Embed Size (px)
Citation preview
Compression of the Left Ventricular OutflowTract During Cardiopulmonary ResuscitationSung Oh Hwang, MD, Pei Ge Zhao, MD, Han Joo Choi, MD, Kyung Hye Park, MD, Kyung Chul Cha,MD, So Mi Park, RN, PhD, Sang Chul Kim, MD, Hyun Kim, MD, and Kang Hyun Lee, MD
AbstractObjectives: This prospective observational study was performed to investigate if the hand position usedfor external chest compressions is in an optimal position for compressing the ventricles during standardcardiopulmonary resuscitation (CPR).
Methods: Transesophageal echocardiography (TEE) was performed during standard CPR in 34 patientswith nontraumatic cardiac arrest (24 males, mean ± standard deviation [SD] age = 56 ± 12 years). On therecorded image of TEE, an area of maximal compression (AMC) was identified, and the degree of com-pression at the AMC and the left ventricular stroke volume was calculated.
Results: A significant narrowing of the left ventricular outflow tract (LVOT) or the aorta was noted in allpatients, with the degree of compression at the AMC ranging from 19% to 83%(mean ± SD = 49 ± 19%). The AMC was found at the aorta in 20 patients (59%) and at the LVOT in 14patients (41%). A significant narrowing of more than 50% of the diameter at the end of the relaxationphase occurred in 15 patients (44%). On linear regression, the left ventricular stroke volume was corre-lated with the location of the AMC (R2 = 0.165, p = 0.017).
Conclusions: The outflow of the left ventricle is affected during standard CPR, resulting in varyingdegrees of narrowing in the LVOT and ⁄ or the aortic root.
ACADEMIC EMERGENCY MEDICINE 2009; 16:928–933 ª 2009 by the Society for Academic EmergencyMedicine
Keywords: cardiopulmonary resuscitation, external chest compressions
Closed-chest cardiopulmonary resuscitation (CPR)was first introduced in 1960,1 and it has beenused worldwide and documented to be effective
in rescuing patients with cardiac arrest. During standardCPR, artificial circulation via external chest compres-sions is achieved with repetitive, rhythmic compressionsof the sternum. External chest compression is presumedto generate blood flow by increasing intrathoracic pres-sure and ⁄ or producing direct compression of the cardiacchambers.2–6 Blood flow generated by external chestcompression is approximately one-third that of normal
cardiac output.7,8 Many researchers have made efforts toimprove the hemodynamic efficacy of external chestcompression during CPR by focusing on the depth orrate of compression.9,10
The 2005 International Consensus Conference onCardiopulmonary Resuscitation and Emergency Car-diac Care Science with Treatment Recommendationrecommends that the rescuer place his or her hands onthe lower half of the victim’s sternum, at the center ofthe chest between the nipples, and depress the sternumapproximately 4 to 5 cm.11 The European ResuscitationCouncil also recommends the middle of the lower halfof the sternum as the correct hand position for externalchest compression.12 The hand position currently rec-ommended by these guidelines is not much differentfrom the position originally suggested in 1960.Although only minor adjustments to the compressionposition have been made to reduce the complications ofexternal chest compression,13,14 there has been noreport about whether the current hand position is mostoptimal for external chest compression during resusci-tation of patients with cardiac arrest.
Direct compression of the ventricles should theoreti-cally be the most effective way to generate blood flowduring CPR.15 Intrathoracic structures, including the
ISSN 1069-6563 ª 2009 by the Society for Academic Emergency Medicine928 PII ISSN 1069-6563583 doi: 10.1111/j.1553-2712.2009.00497.x
From the Department of Emergency Medicine (SOH, PGZ,HJC, KHP, KCC, SCK, HK, KHL) and the Department of Nurs-ing (SMP), Wonju College of Medicine, Institute of LifelongHealth, Yonsei University Wonju, Wonju, Republic of Korea.Received February 27, 2009; revision received May 8, 2009;accepted May 18, 2009.This work won the Young Investigation Award at the Resuscita-tion Science Symposium, American Heart Association, Novem-ber 11, 2006.This study was supported by a grant (A020602) from the Minis-try of Health and Welfare, Republic of Korea.Address for correspondence and reprints: Sung Oh Hwang,MD; e-mail: [email protected].

