Embed Size (px)
Citation preview
✓ Completed Adoption Social History for Adoption Packet
✓ Completed Family Division Notice of Right to Employ Counsel form signed by both petitioner and
custodial parent
✓ Completed PCA 347 (Petitioner's Verified Accounting) signed by both petitioner/s
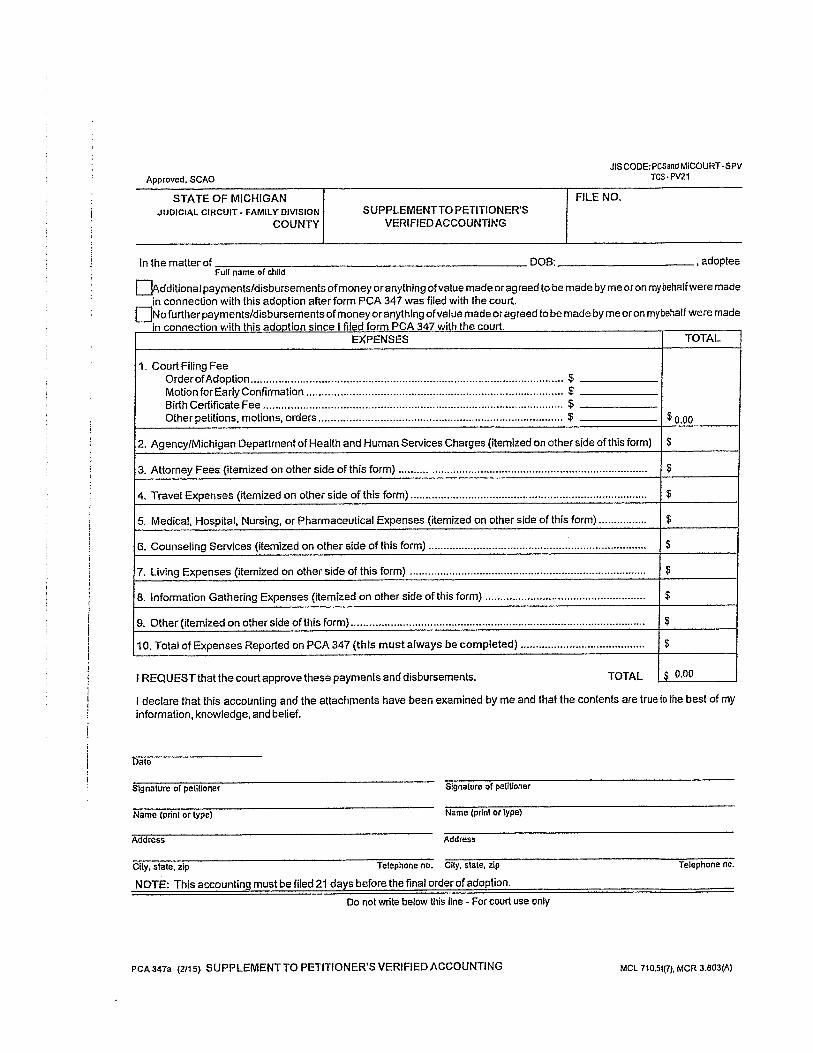
o If you incur additional costs after filing the above document you must file a PCA 347a
(Supplement to Petitioner's Verified Accounting)
✓ Completed Adoption Report Required to Establish a New Michigan Birth Record
o A minimum of $50.00 fee (depending on how many you order) for a new birth certificate
will be required when adoption is finalized and a check made out to the State of Michigan
may be given to the court after the adoption is finalized
✓ Completed Infant/Child Medical Report
✓ Completed Adult Medical Report for petitioner/s
✓ Total filing fee of $185.00 due at time of filing per petition
o $150.00 Filing Fee
o $25.00 Electronic Filing Fee
o $10.00 Certified Copy Fee
Four General Phases of an Adoption Case
l. Acceptance and Processing of Adoption Petition - upon receipt of your adoption petition, a court
clerk will review the documentation and will either accept the petition and add the case (creating a
case number for the adoption) or return the necessary materials that need to be fixed back to you. A
$185.00 filing fee is due at the time the petition is received. This charge includes a Certified Copy of
the adoption order after the finalization of the adoption.
2. Completion of the Home Investigation - after your petition for adoption is properly filed the court
clerk will turn over all necessary documents to the Adoption Investigator who will make contact with
you. An appointment will be made for the Adoption Investigator to visit your home and family to
make sure that the adoption would be in the best interests of the child. The Adoption Investigator
will make a written report for the judge with recommendations regarding the approval of the
adoption.
