Embed Size (px)
Citation preview

Comparison of the Predictive Value of Exercise-Induced ST Depression Versus Exercise Technetium-99m Sestamibi Single-Photon Emission Computed
Tomographic Imaging for Detection of Coronary ArteryDisease in Patients With Left Ventricular Hypertrophy
Dharmesh Patel, MD, MBBS, Timir S. Baman, MD, and George A. Beller, MD
Scant knowledge exists regarding the significance ofeither additional ST depression in the presence ofbaseline depression or new stress-induced ST depres-sion in patients with left ventricular (LV) hypertrophy.Accordingly, the purpose of this investigation is todetermine whether the appearance and/or severityof ST abnormalities during exercise stress testing canaccurately predict the prevalence of ischemic burdenas measured by quantitative technetium-99m-sesta-mibi single-photon emission computed tomographicimaging in patients with LV hypertrophy. The resultsshow that the presence of exercise ST-segment de-pression, as well as its magnitude, are not accuratepredictors for identifying patients with coronary ar-tery disease in the presence of electrocardiographiccriteria for LV hypertrophy. �2004 by ExcerptaMedica, Inc.
(Am J Cardiol 2004;93:333–336)
Many patients with left ventricular (LV) hyper-trophy are referred for exercise stress testing to
detect coronary artery disease (CAD) and determineprognosis. In this patient population, ST-segment ab-normalities during exertion may not reflect ischemiasecondary to a flow-limiting stenosis. Little knowl-edge exists regarding the significance of either addi-tional ST depression in the presence of baseline de-pression or new stress-induced ST depression inpatients with LV hypertrophy. This investigation ex-amines whether the appearance and/or severity of STabnormalities during exercise stress testing can accu-rately predict the prevalence of myocardial ischemicburden in patients with LV hypertrophy by electrocar-diographic criteria.
• • •The study was a retrospective analysis of 679 pa-
tients at the University of Virginia from June 1, 1998,to May 30, 1999. Patients with atrioventricular block,left bundle branch block, pacemaker implantation, andwho used digoxin were excluded. Seventy-nine pa-tients (58 men and 21 women; mean age 58 � 14
years) fulfilled the standard criteria for LV hypertro-phy.1 Patients were referred for exercise stress testingand stress sestamibi with single-photon emission com-puted tomographic (SPECT) perfusion scanning at thebeginning of the study.
Patients underwent symptom-limited Bruce protocolexercise testing. Baseline supine 12-lead electrocardio-grams were inspected for abnormalities of the ST seg-ment and T wave. Exercise electrocardiograms wereinterpreted independently from the results of quantitativetechnetium-99m-sestamibi SPECT imaging. An isch-emic exercise electrocardiogram was defined as �1 mmof ST depression beyond that present on the electrocar-diogram recorded at rest (see Figures 1 and 2).
Patients in a fasting state were injected with 26 �1.5 mCi of technetium-99m sestamibi at exercise, andSPECT imaging was performed with images recon-structed by previously described computerized tech-niques.2 Imaging at rest was previously performedwith a lower dose of the imaging agent (8 to 10 mCi).A composite of the left ventricle was created by com-puter-assisted techniques and divided into 14 seg-ments for analysis of both regional perfusion andfunction. The average count for each segment wasdetermined by quantitative methods and expressed asa percentage of the segment with the greatest tracer
From Penn State Hershey Medical Center, Hershey, Pennsylvania;University of Chicago Hospitals, Chicago, Illinois; and University ofVirginia Health System, Charlottesville, Virginia. Dr. Beller’s address is:Box 800158, University of Virginia Health System, Charlottesville,Virginia 22908-0158. E-mail: [email protected]. Manuscript re-ceived July 31, 2003; revised manuscript received and acceptedOctober 3, 2003.