cardiac chambers and the great vessels, will be sub-jected to external chest compression. However, little isknown about which region of the heart is subjected toexternal chest compression in patients with cardiacarrest. Transesophageal echocardiography (TEE) pro-vides excellent images of the heart during CPR withoutinterrupting resuscitation attempts.16,17 Studies usingTEE have focused on demonstrating valve positions toexplain the mechanism of blood flow generated byexternal chest compression.18,19 However, there hasbeen no report regarding the morphologic change ofthe heart during external chest compression. This studywas performed to investigate whether the recom-mended hand position for external chest compressionis optimal for compressing the ventricles during stan-dard CPR by observing the heart with TEE.
METHODS
Study DesignThis was a prospective observational study. The studywas approved by the institutional review board with awaiver of informed consent. Verbal instructions weregiven to the patients’ families.
Study Setting and PopulationThe study was conducted at a university-based tertiarycare emergency department (ED), in Wonju, Republicof Korea. Prehospital emergency care in Wonju is pro-vided by a 1-1-9 emergency system that includes one-tier basic life support transport with a capability ofautomated external defibrillation.
We enrolled nontraumatic cardiac arrest patientsolder than 18 years who had been admitted to the EDin cardiac arrest or who had developed cardiac arrestduring their stay in the ED. Patients with configurativechanges of intrathoracic structures on chest x-ray takenafter resuscitation attempts were excluded from theanalysis.
Study ProtocolCPR. A team performed CPR as soon as the patientarrived at the ED or immediately following cardiacarrest. CPR was performed in accordance with theAmerican Heart Association (AHA) guidelines for CPRand emergency cardiovascular care.11 Once endotra-cheal intubation was completed, uninterrupted externalchest compressions were performed by an emergencymedicine resident at a rate of 100 times ⁄ min accordingto the rhythm of a metronome. Artificial ventilation wasperformed using a self-inflating bag at a rate of 10 to12 breaths ⁄ min. An intravenous dose of 1 mg of epi-nephrine was administered every 3 min through a veinin the upper extremities or through a central vein.
TEE. Transesophageal echocardiography was per-formed during CPR following tracheal intubation andthe first injected dose of epinephrine. A multiplanetransesophageal probe (5 MHz, Ultramark-9, AdvancedTechnology Laboratories Inc., Bothell, WA; or 5 MHz,Sequoia C256 echocardiography system, Acuson Corp.,Malvern, PA) was introduced into the esophagus toobserve the heart and the ascending aorta. Chest com-
pression was continued during introduction of theprobe. Immediately after the transesophageal probewas inserted, the heart was briefly examined to searchfor possible causes of the cardiac arrest. A horizontalfour-chamber view was used to evaluate the extent ofleft ventricle compression and observe valve positions.The left ventricle, the left atrium, and the ascendingaorta were assessed through a 135� longitudinal view.All procedures, from intubation to removal of the TEEtransducer, were recorded on an s-VHS videotape.