3. Termination of Parental Rights - after you have received a favorable recommendation from the
Adoption Investigator for the adoption to proceed the parental rights of the parent must be
terminated. For relative adoptions both biological parents must have their parental rights terminated
or consent to the adoption. Once the court terminates the parental rights of the non-custodial parent
and advises them of their rights the non-custodial parent has 63 days to appeal, or ask the judge to
reconsider his/her termination of parental rights. The judge may uphold his decision to terminate or
reinstate the non-custodial parent's parental rights based on information provided for each case. If
the adoptee is 14 years old or over he/she must also consent to the adoption. Please review the
following:
a. When the biological parents agree to the adoption
2
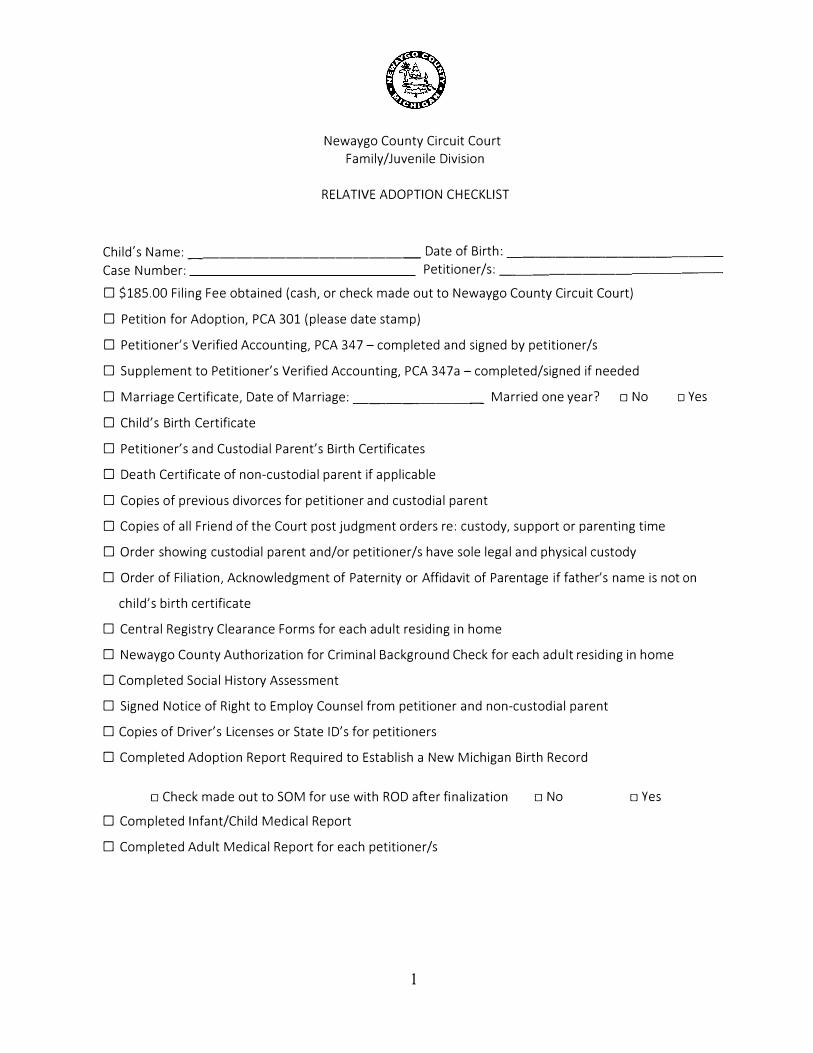
Newaygo County Circuit Court
Family/Juvenile Division
RELATIVE ADOPTION CHECKLIST
Child's Name: ______________ Date of Birth: ____________ _
Case Number: Petitioner/s: _____________ _
D $185.00 Filing Fee obtained (cash, or check made out to Newaygo County Circuit Court)
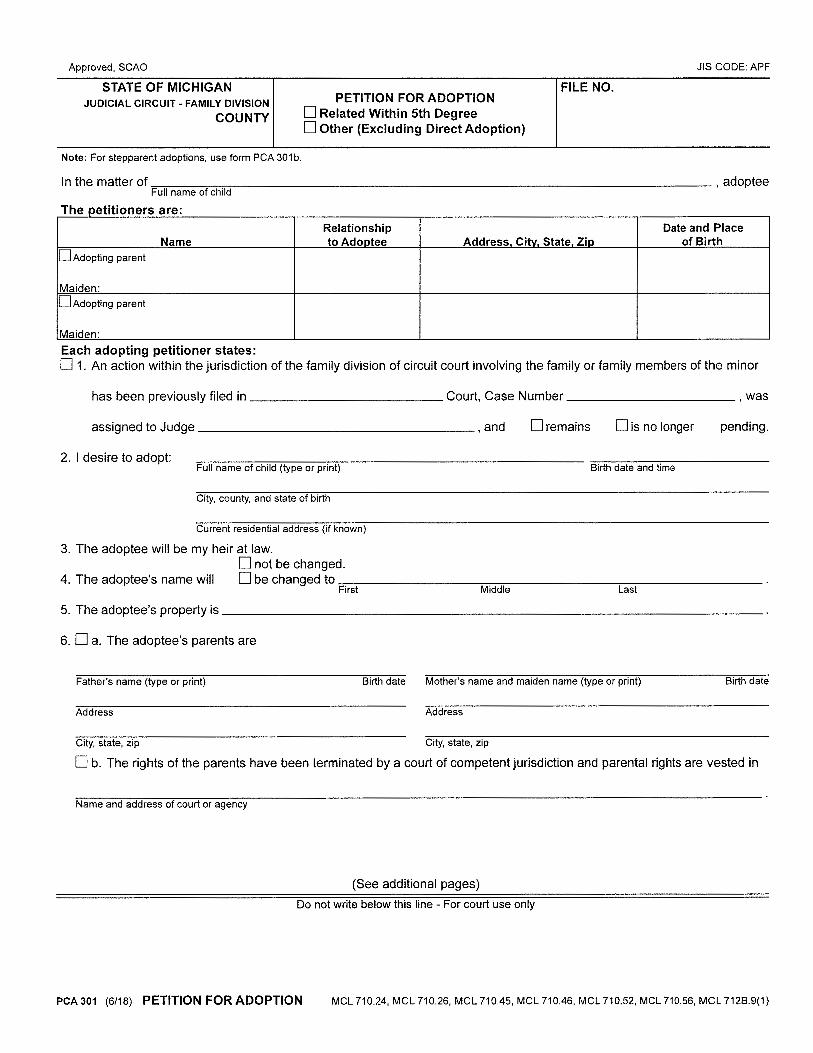
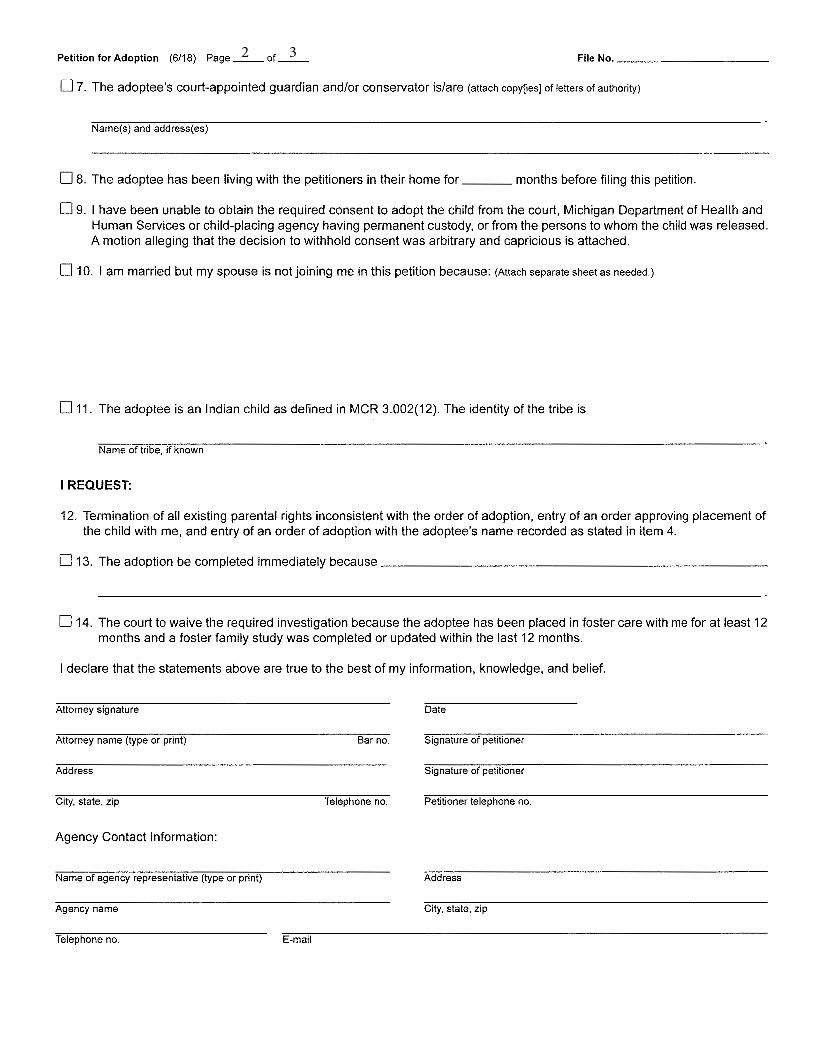
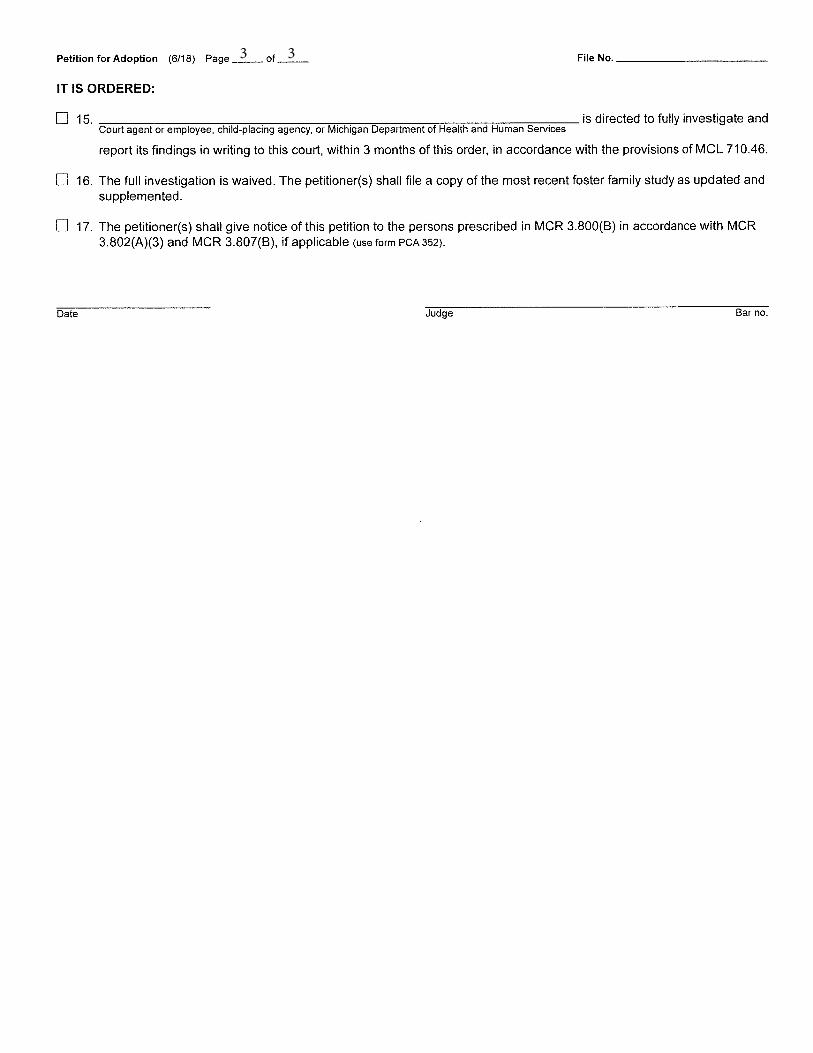
D Petition for Adoption, PCA 301 (please date stamp)
D Petitioner's Verified Accounting, PCA 347- completed and signed by petitioner/s
D Supplement to Petitioner's Verified Accounting, PCA 347a - completed/signed if needed
D Marriage Certificate, Date of Marriage: ________ Married one year? □ No
D Child's Birth Certificate
D Petitioner's and Custodial Parent's Birth Certificates
D Death Certificate of non-custodial parent if applicable
D Copies of previous divorces for petitioner and custodial parent
