-
7/29/2019 Compresor intermitente TVP
1/9
Philippe VignonPierre-Francois DequinAnne RenaultArmelle
MathonnetNicolas PaleironAudrey ImbertDelphine ChatellierValerie
GissotGwenaelle LheritierVictor AboyansGwenael PratDenis
GarotThierry BoulainJean-Luc DiehlLuc BressolletteAurelien
DellucKarine Lacut
The Clinical Research in Intensive Careand Sepsis Group (CRICS
Group)
Intermittent pneumatic compression to prevent
venous thromboembolism in patients with high
risk of bleeding hospitalized in intensive careunits: the CIREA1
randomized trial
Received: 20 July 2012Accepted: 6 January 2013Published online:
31 January 2013 Springer-Verlag Berlin Heidelberg andESICM 2013
P. Vignon
G. LheritierReanimation Polyvalente, CHU Dupuytren,87042
Limoges, France
P. Vignon G. LheritierINSERM, CIC-P 0801, CHU Dupuytren,87042
Limoges, France
P. Vignon G. LheritierUniversite de Limoges,87000 Limoges,
France
P.-F. Dequin D. GarotUniversite Francois Rabelais et servicede
Reanimation Medicale,
CHU de ToursHopital Bretonneau,Tours, France
A. Renault G. PratService de Reanimation Medicale,CHU de la
Cavale Blanche, Brest, France
A. Mathonnet T. BoulainReanimation, CHRHopital de la
Source,Orleans, France
N. PaleironService des maladies respiratoires,HIA
Clermont-Tonnerre, Brest, France
A. Imbert J.-L. DiehlReanimation Medicale,HEGP AP-HP, Paris,
France
D. ChatellierService de Reanimation Medicale,CHU de Poitiers,
Poitiers, France
V. GissotService de Reanimation Polyvalente,CH DAngouleme,
Saint-Michel, France
V. AboyansService de Cardiologie, CHU de Limoges,Limoges,
France
J.-L. DiehlINSERM U765, Universite Paris Descartes,Sorbonne
Paris Cite, France
L. Bressollette A. Delluc K. LacutEA3878, Universite de
Bretagne
Occidentale, 29200 Brest, France
L. BressolletteUnite de Medecine Vasculaire,CHU Brest, 29609
Brest, France
A. DellucDepartement de Medecine Interneet Pneumologie, CHU
Brest,29609 Brest, France
K. LacutINSERM, CIC 0502, Brest, France
K. Lacut ())CIC 0502, Hopital de la Cavale Blanche,Bd Tanguy
Prigent, F-29609 Brest Cedex,Francee-mail:
[email protected].: ?33-29-8145007Fax:
?33-29-8145008
Abstract Purpose: Venousthromboembolism (VTE) is a fre-quent and
serious problem inintensive care units (ICU). Anticoag-ulant
treatments have demonstratedtheir efficacy in preventing
VTE.However, when the bleeding risk ishigh, they are
contraindicated, andmechanical devices are recom-mended. To date,
mechanicalprophylaxis has not been rigorouslyevaluated in any
trials in ICUpatients. Methods: In this multi-center, open-label,
randomized trialwith blinded evaluation of endpoints,we randomly
assigned 407 patientswith a high risk of bleeding to
receiveintermittent pneumatic compression(IPC) associated with
graduatedcompression stockings (GCS) or GCSalone for 6 days during
their ICU
Intensive Care Med (2013) 39:872880DOI 10.1007/s00134-013-2814-2
O R I G I N A L
-
7/29/2019 Compresor intermitente TVP
2/9
stay. The primary endpoint was theoccurrence of a VTE between
days 1and 6, including nonfatal symptom-atic documented VTE, or
death due toa pulmonary embolism, or asymp-tomatic deep vein
thrombosis
detected by ultrasonography system-atically performed on day
6.Results: The primary outcome wasassessed in 363 patients (89.2
%). Byday 6, the incidence of the primaryoutcome was 5.6 % (10 of
179
patients) in the IPC ? GCS groupand 9.2 % (17 of 184 patients)
in theGCS group (relative risk 0.60; 95 %confidence interval
0.281.28;p = 0.19). Tolerance of IPC was poorin only 12 patients
(6.0 %). No
intergroup difference in mortality ratewas observed.
Conclusions: Withthe limitation of a low statisticalpower, our
results do not support thesuperiority of the combination ofIPC ?
GCS compared to GCS alone
to prevent VTE in ICU patients athigh risk of bleeding.
Keywords Intermittentpneumatic compression devices Elastic
stockings Venous
thromboembolism
Venousthrombosis Intensive care units
Introduction
Venous thromboembolism (VTE), that occurs as eitherdeep vein
thrombosis (DVT) or pulmonary embolism(PE), is a major cause of
morbidity and mortality in
patients admitted to intensive care units (ICU) [1]. Criti-cally
ill patients have often multiple risk factors for VTE[2, 3]. Most
of these risk factors are related to age or comorbidities (e.g.,
cancer, obesity), or are acquired duringthe ICU stay (e.g., central
venous catheters, mechanicalventilation, or vasopressor use) [24].