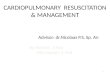
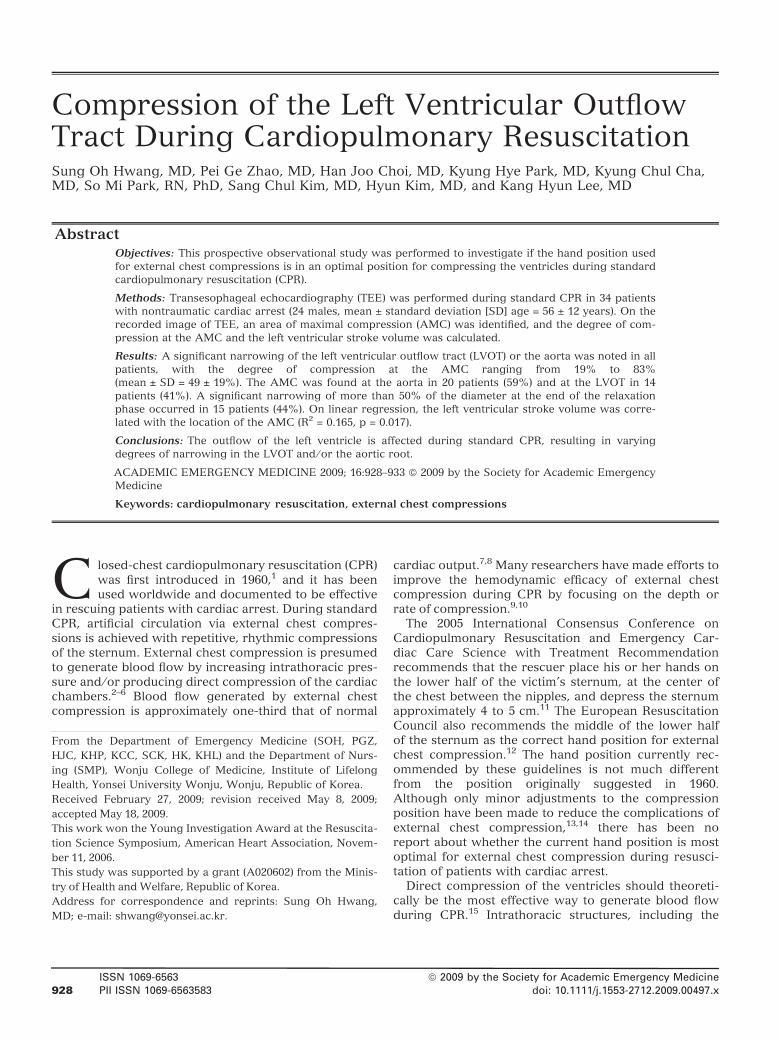
Analyses of Recorded Images. The images recordedduring CPR were analyzed using a cardiac image analy-sis system (Imagevue, Nova MicroSonics Inc., Carmel,IN). After freezing the images recorded with the cardiacanalysis system, the system was calibrated with aninternalized calibrator. The area of maximal compres-sion (AMC) was defined as an area of the left ventricleor the ascending aorta that was most prominently com-pressed at the end of compression phase on a 135�longitudinal view of the left ventricle. The exact positionof the AMC was visually identified on frozen images atthe end of compression. Once the AMC was deter-mined, a distance from the AMC to the aortic valve wasmeasured and maximal and minimal diameters of theAMC during external chest compression were mea-sured. The ratio of maximal diameter to minimal diame-ter was calculated as the degree of compression at theAMC (Figure 1). Left ventricular volume was calculatedusing the area–length method, which involves subtract-ing the volume at the end of the compression phasefrom the volume at the end of the relaxation phase toacquire the left ventricular stroke volume.20 Each mea-surement was determined by an average of five consec-utive compressions.
Data AnalysisThe data were coded into computerized data processingsoftware (SPSS for Windows 12.0, SPSS Inc., Chicago,IL). We conducted a linear regression model to evaluatethe relationship between the left ventricular stroke vol-ume and the location of the AMC and the degree ofcompression at the AMC. Statistical significance wasnoted if the p-value was less than 0.05. All data are pre-sented as mean (± standard deviation [SD]).
RESULTS
General Characteristics of the PatientsIn this study, 36 patients suffering from nontraumaticcardiac arrest received TEE. Two patients wereexcluded who had a marked shift in heart position onchest x-ray. Twenty-eight patients went into cardiacarrest in the field, and six patients went into cardiacarrest in the ED. Total arrest time ranged from 1 to120 minutes, with a mean of 31 (±10) minutes. TotalCPR time ranged from 20 to 92 minutes, with a mean of45 (±14) minutes. The initial presenting rhythm wasventricular fibrillation in four patients, pulseless electri-cal activity in 10 patients, and asystole in 20 patients.Return of spontaneous circulation occurred in eightpatients following CPR. Only four patients survived tohospital discharge. Characteristics of the patients are
ACAD EMERG MED • October 2009, Vol. 16, No. 10 • www.aemj.org 929
detailed in Table 1. The average time from patient arri-val to completion of the TEE probe insertion was 8(±7) minutes. There was no difficulty introducing theTEE probe into the esophagus.
