA n=54, PAFn=20, HC n=38
Dihydroxyphenylaticacid (DOPAC)
Batch aluminaextraction followed byliquid chromatographywith electrochemicaldetection
Decrease in PD,MSA and to alesser degreePAF vs HC
No differencebetweensynucleinopathygroups
Salvesen et al72
PD n=30, DLB n=17, MSAn=14, PSP n=19
DJ1 ELISANo difference amonggroups
Maetzler et al77
PD n=55, PDD n=20, DLBn=20, controls n=76
Uric acidADVIAanalyser+photometricmethods
Increase in PD vs DLB
Shi et al 22Discovery cohort: PDn=126, MSA n=32 ADn=50, controls n=137Validation cohort: PD n=83
DJ1 FractalkineBeadbased multianalyte assay(Luminex)
DJ1: decrease inMSA+PD vscontrols+AD
Fractalkine:decrease in MSAvs PD,AD+controls
LeWitt et al 81PD n=217 (samplescollected ×2 occasions)HC n=26
Homovallinicacid/xanthine ratio
Gas chromatographymass spectrometry
Increased ratio inPD vs HC
Ratio increasedfurther in PDspecimenscollected up to 2years later
Wang et al 79PD n=86, MSA n=20, ADn=38 HC n=91
ComplementC3/factor H (FH)
Beadbased multianalyte assay(Luminex)
C3: decrease inMSA vs PD+HC;increase in AD vsall other groups
FH: increase inAD vs PD+HC
C3/FH ratio:decrease in MSAvs all othergroups

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 13/21
Maetzler et al80
PD n=38, PDD n=20, DLBn=21 m, controls n=23
Neprilysin Fluorometric assayDecrease in DLB+PDDvs PD+ controls
Hong et al 52PD n=117, AD n=50, HCn=132
DJ1Beadbased multianalyte assay(Luminex)
Decreased levelsin PD vs Controlsand AD
No differencebetween AD+controls
AD, Alzheimer's disease; CBD, corticobasal degeneration; CSF, cerebrospinal fluid; DLB, dementia with Lewy bodies; HC,healthy controls; MSA, multiple system atrophy; PAF, pure autonomic failure; PD, Parkinson's disease; PDD, Parkinson'sdisease dementia; PSP, progressive supranuclear palsy.
8Hydroxydeoxyguanosine (8OHdG). 8OHdG is a marker of oxidation and mitochondrial dysfunction inneurodegeneration and malignancy. CSF 8OHdG levels were increased in nondemented PD patients compared withcontrols and there was a negative correlation with MMSE levels in PDD.[74]
Urate. Urate is an endogenous and most potent antioxidant. Even though there is considerable evidence linking low serumlevels of urate to PD,[75,76] CSF studies have shown inconsistent results. Maetzler et al [77] found increase levels in PDcompared with DLB, but Constantinescu et al [78] showed no difference among parkinsonian groups and healthy controls.
Inflammatory Markers
Fractalkine. Fractalkine is an inflammatory cytokine that acts as a neurotrophic and antiapoptotic factor in the centralnervous system. It was decreased in MSA and could alone differentiate between PD and MSA with a sensitivity of 99% and aspecificity of 95%.[22] In addition, the fractalkine/Aβ42 ratio was closely associated with disease severity and progression inPD. These results are in need of replication.
Complement C3/Factor H Ratio. The C3/factor H ratio in CSF was significantly decreased in MSA compared with PD, ADand healthy controls. Increased levels of C3 or factor H, together with decreased levels of Aβ42, correlate positively withdisease severity and progression in PD.[79]
Neurosin. Neurosin is a protein expressed in human brain tissue, and it is one of several enzymes suggested to cleave αSyn. A study comparing neurosin levels in synucleinopathies showed lowest levels in DLB, but no difference among DLB,PDD and PD. However, when pooled together, synucleinopathies had significantly lower neurosin levels compared with ADand controls.[47]
Neprilysin. Neprilysin is a membrane bound presynaptic protein involved in Aβ clearance. CSF levels were significantlydecreased in DLB and PDD compared with PD and controls, and they correlated well with Aβ42 levels in all cohorts.[80]
Catecholamine Metabolites
Homovanillic Acid (HVA)/Xanthine Ratio. HVA is the major catabolite of dopamine and has been extensively studied in thepast in relation to PD, as described above. Xanthine is the immediate precursor of urate. HVA/xanthine ratio was increased inPD compared with controls and correlated with diseased severity.[81]
Dihydroxyphenylatic aCid (DOPAC). Depletion of dopamine (a catecholamine) in basal ganglia is a defining neurochemicalcharacteristic in PD. DOPAC is a neuronal metabolite of catecholamines. It was found to be decreased in PD and MSAcompared with healthy controls, but there was no difference between synucleinopathy groups.[82]
The above compounds may be promising candidate makers, but they need verification in further studies. CSF HVA has beenextensively studied in relation to PD and treatment response but still has no definite place in the clinical routine.