The reported inci-dence rates of VTE in hospitalized patients range
between20 % and 80 % depending to the studied population, thetype
of thromboprophylaxis and the screening test used[5]. In the ICU
setting, PE may account for acute episodesof hemodynamic
instability or hypoxia and may contrib-ute to failure of weaning
from mechanical ventilation[6, 7]. Since VTE is frequently silent
and clinically
unsuspected in ICU patients [810], PE remains one ofthe most
common unexpected autopsy findings in thecritically ill [11], and
is found at autopsy in 7 % to 27 %of ICU fatalities [12, 13].
Surprisingly, little information is yet available on
VTEprophylaxis in the ICU. Randomized trials including ICUpatients
have indicated a benefit of unfractionated or lowmolecular weight
heparin over placebo, without signifi-cant risk of hemorrhage
[1416]. In ICU patients who areat high risk of bleeding,
anticoagulant treatments arecontraindicated, and current guidelines
recommend theoptimal use of mechanical thromboprophylaxis
withgraduated compression stockings (GCS) and/or intermit-
tent pneumatic compression (IPC) at least until thebleeding risk
decreases [17]. IPC has been shown to beeffective in preventing VTE
in neurosurgical patientsundergoing craniotomy [18]. A randomized
trial con-ducted in patients with intracerebral hemorrhage hasshown
that IPC is more efficient in preventing asymp-tomatic DVT than GCS
alone [19]. However, the efficacyand safety of mechanical
prophylaxis of VTE have not yetbeen specifically evaluated in ICU
patients. Accordingly,we carried out an open-label randomized
parallel-group
trial to determine the efficacy and safety of IPC associatedwith
GCS versus GCS alone for the prevention of VTE inICU patients with
a high risk of bleeding.
Materials and methods
Trial design
CIREA 1 (Compression pneumatique Intermittente enREAnimation)
was a multicenter, open-label, random-ized, outcome-blinded trial
conducted at nine ICUs inFrance (see Appendix). The trial protocol
was approvedby the local institutional review board. The
sponsorplayed no role in the analysis or drafting of
themanuscript.
Study population
Patients aged 18 years or older who were at high risk ofbleeding
on ICU admission were eligible for the trial. Ahigh risk of
bleeding was defined as symptomatic bleed-ing or the presence of
organic lesions likely to bleed,hemophilic diseases, hemostatic
abnormalities (plateletcount\50,000/mm3, aPTT ratio[2, prothrombin
time\40 %), or the presence of severe anemia (hemoglobin\7 g/dl)
due to bleeding or unexplained. Prolongedclotting times can be the
result of the use of anticoagu-lants. These parameters alone when
not associated withbleeding or a high risk of bleeding could not be
consid-
ered as inclusion criteria. Other requirements forinclusion were
a willingness to participate for the durationof the trial, and the
provision of written informed consentgiven by the patients next of
kin.
Exclusion criteria were patient refusal, the absence ofa high
risk of bleeding as previously defined, the presenceof a documented
VTE at screening or a recent DVT(\3 months), ICU stay of more than
36 h or likely to be\72 h, a life-support limitation, a
contraindication formechanical prophylaxis (i.e., severe lower
limb
873
-
7/29/2019 Compresor intermitente TVP
3/9
arteriopathy, any arterial graft of the legs, a wound in
thelower limb related to either vascular disease or trauma),and the
presence of a mechanical prosthetic heart valve.
Study procedures
Patients were randomly assigned at ratio of 1:1 to receiveeither
IPC associated with GCS or GCS alone. The ran-domization was
centralized with internet access (Clininfo,Lyon, France), and
stratified by center and age group(1850 years, 5170 years, and[70
years).
GCS consisted of thigh-length GCS (T.E.D.TM anti-embolism
stockings; Covidien, Mansfield, MA) and IPCwas achieved with the
SCD EXPRESSTM compressionsystem with adapted tubing sets and thigh
sleeves (Co-vidien). Nurses were trained in the use of
mechanicaldevices to apply optimal compression (proper sizing
ofboth GCS and sleeves for IPC, and their proper applica-tion). GCS
and IPC were applied to both legs as soon aspossible after
randomization and maintained continuouslyuntil compression
ultrasonography (CUS) was performedon day 6. After that day, the
decision to maintain VTEprophylaxis and its modality were left at
the discretion ofthe investigators. Anticoagulation was not
permittedduring the first 6 days of the study. The use of GCS
andIPC was recorded to monitor compliance and tolerance.Compliance
was considered poor if the mechanicaldevices were used less than 80
% of the time. The GCSand IPC removal date and reasons were
recorded whenapplicable. The use of procoagulant treatments
(pro-thrombin complex concentrate, fresh frozen plasma,platelet
transfusion, vitamin K, coagulation factors, prot-amine sulfate)
between admission and day 6 wasrecorded.