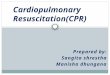
Morphologic Changes of the Heart and Localizationof the AMCOn TEE observation, the base of the heart and theaorta, including the left ventricular outflow tract(LVOT), the ascending aorta, and the right ventricularoutflow tract, were compressed by external chest com-pression. In all patients, a significant narrowing ofeither the aortic root or the LVOT was observed in the135� longitudinal view of the TEE (Figure 2). The AMCwas identified at the aorta (which included the aorticvalve) in 20 patients (59%) and at the LVOT in 14patients (41%). The AMC was located within 2 cm ofthe aortic valve in 79% of the patients. The mitral valvewas closed during the compression phase, and openduring the relaxation phase, whereas the aortic valvewas open during the compression phase and closedduring the relaxation phase.
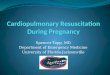
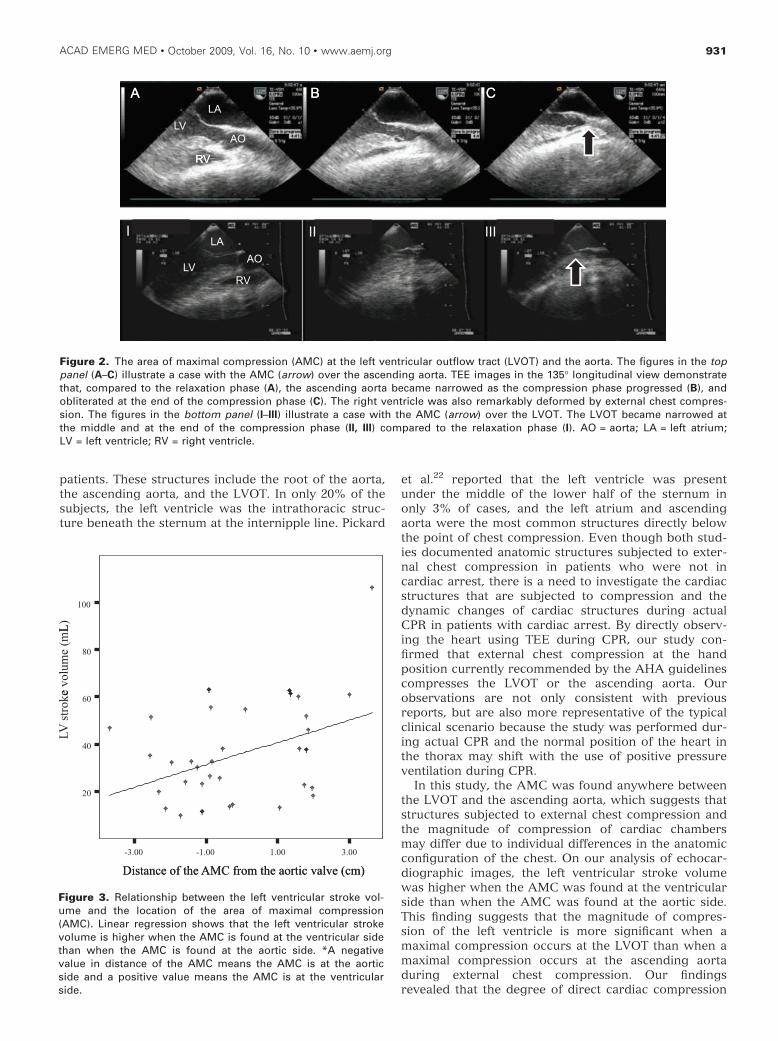
Degree of Compression and Left Ventricular StrokeVolume According to the Location of the AMCVariable degrees of compression of the aorta or theLVOT were observed. The mean diameter at the AMCwas 2.1 (±0.5) cm at the end of the relaxation phase and1.0 (±0.4) cm at the end of the compression phase(p = 0.001). The degree of compression at the AMCranged from 19% to 83% (mean ± sd = 49 ± 19%). Anarrowing of more than 50% of the diameter at theend of the relaxation phase occurred in 15 patients(44%). On linear regression, the left ventricular stokevolume was correlated with the location of the AMC(R2 = 0.165, p = 0.017; Figure 3); that is, the closer theAMC was to the left ventricle, the higher the observedleft ventricular stroke volume. No significant correlationwas found between the left ventricular stroke volumeand the degree of compression at the AMC (R2 = 0.007,p = 0.626).