D Copies of all Friend of the Court post judgment orders re: custody, support or parenting time
D Order showing custodial parent and/or petitioner/s have sole legal and physical custody
□ Yes
D Order of Filiation, Acknowledgment of Paternity or Affidavit of Parentage if father's name is not on
child's birth certificate
D Central Registry Clearance Forms for each adult residing in home
D Newaygo County Authorization for Criminal Background Check for each adult residing in home
D Completed Social History Assessment
D Signed Notice of Right to Employ Counsel from petitioner and non-custodial parent
D Copies of Driver's Licenses or State !D's for petitioners
D Completed Adoption Report Required to Establish a New Michigan Birth Record
□ Check made out to SOM for use with ROD after finalization
D Completed Infant/Child Medical Report
D Completed Adult Medical Report for each petitioner/s
1
□ No □ Yes
2 3
3 3
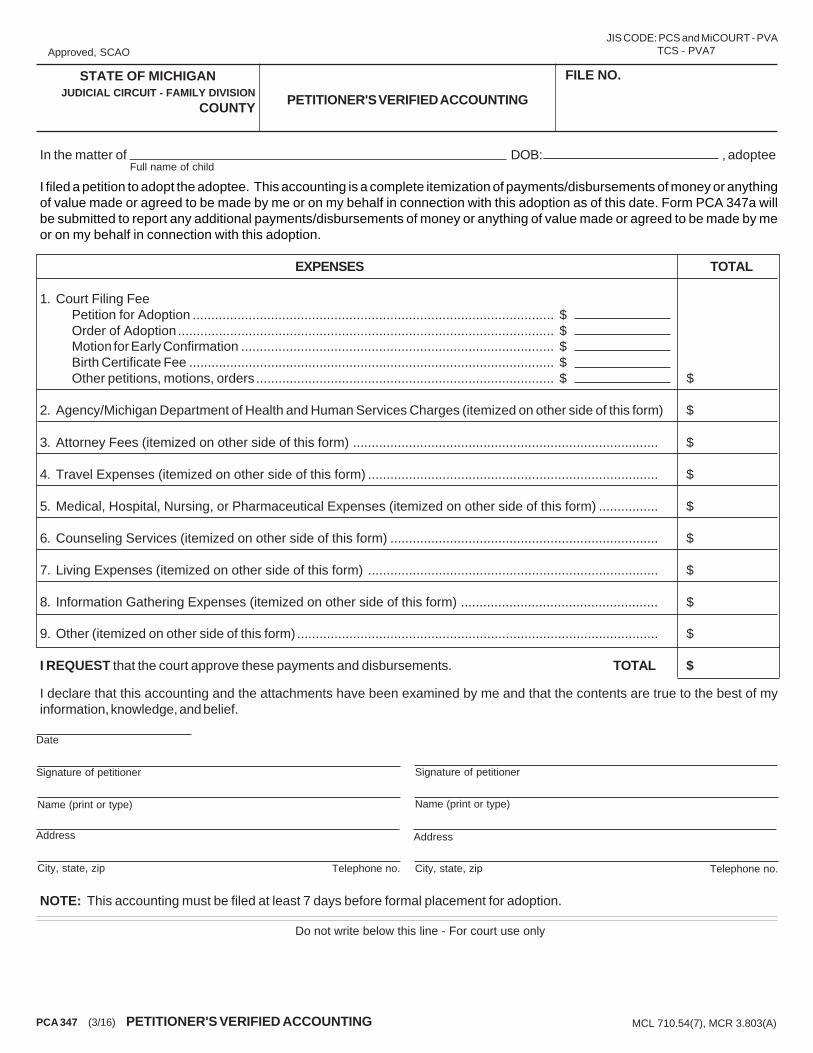
In the matter of DOB: , adoptee
I filed a petition to adopt the adoptee. This accounting is a complete itemization of payments/disbursements of money or anythingof value made or agreed to be made by me or on my behalf in connection with this adoption as of this date. Form PCA 347a willbe submitted to report any additional payments/disbursements of money or anything of value made or agreed to be made by meor on my behalf in connection with this adoption.
EXPENSES TOTAL
1. Court Filing FeePetition for Adoption ................................................................................................. $Order of Adoption ..................................................................................................... $Motion for Early Confirmation .................................................................................... $Birth Certificate Fee .................................................................................................. $Other petitions, motions, orders ................................................................................ $ $
2. Agency/Michigan Department of Health and Human Services Charges (itemized on other side of this form) $
3. Attorney Fees (itemized on other side of this form) .................................................................................. $
4. Travel Expenses (itemized on other side of this form) .............................................................................. $
5. Medical, Hospital, Nursing, or Pharmaceutical Expenses (itemized on other side of this form) ................ $
6. Counseling Services (itemized on other side of this form) ........................................................................ $
7. Living Expenses (itemized on other side of this form) .............................................................................. $
8. Information Gathering Expenses (itemized on other side of this form) ..................................................... $
9. Other (itemized on other side of this form) ................................................................................................. $
I REQUEST that the court approve these payments and disbursements. TOTAL $
I declare that this accounting and the attachments have been examined by me and that the contents are true to the best of myinformation, knowledge, and belief.
NOTE: This accounting must be filed at least 7 days before formal placement for adoption.
Approved, SCAO
FILE NO.
PCA 347 (3/16) PETITIONER'S VERIFIED ACCOUNTING
Full name of child
MCL 710.54(7), MCR 3.803(A)
PETITIONER'S VERIFIED ACCOUNTING
Telephone no.
Date
Telephone no.