Lysosomal Dysfunction
Lysosomes are the cell's waste disposal system, and their dysfunction is an early event in PD pathogenesis.[83] Patientssuffering from Gaucher disease, a rare, autosomalrecessive storage disorder caused by lysosomal enzyme βglucocerebrosidase (GCase) deficiency,[84] have an increased risk of parkinsonism,[85] which appears to be driven by a direct

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 14/21
effect of GCase deficiency and lysosomal dysfunction on αSyn aggregation.[86]
Measuring GCase activity in the CSF could be a useful biomarker in PD. PD[87] and DLB[88] patients were found to havesignificantly reduced GCase activity compared with neurological controls. A recent study showed that the combination ofGCase activity, oligomeric/total αSyn ratio and age discriminates best PD from neurological controls.[89] However, in a Dutchcohort of de novo PD patients and healthy controls, there was a trend towards a reduction in CSF GCase activity.[90] Theusefulness of GCase as a potential biomarker in parkinsonian conditions needs to be evaluated in future studies that includeadditional neurodegenerative groups to PD.
'Omics' Approaches. The markers already discussed have been hypothesis driven based on pathophysiological studies,which have identified potentially deranged pathways in neurodegenerative diseases. The 'omics' techniques offer anunbiased approach of identifying biochemical pathways that are unexpectedly involved in neurodegeneration. Ultimately, theaim is to generate a list of candidate markers deserving further targeted studies.[91] The 'omics' approach results in unbiasedand systematic measurement of patterns of variations in genes (genomics), RNA (transcriptomics), proteins (proteomics) andsmall molecules (metabolomics). We have briefly discussed genomics and touched on metabolomics in previous sections,and we will now review proteomics in parkinsonian disorders.
Abdi et al [92] used a multiplex quantitative proteomic platform to find 72 altered proteins in PD compared with healthycontrols. Apolipoprotein H and ceruplasmin seemed to differentiate PD from healthy controls and from nonPD patients (ADand DLB). Eight of the proposed proteins were validated using a multianalyte CSF profile and showed good PD discriminatorypower compared with AD and healthy controls.[93]
Using surfaceenhanced laser desorption/ionisation timeofflight mass spectrometry (SELDITOF MS), Constantinescu et al[94] found a CSF proteomic profile consisting of four proteins (ubiquitin, β2microglobulin and two secretographin 1fragments), which differentiated PD and healthy controls from atypical parkinsonian patients with an AUC of 0.8. Recently,Ishigami et al [95] were able to differentiate PD from MSA, even at the early stages, using their proteomic pattern (ie, thecombined set of many protein peaks), rather than a single peak. Multiple peaks differentiated MSA and PD from controlgroups, consistent with previous reports that a panel of potential biomarkers is essential to distinguish between diseasestates.[96]
Another recent study attempted to differentiate PD from PDD patients using proteomic technology. Six proteins wereidentified, but only serinprotease inhibitor Serpin A1 was verified using biochemical methods. Performing 2D immunoblots,there was 100% specificity and 58% sensitivity for the test procedure.[97] Testing CSF obtained from PD, PDD patients andnondemented controls using a gelfree proteomics mass spectrometry approach with isotopelabelled samples (iTRAQ) ledto the identification of 16 differentially regulated proteins, which could be potentially diagnostic markers.[98]
While proteomics studies have produced a number of interesting candidate markers, these are still in need of replication andfar from being established. It has also become clear that many of the protein expression changes seen so far representchanges that are common to several neurodegenerative diseases. Reliable detection of diseasespecific changes most likelydepends on the development of more advanced techniques that allow for deeper analyses of the CSF proteome.