DISCUSSION
The results of this study, in which TEE observation wasperformed during CPR, demonstrate that the AMC liesat the base of the heart or at the ascending aorta dur-ing standard CPR, resulting in varying degrees of com-pression in the LVOT and ⁄ or the aortic root. In ourstudy, external chest compressions were performedaccording to the AHA guidelines for CPR and emer-gency cardiovascular care, in which rescuers areinstructed to compress the lower half of the victim’ssternum to a depth of 4 to 5 cm in the middle of thechest between the nipples.11 Considering the cross-sec-tional anatomy of the thorax at the level of the chestcompressions, it is easy to predict which cardiac struc-tures will be subjected to external chest compressions.Two recent studies analyzing chest computed tomogra-phy scans of patients demonstrated the anatomic con-figuration of the intrathoracic structures in thecompression position. Shin et al.21 reported that intra-thoracic structures just beneath the internipple lineformed the cardiac base in 80% of the study’s 189
Figure 1. Measurement of the diameter at the area of maximal compression (AMC) on M-mode tracing. AO = aorta;AMCcom = diameter of the AMC in the compression phase (short arrow); AMCrel = diameter of the AMC in the relaxation phase(long arrow); AV = aortic valve (opening); LA = left atrium; RV = right ventricle.
Table 1Characteristics of Patients (n = 34)
Characteristics Value
Age (yr) 56 ± 12Male (%) 24 (71)Down time (min) 31 ± 10CPR time (min) 45 ± 14Initial rhythm
Asystole (%) 20 (59)VF (%) 4 (12)PEA (%) 10 (29)Survival (%) 4 (12)
The nonpercent values shown are means ± SDs.CPR = cardiopulmonary resuscitation; PEA = pulselesselectrical activity; VF = ventricular fibrillation.
930 Hwang et al. • COMPRESSION OF THE LEFT VENTRICULAR OUTFLOW TRACT DURING CPR
patients. These structures include the root of the aorta,the ascending aorta, and the LVOT. In only 20% of thesubjects, the left ventricle was the intrathoracic struc-ture beneath the sternum at the internipple line. Pickard
et al.22 reported that the left ventricle was presentunder the middle of the lower half of the sternum inonly 3% of cases, and the left atrium and ascendingaorta were the most common structures directly belowthe point of chest compression. Even though both stud-ies documented anatomic structures subjected to exter-nal chest compression in patients who were not incardiac arrest, there is a need to investigate the cardiacstructures that are subjected to compression and thedynamic changes of cardiac structures during actualCPR in patients with cardiac arrest. By directly observ-ing the heart using TEE during CPR, our study con-firmed that external chest compression at the handposition currently recommended by the AHA guidelinescompresses the LVOT or the ascending aorta. Ourobservations are not only consistent with previousreports, but are also more representative of the typicalclinical scenario because the study was performed dur-ing actual CPR and the normal position of the heart inthe thorax may shift with the use of positive pressureventilation during CPR.