Do not write below this line - For court use only
STATE OF MICHIGANJUDICIAL CIRCUIT - FAMILY DIVISION
COUNTY
Address
City, state, zip
Name (print or type)
Signature of petitioner
Address
City, state, zip
Name (print or type)
Signature of petitioner
JIS CODE: PCS and MiCOURT - PVA TCS - PVA7
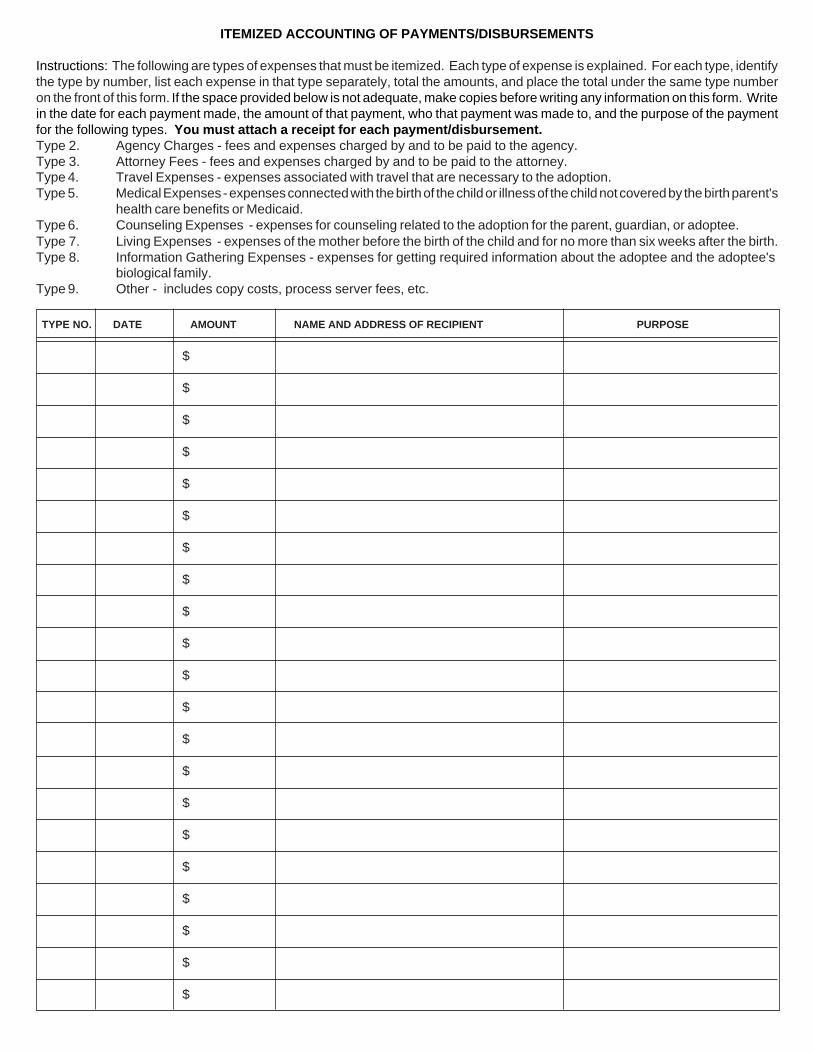
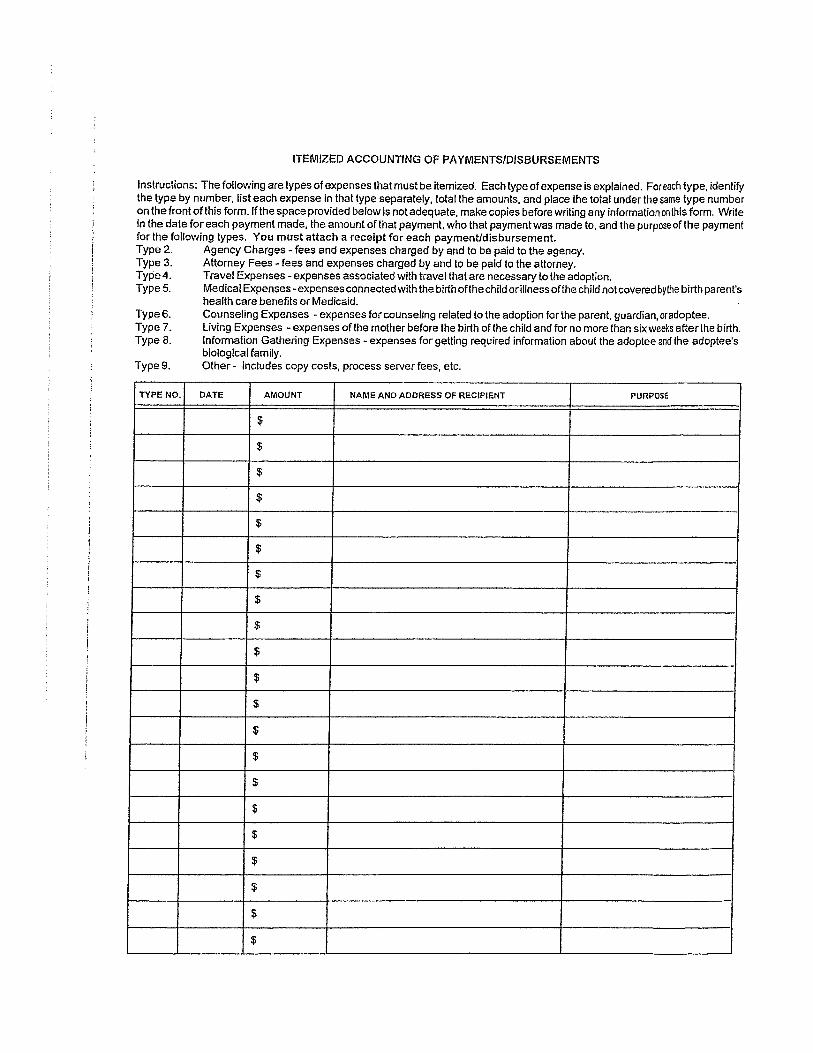
ITEMIZED ACCOUNTING OF PAYMENTS/DISBURSEMENTS
Instructions: The following are types of expenses that must be itemized. Each type of expense is explained. For each type, identifythe type by number, list each expense in that type separately, total the amounts, and place the total under the same type numberon the front of this form. If the space provided below is not adequate, make copies before writing any information on this form. Writein the date for each payment made, the amount of that payment, who that payment was made to, and the purpose of the paymentfor the following types. You must attach a receipt for each payment/disbursement.Type 2. Agency Charges - fees and expenses charged by and to be paid to the agency.Type 3. Attorney Fees - fees and expenses charged by and to be paid to the attorney.Type 4. Travel Expenses - expenses associated with travel that are necessary to the adoption.Type 5. Medical Expenses - expenses connected with the birth of the child or illness of the child not covered by the birth parent's
health care benefits or Medicaid.Type 6. Counseling Expenses - expenses for counseling related to the adoption for the parent, guardian, or adoptee.Type 7. Living Expenses - expenses of the mother before the birth of the child and for no more than six weeks after the birth.Type 8. Information Gathering Expenses - expenses for getting required information about the adoptee and the adoptee's
biological family.Type 9. Other - includes copy costs, process server fees, etc.