Imaging Markers. Even though imaging biomarkers are beyond the scope of this review, we would like to point out thatcombination of CSF and imaging markers can provide increased diagnostic accuracy compared with using either modalityalone. For example, Borroni and colleagues used midsagittal midbraintopons atrophy in addition to CSF tau fragmentslevels to increase the discriminative power in identifying PSP from other neurodegenerative conditions.[66]
Discussion
The vast majority of the studies discussed are crosssectional, retrospective and do not have pathological confirmation. Theaccuracy of the clinical diagnosis is uncertain, and the contribution of comorbidity to the clinical phenotype is unknown.
There is lack of standardisation both of preanalytical (sampling collection, handling and storage) and analytical (analysisexecution/sample processing) factors. For example, CSF contamination by blood can alter study outcomes in αSyn and DJ1assays. In addition, there is lack of assay standardisation; different assays can give different absolute concentrations of theprotein, making it almost impossible to use global reference limits and diagnostic cutoff points.
Furthermore, both disease groups and control groups are heterogeneous. The neurodegenerative groups differ in terms ofage, disease duration and severity. The control groups include a very small proportion of healthy controls and are mostly nonneurodegenerative neurological patients. However, some studies include patients with possible neurodegenerativeconditions, such as mild cognitive impairment or normal pressure hydrocephalus.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 15/21
Finally, there is lack of combination of different biomarker modalities, such as imaging and CSF markers.
A very promising study is the Parkinson's Progression Markers Initiative (PPMI), which aims to identify PD progressionmarkers and to better define subsets of PD patients.[99,100] It is a 5year, multicentre, longitudinal study of drugnaïve PDpatients with earlystage disease, compared with healthy controls. Detailed motor and neuropsychological assessments,DaTscan and CSF examinations are performed. There is strict standardisation of data acquisition, CSF collection andprocessing.[21]
Summary Points: CSF Biomarkers in Parkinsonism
Aβ42 has a role in predicting cognitive decline in Parkinson's disease (PD)
tαSyn: most promising marker; differentiates synucleinopathies from other neurodegenerative diseases and controlsbut is not specific
ttau and ptau: inconsistent data, can help differentiate PD from AD and can be useful in combination with othermarkers
NFL: useful in differentiating PD from atypical parkinsonian conditions
4Rtau: possible marker of disease progression in PSP
DJ1: potential role in discriminating MSA from PD
Oxidative stress/inflammatory/metabolic markers: promising initial results, requiring further validation
Future Developments for the CSF Field in Parkinsonism
We think that several hypothesisdriven biomarkers are going to be investigated at the same time using multiplex platforms.The proteomics field is likely to expand and gain in analytical sensitivity, resulting in the identification of more candidatemarkers, some of which may be unexpected and give new clues on disease mechanisms. There needs to be large,prospective and longitudinal cohorts with serial CSF examinations and pathological confirmation in as many patients aspossible. A very important issue to be resolved is the standardisation of protocols and improvement in quality controls in CSFanalysis. Finally, like in AD, it will likely be important to combine several CSF markers with other modalities, like imaging.
Accurate diagnosis of parkinsonian conditions should occur as early as possible, before too much irreversible neuronaldamage has accumulated. This is essential, especially with the emergence of potential diseasemodifying drugs, which mustbe used to target the correct underlying pathology. There is promising progress in the development of an αSyn imagingagent, using radio ligands that bind to αSyn fibrils. This should enable the assessment of the distribution of brain αSynduring life.[101]
Conclusion
Parkinsonian conditions, like most neurodegenerative diseases, have complex and dynamic interaction of several underlyingpathogenic mechanisms. A combination of biomarkers possibly from different modalities in large, longitudinal cohorts mightbe required for early diagnosis and accurate disease prognosis.
References
1. Hughes AJ, Daniel SE, Kilford L, et al. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinicopathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55:181–4.
2. Fahn S. Secondary Parkinsonism. Sci Approaches Clin Neurol 1977:1159–89.
3. Spillantini MG, Schmidt ML, Lee VMY, et al. Alphasynuclein in Lewy bodies. Nature 1997;388:839–40.
4. Gai WP, Power JHT, Blumbergs PC, et al. Multiplesystem atrophy: a new alphasynuclein disease? Lancet1998;352:547–8.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 16/21
5. Litvan I, Hauw J, Bartko JJ, et al. Validity and reliability of the preliminary NINDS neuropathologic criteria forprogressive supranuclear palsy and related disorders. J Neuropathol Exp Neurol 1996;55:97–105.