In this study, the AMC was found anywhere betweenthe LVOT and the ascending aorta, which suggests thatstructures subjected to external chest compression andthe magnitude of compression of cardiac chambersmay differ due to individual differences in the anatomicconfiguration of the chest. On our analysis of echocar-diographic images, the left ventricular stroke volumewas higher when the AMC was found at the ventricularside than when the AMC was found at the aortic side.This finding suggests that the magnitude of compres-sion of the left ventricle is more significant when amaximal compression occurs at the LVOT than when amaximal compression occurs at the ascending aortaduring external chest compression. Our findingsrevealed that the degree of direct cardiac compression
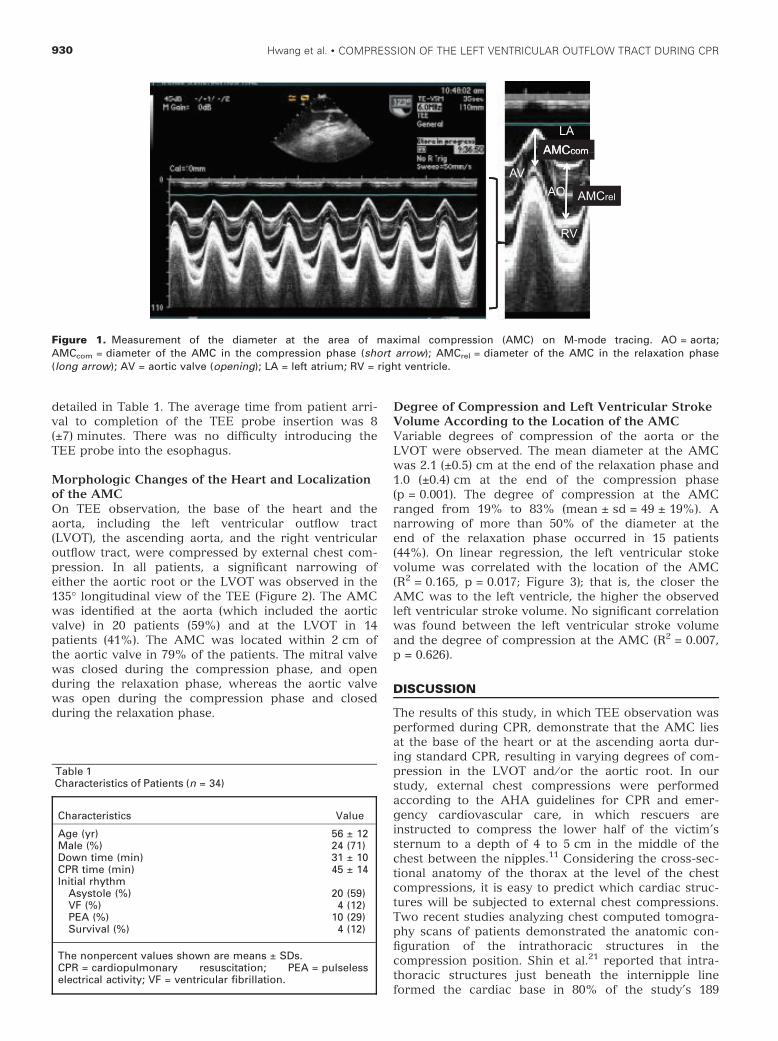
Figure 2. The area of maximal compression (AMC) at the left ventricular outflow tract (LVOT) and the aorta. The figures in the toppanel (A–C) illustrate a case with the AMC (arrow) over the ascending aorta. TEE images in the 135� longitudinal view demonstratethat, compared to the relaxation phase (A), the ascending aorta became narrowed as the compression phase progressed (B), andobliterated at the end of the compression phase (C). The right ventricle was also remarkably deformed by external chest compres-sion. The figures in the bottom panel (I–III) illustrate a case with the AMC (arrow) over the LVOT. The LVOT became narrowed atthe middle and at the end of the compression phase (II, III) compared to the relaxation phase (I). AO = aorta; LA = left atrium;LV = left ventricle; RV = right ventricle.
Figure 3. Relationship between the left ventricular stroke vol-ume and the location of the area of maximal compression(AMC). Linear regression shows that the left ventricular strokevolume is higher when the AMC is found at the ventricular sidethan when the AMC is found at the aortic side. *A negativevalue in distance of the AMC means the AMC is at the aorticside and a positive value means the AMC is at the ventricularside.
ACAD EMERG MED • October 2009, Vol. 16, No. 10 • www.aemj.org 931

might be dependent on the configuration of the heart inthe thorax.
In addition to the compression of the cardiac baserather than the left ventricle, the outflow of the left ven-tricle narrowed at the end of compression. In a fewpatients, the aorta was totally obliterated during thecompression phase. Therefore, there is a possibility thata higher degree of narrowing of the outflow tract mayoccur during external chest compression. Compressionof the LVOT (or the aortic root) may have an adverseeffect on the efficacy of CPR by increasing resistance toforward blood flow from the left ventricle.