Prior to randomization, CUS was recommended inpatients
transferred to the ICU from another hospital oranother unit after
hospitalization of at least 48 h. Thisbaseline CUS was performed to
exclude prevalent DVT(exclusion criterion). We assumed that
patients admitteddirectly to the ICU for an acute event had no
prevalentDVT but those who were already hospitalized
beforeadmission to the ICU could have developed DVT duringthe first
days of hospitalization.
All included patients were visited on day 6, and sub-sequently
followed up on day 30 and day 90 (visit or
phone call). Patients or their relatives were questionedabout
VTE events after ICU discharge. If a patient died,the date and the
most probable cause of death wererecorded.
Endpoints
The primary endpoint with respect to efficacy was theincidence
of VTE on day 6 assessed by a composite
criterion: (1) symptomatic DVT of a lower limb (objec-tively
confirmed by CUS) or symptomatic, nonfatal andobjectively confirmed
PE, (2) death between day 1 andday 6 related to a PE, and (3)
asymptomatic DVT (eitherdistal or proximal) of a lower limb
detected by CUSsystematically performed on day 6. All reported
symp-
tomatic VTE and all deaths that occurred between day 1and day 6
were judged on the basis of standardized cri-teria by an
independent adjudication committee unawareof the randomized
treatment assignments. Only confirmedVTE and deaths considered as
definitely related to PEwere included in the analysis of the
primary endpoint. TheCUS performed on day 6 by trained
ultrasonographerswas standardized [20] and was done blindly, i.e.,
thepatients had bare legs, and mechanical devices wereremoved and
hidden before the procedure. All examina-tions were videotaped and
sent to the coordination centerfor validation by an expert
ultrasonographer who wasunaware of the treatment group. DVT of the
upper limbwas not considered as a primary endpoint.
Secondaryendpoints were the occurrence of a symptomatic VTEbetween
day 6 and day 90, and death from any cause up today 30 or day
90.
Adverse events were recorded during the use ofmechanical devices
and the tolerability of GCS and IPCwas assessed using a specific
chart.
Statistical analysis
Primary analysis was performed on an intention-to-treatbasis.
Randomized patients who had a documented clin-ical endpoint or a
CUS examination by day 6 wereincluded in the efficacy endpoint
analysis. The incidenceof the composite primary endpoint on day 6
was com-pared between groups using an exact two-sided Fishertest.
Relative risk and absolute risk reduction were com-puted with their
95 % confidence intervals.
Assuming an incidence of VTE of 15 % in the GCSgroup [6, 19], we
calculated that 356 patients wererequired for the study to detect a
60 % reduction in theincidence of VTE with the combination IPC ?
GCS, witha power of 80 % and a two-sided alpha level of 5 %.Because
approximately 20 % of patients were expected todie during the first
days of their ICU stay, we decided toenroll 400 patients.
Results
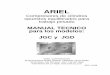
Between 21 November 2007 and 20 December 2010 atotal of 407
patients underwent randomization in the CI-REA1 study, 205 in the
IPC ? GCS group and 202 in theGCS group (Fig. 1). The systematic
CUS was performed5.8 1.6 days after ICU admission in the IPC ?
GCS
874
-
7/29/2019 Compresor intermitente TVP
4/9
group and after 6.0 1.4 days in the GCS group. Threepatients in
the GCS group and one in the IPC ? GCSgroup received at least one
dose of curative anticoagulanttreatment before the CUS evaluation
for symptomaticDVT of an upper limb (n = 2), atrial fibrillation (n
= 1)and unspecified reason (n = 1). Six patients in the GCS
group and one in the IPC?
GCS group received at leastone dose of preventive
anticoagulation treatment beforethe CUS evaluation.
Baseline characteristics were well balanced betweenthe two
groups (Table 1). About half of the patients had aspontaneous or
traumatic intracranial hemorrhage. In 29patients (7.1 %),
anticoagulant treatment was adminis-tered at a therapeutic dose
before ICU admission (atrialfibrillation in 16, previous VTE[3
months in 7, throm-bolysis for myocardial infarction in 2,
antiphospholipidsyndrome in 1, coronary disease in 1 and unknown
reason
in 2) and 29 patients (7.1 %) received thromboprophy-laxis,
mainly mechanical thromboprophylaxis with GCS.More than 70 % of the
patients had a central venouscatheter at inclusion, but less than
10 % in the femoralsite. Nearly 30 % of patients had had recent
surgerywhich was predominantly related to the reason for ICU
admission. Mean biological values were within normalranges
(Table 1). In 96 of 341 patients for whom theinformation was
available, procoagulant treatment wasadministered between admission
and day 6, 42 in theIPC ? GCS group and 54 in the GCS group (p =
0.12).