TYPE NO. DATE AMOUNT NAME AND ADDRESS OF RECIPIENT PURPOSE
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
DHS-1929 (Rev. 4-21) Previous edition obsolete. 1
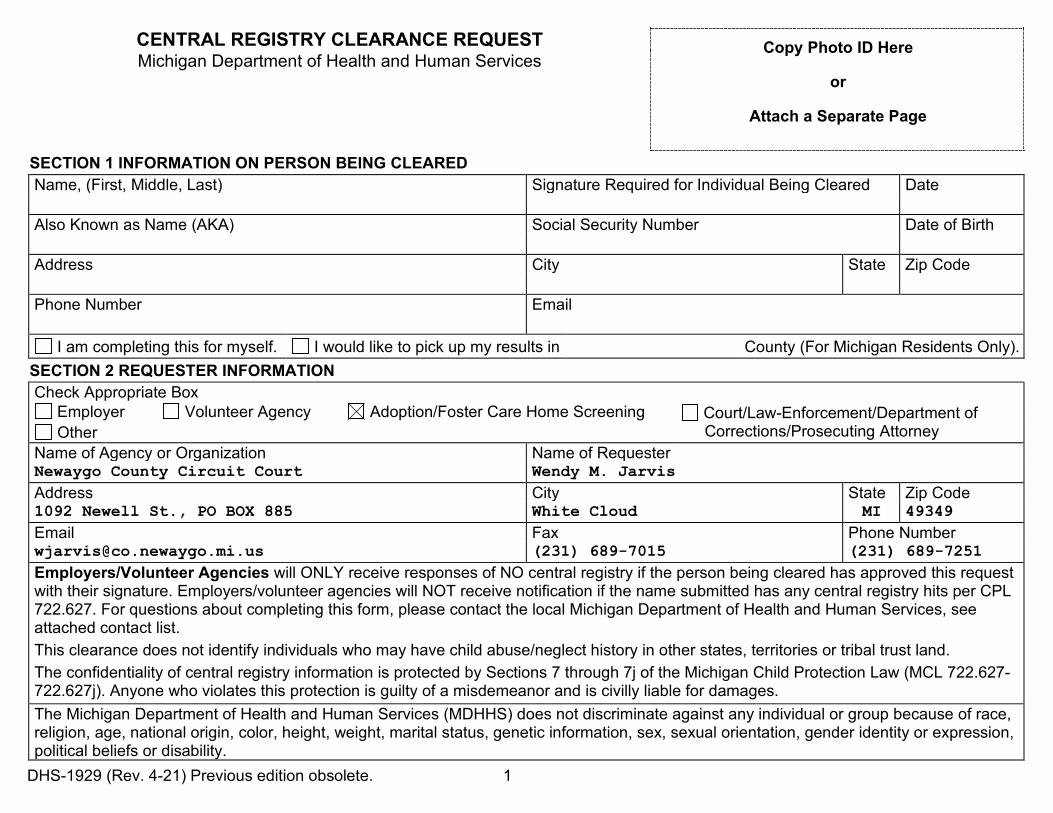
CENTRAL REGISTRY CLEARANCE REQUEST Copy Photo ID Here
or
Attach a Separate Page
Michigan Department of Health and Human Services
SECTION 1 INFORMATION ON PERSON BEING CLEARED Name, (First, Middle, Last) Signature Required for Individual Being Cleared Date Also Known as Name (AKA) Social Security Number Date of Birth Address City State Zip Code Phone Number Email
I am completing this for myself. I would like to pick up my results in County (For Michigan Residents Only). SECTION 2 REQUESTER INFORMATION Check Appropriate Box
Employer Volunteer Agency Adoption/Foster Care Home Screening Court/Law-Enforcement/Department of Corrections/Prosecuting Attorney Other
Name of Agency or Organization Name of Requester Newaygo County Circuit Court Wendy M. Jarvis Address City State Zip Code 1092 Newell St., PO BOX 885 White Cloud MI 49349 Email Fax Phone Number [email protected] (231) 689-7015 (231) 689-7251 Employers/Volunteer Agencies will ONLY receive responses of NO central registry if the person being cleared has approved this request with their signature. Employers/volunteer agencies will NOT receive notification if the name submitted has any central registry hits per CPL 722.627. For questions about completing this form, please contact the local Michigan Department of Health and Human Services, see attached contact list. This clearance does not identify individuals who may have child abuse/neglect history in other states, territories or tribal trust land. The confidentiality of central registry information is protected by Sections 7 through 7j of the Michigan Child Protection Law (MCL 722.627-722.627j). Anyone who violates this protection is guilty of a misdemeanor and is civilly liable for damages. The Michigan Department of Health and Human Services (MDHHS) does not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, genetic information, sex, sexual orientation, gender identity or expression, political beliefs or disability.