TABLE 1 Patient Characteristics and Results of ExerciseTreadmill Testing and Technetium-99m SPECT in Patients withElectrocardiographic (ECG) Evidence of Left VentricularHypertraphy (LVH)
Variable ECG-LVH
No. of patients N � 79Age (yrs) 58 � 13.8Men 58 (73%)� Blockers 22 (28%)Calcium channel blockers 12 (15%)Nitrates 10 (12%)METs 8.8 � 3.6Mean heart rate (beats/min) 138 � 23% Maximum achieved predicted heart rate
(beats/min)84 � 11%
Systolic blood pressure (mm Hg) 178 � 32Rate-pressure product 29 � 11Angina 8 (11%)Baseline ST abnormalities 9 (11%)ST abnormalities upon exertion 42 (53%)No. of scans with either reversible or irreversible
defects28 (35%)
No. of scans with only reversible defects 14 (18%)Ejection fraction 52.5 � 10%
333©2004 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matterThe American Journal of Cardiology Vol. 93 February 1, 2004 doi:10.1016/j.amjcard.2003.10.014

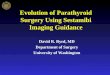
uptake.2 The presence of CAD was determined byaveraging the sestamibi uptake of each segment withassessment of abnormal wall motion on gated images(see Figure 3). Defects were classified as reversible ornonreversible according to previously described crite-ria and methods. Gender-specific normal databaseswere employed in this quantitative approach toSPECT analysis. Segments were classified as viable ifthey had �50% uptake on the scan at rest.3,4
Data are expressed as mean � 1 SD, except wherenoted. Univariate analysis of ST changes versus scanfindings within the LV hypertrophy group was per-formed by the chi-square test. Group differences wereconsidered significant at a p value of �0.05 (2-sided).
Table 1 lists the baseline characteristics of 79 pa-
tients with LV hypertrophy; 58% were men, and mostwere not taking cardiac medications. Abnormalities ofthe ST segment at baseline were seen in 11% ofpatients in the LV hypertrophy group. On exercisestress testing, 53% of the patients in the LV hypertro-phy group displayed ST depression. A perfusion scandepicting either reversible or irreversible defects wasseen in 35% of the LV hypertrophy group; only 18%had reversible defects.
Figure 4 is a graphic depiction relating the percent-age of perfusion scans showing abnormal uptake tothe degree of ST depression with exertion. The per-centage of perfusion scans exhibiting either reversibleor irreversible defects in patients with LV hypertrophyand 0 to 0.9, 1.0 to 1.9, and �2 mm of ST depression
FIGURE 1. Electrocar-diogram at rest in arepresentative patientshowing typical voltageand ST-T wave changesof LV hypertrophy.
FIGURE 2. The exerciseelectrocardiogram in thesame patient as Figure 1,showing additional ST-segment depression atpeak exercise.
334 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 93 FEBRUARY 1, 2004

were 28%, 41%, and 43%, respectively, suggestingthat most patients with LV hypertrophy and STchanges during exercise have normal scans.
Also, of the patients with LV hypertrophy withadditional ST depression during exertion, 43% hadabnormal sestamibi perfusion scans (p � 0.27). Thus,less than half of the patients with additional ST de-pression during exercise had an abnormal scan.
• • •
Our study was a retrospectiveanalysis of 679 patients conductedto examine whether the occurrenceof ST depression on exercise testinghas any value in detecting CAD inpatients with LV hypertrophy, as de-fined by electrocardiographic crite-ria. The presence of CAD was de-termined by gated technetium-99msestamibi SPECT imaging, whichhas been shown to display a highspecificity in a previous study.5
With respect to patients with LVhypertrophy referred for stress test-ing, our results show that 11% hadbaseline ST abnormalities and 53%displayed ST depression during ex-ercise stress testing. Only 35% ofthe patients with LV hypertrophywere found to have any reversible orfixed defects by SPECT criteria. As-sociations between ST depressionand evidence of CAD have beenfound to be inconsistent in numer-ous previous studies.6–8 Massie etal9 showed that exercise and ambu-latory electrocardiograms appearedto yield false-positive results in pa-
tients with echocardiographic evidence of LV hyper-trophy. Patient characteristics and selection bias havebeen known to influence the sensitivity and specificityof exercise stress tests in previous investigations.10,11
No previously reported study has examined pa-tients with LV hypertrophy for the relation betweenthe degree of ST depression during exertion and itscorrelation with SPECT perfusion abnormalities. Fig-ure 4 shows that of those subjects with LV hypertro-phy and 0 to 0.9, 1 to 1.9, and �2 mm of ST depres-sion, the corresponding frequency of perfusion scanswith reversible or fixed defects were 28%, 41%, and43%, respectively. The sensitivity and specificity ofST changes during stress testing for the diagnosis ofCAD was 64% and 52% for the LV hypertrophygroup, respectively. Thus, these data show no signif-icant relation between the occurrence and/or magni-tude of ST depression and the prevalence of perfusiondefects in patients with LV hypertrophy.