By day 6, no death was considered by the adjudicationcommittee
as due to fatal PE. PE occurred in one patientin the GCS group. No
symptomatic DVT was observed.The systematic CUS detected 18 distal
DVT and 8proximal DVT. The incidence of the primary endpointwas 5.6
% (10 of 179 patients) in the IPC ? GCS group
IPC + GCS
(n = 205)
GCS
(n = 202)
Randomized patients
(n = 407)
Evaluable for efficacy
endpoint at day 6
( n= 179)
Evaluable for efficacy
endpoint at day 6
(n = 184)
Excluded n = 1
Nonevaluable for
ultrasonography at day6 n = 25
- Death n = 21
- Transfer to another site before
ultrasonography n = 3
- Withdrawal of consent n = 1
Nonevaluable for
ultrasonography at
day6 n = 18- Death n = 17
- Transfer to another site
before ultrasonography n = 1
Followed-up until day 30(n= 142)
Death n = 40
Followed-up until day 90
(n = 133)
Death n = 8
Lost to follow-up n = 1
Followed-up until day 30(n= 144)
Death n = 41
Followed-up until day 90
(n = 133)
Death n = 10
Lost to follow-up n = 1
Screened patients
(n = 954)Non included n = 547- Admission > 36 hours n =
107
- Expected stay < 72 hours n = 141
- Contraindication to GCS and/or IPC n =55
- Life support limitation n = 156
- Refusal n = 53
- Mechanical heart valve n= 14
- Logistical reason n= 13
Fig. 1 Flow of patientsthrough the trial
875
-
7/29/2019 Compresor intermitente TVP
5/9
and 9.2 % (17 of 184 patients) in the GCS group, leadingto a
nonsignificant risk reduction of 40.0 % (relative risk,RR, 0.60; 95
% CI 0.281.28; p = 0.19; Table 2).
The incidence of VTE was 10.3 % (3 of 29 patients) inpatients
previously treated with anticoagulant and 6.4 %(24 of 377 patients)
in patients without previous antico-
agulant treatment (p=
0.41). Among the 96 patientstreated with procoagulant treatments
between admissionand day 6, 7 (7.3 %) had VTE on day 6, and among
the245 patients without procoagulant treatment, 18 (7.3 %)had VTE
on day 6 (p = 0.98).
The effect of IPC ? GCS on the primary endpointwas globally
homogeneous among subgroups (Fig. 2).Anticoagulation was resumed
during the ICU stay in
53 % of survivors, after a median delay of 2 days(interquartile
range 027 days) following the day-6CUS.
Between day 6 and day 90, no additional VTEoccurred in the GCS
group but four symptomatic VTEevents occurred in the IPC ? GCS
group (two proximal
DVT, one distal DVT and one PE). The incidence ofsymptomatic VTE
on day 90 was 2.0 % (4/203 patients)in the IPC ? GCS group and 0.5
% (1/202 patients) in theGCS group (RR 4.0; 95 % CI 0.535.3; p =
0.4). Theincidence of all VTE events (symptomatic and
asymp-tomatic) on day 90 was 7.8 % (14/179 patients) in theIPC ?
GCS group and 9.2 % (17/184 patients) in theGCS group (RR 0.9; 95 %
CI 0.41.7; p = 0.63).
Table 1 Baseline characteristics of patients
Characteristics All patients(n = 406)
IPC ? GCS group(n = 204)
GCS group(n = 202)
p value
Age (years), mean SD 55.4 17 56.3 16.5 54.6 17.5 0.32Female
gender, n (%) 137 (33.5 %) 72 (35.3 %) 65 (32.2 %) 0.51BMI (kg/m2),
mean SD 25.5 5.2 25.6 4.9 25.4 5.5 0.72SAPS II score, mean SD 42.7
18.1 41.6 18.3 43.7 17.8 0.24Primary admission diagnostic category,
n (%)Spontaneous intracranial hemorrhage 146 (36.0) 81 (39.7) 65
(32.2) 0.12Traumatic intracranial hemorrhage 87 (21.4) 41 (20.1) 46
(22.8) 0.51Multisystem trauma 44 (10.8) 21 (10.3) 23 (11.4)
0.72Other hemorrhage 40 (9.9) 19 (9.3) 21 (10.4) 0.71Severe sepsis
or septic shock 39 (9.6) 18 (8.8) 21 (10.4) 0.59Acute respiratory
distress syndrome
with biological abnormalities24 (5.9) 14 (6.8) 10 (5.0) 0.41
Other diagnoses 26 (6.4) 10 (4.9) 16 (7.9) 0.22On ICU admission,
n (%)Hospitalization more than 48 h prior
to ICU admission68 (16.7) 35 (17.2) 33 (16.3) 0.83
Therapeutic anticoagulation 29 (7.1) 13 (6.4) 16 (7.9)
0.54Thromboprophylaxis 29 (7.1) 17 (8.3) 12 (5.9) 0.35
At inclusion, n (%)Sepsis 46 (11.3) 20 (9.8) 26 (12.9)
0.33Central venous catheter 295 (72.6) 148 (72.5) 147 (72.8)
0.96Mechanical ventilation 336 (82.8) 169 (82.8) 167 (82.7)
0.96Sedation 317 (78.1) 159 (77.9) 158 (78.2) 0.95
Risk factors for VTE before ICU admission, n (%)Previous VTE 12
(3.0) 5 (2.5) 7 (3.4) 0.55Cancer 52 (12.8) 27 (13.2) 25 (12.4)
0.80Recent surgery or trauma 118 (29.1) 58 (28.4) 60 (29.7)
0.78Pregnancy or post-partum 4 (1.0) 2 (1.0) 2 (1.0) 1.0Estrogen
use 6 (1.5) 2 (1.0) 4 (2.0) 0.45Known thrombophilia 2 (0.5) 2 (1.0)
0 (0) 0.15Plaster cast immobilization 0 (0) 0 (0) 0 (0) Previous
stroke 13 (3.2) 6 (3.0) 7 (3.5) 0.76
Cardiac insufficiency 20 (4.9) 6 (3.0) 14 (6.9) 0.07Respiratory
insufficiency 64 (15.8) 32 (15.7) 32 (15.8) 0.96
Biological dataPlatelet count (G/l), mean SD 187.5 108.0 192.3
109.2 182.7 107.0 0.37Platelet count\50,000/mm3, n (%) 47 (11.6) 22