DHS-1929 (Rev. 4-21) Previous edition obsolete. 2
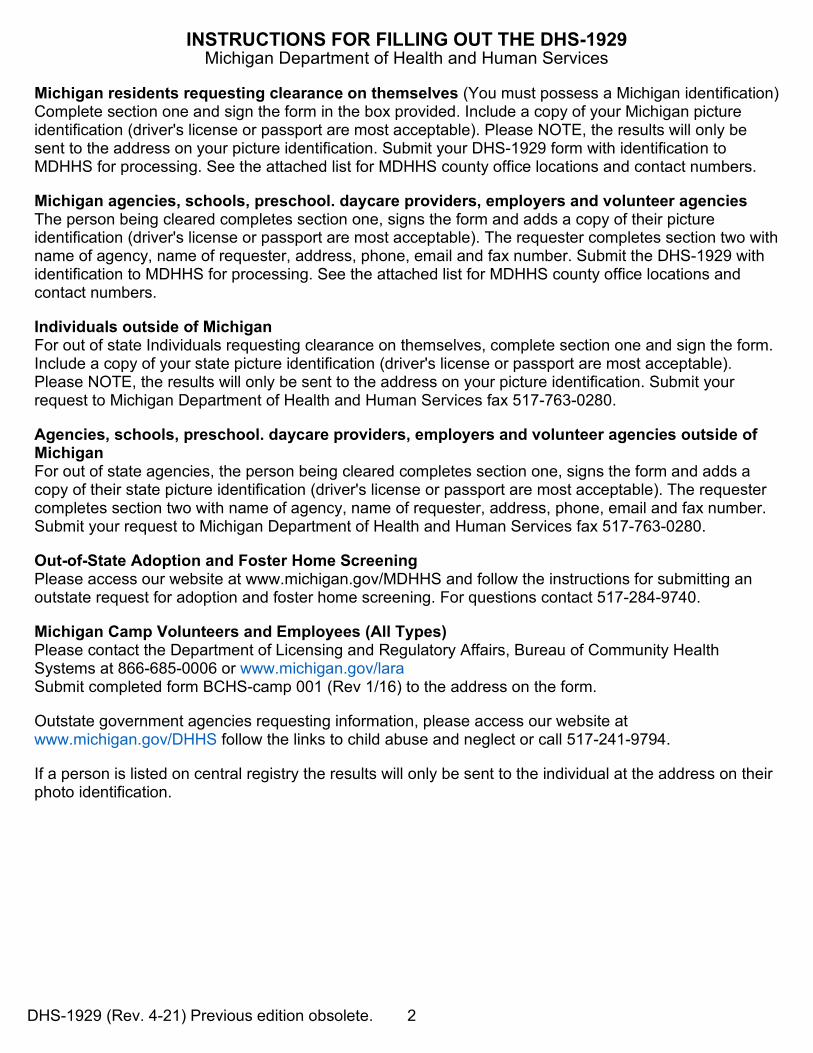
INSTRUCTIONS FOR FILLING OUT THE DHS-1929 Michigan Department of Health and Human Services
Michigan residents requesting clearance on themselves (You must possess a Michigan identification) Complete section one and sign the form in the box provided. Include a copy of your Michigan picture identification (driver's license or passport are most acceptable). Please NOTE, the results will only be sent to the address on your picture identification. Submit your DHS-1929 form with identification to MDHHS for processing. See the attached list for MDHHS county office locations and contact numbers.
Michigan agencies, schools, preschool. daycare providers, employers and volunteer agencies The person being cleared completes section one, signs the form and adds a copy of their picture identification (driver's license or passport are most acceptable). The requester completes section two with name of agency, name of requester, address, phone, email and fax number. Submit the DHS-1929 with identification to MDHHS for processing. See the attached list for MDHHS county office locations and contact numbers.
Individuals outside of Michigan For out of state Individuals requesting clearance on themselves, complete section one and sign the form. Include a copy of your state picture identification (driver's license or passport are most acceptable). Please NOTE, the results will only be sent to the address on your picture identification. Submit your request to Michigan Department of Health and Human Services fax 517-763-0280.
Agencies, schools, preschool. daycare providers, employers and volunteer agencies outside of Michigan For out of state agencies, the person being cleared completes section one, signs the form and adds a copy of their state picture identification (driver's license or passport are most acceptable). The requester completes section two with name of agency, name of requester, address, phone, email and fax number. Submit your request to Michigan Department of Health and Human Services fax 517-763-0280.
Out-of-State Adoption and Foster Home Screening Please access our website at www.michigan.gov/MDHHS and follow the instructions for submitting an outstate request for adoption and foster home screening. For questions contact 517-284-9740.
Michigan Camp Volunteers and Employees (All Types) Please contact the Department of Licensing and Regulatory Affairs, Bureau of Community Health Systems at 866-685-0006 or www.michigan.gov/lara Submit completed form BCHS-camp 001 (Rev 1/16) to the address on the form.
Outstate government agencies requesting information, please access our website at www.michigan.gov/DHHS follow the links to child abuse and neglect or call 517-241-9794.
If a person is listed on central registry the results will only be sent to the individual at the address on their photo identification.
DHS-1929 (Rev. 4-21) Previous edition obsolete. 1
CENTRAL REGISTRY CLEARANCE REQUEST Copy Photo ID Here
or
Attach a Separate Page
Michigan Department of Health and Human Services
SECTION 1 INFORMATION ON PERSON BEING CLEARED Name, (First, Middle, Last) Signature Required for Individual Being Cleared Date Also Known as Name (AKA) Social Security Number Date of Birth Address City State Zip Code Phone Number Email
I am completing this for myself. I would like to pick up my results in County (For Michigan Residents Only). SECTION 2 REQUESTER INFORMATION Check Appropriate Box
Employer Volunteer Agency Adoption/Foster Care Home Screening Court/Law-Enforcement/Department of Corrections/Prosecuting Attorney Other
Name of Agency or Organization Name of Requester Newaygo County Circuit Court Wendy M. Jarvis Address City State Zip Code 1092 Newell St., PO BOX 885 White Cloud MI 49349 Email Fax Phone Number [email protected] (231) 689-7015 (231) 689-7251 Employers/Volunteer Agencies will ONLY receive responses of NO central registry if the person being cleared has approved this request with their signature. Employers/volunteer agencies will NOT receive notification if the name submitted has any central registry hits per CPL 722.627. For questions about completing this form, please contact the local Michigan Department of Health and Human Services, see attached contact list. This clearance does not identify individuals who may have child abuse/neglect history in other states, territories or tribal trust land. The confidentiality of central registry information is protected by Sections 7 through 7j of the Michigan Child Protection Law (MCL 722.627-722.627j). Anyone who violates this protection is guilty of a misdemeanor and is civilly liable for damages. The Michigan Department of Health and Human Services (MDHHS) does not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, genetic information, sex, sexual orientation, gender identity or expression, political beliefs or disability.