Our observations suggest that the compression loca-tion currently recommended by the AHA guidelinesmay not be effective in generating forward blood flowduring CPR. Compression of the sternum with handplacement caudal to the currently recommended loca-tion appears to be optimal to avoid compression of leftventricular outflow. The alternative location we suggestis the area on the sternum between the standard posi-tion and the xiphoid process. If the compression is cen-tered on the extreme caudal part on the xiphoidprocess, it may be driven into the left lobe of the liver,resulting in a laceration of the liver.23 Lateral shifts inthe location of the compression may cause subluxationof the costochondral junctions or rib fractures. Com-pression of the caudal part of the sternum might havean additional advantage. As the cephalic part of thesternum is attached to the clavicles, the sternum maybe easier to compress with adequate depth when rescu-ers compress the caudal part of the sternum. Therefore,it is possible that compressing the caudal part of thesternum will improve the quality of CPR and reducerescuer fatigue. Further research is needed to examinethese possibilities.
LIMITATIONS
The time from onset of cardiac arrest to initiation ofTEE varied among patients. Differences in time elapsedfrom cardiac arrest may affect myocardial stiffness,which influences the degree of compression of theheart.24,25 Due to the limitations of two-dimensionalechocardiography, we measured the diameter at theAMC with the assumption that the LVOT and aorta arecircular. Even though the LVOT or aorta may undergomorphologic changes during cardiac arrest, the changein its diameter may reflect a degree of compressionduring external chest compression. Thoracic configura-tion differences are attributed to various body typesand the sex and age of individuals.26–28 Some pleural,pulmonary, or cardiovascular diseases can also alterthe relative position of the heart and sternum.29 Wecould not investigate the relationship between bodyfeatures and the location of the AMC because a detailedbody measurement could not be performed.
CONCLUSIONS
Direct observation with transesophageal echocardiog-raphy during resuscitation shows that the outflow ofthe left ventricle is affected during standard cardiopul-monary resuscitation, resulting in varying degrees of
narrowing in the left ventricular outflow tract and ⁄ orthe aortic root.
References
1. Kouwenhoven WB, Jude JR, Knickerbocker GG.Closed-chest cardiac massage. JAMA. 1960;173:1064–7.
2. Beattie C, Guerci AD, Hall T, et al. Mechanisms ofblood flow during pneumatic vest cardiopulmonaryresuscitation. J Appl Physiol. 1991; 70:454–65.
3. Halperin HR, Tsitlik JE, Guerci AD, et al. Determi-nants of blood flow to vital organs during cardio-pulmonary resuscitation in dogs. Circulation. 1986;73:539–50.
4. Maier GW, Tyson GS Jr, Olsen CO, et al. The physi-ology of external cardiac massage: high-impulsecardiopulmonary resuscitation. Circulation. 1984;70:86–101.
5. Mair P, Kornberger E, Schwarz B, Baubin M, Hoer-mann C. Forward blood flow during cardiopulmo-nary resuscitation in patients with severe accidentalhypothermia. An echocardiographic study. ActaAnaesthesiol Scand. 1998; 42:1139–44.
6. Kim H, Hwang SO, Lee CC, et al. Direction of bloodflow from the left ventricle during cardiopulmonaryresuscitation in humans: its implications for mecha-nism of blood flow. Am Heart J. 2008; 156:1222 e1–7.
7. Fitzgerald KR, Babbs CF, Frissora HA, Davis RW,Silver DI. Cardiac output during cardiopulmonaryresuscitation at various compression rates anddurations. Am J Physiol. 1981; 241:H442–8.
8. Klouche K, Weil MH, Sun S, Tang W, Povoas H,Bisera J. Stroke volumes generated by precordialcompression during cardiac resuscitation. Crit CareMed. 2002; 30:2626–31.
9. Ornato JP, Levine RL, Young DS, Racht EM, GarnettAR, Gonzalez ER. The effect of applied chestcompression force on systemic arterial pressure andend-tidal carbon dioxide concentration during CPRin human beings. Ann Emerg Med. 1989; 18:732–7.
10. Maier GW, Newton JR Jr, Wolfe JA, et al. The influ-ence of manual chest compression rate on hemody-namic support during cardiac arrest: high-impulsecardiopulmonary resuscitation. Circulation. 1986;74(6 Pt 2):IV51–9.
11. 2005 American Heart Association. Guidelines forcardiopulmonary resuscitation and emergency car-diovascular care. Circulation. 2005; 112(24 Suppl):IV1–203.