(10.8) 25 (12.4) 0.62Hemoglobin (g/dl), mean SD 12.3 7.5 11.6 2.4
12.9 10.4 0.08Hemoglobin\7 g/dl, n (%) 12 (3.0) 9 (4.4) 3 (1.5)
0.09aPTT ratio, mean SD 1.16 0.40 1.16 0.50 1.15 0.40 0.96aPTT
ratio[2, n (%) 8 (2.0) 5 (2.5) 3 (1.5) 0.49Prothrombin time (%),
mean SD 71.9 21.1 73.5 20.5 70.2 21.8 0.13Prothrombin time\40 %, n
(%) 42 (10.3) 22 (10.8) 20 (9.9) 0.77Creatinine (lmol/l), mean SD
101.6 104.7 100.6 103.4 102.5 106.2 0.12
876
-
7/29/2019 Compresor intermitente TVP
6/9
Compliance with GCS was poor in eight patients(2.0 %, one in the
GCS group and seven in theIPC ? GCS group). Tolerance of GCS was
poor in 13patients (3.3 %) in both groups with no differencebetween
groups. The reported adverse effects (noneserious) were mild
cutaneous injuries (n = 8) or dis-comfort (sweating, warmth, and
tight GCS).Compliance with IPC was poor in 14 patients (7.0 %)
in the IPC ? GCS group. Tolerance of IPC was poor in12 patients
(6.0 %) and early removal of IPC wasnecessary in seven patients.
The most frequent reasonsfor discontinuation of IPC were
discomfort, noise andrestlessness. No serious adverse event was
reportedwith IPC. By day 6, 15 deaths were related to
fatalhemorrhage with no difference between the groups: 7(3.4 %) in
the IPC ? GCS group and 8 (4 %) in theGCS group (p = 0.78).
Nonfatal major hemorrhage wasobserved in 22 patients: 10 (4.9 %) in
the IPC ? GCSgroup and 12 (5.9 %) in the GCS group (p = 0.65).
Byday 30, 58 patients (29 %) in the GCS group and 61patients (30 %)
in the IPC ? GCS group had died
(p = 0.79). By day 90, 68 patients (34 %) in the GCSgroup and 69
patients (34 %) in the IPC ? GCS grouphad died (p = 0.97).
Discussion
In this first randomized trial specifically designed toevaluate
the potential benefit of two distinct mechanicaldevices in ICU
patients with a high risk of bleeding, wefound no significant
difference in the incidence of VTEbetween those receiving IPC
together with GCS and those
receiving GCS alone.For critically ill patients who are at high
risk ofbleeding, current guidelines recommend the optimal useof
mechanical thromboprophylaxis with GCS and/or IPCto prevent VTE at
least until the bleeding risk decreases[17]. However, little is
known about the efficacy andsafety of mechanical prophylaxis
methods in ICU patients[21]. From a physiological point of view,
the dynamiccompression produced by IPC is assumed to be more
efficient than the static compression produced by theGCS. In
addition, IPC is thought to have a fibrinolyticaction, primarily by
increasing tissue plasminogen acti-vator and decreasing plasminogen
activator inhibitor [22].Despite these theoretical advantages, the
addition of IPCprovided no additional benefit compared to GCS alone
inour ICU patients with a high risk of bleeding. Neverthe-less, the
lack of statistical power of the present study
(54 % when calculated a posteriori) did not allow us
toconfidently rule out a potential beneficial effect of IPC forthe
prevention of VTE in this specific clinical setting.
This low statistical power may be explained by thelow incidence
of VTE observed in the GCS group(9.2 %), when compared to an
expected 15 % rate. In aprevious randomized clinical trial that
evaluatedIPC ? GCS versus GCS alone in patients with intrace-rebral
hemorrhage, we found a 15.9 % incidence of VTEin the GCS group
using systematic CUS on day 10 [19].In the present trial, the
incidence of VTE in a similarpopulation subset (patients with
intracranial hemorrhagein the GCS group, n = 103) was 12.6 %. In an
observa-
tional study performed in 100 medical ICU patients,lower limb
Doppler ultrasonography performed twice-weekly and 1 week after ICU
discharge detected a DVTin 33 % of patients who were receiving a
mechanicalprophylaxis [6]. A prospective study using
twice-weeklyleg ultrasonography identified a proximal DVT in 25
of261 patients (10 %) during their ICU stay [3]. Takentogether,
these results led us to initially expect a 15 %incidence of VTE in
the GCS group, including asymp-tomatic distal and proximal DVT. The
lower incidence ofVTE observed in the control group of the present
studymay be related to a lower risk of thrombosis in criticallyill
patients at high risk of bleeding when compared to that
of the general ICU population.Early CUS evaluation on day 6
presumably con-tributed to the fairly low incidence of observed VTE
inthe present study. In previous trials, VTE endpointswere
generally evaluated on day 10 or later. Never-theless, in studies
that screened regularly for DVT inICU patients, DVT were identified
in the first days ofICU stay. In a study by Hirsch et al., 23 of 33
DVT(70 %) were detected during the first CUS [6].