Several other studies have also shown a poor corre-lation between exercise ST-segment depression and un-derlying CAD in patients with LV hypertrophy. Mar-wick et al12 studied 147 patients and found that thespecificity of ST-segment interpretation is compromisedin patients with LV hypertrophy, even in patients who donot have ST-segment changes at rest. Alshami et al13
concluded that many patients with LV hypertrophy di-agnosed by electrocardiographic criteria had normal per-fusion scans (73%) on exercise despite a high incidenceof additional electrocardiographic changes (76%). Whencomparing the results of our study, which utilized tech-netium-99m-sestamibi perfusion scans, it is important tonotice the differences between the modalities detectingCAD (arteriography12 vs thallium13). The limitations of
FIGURE 4. Relation between ST depression during exertion andtechnetium-99m-sestamibi SPECT results in patients with LVhypertrophy.
FIGURE 3. Stress and technetium-99m-sestamibi images at rest showing apical, mid-ventricular, and basilar tomograms. Note that there is a reversible defect in the infe-rior wall as well as reversibility in the apex. The numbers in the diagrams below theimages represent the percent technetium-99m-sestamibi uptake in various segmentsduring stress (top numbers) and at rest (bottom numbers). For the mid-inferior defect,there was a 16% change from stress to at rest, indicating reversibility. This reversibil-ity was statistically significant (*2 SDs from the normal variation from stress to imagesat rest). Finally, there is also a mild reversible defect in the anterior wall.
BRIEF REPORTS 335

technetium-99m-sestamibi SPECT include interpretationof attenuation artifacts as defects attributed to CAD, poorquality images in obese patients, and lower sensitivity indetecting mild stenoses of 50% to 70% in diametercompared with more severe lesions. Also, if patients areimaged while taking antianginal drugs, such as � block-ers and nitrates, sensitivity may be diminished.
The present study also sought to determine whetherthe degree of ST-segment depression corresponded tothe frequency of perfusion abnormalities on techne-tium-99m-sestamibi SPECT in a population of pa-tients with LV hypertrophy. Our results indicate thatwith similar levels of exercise, patients with a greatermagnitude of ST depression do not have a correspond-ing higher frequency of abnormal perfusion defectscompared with patients with lesser magnitudes of STdepression. Moreover, we found that many patients inthe LV hypertrophy subpopulation exhibited ischemicelectrocardiographic changes during exercise but nodefects on perfusion imaging.
Limitations of our study include its retrospectiveanalysis, its specific patient population with LV hy-pertrophy, its high percentage of men, and the limita-tions of the electrocardiogram in diagnosing patientswith LV hypertrophy.
1. Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP.Determinants of sensitivity and specificity of electrocardiographic criteria for leftventricular hypertrophy. Circulation 1990;81:815–820.