12. Handley AJ, Koster R, Monsieurs K, Perkins GD,Davies S, Bossaert L. European Resuscitation Coun-cil guidelines for resuscitation 2005. Section 2.Adult basic life support and use of automated exter-nal defibrillators. Resuscitation. 2005; 1:S7–23.
13. Orlowski JP. Optimum position for external cardiaccompression in infants and young children. AnnEmerg Med. 1986; 15:667–73.
14. Thaler MM, Stobie GH. An improved technique ofexternal cardiac compression in infants and youngchildren. N Engl J Med. 1963; 269:606–10.
15. Bartlett RL, Stewart NJ Jr, Raymond J, Anstadt GL,Martin SD. Comparative study of three methods of
932 Hwang et al. • COMPRESSION OF THE LEFT VENTRICULAR OUTFLOW TRACT DURING CPR
resuscitation: closed-chest, open-chest manual, anddirect mechanical ventricular assistance. AnnEmerg Med. 1984; 13(9 Pt 2):773–7.
16. Higano ST, Oh JK, Ewy GA, Seward JB. The mech-anism of blood flow during closed chest cardiacmassage in humans: transesophageal echocardio-graphic observations. Mayo Clin Proc. 1990; 65:1432–40.
17. Redberg RF, Tucker KJ, Cohen TJ, Dutton JP,Callaham ML, Schiller NB. Physiology of blood flowduring cardiopulmonary resuscitation. A trans-esophageal echocardiographic study. Circulation.1993; 88:534–42.
18. Ma MH, Hwang JJ, Lai LP, et al. Transesophagealechocardiographic assessment of mitral valve posi-tion and pulmonary venous flow during cardiopul-monary resuscitation in humans. Circulation. 1995;92:854–61.
19. Porter TR, Ornato JP, Guard CS, Roy VG, BurnsCA, Nixon JV. Transesophageal echocardiographyto assess mitral valve function and flow during car-diopulmonary resuscitation. Am J Cardiol. 1992;70:1056–60.
20. Schiller NB, Shah PM, Crawford M, et al. Recom-mendations for quantitation of the left ventricle bytwo-dimensional echocardiography. American Soci-ety of Echocardiography Committee on Standards,Subcommittee on Quantitation of Two-DimensionalEchocardiograms. J Am Soc Echocardiogr. 1989;2:358–67.
21. Shin J, Rhee JE, Kim K. Is the inter-nipple line thecorrect hand position for effective chest compres-sion in adult cardiopulmonary resuscitation? Resus-citation. 2007; 75:305–10.
22. Pickard A, Darby M, Soar J. Radiological assess-ment of the adult chest: implications for chest com-pressions. Resuscitation. 2006; 71:387–90.
23. Monsuez JJ, Charniot JC, Veilhan LA, Mougue F,Bellin MF, Boissonnas A. Subcapsular liver haema-toma after cardiopulmonary resuscitation byuntrained personnel. Resuscitation. 2007; 73:314–7.
24. Klouche K, Weil MH, Sun S, et al. Evolution of thestone heart after prolonged cardiac arrest. Chest.2002; 122:1006–11.
25. Takino M, Okada Y. Firm myocardium in cardiopul-monary resuscitation. Resuscitation. 1996; 33:101–6.
26. Bellemare F, Jeanneret A, Couture J. Sex differ-ences in thoracic dimensions and configuration. AmJ Respir Crit Care Med. 2003; 168:305–12.
27. Dansereau J, Stokes IA. Measurements of the three-dimensional shape of the rib cage. J Biomech. 1988;21:893–901.
28. Wilson TA, Rehder K, Krayer S, Hoffman EA, Whit-ney CG, Rodarte JR. Geometry and respiratory dis-placement of human ribs. J Appl Physiol. 1987;62:1872–7.
29. Cassart M, Gevenois PA, Estenne M. Rib cagedimensions in hyperinflated patients with severechronic obstructive pulmonary disease. Am J RespirCrit Care Med. 1996; 154(3 Pt 1):800–5.
ACAD EMERG MED • October 2009, Vol. 16, No. 10 • www.aemj.org 933