6. Schneider JA, Watts RL, Gearing M, et al. Corticobasal degeneration: neuropathologic and clinical heterogeneity.Neurology 1997;48:959–69.
7. Constantinescu R. Cerebrospinal fluid biomarker candidates for Parkinsonian disorders. Front Neurol 2013;3:1–15.
8. Vekrellis K, Xilouri M, Emmanouilidou E, et al. Pathological roles of alphasynuclein in neurological disorders. LancetNeurol 2011;10:1015–25.
9. Giasson BI, Duda JE, Quinn SM, et al. Neuronal alphasynucleinopathy with severe movement disorder in miceexpressing A53T human alphasynuclein. Neuron 2002;34:521–33.
10. Waxman EA, Giasson BI. Induction of intracellular tau aggregation is promoted by alphasynuclein seeds and providesnovel insights into the hyperphosphorylation of tau. J Neurosci 2011;31:7604–18.
11. Tsigelny IF, Crews L, Desplats P, et al. Mechanisms of hybrid oligomer formation in the pathogenesis of combinedAlzheimer's and Parkinson's diseases. PLoS One 2008;3:e3135.
12. Polymeropoulos MH, Lavedan C, Leroy E, et al. Mutation in the alphasynuclein gene identified in families withParkinson's disease. Science 1997;276:2045–7.
13. Cookson MR. DJ1, PINK1, and their effects on mitochondrial pathways. Mov Disord 2010;25(Suppl 1):S44–8.
14. Hardy J, Lewis P, Revesz T, et al. The genetics of Parkinson's syndromes: a critical review. Curr Opin Genet Dev2009;19:254–65.
15. Vandrovcova J, Anaya F, Kay V, et al. Disentangling the role of the tau gene locus in sporadic tauopathies. CurrAlzheimer Res 2010;7:726–34.
16. Hardy J. Genetic analysis of pathways to Parkinson's disease. Neuron 2010;68:201–6.
17. Biomarkers Definitions Working, G. Biomarkers and surrogate endpoints: preferred definitions and conceptualframework. Clin Pharmacol Ther 2001;69:89–95.
18. Gottfries CG, Gottfries I, Roos BE. Homovanillic acid and 5hydroxyindoleacetic acid in the cerebrospinal fluid ofpatients with senile dementia, presenile dementia and parkinsonism. J Neurochem 1969;16:1341–5.
19. Curzon G, GodwinAusten RB, Tomlinson EB, et al. The cerebrospinal fluid homovanillic acid concentration in patientswith Parkinsonism treated with Ldopa. J Neurol Neurosurg Psychiatry 1970;33:1–6.
20. Eller M, Williams DR. Biological fluid biomarkers in neurodegenerative parkinsonism. Nat Rev Neurol 2009;5:561–70.
21. Kang JH, Irwin DJ, ChenPlotkin AS, et al. Association of cerebrospinal fluid βAmyloid 1–42, Ttau, Ptau 181, and αsynuclein levels with clinical features of drugnaive patients with early Parkinson's disease. JAMA Neurol2013;10:1277–87.
22. Shi M, Bradner J, Hancock AM, et al. Cerebrospinal fluid biomarkers for Parkinson's disease diagnosis andprogression. Ann Neurol 2011;69:570–80.
23. Alves G, Bronnick K, Aarsland D, et al. CSF amyloidβ and tau proteins, and cognitive performance, in early anduntreated Parkinson's Disease: the Norwegian ParkWest study. J Neurol Neurosurg Psychiatry 2010;81:1080–6.
24. Compta Y, Martí MJ, IbarretxeBilbao N, et al. Cerebrospinal tau, phosphotau, and betaamyloid andneuropsychological functions in Parkinson's disease. Mov Disord 2009;24:2203–10.
25. Parnetti L, Tiraboschi P, Lanari A, et al. Cerebrospinal fluid biomarkers in Parkinson's disease with dementia anddementia with Lewy bodies. Biol Psychiatry 2008;64:850–5.