Table 2 Venous thromboembolic events by day 6
Outcome IPC ? GCS group,n/N (%)
GCS group,n/N (%)
Relative risk 95 % confidence interval p value
Fatal pulmonary embolism 0/204 0/202 Symptomatic pulmonary
embolism 0/204 1/202 Symptomatic deep vein thrombosis 0/204 0/202
Asymptomatic distal deep vein thrombosis 6/179 (3.4) 12/183 (6.6) 0
.51 0.21.33 0.17
Asymptomatic proximal deep vein thrombosis 4/179 (2.2) 4/183
(2.2) 1.02 0.264.03 0.975Primary endpoint on day 6 10/179 (5.6)
17/184 (9.2) 0.60 0.281.28 0.191
877
-
7/29/2019 Compresor intermitente TVP
7/9
Similarly, Cook et al. [3] reported that 50 % of DVTwere
detected before day 8 (median day 8; interquartilerange day 414).
We also chose to perform the CUSevaluation early because in
patients admitted to an ICUwith a high bleeding risk, the American
Collegeof Chest Physicians guidelines recommend that
pharmacological thromboprophylaxis be substituted foror added to
the mechanical thromboprophylaxis as soonas the high bleeding risk
decreases [17]. In the presentstudy, anticoagulation was resumed
during the ICU stayin the majority of the survivors early after the
sys-tematic CUS on day 6.
Fig. 2 Rates of the primaryefficacy outcome on day 6
insubgroups. The primaryefficacy endpoint was acomposite, combining
fatal PE,symptomatic PE, symptomaticDVT, or asymptomatic
DVTdetected by systematic CUS on
day 6. The size of each square isin proportion to the number
ofpatients in the comparison. Noadjustment for multiplecomparisons
was made, sincesubgroup analyses wereperformed for
exploratorypurposes only. BMI is bodyweight in kilograms divided
bythe square of the height inmeters
878
-
7/29/2019 Compresor intermitente TVP
8/9
Since VTE is often silent and clinically unsuspectedin ICU
patients [10, 11], PE is one of the most com-mon unexpected autopsy
findings in this specificpopulation [11]. The recent PROTECT study
showed asignificantly reduced incidence of PE in ICU
patientstreated with dalteparin when compared with the group
treated with unfractionated heparin, but no reduction
inasymptomatic DVT [16]. This result questions thevalidity of
asymptomatic DVT as a surrogate primaryendpoint in prophylaxis
trials in VTE. In the presenttrial, we failed to detect any
intergroup difference inclinically relevant events, such as
symptomatic VTE ordeath.
The compliance with IPC was fairly good in thepresent study. The
high proportion of sedated patients atinclusion (78 %) presumably
accounts for this result.Nevertheless, a few patients without
sedation poorly tol-erated the inflation or the noise of IPC. No
serious adverseevent was related to the use of IPC.
The present trial had substantial limitations. First,
asdiscussed above, the study was underpowered to dem-onstrate a
significant 60 % reduction in incidence in theIPC ? GCS group.
Second, autopsy was not performedfor all fatalities, especially
when death occurred in theICU. This may have led to underestimation
of the PE-related death rate. Third, this study was not blinded,
butday 6 CUS was performed without knowledge of themechanical
device used for VTE prophylaxis andvalidation of CUS was performed
by an expert ultraso-nographer who was unaware of the patients
assignment.
In conclusion, the current trial was not able to showthe
superiority of the combination of IPC ? GCS overGCS alone in
preventing VTE in ICU patients at high riskof bleeding. However, an
additional preventing effect ofIPC cannot be confidently ruled out
based on the results ofthis study which lacked power, mainly
because of a lowincidence of VTE in the control group.
Nevertheless, thisstudy provides the basis for performing new large
clinicaltrials to evaluate mechanical devices to prevent VTE
invarious subsets of ICU patients with a high risk ofbleeding.
Acknowledgments This study was supported by a grant from
theFrench Ministry of Health (PHRCN 2005 no. 08-13).
COVIDIENsupplied the GCS (T.E.D.TM anti-embolism stockings) and the
IPC(SCD EXPRESSTM compression systems with tubing sets and
sleeves). The sponsor had no role in the study. We thank
theresearch coordinator I. Pichon, the members of the CIC-P 0502
andthe CIC-P 0801, the study nurses of the Clinical Research
inIntensive Care and Sepsis Group (CRICS group), the Direction dela
Recherche Clinique et Innovation (DRCI) of Brest UniversityHospital
for their invaluable work, as well as Z. Alavi for herpertinent
advice.