DHS-1929 (Rev. 4-21) Previous edition obsolete. 2
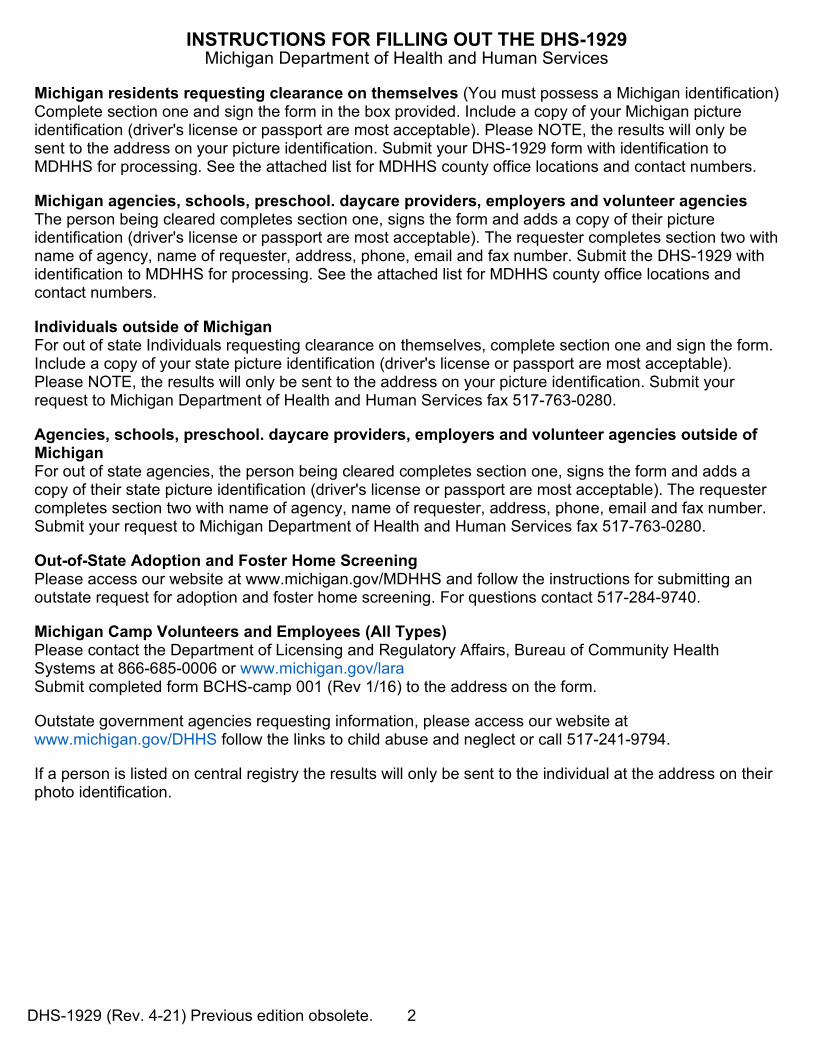
INSTRUCTIONS FOR FILLING OUT THE DHS-1929 Michigan Department of Health and Human Services
Michigan residents requesting clearance on themselves (You must possess a Michigan identification) Complete section one and sign the form in the box provided. Include a copy of your Michigan picture identification (driver's license or passport are most acceptable). Please NOTE, the results will only be sent to the address on your picture identification. Submit your DHS-1929 form with identification to MDHHS for processing. See the attached list for MDHHS county office locations and contact numbers.
Michigan agencies, schools, preschool. daycare providers, employers and volunteer agencies The person being cleared completes section one, signs the form and adds a copy of their picture identification (driver's license or passport are most acceptable). The requester completes section two with name of agency, name of requester, address, phone, email and fax number. Submit the DHS-1929 with identification to MDHHS for processing. See the attached list for MDHHS county office locations and contact numbers.
Individuals outside of Michigan For out of state Individuals requesting clearance on themselves, complete section one and sign the form. Include a copy of your state picture identification (driver's license or passport are most acceptable). Please NOTE, the results will only be sent to the address on your picture identification. Submit your request to Michigan Department of Health and Human Services fax 517-763-0280.
Agencies, schools, preschool. daycare providers, employers and volunteer agencies outside of Michigan For out of state agencies, the person being cleared completes section one, signs the form and adds a copy of their state picture identification (driver's license or passport are most acceptable). The requester completes section two with name of agency, name of requester, address, phone, email and fax number. Submit your request to Michigan Department of Health and Human Services fax 517-763-0280.
Out-of-State Adoption and Foster Home Screening Please access our website at www.michigan.gov/MDHHS and follow the instructions for submitting an outstate request for adoption and foster home screening. For questions contact 517-284-9740.
Michigan Camp Volunteers and Employees (All Types) Please contact the Department of Licensing and Regulatory Affairs, Bureau of Community Health Systems at 866-685-0006 or www.michigan.gov/lara Submit completed form BCHS-camp 001 (Rev 1/16) to the address on the form.
Outstate government agencies requesting information, please access our website at www.michigan.gov/DHHS follow the links to child abuse and neglect or call 517-241-9794.
If a person is listed on central registry the results will only be sent to the individual at the address on their photo identification.