26. Hall S, Öhrfelt A, Constantinescu R, et al. Accuracy of a panel of 5 cerebrospinal fluid biomarkers in the differentialdiagnosis of patients with dementia and/or Parkinsonian disorders. Arch Neurol 2012;69:1445.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 17/21
27. Parnetti L, Chiasserini D, Bellomo G, et al. Cerebrospinal fluid Tau/αsynuclein ratio in Parkinson's disease anddegenerative dementias. Mov Disord 2011;26:1428–35.
28. Montine TJ, Shi M, Quinn JF, et al. CSF Abeta(42) and tau in Parkinson's disease with cognitive impairment. MovDisord 2010;25:2682–5.
29. Sussmuth SD, Uttner I, Landwehrmeyer B, et al. Differential pattern of brainspecific CSF proteins tau and amyloidbeta in Parkinsonian syndromes. Mov Disord 2010;25:1284–8.
30. Ohrfelt A, Grognet P, Andreasen N, et al. Cerebrospinal fluid alphasynuclein in neurodegenerative disordersa markerof synapse loss? Neurosci Lett 2009;450:332–5.
31. Compta Y, Pereira JB, Ríos J, et al. Combined dementiarisk biomarkers in Parkinson's disease: A prospectivelongitudinal study. Parkinsonism Relat Disord 2013;19:717–24.
32. Bech S, Hjermind LE, Salvesen L, et al. Amyloidrelated biomarkers and axonal damage proteins in parkinsoniansyndromes. Parkinsonism Related Disord 2012;18:69–72.
33. Schoonenboom NS, Reesink FE, Verwey NA, et al. Cerebrospinal fluid markers for differential dementia diagnosis in alarge memory clinic cohort. Neurology 2012;78:47–54.
34. Andersson M, Zetterberg H, Minthon L, et al. The cognitive profile and CSF biomarkers in dementia with Lewy bodiesand Parkinson's disease dementia. Int J Geriatr Psychiatry 2011;26:100–5.
35. Jellinger KA, Attems J. Prevalence and impact of vascular and Alzheimer pathologies in Lewy body disease. ActaNeuropathol 2008;115:427–36.
36. Ballard C, Ziabreva I, Perry R, et al. Differences in neuropathologic characteristics across the Lewy body dementiaspectrum. Neurology 2006;67:1931–4.
37. Halliday G, Hely M, Reid W, et al. The progression of pathology in longitudinally followed patients with Parkinson'sdisease. Acta Neuropathol 2008;115:409–15.
38. Siderowf A, Xie SX, Hurtig H, et al. CSF amyloid beta 1–42 predicts cognitive decline in Parkinson's disease.Neurology 2010;75:1055–61.
39. Stefanis L. alphaSynuclein in Parkinson's disease. Cold Spring Harb Perspect Med 2012;2:a009399.
40. Henchcliffe C, Dodel R, Beal MF. Biomarkers of Parkinson's disease and Dementia with Lewy bodies. Prog Neurobiol2011;95:601–13.
41. Ohrfelt A, Zetterberg H, Andersson K, et al. Identification of novel alphasynuclein isoforms in human brain tissue byusing an online nanoLCESIFTICRMS method. Neurochem Res 2011;36:2029–42.
42. Conway KA, Lee SJ, Rochet JC, et al. Acceleration of oligomerization, not fibrillization, is a shared property of bothalphasynuclein mutations linked to earlyonset Parkinson's disease: implications for pathogenesis and therapy. ProcNatl Acad Sci USA 2000;97:571–6.
43. Aerts MB, Esselink RA, Abdo WF, et al. CSF αsynuclein does not differentiate between parkinsonian disorders. NBA2012;33:430.e1–e3.
44. NoguchiShinohara M, Tokuda T, Yoshita M, et al. CSF alphasynuclein levels in dementia with Lewy bodies andAlzheimer's disease. Brain Res 2009;1251:1–6.
45. Spies PE, Melis RJ, Sjögren MJ, et al. Cerebrospinal fluid alphasynuclein does not discriminate between dementiadisorders. J Alzheimers Dis 2009;16:363–9.
46. van Dijk KB, Weiss M, Raijmakers A, et al. Reduced asynuclein levles in cerebrospinal fluid in Parkinson's diseaseare unrelated to clinical and imaging measures of disease severity. Eur J Neurol 2013;3:388–94.