Conflicts of interest The authors state that they have no
conflictof interest.
Appendix
CIREA1 collaborators:Steering Committee: Pr Jean-Luc Diehl, Pr
Philippe
Vignon, Dr Anne Renault, Pr Karine LacutAdjudication Committee:
Pr L. Bressollette (expert
ultrasonographer), Pr Erwan LHerData manager and
Biostatistician: Elise Poulhazan,Emmanuel Nowak
Investigators:Service de Reanimation Polyvalente, CH
dAngouleme,Saint-Michel: Dr Thierry Baudin-Jacquemin, Dr
SylvieNicole Calvat, Dr Arnaud Desachy, Dr Florence Hospital
Service de Reanimation Medicale, CHU de la CavaleBlanche, Brest:
Dr Montaine Lefevre, Dr Jean-MarieTonnelier, Dr Alexandre
Tonnelier
Federation dAnesthesie, Reanimation Urgences,
HIAClermont-Tonnerre, Brest : Dr Christophe Giarcardi,Dr Bruno
Ralec, Dr Mehdi Ould-Ahmed, Dr Didier
Fourel, Dr Ba Vinh N Guyen, Dr Diane Commandeur.Reanimation
Polyvalente, CHU de Limoges, Limoges:Dr Jean-Bernard Amiel, Dr Marc
Clavel, Dr AnthonyDugard, Dr Caroline Etchecopar-Chevreuil, Dr
BrunoFrancois, Dr Nicolas Pichon, Dr Jean-Claude Voultoury.
Service de Reanimation Medicale, CHU Hotel Dieu,Nantes: Dr
Olivier Zambon
Reanimation, CHRHopital de la Source, Orleans:Dr Isabelle Runge,
Dr Christian Fleury, Dr MarieSkarzynski, Dr Dalila
Benzekri-Lefevre, Dr Anne Bre-tagnol, Dr Nicolas Bercault
Reanimation Medicale, HEGP, AP-HP Paris: Dr Em-manuel Guerot, Dr
Ana Novara, Dr Christophe Faisy,Dr Iris Pelieu, Pr Nicolas
Lerolle
Service de Reanimation Medicale, CHU de Poitiers,Poitiers: Pr
Olivier Pourrat, Dr Julien Voultoury, DrMichel Pinsard, Dr Anne
Veinstein, Dr Jean-Pierre Frat,Dr Julie Badin, Pr Rene Robert
Service de Reanimation Medicale, CHU de ToursHopital Bretonneau,
Tours: Dr Annick Legras, Dr Em-manuelle Mercier, Dr Laure
Batias-Moreau, Dr StephaneEhrmann, Dr Stephanie Benardeau, Dr Maud
Jonas,Dr Antoine Guillon, Dr Jennifer Buret, Dr ElodieMasseret
Vascular Ultrasonography Collaborators:Imagerie Medicale, CH
dAngouleme, Saint-Michel:Dr Florence Hospital, Dr Daniele Colin, Dr
Thierry Landois
Radiologie, HIA, Clermont-Tonnerre, Brest : Dr JeanRousset, Dr
Marc Garetier, Dr Diouf, Dr Sandra Chinel-lato, Dr Valentin
Tissot
Unite Vasculaire du service de Chirurgie Thoraciqueet
Cardiovasculaire, CHU de Limoges, Limoges: Pr Phi-lippe Lacroix, Dr
Tiphaine Bonnafy
Service dexplorations vasculaires, CHU Hotel Dieu,Nantes: Dr
Jerome Connault
879
-
7/29/2019 Compresor intermitente TVP
9/9
Angiologie, CHRHopital de la Source, Orleans:Dr Carole Bazzi
Medecine vasculaire et hypertension arterielle,HEGP, AP-HP
Paris: Pr Joseph Emmerich, Dr Emman-uel Messas
Radiologie, Echographie-Doppler, CHU de Poitiers,Poitiers: Dr
Elisabeth Escure, Dr Cecile Thollot, Dr Jer-ome Roumy
Pole imagerie medicale, CHU de ToursHopitalBretonneau, Tours: Dr
Nicole Ferreira, Pr Frederic Patat
References
1. Attia J, Ray JG, Cook DJ, Douketis J,Ginsberg JS, Geerts WH
(2001) Deepvein thrombosis and its prevention incritically ill
adults. Arch Intern Med161:12681279
2. Shorr AF, Williams MD (2009) Venousthromboembolism in
critically illpatients. Observations from arandomized trial in
sepsis. ThrombHaemost 101:139144
3. Cook D, Crowther M, Meade M,Rabbat C, Griffith L, Schiff D,
Geerts
W, Guyatt G (2005) Deep venousthrombosis in
medical-surgicalcritically ill patients: prevalence,incidence, and
risk factors. Crit CareMed 33:15651571
4. Cook D, Douketis J, Meade M, GuyattG, Zytaruk N, Granton J,
Skrobik Y,Albert M, Fowler R, Hebert P,Pagliarello G, Friedrich J,
Freitag A,Karachi T, Rabbat C, Heels-Ansdell D,Geerts W, Crowther
M; CanadianCritical Care Trials Group (2008)Venous thromboembolism
and bleedingin critically ill patients with severe
renalinsufficiency receiving dalteparinthromboprophylaxis:
prevalence,
incidence and risk factors. Crit Care12:R32
5. Geerts WH, Heit JA, Clagett GP, PineoGF, Colwell CW, Anderson
FA Jr,Wheeler HB (2001) Prevention ofvenous thromboembolism.