2. Smith WH, Kastner RJ, Calnon DA, Segalla D, Beller GA, Watson DD.Quantitative gated single photo emission computed tomography imaging: acounts-based method for display and measurement of regional and global ven-tricular systolic function. J Nucl Cardiol 1997;4:451–463.3. Marzullo P, Sambuceti G, Parodi O. The role of sestamibi scintigraphy in theradioisotopic assessment of myocardial viability. J Nucl Med 1992;33:1925–1930.4. Kauffman GJ, Boyne TS, Watson DD, Smith WH, Beller GA. Comparison ofrest thallium 201 imaging and rest technetium-99m sestamibi imaging for assess-ment of myocardial viability in patients with coronary artery disease and severeleft ventricular dysfunction. J Am Coll Cardiol 199;27:1592–1597.5. Smanio P, Watson DD, Segalla DL, Vinson EL, Smith WH, Beller GA. Valueof gating of technetium-99m sestamibi single-photon emission computed tomo-graphic imaging. J Am Coll Cardiol 1997;30:1687–1692.6. Mark DB, Hlatky MA, Harrell FE, Lee KL, Califf RM, Pryor DB. Exercisetreadmill score for predicting prognosis in coronary artery disease. Ann InternMed 1987;106:793–800.7. Mark DB, Shaw L, Harrell FE, Hlatky MA, Lee KL, Bengtson JR, McCantsCB, Califf RM, Pryor DB. Prognostic value of a treadmill exercise score inoutpatients with suspected coronary artery disease. N Engl J Med 1991;325:849–853.8. Froelicher VF, Thomas MM, Pillow C, Lancaster MC. Epidemiologic study ofasymptomatic men screened by maximal treadmill testing for latent coronaryartery disease. Am J Cardiol 1974;34:770–776.9. Massie BM, Szlachcic Y, Tubau JF, O’Kelly BF, Ammon S, Chin W.Scintigraphic and electrocardiographic evidence of silent coronary artery diseasein asymptomatic hypertension: a case control study. J Am Coll Cardiol 1993;22:1598–1606.10. Hlatky MA, Pryor DB, Harrell FE, Califf RM, Mark DB, Rosati RA. Factorsaffecting sensitivity and specificity of exercise electrocardiography. Am J Med1984;77:64–71.11. Philbrick JT, Horowitz RI, Feinstein AR, Langou RA, Chandler JP. Thelimited spectrum of patients studied in exercise test research. JAMA 1982;248:2467–2470.12. Marwick TH, Torelli J, Harjai K, Haluska B, Pashkow F, Stewart W, ThomasJT. Influence of left ventricular hypertrophy on detection of coronary arterydisease using exercise echocardiography. J Am Coll Cardiol 1995;26:1180–1186.13. Alshami A, Jolly S, Smith F, Reeves W, Movahed A. Exercise testing inpatients with electrocardiographic evidence of left ventricular hypertrophy. ClinNucl Med 1994;19:904–909.
Prevalence of Anxiety in Coronary Patients WithImprovement Following Cardiac Rehabilitation and
Exercise Training
Carl J. Lavie, MD, and Richard V. Milani, MD
Numerous studies have indicated that psychologicaldistress, including anxiety, is a significant risk factorfor coronary artery disease (CAD). We studied 500consecutive patients after recent CAD events anddemonstrated a very high prevalence of generalizedanxiety and moderate to severe anxiety symptoms,particularly in younger patients. In addition, our datademonstrate the abnormal CAD risk profiles in theseanxious patients with CAD and the marked improve-ments in the overall risk profiles, levels of anxiety,and overall quality of life after cardiac rehabilitationand exercise training programs. Greater attention atdetecting and treating chronic anxiety, particularly
with formal cardiac rehabilitation, is needed for thesecondary prevention of CAD. �2004 by ExcerptaMedica, Inc.
(Am J Cardiol 2004;93:336–339)
Numerous studies indicate that psychological dis-tress is a significant risk factor for coronary ar-
tery disease (CAD), which adversely affects recoveryafter major CAD events.1 Although most studies focuson depression and hostility,2–6 acute and chronic anx-iety also adversely affect cardiovascular risk.1,7–9 Weand others have demonstrated the beneficial effects ofcardiac rehabilitation and exercise training programson improving exercise capacity, obesity indexes,plasma lipids, and behavioral characteristics, espe-cially depression and hostility,2–6 as well as reducingsubsequent hospitalization costs and overall morbidityand mortality.10,11 To our knowledge, however, onlylimited information is available on the effects of thistherapy in patients with CAD with high levels ofanxiety.
From the Ochsner Heart and Vascular Institute, Ochsner Clinic Foun-dation, New Orleans, Lousiana. Dr. Lavie’s address is: Department ofCardiology; Ochsner Clinic Foundation, 1514 Jefferson Highway;New Orleans, Lousiana 70121. E-mail: [email protected]. Manu-script received July 24, 2003; revised manuscript received and ac-cepted October 2, 2003.
336 ©2004 by Excerpta Medica, Inc. All rights reserved. 0002-9149/04/$–see front matterThe American Journal of Cardiology Vol. 93 February 1, 2004 doi:10.1016/j.amjcard.2003.10.015