47. Wennström M, Surova Y, Hall S, et al. Low CSF Levels of both αsynuclein and the αsynuclein cleaving enzyme

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 18/21
neurosin in patients with synucleinopathy. PLoS ONE 2013;8:e53250.
48. Mollenhauer B, Trautmann E, Taylor P, et al. Total CSF αsynuclein is lower in de novo Parkinson patients than inhealthy subjects. Neurosci Lett 2013;532:44–8.
49. Tateno F, Sakakibara R, Kawai T, et al. Alphasynuclein in the cerebrospinal fluid differentiates synucleinopathies(Parkinson Disease, dementia with Lewy bodies, multiple system atrophy) from Alzheimer disease. Alzheimer DisAssoc Disord 2012;26:213–16.
50. Wang Y, Shi M, Chung KA, et al. Phosphorylated αsynuclein in Parkinson's disease. Sci Transl Med 2012;4:121ra20.
51. Mollenhauer B, SchulzSchaeffer WJ, Schlossmacher MG. CSF αsynuclein, tau, and amyloid β in Parkinson'sdisease. Authors' reply. Lancet Neurol 2011;10:681–3.
52. Hong Z, Chung KA, Quinn JF, et al. DJ1 and αsynuclein in human cerebrospinal fluid as biomarkers of Parkinson'sdisease. Brain 2010;133:713–26.
53. Mollenhauer B, Cullen V, Kahn I, et al. Direct quantification of CSF alphasynuclein by ELISA and first crosssectionalstudy in patients with neurodegeneration. Exp Neurol 2008;213:315–25.
54. Mollenhauer B, Locascio JJ, SchulzSchaeffer W, et al. αSynuclein and tau concentrations in cerebrospinal fluid ofpatients presenting with parkinsonism: a cohort study. Lancet Neurol 2011;10:230–40.
55. Tokuda T, Salem SA, Allsop D, et al. Decreased alphasynuclein in cerebrospinal fluid of aged individuals andsubjects with Parkinson's disease. Biochem Biophys Res Commun 2006;349:162–6.
56. Blennow K, Hampel H, Weiner M, et al. Cerebrospinal fluid and plasma biomarkers in Alzheimer's disease. Nat RevNeurol 2010;6:131–44.
57. Tokuda T, Qureshi MM, Ardah MT, et al. Detection of elevated levels of αsynuclein oligomers in CSF from patientswith Parkinson's disease. Neurology 2010;75:1766–70.
58. Park MJ, Cheon SM, Bae HR, et al. Elevated levels of αsynuclein oligomer in the cerebrospinal fluid of drugnaïvepatients with Parkinson's disease. J Clin Neurol 2011;7:215.
59. Sierks MR, Chatterjee G, McGraw C, et al. CSF levels of oligomeric alphasynuclein and betaamyloid as biomarkersfor neurodegenerative disease. Integr Biol 2011;3:1188.
60. Foulds PG, Yokota O, Thurston A, et al. Post mortem cerebrospinal fluid αsynuclein levels are raised in multiplesystem atrophy and distinguish this from the other αsynucleinopathies, Parkinson's disease and Dementia with Lewybodies. Neurobiol Dis 2012;45:188–95.
61. Kouri N, Whitwell JL, Josephs KA, et al. Corticobasal degeneration: a pathologically distinct 4R tauopathy. Nat RevNeurol 2011;7:263–72.
62. Goedert M, Spillantini MG, Potier MC, et al. Cloning and sequencing of the cDNA encoding an isoform of microtubuleassociated protein tau containing four tandem repeats: differential expression of tau protein mRNAs in human brain.EMBO J 1989;8:393–9.
63. de Silva R, Lashley T, Gibb G, et al. Pathological inclusion bodies in tauopathies contain distinct complements of tauwith three or four microtubulebinding repeat domains as demonstrated by new specific monoclonal antibodies.Neuropathol Appl Neurobiol 2003;29:288–302.
64. Luk C, Compta Y, Magdalinou N, et al. Development and assessment of sensitive immunoPCR assays for thequantification of cerebrospinal fluid threeand fourrepeat tau isoforms in tauopathies. J Neurochem 2012;123:396–405.
65. Borroni B, Malinverno M, Gardoni F, et al. Tau forms in CSF as a reliable biomarker for progressive supranuclearpalsy. Neurology 2008;71:1796–803.