Chest119:132S175S
6. Hirsch DR, Ingenito EP, Goldhaber SZ(1995) Prevalence of deep
venousthrombosis among patients in medicalintensive care. JAMA
274:335337
7. McKelvie PA (1994) Autopsy evidenceof pulmonary
thromboembolism. Med JAust 160:127128
8. Moser KM, Fedullo PF, LitteJohn JK,Crawford R (1994)
Frequent
asymptomatic pulmonary embolism inpatients with deep venous
thrombosis.JAMA 271:223225
9. Stein PD, Henry JW (1995) Prevalenceof acute pulmonary
embolism amongpatients in a general hospital and atautopsy. Chest
108:978981
10. Karwinski B, Svendsen E (1989)Comparison of clinical and
postmortemdiagnosis of pulmonary embolism.J Clin Pathol
42:135139
11. Twigg SJ, McCrirrick A, Sanderson PM(2001) A comparison of
post mortemfindings with post hoc estimated clinicaldiagnoses of
patients who die in a
United Kingdom intensive care unit.Intensive Care Med
27:706710
12. Blosser SA, Zimmerman HE, StaufferJL (1998) Do autopsies of
critically illpatients reveal important findings thatwere
clinically undetected? Crit CareMed 26:13321336
13. Mort TC, Yeston NS (1999) Therelationship of pre-mortem
diagnosesand post-mortem findings in a surgicalintensive care unit.
Crit Care Med27:299303
14. Cade JF (1982) High risk of thecritically ill for
venousthromboembolism. Crit Care Med10:448450
15. Fraisse F, Holzapfel L, Couland JM,Simonneau G, Bedock B,
Feissel M,Herbecq P, Pordes R, Poussel JF, RouxL (2000) Nadroparin
in the preventionof deep vein thrombosis in acutedecompensated
COPD. Am J RespirCrit Care Med 161:11091114
16. PROTECT Investigators for theCanadian Critical Care Trials
Groupand the Australian and New ZealandIntensive Care Society
Clinical TrialsGroup, Cook D, Meade M, Guyatt G,Walter S,
Heels-Ansdell D, WarkentinTE, Zytaruk N, Crowther M, Geerts
W,Cooper DJ, Vallance S, Qushmaq I,Rocha M, Berwanger O, Vlahakis
NE
(2011) Dalteparin versus unfractionatedheparin in critically ill
patients. N EnglJ Med 364:13051314
17. Kahn SR, Lim W, Dunn AS, CushmanM, Dentali F, Akl EA, Cook
DJ,Balekian AA,Klein RC,Le H, SchulmanS, Murad MH; American College
ofChest Physicians (2012) Prevention ofVTE in nonsurgical
patients:Antithrombotic Therapy and Preventionof Thrombosis, 9th
ed: AmericanCollege of Chest Physicians Evidence-Based Clinical
Practice Guidelines.Chest 141(2 Suppl):e195Se226S
18. Turpie AGG, Hirsh J, Gent M, Julian D,
Johnson J (1989) Prevention of deepvein thrombosis in
potentialneurosurgical patients. A randomizedtrial comparing
graduated compressionstockings alone or graduatedcompression
stockings plus intermittentpneumatic compression with control.Arch
Intern Med 149:679681
19. Lacut K, Bressollette L, Le Gal G,Etienne E, De Tinteniac A,
Renault A,Rouhart F, Besson G, Garcia JF,Mottier D, Oger E,
VICTORIAh(Venous Intermittent Compression andThrombosis Occurrence
Related toIntra-cerebral Acute hemorrhage)Investigators (2005)
Prevention of
venous thrombosis in patients withacute intra-cerebral
hemorrhage.Neurology 65:865869
20. Goodacre S, Sampson F, Thomas S, vanBeek E, Sutton A (2005)
Systematicreview and meta-analysis of thediagnostic accuracy of
ultrasonographyfor deep vein thrombosis. BMC MedImaging 5:6
21. Limpus A, Chaboyer W, McDonald E,Thalib L (2006)
Mechanicalthromboprophylaxis in critically illpatients: a
systematic review and meta-analysis. Am J Crit Care 15:402410
22. Jacobs DG, Piotrowski JJ,Hoppensteadt DA, Salvator AE,
Fareed
J (1996) Hemodynamic and fibrinolyticconsequences of
intermittent pneumaticcompression: preliminary results.J Trauma
40:710716
880