66. Borroni B, Malinverno M, Gardoni F, et al. A combination of CSF tau ratio and midsaggital midbraintopons atrophyfor the early diagnosis of progressive supranuclear palsy. J Alzheimers Dis 2010;22:195–203.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 19/21
67. Kuiperij HB, Verbeek MM. Diagnosis of progressive supranuclear palsy: can measurement of tau forms help?Neurobiol Aging 2012;33:204 e17–18.
68. Meredith JE Jr, Sankaranarayanan S, Guss V, et al. Characterization of Novel CSF Tau and ptau Biomarkers forAlzheimer's Disease. PLoS One 2013;8:e76523.
69. Lasec R. Studying the intrinsic determinants of neuronal form and function. Intrinsic Determinants of Neuronal Formand Function, 1988:1–60.
70. Brettschneider J, Petzold A, Süssmuth SD, et al. Neurofilament heavychain NfH (SMI35) in cerebrospinal fluidsupports the differential diagnosis of Parkinsonian syndromes. Mov Disord 2006;21:2224–7.
71. Constantinescu R, Rosengren L, Johnels B, et al. Consecutive analyses of cerebrospinal fluid axonal and glialmarkers in Parkinson's disease and atypical parkinsonian disorders. Parkinsonism Relat Disord 2010;16:142–5.
72. Salvesen L, Bech S, Lokkegaard A, et al. The DJ1 concentration in cerebrospinal fluid does not differentiate amongparkinsonian syndromes. Parkinsonism Relat Disord 2012;18:899–901.
73. Herbert MK, Eeftens JM, Aerts MB, et al. CSF levels of DJ1 and tau distinguish MSA patients from PD patients andcontrols. Parkinsonism Relat Disord 2013;1:1–4.
74. Gmitterova K, Heinemann U, Gawinecka J, et al. 8OHdG in cerebrospinal fluid as a marker of oxidative stress invarious neurodegenerative diseases. Neurodegener Dis 2009;6:263–9.
75. Davis JW, Grandinetti A, Waslien CJ, et al. Observations on serum uric acid levels and the risk of idiopathicParkinson's disease. Am J Epidemiol 1996;144:480–4.
76. Annanmaki T, Muuronen A, Murros K. Low plasma uric acid level in Parkinson's disease. Mov Disord 2007;22:1133–7.
77. Maetzler W, Stapf AK, Schulte C, et al. Serum and cerebrospinal fluid uric acid levels in lewy body disorders:associations with disease occurrence and amyloidbeta pathway. J Alzheimers Dis 2011;27:119–26.
78. Constantinescu R, Andreasson U, Holmberg B, et al. Serum and cerebrospinal fluid urate levels in synucleinopathiesversus tauopathies. Acta Neurol Scand 2013;127: e8–12.
79. Wang Y, Hancock AM, Bradner J, et al. Complement 3 and factor h in human cerebrospinal fluid in Parkinson'sdisease, Alzheimer's disease, and multiplesystem atrophy. Am J Pathol 2011;178:1509–16.
80. Maetzler W, Stoycheva V, Schmid B, et al. Neprilysin activity in cerebrospinal fluid is associated with dementia andamyloidbeta42 levels in Lewy body disease. J Alzheimers Dis 2010;22:933–8.
81. LeWitt P, Schultz L, Auinger P, et al. CSF xanthine, homovanillic acid, and their ratio as biomarkers of Parkinson'sdisease. Brain Res 2011;1408:88–97.
82. Goldstein DS, Holmes C, Sharabi Y. Cerebrospinal fluid biomarkers of central catecholamine deficiency in Parkinson'sdisease and other synucleinopathies. Brain 2012;135:1900–13.
83. Parnetti L, Castrioto A, Chiasserini D, et al. Cerebrospinal fluid biomarkers in Parkinson's disease. Nat Rev Neurol2013;3:131–40.
84. Brady RO, Kanfer J, Shapiro D. The metabolism of glucocerebrosides. I. Purification and properties ofglucocerebrosidasecleaving enzyme from spleen tissue. J Biol Chem 1965;240:39–43.
85. Sidransky E, Nalls MA, Aasly JO, et al. Multicenter analysis of glucocerebrosidase mutations in Parkinson's disease. NEngl J Med 2009;361:1651–61.
86. Mazzulli JR, Xu YH, Sun Y, et al. Gaucher disease glucocerebrosidase and alphasynuclein form a bidirectionalpathogenic loop in synucleinopathies. Cell 2011;146:37–52.
87. Balducci C, Pierguidi L, Persichetti E, et al. Lysosomal hydrolases in cerebrospinal fluid from subjects with Parkinson'sdisease. Mov Disord 2007;22:1481–4.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 20/21
Acknowledgements
We would like to thank Dr Janice Holton for kindly providing the pathological images.
Contributors
All authors contributed to the design of this review. NM drafted the manuscript, and HZ and AJL revised it.
Funding
NM is funded through the PSP association. HZ is funded through the Leonard Wolfson Experimental Neurology Centre.
Competing interests
None.
88. Parnetti L, Balducci C, Pierguidi L, et al. Cerebrospinal fluid betaglucocerebrosidase activity is reduced in Dementiawith Lewy Bodies. Neurobiol Dis 2009;34:484–6.
89. Parnetti L, Chiasserini D, Persichetti E, et al. Cerebrospinal fluid lysosomal enzymes and alphasynuclein inParkinson's disease. Mov Disord 2014. doi:10.1002/mds. 25772. (Epub ahead of print).
90. van Dijk KD, Persichetti E, Chiasserini D, et al. Changes in endolysosomal enzyme activities in cerebrospinal fluid ofpatients with Parkinson's disease. Mov Disord 2013;28:747–54.
91. Caudle WM, Bammler TK, Lin Y, et al. Using 'omics' to define pathogenesis and biomarkers of Parkinson's disease.Expert Rev Neurother 2010;10:925–42.
92. Abdi F, Quinn JF, Jankovic J, et al. Detection of biomarkers with a multiplex quantitative proteomic platform incerebrospinal fluid of patients with neurodegenerative disorders. J Alzheimer's Dis 2006;9:293–348.
93. Zhang J, Sokal I, Peskind ER, et al. CSF Multianalyte Profile Distinguishes Alzheimer and Parkinson Diseases. Am JClin Pathol 2008;129:526–9.
94. Constantinescu R, Andreasson U, Li S, et al. Proteomic profiling of cerebrospinal fluid in parkinsonian disorders.Parkinsonism Relat Disord 2010;16:545–9.
95. Ishigami N, Tokuda T, Ikegawa M, et al. Cerebrospinal fluid proteomic patterns discriminate Parkinson's disease andmultiple system atrophy. Mov Disord 2012;27:851–7.
96. Mattison HA, Stewart T, Zhang J. Applying bioinformatics to proteomics: Is machine learning the answer to biomarkerdiscovery for PD and MSA? Movement Disorders 2012;27:1595–7.
97. Jesse S, Lehnert S, Jahn O, et al. Differential sialylation of serpin A1 in the early diagnosis of Parkinson's diseasedementia. PLoS One 2012;7:e48783.
98. Lehnert S, Jesse S, Rist W, et al. iTRAQ and multiple reaction monitoring as proteomic tools for biomarker search incerebrospinal fluid of patients with Parkinson's disease dementia. Exp Neurol 2012;234:499–505.
99. The Lancet N. Biomarker promise for Parkinson's disease. Lancet Neurol 2010;9:1139.
100. Parkinson Progression Marker I. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol 2011;95:629–35.
101. Bagchi DP, Yu L, Perlmutter JS, et al. Binding of the radioligand SIL23 to alphasynuclein fibrils in Parkinson diseasebrain tissue establishes feasibility and screening approaches for developing a Parkinson disease imaging agent. PLoSONE 2013;8:e55031.
102. Kuiperij HB, Verbeek MM, Borroni B. Tau forms in CSF as a reliable biomarker for progressive supranuclear palsy.Neurology 2011;76:1443; author reply 1443.
103. Borroni B, Malinverno M, Gardoni F, et al. A combination of CSF tau ratio and midsaggital midbraintopons atrophyfor the early diagnosis of progressive supranuclear palsy. J Alzheimer 's Dis 2010;22:195–203.

20/11/2014 www.medscape.com/viewarticle/832659_print
http://www.medscape.com/viewarticle/832659_print 21/21
Provenance and peer review
Not commissioned; externally peer reviewed.
J Neurol Neurosurg Psychiatry. 2014;85(10):10651075. © 2014 BMJ Publishing Group